Multiple-Micronutrient Fortified Non-Dairy Beverage Interventions Reduce the Risk of Anemia and Iron Deficiency in School-Aged Children in Low-Middle Income Countries: A Systematic Review and Meta-Analysis (i–iv)

Abstract
:1. Introduction
2. Methods
2.1. Search Strategy

{kind=link}
| Step | Search Strategy 1 1 | Search Strategy 2 1 |
|---|---|---|
| 1 | “beverages” [MeSH] 2 NOT “milk” [MeSH] | Beverage * 3 [TIAB] 4 NOT milk * [TIAB] |
| 2 | “food, fortified” [MeSH] | Fortif * [TIAB] |
| 3 | 1 AND 2 | 1 AND 2 |
| 4 | “beverages” [MeSH] NOT “milk” [MeSH] | Beverage * [TIAB] NOT milk * [TIAB] |
| 5 | “micronutrients” [MeSH] | Micronutrient * [TIAB] OR vitamin * [TIAB] or mineral * [TIAB] OR iron [TIAB] OR vitamin A [TIAB] OR zinc [TIAB] |
| 6 | 4 AND 5 | 4 AND 5 |
| 7 | 3 OR 6 | 3 OR 6 |
2.2. Study Eligibility Criteria
2.3. Statistical Analyses
2.4. Assessment of Heterogeneity, Sensitivity, and Risk of Bias
3. Results
3.1. Search Results and Study Characteristics
3.2. Methodological Quality
| Reference | Population | Intervention | Control | Duration | Outcomes | Main Results |
|---|---|---|---|---|---|---|
| Aaron et al., 2011[17] | Country: Nigeria Geography: rural Population: M and F 5–13 years (n = 566) Exclusion criteria: Hb < 70 g/L, signs of acute illness | RTC beverage fortified with: 11 vitamins, 12 minerals, and bioflavonoids | Iso-caloric non-fortified beverage | 6 months | Hb, ferritin, retinol, zinc, anthropometry, and cognitive performance | Change in Hb, retinol and zinc significantly greater in fortified group. No significant difference between groups in Hb, ferritin, anthropometry, or cognitive performance. |
| Abrams et al., 2003[18] | Country: Botswana Geography: urban Population: M and F 5–11 years (n = 311) Exclusion criteria: Hb ≤ 60 g/L, weight ≤ 15 kg, known chronic or acute illness | Beverage reconstituted from powder fortified with: 8 vitamins and 4 minerals | Iso-caloric non-fortified beverage reconstituted from powder | 8 weeks | Hb, ferritin, transferrin receptors, retinol, vitamin B12, folate, riboflavin, zinc, anthropometry | Change in Hb, ferritin, folate and riboflavin; final transferrin receptors, zinc adequacy, and anthropometry significantly greater in fortified group. No significant difference between groups in retinol or vitamin B12. |
| Angeles-Agdeppa et al. 2011[10] | Country: Philippines Geography: urban Age: M and F 6-9 years (n = 100) Exclusion criteria: Hb > 120 g/L or Hb < 70 g/L, WAZ < −3), acute illness | RTC beverage fortified with: 2 vitamins, 2 minerals, and lysine. | Iso-caloric beverage fortified only with Vitamin C | 100 days | Hb, ferritin, zinc, anthropometry, adequacy of energy and nutrient intake | Change in Hb and zinc significantly greater in fortified group. No significant difference in ferritin or anthropometry. |
| Ash et al., 2003[19] | Country: Tanzania Geography: rural Population: M and F 6–11 years (n = 830) Exclusion criteria: ocular signs of xerophthalmia, Hb < 70 g/L, serious chronic disease | Beverage reconstituted from powder fortified with: 7 vitamins and 3 minerals | Iso-caloric non-fortified beverage reconstituted from powder | 6 months | Hb, ferritin, erythrocyte protoporphyrin, retinol, anthropometry | Change in all measured biochemical and anthropometric indices significantly greater in fortified group. |
| Hyder et al., 2007[15] | Country: Bangladesh Geography: rural Population: F 12 ± 1.9 years (n = 1125) Exclusion criteria: Hb < 70 g/L, night blindness, goiter, acute illness | Beverage reconstituted from powder fortified with: 8 vitamins and 3 minerals | Iso-caloric non-fortified beverage powder | 6 months | Hb, ferritin, retinol, zinc, anthropometry | Change in Hb, ferritin, retinol, and anthropometry significantly greater in fortified group from 0–6 months, but not from 6–12 months. No significant difference between groups in zinc. |
