
Plant Extract-Synthesized Silver Nanoparticles for Application in Dental Therapy

 ,
,  , and
, and
Abstract
:1. Introduction
1.1. Dental Caries
Pathophysiology of Dental Caries
1.2. Prevention of Dental Caries
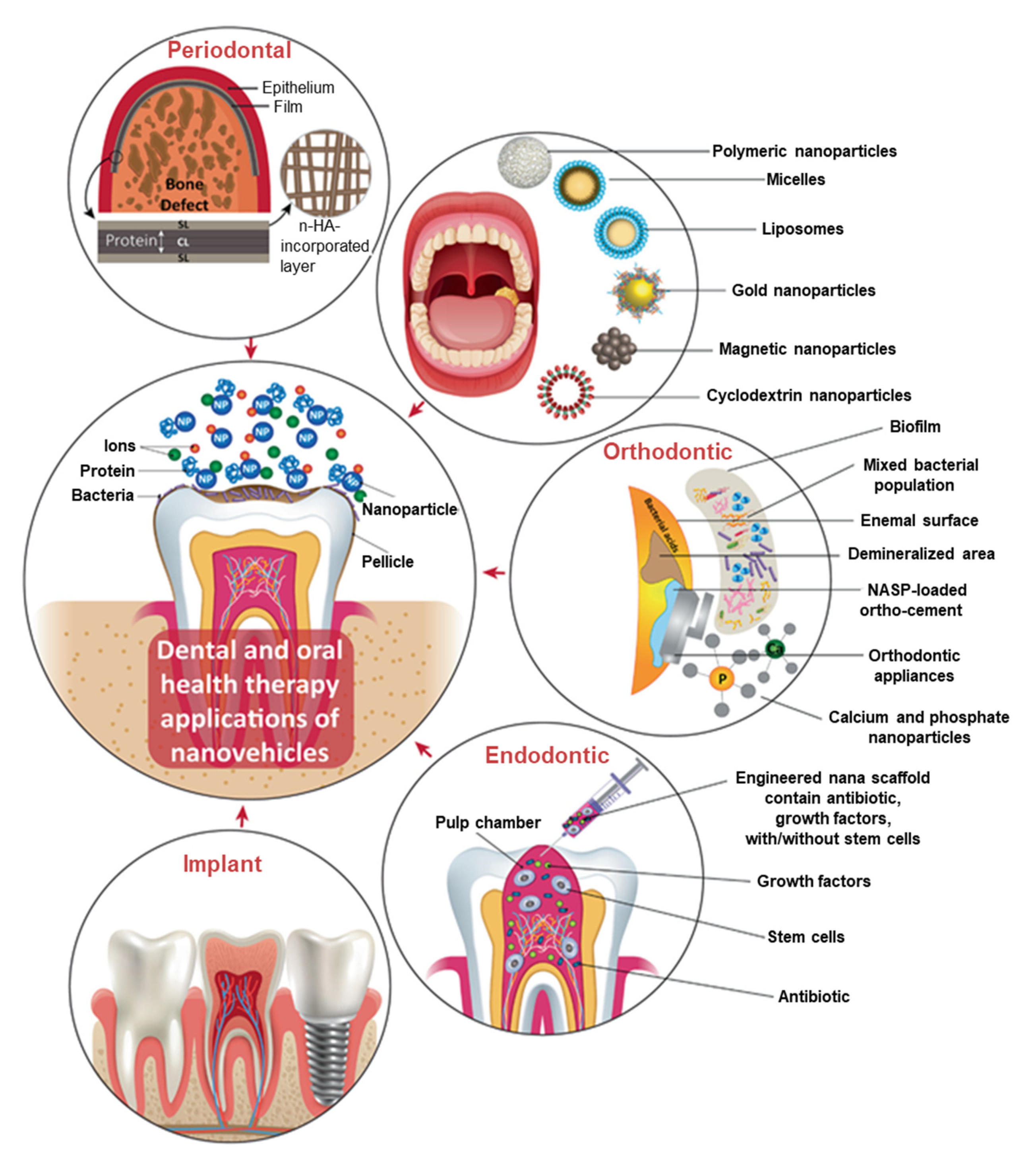
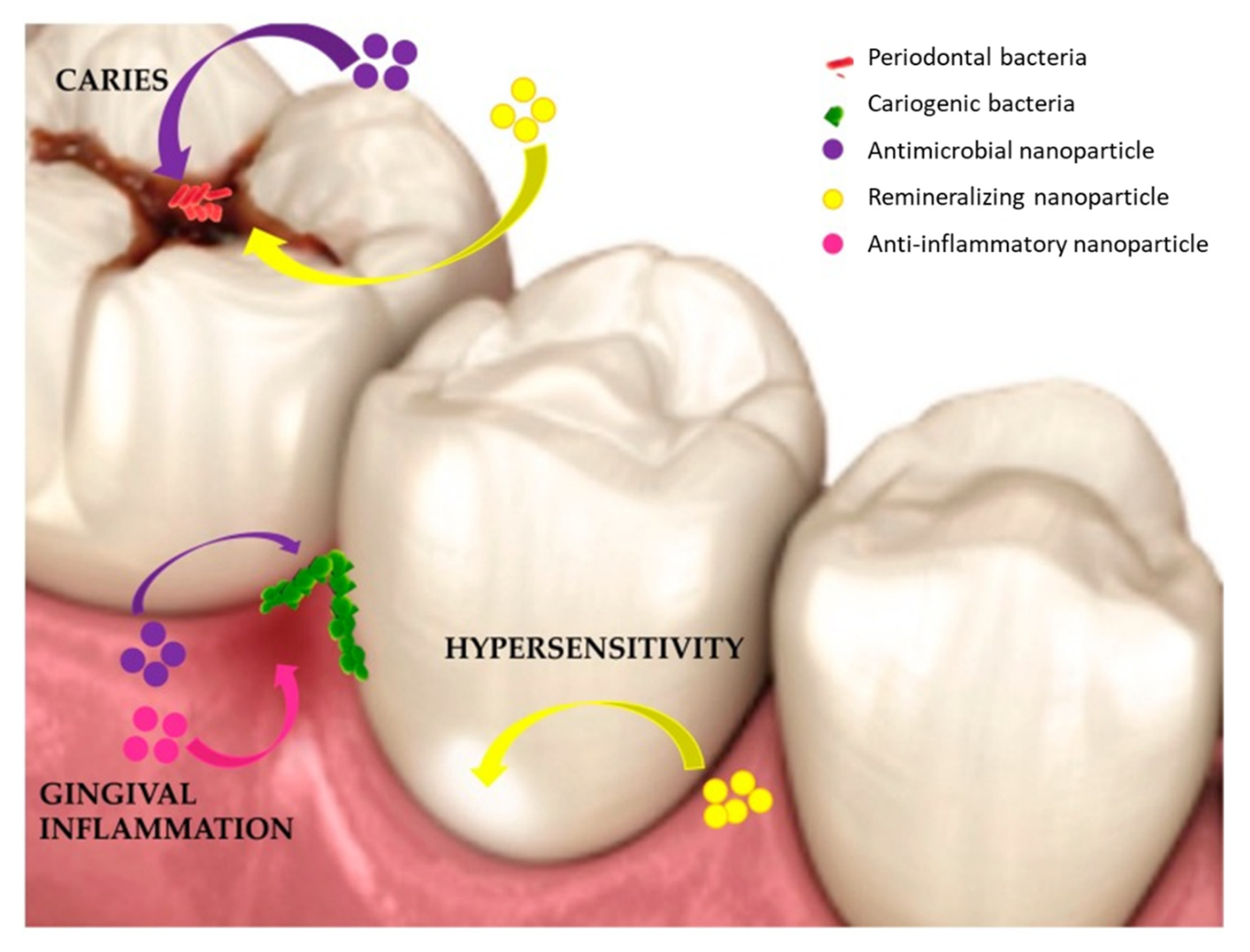
1.3. Application of Nanomaterials in Dental Therapy
1.3.1. AgNPs in Dental Therapy
1.3.2. Plant-Synthesized AgNPs for Treatment of Dental Diseases
Synthesis of AgNPs Using Plant Extracts
Plant Extract-Synthesized AgNPs for Treatment of Dental Diseases
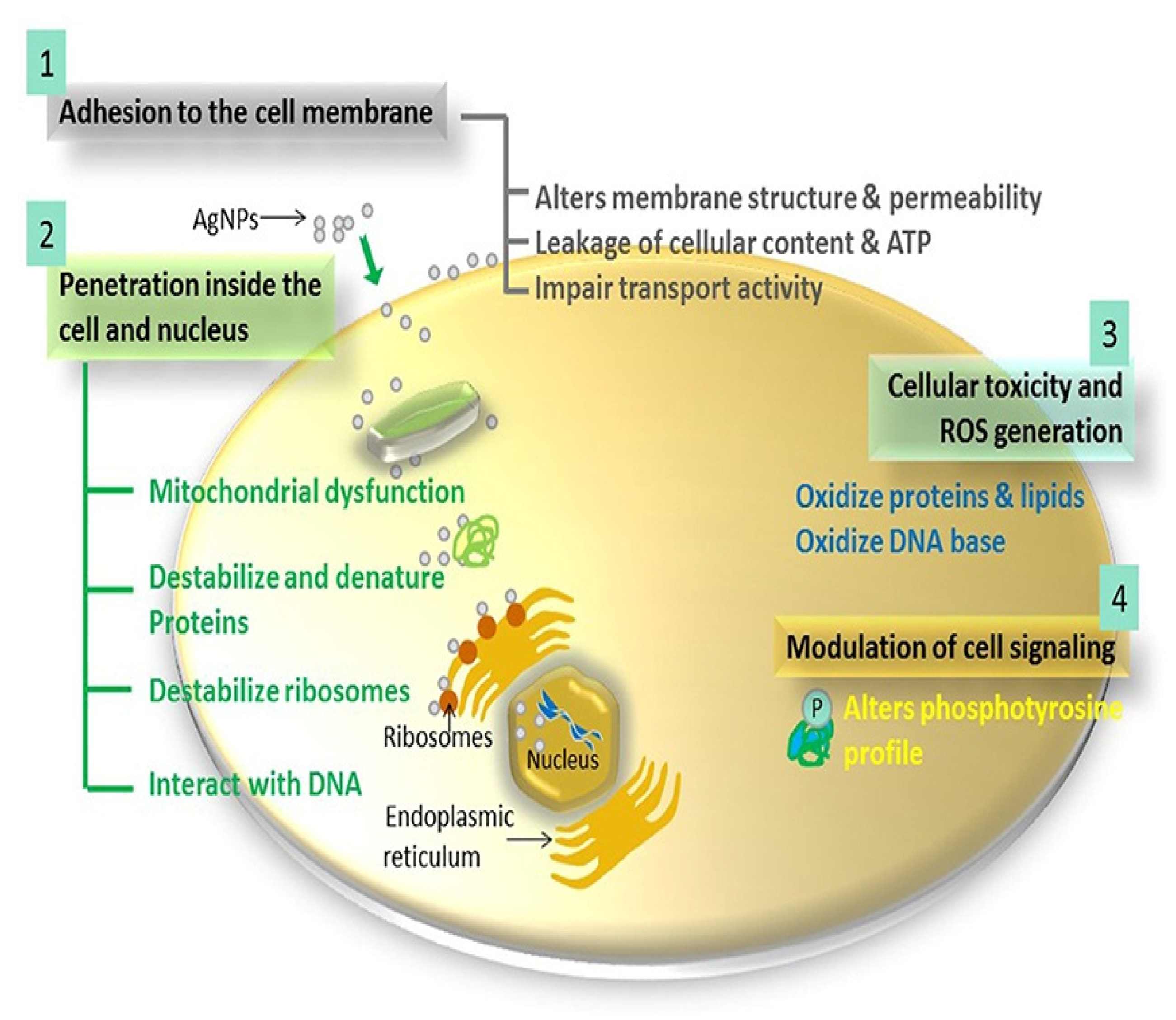
1.4. Antimicrobial Mechanism of AgNPs
1.5. Toxicity of AgNPs
2. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kanjevac, T.; Taso, E.; Stefanovic, V.; Petkovic-Curcin, A.; Supic, G.; Markovic, D.; Djukic, M.; Djuran, B.; Vojvodic, D.; Sculean, A.; et al. Estimating the effects of dental caries and its restorative treatment on periodontal inflammatory and oxidative status: A short controlled longitudinal study. Front. Immunol. 2021, 12, 716359. [Google Scholar] [CrossRef]
- Winning, L.; Lundy, F.T.; Blackwood, B.; McAuley, D.F.; El Karim, I. Oral health care for the critically ill: A narrative review. Crit. Care 2021, 25, 353. [Google Scholar] [CrossRef] [PubMed]
- WHO. Oral Health. 2020. Available online: https://www.Who.Int/News-Room/Fact-Sheets/Detail/Oral-Health (accessed on 3 July 2020).
- Qiu, W.; Zhou, Y.; Li, Z.; Huang, T.; Xiao, Y.; Cheng, L.; Peng, X.; Zhang, L.; Ren, B. Application of antibiotics/antimicrobial agents on dental caries. BioMed Res. Int. 2020, 2020, 5658212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kassebaum, N.J.; Bernabe, E.; Dahiya, M.; Bhandari, B.; Murray, C.J.L.; Marcenes, W. Marcenes, Global burden of severe periodontitis in 1990-2010: A systematic review and meta-regression. J. Dent. Res. 2014, 93, 1045–1053. [Google Scholar] [CrossRef]
- Peres, M.A.; Macpherson, L.M.; Weyant, R.J.; Daly, B.; Venturelli, R.; Mathur, M.R.; Listl, S.; Celeste, R.K.; Guarnizo-Herreño, C.C.; Kearns, C.; et al. Watt, Oral diseases: A global public health challenge. Lancet 2019, 394, 249–260. [Google Scholar] [CrossRef]
- Valm, A.M. The Structure of Dental plaque microbial communities in the transition from health to dental caries and periodontal disease. J. Mol. Biol. 2019, 431, 2957–2969. [Google Scholar] [CrossRef] [PubMed]
- Song, W.; Ge, S. Application of antimicrobial nanoparticles in dentistry. Molecules 2019, 24, 1033. [Google Scholar] [CrossRef] [Green Version]
- WHO. Sugars and Dental Caries, World Heal. Organ. 2017. Available online: https://apps.who.int/iris/bitstream/handle/10665/259413/WHO-NMH-NHD-17.12-eng.pdf (accessed on 3 July 2020).
- WHO. WHO Model List of Essential Medicines. 2017. Available online: https://apps.who.int/iris/bitstream/handle/10665/273826/EML-20-eng.pdf?sequence=1&isAllowed=y (accessed on 3 July 2020).
