
A Retrospective Study of the Seroprevalence of Dengue Virus and Chikungunya Virus Exposures in Nigeria, 2010–2018

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Results
2.1. Dengue Virus Exposure
2.2. Chikungunya Virus Exposure
2.3. Prior Dengue Virus L and Chikungunya Virus Exposures
3. Discussion
4. Materials and Methods
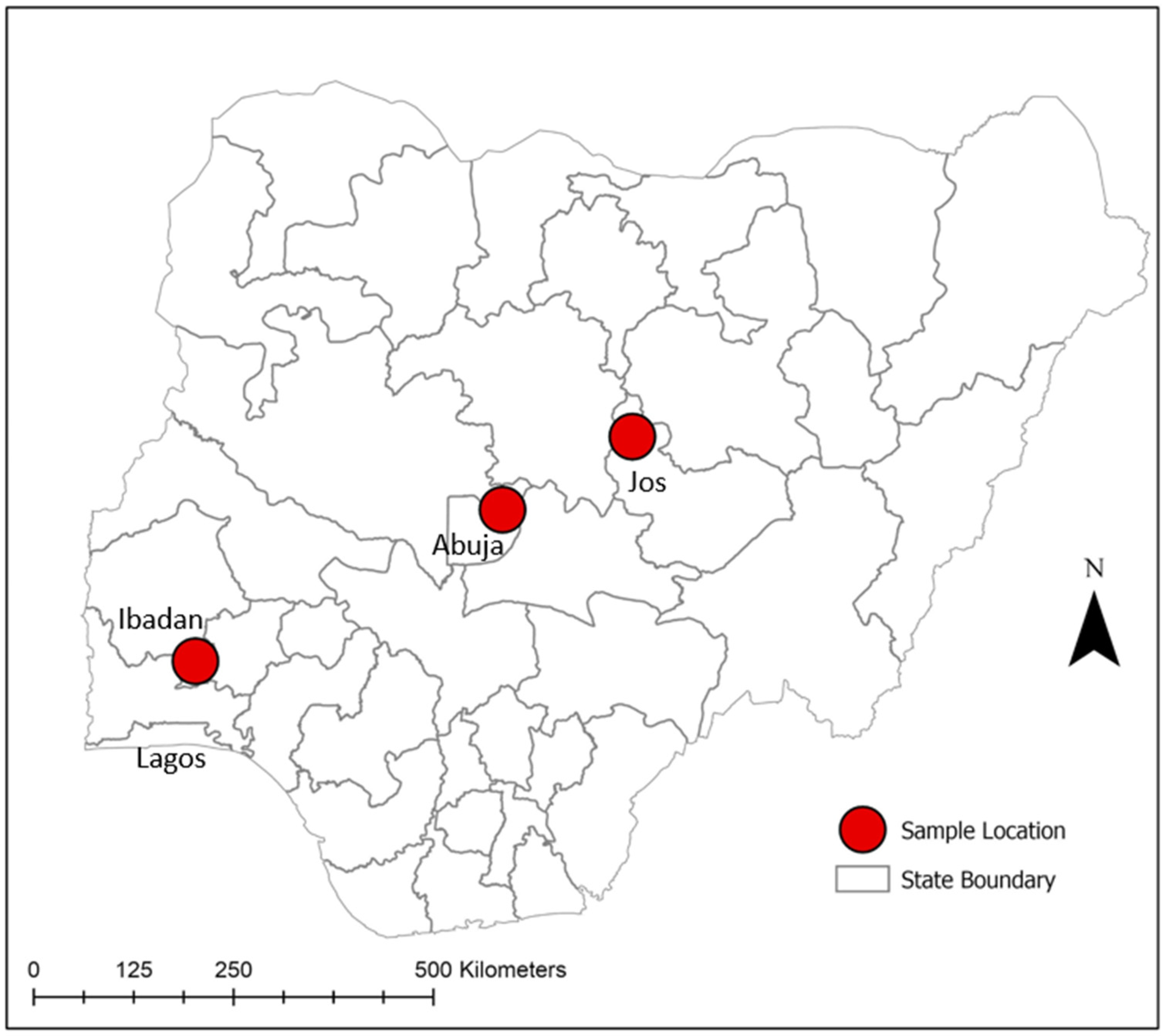
4.1. Study Area and Sample Population
4.2. Serological Analysis
4.3. Malaria Microscopy
4.4. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yousseu, F.B.S.; Nemg, F.B.S.; Ngouanet, S.A.; Mekanda, F.M.O.; Demanou, M. Detection and serotyping of dengue viruses in febrile patients consulting at the New-Bell District Hospital in Douala, Cameroon. PLoS ONE 2018, 13, e0204143. [Google Scholar] [CrossRef] [PubMed]
- Chevillon, C.; Briant, L.; Renaud, F.; Devaux, C. The Chikungunya threat: An ecological and evolutionary perspective. Trends Microbiol. 2008, 16, 80–88. [Google Scholar] [CrossRef] [PubMed]
- Munnoz, J.; Eritja, R.; Alcaide, M.; Montalvo, T.; Soriguer, R.C.; Figuerola, J. Host-feeding patterns of native Culex pipiens and invasive Aedes albopictus mosquitoes (Diptera: Culicidae) in urban zones from Barcelona, Spain. J. Med. Entomol. 2011, 48, 956–960. [Google Scholar] [CrossRef]
- Vu, D.M.; Banda, T.; Teng, C.Y.; Heimbaugh, C.; Muchiri, E.M.; Mungai, P.L.; Mutuku, F.M.; Brichard, J.; Gildengorin, G.; Borland, E.M.; et al. Dengue and West Nile Virus Transmission in Children and Adults in Coastal Kenya. Am. J. Trop. Med. Hyg. 2017, 96, 141–143. [Google Scholar] [CrossRef]
- Vu, D.M.; Jungkind, D.; LaBeaud, A.D. Chikungunya Virus. Clin. Lab. Med. 2017, 37, 371–382. [Google Scholar] [CrossRef] [PubMed]
- Fagbami, A.H.; Onoja, A.B. Dengue haemorrhagic fever: An emerging disease in Nigeria, West Africa. J. Infect. Public Health 2018, 11, 757–762. [Google Scholar] [CrossRef] [PubMed]
- Zappa, A.; Amendola, A.; Romano, L.; Zanetti, A. Emerging and re-emerging viruses in the era of globalisation. Blood Transfus. 2009, 7, 167–171. [Google Scholar] [CrossRef]
- Burt, F.J.; Rolph, M.S.; Rulli, N.E.; Mahalingam, S.; Heise, M.T. Chikungunya: A re-emerging virus. Lancet 2012, 379, 662–671. [Google Scholar] [CrossRef]
- Devaux, C.A. Emerging and re-emerging viruses: A global challenge illustrated by Chikungunya virus outbreaks. World J. Virol. 2012, 1, 11–22. [Google Scholar] [CrossRef]
