An Integrated Health-System Specialty Pharmacy Model for Coordinating Transitions of Care: Specialty Medication Challenges and Specialty Pharmacist Opportunities

 ,
,
Abstract
:1. Introduction
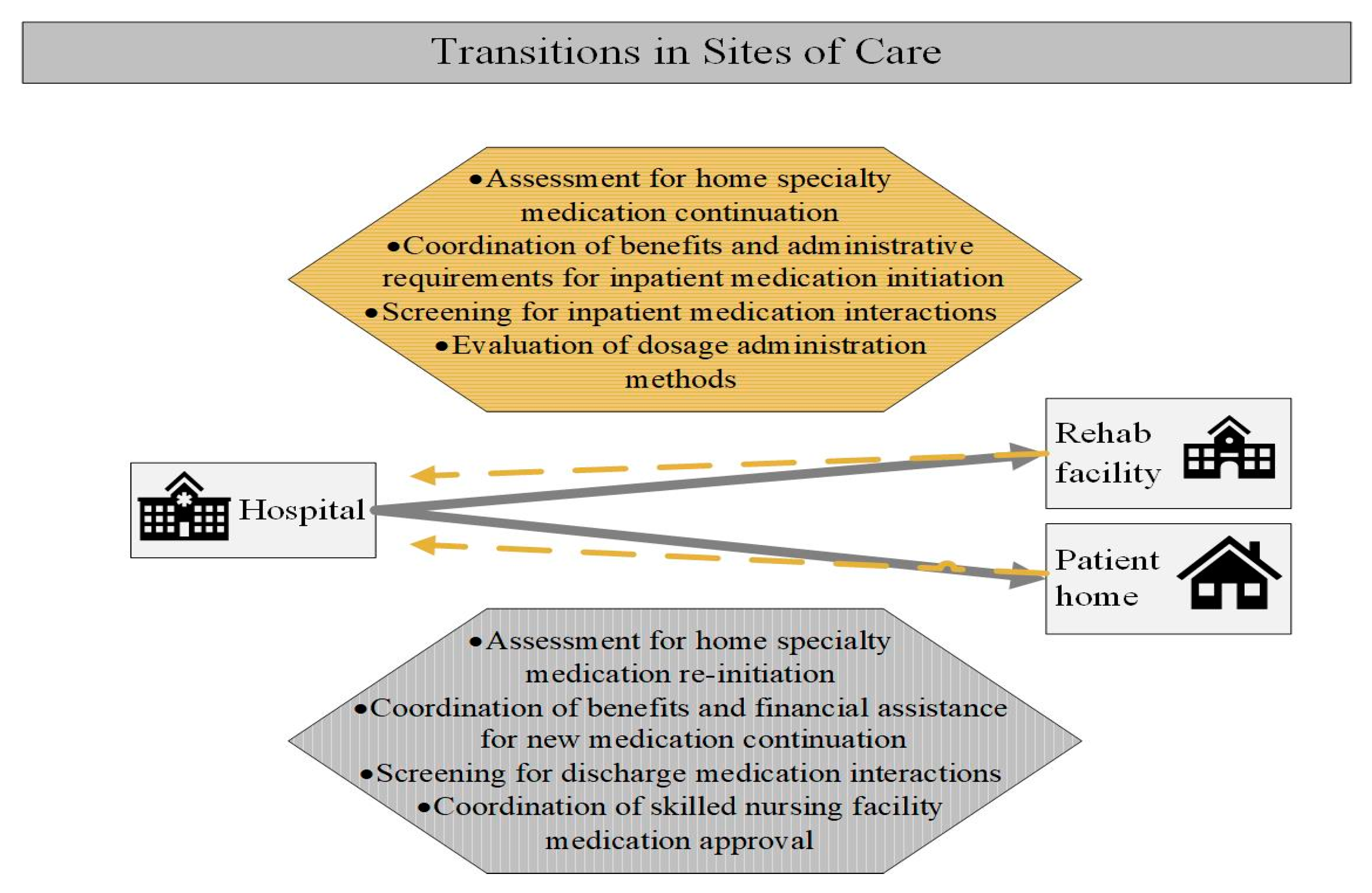
2. Transitions in Sites of Care Utilized by Specialty Patients
2.1. Transition Considerations
2.2. Transition into Hospital
2.3. During Hospitalization
2.4. Hospital Discharge
2.5. Integrated Health-System Specialty Pharmacist Role
