Doxycycline-Eluting Core-Shell Type Nanofiber-Covered Trachea Stent for Inhibition of Cellular Metalloproteinase and Its Related Fibrotic Stenosis

Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Preparation of Nanofiber Solution
2.3. Fabrication of Core and Core-shell Type Nanofiber
2.4. High-Performance Liquid Chromatography (HPLC)
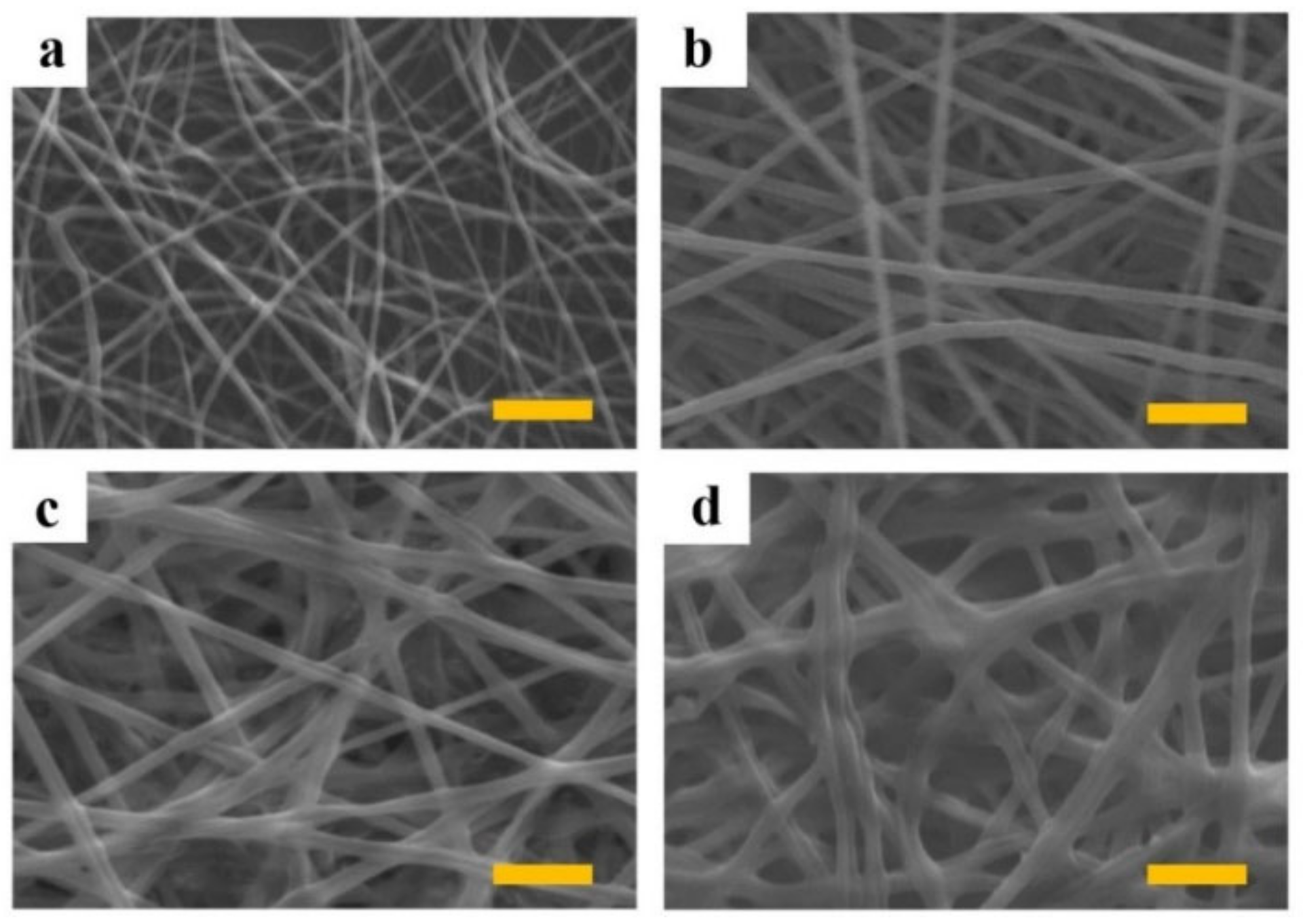
2.5. Scanning Electron Microscopy (SEM)
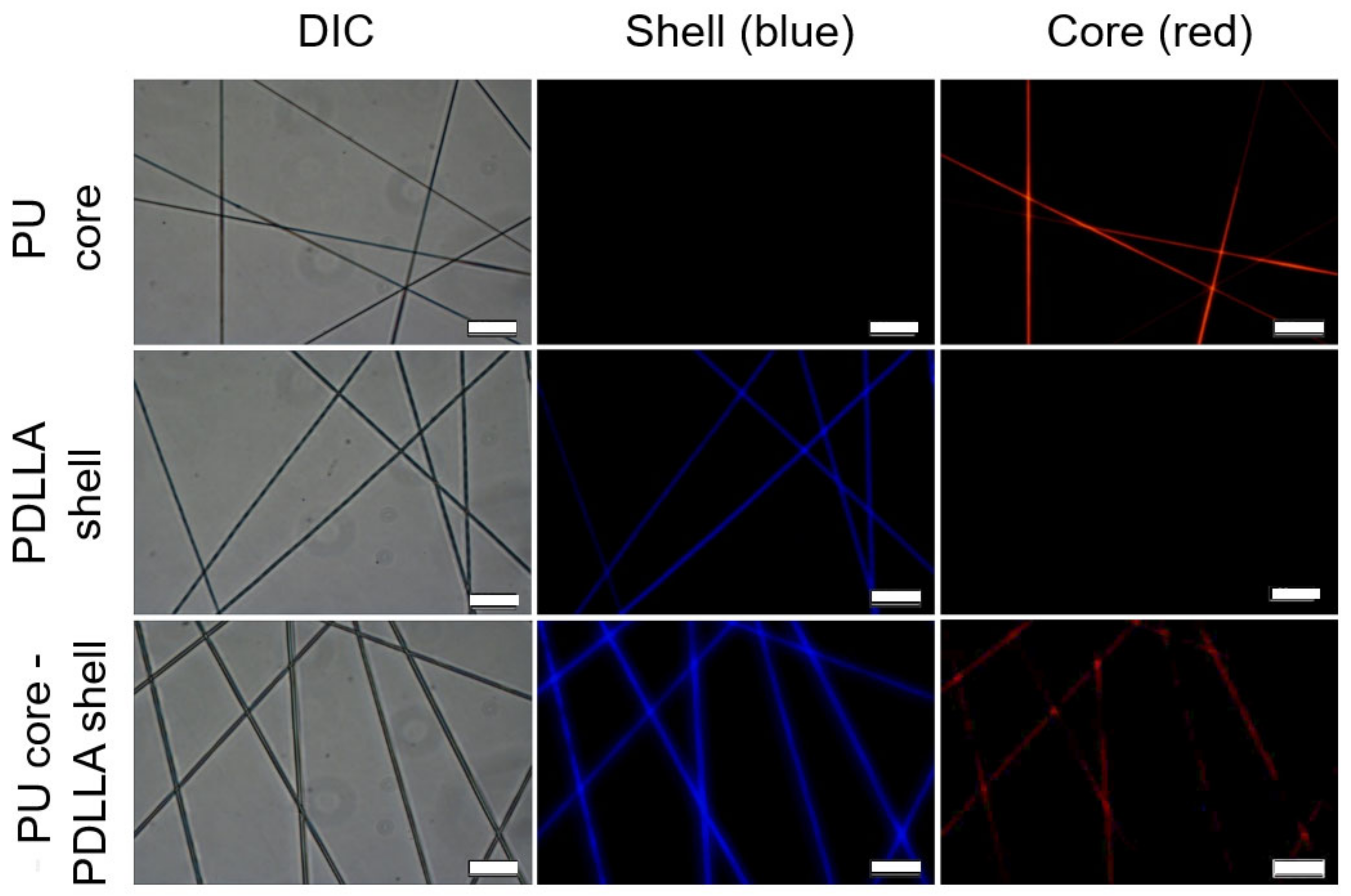
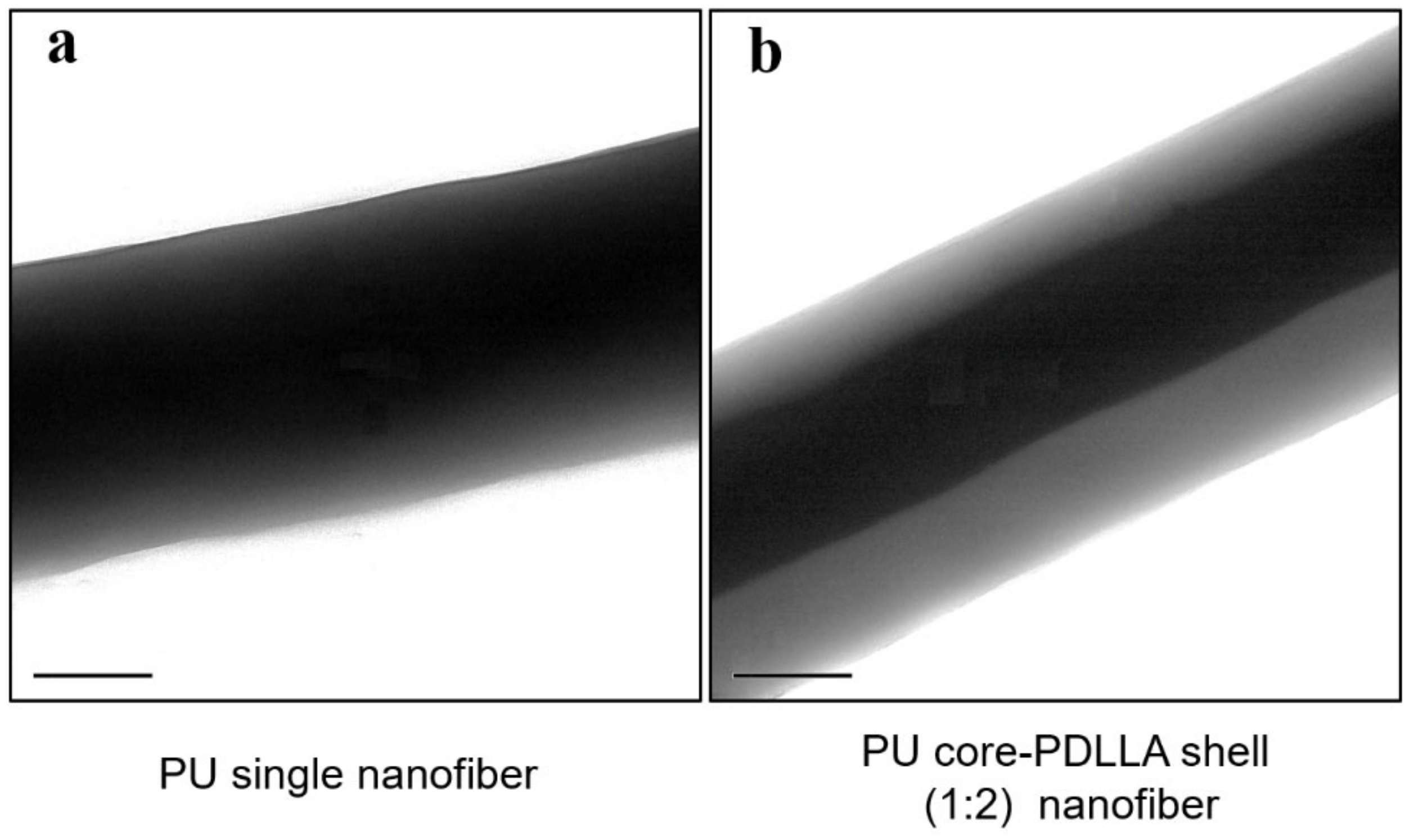
2.6. Identification of the Core-shell Structure
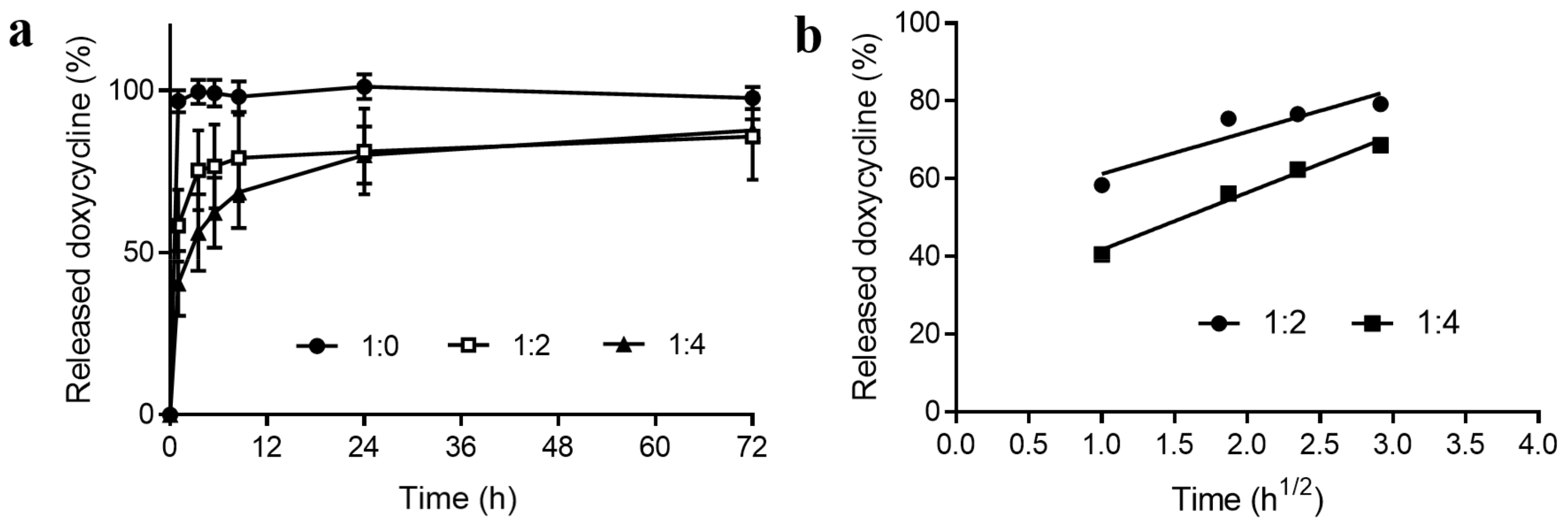
2.7. Doxycycline Release Study
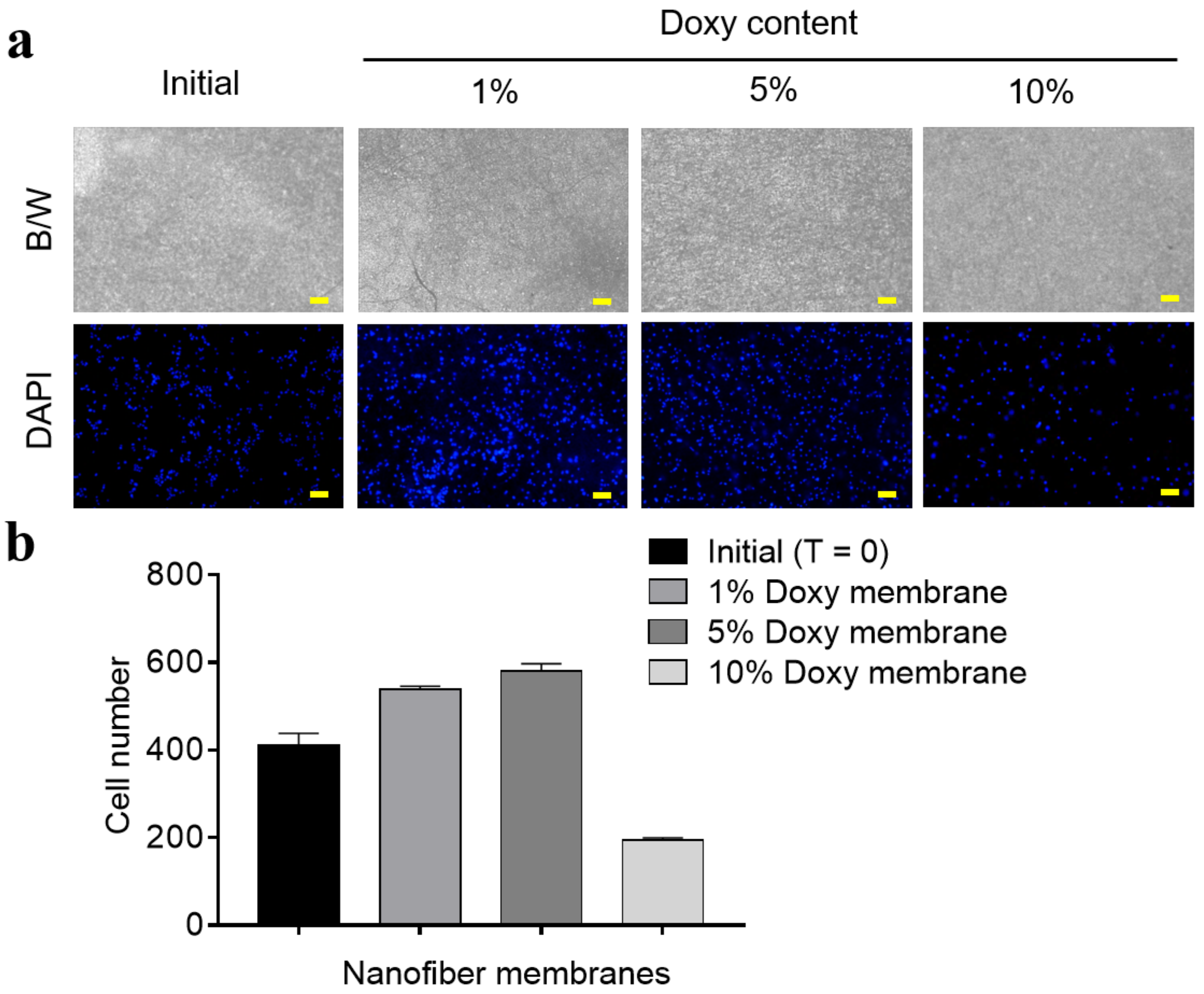
2.8. Growth of Fibrosarcoma Cells on the Nanofiber Membrane
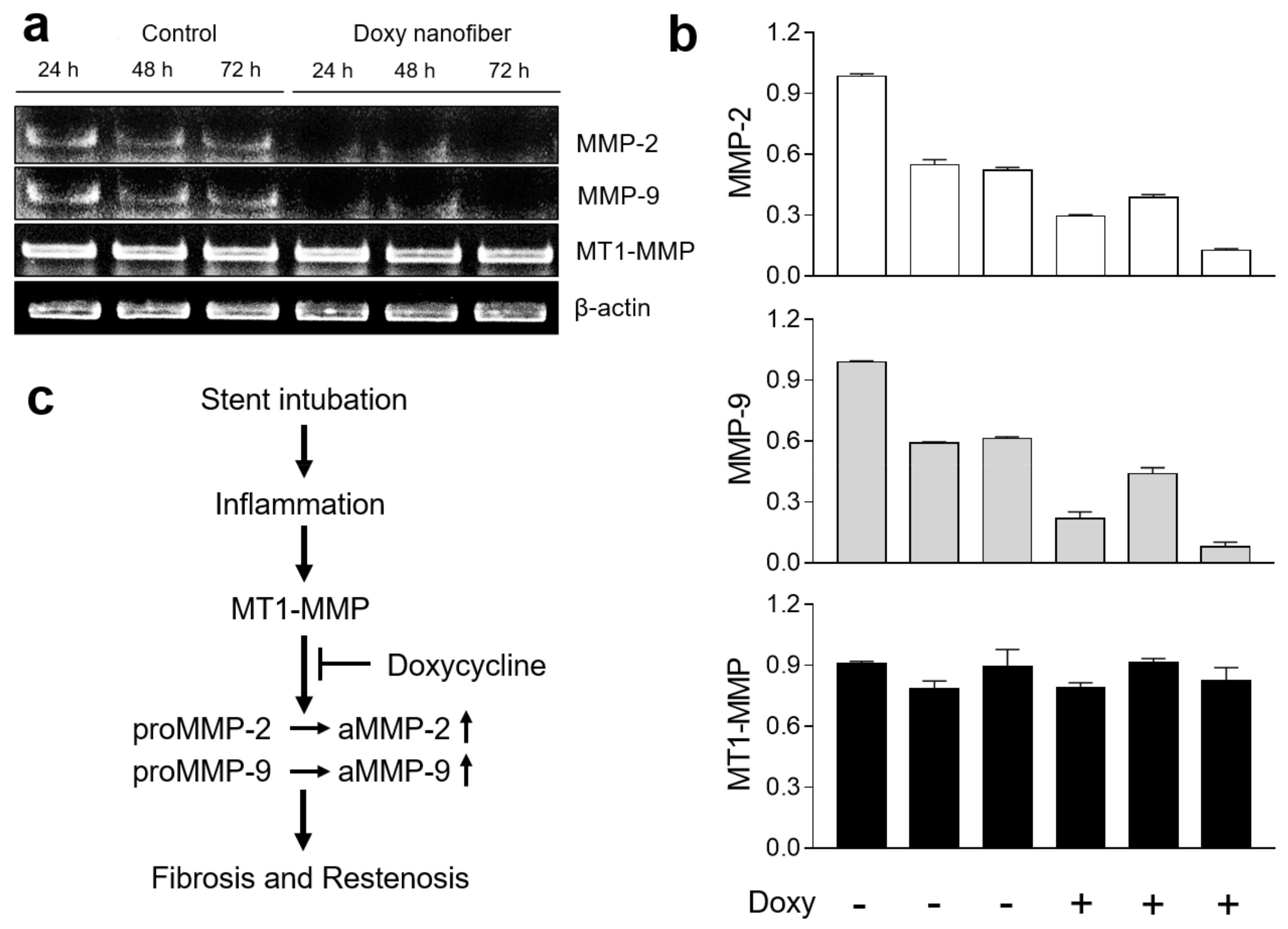
2.9. Quantitative Real Time Polymerase Chain Reaction (PCR) Estimation
2.10. Statistical Analysis
3. Results and Discussion
4. Conclusion
Supplementary Materials
Author Contributions
Funding
Acknowledgements
Conflicts of Interest
References
- Spittle, N.; McCluskey, A. Tracheal stenosis after intubation. BMJ 2000, 321, 1000–1002. [Google Scholar] [CrossRef] [PubMed]
- Wassermann, K.; Mathen, F.; Edmund Eckel, H. Malignant laryngotracheal obstruction: A way to treat serial stenoses of the upper airways. Ann. Thorac. Surg. 2000, 70, 1197–1201. [Google Scholar] [CrossRef]
