
Minimally Invasive Autopsy Practice in COVID-19 Cases: Biosafety and Findings †

 ,
,  , , , , , , , , , , , , , add
Show full author list
, , , , , , , , , , , , , add
Show full author list
Abstract
:1. Introduction
2. Methods
2.1. Study Setting
2.2. Preparation for the MIA: PPE Donning and Personnel
2.3. Preparation and Performance of the MIA Procedure
2.4. After the MIA: Removal of the PPE, Autopsy Room Cleaning and Follow-Up of the Personnel Involved
2.5. Complete Autopsy Procedure
2.6. SARS-CoV-2 Testing of the Personnel Involved in the MIA and the Complete Autopsy
2.7. Handling of the Specimens, Pathological and Microbiological Methods, and Attribution of Cause of Death
3. Results
3.1. Clinical Characteristics of the Deceased Patients
3.2. Histological and Microbiological Results of the MIA, Complete Autopsy Findings and Cause of Death Attribution
3.3. Follow-Up of the Personnel Involved in the MIA and Complete Autopsy
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Naming the Coronavirus Disease (COVID-19) and the Virus That Causes It. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance/naming-the-coronavirus-disease-(covid-2019)-and-the-virus-that-causes-it (accessed on 20 February 2021).
- Karia, R.; Gupta, I.; Khandait, H.; Yadav, A.; Yadav, A. COVID-19 and its Modes of Transmission. SN Compr. Clin. Med. 2020, 1, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Wang, X.; Jia, X.; Li, J.; Hu, K.; Chen, G.; Wei, J.; Gong, Z.; Zhou, C.; Yu, H.; et al. Risk factors for disease severity, unimprovement, and mortality of COVID-19 patients in Wuhan, China. Clin. Microbiol. Infect. 2020, 26, 767–772. [Google Scholar] [CrossRef] [PubMed]
- Shieh, W.J.; Blau, D.M.; Denison, A.M.; DeLeon-Carnes, M.; Adem, P.; Bhatnagar, J.; Sumner, J.; Liu, L.; Patel, M.; Batten, B.; et al. 2009 Pandemic influenza A (H1N1): Pathology and pathogenesis of 100 fatal cases in the United States. Am. J. Pathol. 2010, 177, 166–175. [Google Scholar] [CrossRef]
- Costache, M.; Lazaroiu, A.M.; Contolenco, A.; Costache, D.; George, S.; Sajin, M.; Patrascu, O.M. Clinical or postmortem? The importance of the autopsy; a retrospective study. Maedica 2014, 9, 261–265. [Google Scholar] [PubMed]
- Salerno, M.; Sessa, F.; Piscopo, A.; Montana, A.; Torrisi, M.; Patanè, F.; Murabito, P.; Li Volti, G.; Pomara, C. No Autopsies on COVID-19 Deaths: A Missed Opportunity and the Lockdown of Science. J. Clin. Med. 2020, 9, 1472. [Google Scholar] [CrossRef] [PubMed]
- Hanley, B.; Lucas, S.B.; Youd, E.; Swift, B.; Osborn, M. Autopsy in suspected COVID-19 cases. J. Clin. Pathol. 2020, 73, 239–242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lacy, J.M.; Brooks, E.G.; Akers, J.; Armstrong, D.; Decker, L.; Gonzalez, A.; Humphrey, W.; Mayer, R.; Miller, M.; Perez, C.; et al. COVID-19: Postmortem diagnostic and biosafety considerations. Am. J. Forensic Med. Pathol. 2020, 41, 143–151. [Google Scholar] [CrossRef] [PubMed]
- González-Arnay, E.; Martín-Olivera, R.; Quintero-Quintero, Y.C.; Hernández-Guerra, A.I. Proposal for a harmonized protocol for COVID-19 screening and necropsy in forensic sciences facilities. J. Forensic Leg. Med. 2020, 76, 102067. [Google Scholar] [CrossRef]
- Keten, D.; Okdemir, E.; Keten, A. Precautions in postmortem examinations in Covid-19—Related deaths: Recommendations from Germany. J. Forensic Leg. Med. 2020, 73, 102000. [Google Scholar] [CrossRef]
