Comparison of Walking Protocols and Gait Assessment Systems for Machine Learning-Based Classification of Parkinson’s Disease

 ,
,  ,
, 
Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Demographic and Clinical Measures
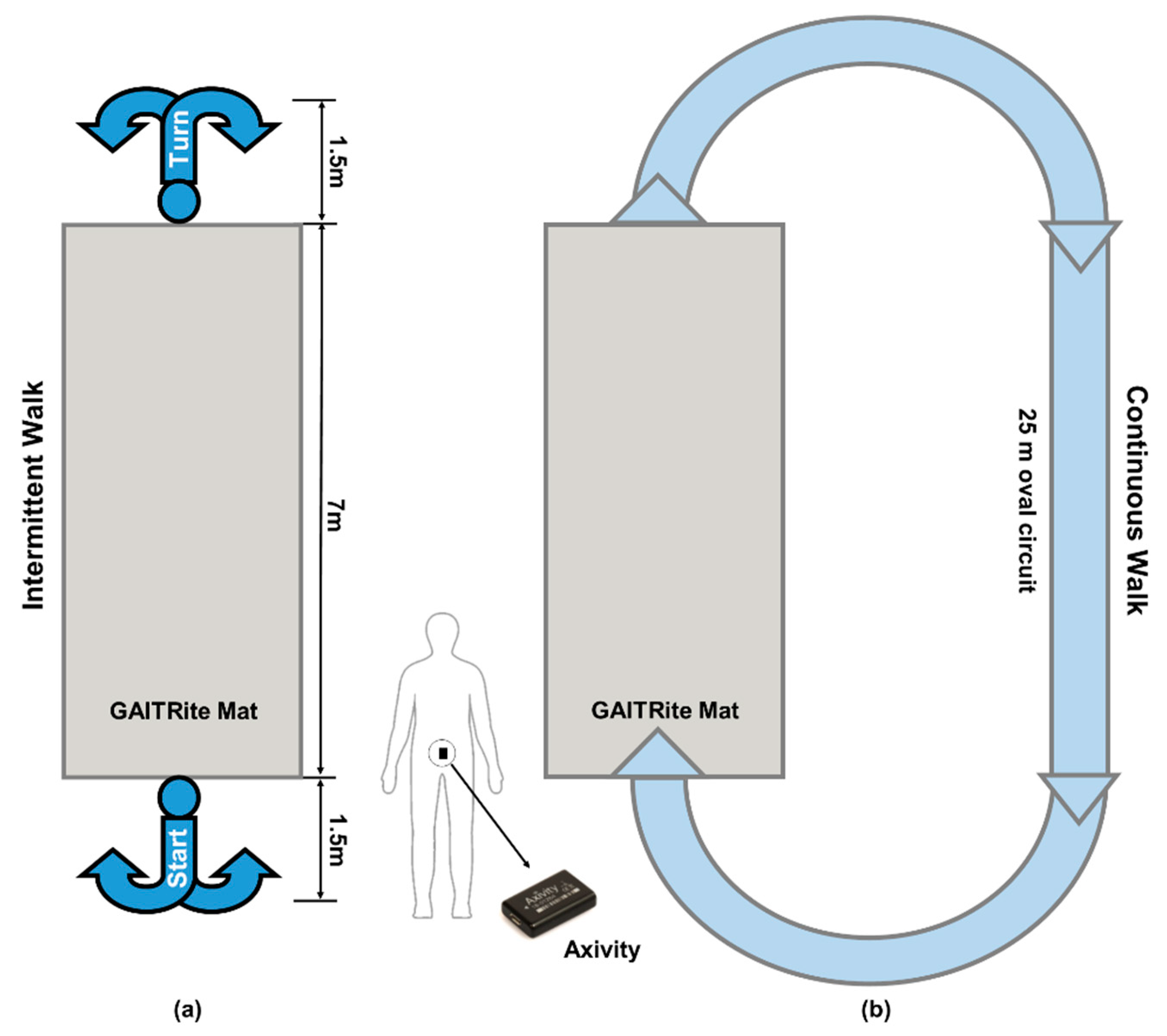
2.3. Walking Protocols and Data Collection
- (1)
- (2)
- Two minute continuous walking test (CW). Participants were asked to walk continuously around at 25 m oval circuit at their preferred speed (Figure 1b).
