
Combined Therapy of Chitosan and Exercise Improves the Lipid Profile, Adipose Tissue and Hepatic Alterations in an In Vivo Model of Induced-Hyperlipidemia

 ,
,  , , , ,
, , , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Animals
2.2. Hyperlipidemia Induction
2.3. Chitosan
2.4. Hyperlipidemia Induction Procedure
2.5. Treatment Phase
2.5.1. Physical Training
2.5.2. Chitosan Treatment
2.6. Assessment of Body Mass and Lee’s Obesity Index
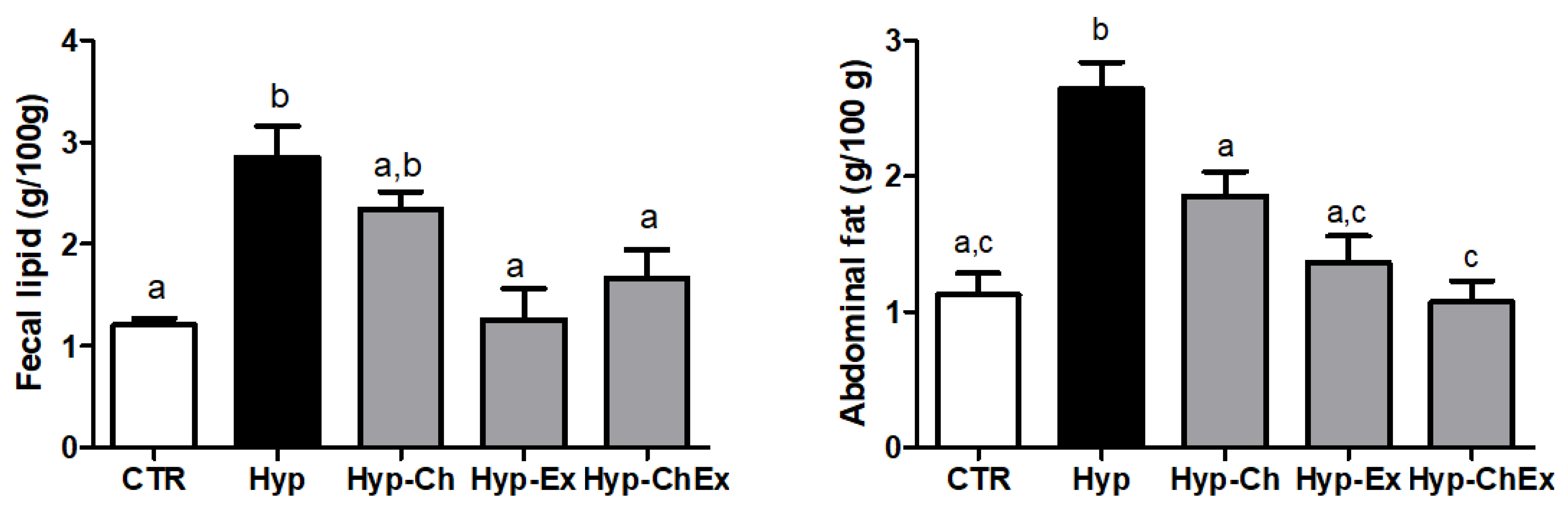
2.7. Determination of Lipid Percentage in Feces
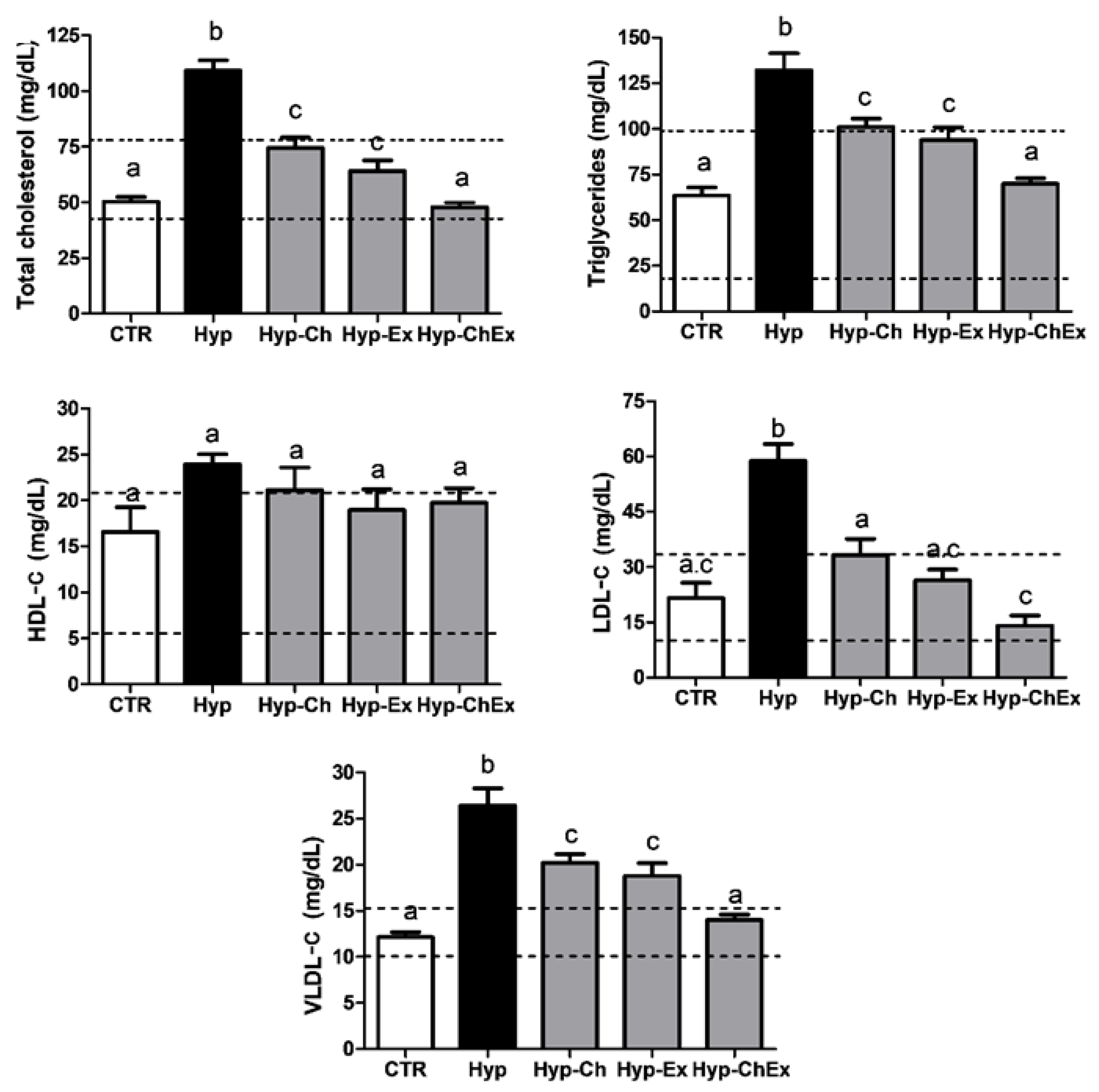
2.8. Biochemical Analysis of Serum Lipid Concentrations
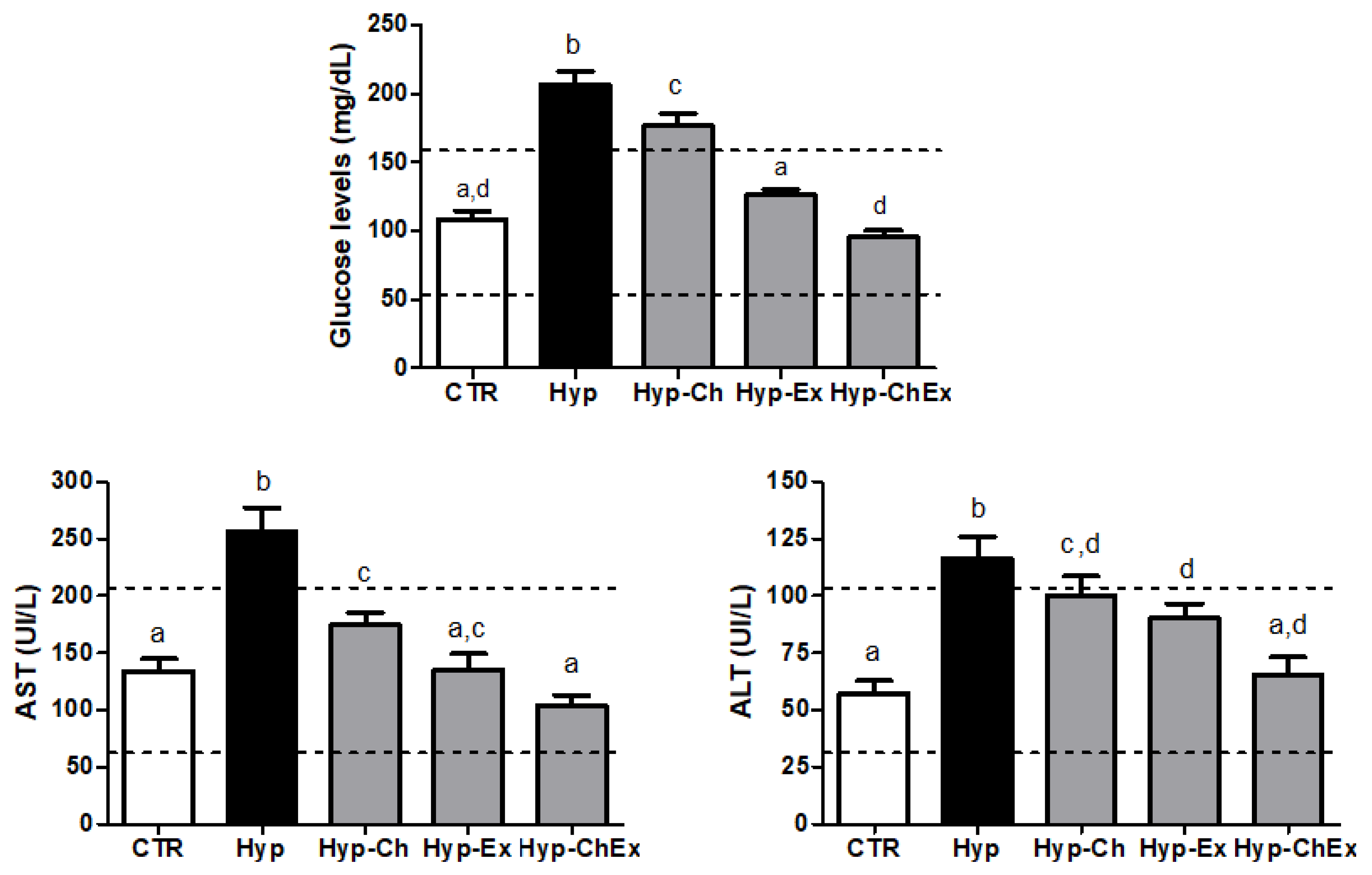
2.9. Biochemical Analysis of Liver Enzyme and Glucose Dosages
2.10. Animal Euthanasia
2.11. Assessment of Abdominal Adipose Tissue Weight
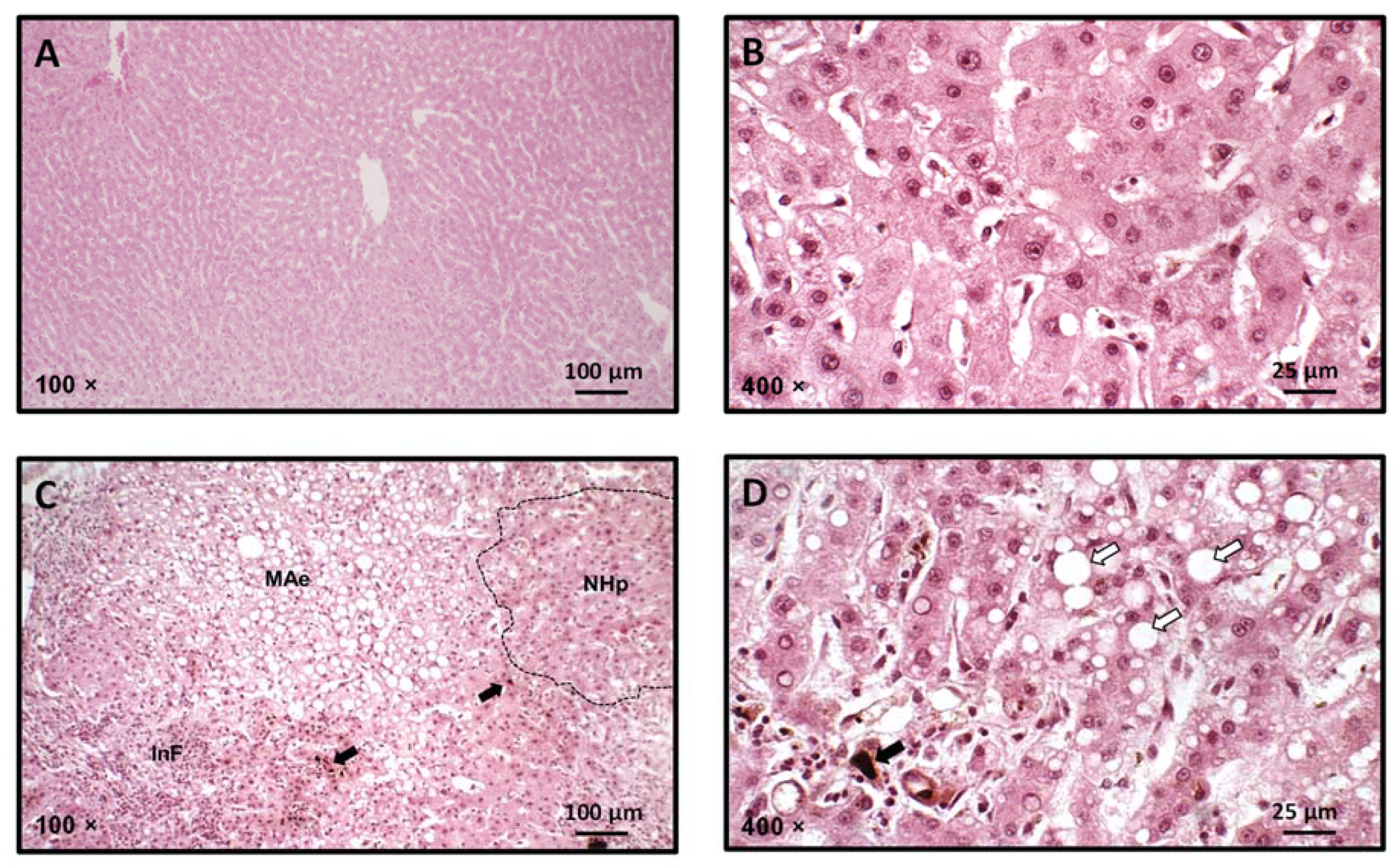
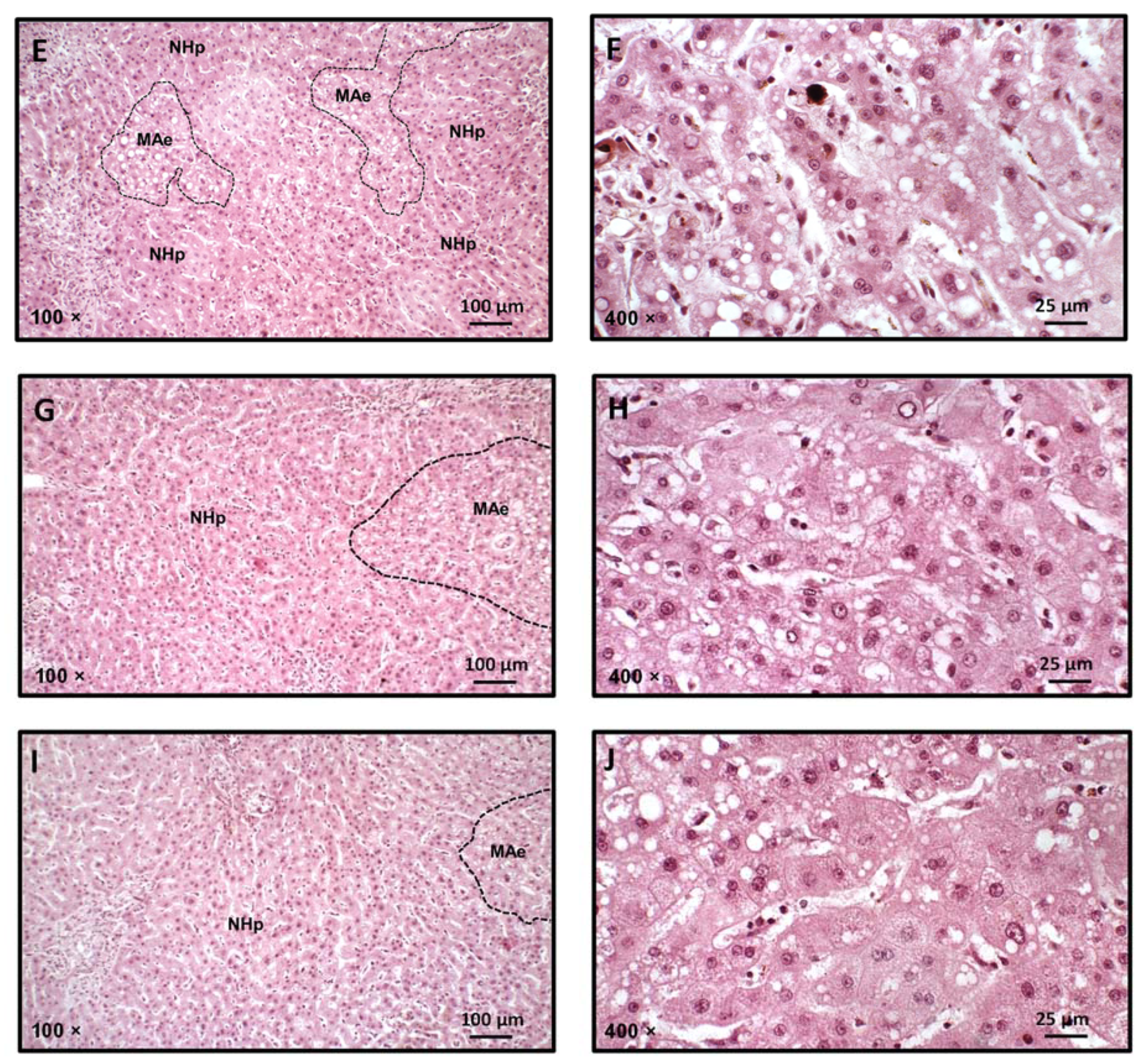