- Fusco, F.M.; Scappaticci, L.; Schilling, S.; De Iaco, G.; Brouqui, P.; Maltezou, H.C.; Brodt, H.R.; Bannister, B.; Ippolito, G.; Puro, V. A 2009 cross-sectional survey of procedures for post-mortem management of highly infectious disease patients in 48 isolation facilities in 16 countries: Data from EuroNHID. Infection 2016, 44, 57–64. [Google Scholar] [CrossRef]
- Rakislova, N.; Ismail, M.R.; Martinez, A.; Carrilho, C.; Martínez, M.; Bassat, Q.; Ordi, J.; Menéndez, C. Minimally Invasive Autopsy: A more feasible and safer alternative to conventional autopsy in the COVID-19 pandemic era? Med. Clin. Sci. 2020, 2, 1–5. [Google Scholar] [CrossRef]
- Paganelli, C.R.; Goco, N.J.; McClure, E.M.; Banke, K.K.; Blau, D.M.; Breiman, R.F.; Menéndez, C.; Rakislova, N.; Bassat, Q. The evolution of minimally invasive tissue sampling in postmortem examination: A narrative review. Glob. Health Action 2020, 13, 1792682. [Google Scholar] [CrossRef]
- Rakislova, N.; Fernandes, F.; Lovane, L.; Jamisse, L.; Castillo, P.; Sanz, A.; Marimon, L.; Jesri, S.; Ferrando, M.; Delgado, V.; et al. Standardization of Minimally Invasive Tissue Sampling Specimen Collection and Pathology Training for the Child Health and Mortality Prevention Surveillance Network. Clin. Infect. Dis. 2019, 69 (Suppl. 4), S302–S310. [Google Scholar] [CrossRef]
- Castillo, P.; Martínez, M.J.; Ussene, E.; Jordao, D.; Lovane, L.; Ismail, M.R.; Carrilho, C.; Lorenzoni, C.; Fernandes, F.; Bene, R.; et al. Validity of a Minimally Invasive Autopsy for Cause of Death Determination in Adults in Mozambique: An Observational Study. PLoS Med. 2016, 13, e1002171. [Google Scholar] [CrossRef] [Green Version]
- Bassat, Q.; Castillo, P.; Martínez, M.J.; Jordao, D.; Lovane, L.; Hurtado, J.C.; Nhampossa, T.; Santos Ritchie, P.; Bandeira, S.; Sambo, C.; et al. Validity of a minimally invasive autopsy tool for cause of death determination in pediatric deaths in Mozambique: An observational study. PLoS Med. 2017, 14, e1002317. [Google Scholar] [CrossRef] [Green Version]
- Menendez, C.; Castillo, P.; Martínez, M.J.; Jordao, D.; Lovane, L.; Ismail, M.R.; Carrilho, C.; Lorenzoni, C.; Fernandes, F.; Nhampossa, T.; et al. Validity of a minimally invasive autopsy for cause of death determination in stillborn babies and neonates in Mozambique: An observational study. PLoS Med. 2017, 14, e1002318. [Google Scholar] [CrossRef] [Green Version]
- Castillo, P.; Hurtado, J.C.; Martínez, M.J.; Jordao, D.; Lovane, L.; Ismail, M.R.; Carrilho, C.; Lorenzoni, C.; Fernandes, F.; Mocumbi, S.; et al. Validity of a minimally invasive autopsy for cause of death determination in maternal deaths in Mozambique: An observational study. PLoS Med. 2017, 14, e1002431. [Google Scholar] [CrossRef] [Green Version]
- Maixenchs, M.; Anselmo, R.; Zielinski-Gutiérrez, E.; Odhiambo, F.O.; Akello, C.; Ondire, M.; Zaidi, S.S.H.; Soofi, S.B.; Bhutta, Z.A.; Diarra, K.; et al. Willingness to Know the Cause of Death and Hypothetical Acceptability of the Minimally Invasive Autopsy in Six Diverse African and Asian Settings: A Mixed Methods Socio-Behavioural Study. PLoS Med. 2016, 13, e1002172. [Google Scholar] [CrossRef] [Green Version]
- Castillo, P.; Ussene, E.; Ismail, M.R.; Jordao, D.; Lovane, L.; Carrilho, C.; Lorenzoni, C.; Lacerda, M.V.; Palhares, A.; Rodríguez-Carunchio, L.; et al. Pathological Methods Applied to the Investigation of Causes of Death in Developing Countries: Minimally Invasive Autopsy Approach. PLoS ONE 2015, 10, e0132057. [Google Scholar] [CrossRef]
