
Influence of Alcohol Consumption on the Development of Erosive Esophagitis in Both Sexes: A Longitudinal Study
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Study Population
2.2. Data Collection
2.3. Esophagogastroduodenoscopy
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics According to Sex
3.2. Changes in Drinking Quantity between Baseline and Final Measurements
3.3. Changes in Drinking Frequency between Baseline and Final Measurements
3.4. Presence or Absence of EE in Patients without EE at Baseline
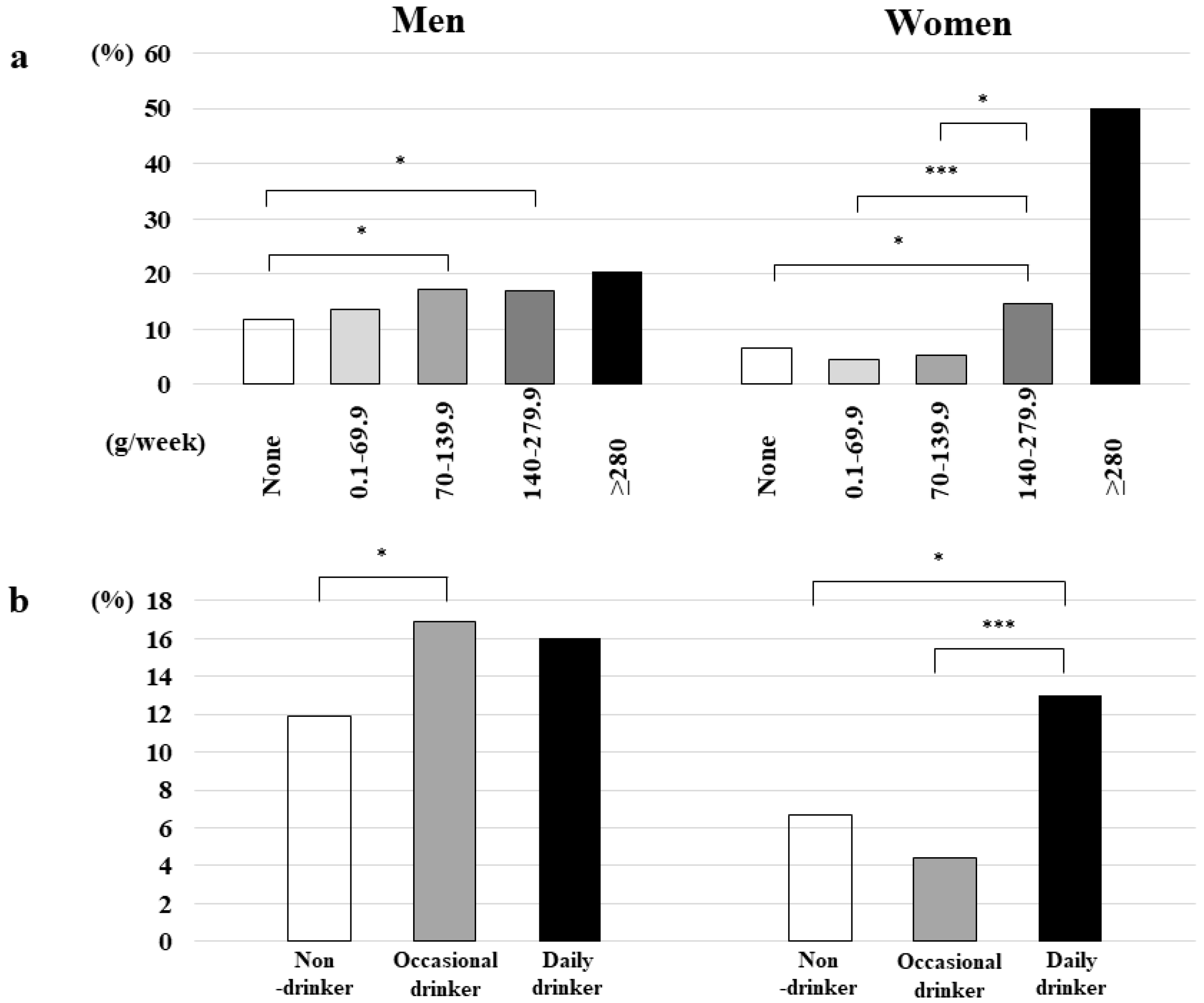
3.5. Prevalence of EE According to Drinking Quantity and Frequency Categories
3.6. Relationship between EE Development and Alcohol Quantity
3.7. Relationship between EE Development and Drinking Frequency
3.8. Relationship between Alcohol Consumption and EE Severity in Patients with Newly Developed EE
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Velanovich, V. Quality of life and severity of symptoms in gastro-oesophageal reflux disease: A clinical review. Eur. J. Surg. 2000, 166, 516–525. [Google Scholar] [CrossRef] [PubMed]
- El-Serag, H.B.; Sweet, S.; Winchester, C.C.; Dent, J. Update on the epidemiology of gastro-oesophageal reflux disease: A systematic review. Gut 2014, 63, 871–880. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goh, K.L. Gastroesophageal reflux disease in Asia: A historical perspective and present challenges. J. Gastroenterol. Hepatol. 2011, 26, 2–10. [Google Scholar] [CrossRef]
- Gyawali, C.P.; Kahrilas, P.J.; Savarino, E.; Zerbib, F.; Mion, F.; Smout, A.J.P.M.; Vaezi, M.; Sifrim, D.; Fox, M.R.; Vela, M.F.; et al. Modern diagnosis of GERD: The Lyon consensus. Gut 2018, 67, 1351–1362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ronkainen, J.; Talley, N.J.; Storskrubb, T.; Johansson, S.E.; Lind, T.; Vieth, M.; Agréus, L.; Aro, P. Erosive esophagitis is a risk factor for Barrett’s esophagus: A community-based endoscopic follow-up study. Am. J. Gastroenterol. 2011, 106, 1946–1952. [Google Scholar] [CrossRef]
- Järveläinen, H.A.; Lukkari, T.A.; Heinaro, S.; Sippel, H.; Lindros, K.O. The antiestrogen toremifene protects against alcoholic liver injury in female rats. J. Hepatol. 2001, 35, 46–52. [Google Scholar] [CrossRef]
- Mauvais-Jarvis, F.; Bairey Merz, N.B.; Barnes, P.J.; Brinton, R.D.; Carrero, J.J.; DeMeo, D.L.; De Vries, G.J.; Epperson, C.N.; Govindan, R.; Klein, S.L.; et al. Sex and gender: Modifiers of health, disease, and medicine. Lancet 2020, 396, 565–582. [Google Scholar] [CrossRef]
- Asanuma, K.; Iijima, K.; Shimosegawa, T. Gender difference in gastro-esophageal reflux diseases. World J. Gastroenterol. 2016, 22, 1800–1810. [Google Scholar] [CrossRef]
- World Health Organization. Global Status Report on Alcohol and Health 2014; WHO: Geneva, Switzerland, 2014. [Google Scholar]