- Levinson, R.S.; Strauss, J.H.; Strauss, E.G. Complete sequence of the genomic RNA of O’nyong-nyong virus and its use in the construction of alphavirus phylogenetic trees. Virology 1990, 175, 110–123. [Google Scholar] [CrossRef]
- Wilder-Smith, A.; Chen, L.H.; Massad, E.; Wilson, M.E. Threat of dengue to blood safety in dengue-endemic countries. Emerg. Infect. Dis. 2009, 15, 8–11. [Google Scholar] [CrossRef] [PubMed]
- Weaver, S.C.; Barrett, A.D. Transmission cycles, host range, evolution and emergence of arboviral disease. Nat. Rev. Microbiol. 2004, 2, 789–801. [Google Scholar] [CrossRef] [PubMed]
- Powers, A.M.; Logue, C.H. Changing patterns of chikungunya virus: Re-emergence of a zoonotic arbovirus. J. Gen. Virol. 2007, 88, 2363–2377. [Google Scholar] [CrossRef] [PubMed]
- Bello, O.; Aminu, M.U.; Jatau, E.D. Seroprevalence of IgM Antibodies to Dengue Fever Virus among Patients Presenting with Symptoms of Fever in Some Hospitals in Kaduna State, Nigeria. Int. J. Sci. Res. 2016, 5, 1255–1259. [Google Scholar] [CrossRef]
- Kolawole, O.M.; Bello, K.E.; Seriki, A.A.; Irekeola, A.A. Serological survey of Chikungunya virus in Ilorin Metropolis, Nigeria. Braz. J. Infect. Dis. 2017, 21, 365–366. [Google Scholar] [CrossRef]
- Baba, M.; Logue, C.H.; Oderinde, B.; Abdulmaleek, H.; Williams, J.; Lewis, J.; Laws, T.R.; Hewson, R.; Marcello, A.; D’Agaro, P. Evidence of arbovirus co-infection in suspected febrile malaria and typhoid patients in Nigeria. J. Infect. Dev. Ctries. 2013, 7, 51–59. [Google Scholar] [CrossRef]
- Ayorinde, A.F.; Oyeyiga, A.M.; Nosegbe, N.O.; Folarin, O.A. A survey of malaria and some arboviral infections among suspected febrile patients visiting a health centre in Simawa, Ogun State, Nigeria. J. Infect. Public Health 2016, 9, 52–59. [Google Scholar] [CrossRef] [Green Version]
- Ochieng, C.; Ahenda, P.; Vittor, A.Y.; Nyoka, R.; Gikunju, S.; Wachira, C.; Waiboci, L.; Umuro, M.; Kim, A.A.; Nderitu, L.; et al. Seroprevalence of Infections with Dengue, Rift Valley Fever and Chikungunya Viruses in Kenya, 2007. PLoS ONE 2015, 10, e0132645. [Google Scholar] [CrossRef] [Green Version]
- Grossi-Soyster, E.N.; Cook, E.A.J.; de Glanville, W.A.; Thomas, L.F.; Krystosik, A.R.; Lee, J.; Wamae, C.N.; Kariuki, S.; Fevre, E.M.; LaBeaud, A.D. Serological and spatial analysis of alphavirus and flavivirus prevalence and risk factors in a rural community in western Kenya. PLoS Negl. Trop. Dis. 2017, 11, e0005998. [Google Scholar] [CrossRef] [Green Version]
