
Longitudinal Associations of Dietary Fiber Intake with Glycated Hemoglobin and Estimated Insulin Sensitivity in Adults with and without Type 1 Diabetes
 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Dietary Data and Glycemic Control
2.2. Statistical Analyses
3. Results
3.1. Baseline and Year 6 Participant Characteristics
3.2. Longitudinal Six-Year Associations of Dietary Fiber Intake with HbA1c and eIS
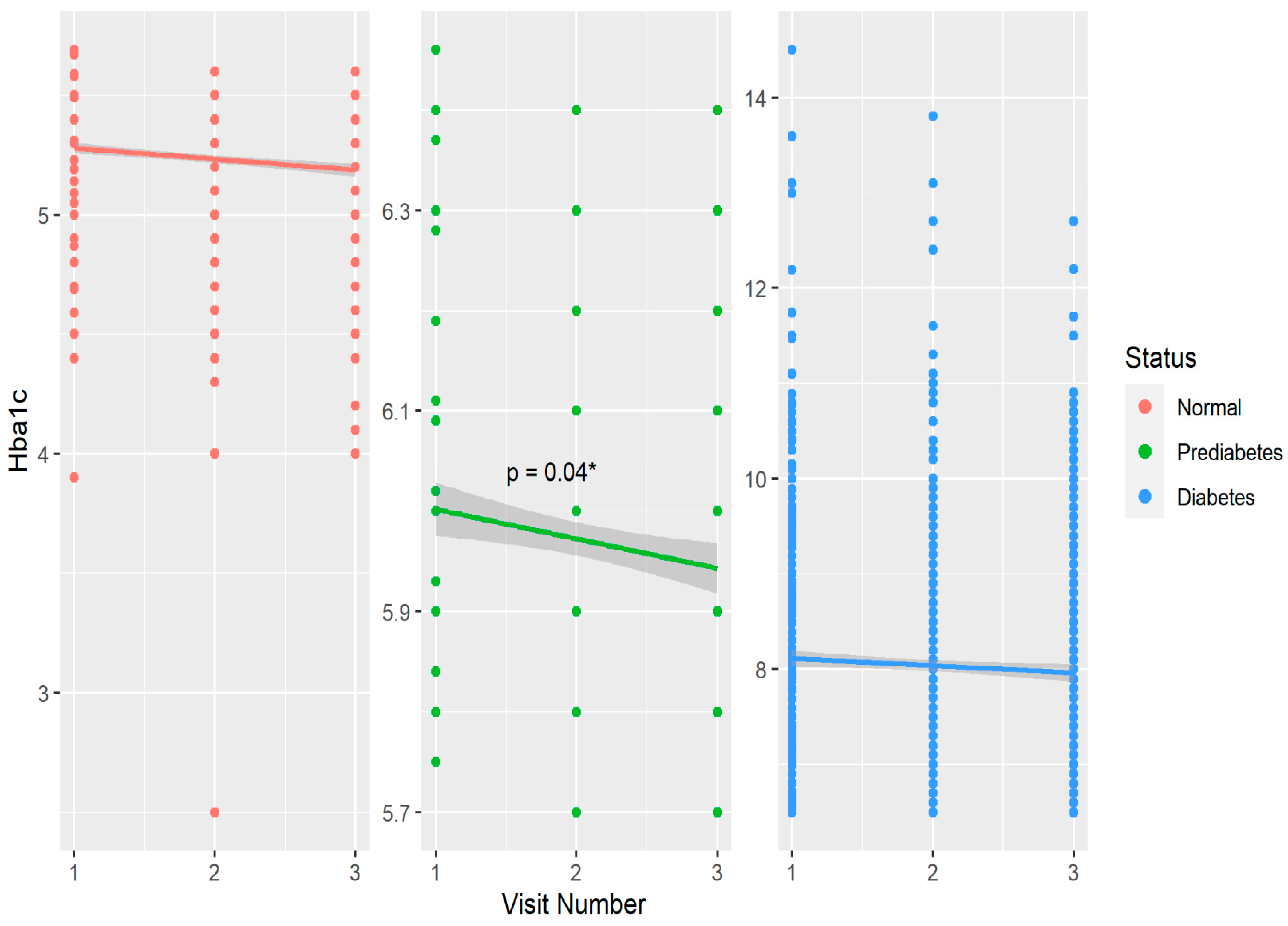
3.3. Longitudinal Six-Year Associations of Dietary Fiber Intake with HbA1c by Glycemic Control
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vanderniet, J.A.; Jenkins, A.J.; Donaghue, K.C. Epidemiology of Type 1 Diabetes. Curr. Cardiol. Rep. 2022, 24, 1455–1465. [Google Scholar] [CrossRef] [PubMed]
- Kohil, A.; Al-Asmakh, M.; Al-Shafai, M.; Terranegra, A. The Interplay Between Diet and the Epigenome in the Pathogenesis of Type-1 Diabetes. Front. Nutr. 2020, 7, 612115. [Google Scholar] [CrossRef] [PubMed]
- Zajec, A.; Trebušak Podkrajšek, K.; Tesovnik, T.; Šket, R.; Čugalj Kern, B.; Jenko Bizjan, B.; Šmigoc Schweiger, D.; Battelino, T.; Kovač, J. Pathogenesis of Type 1 Diabetes: Established Facts and New Insights. Genes 2022, 13, 706. [Google Scholar] [CrossRef] [PubMed]
- Mariño, E.; Richards, J.L.; McLeod, K.H.; Stanley, D.; Yap, Y.A.; Knight, J.; McKenzie, C.; Kranich, J.; Oliveira, A.C.; Rossello, F.J.; et al. Gut microbial metabolites limit the frequency of autoimmune T cells and protect against type 1 diabetes. Nat. Immunol. 2017, 18, 552–562. [Google Scholar] [CrossRef] [PubMed]
- Echouffo-Tcheugui, J.B.; Perreault, L.; Ji, L.; Dagogo-Jack, S. Diagnosis and Management of Prediabetes: A Review. JAMA 2023, 329, 1206–1216. [Google Scholar] [CrossRef] [PubMed]
- Anderson, J.W.; Baird, P.; Davis, R.H., Jr.; Ferreri, S.; Knudtson, M.; Koraym, A.; Waters, V.; Williams, C.L. Health benefits of dietary fiber. Nutr. Rev. 2009, 67, 188–205. [Google Scholar] [CrossRef] [PubMed]
- Chandalia, M.; Garg, A.; Lutjohann, D.; von Bergmann, K.; Grundy, S.M.; Brinkley, L.J. Beneficial effects of high dietary fiber intake in patients with type 2 diabetes mellitus. N. Engl. J. Med. 2000, 342, 1392–1398. [Google Scholar] [CrossRef] [PubMed]
- Dreher, M.L. Whole Fruits and Fruit Fiber Emerging Health Effects. Nutrients 2018, 10, 1833. [Google Scholar] [CrossRef]
- Weickert, M.O.; Pfeiffer, A.F.H. Impact of Dietary Fiber Consumption on Insulin Resistance and the Prevention of Type 2 Diabetes. J. Nutr. 2018, 148, 7–12. [Google Scholar] [CrossRef]
- Reynolds, A.N.; Akerman, A.P.; Mann, J. Dietary fibre and whole grains in diabetes management: Systematic review and meta-analyses. PLoS Med. 2020, 17, e1003053. [Google Scholar] [CrossRef]