2.4. Gait Assessment Systems
2.5. Data Processing and Gait Characteristics Extraction
2.6. Statistical Analysis, Gait Normalization and Classification Modeling
3. Results
4. Discussion
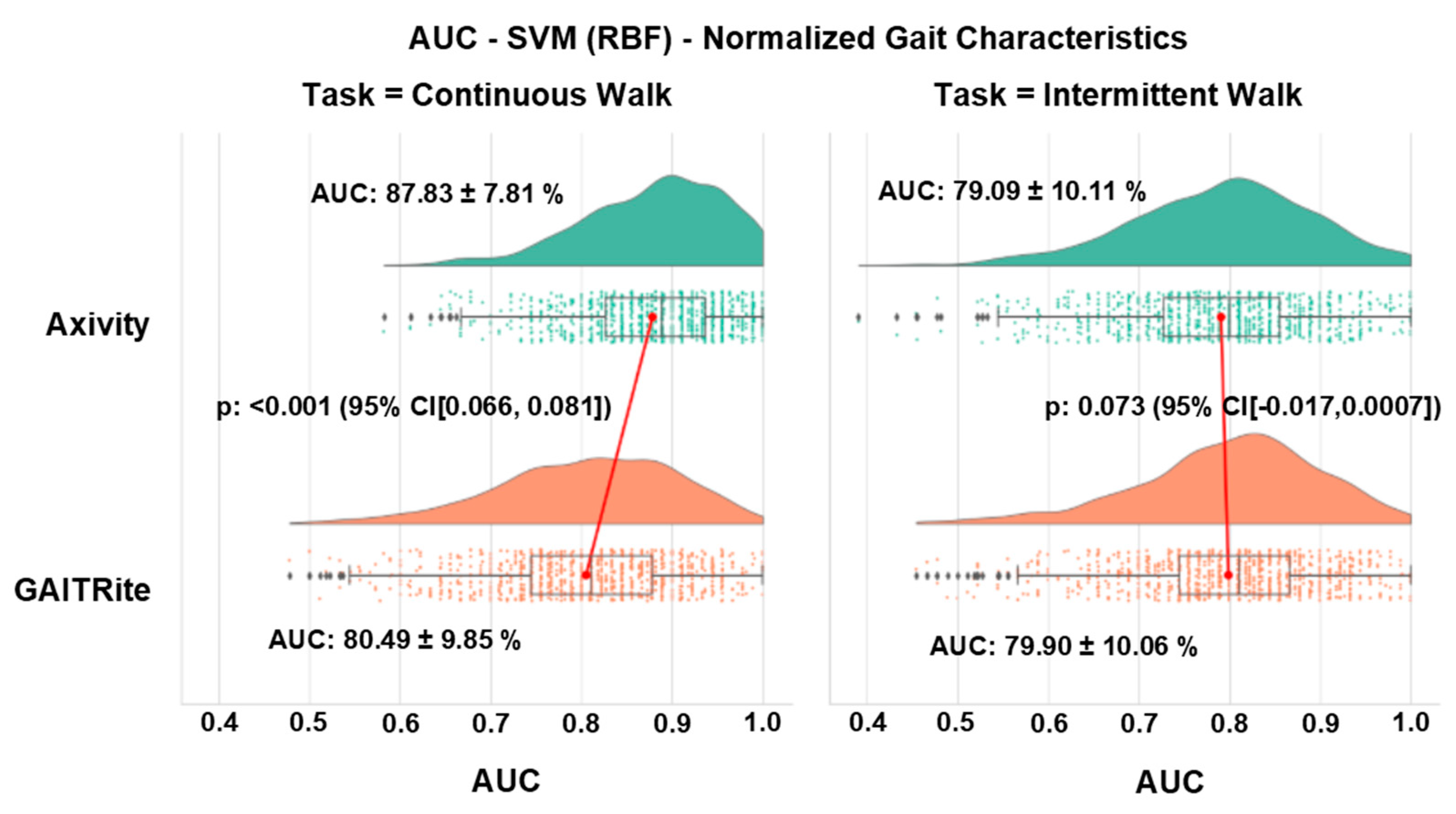
4.1. ML Performance: An Overview
4.2. Effect of Walking Protocols on ML Model and Performance
4.3. Effect of Gait Assessment Systems on ML Model and Performance
4.4. Effect of Gait Normalization on ML Performance
4.5. Limitations
5. Clinical Implications
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Dorsey, E.R.; George, B.P.; Leff, B.; Willis, A.W. The coming crisis: Obtaining care for the growing burden of neurodegenerative conditions. Neurology 2013, 80, 1989–1996. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jankovic, J. Parkinson’s disease: Clinical features and diagnosis. J. Neurol. Neurosurg. Psychiatry 2008, 79, 368–376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perez-Lloret, S.; Negre-Pages, L.; Damier, P.; Delval, A.; Derkinderen, P.; Destee, A.; Meissner, W.G.; Schelosky, L.; Tison, F.; Rascol, O. Prevalence, determinants, and effect on quality of life of freezing of gait in parkinson disease. JAMA Neurol. 2014, 71, 884–890. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- von Campenhausen, S.; Winter, Y.; e Silva, A.R.; Sampaio, C.; Ruzicka, E.; Barone, P.; Poewe, W.; Guekht, A.; Mateus, C.; Pfeiffer, K.-P. Costs of illness and care in parkinson’s disease: An evaluation in six countries. Eur. Neuropsychopharmacol. 2011, 21, 180–191. [Google Scholar] [CrossRef]
- Hoehn, M.M.; Yahr, M.D. Parkinsonism: Onset, progression, and mortality. Neurology 1998, 50, 318. [Google Scholar] [CrossRef]
- Buckley, C.; Alcock, L.; McArdle, R.; Rehman, R.Z.U.; Del Din, S.; Mazzà, C.; Yarnall, A.J.; Rochester, L. The role of movement analysis in diagnosing and monitoring neurodegenerative conditions: Insights from gait and postural control. Brain Sci. 2019, 9, 34. [Google Scholar] [CrossRef] [Green Version]
- Mirelman, A.; Bonato, P.; Camicioli, R.; Ellis, T.D.; Giladi, N.; Hamilton, J.L.; Hass, C.J.; Hausdorff, J.M.; Pelosin, E.; Almeida, Q.J. Gait impairments in parkinson’s disease. Lancet Neurol. 2019, 18, 697–708. [Google Scholar] [CrossRef]
- Del Din, S.; Elshehabi, M.; Galna, B.; Hobert, M.A.; Warmerdam, E.; Suenkel, U.; Brockmann, K.; Metzger, F.; Hansen, C.; Berg, D. Gait analysis with wearables predicts conversion to parkinson disease. Ann. Neurol. 2019, 86, 357–367. [Google Scholar] [CrossRef]
- Del Din, S.; Hickey, A.; Hurwitz, N.; Mathers, J.C.; Rochester, L.; Godfrey, A. Measuring gait with an accelerometer-based wearable: Influence of device location, testing protocol and age. Physiol. Meas. 2016, 37, 1785. [Google Scholar] [CrossRef]