- Eslam, M.; Newsome, P.N.; Sarin, S.K.; Anstee, Q.M.; Targher, G.; Romero-Gomez, M.; Zelber-Sagi, S.; Wai-Sun Wong, V.; Dufour, J.F.; Schattenberg, J.M.; et al. A new definition for metabolic dysfunction-associated fatty liver disease: An international expert consensus statement. J. Hepatol. 2020, 73, 202–209. [Google Scholar] [CrossRef]
- Albert, P.S.; Follmann, D.A.; Barnhart, H.X. A generalized estimating equation approach for modeling random length binary vector data. Biometrics 1997, 53, 1116–1124. [Google Scholar] [CrossRef]
- Zamani, M.; Alizadeh-Tabari, S.; Hasanpour, A.H.; Eusebi, L.H.; Ford, A.C. Systematic review with meta-analysis: Association of Helicobacter pylori infection with gastro-oesophageal reflux and its complications. Aliment. Pharmacol. Ther. 2021, 54, 988–998. [Google Scholar] [CrossRef] [PubMed]
- Xie, T.; Cui, X.; Zheng, H.; Chen, D.; He, L.; Jiang, B. Meta-analysis: Eradication of Helicobacter pylori infection is associated with the development of endoscopic gastroesophageal reflux disease. Eur. J. Gastroenterol. Hepatol. 2013, 25, 1195–1205. [Google Scholar] [CrossRef] [PubMed]
- Rajendra, S.; Ackroyd, R.; Robertson, I.K.; Ho, J.J.; Karim, N.; Kutty, K.M. Helicobacter pylori, ethnicity, and the gastroesophageal reflux disease spectrum: A study from the East. Helicobacter 2007, 12, 177–183. [Google Scholar] [CrossRef]
- National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third report of the National Cholesterol Education Program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (adult treatment panel III) final report. Circulation 2002, 106, 3143–3421. [Google Scholar] [CrossRef]
- Lee, Y.C.; Yen, A.M.; Tai, J.J.; Chang, S.H.; Lin, J.T.; Chiu, H.M.; Wang, H.P.; Wu, M.S.; Chen, T.H. The effect of metabolic risk factors on the natural course of gastro-oesophageal reflux disease. Gut 2009, 58, 174–181. [Google Scholar] [CrossRef] [Green Version]
- Lluch, I.; Ascaso, J.F.; Mora, F.; Minguez, M.; Peña, A.; Hernandez, A.; Benages, A. Gastroesophageal reflux in diabetes mellitus. Am. J. Gastroenterol. 1999, 94, 919–924. [Google Scholar] [CrossRef]
- Toki, Y.; Yamauchi, R.; Kayashima, E.; Adachi, K.; Kishi, K.; Suetsugu, H.; Wada, T.; Endo, H.; Yamada, H.; Osaga, S.; et al. Predictive factors for future onset of reflux esophagitis: A longitudinal case-control study using health checkup records. J. Neurogastroenterol. Motil. 2022, 28, 86–94. [Google Scholar] [CrossRef] [PubMed]
- Verne, G.N.; Sninsky, C.A. Diabetes and the gastrointestinal tract. Gastroenterol. Clin. N. Am. 1998, 27, 861–874. [Google Scholar] [CrossRef]
- Loke, S.S.; Yang, K.D.; Chen, K.D.; Chen, J.F. Erosive esophagitis associated with metabolic syndrome, impaired liver function, and dyslipidemia. World J. Gastroenterol. 2013, 19, 5883–5888. [Google Scholar] [CrossRef]