- Salzberg, N.T.; Sivalogan, K.; Bassat, Q.; Taylor, A.W.; Adedini, S.; El Arifeen, S.; Assefa, N.; Blau, D.M.; Chawana, R.; Cain, C.J.; et al. Mortality Surveillance Methods to Identify and Characterize Deaths in Child Health and Mortality Prevention Surveillance Network Sites. Clin. Infect. Dis. 2019, 69, S262–S273. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Basteiro, A.L.; Hurtado, J.C.; Castillo, P.; Fernandes, F.; Navarro, M.; Lovane, L.; Casas, I.; Quintó, L.; Jordao, D.; Ismail, M.R.; et al. Performance of the Xpert MTB/RIF Ultra Assay for Determining Cause of Death by TB in Tissue Samples Obtained by Minimally Invasive Autopsies. Chest 2021, 159, 103–107. [Google Scholar] [CrossRef]
- Gurley, E.S.; Parveen, S.; Islam, M.S.; Hossain, M.J.; Nahar, N.; Homaira, N.; Sultana, R.; Sejvar, J.J.; Rahman, M.; Luby, S.P. Family and community concerns about post-mortem needle biopsies in a Muslim society. BMC Med. Ethics 2011, 12, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Duarte-Neto, A.N.; de Almeida Monteiro, R.A.; Johnsson, J.; dos Passos Cunha, M.; Pour, S.Z.; Saraiva, A.C.; Ho, Y.L.; da Silva, L.F.; Mauad, T.; de Andrade Zanotto, P.M.; et al. Ultrasound-guided minimally invasive autopsy as a tool for rapid post-mortem diagnosis in the 2018 Sao Paulo yellow fever epidemic: Correlation with conventional autopsy. PLoS Negl. Trop. Dis. 2019, 13, e0007625. [Google Scholar] [CrossRef] [Green Version]
- European Centre for Disease Prevention and Control (ECDC) Technical Report: Infection Prevention and Control for COVID-19 in Healthcare Settings—Sixth Update 9 February 2021. Available online: https://www.ecdc.europa.eu/en/publications-data/infection-prevention-and-control-and-preparedness-covid-19-healthcare-settings (accessed on 15 February 2021).
- Mao, D.; Zhou, N.; Zheng, D.; Yue, J.; Zhao, Q.; Luo, B.; Guan, D.; Zhou, Y.; Hu, B. Guide to forensic pathology practice for death cases related to coronavirus disease 2019 (COVID-19) (Trial draft). Forensic Sci. Res. 2020, 5, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Infection Prevention and Control for the Safe Management of a Dead Body in the Context of COVID-19 Interim Guidance 4 September 2020; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar] [CrossRef] [Green Version]
- Davis, G.G.; Williamson, A.K. Risk of COVID-19 Transmission During Autopsy. Arch. Pathol. Lab. Med. 2020, 144, 1445a–1445. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.-Y.; Cheong, H.; Kim, H.-S. Proposal of the Autopsy Guideline for Infectious Diseases: Preparation for the Post-COVID-19 Era (abridged translation). J. Korean Med. Sci. 2020, 35, 310. [Google Scholar] [CrossRef] [PubMed]
- Mbanuzuru, A.V.; Okoro, C.C.; Mbanuzuru, C.M.; Ibeh, C.C. Call for proper documentation of COVID-19 deaths in poor resource setting: A necessity for management of future occurrences. Expert Rev. Anti. Infect. Ther. 2020, 19, 17–21. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention Centers for Disease Control and Prevention: Collection and Submission of Postmortem Specimens from Deceased Persons with Confirmed or Suspected COVID-19. Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/guidance-postmortem-specimens.html (accessed on 10 May 2020).
- Osborn, M.; Lucas, S.; Stewart, R.; Swift, B.; Youd, E. The Royal College of Pathologists: Autopsy Practice Relating to Possible Cases of COVID-19. Available online: www.rcpath.org (accessed on 26 August 2020).
