
Effects of Internet-Based Nutrition and Exercise Interventions on the Prevention and Treatment of Sarcopenia in the Elderly

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Sample
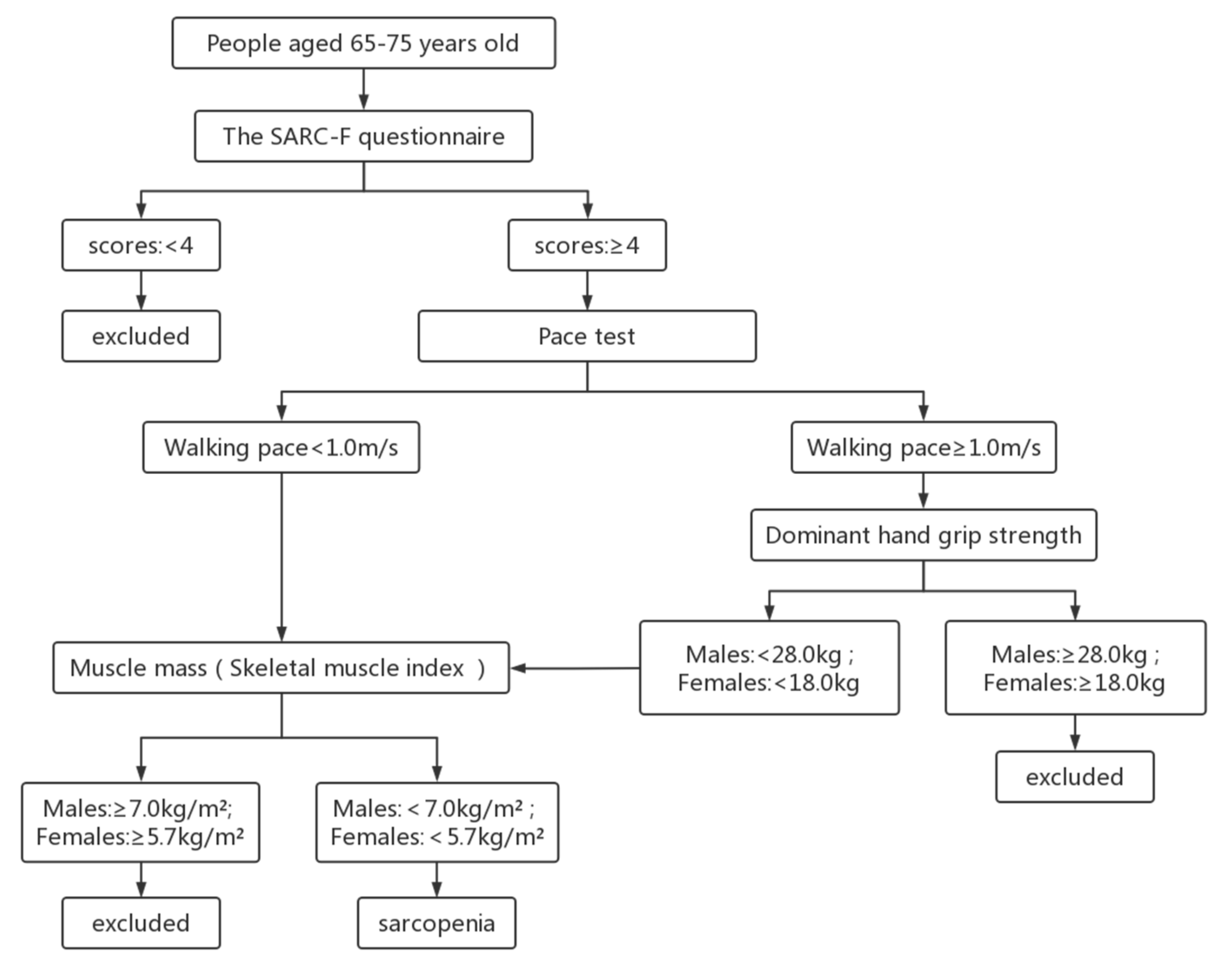
2.2. Sarcopenia Criteria
2.3. Interventions
2.4. Data Collection
2.5. Statistical Analysis
3. Results
3.1. Study Population and Use Frequency of APP by Participants
3.2. Baseline Comparisons
3.3. Comparison of Diet and Exercise Status before and after the Intervention
3.4. Comparison of Quantity and Function of Skeletal Muscle before and after the Intervention

{kind=link}
| Variable | Control Group | Comprehensive Group | Nutrition Group | Exercise Group | p | p1 | p2 | p3 | p4 | p5 | p6 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Energy, kJ | 0.118 | 0.061 | 0.034 | 0.364 | 0.594 | 0.293 | 0.154 | ||||
| Baseline | 7266 ± 3441 | 7204 ± 2789 | 7704 ± 3773 | 7711 ± 3914 | |||||||
| After the intervention | 7362 ± 3081 | 8857 ± 3844 | 9154 ± 2744 | 8343 ± 4176 | |||||||
| Total protein, g | 0.081 | 0.059 | 0.124 | 0.930 | 0.924 | 0.038 | 0.094 | ||||
| Baseline | 70.29 ± 39.24 | 69.10 ± 23.12 | 83.07 ± 41.70 | 73.06 ± 41.09 | |||||||
| After the intervention | 78.08 ± 45.47 | 92.28 ± 45.67 | 97.25 ± 34.59 | 76.74 ± 36.07 | |||||||
| High-quality protein, g | 0.022 | 0.017 | 0.076 | 0.990 | 0.778 | 0.012 | 0.067 | ||||
| Baseline | 37.98 ± 27.66 | 37.72 ± 12.10 | 45.25 ± 27.56 | 38.49 ± 32.31 | |||||||
| After the intervention | 36.26 ± 15.89 | 51.25 ± 26.54 | 54.62 ± 23.20 | 38.28 ± 20.05 | |||||||
| BMI, kg/m2 | <0.001 | 0.006 | 0.022 | 0.080 | 0.943 | <0.001 | <0.001 | ||||
| Baseline | 22.67 ± 3.07 | 23.68 ± 3.87 | 22.26 ± 2.4 | 23.15 ± 2.89 | |||||||
| After the intervention | 23.35 ± 3.14 | 25.30 ± 3.70 | 24.60 ± 3.22 | 23.26 ± 2.82 | |||||||
| Average daily time of moderate physical activity, median (P25, P75) | 0.759 | ||||||||||
| Baseline | 0.00 (0.00, 14.28) | 0.00 (0.00, 0.00) | 0.00 (0.00, 17.68) | 0.00 (0.00, 37.50) | |||||||
| After the intervention | 0.00 (0.00, 0.00) | 0.00 (0.00, 2.89) | 0.00 (0.00, 25.71) | 10.00 (0.00, 45.00) | |||||||
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Akimov, A.V.; Gemueva, K.A.; Semenova, N.K. The Seventh Population Census in the PRC: Results and Prospects of the Country’s Demographic Development. Her. Russ. Acad. Sci. 2022, 91, 724–735. [Google Scholar] [CrossRef] [PubMed]
- Bouchard, D.R.; Heroux, M.; Janssen, I. Association between muscle mass, leg strength, and fat mass with physical function in older adults: Influence of age and sex. J. Aging Health 2011, 23, 313–328. [Google Scholar] [CrossRef] [PubMed]