- American Diabetes Association. 5. Lifestyle Management: Standards of Medical Care in Diabetes—2019. Diabetes Care 2019, 42 (Suppl. 1), S46–S60. [Google Scholar] [CrossRef] [PubMed]
- Meyer, K.A.; Kushi, L.H.; Jacobs, D.R., Jr.; Slavin, J.; Sellers, T.A.; Folsom, A.R. Carbohydrates, dietary fiber, and incident type 2 diabetes in older women. Am. J. Clin. Nutr. 2000, 71, 921–930. [Google Scholar] [CrossRef] [PubMed]
- Beretta, M.V.; Bernaud, F.R.; Nascimento, C.; Steemburgo, T.; Rodrigues, T.C. Higher fiber intake is associated with lower blood pressure levels in patients with type 1 diabetes. Arch. Endocrinol. Metab. 2018, 62, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Gingras, V.; Leroux, C.; Desjardins, K.; Savard, V.; Lemieux, S.; Rabasa-Lhoret, R.; Strychar, I. Association between Cardiometabolic Profile and Dietary Characteristics among Adults with Type 1 Diabetes Mellitus. J. Acad. Nutr. Diet. 2015, 115, 1965–1974. [Google Scholar] [CrossRef] [PubMed]
- Leroux, C.; Gingras, V.; Desjardins, K.; Brazeau, A.S.; Ott-Braschi, S.; Strychar, I.; Rabasa-Lhoret, R. In adult patients with type 1 diabetes healthy lifestyle associates with a better cardiometabolic profile. Nutr. Metab. Cardiovasc. Dis. 2015, 25, 444–451. [Google Scholar] [CrossRef] [PubMed]
- Katz, M.L.; Mehta, S.; Nansel, T.; Quinn, H.; Lipsky, L.M.; Laffel, L.M. Associations of nutrient intake with glycemic control in youth with type 1 diabetes: Differences by insulin regimen. Diabetes Technol. Ther. 2014, 16, 512–518. [Google Scholar] [CrossRef]
- Zhang, S.; Meng, G.; Zhang, Q.; Liu, L.; Yao, Z.; Wu, H.; Gu, Y.; Wang, Y.; Zhang, T.; Wang, X.; et al. Dietary fibre intake and risk of prediabetes in China: Results from the Tianjin Chronic Low-grade Systemic Inflammation and Health (TCLSIH) Cohort Study. Br. J. Nutr. 2022, 128, 753–761. [Google Scholar] [CrossRef] [PubMed]
- Zhu, R.; Larsen, T.M.; Fogelholm, M.; Poppitt, S.D.; Vestentoft, P.S.; Silvestre, M.P.; Jalo, E.; Navas-Carretero, S.; Huttunen-Lenz, M.; Taylor, M.A.; et al. Dose-Dependent Associations of Dietary Glycemic Index, Glycemic Load, and Fiber with 3-Year Weight Loss Maintenance and Glycemic Status in a High-Risk Population: A Secondary Analysis of the Diabetes Prevention Study PREVIEW. Diabetes Care 2021, 44, 1672–1681. [Google Scholar] [CrossRef]
- Sato, K.; Sasaki, M.; Nishimura, M.; Yamauchi, T. Correlation between habitual dietary fibre intake and postprandial plasma glucose levels in early adulthood. Ann. Hum. Biol. 2019, 46, 340–346. [Google Scholar] [CrossRef]