- Bapat, R.A.; Chaubal, T.V.; Joshi, C.P.; Bapat, P.R.; Choudhury, H.; Pandey, M.; Gorain, B.; Kesharwani, P. An overview of application of silver nanoparticles for biomaterials in dentistry. Mater. Sci. Eng. C 2018, 91, 881–898. [Google Scholar] [CrossRef]
- Saafan, A.; Zaazou, M.H.; Sallam, M.K.; Mosallam, O.; El Danaf, H.A. Assessment of photodynamic therapy and nanoparticles effects on caries models. Open Access Maced. J. Med Sci. 2018, 6, 1289–1295. [Google Scholar] [CrossRef] [Green Version]
- Bowen, W.H.; Burne, R.A.; Wu, H.; Koo, H. Oral Biofilms: Pathogens, matrix, and polymicrobial interactions in microenvironments. Trends Microbiol. 2018, 26, 229–242. [Google Scholar] [CrossRef]
- Veiga, N.; Aires, D.; Douglas, F.; Pereira, M.; Vaz, A.; Rama, L.; Silva, M.; Miranda, V.; Pereira, F.; Vidal, B.; et al. Exploring the world of science dental caries: A review. J. Dent. Oral Heal. 2016, 2. [Google Scholar]
- Flemming, H.-C.; Wingender, J.; Szewzyk, U.; Steinberg, P.; Rice, S.A.; Kjelleberg, S. Biofilms: An emergent form of bacterial life. Nat. Rev. Microbiol. 2016, 14, 563–575. [Google Scholar] [CrossRef]
- Marsh, P.D.; Do, T.; Beighton, D.; Devine, D.A. Influence of saliva on the oral microbiota. Periodontology 2000 2016, 70, 80–92. [Google Scholar] [CrossRef]
- Hoare, A.; Marsh, P.D.; Diaz, P.I. Ecological therapeutic opportunities for oral diseases. Microbiol. Spectr. 2017, 5. [Google Scholar] [CrossRef]
- Siqueira, W.; Custodio, W.; McDonald, E. New insights into the composition and functions of the acquired enamel pellicle. J. Dent. Res. 2012, 91, 1110–1118. [Google Scholar] [CrossRef]
- Aroonsang, W.; Sotres, J.; El-Schich, Z.; Arnebrant, T.; Lindh, L. Influence of substratum hydrophobicity on salivary pellicles: Organization or composition? Biofouling 2014, 30, 1123–1132. [Google Scholar] [CrossRef]
- Yadav, K.; Prakash, S. Dental Caries: A Review. Asian J. Biomed. Pharm. Sci. 2016, 6, 1–7. [Google Scholar] [CrossRef]
- Cochrane, N.; Cai, F.; Huq, N.L.; Burrow, M.; Reynolds, E. New approaches to enhanced remineralization of tooth enamel. J. Dent. Res. 2010, 89, 1187–1197. [Google Scholar] [CrossRef]
- Mattousch, T.; Van Der Veen, M.; Zentner, A. Caries lesions after orthodontic treatment followed by quantitative light-induced fluorescence: A 2-year follow-up. Eur. J. Orthod. 2007, 29, 294–298. [Google Scholar] [CrossRef] [Green Version]
- Schmidlin, P.; Zobrist, K.; Attin, T.; Wegehaupt, F. In vitro re-hardening of artificial enamel caries lesions using enamel matrix proteins or self-assembling peptides. J. Appl. Oral Sci. 2016, 24, 31–36. [Google Scholar] [CrossRef] [Green Version]
- Spolarich, A.E.; Panagakos, F.S. Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions; Professional Audience Communications Inc.: Charlotte, NC, USA, 2017; Available online: https://saskohc.ca/images/documents/PDF//Reports//Prevention-Across-the-Lifespan-A-Review-of-Evidence-Based-Interventions-for-Common-Oral-Conditions.pdf (accessed on 3 July 2020).