- Labeaud, A.D.; Bashir, F.; King, C.H. Measuring the burden of arboviral diseases: The spectrum of morbidity and mortality from four prevalent infections. Popul. Health Metr. 2011, 9, 1. [Google Scholar] [CrossRef] [Green Version]
- Baba, M.; Sarom, M.F.; Vorndam, A.V.; Adeniji, J.A.; Diop, O.; Olaleye, D. Dengue Virus Infections in Patients Suspected of Malaria/Typhoid in Nigeria. J. Am. Sci. 2009, 5, 129–134. [Google Scholar]
- Kolawole, O.; Seriki, A.A.; Irekeola, A.A.; Ogah, J. The Neglect and Fast Spread of Some Arboviruses: A Note for Healthcare Providers in Nigeria. Diseases 2018, 6, 99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fagbami, A.H.; Monath, T.P.; Fabiyi, A. Dengue virus infections in Nigeria: A survey for antibodies in monkeys and humans. Trans. R. Soc. Trop. Med. Hyg. 1977, 71, 60–65. [Google Scholar] [CrossRef]
- Oyero, O.G.; Ayukekbong, J.A. High dengue NS1 antigenemia in febrile patients in Ibadan, Nigeria. Virus Res. 2014, 191, 59–61. [Google Scholar] [CrossRef] [PubMed]
- Souza, N.; Félix, A.C.; de Paula, A.V.; Levi, J.E.; Pannuti, C.S.; Romano, C.M. Evaluation of serological cross-reactivity between yellow fever and other flaviviruses. Int. J. Infect. Dis. IJID Off. Publ. Int. Soc. Infect. Dis. 2019, 81, 4–5. [Google Scholar] [CrossRef] [Green Version]
- Kingsley, U.B.; Tabitha, V.S.; Lohya, N.; Joseph, A.O.A. Dengue Virus Antibodies in Patients Presenting with Pyrexia attending Jos University Teaching Hospital, Jos, Nigeria. Saudi J. Pathol. Microbiol. 2018, 3, 47–55. [Google Scholar] [CrossRef]
- Hamisu, T.M.; Yuguda, A.D.E.; Abubakar, M.B.; Shettima, Y.M.; Maina, M.M.; Zanna, M.Y.; Baba, S.S.; Andrew, A.; Terhemen, I.C. Prevalence of Dengue Virus Infection Among Febrile Outpatients Attending University of Maiduguri Teaching Hospital in Borno State, Nigeria. IOSR J. Dent. Med. Sci. 2017, 16, 155–159. [Google Scholar] [CrossRef]
- Chukwuma, G.O.; Audu, J.S.; Chukwuma, O.M.; Manafa, P.O.; Ebugosi, R.S.; Akulue, J.C.; Aneke, J.C.; Ahaneku, G.I.; Nchinda, G.W.; Esimone, C.O. Seroprevalence of dengue virus among children with febrile illness in Nnewi, Nigeria. J. Med. Res. 2018, 4, 24–30. [Google Scholar] [CrossRef]
- Muhibi, M.A.; Adeleke, M.A.; Shittu, B.T.; Jeremiah, Z.A. Dengue Virus Infection among Voluntary Blood Donors in Osogbo, Southwestern Nigeria. Am. J. Biomed. Sci. 2017, 9, 113–118. [Google Scholar] [CrossRef]
