Is the Tradeoff between Folic Acid or/and Multivitamin Supplementation against Birth Defects in Early Pregnancy Reconsidered? Evidence Based on a Chinese Birth Cohort Study

 ,
,
Abstract
:1. Introduction
2. Methods
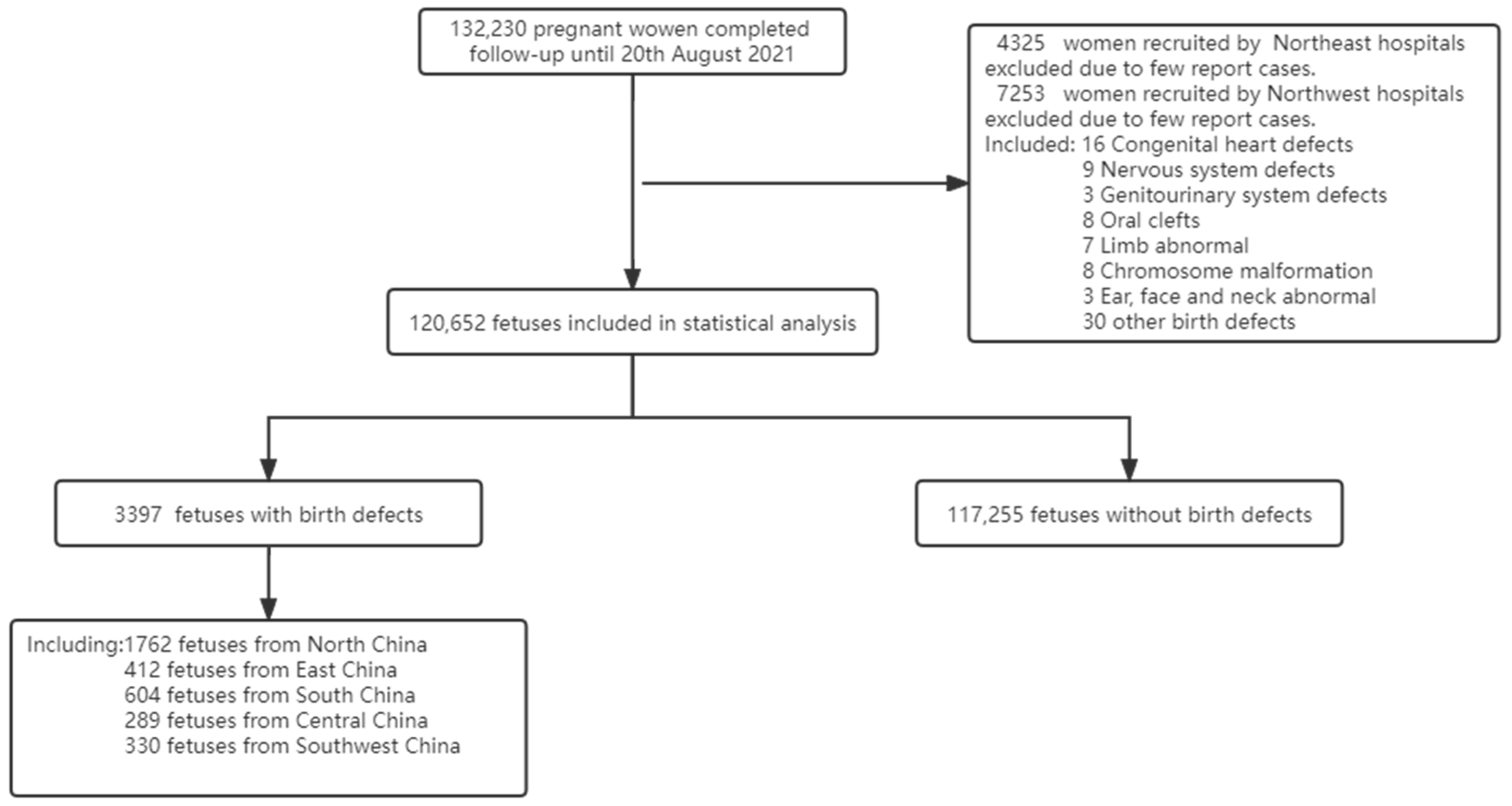
2.1. Participants
2.2. Classification of Birth Defects
2.3. Statistical Analysis
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pai, G.S.; Gadewar, S.B. Diagnostic approach to children with birth defects. Indian J. Pediatr. 2000, 67, 819–823. [Google Scholar] [CrossRef]
- Tuan, R.S. Birth Defects: Etiology, screening, and detection. Birth Defects Res. 2017, 109, 723–724. [Google Scholar] [CrossRef] [Green Version]
- GBD 2015 Child Mortality Collaborators. Global, regional, national, and selected subnational levels of stillbirths, neonatal, infant, and under-5 mortality, 1980–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1725–1774. [Google Scholar] [CrossRef] [Green Version]
- He, C.; Liu, L.; Chu, Y.; Perin, J.; Dai, L.; Li, X.; Miao, L.; Kang, L.; Li, Q.; Scherpbier, R.; et al. National and subnational all-cause and cause-specific child mortality in China, 1996–2015: A systematic analysis with implications for the Sustainable Development Goals. Lancet Glob. Health 2017, 5, e186–e197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gernand, A.D.; Schulze, K.J.; Stewart, C.P.; West, K.P.; Christian, P. Micronutrient deficiencies in pregnancy worldwide: Health effects and prevention. Nat. Rev. Endocrinol. 2016, 12, 274–289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MRC Vitamin Study Research Group. Prevention of neural tube defects: Results of the Medical Research Council Vitamin Study. Lancet 1991, 338, 131–137. [Google Scholar] [CrossRef]
- Czeizel, A.E.; Dudas, I. Prevention of the first occurrence of neural-tube defects by periconceptional vitamin supplementation. N. Engl. J. Med. 1992, 327, 1832–1835. [Google Scholar] [CrossRef]
- Liu, J.; Jin, L.; Meng, Q.; Gao, L.; Zhang, L.; Li, Z.; Ren, A. Changes in folic acid supplementation behaviour among women of reproductive age after the implementation of a massive supplementation programme in China. Public Health Nutr. 2015, 18, 582–588. [Google Scholar] [CrossRef]
- Oyen, N.; Olsen, S.F.; Basit, S.; Leirgul, E.; Strøm, M.; Carstensen, L.; Granström, C.; Tell, G.S.; Magnus, P.; Vollset, S.E.; et al. Association Between Maternal Folic Acid Supplementation and Congenital Heart Defects in Offspring in Birth Cohorts from Denmark and Norway. J. Am. Heart Assoc. 2019, 8, e11615. [Google Scholar] [CrossRef] [Green Version]