- Devarajan, H.; Somasundaram, S. Salivary proteins and its effects on dental caries—A review. Drug Invention Today. 2019, 11, 1406–1411. [Google Scholar]
- Twetman, S. Prevention of dental caries as a non-communicable disease. Eur. J. Oral Sci. 2018, 126, 19–25. [Google Scholar] [CrossRef] [Green Version]
- Doméjean, S.; Muller-Bolla, M.; Featherstone, J.D.B. Caries preventive therapy. Clin. Dent. Rev. 2018, 2, 14. [Google Scholar] [CrossRef]
- Grigalauskienė, R.; Slabšinskienė, E.; Vasiliauskienė, I. Biological approach of dental caries management. Stomatologija 2015, 17, 107–112. [Google Scholar] [PubMed]
- Figuero, E.; Nóbrega, D.F.; García-Gargallo, M.; Tenuta, L.M.A.; Herrera, D.; Carvalho, J.C. Mechanical and chemical plaque control in the simultaneous management of gingivitis and caries: A systematic review. J. Clin. Periodontol. 2017, 44, S116–S134. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, F.; Prashanth, S.T.; Sindhu, K.; Nayak, A.; Chaturvedi, S. Antimicrobial efficacy of nanosilver and chitosan against Streptococcus mutans, as an ingredient of toothpaste formulation: An in vitro study. J. Indian Soc. Pedod. Prev. Dent. 2019, 37, 46. [Google Scholar] [CrossRef] [PubMed]
- Aoun, A.; Darwiche, F.; Al Hayek, S.; Doumit, J. The fluoride debate: The pros and cons of fluoridation. Prev. Nutr. Food Sci. 2018, 23, 171–180. [Google Scholar] [CrossRef]
- WHO, Executive summary. The Selection and Use of Essential Medicines 2021 Report of the 23rd WHO Expert Committee on the Selection and Use of Essential Medicines. 2021. Available online: file:///C:/Users/Admin/AppData/Local/Temp/WHO-MHP-HPS-EML-2021.01-eng.pdf (accessed on 20 August 2021).
- Sheiham, A.; James, W.P.T. Diet and dental caries: The pivotal role of free sugars reemphasized. J. Dent. Res. 2015, 94, 1341–1347. [Google Scholar] [CrossRef]
- Sheiham, A.; James, W.P.T. A new understanding of the relationship between sugars, dental caries and fluoride use: Implications for limits on sugars consumption. Public Health Nutr. 2014, 17, 2176–2184. [Google Scholar] [CrossRef] [Green Version]
- Rosier, B.; Marsh, P.; Mira, A. Resilience of the oral microbiota in health: Mechanisms that prevent dysbiosis. J. Dent. Res. 2017, 97, 371–380. [Google Scholar] [CrossRef]
- Zhang, H.; Du, A.; Hong, L.; Wang, Y.; Cheng, B.; Zhang, Z. Identification and analysis of fluoride-resistant Streptococcus mutans genomic mutation based on silicon solid nanopore. Mater. Express 2020, 10, 479–489. [Google Scholar] [CrossRef]
- Srivastava, S.; Flora, S.J.S. Fluoride in drinking water and skeletal fluorosis: A review of the global impact. Curr. Environ. Health Rep. 2020, 7, 140–146. [Google Scholar] [CrossRef]
- Philip, N.; Walsh, L. The potential ecological effects of casein phosphopeptide-amorphous calcium phosphate in dental caries prevention. Aust. Dent. J. 2018, 64, 66–71. [Google Scholar] [CrossRef] [Green Version]
- Zero, D.T.; Brennan, M.T.; Daniels, T.E.; Papas, A.; Stewart, C.; Pinto, A.; Al-Hashimi, I.; Navazesh, M.; Rhodus, N.; Sciubba, J.; et al. Clinical practice guidelines for oral management of Sjögren disease. J. Am. Dent. Assoc. 2016, 147, 295–305. [Google Scholar] [CrossRef]
- Keller, M.K.; Brandsborg, E.; Holmstrøm, K.; Twetman, S. Effect of tablets containing probiotic candidate strains on gingival inflammation and composition of the salivary microbiome: A randomised controlled trial. Benef. Microbes 2018, 9, 487–494. [Google Scholar] [CrossRef]
- Gibson, G.R.; Probert, H.M.; Van Loo, J.; Rastall, R.A.; Roberfroid, M.B. Dietary modulation of the human colonic microbiota: Updating the concept of prebiotics. Nutr. Res. Rev. 2004, 17, 259–275. [Google Scholar] [CrossRef] [Green Version]
- Ma, Y.; Oliver, R.; Chen, H. The oral biome in the aetiology and management of dental disease: Current concepts and ethical considerations. Bioethics 2019, 33, 937–947. [Google Scholar] [CrossRef]
- Scharnow, A.M.; Solinski, A.E.; Wuest, W.M. Targeting S. mutans biofilms: A perspective on preventing dental caries. MedChemComm 2019, 10, 1057–1067. [Google Scholar] [CrossRef]
- Adams, S.E.; Arnold, D.; Murphy, B.; Carroll, P.; Green, A.K.; Smith, A.; Marsh, P.D.; Chen, T.; Marriott, R.E.; Brading, M.G. A randomised clinical study to determine the effect of a toothpaste containing enzymes and proteins on plaque oral microbiome ecology. Sci. Rep. 2017, 7, 43344. [Google Scholar] [CrossRef]
- Liao, Y.; Brandt, B.W.; Li, J.; Crielaard, W.; Van Loveren, C.; Deng, D.M. Fluoride resistance in Streptococcus mutans: A mini review. J. Oral Microbiol. 2017, 9, 1344509. [Google Scholar] [CrossRef] [Green Version]
- Hamilton, I.R. Growth characteristics of adapted and ultraviolet-induced mutants of Streptococcus salivarius resistant to sodium fluoride. Can. J. Microbiol. 1969, 15, 287–295. [Google Scholar] [CrossRef]
- Fontana, M. Enhancing fluoride: Clinical human studies of alternatives or boosters for caries management. Caries Res. 2016, 50, 22–37. [Google Scholar] [CrossRef]
- Chaudhary, I.; Tripathi, A.M. Effect of Casein phosphopeptide–amorphous calcium phosphate and calcium sodium phosphosilicate on artificial carious lesions: An in vitro study. Int. J. Clin. Pediatr. Dent. 2017, 10, 261–266. [Google Scholar] [CrossRef]
- Hedge, S.; Roma, M.; Shetty, D. Non-fluoridated remineralization agents in dentistry. J. Pharm. Sci. & Res. 2016, 8, 884–887. [Google Scholar]
- GÜÇLÜ, Z.A.; Alaçam, A.; Coleman, N.J. A 12-week assessment of the treatment of white spot lesions with cpp-acp paste and/or fluoride varnish. BioMed Res. Int. 2016, 2016, 8357621. [Google Scholar] [CrossRef] [Green Version]
- Heravi, F.; Ahrari, F.; Tanbakuchi, B. Effectiveness of MI paste plus and remin pro on remineralization and color improvement of postorthodontic white spot lesions. Dent. Res. J. 2018, 15, 19–103. [Google Scholar]
- Singh, S.; Singh, S.P.; Goyal, A.; Utreja, A.K.; Jena, A.K. Effects of various remineralizing agents on the outcome of post-orthodontic white spot lesions (WSLs): A clinical trial. Prog. Orthod. 2016, 17, 25. [Google Scholar] [CrossRef] [Green Version]
- González-Cabezas, C.; Fernandez, C.E. Recent advances in remineralization therapies for caries lesions. Adv. Dent. Res. 2018, 29, 55–59. [Google Scholar] [CrossRef] [PubMed]
- Llena, C.; Leyda, A.M.; Forner, L. CPP-ACP and CPP-ACFP versus fluoride varnish in remineralisation of early caries lesions. A prospective study. Eur. J. Paediatr. Dent. 2015, 16, 181–186. [Google Scholar] [PubMed]
- Moynihan, P. Sugars and dental caries: Evidence for setting a recommended threshold for intake. Adv. Nutr. Int. Rev. J. 2016, 7, 149–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marinho, V.C.; Chong, L.-Y.; Worthington, H.V.; Walsh, T. Fluoride mouthrinses for preventing dental caries in children and adolescents. Cochrane Database Syst. Rev. 2016, 2021, CD002284. [Google Scholar] [CrossRef]
- Marsh, P.D. Ecological Events in Oral Health and Disease: New Opportunities for Prevention and Disease Control? CDA J. 2017, 45, 525–537. [Google Scholar]