- Otu, A.A.; Udoh, U.A.; Ita, O.I.; Hicks, J.P.; Egbe, W.O.; Walley, J. A cross-sectional survey on the seroprevalence of dengue fever in febrile patients attending health facilities in Cross River State, Nigeria. PLoS ONE 2019, 14, e0215143. [Google Scholar] [CrossRef]
- Salam, N.; Mustafa, S.; Hafiz, A.; Chaudhary, A.A.; Deeba, F.; Parveen, S. Global prevalence and distribution of coinfection of malaria, dengue and chikungunya: A systematic review. BMC Public Health 2018, 18, 710. [Google Scholar] [CrossRef] [PubMed]
- Basurko, C.; Matheus, S.; Hilderal, H.; Everhard, S.; Restrepo, M.; Cuadro-Alvarez, E.; Lambert, V.; Boukhari, R.; Duvernois, J.P.; Favre, A.; et al. Estimating the Risk of Vertical Transmission of Dengue: A Prospective Study. Am. J. Trop. Med. Hyg. 2018, 98, 1826–1832. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Argolo, A.F.; Feres, V.C.; Silveira, L.A.; Oliveira, A.C.; Pereira, L.A.; Junior, J.B.; Braga, C.; Martelli, C.M. Prevalence and incidence of dengue virus and antibody placental transfer during late pregnancy in central Brazil. BMC Infect. Dis. 2013, 13, 254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ribeiro, C.F.; Lopes, V.G.; Brasil, P.; Coelho, J.; Muniz, A.G.; Nogueira, R.M. Perinatal transmission of dengue: A report of 7 cases. J. Pediatr. 2013, 163, 1514–1516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laoprasopwattana, K.; Suntharasaj, T.; Petmanee, P.; Suddeaugrai, O.; Geater, A. Chikungunya and dengue virus infections during pregnancy: Seroprevalence, seroincidence and maternal-fetal transmission, southern Thailand, 2009–2010. Epidemiol. Infect. 2016, 144, 381–388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cardona-Correa, S.E.; Castano-Jaramillo, L.M.; Quevedo-Velez, A. Vertical transmission of chikungunya virus infection. Case Report. Rev. Chil. Pediatr. 2017, 88, 285–288. [Google Scholar] [CrossRef] [Green Version]
- Ramful, D.; Carbonnier, M.; Pasquet, M.; Bouhmani, B.; Ghazouani, J.; Noormahomed, T.; Beullier, G.; Attali, T.; Samperiz, S.; Fourmaintraux, A.; et al. Mother-to-child transmission of Chikungunya virus infection. Pediatr. Infect. Dis. J. 2007, 26, 811–815. [Google Scholar] [CrossRef]
- Oliveira, R.; Barreto, F.K.A.; Maia, A.; Gomes, I.P.; Simiao, A.R.; Barbosa, R.B.; Rodrigues, A.S.R.; Lopes, K.W.; Araujo, F.M.C.; do Vale, R.L.S.; et al. Maternal and infant death after probable vertical transmission of chikungunya virus in Brazil—case report. BMC Infect. Dis. 2018, 18, 333. [Google Scholar] [CrossRef] [Green Version]