- Tian, S.; Xiong, Y.; Liu, H.; Niu, L.; Guo, J.; Liao, M.; Xiao, S.Y. Pathological study of the 2019 novel coronavirus disease (COVID-19) through postmortem core biopsies. Mod. Pathol. 2020, 33, 1007–1014. [Google Scholar] [CrossRef] [Green Version]
- Xu, Z.; Shi, L.; Wang, Y.; Zhang, J.; Huang, L.; Zhang, C.; Liu, S.; Zhao, P.; Liu, H.; Zhu, L.; et al. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir. Med. 2020, 8, 420–422. [Google Scholar] [CrossRef]
- D’Onofrio, V.; Donders, E.; Abeele, M.E.V.; Dubois, J.; Cartuyvels, R.; Achten, R.; Lammens, M.; Dendooven, A.; Driessen, A.; Augsburg, L.; et al. The clinical value of minimal invasive autopsy in COVID-19 patients. PLoS ONE 2020, 15, e0242300. [Google Scholar] [CrossRef]
- Yao, X.H.; Li, T.Y.; He, Z.C.; Ping, Y.F.; Liu, H.W.; Yu, S.C.; Mou, H.M.; Wang, L.H.; Zhang, H.R.; Fu, W.J.; et al. A pathological report of three COVID-19 cases by minimally invasive autopsies. Chin. J. Pathol. 2020, 49, 411–417. [Google Scholar] [CrossRef]
- Zhang, H.; Zhou, P.; Wei, Y.; Yue, H.; Wang, Y.; Hu, M.; Zhang, S.; Cao, T.; Yang, C.; Li, M.; et al. Histopathologic Changes and SARS–CoV-2 Immunostaining in the Lung of a Patient with COVID-19. Ann. Intern. Med. 2020, 172, 629–632. [Google Scholar] [CrossRef] [Green Version]
- Wu, J.H.; Li, X.; Huang, B.; Su, H.; Li, Y.; Luo, D.J.; Chen, S.; Ma, L.; Wang, S.H.; Nie, X.; et al. Pathological changes of fatal coronavirus disease 2019 (COVID-19) in the lungs: Report of 10 cases by postmortem needle autopsy. Chin. J. Pathol. 2020, 49, 568–575. [Google Scholar] [CrossRef]
- Monteiro, R.A.; Duarte-Neto, A.N.; Silva, L.F.; Oliveira, E.P.; Santos, G.A.; Oliveira, I.R.; Mauad, T.; Saldiva, P.H.; Dolhnikoff, M. Ultrasound-guided minimally invasive autopsies: A protocol for the study of pulmonary and systemic involvement of COVID-19. Clinics 2020, 75, 1–2. [Google Scholar] [CrossRef]
- Shao, C.; Liu, H.; Meng, L.; Sun, L.; Wang, Y.; Yue, Z.; Kong, H.; Li, H.; Weng, H.; Lv, F.; et al. Evolution of severe acute respiratory syndrome coronavirus 2 RNA test results in a patient with fatal coronavirus disease 2019: A case report. Hum. Pathol. 2020, 101, 82–88. [Google Scholar] [CrossRef]
- Copin, M.C.; Parmentier, E.; Duburcq, T.; Poissy, J.; Mathieu, D.; Caplan, M.; Cousin, N.; Durand, A.; Goutay, J.; Kalioubie, A.E.; et al. Time to consider histologic pattern of lung injury to treat critically ill patients with COVID-19 infection. Intensive Care Med. 2020, 46, 1124–1126. [Google Scholar] [CrossRef] [Green Version]
- Golmai, P.; Larsen, C.P.; DeVita, M.V.; Wahl, S.J.; Weins, A.; Rennke, H.G.; Bijol, V.; Rosenstock, J.L. Histopathologic and Ultrastructural Findings in Postmortem Kidney Biopsy Material in 12 Patients with AKI and COVID-19. J. Am. Soc. Nephrol. 2020, 31, 1944–1947. [Google Scholar] [CrossRef]
- Yao, X.H.; He, Z.C.; Li, T.Y.; Zhang, H.R.; Wang, Y.; Mou, H.; Guo, Q.; Yu, S.C.; Ding, Y.; Liu, X.; et al. Pathological evidence for residual SARS-CoV-2 in pulmonary tissues of a ready-for-discharge patient. Cell Res. 2020, 30, 541–543. [Google Scholar] [CrossRef]