- Guo, L.; Edlund, A. Targeted antimicrobial peptides: A novel technology to eradicate harmful Streptococcus Mutans current anti-caries approaches. J. Calif. Dent. Assoc. 2017, 45, 557–564. [Google Scholar]
- Garcia, S.S.; Blackledge, M.S.; Michalek, S.; Su, L.; Patcek, T.; Eipers, P.; Morrow, C.; Lefkowitz, E.J.; Melander, C.; Wu, H. Targeting of Streptococcus Mutans by a novel small molecule prevents dental caries and preserves the oral microbiome. J. Dent. Res. 2017, 96, 807–814. [Google Scholar] [CrossRef]
- Gruner, D.; Paris, S.; Schwendicke, F. Probiotics for managing caries and periodontitis: Systematic review and meta-analysis. J. Dent. 2016, 48, 16–25. [Google Scholar] [CrossRef]
- Zaura, E.; Twetman, S. Critical appraisal of oral pre-and probiotics for caries prevention and care. Caries Res. 2019, 53, 514–526. [Google Scholar] [CrossRef]
- Liu, C.; Guo, J.; Yan, X.; Tang, Y.; Mazumder, A.; Wu, S.; Liang, Y. Antimicrobial nanomaterials against biofilms: An alternative strategy. Environ. Rev. 2017, 25, 225–244. [Google Scholar] [CrossRef] [Green Version]
- Koopman, J.E.; Hoogenkamp, M.A.; Buijs, M.J.; Brandt, B.W.; Keijser, B.J.; Crielaard, W.; Cate, J.M.T.; Zaura, E. Changes in the oral ecosystem induced by the use of 8% arginine toothpaste. Arch. Oral Biol. 2017, 73, 79–87. [Google Scholar] [CrossRef]
- Nascimento, M.; Browngardt, C.; Xiaohui, X.; Klepac-Ceraj, V.; Paster, B.; Burne, R. The effect of arginine on oral biofilm communities. Mol. Oral Microbiol. 2014, 29, 45–54. [Google Scholar] [CrossRef]
- Zheng, X.; Cheng, X.; Wang, L.; Qiu, W.; Wang, S.; Zhou, Y.; Li, M.; Li, Y.; Cheng, L.; Li, J.; et al. Combinatorial effects of arginine and fluoride on oral bacteria. J. Dent. Res. 2014, 94, 344–353. [Google Scholar] [CrossRef] [Green Version]
- Jiao, Y.; Tay, F.; Niu, L.-N.; Chen, J.-H. Advancing antimicrobial strategies for managing oral biofilm infections. Int. J. Oral Sci. 2019, 11, 28. [Google Scholar] [CrossRef] [Green Version]
- Meyer, F.; Enax, J.; Epple, M.; Amaechi, B.; Simader, B. Cariogenic biofilms: Development, properties, and biomimetic preventive agents. Dent. J. 2021, 9, 88. [Google Scholar] [CrossRef]
- Janus, M.M.; Crielaard, W.; Zaura, E.; Keijser, B.J.; Brandt, B.W.; Krom, B.P. A novel compound to maintain a healthy oral plaque ecology in vitro. J. Oral Microbiol. 2016, 8, 32513. [Google Scholar] [CrossRef] [Green Version]
- Frencken, J.E.; Peters, M.C.; Manton, D.; Leal, S.; Gordan, V.V.; Eden, E. Minimal intervention dentistry for managing dental caries—A review: Report of a fdi task group. Int. Dent. J. 2012, 62, 223–243. [Google Scholar] [CrossRef] [Green Version]
- Rokaya, D.; Srimaneepong, V.; Sapkota, J.; Qin, J.; Siraleartmukul, K.; Siriwongrungson, V. Polymeric materials and films in dentistry: An overview. J. Adv. Res. 2018, 14, 25–34. [Google Scholar] [CrossRef]
- Roque, L.; Castro, P.; Molpeceres, J.; Viana, A.S.; Roberto, A.; Reis, C.; Rijo, P.; Tho, I.; Sarmento, B.; Reis, C. Bioadhesive polymeric nanoparticles as strategy to improve the treatment of yeast infections in oral cavity: In-vitro and ex-vivo studies. Eur. Polym. J. 2018, 104, 19–31. [Google Scholar] [CrossRef]
- Ishihara, M.; Kishimoto, S.; Nakamura, S.; Sato, Y.; Hattori, H. Polyelectrolyte complexes of natural polymers and their biomedical applications. Polymers 2019, 11, 672. [Google Scholar] [CrossRef] [Green Version]
- Cao, W.; Zhang, Y.; Wang, X.; Li, Q.; Xiao, Y.; Li, P.; Wang, L.; Ye, Z.; Xing, X. Novel resin-based dental material with anti-biofilm activity and improved mechanical property by incorporating hydrophilic cationic copolymer functionalized nanodiamond. J. Mater. Sci. Mater. Med. 2018, 29, 162. [Google Scholar] [CrossRef]
- Fadaka, A.O.; Sibuyi, N.R.S.; Madiehe, A.M.; Meyer, M. Nanotechnology-based delivery systems for antimicrobial peptides. Pharmaceutics 2021, 13, 1795. [Google Scholar] [CrossRef]
- Rafique, M.; Sadaf, I.; Rafique, M.S.; Tahir, M.B. A review on green synthesis of silver nanoparticles and their applications. Artif. Cells Nanomed. Biotechnol. 2017, 45, 1272–1291. [Google Scholar] [CrossRef]
- Makvandi, P.; Josic, U.; Delfi, M.; Pinelli, F.; Jahed, V.; Kaya, E.; Ashrafizadeh, M.; Zarepour, A.; Rossi, F.; Zarrabi, A.; et al. Drug Delivery (Nano)platforms for oral and dental applications: Tissue regeneration, infection control, and cancer management. Adv. Sci. 2021, 8, 2004014. [Google Scholar] [CrossRef] [PubMed]
- Aboyewa, J.A.; Sibuyi, N.R.S.; Meyer, M.; Oguntibeju, O.O. Green synthesis of metallic nanoparticles using some selected medicinal plants from southern africa and their biological applications. Plants 2021, 10, 1929. [Google Scholar] [CrossRef] [PubMed]
- Peng, J.J.; Botelho, M.G.; Matinlinna, J.P. Silver compounds used in dentistry for caries management: A review. J. Dent. 2012, 40, 531–541. [Google Scholar] [CrossRef]
- Al-Ansari, M.M.; Al-Dahmash, N.D.; Ranjitsingh, A. Synthesis of silver nanoparticles using gum Arabic: Evaluation of its inhibitory action on Streptococcus mutans causing dental caries and endocarditis. J. Infect. Public Health 2021, 14, 324–330. [Google Scholar] [CrossRef] [PubMed]
- Noronha, V.; Paula, A.J.; Durán, G.; Galembeck, A.; Cogo-Muller, K.; Franz-Montan, M.; Durán, N. Silver nanoparticles in dentistry. Dent. Mater. 2017, 33, 1110–1126. [Google Scholar] [CrossRef] [PubMed]
- Tirupathi, S.P.; Svsg, N.; Rajasekhar, S.; Nuvvula, S. Comparative cariostatic efficacy of a novel Nano-silver fluoride varnish with 38% silver diamine fluoride varnish a double-blind randomized clinical trial. J. Clin. Exp. Dent. 2019, 11, e105–e112. [Google Scholar] [CrossRef] [PubMed]
- dos Santos, V.E., Jr.; Filho, A.V.; Targino, A.G.R.; Flores, M.A.P.; Galembeck, A.; Caldas, A.F.; Rosenblatt, A. A New “Silver-Bullet” to treat caries in children–Nano Silver Fluoride: A randomised clinical trial. J. Dent. 2014, 42, 945–951. [Google Scholar] [CrossRef] [Green Version]
- Gao, S.; Zhao, I.S.; Hiraishi, N.; Duangthip, D.; Mei, M.L.; Lo, E.; Chu, C. Clinical trials of silver diamine fluoride in arresting caries among children. JDR Clin. Transl. Res. 2016, 1, 201–210. [Google Scholar] [CrossRef]
- Koizumi, H.; Hamama, H.H.; Burrow, M.F. Effect of a silver diamine fluoride and potassium iodide-based desensitizing and cavity cleaning agent on bond strength to dentine. Int. J. Adhes. Adhes. 2016, 68, 54–61. [Google Scholar] [CrossRef]
- Lee, S.H.; Jun, B.-H. Silver nanoparticles: Synthesis and application for nanomedicine. Int. J. Mol. Sci. 2019, 20, 865. [Google Scholar] [CrossRef] [Green Version]
- Schwass, D.; Lyons, K.; Love, R.; Tompkins, G.; Meledandri, C. Antimicrobial activity of a colloidal AgNP suspension demonstrated in vitro against monoculture biofilms: Toward a novel tooth disinfectant for treating dental caries. Adv. Dent. Res. 2018, 29, 117–123. [Google Scholar] [CrossRef]
- Le Ouay, B.; Stellacci, F. Antibacterial activity of silver nanoparticles: A surface science insight. Nano Today 2015, 10, 339–354. [Google Scholar] [CrossRef] [Green Version]