- De-Regil, L.M.; Pena-Rosas, J.P.; Fernandez-Gaxiola, A.C.; Rayco-Solon, P. Effects and safety of periconceptional oral folate supplementation for preventing birth defects. Cochrane Database Syst. Rev. 2015, 12, D7950. [Google Scholar] [CrossRef]
- Werler, M.M.; Hayes, C.; Louik, C.; Shapiro, S.; Mitchell, A.A. Multivitamin supplementation and risk of birth defects. Am. J. Epidemiol. 1999, 150, 675–682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Botto, L.D.; Olney, R.S.; Erickson, J.D. Vitamin supplements and the risk for congenital anomalies other than neural tube defects. Am. J. Med. Genet. C Semin. Med. Genet. 2004, 125C, 12–21. [Google Scholar] [CrossRef] [PubMed]
- Compilation expert group of “Multidisciplinary Expert Consensus on Rational Clinical Supplementation of Folic Acid in China”. Multidisciplinary expert consensus on rational folic acid supplementation in China. Her. Med. 2021, 40, 1–19. [Google Scholar] [CrossRef]
- Smedts, H.P.; de Vries, J.H.; Rakhshandehroo, M.; Wildhagen, M.F.; Verkleij-Hagoort, A.C.; Steegers, E.A.; Steegers-Theunissen, R.P. High maternal vitamin E intake by diet or supplements is associated with congenital heart defects in the offspring. BJOG 2009, 116, 416–423. [Google Scholar] [CrossRef] [PubMed]
- Hanson, C.; Jones, G.; Lyden, E.; Kaufmann, M.; Armas, L.; Anderson-Berry, A. Vitamin D metabolism in the premature newborn: A randomized trial. Clin. Nutr. 2016, 35, 835–841. [Google Scholar] [CrossRef] [PubMed]
- Rumbold, A.; Ota, E.; Hori, H.; Miyazaki, C.; Crowther, C.A. Vitamin E supplementation in pregnancy. Cochrane Database Syst. Rev. 2015, 9, D4069. [Google Scholar]
- Ackermans, M.M.; Zhou, H.; Carels, C.E.; Wagener, F.A.; Von den Hoff, J.W. Vitamin A and clefting: Putative biological mechanisms. Nutr. Rev. 2011, 69, 613–624. [Google Scholar] [CrossRef]
- Yue, W.; Zhang, E.; Liu, R.; Zhang, Y.; Wang, C.; Gao, S.; Su, S.; Gao, X.; Wu, Q.; Yang, X.; et al. The China birth cohort study (CBCS). Eur. J. Epidemiol. 2022, 37, 295–304. [Google Scholar] [CrossRef]
- Zhang, X.; Liu, J.; Jin, Y.; Yang, S.; Song, Z.; Jin, L.; Wang, L.; Ren, A. Folate of pregnant women after a nationwide folic acid supplementation in China. Matern. Child. Nutr. 2019, 15, e12828. [Google Scholar] [CrossRef]
- Hirsch, J.A.; Leslie-Mazwi, T.M.; Nicola, G.N.; Oklu, R.; Schoppe, K.A.; Silva, E., 3rd; Manchikanti, L. The ICD-10 system: A gift that keeps on taking. J. Neurointerv. Surg. 2015, 7, 619–622. [Google Scholar] [CrossRef]
- Haukoos, J.S.; Lewis, R.J. The Propensity Score. JAMA 2015, 314, 1637–1638. [Google Scholar] [CrossRef] [PubMed]
- Yan, R.; Liu, T.; Peng, Y. Can statistical adjustment guided by causal inference improve the accuracy of effect estimation? A simulation and empirical research based on meta-analyses of case-control studies. BMC Med. Inform. Decis. Mak. 2020, 20, 333. [Google Scholar] [CrossRef] [PubMed]