- Mayer, E.M.; Grabowski, C.J.; Fisher, R.S. Effects of graded doses of alcohol upon esophageal motor function. Gastroenterology 1978, 75, 1133–1136. [Google Scholar] [CrossRef]
- Anderson, L.A.; Cantwell, M.M.; Watson, R.G.; Johnston, B.T.; Murphy, S.J.; Ferguson, H.R.; McGuigan, J.; Comber, H.; Reynolds, J.V.; Murray, L.J. The association between alcohol and reflux esophagitis, Barrett’s esophagus, and esophageal adenocarcinoma. Gastroenterology 2009, 136, 799–805. [Google Scholar] [CrossRef] [PubMed]
- Kubo, A.; Levin, T.R.; Block, G.; Rumore, G.J.; Quesenberry, C.P.; Buffler, P.; Corley, D.A. Alcohol types and sociodemographic characteristics as risk factors for Barrett’s esophagus. Gastroenterology 2009, 136, 806–815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kubo, A.; Block, G.; Quesenberry, C.P.; Buffler, P.; Corley, D.A. Dietary guideline adherence for gastroesophageal reflux disease. BMC Gastroenterol. 2014, 14, 144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gammon, M.D.; Schoenberg, J.B.; Ahsan, H.; Risch, H.A.; Vaughan, T.L.; Chow, W.H.; Rotterdam, H.; West, A.B.; Dubrow, R.; Stanford, J.L.; et al. Tobacco, alcohol, and socioeconomic status and adenocarcinomas of the esophagus and gastric cardia. J. Natl. Cancer Inst. 1997, 89, 1277–1284. [Google Scholar] [CrossRef] [Green Version]
- Pandeya, N.; Williams, G.; Green, A.C.; Webb, P.M.; Whiteman, D.C.; Australian Cancer Study. Alcohol consumption and the risks of adenocarcinoma and squamous cell carcinoma of the esophagus. Gastroenterology 2009, 136, 1215–1224. [Google Scholar] [CrossRef]
- Martinez-Gomez, A.; Caballero, I.; Blanco, C.A. Phenols and melanoidins as natural antioxidants in beer. Structure, reactivity and antioxidant activity. Biomolecules 2020, 10, 400. [Google Scholar] [CrossRef] [Green Version]
- Snopek, L.; Mlcek, J.; Sochorova, L.; Baron, M.; Hlavacova, I.; Jurikova, T.; Kizek, R.; Sedlackova, E.; Sochor, J. Contribution of red wine consumption to human health protection. Molecules 2018, 23, 1684. [Google Scholar] [CrossRef] [Green Version]
- Souza, R.F. Reflux esophagitis and its role in the pathogenesis of Barrett’s metaplasia. J. Gastroenterol. 2017, 52, 767–776. [Google Scholar] [CrossRef] [Green Version]
- Thrift, A.P.; Kramer, J.R.; Richardson, P.A.; El-Serag, H.B. No significant effects of smoking or alcohol consumption on risk of Barrett’s esophagus. Dig. Dis. Sci. 2014, 59, 108–116. [Google Scholar] [CrossRef] [Green Version]
- Thrift, A.P.; Cook, M.B.; Vaughan, T.L.; Anderson, L.A.; Murray, L.J.; Whiteman, D.C.; Shaheen, N.J.; Corley, D.A. Alcohol and the risk of Barrett’s esophagus: A pooled analysis from the International BEACON Consortium. Am. J. Gastroenterol. 2014, 109, 1586–1594. [Google Scholar] [CrossRef]