- Contopoulos-Ioannidis, D.; Newman-Lindsay, S.; Chow, C.; LaBeaud, A.D. Mother-to-child transmission of Chikungunya virus: A systematic review and meta-analysis. PLoS Negl. Trop. Dis. 2018, 12, e0006510. [Google Scholar] [CrossRef] [Green Version]
- Boumahni, B.; Bintner, M. Five-year outcome of mother-to-child transmission of chikungunya virus. Med. Trop. (Mars) 2012, 72, 94–96. [Google Scholar]
- Perret, C.; Chanthavanich, P.; Pengsaa, K.; Limkittikul, K.; Hutajaroen, P.; Bunn, J.E.G.; Brabin, B.J. Dengue infection during pregnancy and transplacental antibody transfer in Thai mothers. J. Infect. 2005, 51, 287–293. [Google Scholar] [CrossRef]
- Watanaveeradej, V.; Endy, T.P.; Simasathien, S.; Kerdpanich, A.; Polprasert, N.; Aree, C.; Vaughn, D.W.; Nisalak, A. Transplacental chikungunya virus antibody kinetics, Thailand. Emerg. Infect. Dis. 2006, 12, 1770–1772. [Google Scholar] [CrossRef] [PubMed]
- Foeller, M.E.; Nosrat, C.; Krystosik, A.; Noel, T.; Gerardin, P.; Cudjoe, N.; Mapp-Alexander, V.; Mitchell, G.; Macpherson, C.; Waechter, R.; et al. Chikungunya infection in pregnancy—reassuring maternal and perinatal outcomes: A retrospective observational study. Bjog-Int. J. Obs. Gy. 2021, 128, 1077–1086. [Google Scholar] [CrossRef] [PubMed]
- Macneil, A.; Reed, Z.; Rollin, P.E. Serologic cross-reactivity of human IgM and IgG antibodies to five species of Ebola virus. PLoS Negl. Trop. Dis. 2011, 5, e1175. [Google Scholar] [CrossRef] [PubMed]
- Aworh, M.K.; Okolocha, E.; Kwaga, J.; Fasina, F.; Lazarus, D.; Suleman, I.; Poggensee, G.; Nguku, P.; Nsubuga, P. Human brucellosis: Seroprevalence and associated exposure factors among abattoir workers in Abuja, Nigeria—2011. Pan Afr. Med. J. 2013, 16, 103. [Google Scholar] [CrossRef] [PubMed]
- LaBeaud, A.D.; Banda, T.; Brichard, J.; Muchiri, E.M.; Mungai, P.L.; Mutuku, F.M.; Borland, E.; Gildengorin, G.; Pfeil, S.; Teng, C.Y.; et al. High rates of o’nyong nyong and Chikungunya virus transmission in coastal Kenya. PLoS Negl. Trop. Dis. 2015, 9, e0003436. [Google Scholar] [CrossRef]
- Trape, J.F.; Peelman, P.; Morault-Peelman, B. Criteria for diagnosing clinical malaria among a semi-immune population exposed to intense and perennial transmission. Trans. R. Soc. Trop. Med. Hyg. 1985, 79, 435–442. [Google Scholar] [CrossRef]