- Batsis, J.A.; Villareal, D.T. Sarcopenic obesity in older adults: Aetiology, epidemiology and treatment strategies. Nat. Rev. Endocrinol. 2018, 14, 513–537. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Chou, M.Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307. [Google Scholar] [CrossRef]
- Zhang, Y.; Chen, X.; Hou, L.; Lin, X.; Qin, D.; Wang, H.; Hai, S.; Cao, L.; Dong, B. Prevalence and Risk Factors Governing the Loss of Muscle Function in Elderly Sarcopenia Patients: A longitudinal Study in China with 4 Years of Follow-Up. J. Nutr. Health Aging 2020, 24, 518–524. [Google Scholar] [CrossRef]
- van den Helder, J.; Mehra, S.; van Dronkelaar, C.; Ter Riet, G.; Tieland, M.; Visser, B.; Krose, B.; Engelbert, R.; Weijs, P. Blended home-based exercise and dietary protein in community-dwelling older adults: A cluster randomized controlled trial. J. Cachexia Sarcopenia Muscle 2020, 11, 1590–1602. [Google Scholar] [CrossRef]
- Scotto, D.P.A.; McSwiney, F.T.; Hone, M.; McMorrow, A.M.; Lynch, G.; De Vito, G.; Egan, B. Effects of a Long Chain n-3 Polyunsaturated Fatty Acid-rich Multi-ingredient Nutrition Supplement on Body Composition and Physical Function in Older Adults with Low Skeletal Muscle Mass. J. Diet Suppl. 2021, 1–16. [Google Scholar] [CrossRef]
- Reinders, I.; Wijnhoven, H.; Jyvakorpi, S.K.; Suominen, M.H.; Niskanen, R.; Bosmans, J.E.; Brouwer, I.A.; Fluitman, K.S.; Klein, M.; Kuijper, L.D.; et al. Effectiveness and cost-effectiveness of personalised dietary advice aiming at increasing protein intake on physical functioning in community-dwelling older adults with lower habitual protein intake: Rationale and design of the PROMISS randomised controlled trial. BMJ Open 2020, 10, e40637. [Google Scholar]
- Chanet, A.; Verlaan, S.; Salles, J.; Giraudet, C.; Patrac, V.; Pidou, V.; Pouyet, C.; Hafnaoui, N.; Blot, A.; Cano, N.; et al. Supplementing Breakfast with a Vitamin D and Leucine-Enriched Whey Protein Medical Nutrition Drink Enhances Postprandial Muscle Protein Synthesis and Muscle Mass in Healthy Older Men. J. Nutr. 2017, 147, 2262–2271. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; Zhang, Y.; Zeng, X.; Cheng, Y.; Tang, L.; Hong, D.; Yang, X. Lycopene ameliorates insulin resistance and increases muscle capillary density in aging via activation of SIRT1. J. Nutr. Biochem. 2022, 99, 108862. [Google Scholar] [CrossRef]