- Mudambi, L.; Miller, R.; Eapen, G.A. Malignant central airway obstruction. J.Thorac. Dis. 2017, 9, S1087–S1110. [Google Scholar] [CrossRef] [Green Version]
- Sakles, J.C.; Laurin, E.G.; Rantapaa, A.A.; Panacek, E.A. Airway management in the emergency department: A one-year study of 610 tracheal intubations. Ann. Emerg. Med 1998, 31, 325–332. [Google Scholar] [CrossRef]
- Overbeck, M.C. Airway Management of Respiratory Failure. Emerg. Med. Clin. N. Am. 2016, 34, 97–127. [Google Scholar] [CrossRef] [PubMed]
- Wijdicks, E.F.; Sheth, K.N.; Carter, B.S.; Greer, D.M.; Kasner, S.E.; Kimberly, W.T.; Schwab, S.; Smith, E.E.; Tamargo, R.J.; Wintermark, M. Recommendations for the management of cerebral and cerebellar infarction with swelling: A statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2014, 45, 1222–1238. [Google Scholar] [CrossRef] [PubMed]
- Perini, S.; Gordon, R.L.; Golden, J.A.; LaBerge, J.M.; Wilson, M.W.; Kerlan, R.K., Jr. Deformation and migration of Palmaz stents after placement in the tracheobronchial tree. JVIR 1999, 10, 209–215. [Google Scholar] [CrossRef]
- Rowe, S.M.; Miller, S.; Sorscher, E.J. Cystic fibrosis. The N. Engl. J. Med 2005, 352, 1992–2001. [Google Scholar] [CrossRef]
