
The Effects of Berry Polyphenols on the Gut Microbiota and Blood Pressure: A Systematic Review of Randomized Clinical Trials in Humans

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Information Sources
2.2. Search Strategy
2.3. Inclusion and Exclusion Criteria
2.4. Data Extraction
2.5. Quality Assessment
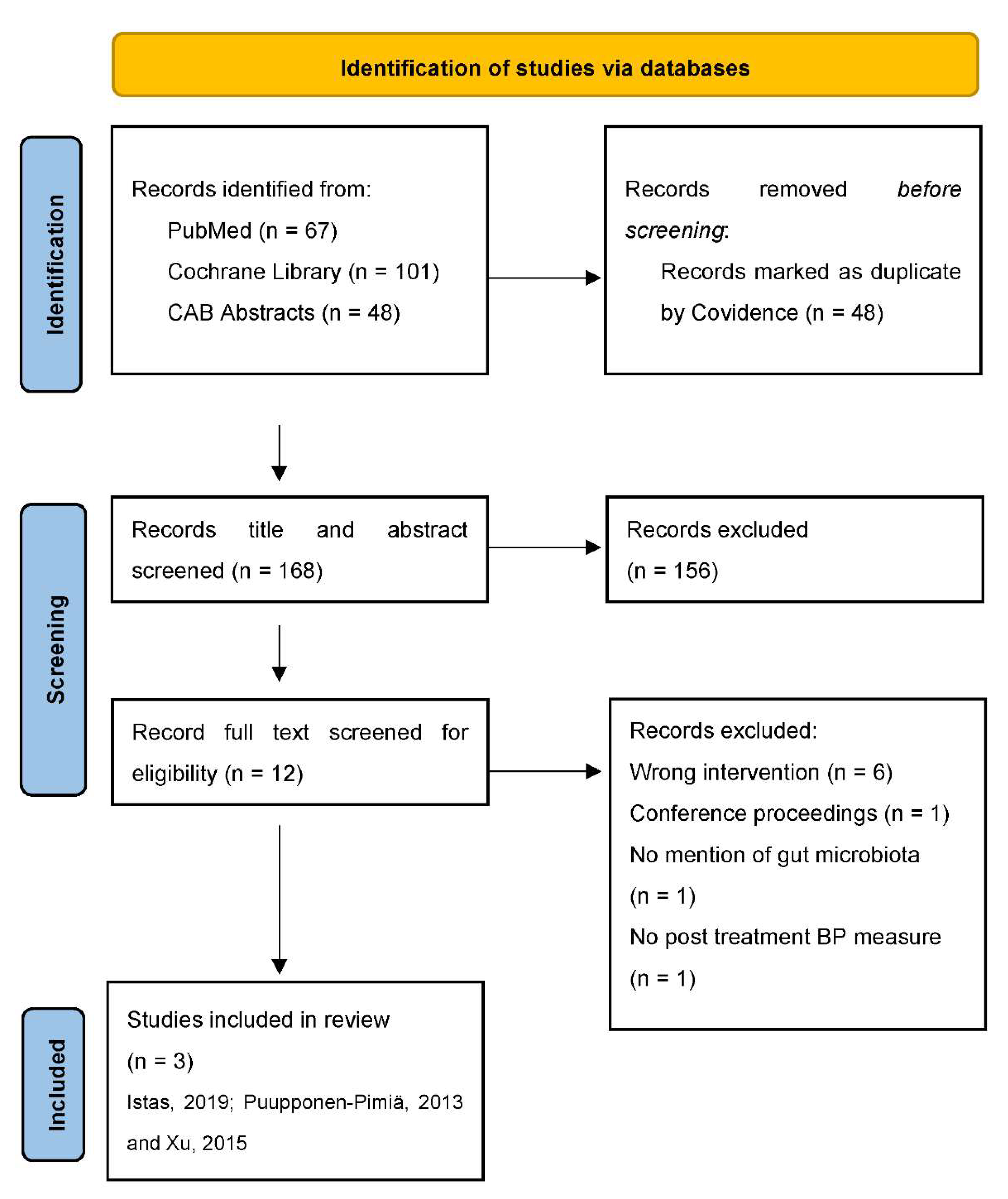
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Borghi, C.; Tsioufis, K.; Agabiti-Rosei, E.; Burnier, M.; Cicero, A.F.G.; Clement, D.; Coca, A.; Desideri, G.; Grassi, G.; Lovic, D.; et al. Nutraceuticals and blood pressure control: A European Society of Hypertension position document. J. Hypertens. 2020, 38, 799–812. [Google Scholar] [CrossRef]
- Cicero, A.F.G.; Grassi, D.; Tocci, G.; Galletti, F.; Borghi, C.; Ferri, C. Nutrients and Nutraceuticals for the Management of High Normal Blood Pressure: An Evidence-Based Consensus Document. High Blood Press. Cardiovasc. Prev. 2019, 26, 9–25. [Google Scholar] [CrossRef] [PubMed]
- Cicero, A.F.G.; Veronesi, M.; Fogacci, F. Dietary Intervention to Improve Blood Pressure Control: Beyond Salt Restriction. High Blood Press. Cardiovasc. Prev. 2021, 28, 547–553. [Google Scholar] [CrossRef] [PubMed]
- Perez-Jimenez, J.; Neveu, V.; Vos, F.; Scalbert, A. Identification of the 100 richest dietary sources of polyphenols: An application of the Phenol-Explorer database. Eur. J. Clin. Nutr. 2010, 64 (Suppl. S3), S112–S120. [Google Scholar] [CrossRef] [PubMed]
- Manach, C.; Mazur, A.; Scalbert, A. Polyphenols and prevention of cardiovascular diseases. Curr. Opin. Lipidol. 2005, 16, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.; Vance, T.M.; Chun, O.K. Estimated intake and major food sources of flavonoids among US adults: Changes between 1999–2002 and 2007–2010 in NHANES. Eur. J. Nutr. 2016, 55, 833–843. [Google Scholar] [CrossRef] [PubMed]
- Cassidy, A.; O’Reilly, E.J.; Kay, C.; Sampson, L.; Franz, M.; Forman, J.P.; Curhan, G.; Rimm, E.B. Habitual intake of flavonoid subclasses and incident hypertension in adults. Am. J. Clin. Nutr. 2011, 93, 338–347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jennings, A.; Welch, A.A.; Fairweather-Tait, S.J.; Kay, C.; Minihane, A.M.; Chowienczyk, P.; Jiang, B.; Cecelja, M.; Spector, T.; Macgregor, A.; et al. Higher anthocyanin intake is associated with lower arterial stiffness and central blood pressure in women. Am. J. Clin. Nutr. 2012, 96, 781–788. [Google Scholar] [CrossRef] [Green Version]
- Stevens, S.L.; Wood, S.; Koshiaris, C.; Law, K.; Glasziou, P.; Stevens, R.J.; McManus, R.J. Blood pressure variability and cardiovascular disease: Systematic review and meta-analysis. Br. Med. J. 2016, 354, i4098. [Google Scholar] [CrossRef] [Green Version]
- Tjelle, T.E.; Holtung, L.; Bohn, S.K.; Aaby, K.; Thoresen, M.; Wiik, S.A.; Paur, I.; Karlsen, A.S.; Retterstol, K.; Iversen, P.O.; et al. Polyphenol-rich juices reduce blood pressure measures in a randomised controlled trial in high normal and hypertensive volunteers. Br. J. Nutr. 2015, 114, 1054–1063. [Google Scholar] [CrossRef] [Green Version]