- Daly, R.M.; Gianoudis, J.; Prosser, M.; Kidgell, D.; Ellis, K.A.; O’Connell, S.; Nowson, C.A. The effects of a protein enriched diet with lean red meat combined with a multi-modal exercise program on muscle and cognitive health and function in older adults: Study protocol for a randomised controlled trial. Trials 2015, 16, 339. [Google Scholar] [CrossRef] [PubMed]
- McConell, G.K. It’s well and truly time to stop stating that AMPK regulates glucose uptake and fat oxidation during exercise. Am. J. Physiol. Endocrinol. Metab. 2020, 318, E564–E567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kemmler, W.; Kohl, M.; Jakob, F.; Engelke, K.; von Stengel, S. Effects of High Intensity Dynamic Resistance Exercise and Whey Protein Supplements on Osteosarcopenia in Older Men with Low Bone and Muscle Mass. Final Results of the Randomized Controlled FrOST Study. Nutrients 2020, 12, 2341. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.; Zhang, J.; Chang, C.; Zhu, H.; Huang, C.; Cao, W.; Jiang, Y.; He, G.; Mo, B.; Fu, P.; et al. Chinese expert consensus on nutrition and exercise intervention for sarcopenia syndrome (excerpt). Acta Nutr. Sin. 2015, 37, 320–324. [Google Scholar]
- Sun, X.; Yan, W.; Zhou, H.; Wang, Z.; Zhang, X.; Huang, S.; Li, L. Internet use and need for digital health technology among the elderly: A cross-sectional survey in China. BMC Public Health 2020, 20, 1386. [Google Scholar] [CrossRef]
- Pereira, K.; Phillips, B.; Johnson, C.; Vorderstrasse, A. Internet delivered diabetes self-management education: A review. Diabetes Technol. Ther. 2015, 17, 55–63. [Google Scholar] [CrossRef]
- Zhang, Y.; Tan, Y.; Huang, X.; Zhang, Z.; Bai, J.; Zhang, M.; Huang, Y.; Cheng, J.; Wang, J.; Bao, Z. Analysis of the prevalence and related risk factors of sarcopenia among the elderly in Shanghai community. Geriatr. Health Care 2018, 24, 608–613. [Google Scholar]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyere, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [Green Version]
- Song, J.; Zang, J.; Tang, H.; Li, W.; Wang, Z.; Zou, S.; Jia, X. Relative validity of food frequency questionnaire for estimating dietary nutrients intake. Wei Sheng Yan Jiu J. Hyg. Res. 2016, 45, 743–748. [Google Scholar]
- Janssen, I.; Shepard, D.S.; Katzmarzyk, P.T.; Roubenoff, R. The healthcare costs of sarcopenia in the United States. J. Am. Geriatr. Soc. 2004, 52, 80–85. [Google Scholar] [CrossRef]