- Dankovich, T.A.; Gray, D.G. Bactericidal paper impregnated with silver nanoparticles for point-of-use water treatment. Environ. Sci. Technol. 2011, 45, 1992–1998. [Google Scholar] [CrossRef]
- Sundeep, D.; Vijaya Kumar, T.; Rao, P.S.S.; Ravikumar, R.V.S.S.N.; Gopala Krishna, A. Green synthesis and characterization of Ag nanoparticles from Mangifera indica leaves for dental restoration and antibacterial applications. Prog. Biomater. 2017, 6, 57–66. [Google Scholar] [CrossRef] [Green Version]
- Carrouel, F.; Viennot, S.; Ottolenghi, L.; Gaillard, C.; Bourgeois, D. Nanoparticles as anti-microbial, anti-inflammatory, and remineralizing agents in oral care cosmetics: A review of the current situation. Nanomaterials 2020, 10, 140. [Google Scholar] [CrossRef] [Green Version]
- González-Luna, P.-I.; Martinez-Castanon, G.-A.; Zavala-Alonso, N.-V.; Patiño-Marin, N.; Niño, N.; Martínez, J.M.; Ramírez-González, J.-H. Bactericide effect of silver nanoparticles as a final irrigation agent in endodontics on Enterococcus Faecalis: An ex vivo study. J. Nanomater. 2016, 2016, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Acosta-Torres, L.S.; Mendieta, I.; Nuñez-Anita, R.E.; Cajero-Juárez, M.; Castaño, V.M. Cytocompatible antifungal acrylic resin containing silver nanoparticles for dentures. Int. J. Nanomed. 2012, 7, 4777–4786. [Google Scholar] [CrossRef] [Green Version]
- Kligman, S.; Ren, Z.; Chung, C.-H.; Perillo, M.; Chang, Y.-C.; Koo, H.; Zheng, Z.; Li, C. The impact of dental implant surface modifications on osseointegration and biofilm formation. J. Clin. Med. 2021, 10, 1641. [Google Scholar] [CrossRef]
- Zhu, Y.; Cao, H.; Qiao, S.; Gu, Y.; Luo, H.; Liu, X.; Lai, H.; Wang, M.; Meng, F. Hierarchical micro/nanostructured titanium with balanced actions to bacterial and mammalian cells for dental implants. Int. J. Nanomed. 2015, 10, 6659–6674. [Google Scholar] [CrossRef] [Green Version]
- Rani, S.; Chandra, R.V.; Reddy, A.A.; Reddy, B.H.; Nagarajan, S.; Naveen, A. Evaluation of the antibacterial effect of silver nanoparticles on guided tissue regeneration membrane colonization--An in vitro study. J. Int. Acad. Periodontol. 2015, 17, 66–76. [Google Scholar]
- Hernández-Sierra, J.F.; Ruiz, F.; Pena, D.C.C.; Martínez-Gutiérrez, F.; Martínez, A.E.; Pozos-Guillen, A.; Tapia-Pérez, H.; Martinez-Castanon, G.-A. The antimicrobial sensitivity of Streptococcus mutans to nanoparticles of silver, zinc oxide, and gold. Nanomed. Nanotechnol. Biol. Med. 2008, 4, 237–240. [Google Scholar] [CrossRef] [PubMed]
- Panpaliya, N.P.; Dahake, P.T.; Kale, Y.J.; Dadpe, M.V.; Kendre, S.B.; Siddiqi, A.G.; Maggavi, U.R. In vitro evaluation of antimicrobial property of silver nanoparticles and chlorhexidine against five different oral pathogenic bacteria. Saudi Dent. J. 2018, 31, 76–83. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Zhang, T.; Li, P.; Huang, W.; Tang, J.; Wang, P.; Liu, J.; Yuan, Q.; Bai, R.; Li, B.; et al. Use of synchrotron radiation-analytical techniques to reveal chemical origin of silver-nanoparticle cytotoxicity. ACS Nano 2015, 9, 6532–6547. [Google Scholar] [CrossRef] [PubMed]
- Chien, C.-S.; Lin, C.-J.; Ko, C.-J.; Tseng, S.-P.; Shih, C.-J. Antibacterial activity of silver nanoparticles (AgNP) confined to mesostructured silica against methicillin-resistant Staphylococcus aureus (MRSA). J. Alloy. Compd. 2018, 747, 1–7. [Google Scholar] [CrossRef]
- Panzarini, E.; Mariano, S.; Vergallo, C.; Carata, E.; Fimia, G.M.; Mura, F.; Rossi, M.; Vergaro, V.; Ciccarella, G.; Corazzari, M.; et al. Glucose capped silver nanoparticles induce cell cycle arrest in HeLa cells. Toxicol. Vitr. 2017, 41, 64–74. [Google Scholar] [CrossRef] [PubMed]
- He, H.; Tao, G.; Wang, Y.; Cai, R.; Guo, P.; Chen, L.; Zuo, H.; Zhao, P.; Xia, Q. In situ green synthesis and characterization of sericin-silver nanoparticle composite with effective antibacterial activity and good biocompatibility. Mater. Sci. Eng. C 2017, 80, 509–516. [Google Scholar] [CrossRef] [PubMed]
- Nqakala, Z.B.; Sibuyi, N.R.S.; Fadaka, A.O.; Meyer, M.; Onani, M.O.; Madiehe, A.M. Advances in nanotechnology towards development of silver nanoparticle-based wound-healing agents. Int. J. Mol. Sci. 2021, 22, 11272. [Google Scholar] [CrossRef] [PubMed]
- Abdelghany, T.M.; Al-Rajhi, A.M.H.; Al Abboud, M.A.; AlAwlaqi, M.M.; Magdah, A.G.; Helmy, E.A.M.; Mabrouk, A.S. Recent advances in green synthesis of silver nanoparticles and their applications: About future directions. A review. BioNanoScience 2017, 8, 5–16. [Google Scholar] [CrossRef]
- Emmanuel, R.; Palanisamy, S.; Chen, S.-M.; Chelladurai, K.; Padmavathy, S.; Saravanan, M.; Prakash, P.; Ali, M.A.; Al-Hemaid, F.M. Antimicrobial efficacy of green synthesized drug blended silver nanoparticles against dental caries and periodontal disease causing microorganisms. Mater. Sci. Eng. C 2015, 56, 374–379. [Google Scholar] [CrossRef]
- Mousavi, S.M.; Hashemi, S.A.; Ghasemi, Y.; Atapour, A.; Amani, A.M.; Savar Dashtaki, A.; Babapoor, A.; Arjmand, O. Green synthesis of silver nanoparticles toward bio and medical applications: Review study. Artif. Cells Nanomed. Biotechnol. 2018, 46, S855–S872. [Google Scholar] [CrossRef] [Green Version]
- Majoumouo, M.S.; Sibuyi, N.R.S.; Tincho, M.B.; Mbekou, M.; Boyom, F.F.; Meyer, M. Enhanced anti-bacterial activity of biogenic silver nanoparticles synthesized from Terminalia mantaly Extracts. Int. J. Nanomed. 2019, ume 14, 9031–9046. [Google Scholar] [CrossRef] [Green Version]
- Simon, S.; Sibuyi, N.R.S.; Fadaka, A.O.; Meyer, M.; Madiehe, A.M.; du Preez, M.G. The antimicrobial activity of biogenic silver nanoparticles synthesized from extracts of Red and Green European pear cultivars. Artif. Cells Nanomed. Biotechnol. 2021, 49, 614–625. [Google Scholar] [CrossRef]
- Verma, A.; Gautam, S.P.; Bansal, K.K.; Prabhakar, N.; Rosenholm, J.M. Green nanotechnology: Advancement in phytoformulation research. Medicines 2019, 6, 39. [Google Scholar] [CrossRef] [Green Version]
- Velusamy, P.; Das, J.; Pachaiappan, R.; Vaseeharan, B.; Pandian, K. Greener approach for synthesis of antibacterial silver nanoparticles using aqueous solution of neem gum (Azadirachta indica L.). Ind. Crop. Prod. 2015, 66, 103–109. [Google Scholar] [CrossRef]
- Srikar, S.K.; Giri, D.D.; Pal, D.B.; Mishra, P.K.; Upadhyay, S.N. Green synthesis of silver nanoparticles: A review. Green Sustain. Chem. 2016, 6, 34–56. [Google Scholar] [CrossRef] [Green Version]
- Shaikh, W.A.; Chakraborty, S.; Owens, G.; Islam, R.U. A review of the phytochemical mediated synthesis of AgNP (silver nanoparticle): The wonder particle of the past decade. Appl. Nanosci. 2021, 11, 2625–2660. [Google Scholar] [CrossRef]
- Sadeghi, B.; Gholamhoseinpoor, F. A study on the stability and green synthesis of silver nanoparticles using Ziziphora tenuior (Zt) extract at room temperature. Spectrochim. Acta Part A Mol. Biomol. Spectrosc. 2015, 134, 310–315. [Google Scholar] [CrossRef]
- Khalil, M.M.H.; Ismail, E.H.; El-Baghdady, K.Z.; Mohamed, D. Green synthesis of silver nanoparticles using olive leaf extract and its antibacterial activity. Arab. J. Chem. 2014, 7, 1131–1139. [Google Scholar] [CrossRef] [Green Version]