- Terrier, B.; Dechartres, A.; Girard, C.; Jouneau, S.; Kahn, J.E.; Dhote, R.; Lazaro, E.; Cabane, J.; Papo, T.; Schleinitz, N.; et al. Granulomatosis with polyangiitis: Endoscopic management of tracheobronchial stenosis: Results from a multicentre experience. Rheumatology 2015, 54, 1852–1857. [Google Scholar] [CrossRef]
- Girard, C.; Charles, P.; Terrier, B.; Bussonne, G.; Cohen, P.; Pagnoux, C.; Cottin, V.; Cordier, J.F.; Guillevin, L. Tracheobronchial Stenoses in Granulomatosis With Polyangiitis (Wegener’s): A Report on 26 Cases. Medicine 2015, 94, e1088. [Google Scholar] [CrossRef]
- Wain, J.C., Jr. Postintubation tracheal stenosis. Semin. Thorac. Cardiovasc. Surg. 2009, 21, 284–289. [Google Scholar] [CrossRef]
- Corbel, M.; Theret, N.; Caulet-Maugendre, S.; Germain, N.; Lagente, V.; Clement, B.; Boichot, E. Repeated endotoxin exposure induces interstitial fibrosis associated with enhanced gelatinase (MMP-2 and MMP-9) activity. Inflamm. Res. 2001, 50, 129–135. [Google Scholar] [CrossRef]
- Franco, C.; Ho, B.; Mulholland, D.; Hou, G.; Islam, M.; Donaldson, K.; Bendeck, M.P. Doxycycline alters vascular smooth muscle cell adhesion, migration, and reorganization of fibrillar collagen matrices. Ame. J. Pathol. 2006, 168, 1697–1709. [Google Scholar] [CrossRef]