- Cawthon, P.M.; Lui, L.Y.; Taylor, B.C.; McCulloch, C.E.; Cauley, J.A.; Lapidus, J.; Orwoll, E.; Ensrud, K.E. Clinical Definitions of Sarcopenia and Risk of Hospitalization in Community-Dwelling Older Men: The Osteoporotic Fractures in Men Study. J. Gerontol. A Biol. Sci. Med. Sci. 2017, 72, 1383–1389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cawthon, P.M.; Lui, L.Y.; McCulloch, C.E.; Cauley, J.A.; Paudel, M.L.; Taylor, B.; Schousboe, J.T.; Ensrud, K.E. Sarcopenia and Health Care Utilization in Older Women. J. Gerontol. A Biol. Sci. Med. Sci. 2017, 72, 95–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, L.F.; Chan, Y.H.; Tay, A.; Jayasundram, J.; Low, N.A.; Merchant, R.A. Practicality and Reliability of Self Vs Administered Rapid Geriatric Assessment Mobile App. J. Nutr. Health Aging 2021, 25, 1064–1069. [Google Scholar] [CrossRef]
- Zhao, Y.C.; Zhao, M.; Song, S. Online Health Information Seeking Behaviors among Older Adults: Systematic Scoping Review. J. Med. Internet Res. 2022, 24, e34790. [Google Scholar] [CrossRef] [PubMed]
- Yang, K.; Oh, D.; Noh, J.M.; Yoon, H.G.; Sun, J.M.; Kim, H.K.; Zo, J.I.; Shim, Y.M.; Ko, H.; Lee, J.; et al. Feasibility of an Interactive Health Coaching Mobile App to Prevent Malnutrition and Muscle Loss in Esophageal Cancer Patients Receiving Neoadjuvant Concurrent Chemoradiotherapy: Prospective Pilot Study. J. Med. Internet Res. 2021, 23, e28695. [Google Scholar] [CrossRef] [PubMed]
- Hanach, N.I.; McCullough, F.; Avery, A. The Impact of Dairy Protein Intake on Muscle Mass, Muscle Strength, and Physical Performance in Middle-Aged to Older Adults with or without Existing Sarcopenia: A Systematic Review and Meta-Analysis. Adv. Nutr. 2019, 10, 59–69. [Google Scholar] [CrossRef] [Green Version]
- Jarzaguet, M.; Polakof, S.; David, J.; Migne, C.; Joubrel, G.; Efstathiou, T.; Remond, D.; Mosoni, L.; Dardevet, D. A meal with mixed soy/whey proteins is as efficient as a whey meal in counteracting the age-related muscle anabolic resistance only if the protein content and leucine levels are increased. Food Funct. 2018, 9, 6526–6534. [Google Scholar] [CrossRef]
- Mitchell, C.J.; Della, G.P.; Petersen, A.C.; Cameron-Smith, D.; Markworth, J.F. Soy protein ingestion results in less prolonged p70S6 kinase phosphorylation compared to whey protein after resistance exercise in older men. J. Int. Soc. Sports Nutr. 2015, 12, 6. [Google Scholar] [CrossRef] [Green Version]
- Bauer, J.; Biolo, G.; Cederholm, T.; Cesari, M.; Cruz-Jentoft, A.J.; Morley, J.E.; Phillips, S.; Sieber, C.; Stehle, P.; Teta, D.; et al. Evidence-based recommendations for optimal dietary protein intake in older people: A position paper from the PROT-AGE Study Group. J. Am. Med. Dir. Assoc. 2013, 14, 542–559. [Google Scholar] [CrossRef]