| Makola et al., 2003[21] | Country: Tanzania Geography: rural Population: pregnant women (n = 439) Exclusion criteria: Gestation <12 or > 34 weeks, Hb <80 g/L, serious medical condition or pregnancy complication | Beverage reconstituted from powder fortified with: 8 vitamins and 3 minerals | Iso-caloric non-fortified beverage powder for home reconstitution | 8 weeks | Hb, ferritin, retinol, thyroid stimulating hormone | Change in Hb and ferritin significantly greater in fortified group. No significant difference between groups in retinol and thyroid stimulating hormone. |
| Solon et al., 2003[20] | Country: Philippines Geography: urban Age: M and F grade 1–6, mean age 9.9 ± 2.2 years (n = 831) Exclusion criteria: Hb ≤ 80 g/L | Beverage reconstituted from powder fortified with: 8 vitamins and 3 minerals | Iso-caloric non-fortified beverage reconstituted from powder | 16 weeks | Hb, urinary iodine, anthropometry, physical fitness, cognitive performance | Change in iodine significantly greater in fortified group. No significant difference between groups in Hb, anthropometry, physical fitness, or cognitive performance. |
| Taljaard et al., 2013[14] | Country: South Africa Geography: peri-urban Age: M and F 6–11 years (n = 414) Exclusion criteria: health condition precluding cognitive testing, medication or supplement use | Beverage reconstituted from powder fortified with: 8 vitamins and 4 minerals (with or without nutritive sweetener; group receiving sweetened beverage included in meta-analysis) | Iso-caloric non-fortified beverage reconstituted from powder (with or without nutritive sweetener; group receiving sweetened beverage included in meta-analysis) | 8.5 months | Hb, ferritin, transferrin receptors, zinc protoporphyrin, retinol, zinc, anthropometry, cognitive performance | Change in Hb, ferritin, zinc protoporphyrin, and some cognitive performance indicators significantly greater in MMN fortified groups; MMN groups w/ significantly decreased odds of iron deficiency. No significant difference between groups in transferrin receptors, retinol or zinc. |
| Thankachan et al., 2012[11] | Country: India Geography: urban Population: M and F 6–12 years (n = 246) Exclusion criteria: Hb < 80 g/L, chronic illness, physical handicaps, WAZ or HAZ < −3 | Beverage reconstituted from powder fortified with: 5 vitamins and 2 minerals | Iso-caloric non-fortified beverage reconstituted from powder | 8 weeks | Hb, ferritin, transferrin receptors, zinc protoporphyrin, retinol, zinc, vitamin B12, RBC folate, body iron stores, vitamin C, anthropometry, morbidity | Change in Hb, ferritin, transferrin receptors, zinc protoporphyrin, retinol, vitamin B12, folate, body iron stores and vitamin C significantly greater in fortified group. No significant difference between groups in zinc, anthropometry, or morbidity. |
| Vaz et al., 2011[13] | Country: India Geography: urban Population: M and F 7–10.5 years (n = 190) Exclusion criteria: Hb < 80 g/L, cardiovascular or respiratory disease, physical disability, recent history of serious infections, surgery, or injuries, nutritional supplements use | Beverage reconstituted from powder fortified with: 11 vitamins and 6 minerals | Iso-caloric non-fortified beverage reconstituted from powder, non-intervention control (placebo control only included in meta-analysis) | 4 months | Ferritin, transferrin receptors, vitamin B12, vitamin C, RBC thiamin, folate, and riboflavin, pyridoxal phosphate, niacin, aerobic capacity, whole body endurance | Change in ferritin, transferrin receptors, vitamin B12, vitamin C, pyridoxal phosphate, RBC thiamin, folate, and riboflavin, aerobic capacity, and whole body endurance significantly greater in fortified group. No significant difference between groups in niacin. |