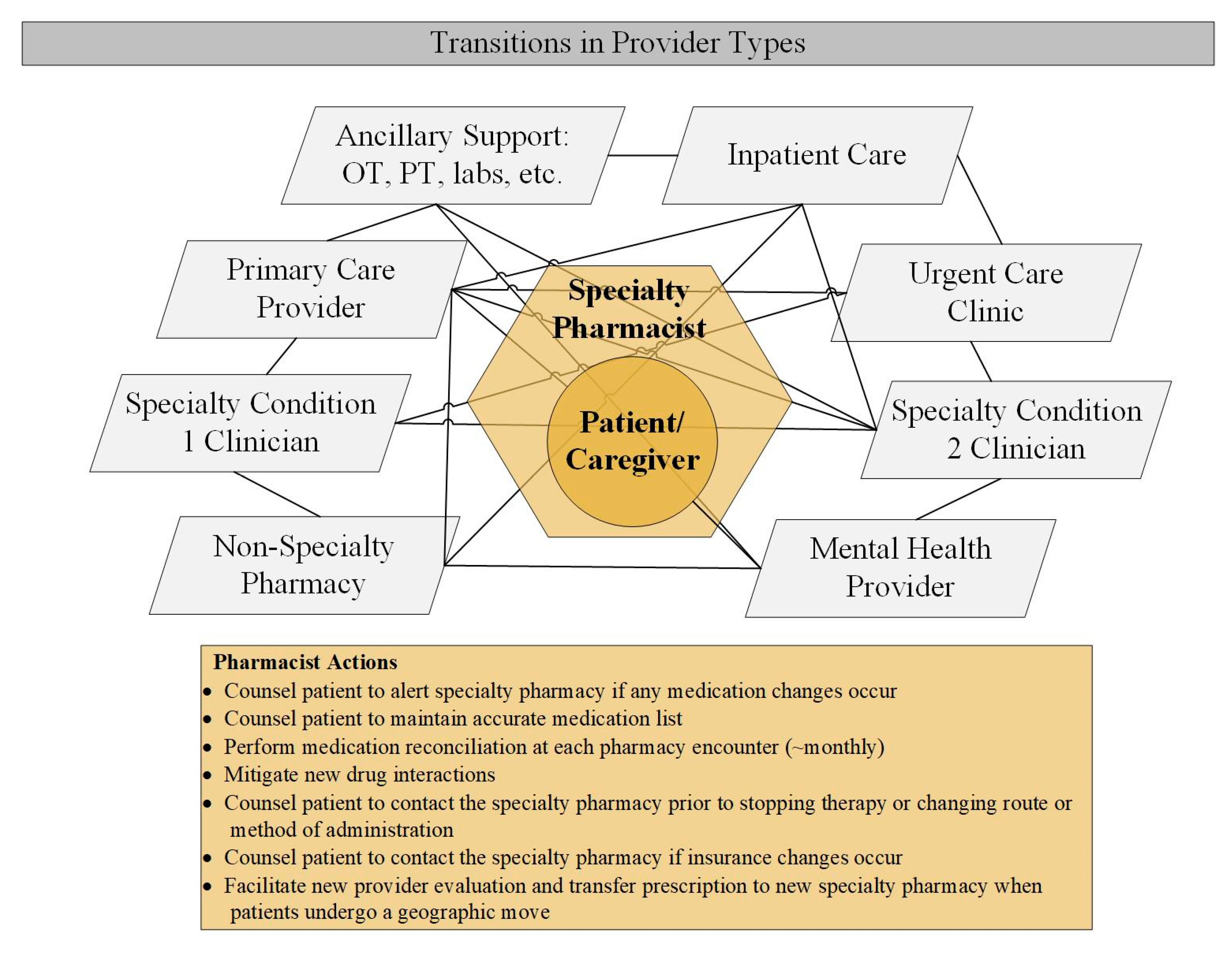
3. Transitions in Provider Types seen by Specialty Patients
3.1. Transition Considerations
3.2. Integrated Health-System Specialty Pharmacist Role
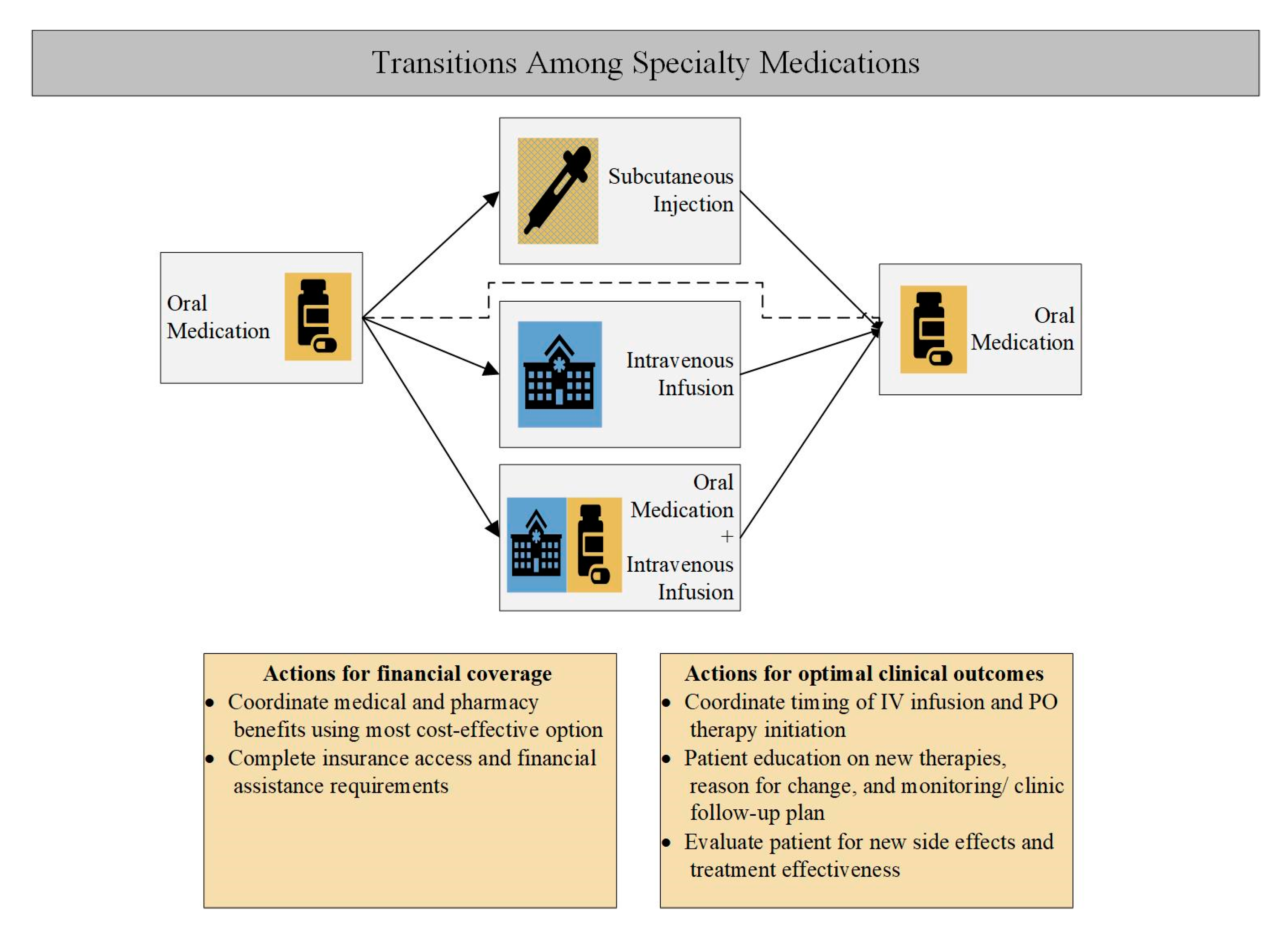
4. Transitions in Specialty Medications
4.1. Transition Considerations
4.2. Integrated Health-System Specialty Pharmacist Role
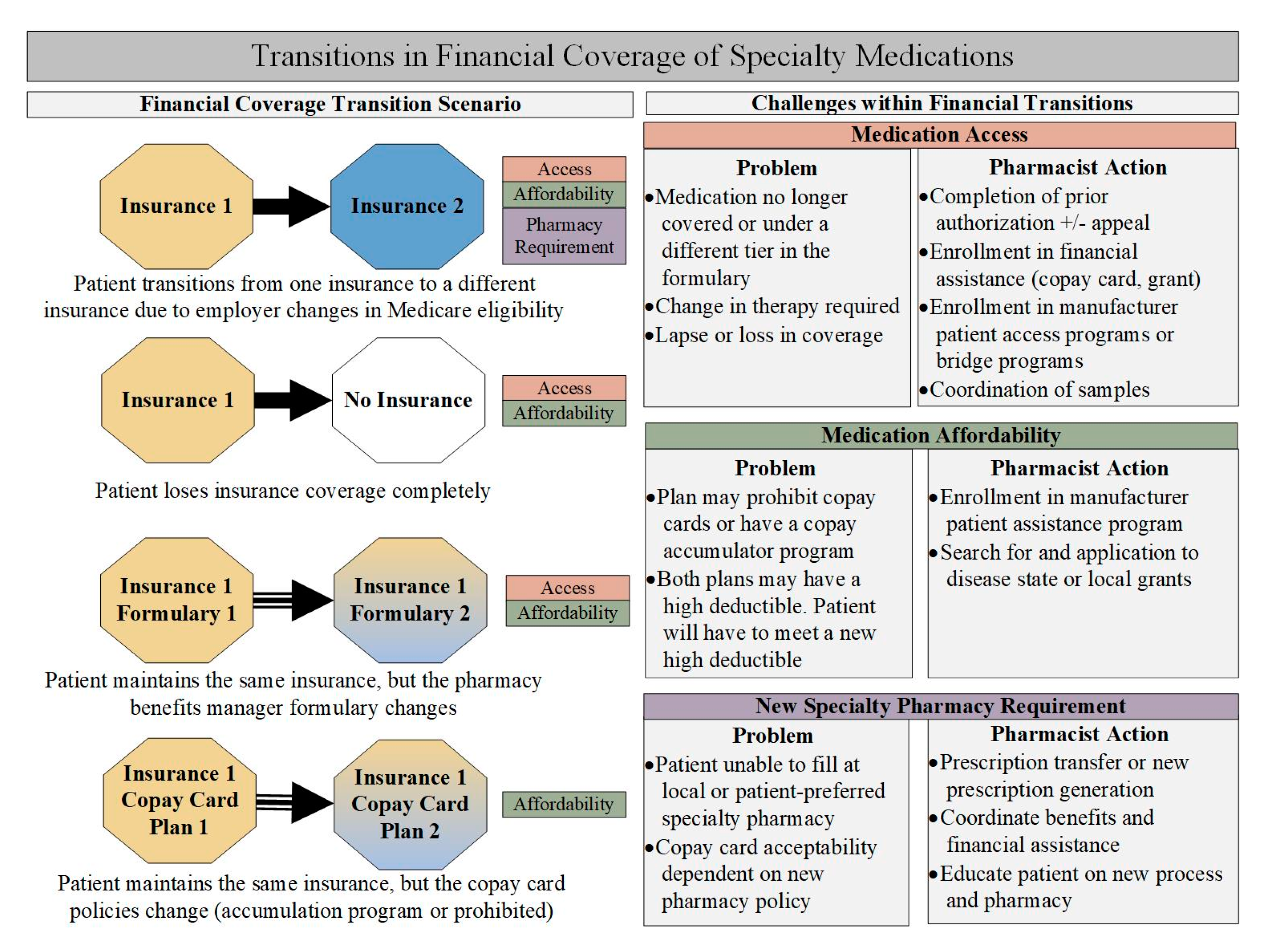
5. Transitions in Financial Coverage of Specialty Medications
5.1. Transition Considerations
5.2. Integrated Health-System Specialty Pharmacist Role
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Gleason, P.P.; Alexander, G.C.; Starner, C.I.; Ritter, S.T.; Van Houten, H.K.; Gunderson, B.W.; Shah, N.D. Health plan utilization and costs of specialty drugs within 4 chronic conditions. J. Manag. Care Pharm. 2013, 19, 542–548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- NASP. NASP Definitions of Specialty Pharmacy and Specialty Medications. Available online: http://naspnet.org/wp-content/uploads/2017/02/NASP-Defintions-final-2.16.pdf (accessed on 15 November 2019).
- AMCP. The AMCP Format for Formulary Submissions; AMCP: Alexandria, VA, USA, 2016. [Google Scholar]
- U.S. Food and Drug Administration. 2018 New Drug Therapy Approvals; U.S. Food and Drug Administration, Center for Drug Evaluation and Research: Silver Spring, MD, USA, 2019.