{kind=link}
| Variable | n/N | Seroprevalence % (95% CI) | Unadjusted Odds Ratio (95% CI) | p-Value | Adjusted Odds Ratio (95% CI) | p-Value |
|---|---|---|---|---|---|---|
| Age (continuous) | 379/701 | 54.1 (50.2, 57.8) | 1.00 (0.99, 1.01) | 0.251 | 1.00 (0.99, 1.01) | 0.757 |
| 0–17 | 78/126 | 61.9 (52.8, 70.4) | REF | |||
| 18–90 | 301/575 | 52.3 (48.1, 56.4) | 0.67 (0.45, 1.00) | 0.052 | 1.10 (0.71, 1.71) | 0.648 |
| Gender | ||||||
| Female | 193/329 | 58.6 (53.1, 64.0) | 1.41 (1.05, 1.91) | 0.022 | 0.98 (0.67, 1.44) | 0.933 |
| Male | 186/372 | 50.0 (44.8, 55.1) | REF | |||
| Location, Year | ||||||
| Ibadan, 2018 | 187/300 | 62.3 (56.5, 67.8) | 3.49 (2.38, 5.12) | <0.001 | 4.26 (0.78, 23.04) | 0.092 |
| Jos, 2017 | 120/177 | 67.7 (60.3, 74.6) | 4.44 (2.85, 6.93) | |||
| Abuja, 2011 | 72/224 | 32.1 (26.0, 38.6) | REF | |||
| Occupation | ||||||
| Butcher/Meat seller | 45/141 | 31.9 (24.3, 40.2) | 0.30 (0.19, 0.46) | <0.001 | 2.44 (0.48, 12.61) | 0.284 |
| Livestock Trader/Vet | 9/27 | 33.3 (16.5, 53.9) | 0.32 (0.12, 0.78) | 2.70 (0.45, 16.16) | 0.276 | |
| Abattoir worker | 16/46 | 34.7 (21.3, 50.2) | 0.34 (0.16, 0.68) | 3.59 (0.63, 20.30) | 0.147 | |
| Unknown | 120/177 | 67.7 (60.3, 74.6) | 1.34 (0.89, 2.03) | 6.51 (1.25, 33.74) | 0.026 | |
| Others | 189/310 | 60.9 (55.2, 66.4) | REF | |||
| Animal exposure | ||||||
| Unknown | 120/177 | 67.7 (60.3, 74.6) | 1.04 (0.62, 1.72) | <0.001 | ||
| Yes | 168/388 | 43.2 (38.3, 48.3) | 0.37 (0.24, 0.57) | 0.43 (0.25, 0.73) | 0.002 | |
| No | 91/136 | 66.9 (58.3, 74.7) | REF | |||
| Health status | ||||||
| Sick individual | 307/477 | 64.3 (59.8, 68.6) | 3.81 (2.68, 5.42) | <0.001 | ||
| Non-sick individual | 72/224 | 32.1 (26.0, 38.6) | REF | |||
| Presence of fever | ||||||
| Yes | 339/595 | 56.9 (52.8, 60.9) | 2.18 (1.42, 3.34) | <0.001 | 0.60 (0.33, 1.10) | 0.100 |
| No | 40/106 | 37.7 (28.5, 47.6) | REF | |||
| Malaria parasite | ||||||
| Unknown | 192/401 | 47.8 (42.8, 52.8) | 0.78 (0.44, 1.38) | <0.001 | ||
| Yes | 153/237 | 64.5 (58.1, 70.6) | 1.55 (0.84, 2.82) | 2.43 (1.27, 4.66) | 0.007 | |
| No | 34/63 | 53.9 (40.9, 66.6) | REF |
| Variable | n/N | Seroprevalence % (95% CI) | Unadjusted Odds Ratio (95% CI) | p-Value | Adjusted Odds Ratio (95% CI) | p-Value |
|---|---|---|---|---|---|---|
| Age (continuous) | 290/701 | 41.3 (37.6, 45.1) | 1.01 (1.00, 1.02) | <0.001 | 1.01 (1.01, 1.02) | <0.001 |