- Achem, A.C.; Achem, S.R.; Stark, M.E.; DeVault, K.R. Failure of esophageal peristalsis in older patients: Association with esophageal acid exposure. Am. J. Gastroenterol. 2003, 98, 35–39. [Google Scholar] [CrossRef] [PubMed]
- Park, C.H.; Kim, K.O.; Baek, I.H.; Choi, M.H.; Jang, H.J.; Kae, S.H.; Kim, J.B.; Baik, G.H.; Shin, W.G.; Kim, K.H.; et al. Differences in the risk factors of reflux esophagitis according to age in Korea. Dis. Esophagus. 2014, 27, 116–121. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, I.; Kamochi, M.; Yoshikawa, H.; Nakayama, Y. Gender difference in alcoholic liver disease. In Trends in Alcoholic Liver Disease Research: Clinical and Scientific Aspects; Shimizu, I., Ed.; InTech: Rijeka, Croatia, 2011; pp. 23–40. [Google Scholar]
- Guy, J.; Peters, M.G. Liver disease in women: The influence of gender on epidemiology, natural history, and patient outcomes. Gastroenterol. Hepatol. 2013, 9, 633–639. [Google Scholar]


{kind=link}
| Total Participants | Men | Women | p-Value | ||
|---|---|---|---|---|---|
| Number | n (%) | 2582 | 1405 (54.4) | 1177 (45.6) | |
| Age | (years) | 52.6 ± 9.0 (25–80) | 52.7 ± 9.1 (25–80) | 52.4 ± 8.9 (26–77) | 0.317 |
| BMI | (kg/m2) | 23.2 ± 3.7 (14–48) | 24.0 ± 3.4 (15–42) | 22.2 ± 3.7 (14–48) | <0.001 |
| WC | (cm) | 82.4 ± 9.8 (56–131) | 84.6 ± 9.1 (58–126) | 79.9 ± 9.9 (56–131) | <0.001 |
| Current smokers | n (%) | 412 (16.0) | 366 (26.0) | 46 (3.9) | <0.001 |
| Drinkers | n (%) | 1504 (58.2) | 1044 (74.3) | 460 (39.1) | <0.001 |
| Alcohol quantity (g/week) | |||||
| None | n (%) | 1078 (41.8) | 361 (25.7) | 717 (60.9) | <0.001 |
| 0.1–69.9 | 545 (21.1) | 277 (19.7) | 268 (22.8) | ||
| 70–139.9 | 355 (13.7) | 244 (17.4) | 111 (9.4) | ||
| 140–279.9 | 571 (22.1) | 493 (35.1) | 78 (6.6) | ||
| ≥280 | 33 (1.3) | 30 (2.1) | 3 (0.3) | ||
| Drinking frequency | |||||
| Non-drinker | n (%) | 1078 (41.8) | 361 (25.7) | 717 (60.9) | <0.001 |
| Occasional drinker | 841 (32.6) | 495 (35.2) | 346 (29.4) | ||
| Daily drinker | 663 (25.7) | 549 (39.1) | 114 (9.7) | ||
| Regular exercise | n (%) | 671 (26.0) | 454 (32.3) | 217 (18.4) | <0.001 |
| Eating before going to bed | n (%) | 826 (32.0) | 527 (37.5) | 299 (25.4) | <0.001 |
| Custom of having breakfast | n (%) | 295 (11.4) | 180 (12.8) | 115 (9.8) | <0.05 |
| SBP | (mmHg) | 123.9 ± 16.9 (80–204) | 127.3 ± 16.0 (87–204) | 119.8 ± 17.1 (80–194) | <0.001 |
| DBP | (mmHg) | 78.1 ± 12.0 (43–128) | 81.6 ± 11.5 (46–128) | 73.9 ± 11.0 (43–116) | <0.001 |
| Hypertension | n (%) | 1208 (46.8) | 796 (56.7) | 412 (35.0) | <0.001 |
| T-CHO | (mg/dL) | 213.0 ± 35.1 (112–375) | 208.5 ± 33.8 (112–375) | 218.5 ± 35.8 (121–339) | <0.001 |