| Author, year | Adequate Sequence Generation? | Adequate Allocation Concealment? | Blinding | Loss to Follow-Up | Intention to Treat Analysis? | Free of Selective Reporting? | Other Bias? | Comments | Grade |
|---|---|---|---|---|---|---|---|---|---|
| Aaron, 2011 [17] | Yes, groups stratified proportionate to number of students in each school and class level | Yes, beverages identical in taste and appearance | Double blind, placebo controlled | 6% (n = 32) due to relocation or school withdrawal | Yes | Yes | 2 schools | Beverage contained maize, soy isolate and bioflavonoids in addition to MMN, de-worming 1 month prior to end point per school policy | High |
| Abrams, 2003[18] | No, students in 2 schools assigned to intervention and control groups, respectively | Yes, beverages identical in flavor and appearance | Double blind, placebo controlled | 15% (n = 44), reasons for loss not stated | Yes | Yes | Lack of participant-level randomization | β-carotene rather than retinol as source of vitamin A, short (8 week) intervention period | Moderate (inadequate sequence generation) |
| Angeles-Agdeppa, 2011[10] | Detailed method not stated. | Not stated directly, beverages provided in foil packs | Double blind placebo controlled | 11% (n = 11) due to relocation, school change, or absence during data collection | Not stated | Yes | Low (method of randomization not reported, all children moderately anemic at baseline) | ||
| Ash, 2003[19] | Method not stated, students stratified by median Hb prior to randomization | Yes, beverages identical in taste and appearance | Double blind, placebo controlled | 7% (n = 56) due to poor attendance, leaving school, refusing venipuncture | Yes | Yes | Baseline ferritin differed significantly between groups | -- | Moderate (method of randomization not reported) |
| Hyder, 2007[15] | Yes , random # assigned to participants, groups defined as even and odd | Yes, beverages identical in weight, color, flavor and appearance | Double blind, placebo controlled | 12% (n = 136) due to missing data, illness, refusal | Yes | Yes | Parasitic infection not measured, analysis involved females only | Energy content of intervention/placebo not reported, target population adolescent girls, 0-6 month intervention period included in meta-analysis | Moderate (included F only so not generalizable) |
| Makola, 2003[21] | Yes, block randomization (10 subjects per block) at each of 6 study centers | Yes, beverages identical in appearance, color and taste and packaged similarly | Double blind, placebo controlled | 41% (n = 180) due to logistic problems, early delivery | Not stated | Yes | 2nd–3rd trimester pregnant women included, short (8 week) intervention period. Variable simultaneous use of iron/folic acid supplements | Moderate (high loss to follow-up) | |
| Solon, 2003[20] | Not stated, students randomized into 4 groups (2*2, beverage*de-worming tablets) | Yes, beverages indistinguishable in appearance, smell, and taste | Double blind, placebo controlled | 5% (n = 43), reasons not described | Not stated | Yes | Approximately half of subjects in fortified and placebo beverage group received de-worming treatment. | Effects on micronutrient status other than iron and iodine not reported. All participants included in meta-analysis by beverage group. | Moderate (method of randomization not reported) |
| Taljaard, 2013[14] | Not stated, randomisation to 4 groups (2*2 MMN*sugar) by school, classroom, and gender | Yes, beverages identical in color and taste. | Double blind, placebo controlled | 3.9% (n = 16) due to leaving school | Not stated | Yes | Only iso-caloric MMN + sugar and sugar only interventions included in meta-analysis. De-worming prior to intervention | High | |