- Erlund, I.; Koli, R.; Alfthan, G.; Marniemi, J.; Puukka, P.; Mustonen, P.; Mattila, P.; Jula, A. Favorable effects of berry consumption on platelet function, blood pressure, and HDL cholesterol. Am. J. Clin. Nutr. 2008, 87, 323–331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basu, A.; Du, M.; Leyva, M.J.; Sanchez, K.; Betts, N.M.; Wu, M.; Aston, C.E.; Lyons, T.J. Blueberries decrease cardiovascular risk factors in obese men and women with metabolic syndrome. J. Nutr. 2010, 140, 1582–1587. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, S.A.; Figueroa, A.; Navaei, N.; Wong, A.; Kalfon, R.; Ormsbee, L.T.; Feresin, R.G.; Elam, M.L.; Hooshmand, S.; Payton, M.E.; et al. Daily blueberry consumption improves blood pressure and arterial stiffness in postmenopausal women with pre- and stage 1-hypertension: A randomized, double-blind, placebo-controlled clinical trial. J. Acad. Nutr. Diet. 2015, 115, 369–377. [Google Scholar] [CrossRef] [PubMed]
- Stote, K.S.; Sweeney, M.I.; Kean, T.; Baer, D.J.; Novotny, J.A.; Shakerley, N.L.; Chandrasekaran, A.; Carrico, P.M.; Melendez, J.A.; Gottschall-Pass, K.T. The effects of 100% wild blueberry (Vaccinium angustifolium) juice consumption on cardiometablic biomarkers: A randomized, placebo-controlled, crossover trial in adults with increased risk for type 2 diabetes. BMC Nutr. 2017, 3, 45. [Google Scholar] [CrossRef]
- Garcia-Conesa, M.T.; Chambers, K.; Combet, E.; Pinto, P.; Garcia-Aloy, M.; Andres-Lacueva, C.; de Pascual-Teresa, S.; Mena, P.; Konic Ristic, A.; Hollands, W.J.; et al. Meta-Analysis of the Effects of Foods and Derived Products Containing Ellagitannins and Anthocyanins on Cardiometabolic Biomarkers: Analysis of Factors Influencing Variability of the Individual Responses. Int. J. Mol. Sci. 2018, 19, 694. [Google Scholar] [CrossRef] [Green Version]
- Feresin, R.G.; Johnson, S.A.; Pourafshar, S.; Campbell, J.C.; Jaime, S.J.; Navaei, N.; Elam, M.L.; Akhavan, N.S.; Alvarez-Alvarado, S.; Tenenbaum, G.; et al. Impact of daily strawberry consumption on blood pressure and arterial stiffness in pre- and stage 1-hypertensive postmenopausal women: A randomized controlled trial. Food Funct. 2017, 8, 4139–4149. [Google Scholar] [CrossRef]
- Stull, A.J.; Cash, K.C.; Champagne, C.M.; Gupta, A.K.; Boston, R.; Beyl, R.A.; Johnson, W.D.; Cefalu, W.T. Blueberries improve endothelial function, but not blood pressure, in adults with metabolic syndrome: A randomized, double-blind, placebo-controlled clinical trial. Nutrients 2015, 7, 4107–4123. [Google Scholar] [CrossRef]
- Bell, D.R.; Gochenaur, K. Direct vasoactive and vasoprotective properties of anthocyanin-rich extracts. J. Appl. Physiol. 2006, 100, 1164–1170. [Google Scholar] [CrossRef] [Green Version]
- Warner, E.F.; Rodriguez-Ramiro, I.; O’Connell, M.A.; Kay, C.D. Cardiovascular Mechanisms of Action of Anthocyanins May Be Associated with the Impact of Microbial Metabolites on Heme Oxygenase-1 in Vascular Smooth Muscle Cells. Molecules 2018, 23, 898. [Google Scholar] [CrossRef] [Green Version]
- Parichatikanond, W.; Pinthong, D.; Mangmool, S. Blockade of the renin-angiotensin system with delphinidin, cyanin, and quercetin. Planta Med. 2012, 78, 1626–1632. [Google Scholar] [CrossRef] [Green Version]