- Nie, X.; Liu, X.; Wang, C.; Wu, Z.; Sun, Z.; Su, J.; Yan, R.; Peng, Y.; Yang, Y.; Wang, C.; et al. Assessment of evidence on reported non-genetic risk factors of congenital heart defects: The updated umbrella review. BMC Pregnancy Childbirth 2022, 22, 371. [Google Scholar] [CrossRef] [PubMed]
- Austin, P.C.; Grootendorst, P.; Anderson, G.M. A comparison of the ability of different propensity score models to balance measured variables between treated and untreated subjects: A Monte Carlo study. Stat. Med. 2007, 26, 734–753. [Google Scholar] [CrossRef]
- Austin, P.C.; Stuart, E.A. Moving towards best practice when using inverse probability of treatment weighting (IPTW) using the propensity score to estimate causal treatment effects in observational studies. Stat. Med. 2015, 34, 3661–3679. [Google Scholar] [CrossRef] [Green Version]
- Ren, A.; Zhang, L.; Hao, L.; Li, Z.; Tian, Y.; Li, Z. Comparison of blood folate levels among pregnant Chinese women in areas with high and low prevalence of neural tube defects. Public Health Nutr. 2007, 10, 762–768. [Google Scholar] [CrossRef]
- Birhanu, B.E.; Kebede, D.L.; Kahsay, A.B.; Belachew, A.B. Predictors of teenage pregnancy in Ethiopia: A multilevel analysis. BMC Public Health 2019, 19, 601. [Google Scholar] [CrossRef] [Green Version]
- Peugh, J.L. A practical guide to multilevel modeling. J. Sch. Psychol. 2010, 48, 85–112. [Google Scholar] [CrossRef]
- Dean, J.H.; Pauly, R.; Stevenson, R.E. Neural Tube Defects and Associated Anomalies before and after Folic Acid Fortification. J. Pediatr. 2020, 226, 186–194. [Google Scholar] [CrossRef]
- Dai, L.; Zhu, J.; Liang, J.; Wang, Y.P.; Wang, H.; Mao, M. Birth defects surveillance in China. World J. Pediatr. 2011, 7, 302–310. [Google Scholar] [CrossRef]
- Chen, H.; Zhang, Y.; Wang, D.; Chen, X.; Li, M.; Huang, X.; Jiang, Y.; Dou, Y.; Wang, Y.; Ma, X. Periconception Red Blood Cell Folate and Offspring Congenital Heart Disease: Nested Case-Control and Mendelian Randomization Studies. Ann. Intern. Med. 2022, 175, 1212–1220. [Google Scholar] [CrossRef] [PubMed]
- Gildestad, T.; Bjorge, T.; Haaland, O.A.; Klungsøyr, K.; Vollset, S.E.; Øyen, N. Maternal use of folic acid and multivitamin supplements and infant risk of birth defects in Norway, 1999–2013. Br. J. Nutr. 2020, 124, 316–329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinez-Frias, M.L.; Salvador, J. Epidemiological aspects of prenatal exposure to high doses of vitamin A in Spain. Eur. J. Epidemiol. 1990, 6, 118–123. [Google Scholar] [CrossRef] [PubMed]