- Han, P.; Zhao, J.; Guo, Q.; Wang, J.; Zhang, W.; Shen, S.; Wang, X.; Dong, R.; Ma, Y.; Kang, L.; et al. Incidence, Risk Factors, and the Protective Effect of High Body Mass Index against Sarcopenia in Suburb-Dwelling Elderly Chinese Populations. J. Nutr. Health Aging 2016, 20, 1056–1060. [Google Scholar] [CrossRef]
- Cheng, Q.; Zhu, X.; Zhang, X.; Li, H.; Du, Y.; Hong, W.; Xue, S.; Zhu, H. A cross-sectional study of loss of muscle mass corresponding to sarcopenia in healthy Chinese men and women: Reference values, prevalence, and association with bone mass. J. Bone Miner. Metab. 2014, 32, 78–88. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Cui, M.; Yu, K.; Zhang, X.W.; Li, C.W.; Nie, X.D.; Wang, F. Effects of nutrition supplementation and physical exercise on muscle mass, muscle strength and fat mass among sarcopenic elderly: A randomized controlled trial. Appl. Physiol. Nutr. Metab. 2021, 46, 494–500. [Google Scholar] [CrossRef]
- Cusack, L.; Del, M.C.; Chalmers, I.; Gibson, E.; Hoffmann, T.C. Educational interventions to improve people’s understanding of key concepts in assessing the effects of health interventions: A systematic review. Syst. Rev. 2018, 7, 68. [Google Scholar] [CrossRef] [PubMed]
- Witham, M.D.; Chawner, M.; Biase, S.; Offord, N.; Todd, O.; Clegg, A.; Sayer, A.A. Content of exercise programmes targeting older people with sarcopenia or frailty—Findings from a UK survey. J. Frailty Sarcopenia Falls 2020, 5, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Mittaz, H.A.; Mathieu, N.; Lenoble-Hoskovec, C.; Swanenburg, J.; de Bie, R.; Hilfiker, R. Effects of three home-based exercise programmes regarding falls, quality of life and exercise-adherence in older adults at risk of falling: Protocol for a randomized controlled trial. BMC Geriatr. 2019, 19, 13. [Google Scholar] [CrossRef] [Green Version]
- Yoo, S.Z.; No, M.H.; Heo, J.W.; Park, D.H.; Kang, J.H.; Kim, S.H.; Kwak, H.B. Role of exercise in age-related sarcopenia. J. Exerc. Rehabil. 2018, 14, 551–558. [Google Scholar] [CrossRef]
- Cheng, K.Y.; Chow, S.K.; Hung, V.W.; Wong, C.H.; Wong, R.M.; Tsang, C.S.; Kwok, T.; Cheung, W.H. Diagnosis of sarcopenia by evaluating skeletal muscle mass by adjusted bioimpedance analysis validated with dual-energy X-ray absorptiometry. J. Cachexia Sarcopenia Muscle 2021, 12, 2163–2173. [Google Scholar] [CrossRef]

| App Evaluation Feedback Completed Times | Comprehensive Group (n) | Nutrition Group (n) | Exercise Group (n) | X2 | p |
|---|---|---|---|---|---|
| 5 times and above | 24 | 30 | 25 | 1.967 | 0.742 |
| 3 to 4 times | 20 | 14 | 18 | ||
| 1 to 2 times | 6 | 6 | 7 |