- Hirsch, B.R.; Balu, S.; Schulman, K.A. The impact of specialty pharmaceuticals as drivers of health care costs. Health Aff. 2014, 33, 1714–1720. [Google Scholar] [CrossRef] [PubMed]
- Morris, D.; Palermo, A. How Employers Are Looking at Specialty Pharmacy Today. Benefits Q. 2017, 33, 20–25. [Google Scholar] [PubMed]
- Robinson, J.C.; Howell, S.; Pearson, S.D. Value-Based Pricing and Patient Access for Specialty Drugs. JAMA 2018, 319, 2169–2170. [Google Scholar] [CrossRef]
- Express Scripts. 2018 Drug Trend Report; Express Scripts: St. Louis, MO, USA, 2018. [Google Scholar]
- CVS Health. Trend Report; CVS Health: Woonsocket, RI, USA, 2018. [Google Scholar]
- Hanson, R.L. Specialty pharmacy and the medication access dilemma. Am. J. Health Syst. Pharm. 2015, 72, 695. [Google Scholar] [CrossRef]
- Cocohoba, J.; Pohlman, B.; Tran, J.S.; Kirkham, H.; Joyce, C.; Clark, K.; Stebbins, M. Modeling specialty medicine access: Understanding key health system processes and players. J. Am. Pharm. Assoc. 2019, 59, 43–50. [Google Scholar] [CrossRef]
- Kirschenbaum, B.E. Specialty pharmacies and other restricted drug distribution systems: Financial and safety considerations for patients and health-system pharmacists. Am. J. Health Syst. Pharm. 2009, 66, S13–S20. [Google Scholar] [CrossRef]
- Rim, M.H.; Thomas, K.C.; Chandramouli, J.; Barrus, S.A.; Nickman, N.A. Implementation and quality assessment of a pharmacy services call center for outpatient pharmacies and specialty pharmacy services in an academic health system. Am. J. Health Syst. Pharm. 2018, 75, 633–641. [Google Scholar] [CrossRef] [Green Version]
- Bagwell, A.; Kelley, T.; Carver, A.; Lee, J.B.; Newman, B. Advancing Patient Care Through Specialty Pharmacy Services in an Academic Health System. J. Manag. Care Spec. Pharm. 2017, 23, 815–820. [Google Scholar] [CrossRef]
- Colgan, K.; Beacher, R. Importance of specialty pharmacy to your health system. Am. J. Health Syst. Pharm. 2015, 72, 753–756. [Google Scholar] [CrossRef]
- Pulvermacher, A.; Nelson, C. Benefits of developing a collaborative, outcomes-based specialty pharmacy program. Am. J. Health Syst. Pharm. 2016, 73, 839–843. [Google Scholar] [CrossRef] [PubMed]
- Hanson, R.L. Integrated clinical and specialty pharmacy practice model for management of patients with Multiple Sclerosis. Am. J. Health Syst. Pharm. 2014, 71, 463–469. [Google Scholar] [CrossRef] [PubMed]
- Lussier, M.E.; Evans, H.J.; Wright, E.A.; Gionfriddo, M.R. The impact of community pharmacist involvement on transitions of care: A systematic review and meta-analysis. J. Am. Pharm. Assoc. 2019, 1544–3191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bethishou, L.; Herzik, K.; Fang, N.; Abdo, C.; Tomaszewski, D.M. The impact of the pharmacist on continuity of care during transitions of care: A systematic review. J. Am. Pharm. Assoc. 2019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, T.; Griggs, S.K.; Chung, P.D. Characteristics of patients using specialty medications. Res. Social Adm. Pharm. 2018, 14, 901–908. [Google Scholar] [CrossRef]
- Barnes, E.L.; Kochar, B.; Long, M.D.; Martin, C.F.; Crockett, S.D.; Korzenik, J.R.; Kappelman, M.D. The Burden of Hospital Readmissions among Pediatric Patients with Inflammatory Bowel Disease. J. Pediatrics 2017, 191, 184–189. [Google Scholar] [CrossRef]
- Shah, N.B.; Mitchell, R.E.; Proctor, S.T.; Choi, L.; DeClercq, J.; Jolly, J.A.; Hemnes, A.R.; Zuckerman, A.D. High rates of medication adherence in patients with pulmonary arterial hypertension: An integrated specialty pharmacy approach. PLoS ONE 2019, 14, e0217798. [Google Scholar] [CrossRef]
- Pirttisalo, A.L.; Sipila, J.O.T.; Soilu-Hanninen, M.; Rautava, P.; Kyto, V. Adult hospital admissions associated with multiple sclerosis in Finland in 2004–2014. Ann. Med. 2018, 50, 354–360. [Google Scholar] [CrossRef] [Green Version]
- Hertzka, R.E. Medication “Brown Bagging”; Resolution 827-I-15; Centers for Medicaid and Medicare Services: Baltimore, MD, USA, 2016.