- Del Din, S.; Godfrey, A.; Rochester, L. Validation of an accelerometer to quantify a comprehensive battery of gait characteristics in healthy older adults and parkinson’s disease: Toward clinical and at home use. IEEE J. Biomed. Health Inf. 2016, 20, 838–847. [Google Scholar] [CrossRef]
- Lord, S.; Galna, B.; Verghese, J.; Coleman, S.; Burn, D.; Rochester, L. Independent domains of gait in older adults and associated motor and nonmotor attributes: Validation of a factor analysis approach. J. Gerontol. Ser. A 2013, 68, 820–827. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lord, S.; Galna, B.; Rochester, L. Moving forward on gait measurement: Toward a more refined approach. Mov. Disord. 2013, 28, 1534–1543. [Google Scholar] [CrossRef] [PubMed]
- Klucken, J.; Barth, J.; Kugler, P.; Schlachetzki, J.; Henze, T.; Marxreiter, F.; Kohl, Z.; Steidl, R.; Hornegger, J.; Eskofier, B. Unbiased and mobile gait analysis detects motor impairment in parkinson’s disease. PLoS ONE 2013, 8, e56956. [Google Scholar] [CrossRef] [PubMed]
- Caramia, C.; Torricelli, D.; Schmid, M.; Munoz-Gonzalez, A.; Gonzalez-Vargas, J.; Grandas, F.; Pons, J.L. Imu-based classification of parkinson’s disease from gait: A sensitivity analysis on sensor location and feature selection. IEEE J. Biomed. Health Inf. 2018, 22, 1765–1774. [Google Scholar] [CrossRef] [PubMed]
- Tahir, N.M.; Manap, H.H. Parkinson disease gait classification based on machine learning approach. J. Appl. Sci. 2012, 12, 180–185. [Google Scholar] [CrossRef]
- Wahid, F.; Begg, R.K.; Hass, C.J.; Halgamuge, S.; Ackland, D.C. Classification of parkinson’s disease gait using spatial-temporal gait features. IEEE J. Biomed. Health Inf. 2015, 19, 1794–1802. [Google Scholar] [CrossRef]
- Djurić-Jovičić, M.; Belić, M.; Stanković, I.; Radovanović, S.; Kostić, V.S. Selection of gait parameters for differential diagnostics of patients with de novo parkinson’s disease. Neurol. Res. 2017, 39, 853–861. [Google Scholar] [CrossRef]
- Pham, T.D.; Yan, H. Tensor decomposition of gait dynamics in parkinson’s disease. IEEE Trans. Biomed. Eng. 2018, 65, 1820–1827. [Google Scholar]
- Alam, M.N.; Garg, A.; Munia, T.T.K.; Fazel-Rezai, R.; Tavakolian, K. Vertical ground reaction force marker for parkinson’s disease. PLoS ONE 2017, 12, e0175951. [Google Scholar] [CrossRef]
- Galna, B.; Lord, S.; Burn, D.J.; Rochester, L. Progression of gait dysfunction in incident parkinson’s disease: Impact of medication and phenotype. Mov. Disord. 2015, 30, 359–367. [Google Scholar] [CrossRef]