- Brook, O.R.; Piper, K.G.; Mercado, N.B.; Gebre, M.S.; Barouch, D.H.; Busman-Sahay, K.; Starke, C.E.; Estes, J.D.; Martinot, A.J.; Wrijil, L.; et al. Feasibility and safety of ultrasound-guided minimally invasive autopsy in COVID-19 patients. Abdom. Radiol. 2021, 46, 1263–1271. [Google Scholar] [CrossRef]
- Palhares, A.E.M.; Ferreira, L.; Freire, M.; Castillo, P.; Martinez, M.J.; Hurtado, J.C.; Rakislova, N.; Varo, R.; Navarro, M.; Casas, I.; et al. Performance of the Minimally Invasive Autopsy tool for Cause of Death Determination in Adults Deaths from the Brazilian Amazon: An Observational Study. Virchows Arch. 2019, 475, 649–658. [Google Scholar] [CrossRef] [Green Version]
- Duarte-Neto, A.N.; de Almeida Monteiro, R.A.; da Silva, L.F.; Malheiros, D.M.; de Oliveira, E.P.; Theodoro Filho, J.; Pinho, J.R.; Soares Gomes-Gouvêa, M.; Salles, A.P.; de Oliveira, I.R.; et al. Pulmonary and systemic involvement of COVID-19 assessed by ultrasound-guided minimally invasive autopsy. Histopathology 2020, 77, 186–197. [Google Scholar] [CrossRef] [PubMed]
- Wichmann, D.; Sperhake, J.-P.; Lütgehetmann, M.; Steurer, S.; Edler, C.; Heinemann, A.; Heinrich, F.; Mushumba, H.; Kniep, I.; Schröder, A.S.; et al. Autopsy Findings and Venous Thromboembolism in Patients with COVID-19: A Prospective Cohort Study. Ann. Intern. Med. 2020, 173, 268–277. [Google Scholar] [CrossRef] [PubMed]
- Remmelink, M.; De Mendonça, R.; D’Haene, N.; De Clercq, S.; Verocq, C.; Lebrun, L.; Lavis, P.; Racu, M.L.; Trépant, A.L.; Maris, C.; et al. Unspecific post-mortem findings despite multiorgan viral spread in COVID-19 patients. Crit. Care 2020, 24, 495. [Google Scholar] [CrossRef] [PubMed]
- Menter, T.; Haslbauer, J.D.; Nienhold, R.; Savic, S.; Hopfer, H.; Deigendesch, N.; Frank, S.; Turek, D.; Willi, N.; Pargger, H.; et al. Post-mortem examination of COVID19 patients reveals diffuse alveolar damage with severe capillary congestion and variegated findings of lungs and other organs suggesting vascular dysfunction. Histopathology 2020, 77, 198–209. [Google Scholar] [CrossRef]
- Konopka, K.E.; Nguyen, T.; Jentzen, J.M.; Rayes, O.; Schmidt, C.J.; Wilson, A.M.; Farver, C.F.; Myers, J.L. Diffuse Alveolar Damage (DAD) from Coronavirus Disease 2019 Infection is Morphologically Indistinguishable from Other Causes of DAD. Histopathology 2020, 77, 570–578. [Google Scholar] [CrossRef]
- Lax, S.F.; Skok, K.; Zechner, P.; Kessler, H.H.; Kaufmann, N.; Koelblinger, C.; Vander, K.; Bargfrieder, U.; Trauner, M. Pulmonary Arterial Thrombosis in COVID-19 With Fatal Outcome: Results From a Prospective, Single-Center, Clinicopathologic Case Series. Ann. Intern. Med. 2020, 173, 350–361. [Google Scholar] [CrossRef]
- Fox, S.E.; Akmatbekov, A.; Harbert, J.L.; Li, G.; Quincy Brown, J.; Vander Heide, R.S. Pulmonary and cardiac pathology in African American patients with COVID-19: An autopsy series from New Orleans. Lancet Respir. Med. 2020, 8, 681–686. [Google Scholar] [CrossRef]
