
Maternal Docosahexaenoic Acid Exposure Needed to Achieve Maternal–Newborn EQ

 , ,
, ,
Abstract
:1. Introduction
2. Subjects and Methods
2.1. Subjects
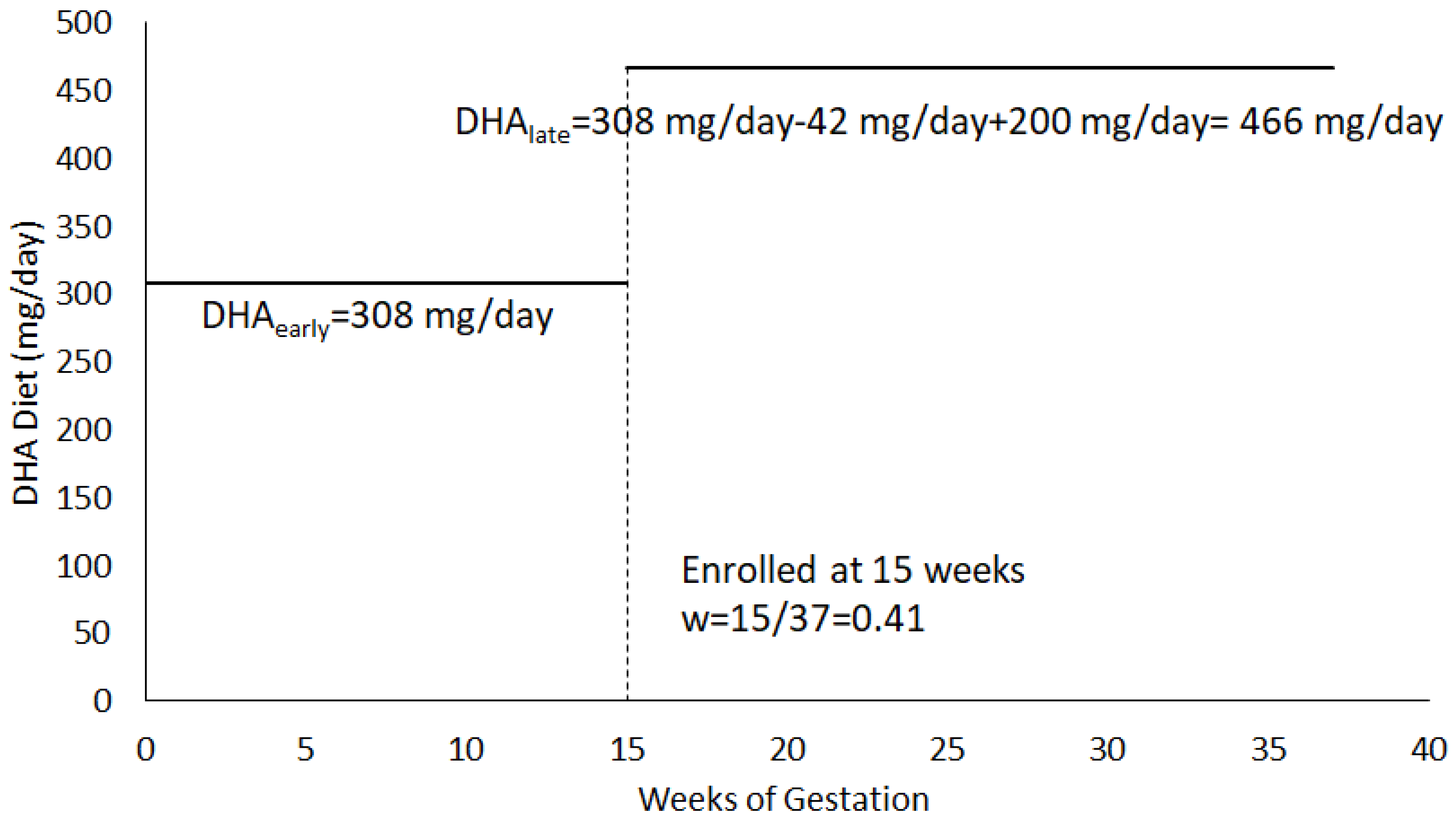
2.2. DHA Exposure
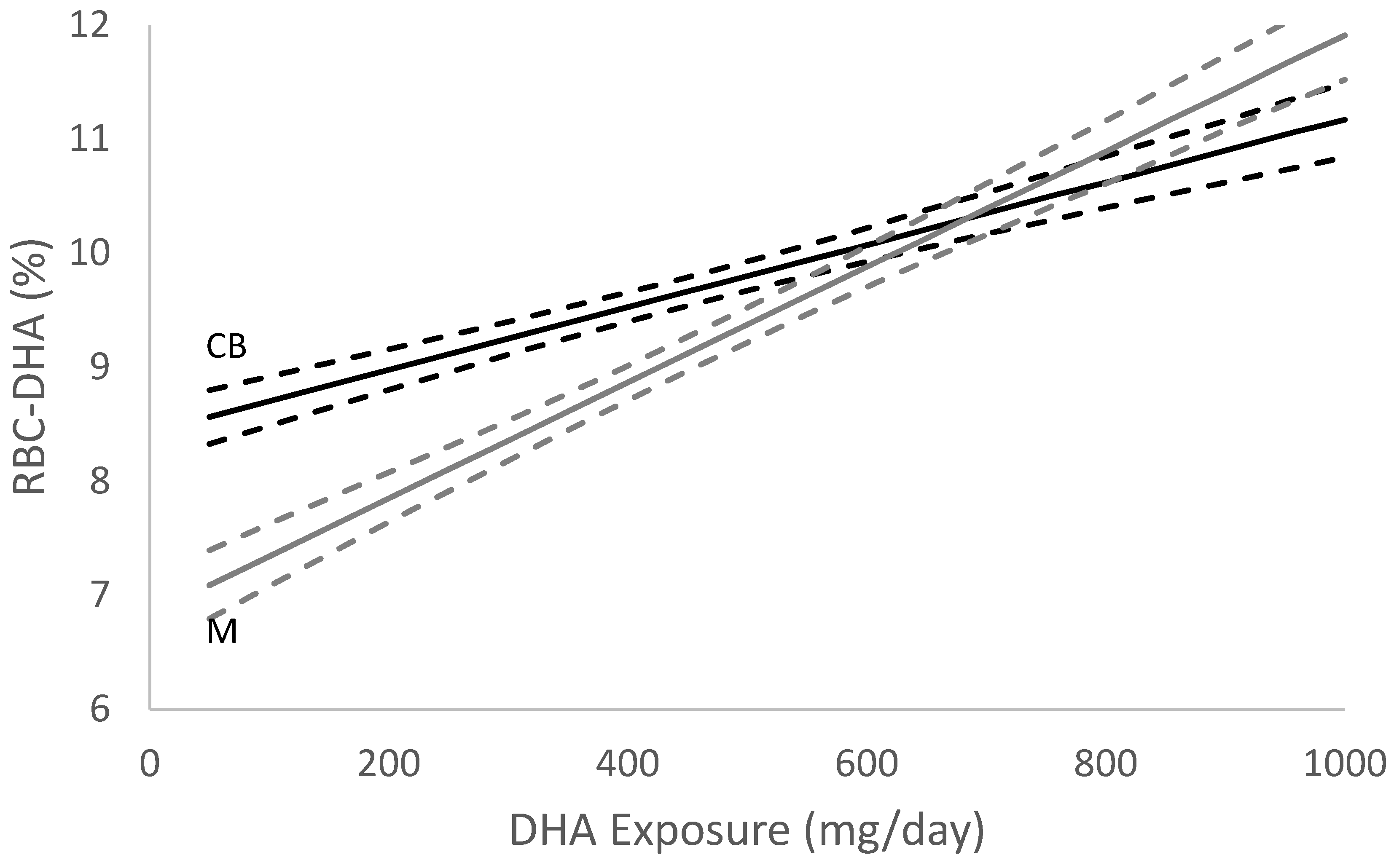
2.3. DHA Status
2.4. Ethics
2.5. Statistics
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhang, Z.; Fulgoni, V.; Kris-Etherton, P.M.; Mitmesser, S.H. Dietary Intakes of EPA and DHA Omega-3 Fatty Acids among US Childbearing-Age and Pregnant Women: An Analysis of NHANES 2001–2014. Nutrients 2018, 10, 416. [Google Scholar] [CrossRef] [PubMed]
- Middleton, P.; Gomersall, J.C.; Gould, J.F.; Shepherd, E.; Olsen, S.F.; Makrides, M. Omega-3 fatty acid addition during pregnancy. Cochrane Database Syst. Rev. 2018, 11, Cd003402. [Google Scholar] [CrossRef]
- Kuipers, R.S.; Luxwolda, M.F.; Sango, W.S.; Kwesigabo, G.; Dijck-Brouwer, D.A.; Muskiet, F.A. Maternal DHA EQ during pregnancy and lactation is reached at an erythrocyte DHA content of 8 g/100 g fatty acids. J. Nutr. 2011, 141, 418–427. [Google Scholar] [CrossRef]
- Luxwolda, M.F.; Kuipers, R.S.; Sango, W.S.; Kwesigabo, G.; Dijck-Brouwer, D.A.; Muskiet, F.A. A maternal erythrocyte DHA content of approximately 6 g% is the DHA status at which intrauterine DHA biomagnifications turns into bioattenuation and postnatal infant DHA EQ is reached. Eur. J. Nutr. 2012, 51, 665–675. [Google Scholar] [CrossRef] [PubMed]