- Zhang, C.; Liu, S.; Solomon, C.G.; Hu, F.B. Dietary fiber intake, dietary glycemic load, and the risk for gestational diabetes mellitus. Diabetes Care 2006, 29, 2223–2230. [Google Scholar] [CrossRef]
- Bruttomesso, D.; Tessari, P. A High-Fiber Diet Decreases Postabsorptive Protein Turnover but Does Not Alter Insulin Sensitivity in Men with Type 1 Diabetes Mellitus. J. Nutr. 2019, 149, 596–604. [Google Scholar] [CrossRef] [PubMed]
- Ho, J.; Nicolucci, A.C.; Virtanen, H.; Schick, A.; Meddings, J.; Reimer, R.A.; Huang, C. Effect of Prebiotic on Microbiota, Intestinal Permeability, and Glycemic Control in Children with Type 1 Diabetes. J. Clin. Endocrinol. Metab. 2019, 104, 4427–4440. [Google Scholar] [CrossRef] [PubMed]
- Igudesman, D.; Crandell, J.L.; Corbin, K.D.; Hooper, J.; Thomas, J.M.; Bulik, C.M.; Pence, B.W.; Pratley, R.E.; Kosorok, M.R.; Maahs, D.M.; et al. Associations of Dietary Intake with the Intestinal Microbiota and Short-Chain Fatty Acids among Young Adults with Type 1 Diabetes and Overweight or Obesity. J. Nutr. 2023, 153, 1178–1188. [Google Scholar] [CrossRef] [PubMed]
- Dabelea, D.; Kinney, G.; Snell-Bergeon, J.K.; Hokanson, J.E.; Eckel, R.H.; Ehrlich, J.; Garg, S.; Hamman, R.F.; Rewers, M. Effect of type 1 diabetes on the gender difference in coronary artery calcification: A role for insulin resistance? The Coronary Artery Calcification in Type 1 Diabetes (CACTI) Study. Diabetes 2003, 52, 2833–2839. [Google Scholar] [CrossRef] [PubMed]
- Snell-Bergeon, J.K.; Hokanson, J.E.; Jensen, L.; MacKenzie, T.; Kinney, G.; Dabelea, D.; Eckel, R.H.; Ehrlich, J.; Garg, S.; Rewers, M. Progression of coronary artery calcification in type 1 diabetes: The importance of glycemic control. Diabetes Care 2003, 26, 2923–2928. [Google Scholar] [CrossRef] [PubMed]
- Snell-Bergeon, J.K.; Chartier-Logan, C.; Maahs, D.M.; Ogden, L.G.; Hokanson, J.E.; Kinney, G.L.; Eckel, R.H.; Ehrlich, J.; Rewers, M. Adults with type 1 diabetes eat a high-fat atherogenic diet that is associated with coronary artery calcium. Diabetologia 2009, 52, 801–809. [Google Scholar] [CrossRef]
- Basu, A.; Alman, A.C.; Snell-Bergeon, J.K. Dietary fiber intake and glycemic control: Coronary artery calcification in type 1 diabetes (CACTI) study. Nutr. J. 2019, 18, 23. [Google Scholar] [CrossRef]
- Basu, A.; Chien, L.C.; Alman, A.C.; Snell-Bergeon, J.K. Associations of dietary patterns and nutrients with coronary artery calcification and pericardial adiposity in a longitudinal study of adults with and without type 1 diabetes. Eur. J. Nutr. 2021, 60, 3911–3925. [Google Scholar] [CrossRef]