- Galna, B.; Lord, S.; Rochester, L. Is gait variability reliable in older adults and parkinson’s disease? Towards an optimal testing protocol. Gait Posture 2013, 37, 580–585. [Google Scholar] [CrossRef] [PubMed]
- Godinho, C.; Domingos, J.; Cunha, G.; Santos, A.T.; Fernandes, R.M.; Abreu, D.; Gonçalves, N.; Matthews, H.; Isaacs, T.; Duffen, J.; et al. A systematic review of the characteristics and validity of monitoring technologies to assess parkinson’s disease. J. Neuroeng. Rehabil. 2016, 13. [Google Scholar]
- Qiu, H.; Rehman, R.Z.U.; Yu, X.; Xiong, S. Application of wearable inertial sensors and a new test battery for distinguishing retrospective fallers from non-fallers among community-dwelling older people. Sci. Rep. 2018, 8, 16349. [Google Scholar] [CrossRef] [PubMed]
- Godfrey, A.; Del Din, S.; Barry, G.; Mathers, J.C.; Rochester, L. Instrumenting gait with an accelerometer: A system and algorithm examination. Med Eng. Phys. 2015, 37, 400–407. [Google Scholar] [CrossRef] [PubMed]
- Morris, M.E. Locomotor training in people with parkinson disease. Phys. Ther. 2006, 86, 1426–1435. [Google Scholar] [CrossRef] [Green Version]
- Herman, T.; Giladi, N.; Gurevich, T.; Hausdorff, J. Gait instability and fractal dynamics of older adults with a “cautious” gait: Why do certain older adults walk fearfully? Gait Posture 2005, 21, 178–185. [Google Scholar] [CrossRef]
- Kang, H.G.; Dingwell, J.B. Separating the effects of age and walking speed on gait variability. Gait Posture 2008, 27, 572–577. [Google Scholar] [CrossRef]
- Andriacchi, T.; Ogle, J.; Galante, J. Walking speed as a basis for normal and abnormal gait measurements. J. Biomech. 1977, 10, 261–268. [Google Scholar] [CrossRef]
- Kirtley, C.; Whittle, M.W.; Jefferson, R. Influence of walking speed on gait parameters. J. Biomed. Eng. 1985, 7, 282–288. [Google Scholar] [CrossRef]
- Schwartz, M.H.; Rozumalski, A.; Trost, J.P. The effect of walking speed on the gait of typically developing children. J. Biomech. 2008, 41, 1639–1650. [Google Scholar] [CrossRef]
- Kamruzzaman, J.; Begg, R.K. Support vector machines and other pattern recognition approaches to the diagnosis of cerebral palsy gait. IEEE Trans. Biomed. Eng. 2006, 53, 2479–2490. [Google Scholar] [CrossRef] [PubMed]
- Khoo, T.K.; Yarnall, A.J.; Duncan, G.W.; Coleman, S.; O’Brien, J.T.; Brooks, D.J.; Barker, R.A.; Burn, D.J. The spectrum of nonmotor symptoms in early parkinson disease. Neurology 2013, 80, 276–281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tombaugh, T.N.; McIntyre, N.J. The mini-mental state examination: A comprehensive review. J. Am. Geriatr. Soc. 1992, 40, 922–935. [Google Scholar] [CrossRef] [PubMed]