- Markhus, M.W.; Rasinger, J.D.; Malde, M.K.; Frøyland, L.; Skotheim, S.; Braarud, H.C.; Stormark, K.M.; Graff, I.E. Docosahexaenoic Acid Status in Pregnancy Determines the Maternal Docosahexaenoic Acid Status 3-, 6- and 12 Months Postpartum. Results from a Longitudinal Observational Study. PLoS ONE 2015, 10, e0136409. [Google Scholar] [CrossRef] [PubMed]
- Gustafson, K.M.; Christifano, D.N.; Hoyer, D.; Schmidt, A.; Carlson, S.E.; Colombo, J.; Mathis, N.B.; Sands, S.A.; Chollet-Hinton, L.; Brown, A.R.; et al. Prenatal docosahexaenoic acid effect on maternal-infant DHA-EQ and fetal neurodevelopment: A randomized clinical trial. Pediatr. Res. 2021, 1–10. [Google Scholar] [CrossRef]
- Carlson, S.E.; Gajewski, B.J.; Valentine, C.J.; Kerling, E.H.; Weiner, C.P.; Cackovic, M.; Buhimschi, C.S.; Rogers, L.K.; Sands, S.A.; Brown, A.R.; et al. Higher dose docosahexaenoic acid supplementation during pregnancy and early preterm birth: A randomised, double-blind, adaptive-design superiority trial. EClinicalMedicine 2021, 36, 100905. [Google Scholar] [CrossRef]
- Kuratko, C. Food-frequency questionnaire for assessing long-chain ω-3 fatty-acid intake: Re: Assessing long-chain ω-3 polyunsaturated fatty acids: A tailored food-frequency questionnaire is better. Nutrition 2013, 29, 807–808. [Google Scholar] [CrossRef] [PubMed]