| 0–17 | 29/126 | 23.0 (15.9, 31.3) | REF | |||
| 18–90 | 261/575 | 45.3 (41.2, 49.5) | 2.78 (1.77, 4.34) | <0.001 | 2.15 (1.33, 3.45) | 0.002 |
| Gender | ||||||
| Female | 132/329 | 40.1 (34.7, 45.6) | 0.90 (0.67, 1.22) | 0.528 | ||
| Male | 158/372 | 42.4 (37.3, 47.6) | REF | |||
| Location, Year | ||||||
| Ibadan, 2018 | 103/300 | 34.3 (28.9, 40.0) | 0.44 (0.31, 0.63) | <0.001 | 0.67 (0.16, 2.72) | 0.577 |
| Jos, 2017 | 66/177 | 37.2 (30.1, 44.8) | 0.50 (0.33, 0.75) | |||
| Abuja, 2011 | 121/224 | 54.0 (47.2, 60.6) | REF | |||
| Occupation | ||||||
| Butcher/Meat seller | 70/141 | 49.6 (41.1, 58.1) | 1.81 (1.21, 2.72) | <0.001 | 0.63 (0.16, 2.39) | 0.500 |
| Livestock Trader/Vet | 13/27 | 48.1 (28.6, 68.0) | 1.71 (0.77, 3.77) | 0.57 (0.12, 2.57) | 0.472 | |
| Abattoir worker | 32/46 | 69.5 (54.2, 82.2) | 4.21 (2.15, 8.23) | 1.66 (0.39, 7.01) | 0.491 | |
| Unknown | 66/177 | 37.2 (30.1, 44.8) | 1.09 (0.74, 1.60) | 0.37 (0.09, 1.47) | 0.162 | |
| Others | 189/310 | 60.9 (55.2, 66.4) | REF | |||
| Animal exposure | ||||||
| Unknown | 66/177 | 37.2 (30.1, 44.8) | 0.96 (0.60, 1.52) | 0.205 | - | - |
| Yes | 172/388 | 44.3 (39.3, 49.4) | 1.28 (0.86, 1.91) | 1.17 (0.69, 1.97) | 0.550 | |
| No | 52/136 | 38.2 (30.0, 46.9) | REF | |||
| Health status | ||||||
| Sick individual | 169/477 | 35.4 (31.1, 39.9) | 0.46 (0.33, 0.65) | < 0.001 | ||
| Non-sick individual | 121/224 | 54.0 (47.2, 60.6) | REF | |||
| Presence of fever | ||||||
| Yes | 237/595 | 39.8 (35.8, 43.8) | 0.66 (0.43, 1.00) | 0.051 | 1.03 (0.59, 1.80) | 0.899 |
| No | 53/106 | 50.0 (40.1, 59.8) | REF | |||
| Malaria parasite | ||||||
| Unknown | 187/401 | 46.6 (41.6, 51.6) | 0.96 (0.56, 1.63) | <0.001 | ||
| Yes | 73/237 | 30.8 (24.9, 37.1) | 0.48 (0.27, 0.86) | 0.43 (0.22, 0.82) | 0.011 | |
| No | 30/63 | 47.6 (34.8, 60.5) | REF |
| Variable | n/N | Seroprevalence % (95% CI) | Unadjusted Odds Ratio (95% CI) | p-Value | Adjusted Odds Ratio (95% CI) | p-Value |
|---|---|---|---|---|---|---|
| Age (continuous) | 141/701 | 20.1 (17.2, 23.2) | 1.01 (1.00, 1.02) | <0.001 | 1.01 (1.01, 1.02) | <0.001 |
| 0–17 | 14/126 | 11.1 (6.21, 17.9) | REF | |||
| 18–90 | 127/575 | 22.0 (18.7, 25.7) | 2.26 (1.25, 4.08) | 0.006 | 2.66 (1.44, 4.91) | 0.002 |
| Gender | ||||||
| Female | 68/329 | 20.6 (16.4, 25.4) | 1.06 (0.73, 1.54) | 0.731 | ||
| Male | 73/372 | 19.6 (15.7, 24.0) | REF | |||
| Location, Year | ||||||
| Ibadan, 2018 | 65/300 | 21.6 (17.1, 26.7) | 1.31 (0.84, 2.03) | 0.464 | ||