- Powell, L.E.; Myers, A.M. The activities-specific balance confidence (abc) scale. J. Gerontol. Ser. A Biol. Sci. Med Sci. 1995, 50, M28–M34. [Google Scholar] [CrossRef] [PubMed]
- Goetz, C.G.; Tilley, B.C.; Shaftman, S.R.; Stebbins, G.T.; Fahn, S.; Martinez-Martin, P.; Poewe, W.; Sampaio, C.; Stern, M.B.; Dodel, R. Movement disorder society-sponsored revision of the unified parkinson’s disease rating scale (mds-updrs): Scale presentation and clinimetric testing results. Mov. Disord. Off. J. Mov. Disord. Soc. 2008, 23, 2129–2170. [Google Scholar] [CrossRef] [PubMed]
- Stebbins, G.T.; Goetz, C.G.; Burn, D.J.; Jankovic, J.; Khoo, T.K.; Tilley, B.C. How to identify tremor dominant and postural instability/gait difficulty groups with the movement disorder society unified parkinson’s disease rating scale: Comparison with the unified parkinson’s disease rating scale. Mov. Disord. 2013, 28, 668–670. [Google Scholar] [CrossRef]
- Lawson, R.A.; Yarnall, A.J.; Duncan, G.W.; Breen, D.P.; Khoo, T.K.; Williams-Gray, C.H.; Barker, R.A.; Collerton, D.; Taylor, J.-P.; Burn, D.J. Cognitive decline and quality of life in incident parkinson’s disease: The role of attention. Parkinsonism Relat. Disord. 2016, 27, 47–53. [Google Scholar] [CrossRef] [Green Version]
- Tomlinson, C.L.; Stowe, R.; Patel, S.; Rick, C.; Gray, R.; Clarke, C.E. Systematic review of levodopa dose equivalency reporting in parkinson’s disease. Mov. Disord. 2010, 25, 2649–2653. [Google Scholar] [CrossRef]
- Allen, M.; Poggiali, D.; Whitaker, K.; Marshall, T.R.; Kievit, R. Raincloud plots: A multi-platform tool for robust data visualization. PeerJ Prepr. 2018, 6, e27137v1. [Google Scholar] [CrossRef] [Green Version]
- Rehman, R.Z.U.; Del Din, S.; Guan, Y.; Yarnall, A.J.; Shi, J.Q.; Rochester, L. Selecting clinically relevant gait characteristics for classification of early parkinson’s disease: A comprehensive machine learning approach. Sci. Rep. 2019, 9, 17269. [Google Scholar] [CrossRef] [Green Version]
- Bradley, A.P. The use of the area under the roc curve in the evaluation of machine learning algorithms. Pattern Recognit. 1997, 30, 1145–1159. [Google Scholar] [CrossRef] [Green Version]
- Guyon, I.; Elisseeff, A. An introduction to variable and feature selection. J. Mach. Learn. Res. 2003, 3, 1157–1182. [Google Scholar]
- Guyon, I.; Weston, J.; Barnhill, S.; Vapnik, V. Gene selection for cancer classification using support vector machines. Mach. Learn. 2002, 46, 389–422. [Google Scholar] [CrossRef]
- Pedregosa, F.; Varoquaux, G.; Gramfort, A.; Michel, V.; Thirion, B.; Grisel, O.; Blondel, M.; Prettenhofer, P.; Weiss, R.; Dubourg, V. Scikit-learn: Machine learning in python. J. Mach. Learn. Res. 2011, 12, 2825–2830. [Google Scholar]