- Duca, L.M.; Maahs, D.M.; Schauer, I.E.; Bergman, B.C.; Nadeau, K.J.; Bjornstad, P.; Rewers, M.; Snell-Bergeon, J.K. Development and Validation of a Method to Estimate Insulin Sensitivity in Patients with and without Type 1 Diabetes. J. Clin. Endocrinol. Metab. 2016, 101, 686–695. [Google Scholar] [CrossRef]
- American Diabetes Association. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes—2018. Diabetes Care 2018, 41 (Suppl. 1), S13–S27. [Google Scholar] [CrossRef]
- Kriska, A.M.; Knowler, W.C.; LaPorte, R.E.; Drash, A.L.; Wing, R.R.; Blair, S.N.; Bennett, P.H.; Kuller, L.H. Development of questionnaire to examine relationship of physical activity and diabetes in Pima Indians. Diabetes Care 1990, 13, 401–411. [Google Scholar] [CrossRef] [PubMed]
- Lie, L.; Brown, L.; Forrester, T.E.; Plange-Rhule, J.; Bovet, P.; Lambert, E.V.; Layden, B.T.; Luke, A.; Dugas, L.R. The Association of Dietary Fiber Intake with Cardiometabolic Risk in Four Countries across the Epidemiologic Transition. Nutrients 2018, 10, 628. [Google Scholar] [CrossRef] [PubMed]
- Shivakoti, R.; Biggs, M.L.; Djoussé, L.; Durda, P.J.; Kizer, J.R.; Psaty, B.; Reiner, A.P.; Tracy, R.P.; Siscovick, D.; Mukamal, K.J. Intake and Sources of Dietary Fiber, Inflammation, and Cardiovascular Disease in Older US Adults. JAMA Netw. Open 2022, 5, e225012. [Google Scholar] [CrossRef]
- Kwon, Y.J.; Lee, H.S.; Park, G.; Kim, H.M.; Lee, J.W. Association of Dietary Fiber Intake with All-Cause Mortality and Cardiovascular Disease Mortality: A 10-Year Prospective Cohort Study. Nutrients 2022, 14, 89. [Google Scholar] [CrossRef] [PubMed]
- Miyazawa, I.; Miura, K.; Miyagawa, N.; Kondo, K.; Kadota, A.; Okuda, N.; Fujiyoshi, A.; Chihara, I.; Nakamura, Y.; Hozawa, A.; et al. Relationship between carbohydrate and dietary fibre intake and the risk of cardiovascular disease mortality in Japanese: 24-year follow-up of NIPPON DATA80. Eur. J. Clin. Nutr. 2020, 74, 67–76. [Google Scholar] [CrossRef] [PubMed]
- Ho, F.K.; Gray, S.R.; Welsh, P.; Petermann-Rocha, F.; Foster, H.; Waddell, H.; Anderson, J.; Lyall, D.; Sattar, N.; Gill, J.M.R.; et al. Associations of fat and carbohydrate intake with cardiovascular disease and mortality: Prospective cohort study of UK Biobank participants. BMJ (Clin. Res. Ed.) 2020, 368, m688. [Google Scholar] [CrossRef] [PubMed]
- Miketinas, D.C.; Tucker, W.J.; Douglas, C.C.; Patterson, M.A. Usual Dietary Fiber Intake According to Diabetes Status in US Adults: NHANES 2013–2018. Br. J. Nutr. 2023, 130, 1056–1064. [Google Scholar] [CrossRef]
- Fujii, H.; Iwase, M.; Ohkuma, T.; Ogata-Kaizu, S.; Ide, H.; Kikuchi, Y.; Idewaki, Y.; Joudai, T.; Hirakawa, Y.; Uchida, K.; et al. Impact of dietary fiber intake on glycemic control, cardiovascular risk factors and chronic kidney disease in Japanese patients with type 2 diabetes mellitus: The Fukuoka Diabetes Registry. Nutr. J. 2013, 12, 159. [Google Scholar] [CrossRef]