- Crawford, S.; Christifano, D.; Kerling, E.; Gajewski, B.; Valentine, C.; Gustafson, K.; Mathis, N.; Camargo, J.; Gibbs, H.; Sullivan, D.; et al. Validation of an abbreviated food frequency questionnaire for estimating DHA intake of pregnant women in the United States. Prostaglandins Leukot. Essent. Fat. Acids 2022, 177, 102398. [Google Scholar] [CrossRef]
- Christifano, D.; Crawford, S.; Lee, G.; Gajewski, B.; Carlson, S. Utility of a 7- question online screener for DHA intake. Prostaglandins Leukot. Essent. Fat. Acids 2022, 177, 102399. [Google Scholar] [CrossRef]
- Carlson, S.E.; Colombo, J.; Gajewski, B.J.; Gustafson, K.M.; Mundy, D.; Yeast, J.; Georgieff, M.K.; Markley, L.A.; Kerling, E.H.; Shaddy, D.J. DHA supplementation and pregnancy outcomes. Am. J. Clin. Nutr. 2013, 97, 808–815. [Google Scholar] [CrossRef] [PubMed]
- Peng, Y.M.; Zhang, T.Y.; Wang, Q.; Zetterström, R.; Strandvik, B. Fatty acid composition in breast milk and serum phospholipids of healthy term Chinese infants during first 6 weeks of life. Acta Paediatr. 2007, 96, 1640–1645. [Google Scholar] [CrossRef] [PubMed]
- Ghebremeskel, K.; Leighfield, M.; Leaf, A.; Costeloe, K.; Crawford, M. Fatty acid composition of plasma and red cell phospholipids of preterm babies fed on breast milk and formulae. Eur. J. Pediatr. 1995, 154, 46–52. [Google Scholar] [CrossRef]
- Brenna, J.T.; Varamini, B.; Jensen, R.G.; Diersen-Schade, D.A.; Boettcher, J.A.; Arterburn, L.M. Docosahexaenoic and arachidonic acid concentrations in human breast milk worldwide. Am. J. Clin. Nutr. 2007, 85, 1457–1464. [Google Scholar] [CrossRef] [PubMed]