- Abbott, B.D.; Harris, M.W.; Birnbaum, L.S. Etiology of retinoic acid-induced cleft palate varies with the embryonic stage. Teratology 1989, 40, 533–553. [Google Scholar] [CrossRef] [PubMed]
- Arnaud, J.; Favier, A.; Herrmann, M.A.; Pilorget, J.J. [Effect of folic acid and folinic acid on zinc absorption]. Ann. Nutr. Metab. 1992, 36, 157–161. [Google Scholar] [CrossRef]
- Milne, D.B.; Canfield, W.K.; Mahalko, J.R.; Sandstead, H.H. Effect of oral folic acid supplements on zinc, copper, and iron absorption and excretion. Am. J. Clin. Nutr. 1984, 39, 535–539. [Google Scholar] [CrossRef]
- Cherry, F.F.; Bennett, E.A.; Bazzano, G.S.; Johnson, L.K.; Fosmire, G.J.; Batson, H.K. Plasma zinc in hypertension/toxemia and other reproductive variables in adolescent pregnancy. Am. J. Clin. Nutr. 1981, 34, 2367–2375. [Google Scholar] [CrossRef]
- Simmer, K.; Thompson, R.P. Maternal zinc and intrauterine growth retardation. Clin. Sci. 1985, 68, 395–399. [Google Scholar] [CrossRef]
- Mukherjee, M.D.; Sandstead, H.H.; Ratnaparkhi, M.V.; Johnson, L.K.; Milne, D.B.; Stelling, H.P. Maternal zinc, iron, folic acid, and protein nutriture and outcome of human pregnancy. Am. J. Clin. Nutr. 1984, 40, 496–507. [Google Scholar] [CrossRef]
- Ghishan, F.K.; Said, H.M.; Wilson, P.C.; Murrell, J.E.; Greene, H.L. Intestinal transport of zinc and folic acid: A mutual inhibitory effect. Am. J. Clin. Nutr. 1986, 43, 258–262. [Google Scholar] [CrossRef]
- Pietrzik, K.; Bailey, L.; Shane, B. Folic acid and L-5-methyltetrahydrofolate: Comparison of clinical pharmacokinetics and pharmacodynamics. Clin. Pharmacokinet. 2010, 49, 535–548. [Google Scholar] [CrossRef] [PubMed]
- Sweeney, M.R.; McPartlin, J.; Scott, J. Folic acid fortification and public health: Report on threshold doses above which unmetabolised folic acid appear in serum. BMC Public Health 2007, 7, 41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bailey, S.W.; Ayling, J.E. The extremely slow and variable activity of dihydrofolate reductase in human liver and its implications for high folic acid intake. Proc. Natl. Acad. Sci. USA 2009, 106, 15424–15429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maruvada, P.; Stover, P.J.; Mason, J.B.; Bailey, R.L.; Davis, C.D.; Field, M.S.; Finnell, R.H.; Garza, C.; Green, R.; Gueant, J.L.; et al. Knowledge gaps in understanding the metabolic and clinical effects of ex-cess folates/folic acid: A summary, and perspectives, from an NIH workshop. Am. J. Clin. Nutr. 2020, 112, 1390–1403. [Google Scholar] [CrossRef] [PubMed]