- Cuzzolin, F.; Sapienza, M.; Esser, P.; Saha, S.; Franssen, M.M.; Collett, J.; Dawes, H. Metric learning for parkinsonian identification from imu gait measurements. Gait Posture 2017, 54, 127–132. [Google Scholar] [CrossRef] [Green Version]
- Arora, S.; Venkataraman, V.; Donohue, S.; Biglan, K.M.; Dorsey, E.R.; Little, M.A. High accuracy discrimination of parkinson’s disease participants from healthy controls using smartphones. In Proceedings of the 2014 IEEE International Conference on Acoustics, Speech and Signal Processing (ICASSP), Florence, Italy, 4–9 May 2014; pp. 3641–3644. [Google Scholar]
- Webster, K.E.; Wittwer, J.E.; Feller, J.A. Validity of the gaitrite® walkway system for the measurement of averaged and individual step parameters of gait. Gait Posture 2005, 22, 317–321. [Google Scholar] [CrossRef]
- Bilney, B.; Morris, M.; Webster, K. Concurrent related validity of the gaitrite® walkway system for quantification of the spatial and temporal parameters of gait. Gait Posture 2003, 17, 68–74. [Google Scholar] [CrossRef]
- Panebianco, G.P.; Bisi, M.C.; Stagni, R.; Fantozzi, S. Analysis of the performance of 17 algorithms from a systematic review: Influence of sensor position, analysed variable and computational approach in gait timing estimation from imu measurements. Gait Posture 2018, 66, 76–82. [Google Scholar] [CrossRef]
- Buganè, F.; Benedetti, M.G.; D’Angeli, V.; Leardini, A. Estimation of pelvis kinematics in level walking based on a single inertial sensor positioned close to the sacrum: Validation on healthy subjects with stereophotogrammetric system. Biomed. Eng. Online 2014, 13, 146. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Demographics | HC (n = 103) Mean ± SD | PD (n = 93) Mean ± SD | p |
|---|---|---|---|
| M/F | 49/54 | 59/34 | 0.026 |
| Age (years) | 72.3 ± 6.7 | 69.2 ± 10.1 | 0.012 |
| Height (m) | 1.7 ± 0.09 | 1.7 ± 0.09 | 0.623 |
| Mass (kg) | 78.6 ± 14.3 | 78.6 ± 15.9 | 0.999 |
| BMI (kg/m²) 1 | 27.2 ± 5.6 | 27.5 ± 4.7 | 0.750 |
| MMSE (0–30) 2 | 28.9 ± 1.9 | 28.4 ± 1.6 | 0.102 |
| ABCs (0–100)% 3 | 91.2 ± 13.8 | 80.6 ± 20.7 | <0.001 |
| LEDD, mg/day 4 | 397.7 ± 217.2 | ||
| Disease Duration (months) | 23.8 ± 4.2 | ||
| Hoehn & Yahr (n) | HY I: 8 | ||
| HY II: 71 | |||
| HY III: 14 | |||
| MDS-UPDRS III 5 | 32.4 ± 10.3 | ||
| (HY I: 17.4 ± 4.5) | |||
| (HY II: 32.9 ± 9.7) | |||
| (HY III: 38.1 ± 7.5) | |||
| Motor Phenotype (n) | 6 PIGD: 34 | ||
| 7 ID: 16 | |||
| 8 TD: 43 |
| Effect Assessment on Gait | MANOVA | ||
|---|---|---|---|
| Wilk’s Lambda | F | p-Value | |
| Group (HC & PD) | 0.803 | 14.198 | <0.001 |
| Walking Protocols | 0.463 | 67.337 | <0.001 |
| Gait Assessment Systems | 0.067 | 805.792 | <0.001 |