| Variable | Control Group | Comprehensive Group | Nutrition Group | Exercise Group | F/X2 | p |
|---|---|---|---|---|---|---|
| Gender, n (%) | 0.779 | 0.854 | ||||
| Male | 7 (13.7) | 8 (16.0) | 9 (18.0) | 10 (20.0) | ||
| Women | 44 (86.3) | 42 (84.0) | 41 (82.0) | 40 (80.0) | ||
| Age, y | 69.88 ± 3.29 | 70.16 ± 4.32 | 68.18 ± 3.93 | 69.72 ± 3.60 | 2.740 | 0.044 |
| Education level, n (%) | 77.518 | <0.001 | ||||
| High school and above | 0 (0) | 14 (28.0) | 21 (42.0) | 4 (8.0) | ||
| Junior high school | 10 (19.6) | 24 (48.0) | 26 (52.0) | 16 (32.0) | ||
| Primary school and illiteracy | 41 (80.4) | 12 (24.0) | 3 (6.0) | 30 (60.0) | ||
| Marital status, n (%) | 9.979 | 0.019 | ||||
| In marriage | 47 (92.2) | 36 (72.0) | 39(78.0) | 45 (90.0) | ||
| Divorced or widowed | 4 (7.8) | 14 (28.0) | 11(22.0) | 5 (10.0) | ||
| Pre-retirement occupation, n (%) | 58.302 | <0.001 | ||||
| Mental work mainly | 7 (13.7) | 22 (44.0) | 44 (88.0) | 19 (38.0) | ||
| Physical labor mainly | 44 (86.3) | 28 (56.0) | 6 (12.0) | 31 (62.0) | ||
| Smoking, n (%) | 2 (3.9) | 6 (12.0) | 6 (12.0) | 8 (16.0) | 6.807 | 0.339 |
| Energy, kj | 7266 ± 3441 | 7204 ± 2789 | 7704 ± 3773 | 7711 ± 3914 | 0.306 | 0.821 |
| Total protein, g | 70.29 ± 39.24 | 69.10 ± 23.12 | 83.07 ± 41.70 | 73.06 ± 41.09 | 1.466 | 0.225 |
| High-quality protein, g | 37.98 ± 27.66 | 37.72 ± 12.10 | 45.25 ± 27.56 | 38.49 ± 32.31 | 0.924 | 0.430 |
| BMI, kg/m2 | 22.67 ± 3.07 | 23.68 ± 3.87 | 22.26 ± 2.4 | 23.15 ± 2.89 | 1.947 | 0.123 |
| Skeletal muscle mass, kg | 13.98 ± 2.37 | 15.33 ± 2.95 | 14.27 ± 2.23 | 14.37 ± 2.20 | 2.850 | 0.039 |
| The score of propensity score | 0.59 ± 0.18 | 0.56 ± 0.18 | 0.34 ± 0.15 | 0.49 ± 0.19 | 19.063 | <0.001 |
| Variable | Control Group | Comprehensive Group | Nutrition Group | Exercise Group | p | p1 | p2 | p3 | p4 | p5 | p6 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Skeletal muscle mass, kg | <0.001 | <0.001 | <0.001 | 0.243 | 0.158 | <0.001 | 0.004 | ||||
| Baseline | 13.98 ± 2.37 | 15.33 ± 2.95 | 14.27 ± 2.23 | 14.37 ± 2.20 | |||||||
| After the intervention | 13.88 ± 2.39 | 16.42 ± 2.98 | 15.52 ± 2.39 | 14.44 ± 2.28 | |||||||
| Skeletal muscle mass/height2 in male, kg/m2 | 0.109 | 0.115 | 0.062 | 0.775 | 0.676 | 0.115 | 0.056 | ||||
| Baseline | 5.64 ± 0.62 | 6.23 ± 1.08 | 5.64 ± 0.54 | 5.79 ± 0.51 | |||||||
| After the intervention | 5.59 ± 0.61 | 6.64 ± 1.05 | 6.14 ± 0.70 | 5.81 ± 0.53 | |||||||
| Skeletal muscle mass/height2 in female, kg/m2 | <0.001 | <0.001 | 0.001 | 0.263 | 0.320 | <0.001 | 0.018 | ||||
| Baseline | 6.11 ± 0.61 | 6.88 ± 1.11 | 6.13 ± 0.68 | 6.33 ± 0.32 | |||||||