- Terrault, N.A.; Zeuzem, S.; Di Bisceglie, A.M.; Lim, J.K.; Pockros, P.J.; Frazier, L.M.; Kuo, A.; Lok, A.S.; Shiffman, M.L.; Ben Ari, Z.; et al. Effectiveness of Ledipasvir-Sofosbuvir Combination in Patients With Hepatitis C Virus Infection and Factors Associated With Sustained Virologic Response. Gastroenterology 2016, 151, 1131–1140. [Google Scholar] [CrossRef] [Green Version]
- Cornish, P. “Avoid the crush”: Hazards of medication administration in patients with dysphagia or a feeding tube. CMAJ 2005, 172, 871–872. [Google Scholar] [CrossRef] [Green Version]
- Oberoi, R.K.; Zhao, W.; Sidhu, D.S.; Viani, R.M.; Trinh, R.; Liu, W. A Phase 1 Study to Evaluate the Effect of Crushing, Cutting Into Half, or Grinding of Glecaprevir/Pibrentasvir Tablets on Exposures in Healthy Subjects. J. Pharm. Sci. 2018, 107, 1724–1730. [Google Scholar] [CrossRef] [PubMed]
- Gadbois, E.A.; Tyler, D.A.; Shield, R.; McHugh, J.; Winblad, U.; Teno, J.M.; Mor, V. Lost in Transition: A Qualitative Study of Patients Discharged from Hospital to Skilled Nursing Facility. J. Gen. Intern. Med. 2019, 34, 102–109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bush, P.W.; Daniels, R. Health Care Systems and Transitions of Care: Implication on Interdisciplinary Pharmacy Services. N. C. Med. J. 2017, 78, 177–180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, T. Health care utilization and expenditures among adults with rheumatoid arthritis using specialty pharmaceuticals. Res. Soc. Adm. Pharm. 2018, 15, 724–729. [Google Scholar] [CrossRef] [PubMed]
- Anderson, G.; Knickman, J.R. Changing the chronic care system to meet people’s needs. Health Aff. 2001, 20, 146–160. [Google Scholar] [CrossRef] [Green Version]
- Parchman, M.L.; Noel, P.H.; Lee, S. Primary care attributes, health care system hassles, and chronic illness. Med. Care 2005, 43, 1123–1129. [Google Scholar] [CrossRef]
- Reynolds, V.W.; Chinn, M.E.; Jolly, J.A.; Kelley, T.N.; Peter, M.E.; Choi, L.; Nwosu, S.; Leon, B.C.; Zuckerman, A.D. Integrated specialty pharmacy yields high PCSK9 inhibitor access and initiation rates. J. Clin. Lipidol. 2019, 13, 254–264. [Google Scholar] [CrossRef]
- Banks, A.M.; Peter, M.E.; Holder, G.M.; Jolly, J.A.; Markley, B.M.; Zuckerman, S.L.; Choi, L.; Nwosu, S.; Zuckerman, A.D. Adherence to Disease-Modifying Therapies at a Multiple Sclerosis Clinic: The Role of the Specialty Pharmacist. J. Pharm. Pract. 2019, 22, 1394–1401. [Google Scholar] [CrossRef]
- Swisher, R.; Feldman, A.; Kasbekar, N. Impact of comprehensive pharmacy services on patient centered outcomes in a hematology and oncology clinic. J. Drug Assess. 2018, 7, 20. [Google Scholar] [CrossRef] [Green Version]
- Simacek, K.F.; Ko, J.J.; Moreton, D.; Varga, S.; Johnson, K.; Katic, B.J. The Impact of Disease-Modifying Therapy Access Barriers on People With Multiple Sclerosis: Mixed-Methods Study. J. Med. Internet Res. 2018, 20, e11168. [Google Scholar] [CrossRef] [Green Version]
- Niccolai, J.L.; Roman, D.L.; Julius, J.M.; Nadour, R.W. Potential Obstacles in the Acquisition of Oral Anticancer Medications. J. Oncol. Pract. 2017, 13, e29–e36. [Google Scholar] [CrossRef] [PubMed]
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: Multiple Myeloma, version 3.2019; National Comprehensive Cancer Network: Jenkintown, PA, USA, 2019. [Google Scholar]
- Khorana, A.A.; Tullio, K.; Elson, P.; Pennell, N.A.; Kalady, M.F.; Raymond, D.; Klein, E.A.; Abraham, J.; Grobmyer, S.R.; Monteleone, E.E.; et al. Increase in time to initiating cancer therapy and association with worsened survival in curative settings: A U.S. analysis of common solid tumors. In Proceedings of the A merican Society of Clinical Oncology Annual Meeting, Chicago, IL, USA, 31 May–4 June 2019. [Google Scholar]