- Ackermann, M.; Verleden, S.E.; Kuehnel, M.; Haverich, A.; Welte, T.; Laenger, F.; Vanstapel, A.; Werlein, C.; Stark, H.; Tzankov, A.; et al. Pulmonary Vascular Endothelialitis, Thrombosis, and Angiogenesis in Covid-19. N. Engl. J. Med. 2020, 383, 120–128. [Google Scholar] [CrossRef]
- Schaller, T.; Hirschbühl, K.; Burkhardt, K.; Braun, G.; Trepel, M.; Märkl, B.; Claus, R. Postmortem Examination of Patients with COVID-19. JAMA J. Am. Med. Assoc. 2020, 323, 2518–2520. [Google Scholar] [CrossRef]
- Dell’Aquila, M.; Cattani, P.; Fantoni, M.; Marchetti, S.; Aquila, I.; Stigliano, E.; Carbone, A.; Oliva, A.; Arena, V. Postmortem swabs in the Sars-CoV-2 Pandemic: Report on 12 complete clinical autopsy cases. Arch. Pathol. Lab. Med. 2020, 144, 1298–1302. [Google Scholar] [CrossRef]
- Edler, C.; Schröder, A.; Aepfelbacher, M.; Fitzek, A.; Heinemann, A.; Heinrich, F.; Klein, A.; Langenwalder, F.; Lütgehetmann, M.; Meißner, K.; et al. Dying with SARS-CoV-2 infection-an autopsy study of the first consecutive 80 cases in Hamburg, Germany. Int. J. Legal Med. 2020, 134. [Google Scholar] [CrossRef]
- Grosse, C.; Grosse, A.; Salzer, H.J.F.; Dünser, M.W.; Motz, R.; Langer, R. Analysis of cardiopulmonary findings in COVID-19 fatalities: High incidence of pulmonary artery thrombi and acute suppurative bronchopneumonia. Cardiovasc. Pathol. 2020, 49, 107263. [Google Scholar] [CrossRef]
- Rapkiewicz, A.V.; Mai, X.; Carsons, S.E.; Pittaluga, S.; Kleiner, D.E.; Berger, J.S.; Thomas, S.; Adler, N.M.; Charytan, D.M.; Gasmi, B.; et al. Megakaryocytes and platelet-fibrin thrombi characterize multi-organ thrombosis at autopsy in COVID-19: A case series. EClinicalMedicine 2020, 24, 100434. [Google Scholar] [CrossRef]
- Evert, K.; Dienemann, T.; Brochhausen, C.; Lunz, D.; Lubnow, M.; Ritzka, M.; Keil, F.; Trummer, M.; Scheiter, A.; Salzberger, B.; et al. Autopsy findings after long-term treatment of COVID-19 patients with microbiological correlation. Virchows Arch. 2021, 1–12. [Google Scholar] [CrossRef]
- Dong, M.; Zhang, J.; Ma, X.; Tan, J.; Chen, L.; Liu, S.; Xin, Y.; Zhuang, L. ACE2, TMPRSS2 distribution and extrapulmonary organ injury in patients with COVID-19. Biomed. Pharmacother. 2021, 131, 110678. [Google Scholar] [CrossRef]
- Mascolo, P.; Feola, A.; Sementa, C.; Leone, S.; Zangani, P.; Della Pietra, B.; Campobasso, C. Pietro A Descriptive Study on Causes of Death in Hospitalized Patients in an Acute General Hospital of Southern Italy during the Lockdown due to Covid-19 Outbreak. Healthcare 2021, 9, 119. [Google Scholar] [CrossRef]
- Yip, C.C.Y.; Sridhar, S.; Cheng, A.K.W.; Leung, K.H.; Choi, G.K.Y.; Chen, J.H.K.; Poon, R.W.S.; Chan, K.H.; Wu, A.K.L.; Chan, H.S.Y.; et al. Evaluation of the commercially available LightMix® Modular E-gene kit using clinical and proficiency testing specimens for SARS-CoV-2 detection. J. Clin. Virol. 2020, 129. [Google Scholar] [CrossRef]