| TG | (mg/dL) | 110.5 ± 85.2 (26–1338) | 130.8 ± 103.5 (28–1338) | 86.2 ± 45.4 (26–423) | <0.001 |
| HDL-C | (mg/dL) | 67.1 ± 18.0 (26–145) | 60.5 ± 15.8 (26–137) | 74.9 ± 17.4 (28–145) | <0.001 |
| LDL-C | (mg/dL) | 129.3 ± 31.8 (29–298) | 128.3 ± 31.6 (29–298) | 130.5 ± 32.1 (48–247) | 0.151 |
| Dyslipidemia | n (%) | 718 (27.8) | 500 (35.6) | 218 (18.5) | <0.001 |
| FPG | (mg/dL) | 98.0 ± 16.7 (63–305) | 101.1 ± 17.7 (63–267) | 94.4 ± 14.5 (67–305) | <0.001 |
| HbA1c | (%) | 5.6 ± 0.55 (4.7–13.8) | 5.7 ± 0.57 (4.7–11.2) | 5.6 ± 0.53 (4.7–13.8) | 0.256 |
| IGT | n (%) | 1098 (42.5) | 701 (49.9) | 397 (33.7) | <0.001 |
| UA | (mg/dL) | 5.3 ± 1.4 (2–11) | 6.0 ± 1.2 (2–10) | 4.5 ± 1.0 (2–11) | <0.001 |
| ALT | (IU/L) | 22.8 ± 14.7 (5–178) | 27.0 ± 16.6 (6–178) | 17.7 ± 9.9 (5–125) | <0.001 |
| AST | (IU/L) | 23.9 ± 8.6 (8–126) | 25.7 ± 9.5 (10–126) | 21.8 ± 6.9 (8–101) | <0.001 |
| GGT | (IU/L) | 37.7 ± 40.7 (7–581) | 50.3 ± 48.2 (9–581) | 22.6 ± 21.1 (7–414) | <0.001 |
| HS-CRP | (mg/L) | 1.05 ± 2.97 (0.1–42.5) | 1.26 ± 3.61 (0.1–42.5) | 0.81 ± 1.95 (0.1–29.5) | <0.001 |
| H. pylori positivity | n (%) | 561 (21.7) | 335 (23.8) | 226 (19.2) | <0.005 |
| Men (n = 1405) | |||||||
| Baseline stage | Most recent stage | ||||||
| Number | Non- drinkers | Drinkers | |||||
| Alcohol quantity (g/week) | None | 0.1–69.9 | 70–139.9 | 140–279.9 | ≥280 | ||
| Non-drinkers | None | 361 (25.7%) | 335 (92.8%) | 21 (5.8%) | 2 (0.6%) | 3 (0.8%) | 0 (0%) |
| Drinkers | 0.1–69.9 | 277 (19.7%) | 71 (25.6) | 133 (48.0%) | 63 (22.7%) | 10 (3.6%) | 0 (0%) |
| 70–139.9 | 244 (17.4%) | 15 (6.1%) | 43 (17.6%) | 127 (52.0%) | 59 (24.2%) | 0 (0%) | |
| 140–279.9 | 493 (35.1%) | 13 (2.6%) | 14 (2.8%) | 79 (16.0%) | 366 (74.2%) | 21 (4.3%) | |
| ≥280 | 30 (2.1%) | 2 (6.7%) | 1 (3.3%) | 2 (6.7%) | 12 (40.0%) | 13 (43.3%) | |
| Women (n = 1177) | |||||||
| Baseline stage | Most recent stage | ||||||
| Number | Non- drinkers | Drinkers | |||||
| Alcohol quantity (g/week) | None | 0.1–69.9 | 70–139.9 | 140–279.9 | ≥280 | ||
| Non-drinkers | None | 717 (60.9%) | 665 (92.7%) | 39 (5.4%) | 11 (1.5%) | 2 (0.3%) | 0 (0%) |
| Drinkers | 0.1–69.9 | 268 (22.8%) | 69 (25.7) | 154 (57.5%) | 41 (15.3%) | 4 (1.5%) | 0 (0%) |
| 70–139.9 | 111 (9.4%) | 11 (9.9%) | 37 (33.3%) | 50 (45.0%) | 13 (11.7%) | 0 (0%) | |
| 140–279.9 | 78 (6.6%) | 2 (2.6%) | 7 (9.0%) | 14 (17.9%) | 54 (69.2%) | 1 (1.3%) | |
| ≥280 | 3 (0.3%) | 0 (0%) | 0 (0%) | 0 (0%) | 2 (66.7%) | 1 (33.3%) | |
| Men (n = 1405) | |||||
| Baseline stage | Most recent stage | ||||
| Number | Non-drinkers | Drinkers | |||
| Drinking frequency | Non-drinking | Occasional drinking | Daily drinking | ||
| Non-drinkers | Non-drinking | 361 (25.7%) | 335 (92.8%) | 22 (6.1%) | 4 (1.1%) |
| Drinkers | Occasional drinking | 495 (35.2%) | 83 (16.8) | 349 (70.5%) | 63 (12.7%) |