| Thankachan, 2012[11] | Yes, block randomization with a computer-generated list in blocks of 20 | Yes, beverages identical in color, size, and taste | Double blind, placebo controlled | 1% (n = 3) due to prolonged school absence or refusal of blood draw | Not stated | Yes | Included only participants who were iron deficient at baseline (serum ferritin < 45 pmol/L) | Short (8 week) intervention period | Moderate (included only iron-deficient participants, not generalizable) |
| Vaz, 2011[13] | Yes, block randomization using computer generated sequence into 3 arms (MMN fortified, unfortified, and no beverage) | Not stated, MMN fortified and unfortified beverages both choco-malt | Double blind placebo controlled | 4% (n = 13) due to withdrawal of consent | Yes | Yes | Baseline ferritin differed significantly between MMN fortified and unfortified beverage groups | Only iso-caloric MMN fortified and unfortified interventions included in meta-analysis | Moderate (allocation concealment not reported directly) |
| Quality Assessment | Summary of Findings | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| No. Studies | I2 (%) | Heterogeneity | Generalizable to Population of Interest? | Generalizable to Intervention of Interest? | Other Sources of Bias (e.g., Major Limitations in Study Design) | No. Participants | Publication Bias r (p-value) | Effect Estimate | |
| Hemoglobin (g/L): Overall quality of evidence grade = moderate | |||||||||
| 8 | 92 | 6 of 8 studies found significantly greater increase in Hb in intervention group. Other studies found no difference between groups. | 7 of 8 studies conducted in M and F school age children in lower-income countries. 1 study in F adolescents in Bangladesh. | Variability in micronutrient composition, dose, and duration. Reconstituted powder used in 6 of 8 studies. | Study w/highest iron dose found no difference between groups, several randomized by school, de-worming protocols inconsistent. | 3835 | 0.25 (0.56) | 2.76 [1.19, 4.33] | |
| Ferritin (pmol/L): Overall quality of evidence grade = moderate | |||||||||
| 8 | 95 | 6 of 8 studies found significantly greater increase in ferritin in intervention group. Other studies found no significant difference between groups. | 7 of 8 studies conducted in M and F school age children in lower-income countries. 1 study in F adolescents in Bangladesh. | Variability in micronutrient composition, dose, and duration. Reconstituted powder used in 6 of 8 studies. | Study w/highest iron dose found no difference between groups, baseline ferritin differed in 1 study, several randomized by school, de-worming protocols inconsistent. | 3891 | 0.94 (0.004) | 15.42 [5.73, 25.12] | |
| Retinol (µmol/L): Overall quality of evidence grade = low | |||||||||
| 5 | 61 | 3 of 5 studies found significantly greater increase in retinol in intervention group. Other studies found no significant difference between groups. | 4 of 5 studies conducted in M and F school age children in lower-income countries. 1 study in F adolescents in Bangladesh. | Variability in micronutrient composition, dose, and duration. Reconstituted powder used in 4 of 5 studies. | Randomization method unclear or at school level in some studies, de-worming protocols inconsistent. | 2049 | 0.30 (0.62) | 0.05 [−0.03, 0.13] | |
| Zinc (µmol/L): Overall quality of evidence grade = low | |||||||||