- Ortega-Arroyo, L.; Martin-Martinez, E.S.; Aguilar-Mendez, M.A.; Cruz-Orea, A.; Hernandez-Pérez, I.; Glorieux, C. Green synthesis method of silver nanoparticles using starch as capping agent applied the methodology of surface response. Starch-Stärke 2013, 65, 814–821. [Google Scholar] [CrossRef]
- Ashraf, S.; Abbasi, A.Z.; Pfeiffer, C.; Hussain, S.Z.; Khalid, Z.M.; Gil, P.R.; Parak, W.J.; Hussain, I. Protein-mediated synthesis, pH-induced reversible agglomeration, toxicity and cellular interaction of silver nanoparticles. Colloids Surf. B Biointerfaces 2013, 102, 511–518. [Google Scholar] [CrossRef]
- Tagad, C.; Dugasani, S.R.; Aiyer, R.; Park, S.; Kulkarni, A.; Sabharwal, S. Green synthesis of silver nanoparticles and their application for the development of optical fiber based hydrogen peroxide sensor. Sens. Actuators B Chem. 2013, 183, 144–149. [Google Scholar] [CrossRef]
- Fayaz, A.M.; Balaji, K.; Kalaichelvan, P.; Venkatesan, R. Fungal based synthesis of silver nanoparticles—An effect of temperature on the size of particles. Colloids Surf. B Biointerfaces 2009, 74, 123–126. [Google Scholar] [CrossRef] [PubMed]
- Kadam, J.; Dhawal, P.; Barve, S.; Kakodkar, S. Green synthesis of silver nanoparticles using cauliflower waste and their multifaceted applications in photocatalytic degradation of methylene blue dye and Hg2+ biosensing. SN Appl. Sci. 2020, 2, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Tyavambiza, C.; Elbagory, A.; Madiehe, A.; Meyer, M.; Meyer, S. The antimicrobial and anti-inflammatory effects of silver nanoparticles synthesised from Cotyledon orbiculata aqueous extract. Nanomaterials 2021, 11, 1343. [Google Scholar] [CrossRef] [PubMed]
- Dube, P.; Meyer, S.; Madiehe, A.; Meyer, M. Antibacterial activity of biogenic silver and gold nanoparticles synthesized from Salvia africana-lutea and Sutherlandia frutescens. Nanotechnology 2020, 31, 505607. [Google Scholar] [CrossRef] [PubMed]
- Abubacker, M.N.; Sathya, C. Synthesis of silver nanoparticles from plant chewing sticks and their antibacterial activity on dental pathogen. Br. Biomed. Bull. 2015, 3, 81–93. [Google Scholar]
- Inbakandan, D.; Kumar, C.; Bavanilatha, M.; Ravindra, D.N.; Kirubagaran, R.; Khan, S.A. Ultrasonic-assisted green synthesis of flower like silver nanocolloids using marine sponge extract and its effect on oral biofilm bacteria and oral cancer cell lines. Microb. Pathog. 2016, 99, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Suwan, T.; Khongkhunthian, S.; Okonogi, S. Green synthesis and inhibitory effects against oral pathogens of silver nanoparticles mediated by rice extracts. Drug Discov. Ther. 2018, 12, 189–196. [Google Scholar] [CrossRef] [Green Version]
- Luckie, R.A.M.; Casatañares, R.L.; Schougall, R.; Reyes, S.C.G.; Mendieta, V.S. Antibacterial effect of silver nanoparticles versus Chlorhexidine against Streptococcus mutans and Lactobacillus casei. In Silver Nanoparticles-Fabrication, Characterization and Applications; IntechOpen: London, UK, 2018. [Google Scholar] [CrossRef] [Green Version]
- Souza, J.A.; Barbosa, D.B.; A Berretta, A.; Amaral, J.G.D.; Gorup, L.F.; Neto, F.N.D.S.; A Fernandes, R.; Fernandes, G.L.; Camargo, E.R.; Agostinho, A.M.; et al. Green synthesis of silver nanoparticles combined to calcium glycerophosphate: Antimicrobial and antibiofilm activities. Futur. Microbiol. 2018, 13, 345–357. [Google Scholar] [CrossRef] [Green Version]
- Venkatesham, M.; Ayodhya, D.; Madhusudhan, A.; Veerabhadram, G. Synthesis of stable silver nanoparticles using gum acacia as reducing and stabilizing agent and study of its microbial properties: A novel green approach. Int. J. Green Nanotechnol. 2012, 4, 199–206. [Google Scholar] [CrossRef]
- Juby, K.; Dwivedi, C.; Kumar, M.; Kota, S.; Misra, H.; Bajaj, P. Silver nanoparticle-loaded PVA/gum acacia hydrogel: Synthesis, characterization and antibacterial study. Carbohydr. Polym. 2012, 89, 906–913. [Google Scholar] [CrossRef]
- Pal, S.; Tak, Y.K.; Song, J.M. Does the antibacterial activity of silver nanoparticles depend on the shape of the nanoparticle? A Study of the Gram-Negative Bacterium Escherichia coli. Appl. Environ. Microbiol. 2007, 73, 1712–1720. [Google Scholar] [CrossRef] [Green Version]
- Jinu, U.; Gomathi, M.; Saiqa, I.; Geetha, N.; Benelli, G.; Venkatachalam, P. Green engineered biomolecule-capped silver and copper nanohybrids using Prosopis cineraria leaf extract: Enhanced antibacterial activity against microbial pathogens of public health relevance and cytotoxicity on human breast cancer cells (MCF-7). Microb. Pathog. 2017, 105, 86–95. [Google Scholar] [CrossRef]
- Lu, Z.; Rong, K.; Li, J.; Yang, H.; Chen, R. Size-dependent antibacterial activities of silver nanoparticles against oral anaerobic pathogenic bacteria. J. Mater. Sci. Mater. Med. 2013, 24, 1465–1471. [Google Scholar] [CrossRef]
- Espinosa-Cristóbal, L.; Martínez-Castañón, G.; Téllez-Déctor, E.; Niño-Martínez, N.; Zavala-Alonso, N.; Loyola-Rodríguez, J. Adherence inhibition of Streptococcus mutans on dental enamel surface using silver nanoparticles. Mater. Sci. Eng. C 2013, 33, 2197–2202. [Google Scholar] [CrossRef]
- Hong, X.; Wen, J.; Xiong, X.; Hu, Y. Shape effect on the antibacterial activity of silver nanoparticles synthesized via a microwave-assisted method. Environ. Sci. Pollut. Res. 2015, 23, 4489–4497. [Google Scholar] [CrossRef]
- Naraginti, S.; Sivakumar, A. Eco-friendly synthesis of silver and gold nanoparticles with enhanced bactericidal activity and study of silver catalyzed reduction of 4-nitrophenol. Spectrochim. Acta Part A Mol. Biomol. Spectrosc. 2014, 128, 357–362. [Google Scholar] [CrossRef]
- Junior, V.E.D.S.; Targino, A.G.R.; Flores, M.A.P.; Rodríguez-Díaz, J.M.; Teixeira, J.A.; Heimer, M.V.; Pessoa, H.D.L.F.; Galembeck, A.; Rosenblatt, A. Antimicrobial activity of silver nanoparticle colloids of different sizes and shapes against Streptococcus mutans. Res. Chem. Intermed. 2017, 43, 5889–5899. [Google Scholar] [CrossRef]
- Xiu, Z.-M.; Zhang, Q.-B.; Puppala, H.L.; Colvin, V.L.; Alvarez, P.J.J. Negligible particle-specific antibacterial activity of silver nanoparticles. Nano Lett. 2012, 12, 4271–4275. [Google Scholar] [CrossRef]
- Lara, H.H.; Ixtepan-Turrent, L.; Garza-Treviño, E.N.; Rodriguez-Padilla, C. PVP-coated silver nanoparticles block the transmission of cell-free and cell-associated hiv-1 in human cervical culture. J. Nanobiotechnology 2010, 8, 15. [Google Scholar] [CrossRef] [Green Version]
- Dakal, T.C.; Kumar, A.; Majumdar, R.S.; Yadav, V. Mechanistic basis of antimicrobial actions of silver nanoparticles. Front. Microbiol. 2016, 7, 1831. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hadrup, N.; Lam, H.R. Oral toxicity of silver ions, silver nanoparticles and colloidal silver – A review. Regul. Toxicol. Pharmacol. 2014, 68, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Medina, C.; Inkielewicz-Stepniak, I.; Santos-Martinez, M.J.; Radomski, M.W. Pharmacological and toxicological effects of co-exposure of human gingival fibroblasts to silver nanoparticles and sodium fluoride. Int. J. Nanomed. 2014, 9, 1677–1687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, T.; Wang, L.; Chen, Q.; Chen, C. Cytotoxic potential of silver nanoparticles. Yonsei Med. J. 2014, 55, 283–291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taleghani, F.; Yaraii, R.; Sadeghi, R.; Haghgoo, R.; Rezvani, M.B. Cytotoxicity of silver nanoparticles on human gingival epithelial cells: An in vitro study introduction. J. Dent. Sch. 2014, 31, 220–226. [Google Scholar]