- Jackson, K.H.; Harris, W.S. Harmonizing blood DHA levels in pregnancy studies: An interlaboratory investigation. Prostaglandins Leukot. Essent. Fat. Acids 2022, 179, 102417. [Google Scholar] [CrossRef] [PubMed]
- The U.S. Departments of Agriculture (USDA) and of Health and Human Services (HHS). Dietary Guidelines for Americans, 2020–2025, 9th edition. 2022. Available online: https://dietaryguidelines.gov/ (accessed on 1 July 2022).
- March of Dimes. Omega-3 Fatty Acids during Pregnancy. Available online: http://www.marchofdimes.com/pnhec/159_55030.asp (accessed on 15 July 2022).
- Simopoulos, A.P.; Leaf, A.; Salem, N., Jr. Workshop statement on the essentiality of and recommended dietary intakes for Omega-6 and Omega-3 fatty acids. Prostaglandins Leukot. Essent. Fat. Acids. 2000, 63, 119–121. [Google Scholar] [CrossRef] [PubMed]
- Koletzko, B.; Lien, E.; Agostoni, C.; Böhles, H.; Campoy, C.; Cetin, I.; Decsi, T.; Dudenhausen, J.W.; Dupont, C.; Forsyth, S. The roles of long-chain polyunsaturated fatty acids in pregnancy, lactation and infancy: Review of current knowledge and consensus recommendations. J. Perinat. Med. 2008, 36, 5–14. [Google Scholar] [CrossRef]
- U.S. Department of Agriculture, A.R.S. FoodData Central Published: 2019. Available online: https://fdc.nal.usda.gov/ (accessed on 15 July 2022).