| Group * Protocol | 0.949 | 3.092 | <0.001 |
| Group * Systems | 0.853 | 9.991 | <0.001 |
| Protocols * Systems | 0.513 | 55.168 | <0.001 |
| Gait Domains | Gait Characteristics | Intermittent Walk (IW) | Continuous Walk (CW) | ||||
|---|---|---|---|---|---|---|---|
| HC (n = 103) Mean ± SD | PD (n = 93) Mean ± SD | p Value | HC (n = 103) Mean ± SD | PD (n = 93) Mean ± SD | p Value | ||
| Gait Characteristics from Axivity | |||||||
| Pace | Step Velocity (m/s) | 1.324 ± 0.153 | 1.252 ± 0.226 | 0.002 | 1.283 ± 0.155 | 1.186 ± 0.262 | 0.009 |
| Step Length (m) | 0.718 ± 0.094 | 0.717 ± 0.074 | 0.010 | 0.694 ± 0.121 | 0.690 ± 0.077 | 0.022 | |
| Swing Time Variability (s) | 0.064 ± 0.084 | 0.123 ± 0.144 | <0.001 | 0.037 ± 0.031 | 0.108 ± 0.082 | 0.058 | |
| Rhythm | Step Time (s) | 0.554 ± 0.052 | 0.614 ± 0.129 | 0.001 | 0.538 ± 0.046 | 0.609 ± 0.133 | <0.001 |
| Swing Time (s) | 0.394 ± 0.047 | 0.448 ± 0.116 | 0.001 | 0.386 ± 0.044 | 0.454 ± 0.125 | <0.001 | |
| Stance Time (s) | 0.705 ± 0.059 | 0.767 ± 0.141 | 0.003 | 0.689 ± 0.054 | 0.763 ± 0.144 | <0.001 | |
| Variability | Step Velocity Variability (m/s) | 0.174 ± 0.097 | 0.196 ± 0.078 | 0.273 | 0.137 ± 0.060 | 0.190 ± 0.076 | <0.001 |
| Step Length Variability (m) | 0.101 ± 0.060 | 0.126 ± 0.059 | 0.022 | 0.072 ± 0.034 | 0.109 ± 0.044 | <0.001 | |
| Step Time Variability (s) | 0.093 ± 0.103 | 0.162 ± 0.157 | <0.001 | 0.037 ± 0.033 | 0.114 ± 0.087 | <0.001 | |
| Stance Time Variability (s) | 0.094 ± 0.103 | 0.166 ± 0.158 | 0.001 | 0.039 ± 0.033 | 0.116 ± 0.088 | <0.001 | |
| Asymmetry | Step Time Asymmetry (s) | 0.031 ± 0.018 | 0.051 ± 0.034 | 0.610 | 0.021 ± 0.016 | 0.026 ± 0.025 | 0.268 |
| Swing Time Asymmetry (s) | 0.023 ± 0.017 | 0.039 ± 0.028 | 0.437 | 0.020 ± 0.018 | 0.023 ± 0.024 | 0.592 | |
| Stance Time Asymmetry (s) | 0.030 ± 0.019 | 0.044 ± 0.027 | 0.771 | 0.020 ± 0.018 | 0.024 ± 0.02 | 0.419 | |
| Postural Control | Step length Asymmetry (m) | 0.078 ± 0.053 | 0.119 ± 0.112 | 0.606 | 0.066 ± 0.052 | 0.126 ± 0.128 | 0.060 |
| Gait Characteristics from GAITRite | |||||||
| Pace | Step Velocity (m/s) | 1.338 ± 0.198 | 1.194 ± 0.223 | <0.001 | 1.301 ± 0.192 | 1.135 ± 0.218 | <0.001 |
| Step Length (m) | 0.697 ± 0.084 | 0.636 ± 0.098 | <0.001 | 0.683 ± 0.083 | 0.616 ± 0.097 | <0.001 | |
| Swing Time Variability (s) | 0.013 ± 0.003 | 0.016 ± 0.008 | 0.327 | 0.013 ± 0.004 | 0.017 ± 0.009 | 0.010 | |
| Rhythm | Step Time (s) | 0.525 ± 0.045 | 0.538 ± 0.047 | <0.001 | 0.528 ± 0.044 | 0.548 ± 0.047 | <0.001 |
| Swing Time (s) | 0.385 ± 0.030 | 0.382 ± 0.033 | <0.001 | 0.385 ± 0.029 | 0.384 ± 0.031 | 0.001 | |
| Stance Time (s) | 0.665 ± 0.068 | 0.695 ± 0.072 | <0.001 | 0.674 ± 0.066 | 0.714 ± 0.074 | <0.001 | |