- Niska, K.; Knap, N.; Kędzia, A.; Jaskiewicz, M.; Kamysz, W.; Inkielewicz-Stepniak, I. Capping agent-dependent toxicity and antimicrobial activity of silver nanoparticles: An in vitro study. concerns about potential application in dental practice. Int. J. Med Sci. 2016, 13, 772–782. [Google Scholar] [CrossRef] [Green Version]
- Vazquez-Munoz, R.; Borrego, B.; Juarez-Moreno, K.; García-García, M.; Mota-Morales, J.D.; Bogdanchikova, N.; Huerta-Saquero, A. Toxicity of silver nanoparticles in biological systems: Does the complexity of biological systems matter? Toxicol. Lett. 2017, 276, 11–20. [Google Scholar] [CrossRef]
- Salarian, A.; Mollamahale, Y.B.; Hami, Z.; Soltani-Rezaee-Rad, M. Cephalexin nanoparticles: Synthesis, cytotoxicity and their synergistic antibacterial study in combination with silver nanoparticles. Mater. Chem. Phys. 2017, 198, 125–130. [Google Scholar] [CrossRef]
- García-Contreras, R.; Argueta-Figueroa, L.; Mejía-Rubalcava, C.; Jiménez-Martínez, R.; Cuevas-Guajardo, S.; Sánchez-Reyna, P.A.; Zeron, H.M. Perspectives for the use of silver nanoparticles in dental practice. Int. Dent. J. 2011, 61, 297–301. [Google Scholar] [CrossRef]
- Sudha, A.; Jeyakanthan, J.; Srinivasan, P. Green synthesis of silver nanoparticles using Lippia nodiflora aerial extract and evaluation of their antioxidant, antibacterial and cytotoxic effects. Resour. Technol. 2017, 3, 506–515. [Google Scholar] [CrossRef]
- El Mahdy, M.M.; Eldin, T.A.S.; Aly, H.S.; Mohammed, F.F.; Shaalan, M. Evaluation of hepatotoxic and genotoxic potential of silver nanoparticles in albino rats. Exp. Toxicol. Pathol. 2015, 67, 21–29. [Google Scholar] [CrossRef] [PubMed]
- Galbiati, V.; Cornaghi, L.; Gianazza, E.; Potenza, M.A.; Donetti, E.; Marinovich, M.; Corsini, E. In vitro assessment of silver nanoparticles immunotoxicity. Food Chem. Toxicol. 2018, 112, 363–374. [Google Scholar] [CrossRef] [PubMed]
- Nosrati, H.; Hamzepoor, M.; Sohrabi, M.; Saidijam, M.; Assari, M.J.; Shabab, N.; Mahmoudian, Z.G.; Alizadeh, Z. The potential renal toxicity of silver nanoparticles after repeated oral exposure and its underlying mechanisms. BMC Nephrol. 2021, 22, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Salama, A. Dicarboxylic cellulose decorated with silver nanoparticles as sustainable antibacterial nanocomposite material. Environ. Nanotechnol. Monit. Manag. 2017, 8, 228–232. [Google Scholar] [CrossRef]
- Boudreau, M.D.; Imam, M.S.; Paredes, A.M.; Bryant, M.S.; Cunningham, C.K.; Felton, R.P.; Jones, M.Y.; Davis, K.J.; Olson, G.R. Differential effects of silver nanoparticles and silver ions on tissue accumulation, distribution, and toxicity in the sprague dawley rat following daily oral gavage administration for 13 Weeks. Toxicol. Sci. 2016, 150, 131–160. [Google Scholar] [CrossRef]
- Kim, Y.S.; Song, M.Y.; Park, J.D.; Song, K.S.; Ryu, H.R.; Chung, Y.H.; Chang, H.K.; Lee, J.H.; Oh, K.H.; Kelman, B.J.; et al. Subchronic oral toxicity of silver nanoparticles. Part. Fibre Toxicol. 2010, 7, 20. [Google Scholar] [CrossRef] [Green Version]
- van der Zande, M.; Vandebriel, R.J.; Van Doren, E.; Kramer, E.; Rivera, Z.H.; Serrano-Rojero, C.S.; Gremmer, E.R.; Mast, J.; Peters, R.J.B.; Hollman, P.C.H.; et al. Distribution, elimination, and toxicity of silver nanoparticles and silver ions in rats after 28-day oral exposure. ACS Nano 2012, 6, 7427–7442. [Google Scholar] [CrossRef]
- Ribeiro, A.; Anbu, S.; Alegria, E.; Fernandes, A.; Baptista, P.; Mendes, R.; Matias, A.; Mendes, M.; da Silva, M.G.; Pombeiro, A. Evaluation of cell toxicity and DNA and protein binding of green synthesized silver nanoparticles. Biomed. Pharmacother. 2018, 101, 137–144. [Google Scholar] [CrossRef] [Green Version]
- Wen, R.; Yang, X.; Hu, L.; Sun, C.; Zhou, Q.; Jiang, G. Brain-targeted distribution and high retention of silver by chronic intranasal instillation of silver nanoparticles and ions in Sprague-Dawley rats. J. Appl. Toxicol. 2015, 36, 445–453. [Google Scholar] [CrossRef] [Green Version]
- Saraf, S.; Alexander, A. Nose-to-brain drug delivery approach: A key to easily accessing the brain for the treatment of Alzheimer’s disease. Neural Regen. Res. 2018, 13, 2102–2104. [Google Scholar] [CrossRef]
- Takamiya, A.S.; Monteiro, D.R.; Bernabé, D.; Gorup, L.F.; Camargo, E.R.; Gomes-Filho, J.E.; Oliveira, S.H.P.; Barbosa, D.B. In vitro and in vivo toxicity evaluation of colloidal silver nanoparticles used in endodontic treatments. J. Endod. 2016, 42, 953–960. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lotfi, M.; Vosoughhosseini, S.; Ranjkesh, B.; Khani, S.; Saghiri, M.; Zand, A. Antimicrobial efficacy of nanosilver, sodium hypochlorite and chlorhexidine gluconate against Enterococcus faecalis. Afr. J. Biotechnol. 2011, 10, 6799–6803. [Google Scholar] [CrossRef]
- Franková, J.; Pivodová, V.; Vágnerová, H.; Juránová, J.; Ulrichova, J. Effects of silver nanoparticles on primary cell cultures of fibroblasts and keratinocytes in a wound-healing model. J. Appl. Biomater. Funct. Mater. 2016, 14, e137–e142. [Google Scholar] [CrossRef] [PubMed]
- Burdușel, A.-C.; Gherasim, O.; Grumezescu, A.M.; Mogoantă, L.; Ficai, A.; Andronescu, E. Biomedical Applications of silver nanoparticles: An up-to-date overview. Nanomaterials 2018, 8, 681. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akter, M.; Sikder, M.T.; Rahman, M.M.; Ullah, A.K.M.A.; Hossain, K.F.B.; Banik, S.; Hosokawa, T.; Saito, T.; Kurasaki, M. A systematic review on silver nanoparticles-induced cytotoxicity: Physicochemical properties and perspectives. J. Adv. Res. 2018, 9, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Luis, O.E.; Hernandez-Delgadillo, R.; Sánchez-Nájera, R.I.; Martínez-Castañón, G.A.; Niño-Martínez, N.; Navarro, M.D.C.S.; Ruiz, F.; Cabral-Romero, C. Green synthesis of silver nanoparticles and their bactericidal and antimycotic activities against oral microbes. J. Nanomater. 2016, 2016, 9204573. [Google Scholar] [CrossRef] [Green Version]
- Moritz, M.; Geszke-Moritz, M. The newest achievements in synthesis, immobilization and practical applications of antibacterial nanoparticles. Chem. Eng. J. 2013, 228, 596–613. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Caries Prevention Agents | Examples | Formulation Type/Tools | Action | Limitation | Refs |
|---|---|---|---|---|---|
| Oral hygiene | Toothbrush Dental floss Mini-brushes Oral irrigators | Delay or prevent oral biofilm formation | Flossing alone may not be effective in reducing caries Personal skills influence the outcome Must be used in combination with toothpaste | [27,29,30] | |