| Daily drinking | 549 (39.1%) | 18 (3.3%) | 66 (12.0%) | 465 (84.7%) | |
| Women (n = 1177) | |||||
| Baseline stage | Most recent stage | ||||
| Number | Non-drinkers | Drinkers | |||
| Drinking frequency | Non-drinking | Occasional drinking | Daily drinking | ||
| Non-drinkers | Non-drinking | 717 (60.9%) | 665 (92.7%) | 48 (6.7%) | 4 (0.6%) |
| Drinkers | Occasional drinking | 346 (29.4%) | 75 (21.7) | 249 (72.0%) | 22 (6.4%) |
| Daily drinking | 114 (9.7%) | 7 (6.1%) | 18 (15.8%) | 89 (78.1%) | |
| Men (n = 1405) | ||||||
| Baseline stage | Most recent stage | |||||
| EE (−) | EE (+) | |||||
| Grade A | Grade B | Grade C | Grade D | |||
| EE (−) | 1405 (100%) | 1194 (85.0%) | 182 (13.0%) | 24 (1.7%) | 4 (0.3%) | 1 (0.1%) |
| Women (n = 1177) | ||||||
| Baseline stage | Most recent stage | |||||
| EE (−) | EE (+) | |||||
| Grade A | Grade B | Grade C | Grade D | |||
| EE (−) | 1177 (100%) | 1098 (93.3%) | 72 (6.1%) | 7 (0.6%) | 0 (0%) | 0 (0%) |
| Alcohol Quantity (g/Week) | OR (95% CI) | OR a (95% CI) | OR b (95% CI) | OR c (95% CI) | OR d (95% CI) | |
|---|---|---|---|---|---|---|
| Men (n = 1405) | ||||||
| Non-drinkers | None | 1 | 1 | 1 | 1 | 1 |
| Drinkers | 1.246 (0.908–1.709) | 1.277 (0.930–1.753) | 1.208 (0.879–1.659) | 1.234 (0.899–1.693) | 1.252 (0.907–1.726) | |
| 0.1–69.9 | 0.938 (0.595–1.476) | 0.938 (0.595–1.476) | 0.929 (0.589–1.466) | 0.952 (0.604–1.502) | 0.971 (0.609–1.547) | |
| 70–139.9 | 1.420 (0.947–2.128) | 1.420 (0.947–2.128) | 1.384 (0.921–2.078) | 1.428 (0.951–2.144) | 1.443 (0.954–2.182) | |
| 140–279.9 | 1.275 (0.894–1.817) | 1.275 (0.894–1.817) | 1.228 (0.862–1.749) | 1.239 (0.867–1.769) | 1.255 (0.875–1.799) | |
| ≥280 | 1.680 (0.720–3.923) | 1.680 (0.720–3.923) | 1.591 (0.681–3.717) | 1.677 (0.715–3.934) | 2.014 (0.848–4.787) | |
| <50 years (n = 468) | ||||||
| Non-drinkers | None | 1 | 1 | 1 | 1 | 1 |
| Drinkers | 2.178 (1.125–4.217) | 2.205 (1.126–4.316) | 2.128 (1.094–4.140) | 2.171 (1.124–4.190) | 2.312 (1.171–4.564) | |
| 0.1–69.9 | 1.073 (0.442–2.608) | 1.131 (0.458–2.791) | 1.052 (0.427–2.590) | 1.085 (0.448–2.631) | 1.154 (0.461–2.885) | |
| 70–139.9 | 2.506 (1.175–5.346) | 2.665 (1.232–5.764) | 2.431 (1.135–5.209) | 2.581 (1.205–5.527) | 2.878 (1.302–6.361) | |
| 140–279.9 | 2.609 (1.284–5.301) | 2.525 (1.222–5.221) | 2.559 (1.260–5.200) | 2.559 (1.255–5.218) | 2.666 (1.283–5.542) | |
| ≥280 | 3.613 (1.004–13.00) | 3.621 (0.990–13.24) | 3.869 (1.056–14.17) | 3.624 (1.015–12.94) | 4.549 (1.228–16.85) | |
| ≥50 years (n = 937) | ||||||
| Non-drinkers | None | 1 | 1 | 1 | 1 | 1 |
| Drinkers | 1.003 (0.696–1.446) | 1.047 (0.723–1.517) | 0.979 (0.679–1.413) | 0.987 (0.685–1.423) | 1.009 (0.694–1.466) | |
| 0.1–69.9 | 0.959 (0.565–1.628) | 0.989 (0.578–1.693) | 0.966 (0.569–1.639) | 0.967 (0.566–1.650) | 0.989 (0.572–1.709) | |