- Valera-Gran, D.; de la Hera, M.G.; Navarrete-Munoz, E.M.; Fernandez-Somoano, A.; Tardón, A.; Julvez, J.; Forns, J.; Lertxundi, N.; Ibarluzea, J.M.; Murcia, M.; et al. Folic acid supplements during pregnancy and child psychomotor development after the first year of life. JAMA Pediatr. 2014, 168, e142611. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shorter, K.R.; Felder, M.R.; Vrana, P.B. Consequences of dietary methyl donor supplements: Is more always better? Prog. Biophys. Mol. Biol. 2015, 118, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Silva, C.; Keating, E.; Pinto, E. The impact of folic acid supplementation on gestational and long term health: Critical temporal windows, benefits and risks. Porto Biomed. J. 2017, 2, 315–332. [Google Scholar] [CrossRef]
- Yajnik, C.S.; Deshpande, S.S.; Jackson, A.A.; Refsum, H.; Rao, S.; Fisher, D.J.; Bhat, D.S.; Naik, S.S.; Coyaji, K.J.; Joglekar, C.V.; et al. Vitamin B12 and folate concentrations during pregnancy and insulin resistance in the offspring: The Pune Maternal Nutrition Study. Diabetologia 2008, 51, 29–38. [Google Scholar] [CrossRef] [Green Version]
- Xie, K.; Xu, P.; Fu, Z.; Gu, X.; Li, H.; Cui, X.; You, L.; Zhu, L.; Ji, C.; Guo, X. Association of maternal folate status in the second trimester of pregnancy with the risk of gestational diabetes mellitus. Food Sci. Nutr. 2019, 7, 3759–3765. [Google Scholar] [CrossRef]
- Chen, X.; Zhang, Y.; Chen, H.; Jiang, Y.; Wang, Y.; Wang, D.; Li, M.; Dou, Y.; Sun, X.; Huang, G.; et al. Association of Maternal Folate and Vitamin B12 in Early Pregnancy With Gestational Diabetes Mellitus: A Prospective Cohort Study. Diabetes Care 2021, 44, 217–223. [Google Scholar] [CrossRef]
- Li, S.; Hou, Y.; Yan, X.; Wang, Y.; Shi, C.; Wu, X.; Liu, H.; Zhang, L.; Zhang, X.; Liu, J.; et al. Joint effects of folate and vitamin B12 imbalance with maternal characteristics on gestational diabetes mellitus. J. Diabetes 2019, 11, 744–751. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Liu, B.; Sun, Y.; Du, Y.; Santillan, M.K.; Santillan, D.A.; Snetselaar, L.G.; Bao, W. Association of Maternal Prepregnancy Diabetes and Gestational Diabetes Mellitus With Congenital Anomalies of the Newborn. Diabetes Care 2020, 43, 2983–2990. [Google Scholar] [CrossRef] [PubMed]
- Sadetzki, S.; Bensal, D.; Novikov, I.; Modan, B. The limitations of using hospital controls in cancer etiology--one more ex-ample for Berkson’s bias. Eur. J. Epidemiol. 2003, 18, 1127–1131. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics (n, %) | Unweighted Cohort | Inverse Probability Weighted Cohort | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Exposure to only FA (n = 40,204) | Exposure to only MV (n = 5567) | Exposure to FA and MV (n = 71,538) | Without Exposure to FA and MV (n = 3343) | Standardized Difference | Exposure to only FA | Exposure to only MV | Exposure to FA and MV | Without Exposure to FA and MV | Standardized Difference | |