- Zhao, L.; Zhang, F.; Ding, X.; Wu, G.; Lam, Y.Y.; Wang, X.; Fu, H.; Xue, X.; Lu, C.; Ma, J.; et al. Gut bacteria selectively promoted by dietary fibers alleviate type 2 diabetes. Science 2018, 359, 1151–1156. [Google Scholar] [CrossRef]
- Ojo, O.; Feng, Q.Q.; Ojo, O.O.; Wang, X.H. The Role of Dietary Fibre in Modulating Gut Microbiota Dysbiosis in Patients with Type 2 Diabetes: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Nutrients 2020, 12, 3239. [Google Scholar] [CrossRef]
- Beulens, J.; Rutters, F.; Rydén, L.; Schnell, O.; Mellbin, L.; Hart, H.E.; Vos, R.C. Risk and management of pre-diabetes. Eur. J. Prev. Cardiol. 2019, 26, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Brannick, B.; Dagogo-Jack, S. Prediabetes and Cardiovascular Disease: Pathophysiology and Interventions for Prevention and Risk Reduction. Endocrinol. Metab. Clin. N. Am. 2018, 47, 33–50. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.; Siegel, K.R.; Ng, B.P.; Jawanda, S.; Proia, K.K.; Zhang, X.; Albright, A.L.; Zhang, P. Cost-effectiveness of Diabetes Prevention Interventions Targeting High-risk Individuals and Whole Populations: A Systematic Review. Diabetes Care 2020, 43, 1593–1616. [Google Scholar] [CrossRef]
- Pedersen, H.K.; Gudmundsdottir, V.; Nielsen, H.B.; Hyotylainen, T.; Nielsen, T.; Jensen, B.A.; Forslund, K.; Hildebrand, F.; Prifti, E.; Falony, G.; et al. Human gut microbes impact host serum metabolome and insulin sensitivity. Nature 2016, 535, 376–381. [Google Scholar] [CrossRef] [PubMed]
- Basu, A.; Izuora, K.; Hooyman, A.; Scofield, H.R.; Ebersole, J.L. Dietary Strawberries Improve Serum Metabolites of Cardiometabolic Risks in Adults with Features of the Metabolic Syndrome in a Randomized Controlled Crossover Trial. Int. J. Mol. Sci. 2023, 24, 2051. [Google Scholar] [CrossRef] [PubMed]
- Strozyk, S.; Rogowicz-Frontczak, A.; Pilacinski, S.; LeThanh-Blicharz, J.; Koperska, A.; Zozulinska-Ziolkiewicz, D. Influence of resistant starch resulting from the cooling of rice on postprandial glycemia in type 1 diabetes. Nutr. Diabetes 2022, 12, 21. [Google Scholar] [CrossRef] [PubMed]
- Davis-Richardson, A.G.; Triplett, E.W. A model for the role of gut bacteria in the development of autoimmunity for type 1 diabetes. Diabetologia 2015, 58, 1386–1393. [Google Scholar] [CrossRef]
- Lattimer, J.M.; Haub, M.D. Effects of dietary fiber and its components on metabolic health. Nutrients 2010, 2, 1266–1289. [Google Scholar] [CrossRef]