- Haas, T.L.; Davis, S.J.; Madri, J.A. Three-dimensional type I collagen lattices induce coordinate expression of matrix metalloproteinases MT1-MMP and MMP-2 in microvascular endothelial cells. J. Biol. Chem. 1998, 273, 3604–3610. [Google Scholar] [CrossRef]
- Fingleton, B. MMPs as therapeutic targets--still a viable option? Semin. Cell Dev. Biol. 2008, 19, 61–68. [Google Scholar] [CrossRef]
- Pavlaki, M.; Zucker, S. Matrix metalloproteinase inhibitors (MMPIs): The beginning of phase I or the termination of phase III clinical trials. Cancer Metastasis Rev. 2003, 22, 177–203. [Google Scholar] [CrossRef]
- Choi, J.S.; Kim, J.M.; Kim, J.W.; Kim, Y.M.; Park, I.S.; Yang, S.G. Prevention of tracheal inflammation and fibrosis using nitinol stent coated with doxycycline. Laryngoscope 2018, 128, 1558–1563. [Google Scholar] [CrossRef]
- Dursun, D.; Kim, M.C.; Solomon, A.; Pflugfelder, S.C. Treatment of recalcitrant recurrent corneal erosions with inhibitors of matrix metalloproteinase-9, doxycycline and corticosteroids. Ame. J. Ophthalmol. 2001, 132, 8–13. [Google Scholar] [CrossRef]
- Benjamin, M.M.; Khalil, R.A. Matrix metalloproteinase inhibitors as investigative tools in the pathogenesis and management of vascular disease. Exp. Suppl. 2012, 103, 209–279. [Google Scholar] [CrossRef]