| After the intervention | 6.05 ± 0.52 | 7.37 ± 1.04 | 6.87 ± 0.74 | 6.38 ± 0.39 | |||||||
| Skeletal muscle mass/body weight | 0.005 | 0.001 | 0.040 | 0.002 | 0.485 | 0.874 | 0.562 | ||||
| Baseline | 0.25 ± 0.03 | 0.26 ± 0.03 | 0.25 ± 0.03 | 0.25 ± 0.03 | |||||||
| After the intervention | 0.24 ± 0.03 | 0.26 ± 0.03 | 0.25 ± 0.03 | 0.25 ± 0.03 | |||||||
| Skeletal muscle mass/BMI | 0.005 | 0.001 | 0.077 | 0.006 | 0.233 | 0.425 | 0.583 | ||||
| Baseline | 0.62 ± 0.11 | 0.65 ± 0.10 | 0.64 ± 0.10 | 0.63 ± 0.11 | |||||||
| After the intervention | 0.60 ± 0.11 | 0.65 ± 0.10 | 0.64 ± 0.10 | 0.63 ± 0.12 | |||||||
| Skeletal muscle mass/body fat percentage | 0.040 | 0.011 | 0.070 | 0.013 | 0.712 | 0.894 | 0.792 | ||||
| Baseline | 0.95 ± 0.43 | 0.83 ± 0.27 | 0.76 ± 0.23 | 0.84 ± 0.30 | |||||||
| After the intervention | 0.89 ± 0.40 | 0.85 ± 0.29 | 0.78 ± 0.26 | 0.88 ± 0.38 | |||||||
| Balance test (third posture) | 0.679 | 0.427 | 0.233 | 0.527 | 0.598 | 0.851 | 0.487 | ||||
| Baseline | 1.69 ± 0.58 | 1.62 ± 0.70 | 1.78 ± 0.51 | 1.72 ± 0.45 | |||||||
| After the intervention | 1.52 ± 0.50 | 1.66 ± 0.66 | 1.82 ± 0.48 | 1.74 ± 0.44 | |||||||
| 4-m timed walking test | 0.732 | 0.636 | 0.269 | 0.483 | 0.475 | 0.825 | 0.586 | ||||
| Baseline | 5.12 ± 1.21 | 5.19 ± 2.09 | 5.08 ± 1.15 | 5.01 ± 1.29 | |||||||
| After the intervention | 5.01 ± 1.83 | 5.13 ± 2.38 | 5.06 ± 1.16 | 4.94 ± 1.01 | |||||||
| Timing sitting and standing test | 0.942 | 0.549 | 0.871 | 0.849 | 0.722 | 0.662 | 0.996 | ||||
| Baseline | 10.71 ± 3.41 | 11.31 ± 5.63 | 11.73 ± 4.57 | 11.66 ± 4.02 | |||||||
| After the intervention | 10.72 ± 4.34 | 9.82 ± 4.54 | 12.02 ± 3.44 | 11.51 ± 4.44 | |||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Z.; Xu, X.; Gao, S.; Wu, C.; Song, Q.; Shi, Z.; Su, J.; Zang, J. Effects of Internet-Based Nutrition and Exercise Interventions on the Prevention and Treatment of Sarcopenia in the Elderly. Nutrients 2022, 14, 2458. https://doi.org/10.3390/nu14122458
Wang Z, Xu X, Gao S, Wu C, Song Q, Shi Z, Su J, Zang J. Effects of Internet-Based Nutrition and Exercise Interventions on the Prevention and Treatment of Sarcopenia in the Elderly. Nutrients. 2022; 14(12):2458. https://doi.org/10.3390/nu14122458
Chicago/Turabian StyleWang, Zhengyuan, Xin Xu, Shanxi Gao, Chunxiang Wu, Qi Song, Zehuan Shi, Jin Su, and Jiajie Zang. 2022. "Effects of Internet-Based Nutrition and Exercise Interventions on the Prevention and Treatment of Sarcopenia in the Elderly" Nutrients 14, no. 12: 2458. https://doi.org/10.3390/nu14122458