- Meier, J.J.; Menge, B.A.; Schenker, N.; Erdmann, S.; Kahle-Stephan, M.; Schliess, F.; Kapitza, C.; Nauck, M.A. Effects of sequential treatment with lixisenatide, insulin glargine, or their combination on meal-related glycaemic excursions, insulin and glucagon secretion, and gastric emptying in patients with type 2 diabetes. Diabetes Obes. Metab. 2020, 22, 599–611. [Google Scholar] [CrossRef]
- Lupoli, R.; Pisano, F.; Capaldo, B. Postprandial Glucose Control in Type 1 Diabetes: Importance of the Gastric Emptying Rate. Nutrients 2019, 11, 1559. [Google Scholar] [CrossRef]
- Bjornstad, P.; Maahs, D.M.; Duca, L.M.; Pyle, L.; Rewers, M.; Johnson, R.J.; Snell-Bergeon, J.K. Estimated insulin sensitivity predicts incident micro- and macrovascular complications in adults with type 1 diabetes over 6 years: The coronary artery calcification in type 1 diabetes study. J. Diabetes Its Complicat. 2016, 30, 586–590. [Google Scholar] [CrossRef] [PubMed]
- Lin, Z.; Tian, H.; Lam, K.S.; Lin, S.; Hoo, R.C.; Konishi, M.; Itoh, N.; Wang, Y.; Bornstein, S.R.; Xu, A.; et al. Adiponectin mediates the metabolic effects of FGF21 on glucose homeostasis and insulin sensitivity in mice. Cell Metab. 2013, 17, 779–789. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Zhang, D.; Vatner, D.F.; Goedeke, L.; Hirabara, S.M.; Zhang, Y.; Perry, R.J.; Shulman, G.I. Mechanisms by which adiponectin reverses high fat diet-induced insulin resistance in mice. Proc. Natl. Acad. Sci. USA 2020, 117, 32584–32593. [Google Scholar] [CrossRef] [PubMed]
- Castro, L.; Brant, L.; Diniz, M.F.; Lotufo, P.; Bensenor, I.J.; Chor, D.; Griep, R.; Barreto, S.M.; Ribeiro, A.L. Association of hypertension and insulin resistance in individuals free of diabetes in the ELSA-Brasil cohort. Sci. Rep. 2023, 13, 9456. [Google Scholar] [CrossRef] [PubMed]
- Adeva-Andany, M.M.; González-Lucán, M.; Fernández-Fernández, C.; Carneiro-Freire, N.; Seco-Filgueira, M.; Pedre-Piñeiro, A.M. Effect of diet composition on insulin sensitivity in humans. Clin. Nutr. ESPEN 2019, 33, 29–38. [Google Scholar] [CrossRef] [PubMed]
- Ding, C.; Chooi, Y.U.C.; Chan, Z.; Lo, J.; Choo, J.; Ding, B.T.K.; Leow, M.K.; Magkos, F. Dose-Dependent Effects of Exercise and Diet on Insulin Sensitivity and Secretion. Med. Sci. Sports Exerc. 2019, 51, 2109–2116. [Google Scholar] [CrossRef] [PubMed]
- Weiss, E.P.; Racette, S.B.; Villareal, D.T.; Fontana, L.; Steger-May, K.; Schechtman, K.B.; Klein, S.; Holloszy, J.O. Improvements in glucose tolerance and insulin action induced by increasing energy expenditure or decreasing energy intake: A randomized controlled trial. Am. J. Clin. Nutr. 2006, 84, 1033–1042. [Google Scholar] [CrossRef]