| 4 | 75 | 2 of 4 studies found significantly greater increase in zinc in intervention group. Other studies found no significant difference between groups. | 3 of 4 studies conducted in M and F school age children in lower-income countries. 1 study in F adolescents in Bangladesh. | Variability in micronutrient composition, dose, and duration. Reconstituted powder used in 2 of 4 studies. | Randomization method not explicit in 2 studies, de-worming protocols inconsistent. | 1690 | 0.09 (0.91) | 0.92 [−1.45, 3.30] | |
| Vitami n B12 (pmol/L): Overall quality of evidence grade = very low | |||||||||
| 3 | 99 | 2 of 3 studies found significantly greater increase in vitamin B12 in intervention group. Other study found no differences between groups. | All studies conducted in M and F school children in lower-income countries. | Variability in micronutrient composition, dose, and duration. Reconstituted powder used in all studies | One study randomized by school, infection and/or parasites not treated or measured consistently. | 644 | 0.91 (0.27) | 96.2 [−142.2, 334.6] | |
| Weight (kg): Overall quality of evidence grade = moderate | |||||||||
| 6 | 85 | 3 of 6 studies found significantly greater increase in vitamin B12 in intervention group. Other studies found no differences between groups. | 5 of 6 studies conducted in M and F school age children in lower-income countries. 1 study in F adolescents in Bangladesh. | Variability in micronutrient composition, dose, and duration. Reconstituted powder used in all studies. | Randomization method unclear or at school level in 4 studies, de-worming protocols inconsistent. | 2977 | 0.04 (0.94) | 0.30 [0.01,0.58] | |
| Height (cm): Overall quality of evidence grade = moderate | |||||||||
| 5 | 78 | 2 of 5 studies found significantly greater increase in vitamin B12 in intervention group. Other studies found no differences between groups. | 4 of 5 studies conducted in M and F school age children in lower-income countries. 1 study in F adolescents in Bangladesh. | Variability in micronutrient composition, dose, and duration. Reconstituted powder used in 4 of 5 studies. | Randomization not outlined specifically in 3 studies, de-worming protocols inconsistent. | 2697 | 0.12 (0.85) | 0.17 [−0.16, 0.50] | |
| Weight-for-age (Z): Overall quality of evidence grade = low | |||||||||
| 4 | 59 | 2 of 4 studies found significantly greater increase in vitamin B12 in intervention group. Other studies found no differences between groups. | All studies conducted in M and F school children in lower-income countries. | Variability in micronutrient composition, dose, and duration. Reconstituted powder used in 3 of 4 studies. | Method of randomization not specific or at school level in all studies, de-worming protocols inconsistent. | 1385 | 0.65 (0.35) | 0.028 [−0.06, 0.12] | |
| Height-for-age (Z): Overall quality of evidence grade=moderate | |||||||||
| 3 | 0 | No significant differences found between groups | All studies conducted in M and F school children in lower-income countries. | Variability in micronutrient composition, dose, and duration. Reconstituted powder used in 2 of 3 studies. | Method of randomization not specific or at school level in all studies, de-worming protocols inconsistent. | 1124 | 0.10 (0.94) | 0.0 [−0.05, 0.05] | |
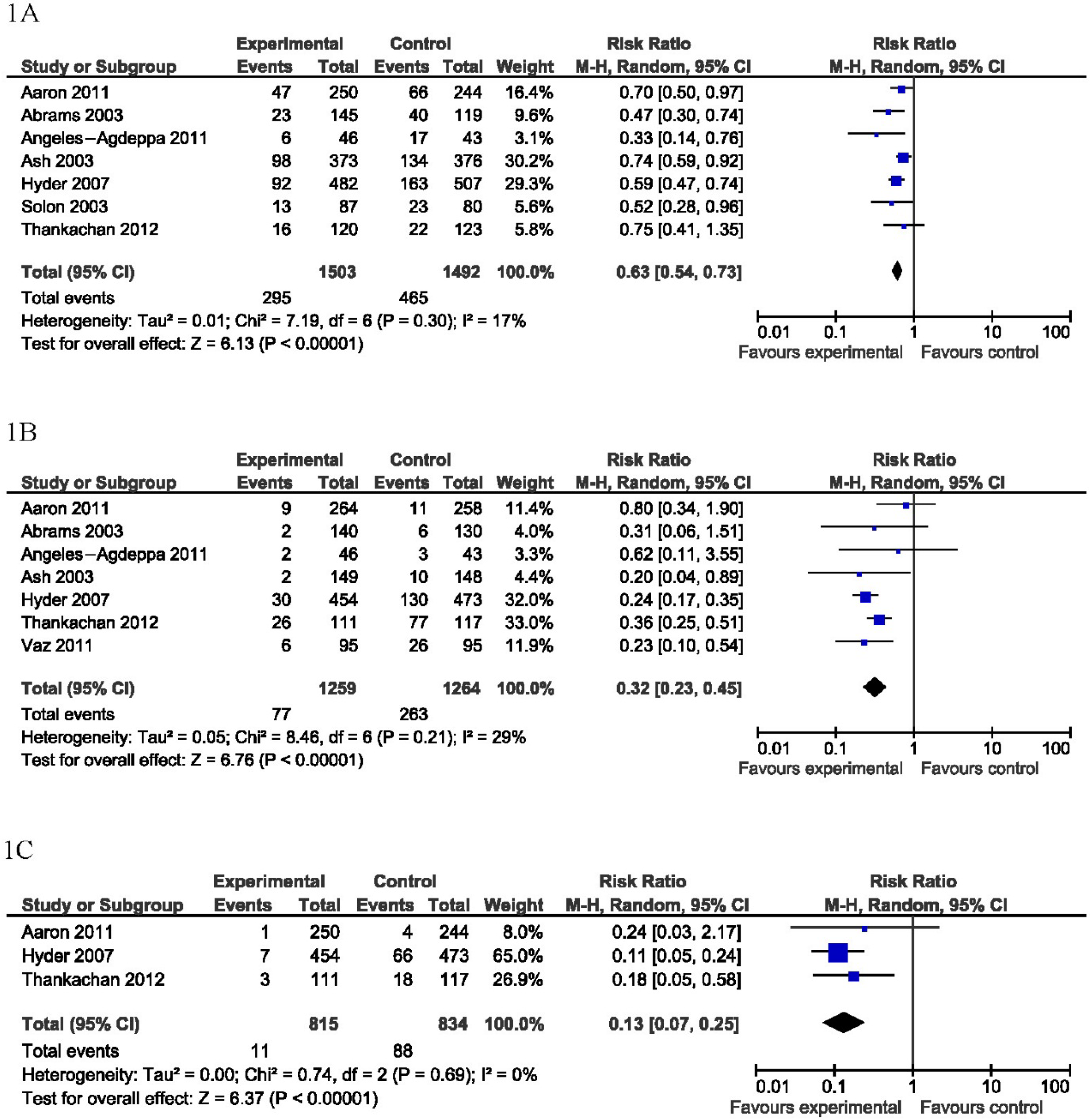
| Anemia (Hb < 110–120 g/L): Overall quality of evidence grade = moderate | |||||||||
| 6 | 84 | 5 of 6 studies found significantly greater reduction in endpoint prevalence of anemia in intervention vs. control group. | 5 of 6 studies conducted in M and F children in lower-income countries. 1 study in F adolescents in Bangladesh. | Variability in micronutrient composition, dose, and duration. Reconstituted powder used in 4 of 6 studies. | Method of randomization not specific or at school level in 3 studies, de-worming protocols inconsistent. Study w/highest iron dose only to find no significant difference between groups in anemia reduction. | 2828 | 0.24 (0.64) | RR 0.63 [0.54, 0.73] | |