- Bhardwaj, N.; Kundu, S.C. Electrospinning: A fascinating fiber fabrication technique. Biotechnol Adv. 2010, 28, 325–347. [Google Scholar] [CrossRef]
- Kim, G.; Kim, W. Highly porous 3D nanofiber scaffold using an electrospinning technique. J. Biomed. Mater. Res. B Appl. Biomater. 2007, 81, 104–110. [Google Scholar] [CrossRef] [PubMed]
- Zilberman, M.; Eberhart, R.C. Drug-eluting bioresorbable stents for various applications. Ann. Rev. Biomed. Eng. 2006, 8, 153–180. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.Y.; Kim, M.; Kim, M.K.; Lee, H.; Lee, D.K.; Lee, D.H.; Yang, S.G. Paclitaxel-eluting nanofiber-covered self-expanding nonvascular stent for palliative chemotherapy of gastrointestinal cancer and its related stenosis. Biomed. Microdevices 2014, 16, 897–904. [Google Scholar] [CrossRef]
- Alameddine, H.S.; Morgan, J.E. Matrix Metalloproteinases and Tissue Inhibitor of Metalloproteinases in Inflammation and Fibrosis of Skeletal Muscles. J. Neuromuscul Dis 2016, 3, 455–473. [Google Scholar] [CrossRef] [Green Version]
- Kim, M.K.; Moon, Y.A.; Song, C.K.; Baskaran, R.; Bae, S.; Yang, S.G. Tumor-suppressing miR-141 gene complex-loaded tissue-adhesive glue for the locoregional treatment of hepatocellular carcinoma. Theranostics 2018, 8, 3891–3901. [Google Scholar] [CrossRef]