- Delahanty, L.M.; Nathan, D.M.; Lachin, J.M.; Hu, F.B.; Cleary, P.A.; Ziegler, G.K.; Wylie-Rosett, J.; Wexler, D.J. Association of diet with glycated hemoglobin during intensive treatment of type 1 diabetes in the Diabetes Control and Complications Trial. Am. J. Clin. Nutr. 2009, 89, 518–524. [Google Scholar] [CrossRef]
- Rosenfalck, A.M.; Almdal, T.; Viggers, L.; Madsbad, S.; Hilsted, J. A low-fat diet improves peripheral insulin sensitivity in patients with Type 1 diabetes. Diabet. Med. J. Br. Diabet. Assoc. 2006, 23, 384–392. [Google Scholar] [CrossRef]
- Basu, A.; Alman, A.C.; Snell-Bergeon, J.K. Associations of Dietary Antioxidants with Glycated Hemoglobin and Insulin Sensitivity in Adults with and without Type 1 Diabetes. J. Diabetes Res. 2022, 2022, 4747573. [Google Scholar] [CrossRef]


{kind=link}
| Non-DM | Pre-DM | T1D | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline (N = 590) | Visit 3 (N = 480) | Baseline (N = 212) | Visit 3 (N = 180) | Baseline (N = 603) | Visit 3 (N = 503) | ||||||||||
| Variables | Count | % | Count | % | p-value † | Count | % | Count | % | p-value † | Count | % | Count | % | p-value † |
| Sex (Female) | 318 | 54 | 243 | 51 | 0.39 | 81 | 38 | 71 | 39 | 0.78 | 297 | 49 | 238 | 47 | 0.86 |
| Median | IQR | Median | IQR | Median | IQR | Median | IQR | Median | IQR | Median | IQR | ||||
| Triglycerides, mg/dL | 98 | (73–141) | 90 | (64–134) | 0.0002 | 103 | (74–162) | 88 | (64–132) | 0.001 | 79 | (62–109) | 64 | (49–93) | <0.0001 |
| Physical Activity, min/week | 110 | (0–240) | 100 | (0–263) | 0.96 | 80 | (0–270) | 90 | (0–240) | 0.61 | 60 | (0–240) | 30 | (0–243) | 0.35 |
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | ||||
| Age, y | 39 | 9 | 45 | 9 | <0.0001 | 43 | 8 | 50 | 8 | <0.0001 | 37 | 9 | 44 | 9 | <0.0001 |
| BMI, kg/m2 | 26.0 | 5.0 | 26.0 | 5.2 | <0.0001 | 27.0 | 5.0 | 27.0 | 5.0 | 0.14 | 26.0 | 4.0 | 27.0 | 5.0 | <0.0001 |
| Calories, kcal/day | 1831 | 635 | 1866 | 636 | 0.17 | 1829 | 663 | 1889 | 679 | 0.08 | 1841 | 752 | 1881 | 708 | 0.325 |
| LDL, mg/dL | 112 | 33 | 106 | 31 | <0.0001 | 119 | 37 | 106 | 36 | <0.0001 | 101 | 29 | 88 | 31 | <0.0001 |
| HbA1c, % | 5.3 | 0.3 | 5.4 | 0.5 | <0.0001 | 6.0 | 0.2 | 6.1 | 0.7 | 0.04 | 8.1 | 1.1 | 8.0 | 1.2 | 0.11 |
| Fiber, g/day | 17.5 | 8.8 | 19.6 | 10.3 | <0.0001 | 16.3 | 7.0 | 18.1 | 8.6 | 0.003 | 17.3 | 8.9 | 18.5 | 9.4 | 0.009 |
| eIS | 16.5 | 8.3 | 16.4 | 8.1 | 0.74 | 9.1 | 4.8 | 10.4 | 6.0 | <0.0001 | 6.1 | 3.0 | 6.6 | 3.5 | 0.0002 |
| Model (M) | Pooled | Non-DM Group | T1D Group | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Parameter Estimate | 95% CI | p-Value | Parameter Estimate | 95% CI | p-Value | Parameter Estimate | 95% CI | p-Value | |