| Iron deficiency (ferritin < 27–45 pmol/L): Overall quality of evidence grade = moderate | |||||||||
| 7 | 96 | 4 of 7 studies found significantly greater reduction in endpoint prevalence of iron deficiency in intervention vs. control group | 6 of 7 studies conducted in M and F children in lower-income countries. 1 study in F adolescents in Bangladesh. | Variability in micronutrient composition, dose, and duration. Reconstituted powder used in 5 of 7 studies. | Method of randomization not specific or at school level in 3 studies, de-worming protocols inconsistent. | 2523 | 0.23 (0.62) | RR 0.32 [0.23,0.45] | |
| Iron deficiency anemia (Hb < 110–120 g/L and ferritin < 27–45 pmol/L): Overall quality of evidence grade = low | |||||||||
| 3 | 97 | 2 of 3 studies found significantly greater reduction in endpoint prevalence of IDA in intervention vs. control group. | 2 of 3 studies conducted in M and F children in lower-income countries. 1 study in F adolescents in Bangladesh. | Variability in micronutrient composition, dose, and duration. Reconstituted powder used in2 of 3 studies. | De-worming protocols inconsistent. | 1649 | 0.88 (0.31) | RR 0.13 [0.07,0.25] | |
3.3. Meta-Analysis

4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Supplementary Files
Conflicts of Interest
References
- Allen, L.H.; Peerson, J.M.; Olney, D.K. Provision of multiple rather than two or fewer micronutrients more effectively improves growth and other outcomes in micronutrient-deficient children and adults. J. Nutr. 2009, 139, 1022–1030. [Google Scholar] [CrossRef] [PubMed]
- Bhutta, Z.; Salam, R. Global nutrition epidemiology and trends. Annu. Nutr. Metab. 2012, 61, 19–27. [Google Scholar] [CrossRef]
- Guerrant, R.L.; Lima, A.A.M.; Davidson, F. Micronutrients and infection: Interactions and implications with enteric and other infections and future priorities. J. Infect. Dis. 2000, 182, S134–S138. [Google Scholar] [CrossRef] [PubMed]
- Black, R.E.; Victora, C.G.; Walker, S.P.; Bhutta, Z.A.; Christian, P.; de Onis, M.; Ezzati, M.; Grantham-McGregor, S.; Katz, J.; Martorell, R.; et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet 2013, 382, 427–451. [Google Scholar] [CrossRef] [PubMed]
- Olney, D.K.; Rawat, R.; Ruel, M.T. Identifying potential programs and platforms to deliver multiple micronutrient interventions. J. Nutr. 2012, 142, 178S–185S. [Google Scholar] [CrossRef] [PubMed]
- Allen, L.H.; de Benoist, B.; Dary, O.; Hurrell, R. Guidelines on Food Fortification with Micronutrients; Allen, L.H., de Benoist, B., Dary, O., Hurrell, R., Eds.; World Health Organization (WHO) and Food and Agricultural Organization (FAO): Geneva, Switzerland, 2006. [Google Scholar]
- Bhutta, Z.A.; Das, J.K.; Rizvi, A.; Gaffey, M.F.; Walker, N.; Horton, S.; Webb, P.; Lartey, A.; Black, R.E. Evidence-based interventions for improvement of maternal and child nutrition: What can be done and at what cost? Lancet 2013, 382, 452–477. [Google Scholar] [CrossRef] [PubMed]
- Brown, K.H.; Rivera, J.A.; Bhutta, Z.; Gibson, R.S.; King, J.C.; Lonnerdal, B.; Ruel, M.T.; Sandtrom, B.; Wasantwisut, E.; Hotz, C.; et al. International zinc nutrition consultative group (izincg) technical document #1. Assessment of the risk of zinc deficiency in populations and options for its control. Food Nutr. Bull. 2004, 25, S99–S203. [Google Scholar] [PubMed]
- Horton, S.; Mannar, V.; Wesley, A. Food Fortification with Iron and Iodine. Copengagen Consensus Best Practice Paper 2008. Available online: http://www.Copenhagenconsensus.Com/sites/default/files/bpp_fortification.Pdf (accessed on 25 February 2015).