- Bibas, B.J.; Terra, R.M.; Oliveira Junior, A.L.; Tamagno, M.F.; Minamoto, H.; Cardoso, P.F.; Pego-Fernandes, P.M. Predictors for postoperative complications after tracheal resection. Ann. Thorac. Surg. 2014, 98, 277–282. [Google Scholar] [CrossRef]
- Wright, C.D.; Grillo, H.C.; Wain, J.C.; Wong, D.R.; Donahue, D.M.; Gaissert, H.A.; Mathisen, D.J. Anastomotic complications after tracheal resection: Prognostic factors and management. J. Thorac. Cardiovasc. Surg. 2004, 128, 731–739. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rizas, K.D.; Mehilli, J. Stent Polymers: Do They Make a Difference? Circ. Cardiovasc. Interv. 2016, 9. [Google Scholar] [CrossRef]
- Simmons, A.; Hyvarinen, J.; Odell, R.A.; Martin, D.J.; Gunatillake, P.A.; Noble, K.R.; Poole-Warren, L.A. Long-term in vivo biostability of poly(dimethylsiloxane)/poly(hexamethylene oxide) mixed macrodiol-based polyurethane elastomers. Biomaterials 2004, 25, 4887–4900. [Google Scholar] [CrossRef]
- Heunis, T.; Bshena, O.; Klumperman, B.; Dicks, L. Release of bacteriocins from nanofibers prepared with combinations of poly(d,l-lactide) (PDLLA) and poly(ethylene oxide) (PEO). Int. J. Mol. Sci. 2011, 12, 2158–2173. [Google Scholar] [CrossRef] [PubMed]