2.12. Histopathological Analysis of Liver Specimens
2.13. Statistical Analysis
3. Results and Discussion
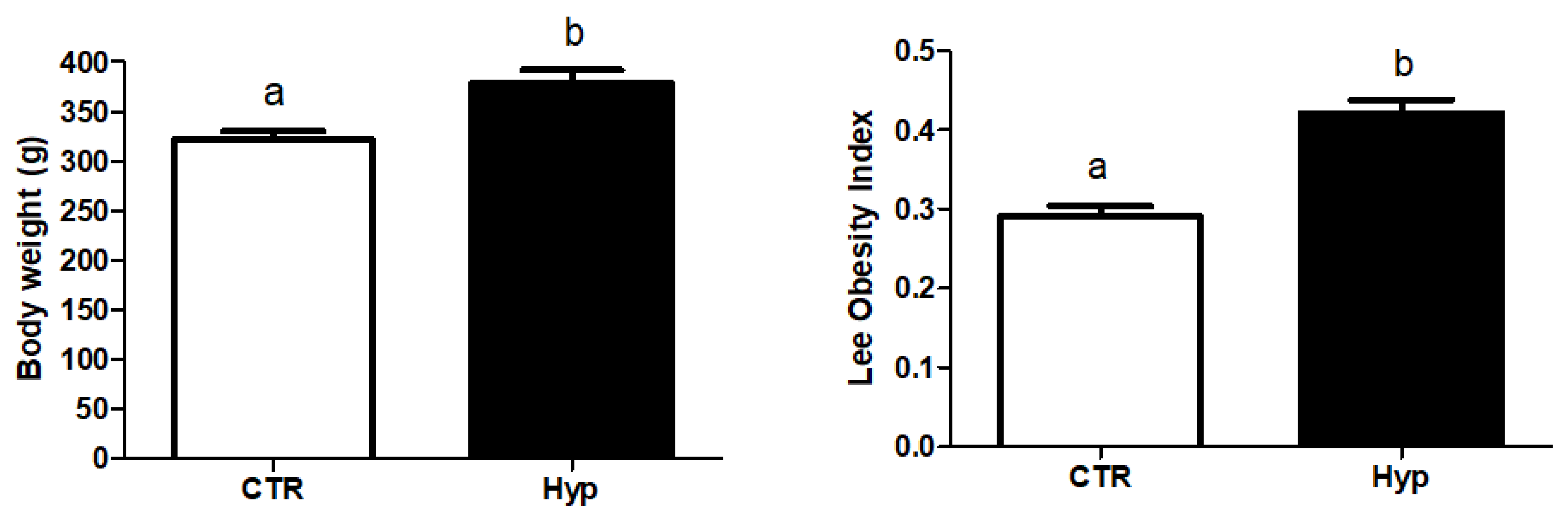
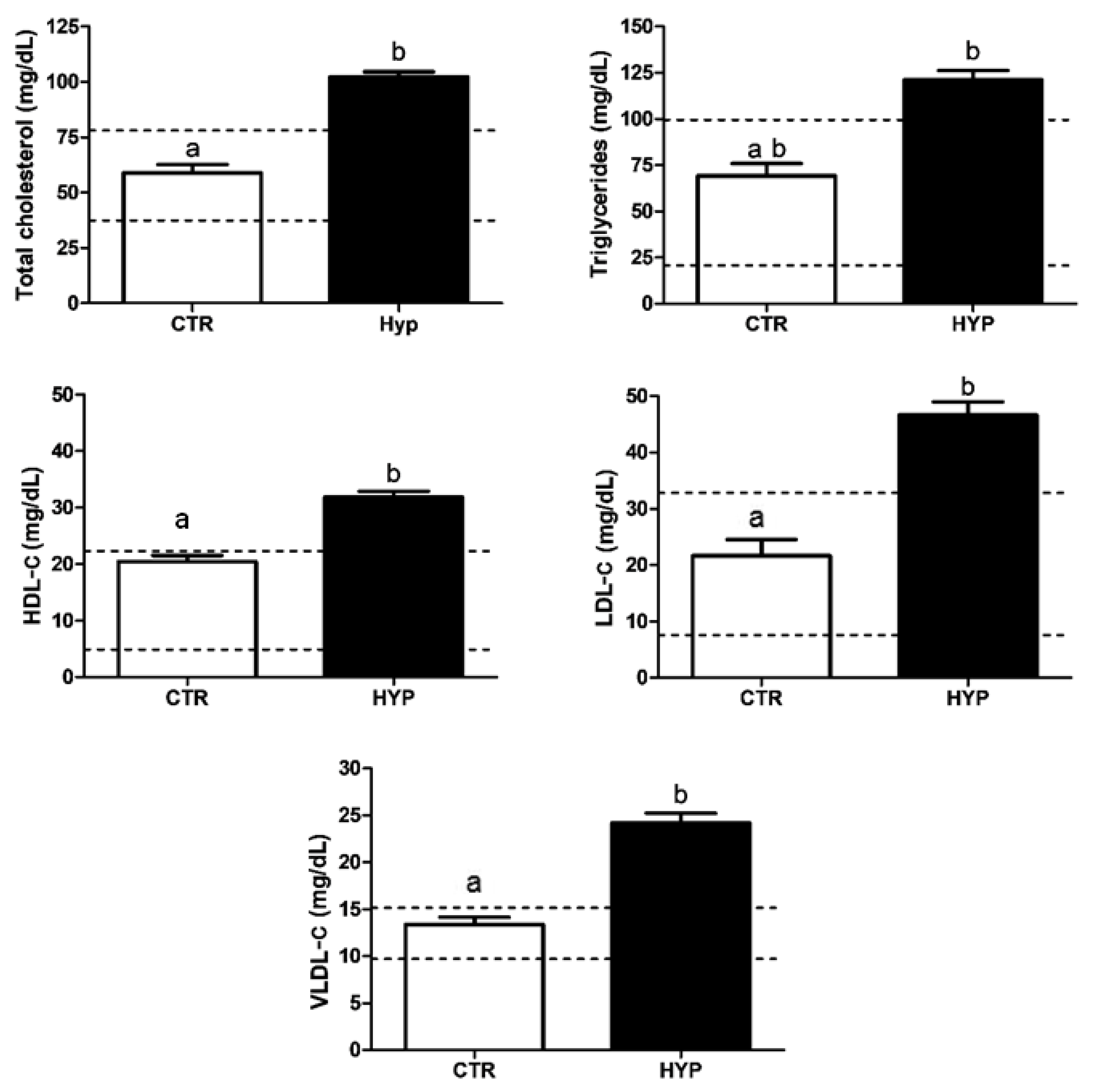
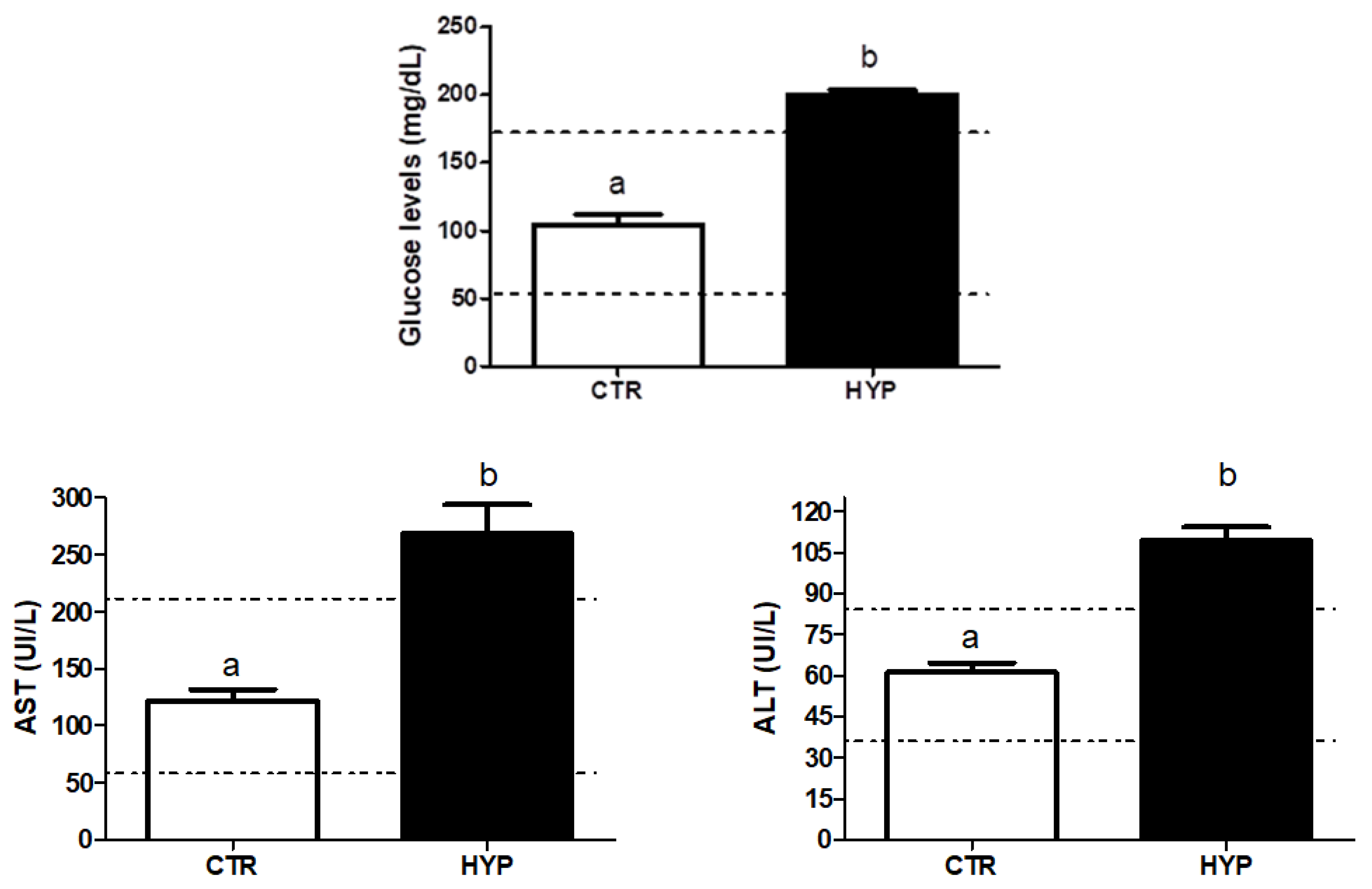
3.1. Hyperlipidemia Induction
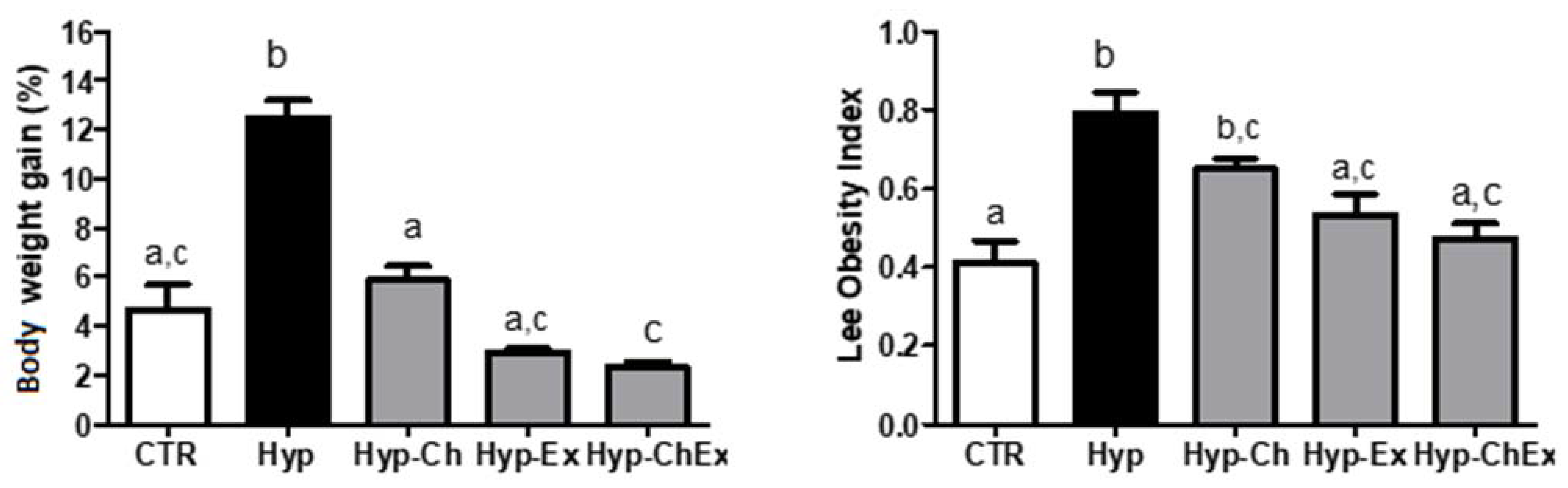
3.2. Physical Training and Chitosan Treatment
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rychter, A.M.; Skrzypczak-Zielinska, M.; Zielinska, A.; Eder, P.; Souto, E.B.; Zawada, A.; Ratajczak, A.E.; Dobrowolska, A.; Krela-Kazmierczak, I. Is the Retinol-Binding Protein 4 a Possible Risk Factor for Cardiovascular Diseases in Obesity? Int. J. Mol. Sci. 2020, 21, 5229. [Google Scholar] [CrossRef] [PubMed]
- Karczewski, J.; Zielińska, A.; Staszewski, R.; Eder, P.; Dobrowolska, A.; Souto, E.B. Obesity and the brain. Int. J. Mol. Sci. 2022; submitted. [Google Scholar]
- Kolb, H.; Martin, S. Environmental/lifestyle factors in the pathogenesis and prevention of type 2 diabetes. BMC Med. 2017, 15, 131. [Google Scholar] [CrossRef] [PubMed]
- Galgani, J.E.; Fernández-Verdejo, R. Pathophysiological role of metabolic flexibility on metabolic health. Obes. Rev. 2021, 22, e13131. [Google Scholar] [CrossRef] [PubMed]
- WHO (World Health Organization). Available online: https://www.who.int/ncds/prevention/physical-activity/inactivity-global-health-problem/en/ (accessed on 8 June 2021).