- Chen, Y.; Chen, L.; Deng, Q.; Zhang, G.; Wu, K.; Ni, L.; Yang, Y.; Liu, B.; Wang, W.; Wei, C.; et al. The presence of SARS-CoV-2 RNA in the feces of COVID-19 patients. J. Med. Virol. 2020, 92, 833–840. [Google Scholar] [CrossRef] [Green Version]
- Papoutsis, A.; Borody, T.; Dolai, S.; Daniels, J.; Steinberg, S.; Barrows, B.; Hazan, S. Detection of SARS-CoV-2 from patient fecal samples by whole genome sequencing. Gut Pathog. 2021, 13. [Google Scholar] [CrossRef]
- Gandhi, M.; Yokoe, D.S.; Havlir, D.V. Asymptomatic Transmission, the Achilles’ Heel of Current Strategies to Control Covid-19. N. Engl. J. Med. 2020, 382, 2158–2160. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Personal Protective Equipment (PPE) | Autopsy Room | Other | |||
|---|---|---|---|---|---|
| Basic | Desirable | Basic | Desirable | Recommendations | |
| Scrub suit | Plastic apron | Well-ventilated | Negative air pressure | All essential equipment prepared before the start of MIA (pre-labelling is desirable) | |
| Waterproof long-sleeved gown | Waterproof gown covering the whole body orcoverall suit with hood | Clean | Clearly identified separation between “clean” and “dirty” areas | Use of pre-filled containers:
| |
| Boots | Specific closed shoes covered by waterproof shoe covers | Adequate lighting | Limit the number of personnel involved in the MIA and in the room | ||
| Long-sleeved double gloves for the MIA specialist (performing the punctures) | Long-sleeved double gloves for all the personnel involved in MIA | Thorough disinfection of the surfaces and tools during and after MIA | |||
| FFP3/N99 | PAPR mask with a surgical mask | Free from unnecessary jars, tools and obstacles | Careful and slow doffing of PPE items | ||
| Lightweight safety goggles | Anti-fog lightweight safety googles or face shield | Provide a list of the personnel participating in MIA to the head of the department | |||
| Surgical cap to protect hair | Hood covering the surgical cap | ||||
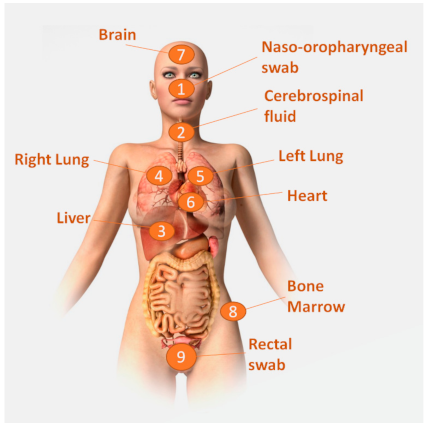
| Tissue/Body Fluid | Site of Collection | Mode of Collection | Needle/Tool | Type | Gauge | Needle Length (mm) |
|---|---|---|---|---|---|---|
| Naso-oropharyngeal secretions | Nasopharynx and oropharynx | Swabbing | Swab | Manual | N/A | N/A |
| Stool | Rectum | Brush sampling | Brush | Manual | N/A | N/A |
| Blood | Subclavian vein or heart | Needle aspiration | Quincke Spinal # | Manual | 20 | 100 |
| Cerebrospinal fluid | Occipital approach to the cisterna magna | Needle aspiration | Quincke Spinal # | Manual | 20 | 100 |
| Liver | Right lateral abdominal wall | Core needle biopsy | Monopty * | Automatic | 14–16 | 115 |
| Thorax (lungs/heart) | Right and left clavicular region down to the diaphragm for microbiology samples. Multiple random thoracic punctures for pathology. | Core needle biopsy | Monopty * | Automatic | 14–16 | 100 |
| Bone marrow | Anterior superior iliac crest | Trephine biopsy | T-Lok ™ trephine ** | Manual | 8 | 100 |
| Central nervous system | Occipital approach, space between occipital bone and first vertebra. Trans-nasal approach through lamina cribrosa | Core needle biopsy | Monopty * | Automatic | 16 | 200 |