- Luca, S.V.; Macovei, I.; Bujor, A.; Miron, A.; Skalicka-Wozniak, K.; Aprotosoaie, A.C.; Trifan, A. Bioactivity of dietary polyphenols: The role of metabolites. Crit. Rev. Food Sci. Nutr. 2020, 60, 626–659. [Google Scholar] [CrossRef] [PubMed]
- Van Duynhoven, J.; Vaughan, E.E.; Jacobs, D.M.; Kemperman, R.A.; van Velzen, E.J.; Gross, G.; Roger, L.C.; Possemiers, S.; Smilde, A.K.; Dore, J.; et al. Metabolic fate of polyphenols in the human superorganism. Proc. Natl. Acad. Sci. USA 2011, 108 (Suppl. S1), 4531–4538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boto-Ordonez, M.; Urpi-Sarda, M.; Queipo-Ortuno, M.I.; Tulipani, S.; Tinahones, F.J.; Andres-Lacueva, C. High levels of Bifidobacteria are associated with increased levels of anthocyanin microbial metabolites: A randomized clinical trial. Food Funct. 2014, 5, 1932–1938. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Espin, J.C.; Gonzalez-Sarrias, A.; Tomas-Barberan, F.A. The gut microbiota: A key factor in the therapeutic effects of (poly)phenols. Biochem. Pharmacol. 2017, 139, 82–93. [Google Scholar] [CrossRef] [PubMed]
- Espley, R.V.; Butts, C.A.; Laing, W.A.; Martell, S.; Smith, H.; McGhie, T.K.; Zhang, J.; Paturi, G.; Hedderley, D.; Bovy, A.; et al. Dietary flavonoids from modified apple reduce inflammation markers and modulate gut microbiota in mice. J. Nutr. 2014, 144, 146–154. [Google Scholar] [CrossRef] [Green Version]
- Morais, C.A.; de Rosso, V.V.; Estadella, D.; Pisani, L.P. Anthocyanins as inflammatory modulators and the role of the gut microbiota. J. Nutr. Biochem. 2016, 33, 1–7. [Google Scholar] [CrossRef]
- Jennings, A.; Koch, M.; Bang, C.; Franke, A.; Lieb, W.; Cassidy, A. Microbial Diversity and Abundance of Parabacteroides Mediate the Associations between Higher Intake of Flavonoid-Rich Foods and Lower Blood Pressure. Hypertension 2021, 78, 1016–1026. [Google Scholar] [CrossRef]
- Igwe, E.O.; Charlton, K.E.; Probst, Y.C.; Kent, K.; Netzel, M.E. A systematic literature review of the effect of anthocyanins on gut microbiota populations. J. Hum. Nutr. Diet. 2019, 32, 53–62. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Gallegos, J.L.; Haskell-Ramsay, C.; Lodge, J.K. Effects of chronic consumption of specific fruit (berries, citrus and cherries) on CVD risk factors: A systematic review and meta-analysis of randomised controlled trials. Eur. J. Nutr. 2021, 60, 615–639. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Br. Med. J. 2021, 372, n71. [Google Scholar] [CrossRef]
- Rethlefsen, M.L.; Kirtley, S.; Waffenschmidt, S.; Ayala, A.P.; Moher, D.; Page, M.J.; Koffel, J.B.; Group, P.-S. PRISMA-S: An extension to the PRISMA Statement for Reporting Literature Searches in Systematic Reviews. Syst. Rev. 2021, 10, 39. [Google Scholar] [CrossRef] [PubMed]