- Stewart, J.; McCallin, T.; Martinez, J.; Chacko, S.; Yusuf, S. Hyperlipidemia. Pediatr. Rev. 2020, 41, 393–402. [Google Scholar] [CrossRef] [PubMed]
- Chanoine, P.; Spector, N.D. Hyperlipidemia, eating disorders, and smoking cessation. Curr. Opin. Pediatr. 2008, 20, 734–739. [Google Scholar] [CrossRef] [PubMed]
- Xi, Y.; Niu, L.; Cao, N.; Bao, H.; Xu, X.; Zhu, H.; Yan, T.; Zhang, N.; Qiao, L.; Han, K.; et al. Prevalence of dyslipidemia and associated risk factors among adults aged ≥35 years in northern China: A cross-sectional study. BMC Public Health 2020, 20, 1068. [Google Scholar] [CrossRef]
- Dankner, R.; Ben Avraham, S.; Harats, D.; Chetrit, A. ApoE Genotype, Lipid Profile, Exercise, and the Associations With Cardiovascular Morbidity and 18-Year Mortality. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2020, 75, 1887–1893. [Google Scholar] [CrossRef]
- Mendonça, M.A.A.; Ribeiro, A.R.S.; Lima, A.K.; Bezerra, G.B.; Pinheiro, M.S.; Albuquerque-Júnior, R.L.C.; Gomes, M.Z.; Padilha, F.F.; Thomazzi, S.M.; Novellino, E.; et al. Red Propolis and Its Dyslipidemic Regulator Formononetin: Evaluation of Antioxidant Activity and Gastroprotective Effects in Rat Model of Gastric Ulcer. Nutrients 2020, 12, 2951. [Google Scholar] [CrossRef]
- Mendoza-Herrera, K.; Pedroza-Tobías, A.; Hernández-Alcaraz, C.; Ávila-Burgos, L.; Aguilar-Salinas, C.A.; Barquera, S. Attributable Burden and Expenditure of Cardiovascular Diseases and Associated Risk Factors in Mexico and other Selected Mega-Countries. Int. J. Environ. Res. Public Health 2019, 16, 4041. [Google Scholar] [CrossRef] [Green Version]
- Gebreegziabiher, G.; Belachew, T.; Mehari, K.; Tamiru, D. Prevalence of dyslipidemia and associated risk factors among adult residents of Mekelle City, Northern Ethiopia. PLoS ONE 2021, 16, e0243103. [Google Scholar] [CrossRef]
- Erem, C.; Hacihasanoglu, A.; Deger, O.; Kocak, M.; Topbas, M. Prevalence of dyslipidemia and associated risk factors among Turkish adults: Trabzon lipid study. Endocrine 2008, 34, 36–51. [Google Scholar] [CrossRef] [PubMed]
- Opoku, S.; Gan, Y.; Fu, W.; Chen, D.; Addo-Yobo, E.; Trofimovitch, D.; Yue, W.; Yan, F.; Wang, Z.; Lu, Z. Prevalence and risk factors for dyslipidemia among adults in rural and urban China: Findings from the China National Stroke Screening and prevention project (CNSSPP). BMC Public Health 2019, 19, 1500. [Google Scholar] [CrossRef] [PubMed]
- Gao, H.; Wang, H.; Shan, G.; Liu, R.; Chen, H.; Sun, S.; Liu, Y. Prevalence of dyslipidemia and associated risk factors among adult residents of Shenmu City, China. PLoS ONE 2021, 16, e0250573. [Google Scholar] [CrossRef] [PubMed]
- Zhang, F.L.; Xing, Y.Q.; Wu, Y.H.; Liu, H.Y.; Luo, Y.; Sun, M.S.; Guo, Z.N.; Yang, Y. The prevalence, awareness, treatment, and control of dyslipidemia in northeast China: A population-based cross-sectional survey. Lipids Health Dis. 2017, 16, 61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mosca, L. Management of Dyslipidemia in Women in the Post–hormone Therapy Era. J. Gen. Intern. Med. 2005, 20, 297–305. [Google Scholar] [CrossRef] [Green Version]
- Yu, K.; Xue, Y.; He, T.; Guan, L.; Zhao, A.; Zhang, Y. Association of Spicy Food Consumption Frequency with Serum Lipid Profiles in Older People in China. J. Nutr. Health Aging 2018, 22, 311–320. [Google Scholar] [CrossRef]
- Sobczak, A.I.S.; Blindauer, C.A.; Stewart, A.J. Changes in Plasma Free Fatty Acids Associated with Type-2 Diabetes. Nutrients 2019, 11, 2022. [Google Scholar] [CrossRef] [Green Version]
- Guerra, R.L.F.; Prado, W.L.; Cheik, N.C.; Viana, F.P.; Botero, J.P.; Vendramini, R.C.; Carlos, I.Z.; Rossi, E.A.; Dâmaso, A.R. Effects of 2 or 5 consecutive exercise days on adipocyte area and lipid parameters in Wistar rats. Lipids Health Dis. 2007, 6, 16. [Google Scholar] [CrossRef] [Green Version]
- Mann, S.; Beedie, C.; Jimenez, A. Differential effects of aerobic exercise, resistance training and combined exercise modalities on cholesterol and the lipid profile: Review, synthesis and recommendations. Sports Med. 2014, 44, 211–221. [Google Scholar] [CrossRef] [Green Version]
- Bahijri, S.M.; Alsheikh, L.; Ajabnoor, G.; Borai, A. Effect of Supplementation With Chitosan on Weight, Cardiometabolic, and Other Risk Indices in Wistar Rats Fed Normal and High-Fat/High-Cholesterol Diets Ad Libitum. Nutr. Metab. Insights 2017, 10, 1178638817710666. [Google Scholar] [CrossRef] [Green Version]
- Jemai, H.; Bouaziz, M.; Fki, I.; El Feki, A.; Sayadi, S. Hypolipidimic and antioxidant activities of oleuropein and its hydrolysis derivative-rich extracts from Chemlali olive leaves. Chem.-Biol. Interact. 2008, 176, 88–98. [Google Scholar] [CrossRef] [PubMed]
- Silva, I.M.V.; Machado, F.; Moreno, M.J.; Nunes, C.; Coimbra, M.A.; Coreta-Gomes, F. Polysaccharide Structures and Their Hypocholesterolemic Potential. Molecules 2021, 26, 4559. [Google Scholar] [CrossRef] [PubMed]