| Skin | Macroscopically detected lesions | Punch biopsy | Biopsy punch ## | Manual | 5 mm | - |
| ID | Age/Sex | Comorbidities | Clinical Symptoms | Time from Symptoms Onset to Death (Days) |
|---|---|---|---|---|
| 1 | 66/M | Diabetes mellitus type II, ischemic heart disease, kidney transplant, severe obesity, | Fever, dyspnea | 4 |
| 2 | 88/F | Diabetes mellitus type II, cerebrovascular disease, chronic renal disease | Jaundice, cough, dyspnea | 11 |
| 3 | 76/M | Hypertension | Fever, cough, hemoptysis, dyspnea | 7 |
| 4 | 66/F | Chronic obstructive pulmonary disease, cor pulmonale, spondylitis | Dyspnea, mucopurulent sputum | 17 |
| 5 | 78/M | Hypertension, diabetes mellitus type II, cerebrovascular disease | Lethargy | Unknown |
| 6 | 85/F | Hypertension | Diarrhea | 3 |
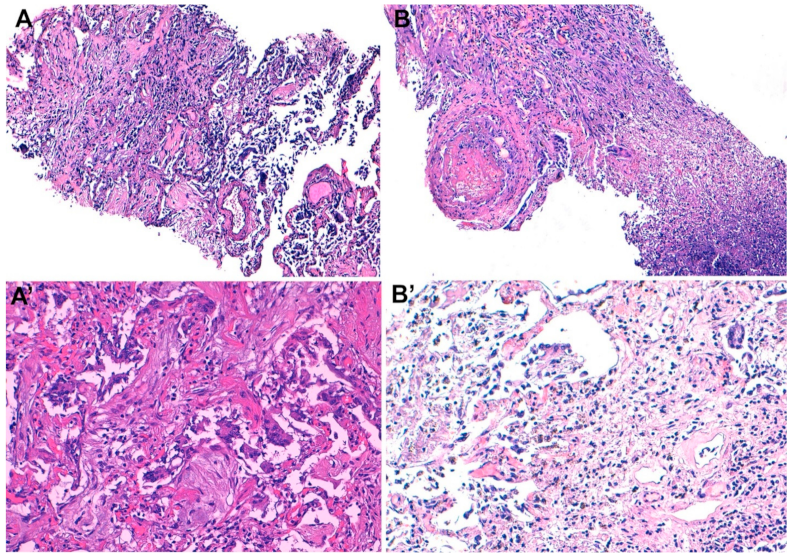
| ID | Pathological Findings in the Lungs | Pathological Findings in Other Organs | Underlying Cause of Death | Intermediate Cause of Death | Immediate Cause of Death | NP/OP PCR | Lungs PCR | Liver PCR | Brain PCR | Stool PCR |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Diffuse alveolar damage (exudative) | Extensive myocardial scarring | COVID-19 (test positive) | Pneumonia | ARDS | + | + | - | + | - |
| 2 | Diffuse alveolar damage (proliferative/exudative), focal bronchiolitis | Cholestatic hepatitis | COVID-19 (test positive) | Pneumonia | ARDS | + | + | - | - | + |
| 3 | Diffuse alveolar damage (proliferative/exudative) | - | COVID-19 (test positive) | Pneumonia | ARDS | + | + | - | - | + |
| 4 | Diffuse alveolar damage (proliferative), necrotizing pneumonia, microthrombi | Cholestasis | COVID-19 (test positive) | Pneumonia | ARDS | + | + | - | - | - |
| 5 | Diffuse necrotizing pneumonia | - | Aspiration pneumonia | Enterococcal septicemia | Septic shock | + | + | - | - | + |
| 6 | Mild interstitial infiltrates | Myocardial infarction with wall rupture | Acute myocardial infarction | Cardiac wall rupture | Cardiogenic shock | + | + | - | - | + |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rakislova, N.; Marimon, L.; Ismail, M.R.; Carrilho, C.; Fernandes, F.; Ferrando, M.; Castillo, P.; Rodrigo-Calvo, M.T.; Guerrero, J.; Ortiz, E.; et al. Minimally Invasive Autopsy Practice in COVID-19 Cases: Biosafety and Findings. Pathogens 2021, 10, 412. https://doi.org/10.3390/pathogens10040412
Rakislova N, Marimon L, Ismail MR, Carrilho C, Fernandes F, Ferrando M, Castillo P, Rodrigo-Calvo MT, Guerrero J, Ortiz E, et al. Minimally Invasive Autopsy Practice in COVID-19 Cases: Biosafety and Findings. Pathogens. 2021; 10(4):412. https://doi.org/10.3390/pathogens10040412
Chicago/Turabian StyleRakislova, Natalia, Lorena Marimon, Mamudo R. Ismail, Carla Carrilho, Fabiola Fernandes, Melania Ferrando, Paola Castillo, Maria Teresa Rodrigo-Calvo, José Guerrero, Estrella Ortiz, and et al. 2021. "Minimally Invasive Autopsy Practice in COVID-19 Cases: Biosafety and Findings" Pathogens 10, no. 4: 412. https://doi.org/10.3390/pathogens10040412