- Clark, J.M.; Sanders, S.; Carter, M.; Honeyman, D.; Cleo, G.; Auld, Y.; Booth, D.; Condron, P.; Dalais, C.; Bateup, S.; et al. Improving the translation of search strategies using the Polyglot Search Translator: A randomized controlled trial. J. Med. Libr. Assoc. 2020, 108, 195–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cumpston, M.; Li, T.; Page, M.J.; Chandler, J.; Welch, V.A.; Higgins, J.P.; Thomas, J. Updated guidance for trusted systematic reviews: A new edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Database Syst. Rev. 2019, 10, ED000142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Istas, G.; Wood, E.; Le Sayec, M.; Rawlings, C.; Yoon, J.; Dandavate, V.; Cera, D.; Rampelli, S.; Costabile, A.; Fromentin, E.; et al. Effects of aronia berry (poly)phenols on vascular function and gut microbiota: A double-blind randomized controlled trial in adult men. Am. J. Clin. Nutr. 2019, 110, 316–329. [Google Scholar] [CrossRef] [PubMed]
- Puupponen-Pimia, R.; Seppanen-Laakso, T.; Kankainen, M.; Maukonen, J.; Torronen, R.; Kolehmainen, M.; Leppanen, T.; Moilanen, E.; Nohynek, L.; Aura, A.M.; et al. Effects of ellagitannin-rich berries on blood lipids, gut microbiota, and urolithin production in human subjects with symptoms of metabolic syndrome. Mol. Nutr. Food Res. 2013, 57, 2258–2263. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Ahrén, I.; Olsson, C.; Jeppsson, B.; Ahrné, S.; Molin, G. Oral and faecal microbiota in volunteers with hypertension in a double blind, randomised placebo controlled trial with probiotics and fermented bilberries. J. Funct. Foods 2015, 18, 275–288. [Google Scholar] [CrossRef]
- Stote, K.S.; Wilson, M.M.; Hallenbeck, D.; Thomas, K.; Rourke, J.M.; Sweeney, M.I.; Gottschall-Pass, K.T.; Gosmanov, A.R. Effect of Blueberry Consumption on Cardiometabolic Health Parameters in Men with Type 2 Diabetes: An 8-Week, Double-Blind, Randomized, Placebo-Controlled Trial. Curr. Dev. Nutr. 2020, 4, nzaa030. [Google Scholar] [CrossRef] [Green Version]
- Cerda, B.; Periago, P.; Espin, J.C.; Tomas-Barberan, F.A. Identification of urolithin a as a metabolite produced by human colon microflora from ellagic acid and related compounds. J. Agric. Food Chem. 2005, 53, 5571–5576. [Google Scholar] [CrossRef]
- Ras, R.T.; Streppel, M.T.; Draijer, R.; Zock, P.L. Flow-mediated dilation and cardiovascular risk prediction: A systematic review with meta-analysis. Int. J. Cardiol. 2013, 168, 344–351. [Google Scholar] [CrossRef]
- Blood Pressure Lowering Treatment Trialists Collaboration. Pharmacological blood pressure lowering for primary and secondary prevention of cardiovascular disease across different levels of blood pressure: An individual participant-level data meta-analysis. Lancet 2021, 397, 1625–1636. [Google Scholar] [CrossRef]
- Blanton, C.; He, Z.; Gottschall-Pass, K.T.; Sweeney, M.I. Probiotics Blunt the Anti-Hypertensive Effect of Blueberry Feeding in Hypertensive Rats without Altering Hippuric Acid Production. PLoS ONE 2015, 10, e0142036. [Google Scholar] [CrossRef] [PubMed]
- Shaughnessy, K.S.; Boswall, I.A.; Scanlan, A.P.; Gottschall-Pass, K.T.; Sweeney, M.I. Diets containing blueberry extract lower blood pressure in spontaneously hypertensive stroke-prone rats. Nutr. Res. 2009, 29, 130–138. [Google Scholar] [CrossRef] [PubMed]
- Basu, A.; Lyons, T.J. Strawberries, blueberries, and cranberries in the metabolic syndrome: Clinical perspectives. J. Agric. Food Chem. 2012, 60, 5687–5692. [Google Scholar] [CrossRef]