| Maternal age, n (%) | 0.106 | 0.007 | ||||||||
| <35 | 37,026 (92.1) | 4864 (87.4) | 64,571 (90.3) | 2892 (86.5) | 90.5 | 90.2 | 90.6 | 90.4 | ||
| ≥35 | 3178 (7.9) | 703 (12.6) | 6967 (9.7) | 451 (13.5) | 9.5 | 9.8 | 9.4 | 9.6 | ||
| Pre-pregnancy BMI, kg/m2, n (%) | 0.075 | 0.019 | ||||||||
| <18.5 | 26,312 (65.4) | 3752 (67.4) | 48,004 (67.1) | 2119 (63.4) | 66.5 | 66.1 | 66.4 | 67 | ||
| 18.5–24 | 5682 (14.1) | 714 (12.8) | 9242 (12.9) | 431 (12.9) | 13.3 | 13.9 | 13.3 | 13.4 | ||
| 24–28 | 6165 (15.3) | 823 (14.8) | 10,904 (15.2) | 544 (16.3) | 15.4 | 15.2 | 15.3 | 14.6 | ||
| ≥28 | 2045 (5.1) | 278 (5.0) | 3388 (4.7) | 249 (7.4) | 4.9 | 4.8 | 4.9 | 5.1 | ||
| Maternal education, n (%) | 0.389 | 0.018 | ||||||||
| Primary school or lower | 222 (0.6) | 7 (0.1) | 225 (0.3) | 60 (1.8) | 0.4 | 0.5 | 0.4 | 0.5 | ||
| High school or lower | 11,400 (28.4) | 628 (11.3) | 11,617 (16.2) | 1249 (37.4) | 20.5 | 20.5 | 20.6 | 21.7 | ||
| Bachelor’s degree or above | 28,582 (71.1) | 4932 (88.6) | 59,696 (83.4) | 2034 (60.8) | 79.1 | 79 | 79 | 77.8 | ||
| Family annually income, Yuan, n (%) | ||||||||||
| <200 K | 29,262(72.8) | 2757 (49.5) | 46,103 (64.4) | 2569 (76.8) | 0.323 | 66.6 | 66.7 | 66.8 | 69.2 | 0.062 |
| ≥200 K | 10,942(27.2) | 2810 (50.5) | 25,435 (35.6) | 774 (23.2) | 33.4 | 33.3 | 33.2 | 30.8 | ||
| Parity, n (%) | 0.311 | 0.012 | ||||||||
| 0 | 18,202 (45.3) | 2633 (47.3) | 36,237 (50.7) | 910 (27.2) | 48.1 | 47.7 | 48 | 47.1 | ||
| 1 | 20,053 (49.9) | 2793 (50.2) | 33,317 (46.6) | 2014 (60.2) | 48.2 | 48.5 | 48.2 | 48.9 | ||
| ≥2 | 1949 (4.8) | 141 (2.5) | 1984 (2.8) | 419 (12.5) | 3.7 | 3.8 | 3.7 | 4 | ||
| Number of fetuses, n (%) | 0.053 | 0.005 | ||||||||
| 1 | 39,633 (98.6) | 5412 (97.2) | 69,933 (97.8) | 3283 (98.2) | 98 | 98 | 98 | 98.1 | ||
| ≥2 | 571 (1.4) | 155 (2.8) | 1605 (2.2) | 60 (1.8) | 2 | 2 | 2 | 1.9 | ||
| Maternal alcohol drinking, n (%) | 0.037 | 0.003 | ||||||||
| No | 38,876 (96.7) | 5323 (95.6) | 69,361 (97.0) | 3227 (96.5) | 96.8 | 96.7 | 96.8 | 96.8 | ||
| Yes | 1328 (3.3) | 244 (4.4) | 2177 (3.0) | 116 (3.5) | 3.2 | 3.3 | 3.2 | 3.2 | ||
| Maternal tobacco exposure, n (%) | 0.095 | 0.006 | ||||||||
| No | 34,956 (86.9) | 4966 (89.2) | 64,228 (89.8) | 2815 (84.2) | 88.8 | 88.5 | 88.7 | 88.5 | ||
| Yes | 5248 (13.1) | 601 (10.8) | 7310 (10.2) | 528 (15.8) | 11.2 | 11.5 | 11.3 | 11.5 | ||
| Mode of conception, n (%) | 0.213 | 0.015 | ||||||||
| Natural pregnancy | 39,342 (97.9) | 5093 (91.5) | 67,111 (93.8) | 3305 (98.9) | 94.9 | 94.8 | 95.2 | 94.5 | ||