| Glycated Hemoglobin | |||||||||
| M1 | 0.0006 | −0.0008, 0.002 | 0.42 | −0.003 | −0.007, −0.0006 | 0.02 | −0.002 | −0.004, 0.0007 | 0.15 |
| M2 | 0.0007 | −0.0007, 0.002 | 0.33 | −0.003 | −0.006, 0.0003 | 0.07 | −0.002 | −0.004, 0.0007 | 0.17 |
| M3 | 0.0006 | −0.0007, 0.002 | 0.38 | −0.003 | −0.006, 0.0007 | 0.12 | −0.002 | −0.004, 0.0003 | 0.09 |
| Estimated insulin sensitivity | |||||||||
| M1 | 0.060 | 0.02, 0.09 | <0.001 | 0.09 | 0.04, 0.14 | <0.001 | 0.004 | −0.02, 0.03 | 0.79 |
| M2 | 0.030 | 0.002, 0.05 | 0.06 | 0.04 | 0.0004, 0.08 | 0.05 | −0.005 | −0.03, 0.02 | 0.68 |
| M3 | 0.026 | 0.00001, 0.05 | 0.049 | 0.04 | 0.004, 0.08 | 0.03 | −0.008 | −0.03, 0.02 | 0.51 |
| Model (M) | Normal (HbA1c: <5.7) | Prediabetes (HbA1c: 5.7–6.4%) | T1D (HbA1c: ≥6.5) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Parameter Estimate | 95% CI | p-Value | Parameter Estimate | 95% CI | p-Value | Parameter Estimate | 95% CI | p-Value | |
| M1 | −0.0009 | −0.003, 0.002 | 0.44 | −0.003 | −0.005, −0.0002 | 0.04 | −0.0007 | −0.003, 0.002 | 0.57 |
| M2 | −0.0009 | −0.0003, 0.002 | 0.49 | −0.002 | −0.005, 0.0003 | 0.08 | −0.0005 | −0.003, 0.002 | 0.62 |
| M3 | −0.0005 | −0.003, 0.002 | 0.69 | −0.003 | −0.005, −0.0001 | 0.04 | −0.0008 | −0.003, 0.002 | 0.50 |
| Covariates | Pooled | Non-DM | T1D | |
|---|---|---|---|---|
| Visit 1 | HbA1c | r = −0.01 p-value = 0.724 | r = −0.08 p-value = 0.044 | r = −0.10 p-value = 0.020 |
| eIS | r = 0.07 p-value = 0.011 | r = 0.19 p-value = <0.0001 | r = 0.10 p-value = 0.023 | |
| Visit 3 | HbA1c | r = −0.07 p-value = 0.031 | r = −0.04 p-value = 0.404 | r = −0.11 p-value = 0.030 |
| eIS | r = 0.13 p-value = 0.0001 | r = 0.19 p-value = <0.0001 | r = 0.05 p-value = 0.308 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Basu, A.; Hooyman, A.; Richardson, L.A.; Alman, A.C.; Snell-Bergeon, J.K. Longitudinal Associations of Dietary Fiber Intake with Glycated Hemoglobin and Estimated Insulin Sensitivity in Adults with and without Type 1 Diabetes. Nutrients 2023, 15, 4620. https://doi.org/10.3390/nu15214620
Basu A, Hooyman A, Richardson LA, Alman AC, Snell-Bergeon JK. Longitudinal Associations of Dietary Fiber Intake with Glycated Hemoglobin and Estimated Insulin Sensitivity in Adults with and without Type 1 Diabetes. Nutrients. 2023; 15(21):4620. https://doi.org/10.3390/nu15214620
Chicago/Turabian StyleBasu, Arpita, Andrew Hooyman, Leigh Ann Richardson, Amy C. Alman, and Janet K. Snell-Bergeon. 2023. "Longitudinal Associations of Dietary Fiber Intake with Glycated Hemoglobin and Estimated Insulin Sensitivity in Adults with and without Type 1 Diabetes" Nutrients 15, no. 21: 4620. https://doi.org/10.3390/nu15214620