- Mai, V.; Katki, H.A.; Harmsen, H.; Gallaher, D.; Schatzkin, A.; Baer, D.J.; Clevidence, B. Effects of a controlled diet and black tea drinking on the fecal microflora composition and the fecal bile acid profile of human volunteers in a double-blinded randomized feeding study. J. Nutr. 2004, 134, 473–478. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.S.; Unno, T.; Kim, B.Y.; Park, M.S. Sex Differences in Gut Microbiota. World J. Men’s Health. 2020, 38, 48–60. [Google Scholar] [CrossRef]
- Environmental chemicals, the human microbiome, and health risk: A research strategy. In The National Academies Collection: Reports funded by National Institutes of Health; National Academy of Sciences: Washington, DC, USA, 2017.
- Buffet-Bataillon, S.; Rizk, G.; Cattoir, V.; Sassi, M.; Thibault, V.; Del Giudice, J.; Gangneux, J.P. Efficient and Quality-Optimized Metagenomic Pipeline Designed for Taxonomic Classification in Routine Microbiological Clinical Tests. Microorganisms 2022, 10, 711. [Google Scholar] [CrossRef]
- Ye, S.H.; Siddle, K.J.; Park, D.J.; Sabeti, P.C. Benchmarking Metagenomics Tools for Taxonomic Classification. Cell 2019, 178, 779–794. [Google Scholar] [CrossRef]
- Rowland, I.; Gibson, G.; Heinken, A.; Scott, K.; Swann, J.; Thiele, I.; Tuohy, K. Gut microbiota functions: Metabolism of nutrients and other food components. Eur. J. Nutr. 2018, 57, 1–24. [Google Scholar] [CrossRef] [Green Version]
- Valle-Gough, R.E.; Samaniego-Gámez, B.Y.; Apodaca-Hernández, J.E.; Chiappa-Carrara, F.X.; Rodríguez-Dorantes, M.; Arena-Ortiz, M.L. RNA-Seq Analysis on the Microbiota Associated with the White Shrimp (Litopenaeus vannamei) in Different Stages of Development. Appl. Sci. 2022, 12, 2483. [Google Scholar] [CrossRef]
- Babu, A.F.; Csader, S.; Mannisto, V.; Tauriainen, M.M.; Pentikainen, H.; Savonen, K.; Klavus, A.; Koistinen, V.; Hanhineva, K.; Schwab, U. Effects of exercise on NAFLD using non-targeted metabolomics in adipose tissue, plasma, urine, and stool. Sci. Rep. 2022, 12, 6485. [Google Scholar] [CrossRef]
- Clish, C.B. Metabolomics: An emerging but powerful tool for precision medicine. Cold Spring Harb. Mol. Case Stud. 2015, 1, a000588. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mennen, L.I.; Walker, R.; Bennetau-Pelissero, C.; Scalbert, A. Risks and safety of polyphenol consumption. Am. J. Clin. Nutr. 2005, 81, 326S–329S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basheer, L.; Kerem, Z. Interactions between CYP3A4 and Dietary Polyphenols. Oxid. Med. Cell. Longev. 2015, 2015, 854015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, J.S.; Piao, Y.J.; Kang, K.W. Effects of quercetin on the bioavailability of doxorubicin in rats: Role of CYP3A4 and P-gp inhibition by quercetin. Arch. Pharm. Res. 2011, 34, 607–613. [Google Scholar] [CrossRef]
- Galli, F. Interactions of polyphenolic compounds with drug disposition and metabolism. Curr. Drug Metab. 2007, 8, 830–838. [Google Scholar] [CrossRef]
- Szaefer, H.; Krajka-Kuzniak, V.; Ignatowicz, E.; Adamska, T.; Baer-Dubowska, W. Chokeberry (Aronia melanocarpa) juice modulates 7,12-dimethylbenz[a]anthracene induced hepatic but not mammary gland phase I and II enzymes in female rats. Environ. Toxicol. Pharmacol. 2011, 31, 339–346. [Google Scholar] [CrossRef]