| Diet modification | Sugar reduction | Food | Control biofilm formation by eliminating plaque Lowers the rate of dental caries | Reducing sugar content is less successful Dietary control of sugar is a challenge | [33,34] |
| Saliva substitutes | Cleans the oral cavity and the pH buffering capacity | [35] | |||
| Fluoride | Toothpaste Varnish Gel Mouthwash Tablets Drops Chewing gum Lozenge | Remineralization | Fluoride classified as a neurotoxicantContinuous use can lead to fluoride-resistant strains Excessive use can lead to tooth fluorosis, discoloration, and gastrointestinal problems Skeletal fluorosis can cause disabilities such as chronic joint pain, stiffness of joint, sporadic pain, calcification of ligaments, and osteosclerosis | [24,36,37] | |
| Non-fluoridated (calcium-based) agents | Amorphous Calcium Phosphate (ACP) | Added into a fluoride toothpaste | Remineralization | Reduce root caries Unstabilized ACP promote dental calculus deposition on the teeth ACP interferes with remineralization by removing free fluoride ions in the oral environment | [21,38] |
| Casein Phosphopeptide- ACP (CPP-ACP) | |||||
| Antimicrobial Therapies | Chlorohexidine (CHX) | Mouthwash | Antimicrobial agent | Brownish staining of the teeth, removable by discontinuing the product Altered taste, persist for several hours after use Oral burning Development of lesions and ulcerations of the gingival mucosa Has a strong, unpleasant taste | [39] |
| Probiotics Prebiotics | Probiotics: dairy products, fermented vegetables, sourdough bread, drops, tablets, and lozenges containing various strains | Reduce harmful gastrointestinal microorganisms, discomfort, and stimulate the immune system | [26,40] | ||
| Prebiotics: chewing gum, oral rinse | Stimulate growth and/or activity of bacteria already resident in the host colon Inhibit the attachment of pathogenic bacteria Alters pH of the environment Stimulate the immune system | [41,42] | |||
| Sugar substitute (sweeteners), e.g, Stevia, Xylitol | Chewing gum | Stevia: reduces plaque formation Acts as a healing agent at the periodontium level | [26] | ||
| Xylitol: reduces plaque formation, and bacterial adherenceInhibits enamel demineralization (i.e., reduces acid production) | [43] |
| AgNP Formulation | Study Title | Conditions | AgNP Activity | Status Online | NCT Identifier |
|---|---|---|---|---|---|
| AgNPs in vanishing cream | Topical silver nanoparticles for microbial activity | Foot fungal and bacterial infections (tinea pedis, capitis, versicolor) | Antimicrobial | Recruiting | NCT03752424 |
| Innocuous containing gel AgNPs | Topical application of silver nanoparticles and oral pathogens in ill patients | Critical patients in ICU (coma or induced coma) | Antimicrobial | Completed | NCT02761525 |
| AgNPs | Silver nanoparticles in multidrug resistant bacteria | Critically ill patients | Antimicrobial | Completed | NCT04431440 |
| 5% NSSF | Nano-silver fluoride to prevent dental biofilms growth | Dental caries | Antimicrobial | Completed | NCT01950546 |
| AgNPs incorporated into the primer orthodontic Transbond XT | Addition of silver nanoparticles to an orthodontic primer in preventing enamel demineralization adjacent brackets | Dental caries | Tooth demineralization | - | NCT02400957 |
| Mouthwash and nose rinse with AgNPs | Evaluation of silver nanoparticles for the prevention of COVID-19 | COVID-19 | SARS-CoV-2 activity | Completed | NCT04894409 |
| Colloidal silver | Colloidal silver, treatment of COVID-19 | Severe Acute Respiratory Syndrome | Recruiting | NCT04978025 | |
| Fluor dental varnish with 25% AgNPs | Fluor varnish with silver nanoparticles for dental remineralization in patients with Trisomy 21 | Dental caries in Trisomy 21 children | Remineralization | Active, not recruiting | NCT01975545 |
| Nano-silver fluoride solution | Radiographic assessment of glass ionomer restorations with and without prior application of nano- silver fluoride in occlusal carious molars treated with partial caries removal technique | Partial dentin caries removal | Caries arrest prior to glass ionomer restoration | Completed | NCT03193606 |
| Hydrogel/nano silver-based dressing | Evaluation of diabetic foot wound healing using hydrogel/nano-silver-based dressing vs. traditional dressing | Diabetic foot ulcer | Wound healing | Completed | NCT04834245 |
| Central venous catheter impregnated with AgNPs (AgTive®) | Comparison of central venous catheters with silver nanoparticles vs. conventional catheters | Central venous catheter-related infections | Completed | NCT00337714 | |
| Silver colloid | The effectiveness of topical silver colloid in treating patients with recalcitrant chronic rhinosinusitis | Recalcitrant Chronic rhinosinusitis | Completed | NCT02403479 | |
| Nano-silver (SilvaSorb®) gel | Efficacy of silver nanoparticle gel vs. a common antibacterial hand gel | Antimicrobial | - | NCT00659204 | |
| Nano-silver Fluoride | Remineralization of dentine caries using two remineralizing agents which are nano-silver fluoride and casein phosphopeptides amorphous calcium phosphate | Dental caries | Remineralization | recruiting | NCT04930458 |
| Nano-silver fluoride | Effect of using different varnishes on dentin hypersensitivity; Na fluoride and nano-silver fluoride | Dentin hypersensitivity | Tooth hypersensitivity | Not yet recruiting | NCT04731766 |
| Nano-silver fluoride varnish | P11-4 and nano-silver fluoride varnish in treatment of white spot carious lesions | WSL | Remineralization in permanent teeth | recruiting | NCT04929509 |
| Nano silver fluoride solution | Antibacterial effect of nano silver fluoride vs. chlorhexidine on occlusal carious molars treated with partial caries removal technique | Dental caries | Antibacterial | Completed | NCT03186261 |
| Nano silver fluoride | Clinical and radiographic evaluation of nano silver fluoride vs. calcium hydroxide in indirect pulp treatment of deep carious second primary molars, randomized clinical trial | Deep caries | - | NCT04005872 | |
| AgNPs vs. copper NPs | Effect of metallic nanoparticles on nosocomial bacteria | Nosocomial infections | Antibacterial | Recruiting | NCT04775238 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahmed, O.; Sibuyi, N.R.S.; Fadaka, A.O.; Madiehe, M.A.; Maboza, E.; Meyer, M.; Geerts, G. Plant Extract-Synthesized Silver Nanoparticles for Application in Dental Therapy. Pharmaceutics 2022, 14, 380. https://doi.org/10.3390/pharmaceutics14020380
Ahmed O, Sibuyi NRS, Fadaka AO, Madiehe MA, Maboza E, Meyer M, Geerts G. Plant Extract-Synthesized Silver Nanoparticles for Application in Dental Therapy. Pharmaceutics. 2022; 14(2):380. https://doi.org/10.3390/pharmaceutics14020380
Chicago/Turabian StyleAhmed, Omnia, Nicole Remaliah Samantha Sibuyi, Adewale Oluwaseun Fadaka, Madimabe Abram Madiehe, Ernest Maboza, Mervin Meyer, and Greta Geerts. 2022. "Plant Extract-Synthesized Silver Nanoparticles for Application in Dental Therapy" Pharmaceutics 14, no. 2: 380. https://doi.org/10.3390/pharmaceutics14020380