- Angeles-Agdeppa, I.; Magsadia, C.; Capanzana, M. Fortified juice drink improved iron and zinc status of schoolchildren. Asia Pac. J. Clin. Nutr. 2011, 20, 535–543. [Google Scholar] [PubMed]
- Thankachan, P.; Selvam, S.; Surendran, D.; Chellan, S.; Pauline, M.; Abrams, S.A.; Kurpad, A.V. Efficacy of a multi micronutrient-fortified drink in improving iron and micronutrient status among schoolchildren with low iron stores in india: A randomised, double-masked placebo-controlled trial. Eur. J. Clin. Nutr. 2013, 67, 36–41. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.; Huffman, S.L. Review of fortified food and beverage products for pregnant and lactating women and their impact on nutritional status. Mater. Child Nutr. 2011, 7, 19–43. [Google Scholar] [CrossRef]
- Vaz, M.; Pauline, M.; Unni, U.S.; Parikh, P.; Thomas, T.; Bharathi, A.V.; Avadhany, S.; Muthayya, S.; Mehra, R.; Kurpad, A.V. Micronutrient supplementation improves physical performance measures in asian indian school-age children. J. Nutr. 2011, 141, 2017–2023. [Google Scholar] [CrossRef] [PubMed]
- Taljaard, C.; Covic, N.M.; van Graan, A.E.; Kruger, H.S.; Smuts, C.M.; Baumgartner, J.; Kvalsvig, J.D.; Wright, H.H.; van Stuijvenberg, M.E.; Jerling, J.C. Effects of a multi-micronutrient-fortified beverage, with and without sugar, on growth and cognition in south african schoolchildren: A randomised, double-blind, controlled intervention. Br. J. Nutr. 2013, 110, 2271–2284. [Google Scholar] [CrossRef] [PubMed]
- Hyder, S.M.; Haseen, F.; Khan, M.; Schaetzel, T.; Jalal, C.S.; Rahman, M.; Lonnerdal, B.; Mannar, V.; Mehansho, H. A multiple-micronutrient-fortified beverage affects hemoglobin, iron, and vitamin a status and growth in adolescent girls in rural bangladesh. J. Nutr. 2007, 137, 2147–2153. [Google Scholar] [PubMed]
- Higgins, J.; Thompson, S.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. Br. Med. J. 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Aaron, G.J.; Kariger, P.; Aliyu, R.; Flach, M.; Iya, D.; Obadiah, M.; Baker, S.K. A multi-micronutrient beverage enhances the vitamin a and zinc status of nigerian primary schoolchildren. J. Nutr. 2011, 141, 1565–1572. [Google Scholar] [CrossRef] [PubMed]
- Abrams, S.A.; Mushi, A.; Hilmers, D.C.; Griffin, I.J.; Davila, P.; Allen, L. A multinutrient-fortified beverage enhances the nutritional status of children in botswana. J. Nutr. 2003, 133, 1834–1840. [Google Scholar] [PubMed]
- Ash, D.M.; Tatala, S.R.; Frongillo, E.A., Jr.; Ndossi, G.D.; Latham, M.C. Randomized efficacy trial of a micronutrient-fortified beverage in primary school children in tanzania. Am. J. Clin. Nutr. 2003, 77, 891–898. [Google Scholar] [PubMed]
- Solon, F.S.; Sarol, J.N., Jr.; Bernardo, A.B.; Solon, J.A.; Mehansho, H.; Sanchez-Fermin, L.E.; Wambangco, L.S.; Juhlin, K.D. Effect of a multiple-micronutrient-fortified fruit powder beverage on the nutrition status, physical fitness, and cognitive performance of schoolchildren in the philippines. Food Nutr. Bull. 2003, 24, 129–140. [Google Scholar]