- Cassano, A. ASHP Specialty Pharmacy Resource Guide; ASHP: Bethesda, MD, USA, 2019. [Google Scholar]
- Fajardo, S.; Zook, F.; Dotson, E. Specialty pharmacy for hematologic malignancies. Am. J. Health Syst. Pharm. 2016, 73, 797–809. [Google Scholar] [CrossRef] [PubMed]
- American Medical Association. 2018 Prior Authorization State Law Chart; American Medical Association: Chicago, IL, USA, 2018. [Google Scholar]
- Fein, A.; Gill, L.; Long, D. Specialty Pharmacy Industry Outlook: What’s Next? In Proceedings of the Asembia Specialty Pharmacy Summit, Las Vegas, NV, USA, 29 April–2 May 2019. [Google Scholar]
- Dusetzina, S.B.; Huskamp, H.A.; Keating, N.L. Specialty Drug Pricing and Out-of-Pocket Spending on Orally Administered Anticancer Drugs in Medicare Part D, 2010 to 2019. JAMA 2019, 321, 2025–2027. [Google Scholar] [CrossRef] [PubMed]
- Bonaccorso, S.; Sturchio, J.L. Perspectives from the pharmaceutical industry. BMJ 2003, 327, 863–864. [Google Scholar] [CrossRef] [Green Version]
- Cutler, T.; She, Y.; Barca, J.; Lester, S.; Xing, G.; Patel, J.; Melnikow, J. Impact of Pharmacy Intervention on Prior Authorization Success and Efficiency at a University Medical Center. J. Manag. Care Spec. Pharm. 2016, 22, 1167–1171. [Google Scholar] [CrossRef]
- Zuckerman, A.; Douglas, A.; Nwosu, S.; Choi, L.; Chastain, C. Increasing success and evolving barriers in the hepatitis C cascade of care during the direct acting antiviral era. PLoS ONE 2018, 13, e0199174. [Google Scholar] [CrossRef]
- Marden, B.; Martineau, C. Emphasize Medication Adherence to Patients. Pharmacy Times. Available online: https://www.pharmacytimes.com/publications/health-system-edition/2019/september2019/emphasize-medication-adherence-to-patients (accessed on 15 November 2019).
- Viswanathan, M.; Golin, C.E.; Jones, C.D.; Ashok, M.; Blalock, S.J.; Wines, R.C.; Coker-Schwimmer, E.J.; Rosen, D.L.; Sista, P.; Lohr, K.N. Interventions to improve adherence to self-administered medications for chronic diseases in the United States: A systematic review. Ann. Intern. Med. 2012, 157, 785–795. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Name |
|---|
| Oncology |
| Hematology |
| Multiple sclerosis |
| Rheumatoid arthritis |
| Inflammatory bowel disease |
| Hepatitis |
| Human Immunodeficiency Virus |
| Cystic fibrosis |
| Asthma |
| Pulmonary arterial hypertension |
| Bone disorders |
| Growth disorders |
| Movement disorders |
| Endocrinology disorders |
| Sickle cell disease |
| Idiopathic pulmonary fibrosis |
| Psychiatric conditions |
| Fertility |
| Nonalcoholic steatohepatitis |
| Hyperlipidemia |
| Immunology |
| Enzyme deficiencies |
| Glycogen storage diseases |
| Specialty Condition | Example Scenario | Integrated Specialty Pharmacist Actions | Proposed Outcome |
|---|---|---|---|
| Transitions in Sites of Care | |||
| Pediatric inflammatory bowel disease | Patient diagnosed with Crohn’s disease while admitted to the hospital and prescribed adalimumab |
|     |
| Hepatitis C | Patient started on glecaprevir/pibrentasvir inpatient following liver transplant and needed therapy to continue without interruption at discharge |
|  |
| Psoriatic arthritis | Patient receiving etanercept was admitted to a rehabilitation facility that did not carry any specialty medications |
| |
| Transition in Provider Types | |||
| Juvenile idiopathic arthritis | Pediatric patient receiving adalimumab moved of state |
| |
| Oncology/Hematology | External provider changed antifungal prophylaxis from posaconazole to fluconazole on a patient with ongoing venetoclax therapy for acute myeloid leukemia. Patient notified pharmacist. |