| 70–139.9 | 1.122 (0.683–1.841) | 1.151 (0.699–1.898) | 1.112 (0.676–1.827) | 1.122 (0.682–1.847) | 1.134 (0.682–1.883) | |
| 140–279.9 | 0.961 (0.633–1.457) | 1.010 (0.662–1.541) | 0.923 (0.609–1.399) | 0.928 (0.614–1.404) | 0.945 (0.621–1.438) | |
| ≥280 | 1.059 (0.314–3.576) | 1.220 (0.350–4.248) | 0.934 (0.274–3.182) | 1.025 (0.304–3.458) | 1.227 (0.354–4.255) | |
| Women (n = 1177) | ||||||
| Non-drinkers | None | 1 | 1 | 1 | 1 | 1 |
| Drinkers | 0.956 (0.604–1.512) | 1.059 (0.666–1.683) | 0.983 (0.612–1.580) | 1.003 (0.634–1.586) | 1.078 (0.666–1.747) | |
| 0.1–69.9 | 0.630 (0.327–1.212) | 0.686 (0.355–1.327) | 0.650 (0.337–1.257) | 0.648 (0.337–1.249) | 0.692 (0.353–1.356) | |
| 70–139.9 | 0.768 (0.327–1.800) | 0.847 (0.360–1.992) | 0.806 (0.338–1.923) | 0.818 (0.346–1.931) | 0.911 (0.375–2.210) | |
| 140–279.9 | 2.195 (1.141–4.221) | 2.755 (1.393–5.449) | 2.399 (1.214–4.741) | 2.427 (1.261–4.670) | 3.040 (1.504–6.146) | |
| ≥280 | 7.152 (1.265–40.45) | 11.18 (1.830–68.29) | 10.18 (1.252–82.73) | 7.531 (1.367–41.50) | 13.26 (1.735–101.4) | |
| <50 years (n = 413) | ||||||
| Non-drinkers | None | 1 | 1 | 1 | 1 | 1 |
| Drinkers | 1.626 (0.716–3.694) | 1.638 (0.704–3.811) | 1.719 (0.735–4.018) | 1.687 (0.724–3.927) | 1.764 (0.736–4.231) | |
| 0.1–69.9 | 1.024 (0.326–3.212) | 1.017 (0.319–3.237) | 1.056 (0.336–3.323) | 1.046 (0.324–3.382) | 1.072 (0.328–3.505) | |
| 70–139.9 | 1.604 (0.437–5.884) | 1.617 (0.450–5.808) | 1.865 (0.480–7.242) | 1.584 (0.425–5.906) | 1.873 (0.481–7.299) | |
| 140–279.9 | 2.553 (0.805–8.093) | 2.708 (0.789–9.291) | 3.014 (0.876–10.37) | 2.810 (0.904–8.736) | 3.074 (0.940–10.05) | |
| ≥280 | 22.03 (4.919–98.62) | 24.21 (5.891–99.46) | 33.96 (3.184–362.1) | 19.90 (6.319–62.64) | 30.87 (3.693–258.1) | |
| ≥50 years (n = 764) | ||||||
| Non-drinkers | None | 1 | 1 | 1 | 1 | 1 |
| Drinkers | 0.759 (0.429–1.344) | 0.885 (0.497–1.576) | 0.747 (0.414–1.347) | 0.788 (0.447–1.389) | 0.853 (0.461–1.581) | |
| 0.1–69.9 | 0.516 (0.230–1.162) | 0.594 (0.261–1.350) | 0.526 (0.232–1.193) | 0.530 (0.236–1.192) | 0.589 (0.253–1.370) | |
| 70–139.9 | 0.519 (0.161–1.675) | 0.606 (0.185–1.986) | 0.528 (0.159–1.751) | 0.555 (0.171–1.799) | 0.619 (0.182–2.110) | |
| 140–279.9 | 2.285 (1.026–5.088) | 2.928 (1.281–6.690) | 2.209 (0.960–5.079) | 2.425 (1.075–5.470) | 3.149 (1.230–8.064) | |
| ≥280 | (−) | (−) | (−) | (−) | (−) | |
| Drinking Frequency | OR (95% CI) | OR a (95% CI) | OR b (95% CI) | OR c (95% CI) | OR d (95% CI) | |
|---|---|---|---|---|---|---|
| Men (n = 1405) | ||||||
| Non-drinkers | None | 1 | 1 | 1 | 1 | 1 |
| Drinkers | Occasional | 1.259 (0.880–1.802) | 1.298 (0.904–1.863) | 1.236 (0.863–1.771) | 1.263 (0.882–1.809) | 1.294 (0.896–1.867) |