- Burke, J.; Donno, R.; d’Arcy, R.; Cartmell, S.; Tirelli, N. The Effect of Branching (Star Architecture) on Poly(d,l-lactide) (PDLLA) Degradation and Drug Delivery. Biomacromolecules 2017, 18, 728–739. [Google Scholar] [CrossRef] [PubMed]
- ten Hallers, E.J.; Rakhorst, G.; Marres, H.A.; Jansen, J.A.; van Kooten, T.G.; Schutte, H.K.; van Loon, J.P.; van der Houwen, E.B.; Verkerke, G.J. Animal models for tracheal research. Biomaterials 2004, 25, 1533–1543. [Google Scholar] [CrossRef]
- Zhao, H.Q.; Jayasinghe, D.; Hossainy, S.; Schwartz, L.B. A theoretical model to characterize the drug release behavior of drug-eluting stents with durable polymer matrix coating. J. Biomed. Mater. Res. A 2012, 100, 120–124. [Google Scholar] [CrossRef] [PubMed]
- Unnithan, A.R.; Barakat, N.A.; Pichiah, P.B.; Gnanasekaran, G.; Nirmala, R.; Cha, Y.S.; Jung, C.H.; El-Newehy, M.; Kim, H.Y. Wound-dressing materials with antibacterial activity from electrospun polyurethane-dextran nanofiber mats containing ciprofloxacin HCl. Carbohydr. Polym. 2012, 90, 1786–1793. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type | PU Core 1) | PDLLA Shell 2) | Nanofiber Thickness (μm, mean ± S.D.) | Doxycycline | |||
|---|---|---|---|---|---|---|---|
| Flow Rate (mL/h) | Polymer Weight (mg) 3) | Flow Rate (mL/h) | Polymer Weight (mg) 3) | Applied Amount for Spinning (mg) | L.E. (%, mean ± S.D., n = 3) 4) | ||