- Strippoli, S.; Lorusso, V.; Albano, A.; Guida, M. Herbal-drug interaction induced rhabdomyolysis in a liposarcoma patient receiving trabectedin. BMC Complement Altern. Med. 2013, 13, 199. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.H.; Chao, P.D.; Hsiu, S.L.; Wen, K.C.; Hou, Y.C. Lethal quercetin-digoxin interaction in pigs. Life Sci. 2004, 74, 1191–1197. [Google Scholar] [CrossRef]
- Lacroix, S.; Klicic Badoux, J.; Scott-Boyer, M.P.; Parolo, S.; Matone, A.; Priami, C.; Morine, M.J.; Kaput, J.; Moco, S. A computationally driven analysis of the polyphenol-protein interactome. Sci. Rep. 2018, 8, 2232. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Category | Data | ||
|---|---|---|---|
| General Information | Title | Lead author contact details | |
| Year of publication | Study region | ||
| Journal name | IRB/REB approval | ||
| Registered clinical trial number | |||
| Characteristics of included studies | Blinding Methods Aim of study Randomization Study type Washout period for crossover design Duration of study Start date End date Study funding sources Study funding sources Possible Conflicts of interest for study authors Participants | Population description Sex Inclusion criteria Exclusion criteria Method of recruitment of participants Total number of participants (randomized at baseline) Dietary treatment 1 Dietary treatment 2 Form of control Dose of control Baseline health | |
| Baseline Population Characteristics | Control Age Sex Race Systolic BP (peripheral) Diastolic BP (peripheral) Systolic BP (central) Systolic BP (central) Diastolic BP (central) BMI Number of Participants | Treatment 1 Age Sex Race Systolic BP (peripheral) Diastolic BP (peripheral) Systolic BP (central) Systolic BP (central) Diastolic BP (central) BMI Number of Participants | Treatment 2 Age Sex Race Systolic BP (peripheral) Diastolic BP (peripheral) Systolic BP (central) Systolic BP (central) Diastolic BP (central) BMI Number of Participants |
| Intervention and Comparisons | Type of Biologicals Samples Time Point of Sample Collection (Military Time) | ||
| Outcomes | Outcome—Time Point 1 Outcome—Time Point 2 Outcome—Time Point 3 Impact on microbial community | Gut microflora Study dropout rate (number and percentage) Power calculation for sample size determination Statistical analysis Statistical design appropriate | Other comments |
| Istas, 2019 [34] | Puupponen-Pimiä, 2013 [35] | Xu, 2015 [36] | ||
|---|---|---|---|---|
| n of Participants (M/F) | 66 (66/0) | 32 (13/19) | 142 (92/50) | |
| Participant age | 23 ± 4 years | 51 ± 7 years | 66 ± 4 years | |
| Health status | Healthy | Metabolic syndrome | Hypertension | |
| Intervention | Aronia melanocarpa: “aronia whole fruit” capsules (12 mg polyphenols, 10 g berries) or Aronia melanocarpa: “aronia extract” capsules (116 mg polyphenols, 75 g berries) | 300 g fresh berries (100 g strawberry purée, 100 g frozen raspberries, 100 g frozen cloudberries) substituting other sources of carbohydrates normally consumed | Fruit drink (10 g fresh bilberries fermented with L. plantarum strain DSM 15313 with placebo probiotic powder) or fruit drink with probiotic powder, L. plantarum strain DSM 15313 (without bilberries) | |