| Daily | 1.234 (0.871–1.748) | 1.261 (0.888–1.789) | 1.184 (0.836–1.676) | 1.209 (0.854–1.713) | 1.215 (0.853–1.731) | |
| <50 years (n = 468) | ||||||
| Non-drinkers | None | 1 | 1 | 1 | 1 | 1 |
| Drinkers | Occasional | 1.879 (0.926–3.815) | 1.929 (0.938–3.966) | 1.854 (0.909–3.782) | 1.897 (0.938–3.836) | 2.051 (0.986–4.268) |
| Daily | 2.588 (1.278–5.242) | 2.597 (1.259–5.353) | 2.515 (1.237–5.112) | 2.536 (1.252–5.136) | 2.692 (1.298–5.586) | |
| ≥50 years (n = 937) | ||||||
| Non-drinkers | None | 1 | 1 | 1 | 1 | 1 |
| Drinkers | Occasional | 1.116 (0.728–1.710) | 1.151 (0.745–1.778) | 1.113 (0.726–1.705) | 1.105 (0.719–1.699) | 1.146 (0.738–1.779) |
| Daily | 0.930 (0.619–1.395) | 0.978 (0.649–1.474) | 0.892 (0.595–1.339) | 0.910 (0.608–1.361) | 0.917 (0.609–1.381) | |
| Women (n = 1177) | ||||||
| Non-drinkers | None | 1 | 1 | 1 | 1 | 1 |
| Drinkers | Occasional | 0.610 (0.336–1.106) | 0.668 (0.368–1.213) | 0.633 (0.345–1.160) | 0.639 (0.352–1.158) | 0.690 (0.374–1.273) |
| Daily | 1.996 (1.121–3.554) | 2.329 (1.281–4.234) | 2.109 (1.159–3.838) | 2.121 (1.193–3.768) | 2.444 (1.320–4.524) | |
| <50 years (n = 413) | ||||||
| Non-drinkers | None | 1 | 1 | 1 | 1 | 1 |
| Drinkers | Occasional | 1.069 (0.395–2.895) | 1.050 (0.387–2.852) | 1.127 (0.412–3.079) | 1.094 (0.397–3.020) | 1.147 (0.409–3.220) |
| Daily | 3.378 (1.234–9.247) | 3.721 (1.275–10.86) | 3.892 (1.288–11.76) | 3.620 (1.343–9.755) | 4.030 (1.404–11.57) | |
| ≥50 years (n = 764) | ||||||
| Non-drinkers | None | 1 | 1 | 1 | 1 | 1 |
| Drinkers | Occasional | 0.472 (0.219–1.016) | 0.546 (0.251–1.185) | 0.484 (0.222–1.056) | 0.490 (0.228–1.056) | 0.553 (0.249–1.230) |
| Daily | 1.603 (0.783–3.282) | 1.957 (0.936–4.091) | 1.522 (0.724–3.197) | 1.676 (0.819–3.431) | 1.860 (0.833–4.154) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sogabe, M.; Okahisa, T.; Kagawa, M.; Ueda, H.; Kagemoto, K.; Tanaka, H.; Kida, Y.; Tomonari, T.; Taniguchi, T.; Miyamoto, H.; et al. Influence of Alcohol Consumption on the Development of Erosive Esophagitis in Both Sexes: A Longitudinal Study. Nutrients 2022, 14, 4760. https://doi.org/10.3390/nu14224760
Sogabe M, Okahisa T, Kagawa M, Ueda H, Kagemoto K, Tanaka H, Kida Y, Tomonari T, Taniguchi T, Miyamoto H, et al. Influence of Alcohol Consumption on the Development of Erosive Esophagitis in Both Sexes: A Longitudinal Study. Nutrients. 2022; 14(22):4760. https://doi.org/10.3390/nu14224760
Chicago/Turabian StyleSogabe, Masahiro, Toshiya Okahisa, Miwako Kagawa, Hiroyuki Ueda, Kaizo Kagemoto, Hironori Tanaka, Yoshifumi Kida, Tetsu Tomonari, Tatsuya Taniguchi, Hiroshi Miyamoto, and et al. 2022. "Influence of Alcohol Consumption on the Development of Erosive Esophagitis in Both Sexes: A Longitudinal Study" Nutrients 14, no. 22: 4760. https://doi.org/10.3390/nu14224760