- Kerling, E.H.; Hilton, J.M.; Thodosoff, J.M.; Wick, J.; Colombo, J.; Carlson, S.E. Effect of Prenatal Docosahexaenoic Acid Supplementation on Blood Pressure in Children With Overweight Condition or Obesity: A Secondary Analysis of a Randomized Clinical Trial. JAMA Netw. Open 2019, 2, e190088. [Google Scholar] [CrossRef]
- Colombo, J.; Gustafson, K.; Gajewski, B.J.; Shaddy, D.J.; Kerling, E.; Thodosoff, J.M.; Doty, T.; Brez, C.C.; Carlson, S.E. Prenatal DHA supplementation and infant attention. Pediatr. Res. 2016, 80, 656–662. [Google Scholar] [CrossRef] [PubMed]
- Birch, E.E.; Hoffman, D.R.; Uauy, R.; Birch, D.G.; Prestidge, C. Visual acuity and the essentiality of docosahexaenoic acid and arachidonic acid in the diet of term infants. Pediatr Res. 1998, 44, 201–209. [Google Scholar] [CrossRef]
- Uhl, O.; Demmelmair, H.; Segura, M.T.; Florido, J.; Rueda, R.; Campoy, C.; Koletzko, B. Effects of obesity and gestational diabetes mellitus on placental phospholipids. Diabetes Res. Clin. Pract. 2015, 109, 364–371. [Google Scholar] [CrossRef] [PubMed]
- Walter, J.D.; Remm, S.; Seeger, M.A. Fatty acid transporter MFSD2A is a multifunctional gatekeeper in brain and placenta. Nat. Struct. Mol. Biol. 2022, 29, 504–506. [Google Scholar] [CrossRef] [PubMed]
- Bakouei, F.; Delavar, M.A.; Mashayekh-Amiri, S.; Esmailzadeh, S.; Taheri, Z. Efficacy of n-3 fatty acids supplementation on the prevention of pregnancy induced-hypertension or preeclampsia: A systematic review and meta-analysis. Taiwan. J. Obstet. Gynecol. 2020, 59, 8–15. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Mean | Median | Standard Deviation | |
|---|---|---|---|
| DHA intake from diet (DHAintakel) (mg/day) | 88.3 | 70.0 | 79.5 |
| DHA exposure in early pregnancy including diet and supplements (DHAearly) (mg/day) | 160.8 | 122.0 | 135.0 |
| DHA exposure in late pregnancy (DHAlate) (mg/day) | 682.3 | 842.0 | 387.3 |
| Total DHA exposure during pregnancy (mg/day) | 445.5 | 487.9 | 228.5 |
| Pre-pregnancy BMI (kg/m2) | 27.9 | 26.5 | 7.0 |
| Age at enrollment (years) | 30.2 | 30.2 | 5.5 |
| GDM (n (%) diagnosed) | 11.3% |
| Estimate | Standard Error | t Value | p-Value | |
|---|---|---|---|---|
| Intercept | −1.6544 | 0.1373 | −12.051 | <0.001 |
| Total DHA Exposure | 0.0026 | 0.003 | 9.346 | <0.001 |
| Centered Pre-Pregnancy BMI | −0.0442 | 0.089 | −4.983 | <0.001 |
| Centered Age at Enrollment | 0.0827 | 0.0116 | 7.121 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Christifano, D.N.; Gustafson, K.M.; Carlson, S.E.; Sultanna, N.; Brown, A.; Sands, S.A.; Colombo, J.; Gajewski, B.J. Maternal Docosahexaenoic Acid Exposure Needed to Achieve Maternal–Newborn EQ. Nutrients 2022, 14, 3300. https://doi.org/10.3390/nu14163300
Christifano DN, Gustafson KM, Carlson SE, Sultanna N, Brown A, Sands SA, Colombo J, Gajewski BJ. Maternal Docosahexaenoic Acid Exposure Needed to Achieve Maternal–Newborn EQ. Nutrients. 2022; 14(16):3300. https://doi.org/10.3390/nu14163300
Chicago/Turabian StyleChristifano, Danielle N., Kathleen M. Gustafson, Susan E. Carlson, Nasrin Sultanna, Alexandra Brown, Scott A. Sands, John Colombo, and Byron J. Gajewski. 2022. "Maternal Docosahexaenoic Acid Exposure Needed to Achieve Maternal–Newborn EQ" Nutrients 14, no. 16: 3300. https://doi.org/10.3390/nu14163300