- Makola, D.; Ash, D.M.; Tatala, S.R.; Latham, M.C.; Ndossi, G.; Mehansho, H. A micronutrient-fortified beverage prevents iron deficiency, reduces anemia and improves the hemoglobin concentration of pregnant tanzanian women. J. Nutr. 2003, 133, 1339–1346. [Google Scholar] [PubMed]
- Best, C.; Neufingerl, N.; Del Rosso, J.M.; Transler, C.; van den Briel, T.; Osendarp, S. Can multi-micronutrient food fortification improve the micronutrient status, growth, health, and cognition of schoolchildren? A systematic review. Nutr. Rev. 2011, 69, 186–204. [Google Scholar] [CrossRef] [PubMed]
- De-Regil, L.M.; Suchdev, P.S.; Vist, G.E.; Walleser, S.; Pena-Rosas, J.P. Home fortification of foods with multiple micronutrient powders for health and nutrition in children under two years of age (review). Evid. Based Child Health 2013, 8, 112–201. [Google Scholar] [CrossRef] [PubMed]
- Adu-Afarwuah, S.; Lartey, A.; Brown, K.H.; Zlotkin, S.; Briend, A.; Dewey, K.G. Randomized comparison of 3 types of micronutrient supplements for home fortification of complementary foods in ghana: Effects on growth and motor development. Am. J. Clin. Nutr. 2007, 86, 412–420. [Google Scholar] [PubMed]
- WHO. Serum Retinol Concentrations for Determining the Prevalence of Vitamin a Deficiency in Populations 2011. Available online: http://www.Who.Int/vmnis/indicators/retinol.Pdf (accessed on 25 February 2015).
- Ramakrishnan, U.; Neufeld, L.M.; Gonzalez-Cossio, T.; Villalpando, S.; Garcia-Guerra, A.; Rivera, J.; Martorell, R. Multiple micronutrient supplements during pregnancy do not reduce anemia or improve iron status compared to iron-only supplements in semirural mexico. J. nutr. 2004, 134, 898–903. [Google Scholar] [PubMed]
- Popkin, B.M.; Armstrong, L.E.; Bray, G.M.; Caballero, B.; Frei, B.; Willett, W.C. A new proposed guidance system for beverage consumption in the united states. Am. J. Clin. Nutr. 2006, 83, 529–542. [Google Scholar] [PubMed]
- De Benoist, B.; MacLean, E.; Egli, I.; Cogswell, M. Worldwide Prevalence of Anaemia 1993–2005: Who Global Database of Anaemia; World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aaron, G.J.; Dror, D.K.; Yang, Z. Multiple-Micronutrient Fortified Non-Dairy Beverage Interventions Reduce the Risk of Anemia and Iron Deficiency in School-Aged Children in Low-Middle Income Countries: A Systematic Review and Meta-Analysis (i–iv). Nutrients 2015, 7, 3847-3868. https://doi.org/10.3390/nu7053847
Aaron GJ, Dror DK, Yang Z. Multiple-Micronutrient Fortified Non-Dairy Beverage Interventions Reduce the Risk of Anemia and Iron Deficiency in School-Aged Children in Low-Middle Income Countries: A Systematic Review and Meta-Analysis (i–iv). Nutrients. 2015; 7(5):3847-3868. https://doi.org/10.3390/nu7053847
Chicago/Turabian StyleAaron, Grant J., Daphna K. Dror, and Zhenyu Yang. 2015. "Multiple-Micronutrient Fortified Non-Dairy Beverage Interventions Reduce the Risk of Anemia and Iron Deficiency in School-Aged Children in Low-Middle Income Countries: A Systematic Review and Meta-Analysis (i–iv)" Nutrients 7, no. 5: 3847-3868. https://doi.org/10.3390/nu7053847