| Jos, 2017 | 37/177 | 20.9 (15.1, 27.6) | 1.25 (0.75, 2.06) | |||
| Abuja, 2011 | 39/224 | 17.4 (12.6, 23.0) | REF | |||
| Occupation | ||||||
| Butcher/Meat seller | 21/141 | 14.8 (9.46, 21.8) | 0.64 (0.37, 1.10) | 0.285 | ||
| Livestock Trader/Vet | 4/27 | 14.8 (4.18, 33.7) | 0.64 (0.21, 1.92) | |||
| Abattoir worker | 13/46 | 28.2 (15.9, 43.3) | 1.45 (0.72, 2.92) | |||
| Unknown | 37/177 | 20.9 (15.1, 27.6) | 0.97 (0.62, 1.53) | |||
| Others | 66/310 | 21.2 (16.8, 26.2) | REF | |||
| Animal exposure | ||||||
| Unknown | 37/177 | 20.9 (15.1, 27.6) | 0.76 (0.44, 1.29) | 0.134 | 0.66 (0.38, 1.14) | 0.179 |
| Yes | 69/388 | 17.7 (14.1, 21.9) | 0.62 (0.39, 0.99) | 0.69 (0.41, 1.18) | 0.141 | |
| No | 35/136 | 25.7 (18.6, 33.9) | REF | |||
| Health status | ||||||
| Sick individual | 102/477 | 21.3 (17.7, 25.3) | 1.29 (0.85, 1.94) | 0.222 | 1.46 (0.87, 2.44) | 0.148 |
| Non-sick individual | 39/224 | 17.4 (12.6, 23.0) | REF | |||
| Presence of fever | ||||||
| Yes | 123/595 | 20.6 (17.4, 24.1) | 1.27 (0.73, 2.19) | 0.383 | ||
| No | 18/106 | 16.9 (10.3, 25.5) | REF | |||
| Malaria parasite | ||||||
| Unknown | 76/401 | 18.9 (15.2, 23.1) | 0.74 (0.39, 1.40) | 0.603 | ||
| Yes | 50/237 | 21.0 (16.0, 26.8) | 0.85 (0.44, 1.65) | |||
| No | 15/63 | 23.8 (13.9, 36.2) | REF |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ekong, P.S.; Aworh, M.K.; Grossi-Soyster, E.N.; Wungak, Y.S.; Maurice, N.A.; Altamirano, J.; Ekong, M.J.; Olugasa, B.O.; Nwosuh, C.I.; Shamaki, D.; et al. A Retrospective Study of the Seroprevalence of Dengue Virus and Chikungunya Virus Exposures in Nigeria, 2010–2018. Pathogens 2022, 11, 762. https://doi.org/10.3390/pathogens11070762
Ekong PS, Aworh MK, Grossi-Soyster EN, Wungak YS, Maurice NA, Altamirano J, Ekong MJ, Olugasa BO, Nwosuh CI, Shamaki D, et al. A Retrospective Study of the Seroprevalence of Dengue Virus and Chikungunya Virus Exposures in Nigeria, 2010–2018. Pathogens. 2022; 11(7):762. https://doi.org/10.3390/pathogens11070762
Chicago/Turabian StyleEkong, Pius S., Mabel K. Aworh, Elysse N. Grossi-Soyster, Yiltawe S. Wungak, Nanven A. Maurice, Jonathan Altamirano, Michael J. Ekong, Babasola O. Olugasa, Chika I. Nwosuh, David Shamaki, and et al. 2022. "A Retrospective Study of the Seroprevalence of Dengue Virus and Chikungunya Virus Exposures in Nigeria, 2010–2018" Pathogens 11, no. 7: 762. https://doi.org/10.3390/pathogens11070762