|  |
| Hepatitis C | Ledipasvir/sofosbuvir prescription received from gastroenterologist for patient prescribed oxcarbazepine by psychiatrist. Significant drug/drug interaction exists between these two medications, potentially resulting in virologic failure of ledipasvir/sofosbuvir |
| |
| Transitions Among Specialty Medications | |||
| Rheumatoid arthritis | Patient well-controlled on abatacept 750 mg IV every 4 weeks relocated to 2 h away from clinic and started to miss or be tardy for infusions |
|  |
| Multiple sclerosis | Patient needed to transition from natalizumab (IV infusion) to fingolimod (PO) |
| |
| Oncology/Hematology | Patient needed to transition from bortezomib (SubQ) to ixazomib (PO) |
| |
| Transitions in Financial Coverage | |||
| Psoriatic arthritis | Patient’s arthritis symptoms were well controlled on secukinumab, but the patient became unemployed and lost insurance and pharmacy coverage |
|  |
| Ankylosing spondylitis | Patient was stable on golimumab 50mg SubQ monthly and received manufacturer copay card for medication. After retiring from her job, the patient transitioned from commercial insurance to Medicare, and was thus ineligible to use manufacturer copay card, resulting in an out-of-patient copayment of >$1000/month |
| |
| Pediatric inflammatory bowel disease | Pediatric IBD patient prescribed adalimumab. Clinic protocol was to receive first adalimumab induction dose in clinic for teaching and monitoring. Patient was unable to fill medication through the integrated specialty pharmacy due to insurance requirements. |
|  |
| Hepatitis C | Patient diagnosed with hepatitis C was prescribed 12-week course of glecaprevir/ pibrentasvir. Medication was required to be filled through an external pharmacy. During the treatment course, patient had difficulty refilling medication due to high cost and contacted the integrated specialty pharmacist for assistance. |
| |
Timely treatment initiation; Complete or effective dosing; Shorter length of hospital stay; Persistence to prescribed therapy; Drug-drug interaction avoided; Lower risk of disease activity/progression; Patient education and understanding of medication administration; Patient monitoring; Lower medication costs. SubQ: subcutaneous; FDA: Food and Drug Administration; IV: Intravenous; PO: Oral; SRF: Start Request Form; FDO: First Dose Observation; PharmD: Pharmacist; REMS: Risk Evaluation and Mitigation Strategy; IBD: Inflammatory Bowel Disease.© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zuckerman, A.D.; Carver, A.; Cooper, K.; Markley, B.; Mitchell, A.; Reynolds, V.W.; Saknini, M.; Wyatt, H.; Kelley, T. An Integrated Health-System Specialty Pharmacy Model for Coordinating Transitions of Care: Specialty Medication Challenges and Specialty Pharmacist Opportunities. Pharmacy 2019, 7, 163. https://doi.org/10.3390/pharmacy7040163
Zuckerman AD, Carver A, Cooper K, Markley B, Mitchell A, Reynolds VW, Saknini M, Wyatt H, Kelley T. An Integrated Health-System Specialty Pharmacy Model for Coordinating Transitions of Care: Specialty Medication Challenges and Specialty Pharmacist Opportunities. Pharmacy. 2019; 7(4):163. https://doi.org/10.3390/pharmacy7040163
Chicago/Turabian StyleZuckerman, Autumn D., Alicia Carver, Katrina Cooper, Brandon Markley, Amy Mitchell, Victoria W. Reynolds, Marci Saknini, Houston Wyatt, and Tara Kelley. 2019. "An Integrated Health-System Specialty Pharmacy Model for Coordinating Transitions of Care: Specialty Medication Challenges and Specialty Pharmacist Opportunities" Pharmacy 7, no. 4: 163. https://doi.org/10.3390/pharmacy7040163