| Control | Control capsules, matched in appearance to both intervention capsules, contains maltodextrin and no polyphenols | Usual diet with berry restriction | Placebo drink plus placebo probiotic powder (without bilberries or L. plantarum strain DSM 15313) | |
| Study design | Parallel (3 groups) | Parallel (2 groups) | Parallel (3 groups) | |
| Duration | 12 week intervention | 16 week (4 week run in with berry restriction, 8 week intervention, 4 week recovery period) | 14 week (2 week run in period, 12 week intervention) | |
| Impact on blood pressure | Change in blood pressure at 12 weeks (mmHg) Aronia whole fruit vs. control: PSBP −0.6 (−6.8, 5.6), PDBP −1.8 (−7.3, 3.7), CSBP −1.8 (−7.3, 3.8), CDBP −2.4 (−9.4, 4.6) Aronia extract vs. control: PSBP −0.4 (−6.7, 5.8), PDBP 0.8 (−4.8, 6.4), CSBP −1.1 (−6.7, 4.5), CDBP 1.2 (−5.8, 8.3) | Change in blood pressure at 12 weeks (mmHg) Berry: SBP −4.8 ± 5.9, DBP −2.8 ± 2.8 Control: SBP −8.2 ± 4.5, DBP −2.9 ± 3.1 | Change in blood pressure at 12 weeks (mmHg) Bilberries fermented by L. plantarum strain DSM 15313: SBP 1 (−6, 8), DBP 2 (−2, 8) L. plantarum strain DSM 15313: SBP −1 (7.25, 7.25), DBP −3 (−7, 2) Placebo control: SBP 1.5 (−5, 7.75), DBP −1 (−4, 5.5) | |
| Impact on microbial community | NC in fecal microbiota diversity Aronia whole fruit capsules: ↑ Bacteroides * Aronia extract capsules: ↑ Anaerostipes * Placebo capsules: ↑ Clostridium XiVb * | NC in fecal microbiota Diversity | NC in oral or fecal microbiota diversity | |
| Author, Year | Sequence Generation 1 | Allocation Concealment 2 | Blinding of Participant and Personnel 3 | Blinding of Outcome Assessor 4 | Incomplete Outcome Data 5 | Selective Outcome Reporting 6 | Other Sources of Bias 7 |
|---|---|---|---|---|---|---|---|
| Istas, 2019 [34] | Low risk | Low risk | Low risk | Low risk | Low risk | Low risk | Low risk |
| Puupponen-Pimiä, 2013 [35] | Low risk | Unclear | High Risk | Unclear | Low risk | Low risk | Unclear |
| Xu, 2015 [36] | Low risk | Low risk | High Risk | Unclear | Low risk | High risk | Unclear |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sweeney, M.; Burns, G.; Sturgeon, N.; Mears, K.; Stote, K.; Blanton, C. The Effects of Berry Polyphenols on the Gut Microbiota and Blood Pressure: A Systematic Review of Randomized Clinical Trials in Humans. Nutrients 2022, 14, 2263. https://doi.org/10.3390/nu14112263
Sweeney M, Burns G, Sturgeon N, Mears K, Stote K, Blanton C. The Effects of Berry Polyphenols on the Gut Microbiota and Blood Pressure: A Systematic Review of Randomized Clinical Trials in Humans. Nutrients. 2022; 14(11):2263. https://doi.org/10.3390/nu14112263
Chicago/Turabian StyleSweeney, Marva, Gracie Burns, Nora Sturgeon, Kim Mears, Kim Stote, and Cynthia Blanton. 2022. "The Effects of Berry Polyphenols on the Gut Microbiota and Blood Pressure: A Systematic Review of Randomized Clinical Trials in Humans" Nutrients 14, no. 11: 2263. https://doi.org/10.3390/nu14112263