- Erickson, N.; Zafron, M.; Harding, S.V.; Marinangeli, C.P.F.; Rideout, T.C. Evaluating the Lipid-Lowering Effects of α-lipoic Acid Supplementation: A Systematic Review. J. Diet. Suppl. 2020, 17, 753–767. [Google Scholar] [CrossRef] [PubMed]
- Poli, A.; Visioli, F. Pharmacology of Nutraceuticals with Lipid Lowering Properties. High Blood Press. Cardiovasc. Prev. 2019, 26, 113–118. [Google Scholar] [CrossRef]
- Yang, M.; Hu, D.; Cui, Z.; Li, H.; Man, C.; Jiang, Y. Lipid-Lowering Effects of Inonotus obliquus Polysaccharide In Vivo and In Vitro. Foods 2021, 10, 3085. [Google Scholar] [CrossRef]
- Derosa, G.; Colletti, A.; Maffioli, P.; D’Angelo, A.; Lupi, A.; Zito, G.B.; Mureddu, G.F.; Raddino, R.; Fedele, F.; Cicero, A.F.G. Lipid-lowering nutraceuticals update on scientific evidence. J. Cardiovasc. Med. 2020, 21, 845–859. [Google Scholar] [CrossRef]
- Hadipour, E.; Taleghani, A.; Tayarani-Najaran, N.; Tayarani-Najaran, Z. Biological effects of red beetroot and betalains: A review. Phytother. Res. PTR 2020, 34, 1847–1867. [Google Scholar] [CrossRef]
- Xiong, Z.; Cao, X.; Wen, Q.; Chen, Z.; Cheng, Z.; Huang, X.; Zhang, Y.; Long, C.; Zhang, Y.; Huang, Z. An overview of the bioactivity of monacolin K/lovastatin. Food Chem. Toxicol. 2019, 131, 110585. [Google Scholar] [CrossRef]
- Gerards, M.C.; Terlou, R.J.; Yu, H.; Koks, C.H.; Gerdes, V.E. Traditional Chinese lipid-lowering agent red yeast rice results in significant LDL reduction but safety is uncertain—A systematic review and meta-analysis. Atherosclerosis 2015, 240, 415–423. [Google Scholar] [CrossRef] [Green Version]
- Hosseini, Z.; Ghaedi, H.; Ahmadi, M.; Hosseini, S.A. Lipid-Lowering Effects of Concurrent Training and Green Tea Consumption in Overweight Women. J. Obes. Metab. Syndr. 2020, 29, 313–319. [Google Scholar] [CrossRef]
- Conte, M.S.; Bradbury, A.W.; Kolh, P.; White, J.V.; Dick, F.; Fitridge, R.; Mills, J.L.; Ricco, J.B.; Suresh, K.R.; Murad, M.H. Global vascular guidelines on the management of chronic limb-threatening ischemia. J. Vasc. Surg. 2019, 69, 3S–125S.e140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pearson, G.J.; Thanassoulis, G.; Anderson, T.J.; Barry, A.R.; Couture, P.; Dayan, N.; Francis, G.A.; Genest, J.; Grégoire, J.; Grover, S.A.; et al. 2021 Canadian Cardiovascular Society Guidelines for the Management of Dyslipidemia for the Prevention of Cardiovascular Disease in Adults. Can. J. Cardiol. 2021, 37, 1129–1150. [Google Scholar] [CrossRef] [PubMed]
- Arocha Rodulfo, J.I. Sedentary lifestyle a disease from xxi century. Clin. Investig. Arterioscler. Publ. Of. Soc. Esp. Arterioscler. 2019, 31, 233–240. [Google Scholar] [CrossRef]
- Naumann, S.; Schweiggert-Weisz, U.; Eglmeier, J.; Haller, D.; Eisner, P. In Vitro Interactions of Dietary Fibre Enriched Food Ingredients with Primary and Secondary Bile Acids. Nutrients 2019, 11, 1424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maezaki, Y.; Tsuji, K.; Nakagawa, Y.; Kawai, Y.; Akimoto, M.; Tsugita, T.; Takekawa, W.; Terada, A.; Hara, H.; Mitsuoka, T. Hypocholesterolemic Effect of Chitosan in Adult Males. Biosci. Biotechnol. Biochem. 1993, 57, 1439–1444. [Google Scholar] [CrossRef]
- Pan, H.; Yang, Q.; Huang, G.; Ding, C.; Cao, P.; Huang, L.; Xiao, T.; Guo, J.; Su, Z. Hypolipidemic effects of chitosan and its derivatives in hyperlipidemic rats induced by a high-fat diet. Food Nutr. Res. 2016, 60, 31137. [Google Scholar] [CrossRef] [Green Version]
- Choi, C.R.; Kim, E.K.; Kim, Y.S.; Je, J.Y.; An, S.H.; Lee, J.D.; Wang, J.H.; Ki, S.S.; Jeon, B.T.; Moon, S.H.; et al. Chitooligosaccharides decreases plasma lipid levels in healthy men. Int. J. Food Sci. Nutr. 2012, 63, 103–106. [Google Scholar] [CrossRef]
- Caffall, K.H.; Mohnen, D. The structure, function, and biosynthesis of plant cell wall pectic polysaccharides. Carbohydr. Res. 2009, 344, 1879–1900. [Google Scholar] [CrossRef]
- Naveed, M.; Phil, L.; Sohail, M.; Hasnat, M.; Baig, M.; Ihsan, A.U.; Shumzaid, M.; Kakar, M.U.; Mehmood Khan, T.; Akabar, M.D.; et al. Chitosan oligosaccharide (COS): An overview. Int. J. Biol. Macromol. 2019, 129, 827–843. [Google Scholar] [CrossRef]
- Swiatkiewicz, S.; Swiatkiewicz, M.; Arczewska-Wlosek, A.; Jozefiak, D. Chitosan and its oligosaccharide derivatives (chito-oligosaccharides) as feed supplements in poultry and swine nutrition. J. Anim. Physiol. Anim. Nutr. 2015, 99, 1–12. [Google Scholar] [CrossRef]
- Zhang, J.; Xia, W.; Liu, P.; Cheng, Q.; Tahirou, T.; Gu, W.; Li, B. Chitosan modification and pharmaceutical/biomedical applications. Mar. Drugs 2010, 8, 1962–1987. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ngo, D.H.; Kim, S.K. Antioxidant effects of chitin, chitosan, and their derivatives. Adv. Food Nutr. Res. 2014, 73, 15–31. [Google Scholar] [CrossRef] [PubMed]
- Riaz Rajoka, M.S.; Zhao, L.; Mehwish, H.M.; Wu, Y.; Mahmood, S. Chitosan and its derivatives: Synthesis, biotechnological applications, and future challenges. Appl. Microbiol. Biotechnol. 2019, 103, 1557–1571. [Google Scholar] [CrossRef] [PubMed]