| Single (1:0) | 0.3 | 30 | - | - | 0.39 ± 0.07 | 3 | 89.9 ± 5.3 |
| Core-shell (1:1) | 0.3 | 30 | 0.9 | 30 | 0.71 ± 0.09 | 6 | 97.1 ± 6.2 |
| Core-shell (1:2) | 0.3 | 30 | 1.8 | 60 | 1.71 ± 0.27 | 9 | 103.8 ± 1.0 |
| Core-shell (1:4) | 0.3 | 30 | 3.6 | 120 | 2.65 ± 0.93 | 15 | 105.0 ± 4.9 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baskaran, R.; Ko, U.-J.; Davaa, E.; Park, J.E.; Jiang, Y.; Lee, J.; Yang, S.-G. Doxycycline-Eluting Core-Shell Type Nanofiber-Covered Trachea Stent for Inhibition of Cellular Metalloproteinase and Its Related Fibrotic Stenosis. Pharmaceutics 2019, 11, 421. https://doi.org/10.3390/pharmaceutics11080421
Baskaran R, Ko U-J, Davaa E, Park JE, Jiang Y, Lee J, Yang S-G. Doxycycline-Eluting Core-Shell Type Nanofiber-Covered Trachea Stent for Inhibition of Cellular Metalloproteinase and Its Related Fibrotic Stenosis. Pharmaceutics. 2019; 11(8):421. https://doi.org/10.3390/pharmaceutics11080421
Chicago/Turabian StyleBaskaran, Rengarajan, Un-Jeong Ko, Enkhzaya Davaa, Ji Eun Park, Yixin Jiang, Junghan Lee, and Su-Geun Yang. 2019. "Doxycycline-Eluting Core-Shell Type Nanofiber-Covered Trachea Stent for Inhibition of Cellular Metalloproteinase and Its Related Fibrotic Stenosis" Pharmaceutics 11, no. 8: 421. https://doi.org/10.3390/pharmaceutics11080421