| Assisted reproduction | 862 (2.1) | 474 (8.5) | 4427 (6.2) | 38 (1.1) | 5.1 | 5.2 | 4.8 | 5.5 | ||
| Family history of birth defects, n (%) | 0.025 | 0.005 | ||||||||
| No | 38,920 (96.8) | 5340 (95.9) | 69,247 (96.8) | 3238 (96.9) | 96.8 | 96.8 | 96.8 | 96.9 | ||
| Yes | 1284 (3.2) | 227 (4.1) | 2291 (3.2) | 105 (3.1) | 3.2 | 3.2 | 3.2 | 3.1 | ||
| History of adverse pregnancy, n (%) | 0.09 | 0.005 | ||||||||
| No | 26,579 (66.1) | 3597 (64.6) | 49,036 (68.5) | 2020 (60.4) | 67.4 | 67.2 | 67.3 | 66.9 | ||
| Yes | 13,625 (33.9) | 1970 (35.4) | 22,502 (31.5) | 1323 (39.6) | 32.6 | 32.8 | 32.7 | 33.1 | ||
| History of previous birth defect pregnancy, n (%) | 0.014 | 0.008 | ||||||||
| No | 39,443 (98.1) | 5446 (97.8) | 70,067 (97.9) | 3282 (98.2) | 98 | 98 | 98 | 98.2 | ||
| Yes | 761 (1.9) | 121 (2.2) | 1471 (2.1) | 61 (1.8) | 2 | 2 | 2 | 1.8 | ||
| Birth Defects | Total (120,652) | Exposure to Only FA (40,204) | Exposure to Only MV (5567) | Exposure to FA and MV (71,538) | Without Exposure to FA and MV (3343) | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| n | Incidence per 10,000 | n | Incidence per 10,000 | n | Incidence per 10,000 | n | Incidence per 10,000 | n | Incidence per 10,000 | |
| Congenital heart defects | 848 | 70.3 (65.6–75.2) | 204 | 50.7 (44.0–58.2) | 57 | 102.4 (77.6–132.5) | 569 | 79.5 (73.2–86.3) | 18 | 53.8 (31.9–85.0) |
| Abnormal chromosome | 517 | 42.9 (39.2–46.7) | 146 | 36.3 (30.7–42.7) | 41 | 73.6 (52.9–99.8) | 321 | 44.9 (40.1–50.0) | 9 | 26.9 (12.3–51.0) |
| Genitourinary system | 509 | 42.2 (38.6–46.0) | 133 | 33.1 (27.7–39.2) | 51 | 91.6 (68.3–120.3) | 319 | 44.6 (39.4–49.8) | 6 | 17.9 (6.6–39.0) |
| Nervous system | 437 | 36.2 (32.9–39.8) | 111 | 27.6 (22.7–33.2) | 27 | 48.5 (32.0–70.4) | 287 | 40.1 (35.6–45.0) | 12 | 35.9 (18.6–62.6) |
| Limb | 376 | 31.2 (28.1–34.5) | 105 | 26.1 (21.4–31.6) | 38 | 68.3 (48.3–93.6) | 223 | 31.2 (27.2–35.5) | 10 | 29.9 (14.4–54.9) |
| Ear, face and neck | 369 | 30.6 (27.5–33.9) | 103 | 25.6 (20.9–31.1) | 32 | 57.5 (39.3–81.1) | 225 | 31.5 (27.5–35.8) | 9 | 26.9 (12.3–51.0) |
| Oral clefts | 174 | 14.4 (12.4–16.7) | 48 | 11.9 (8.8–15.8) | 9 | 16.2 (7.4–30.7) | 114 | 15.9 (13.1–19.1) | 3 | 9.0 (1.8–26.2) |
| Birth Defects | North China (42,968) | South China (22,724) | East China (24,070) | Central China (13,351) | Southwest China (17,539) | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| n | Incidence per 10,000 | n | Incidence per 10,000 | n | Incidence per 10,000 | n | Incidence per 10,000 | n | Incidence per 10,000 | |
| Congenital heart defects | 395 | 91.9 (83.1–101.4) | 155 | 68.2 (57.9–79.8) | 123 | 51.1 (42.5–60.9) | 100 | 74.9 (61.0–91.0) | 75 | 42.8 (33.6–53.6) |