- Chiu, C.Y.; Yen, T.E.; Liu, S.H.; Chiang, M.T. Comparative Effects and Mechanisms of Chitosan and Its Derivatives on Hypercholesterolemia in High-Fat Diet-Fed Rats. Int. J. Mol. Sci. 2019, 21, 92. [Google Scholar] [CrossRef] [Green Version]
- Tong, A.J.; Hu, R.K.; Wu, L.X.; Lv, X.C.; Li, X.; Zhao, L.N.; Liu, B. Ganoderma polysaccharide and chitosan synergistically ameliorate lipid metabolic disorders and modulate gut microbiota composition in high fat diet-fed golden hamsters. J. Food Biochem. 2020, 44, e13109. [Google Scholar] [CrossRef]
- Dos Reis, I.G.M.; Martins, L.E.B.; de Araujo, G.G.; Gobatto, C.A. Forced Swim Reliability for Exercise Testing in Rats by a Tethered Swimming Apparatus. Front. Physiol. 2018, 9, 1839. [Google Scholar] [CrossRef] [Green Version]
- Gonçalves, R.P.; Ferreira, W.H.; Gouvêa, R.F.; Andrade, C.T. Effect of Chitosan on the Properties of Electrospun Fibers From Mixed Poly(Vinyl Alcohol)/ Chitosan Solutions. Mater. Res. 2017, 20, 984–993. [Google Scholar] [CrossRef]
- Shi, P.; Chen, J.; Lin, J.; Zhang, L. High-throughput fat quantifications of hematoxylin-eosin stained liver histopathological images based on pixel-wise clustering. Sci. China Inf. Sci. 2017, 60, 092108. [Google Scholar] [CrossRef]
- Jull, A.B.; Ni Mhurchu, C.; Bennett, D.A.; Dunshea-Mooij, C.A.; Rodgers, A. Chitosan for overweight or obesity. Cochrane Database Syst. Rev. 2008, 16, CD003892. [Google Scholar] [CrossRef]
- Trivedi, V.R.; Satia, M.C.; Deschamps, A.; Maquet, V.; Shah, R.B.; Zinzuwadia, P.H.; Trivedi, J.V. Single-blind, placebo controlled randomised clinical study of chitosan for body weight reduction. Nutr. J. 2016, 15, 3. [Google Scholar] [CrossRef] [Green Version]
- Tungland, B.C.; Meyer, D. Nondigestible Oligo- and Polysaccharides (Dietary Fiber): Their Physiology and Role in Human Health and Food. Compr. Rev. Food Sci. Food Saf. 2002, 1, 90–109. [Google Scholar] [CrossRef] [PubMed]
- Razdan, A.; Pettersson, D. Effect of chitin and chitosan on nutrient digestibility and plasma lipid concentrations in broiler chickens. Br. J. Nutr. 1994, 72, 277–288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yao, H.T.; Chiang, M.T. Plasma lipoprotein cholesterol in rats fed a diet enriched in chitosan and cholesterol. J. Nutr. Sci. Vitaminol. 2002, 48, 379–383. [Google Scholar] [CrossRef] [PubMed]
- Xu, G.; Huang, X.; Qiu, L.; Wu, J.; Hu, Y. Mechanism study of chitosan on lipid metabolism in hyperlipidemic rats. Asia Pac. J. Clin. Nutr. 2007, 16 (Suppl. 1), 313–317. [Google Scholar]
- Wang, D.; Han, J.; Yu, Y.; Li, X.; Wang, Y.; Tian, H.; Guo, S.; Jin, S.; Luo, T.; Qin, S. Chitosan oligosaccharide decreases very-low-density lipoprotein triglyceride and increases high-density lipoprotein cholesterol in high-fat-diet-fed rats. Exp. Biol. Med. 2011, 236, 1064–1069. [Google Scholar] [CrossRef]
- Liu, S.-H.; Cai, F.-Y.; Chiang, M.-T. Long-Term Feeding of Chitosan Ameliorates Glucose and Lipid Metabolism in a High-Fructose-Diet-Impaired Rat Model of Glucose Tolerance. Mar. Drugs 2015, 13, 7302–7313. [Google Scholar] [CrossRef] [Green Version]
- Muscella, A.; Stefàno, E.; Lunetti, P.; Capobianco, L.; Marsigliante, S. The Regulation of Fat Metabolism During Aerobic Exercise. Biomolecules 2020, 10, 1699. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group (n = 8) | Systemic State | Oral Treatment | Physical Exercise |
|---|---|---|---|
| CTR | Normolipidemic | Distilled water | - |
| Hyp | Hyperlipidemic | Distilled water | - |
| Hyp–Ch | Hyperlipidemic | Chitosan | - |
| Hyp–Ex | Hyperlipidemic | Distilled water | Forced swimming |
| Hyp–ChEx | Hyperlipidemic | Chitosan | Forced swimming |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Passos, J.P.G.; Melo, C.R.; Carvalho, F.M.A.; Severino, P.; Cardoso, J.C.; Cunha, J.L.S.; Cano, A.; Souto, E.B.; de Albuquerque-Júnior, R.L.C. Combined Therapy of Chitosan and Exercise Improves the Lipid Profile, Adipose Tissue and Hepatic Alterations in an In Vivo Model of Induced-Hyperlipidemia. Nutraceuticals 2022, 2, 116-131. https://doi.org/10.3390/nutraceuticals2020009
Passos JPG, Melo CR, Carvalho FMA, Severino P, Cardoso JC, Cunha JLS, Cano A, Souto EB, de Albuquerque-Júnior RLC. Combined Therapy of Chitosan and Exercise Improves the Lipid Profile, Adipose Tissue and Hepatic Alterations in an In Vivo Model of Induced-Hyperlipidemia. Nutraceuticals. 2022; 2(2):116-131. https://doi.org/10.3390/nutraceuticals2020009
Chicago/Turabian StylePassos, João P. G., Carlisson R. Melo, Felipe M. A. Carvalho, Patricia Severino, Juliana C. Cardoso, John L. S. Cunha, Amanda Cano, Eliana B. Souto, and Ricardo L. C. de Albuquerque-Júnior. 2022. "Combined Therapy of Chitosan and Exercise Improves the Lipid Profile, Adipose Tissue and Hepatic Alterations in an In Vivo Model of Induced-Hyperlipidemia" Nutraceuticals 2, no. 2: 116-131. https://doi.org/10.3390/nutraceuticals2020009