| Variability | Step Velocity Variability (m/s) | 0.051 ± 0.015 | 0.047 ± 0.014 | 0.946 | 0.050 ± 0.012 | 0.054 ± 0.014 | 0.005 |
| Step Length Variability (m) | 0.019 ± 0.006 | 0.020 ± 0.007 | 0.008 | 0.020 ± 0.006 | 0.023 ± 0.007 | 0.338 | |
| Step Time Variability (s) | 0.014 ± 0.004 | 0.016 ± 0.007 | 0.173 | 0.014 ± 0.004 | 0.018 ± 0.006 | 0.018 | |
| Stance Time Variability (s) | 0.016 ± 0.005 | 0.019 ± 0.011 | 0.260 | 0.017 ± 0.006 | 0.023 ± 0.012 | 0.011 | |
| Asymmetry | Step Time Asymmetry (s) | 0.011 ± 0.008 | 0.018 ± 0.018 | 0.003 | 0.012 ± 0.009 | 0.019 ± 0.022 | 0.007 |
| Swing Time Asymmetry (s) | 0.007 ± 0.006 | 0.014 ± 0.014 | <0.001 | 0.007 ± 0.006 | 0.014 ± 0.014 | 0.003 | |
| Stance Time Asymmetry (s) | 0.007 ± 0.006 | 0.014 ± 0.014 | 0.476 | 0.007 ± 0.006 | 0.015 ± 0.015 | <0.001 | |
| Postural Control | Step length Asymmetry (m) | 0.020 ± 0.016 | 0.022 ± 0.018 | 0.048 | 0.019 ± 0.015 | 0.022 ± 0.020 | 0.036 |
| Sensing System | Intermittent Walk | Continuous Walk | ||
|---|---|---|---|---|
| Characteristic | Importance | Characteristic | Importance | |
| Axivity | Mean Step Length | 0.22 | Step Velocity Variability | 1.10 |
| Mean Stance Time | 0.20 | Mean Swing Time | 0.72 | |
| Mean Swing Time | 0.15 | Mean Step Length | 0.49 | |
| Swing Time Variability | 0.14 | Stance Time Variability | 0.20 | |
| Mean Step Time | 0.07 | Step Length Variability | 0.12 | |
| GAITRite | Mean Step Time | 0.23 | Mean Step Length | 3.80 |
| Step Velocity Variability | 0.22 | Mean Step Time | 2.72 | |
| Step Length Variability | 0.15 | Stance Time Asymmetry | 1.21 | |
| Swing Time Variability | 0.14 | Mean Stance Time | 1.10 | |
| Mean Step Length | 0.09 | Swing Time Asymmetry | 0.72 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rehman, R.Z.U.; Del Din, S.; Shi, J.Q.; Galna, B.; Lord, S.; Yarnall, A.J.; Guan, Y.; Rochester, L. Comparison of Walking Protocols and Gait Assessment Systems for Machine Learning-Based Classification of Parkinson’s Disease. Sensors 2019, 19, 5363. https://doi.org/10.3390/s19245363
Rehman RZU, Del Din S, Shi JQ, Galna B, Lord S, Yarnall AJ, Guan Y, Rochester L. Comparison of Walking Protocols and Gait Assessment Systems for Machine Learning-Based Classification of Parkinson’s Disease. Sensors. 2019; 19(24):5363. https://doi.org/10.3390/s19245363
Chicago/Turabian StyleRehman, Rana Zia Ur, Silvia Del Din, Jian Qing Shi, Brook Galna, Sue Lord, Alison J. Yarnall, Yu Guan, and Lynn Rochester. 2019. "Comparison of Walking Protocols and Gait Assessment Systems for Machine Learning-Based Classification of Parkinson’s Disease" Sensors 19, no. 24: 5363. https://doi.org/10.3390/s19245363