| Abnormal chromosome | 268 | 62.4 (55.1–70.3) | 111 | 48.8 (40.2–58.8) | 39 | 16.2 (11.5–22.1) | 51 | 38.2 (28.5–50.2) | 48 | 27.4 (20.2–36.3) |
| Genitourinary system | 338 | 78.7 (70.5–87.5) | 77 | 33.9 (26.8–42.3) | 40 | 16.6 (11.9–22.6) | 25 | 18.7 (12.1–27.6) | 29 | 16.5 (11.1–23.7) |
| Nervous system | 216 | 50.3 (43.8–57.4) | 103 | 45.3 (37.0–54.9) | 41 | 17.0 (12.2–23.1) | 33 | 24.7 (17.0–34.7) | 44 | 25.1 (18.2–33.7) |
| Limb | 156 | 36.3 (30.8–42.5) | 107 | 47.1 (38.6–56.9) | 41 | 17.0 (12.2–23.1) | 33 | 24.7 (17.0–34.7) | 39 | 22.2 (15.8–30.4) |
| Ear, face, and neck | 281 | 65.4 (58.0–73.5) | 41 | 18.0 (13.0–24.5) | 17 | 7.1 (4.1–11.3) | 7 | 5.2 (2.1–10.8) | 23 | 13.1 (8.3–19.7) |
| Oral clefts | 74 | 17.2 (13.5–21.6) | 27 | 11.9 (7.8–17.3) | 33 | 13.7 (9.4–19.2) | 16 | 12.0 (6.9–19.5) | 24 | 13.7 (8.8–20.3) |
| Diseases | Without Exposure to FA and MV | Exposure to Only FA | Exposure to Only MV | Exposure to FA and MV |
|---|---|---|---|---|
| Congenital heart disease | 1 (Reference) | 0.95 (0.60–1.51) | 1.42 (0.84–2.39) | 1.25 (0.79–1.96) |
| Chromosome | 1 (Reference) | 1.85 (0.87–3.90) | 2.57 (1.16–5.73) * | 1.93 (0.92–4.04) |
| Genitourinary | 1 (Reference) | 1.97 (0.90–4.30) | 3.22 (1.42–7.29) * | 1.98 (0.91–4.30) |
| Nervous system | 1 (Reference) | 0.75 (0.42–1.35) | 0.86 (0.43–1.73) | 0.95 (0.54–1.68) |
| Limb | 1 (Reference) | 0.93 (0.49–1.79) | 1.97 (0.97–4.00) | 0.97 (0.51–1.84) |
| Face, ear, and neck | 1 (Reference) | 0.84 (0.46–1.54) | 0.97 (0.48–1.94) | 0.76 (0.42–1.39) |
| Oral clefts | 1 (Reference) | 1.23 (0.38–4.00) | 1.48 (0.38–5.67) | 1.64 (0.52–5.23) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Su, J.; Gao, S.; Yan, R.; Liu, R.; Su, S.; Nie, X.; Liu, X.; Zhang, E.; Xie, S.; Liu, J.; et al. Is the Tradeoff between Folic Acid or/and Multivitamin Supplementation against Birth Defects in Early Pregnancy Reconsidered? Evidence Based on a Chinese Birth Cohort Study. Nutrients 2023, 15, 279. https://doi.org/10.3390/nu15020279
Su J, Gao S, Yan R, Liu R, Su S, Nie X, Liu X, Zhang E, Xie S, Liu J, et al. Is the Tradeoff between Folic Acid or/and Multivitamin Supplementation against Birth Defects in Early Pregnancy Reconsidered? Evidence Based on a Chinese Birth Cohort Study. Nutrients. 2023; 15(2):279. https://doi.org/10.3390/nu15020279
Chicago/Turabian StyleSu, Jian, Shen Gao, Ruohua Yan, Ruixia Liu, Shaofei Su, Xiaolu Nie, Xiaohang Liu, Enjie Zhang, Shuanghua Xie, Jianhui Liu, and et al. 2023. "Is the Tradeoff between Folic Acid or/and Multivitamin Supplementation against Birth Defects in Early Pregnancy Reconsidered? Evidence Based on a Chinese Birth Cohort Study" Nutrients 15, no. 2: 279. https://doi.org/10.3390/nu15020279