
Efficacy of 4.0 mg versus 0.4 mg Folic Acid Supplementation on the Reproductive Outcomes: A Randomized Controlled Trial

 , , , , , ,
, , , , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Trial Design and Participants
2.2. Randomization and Trial-Group Assignment
2.3. Outcome Measures
2.4. Adverse Events and Adherence
2.5. Statistical Analysis
3. Results
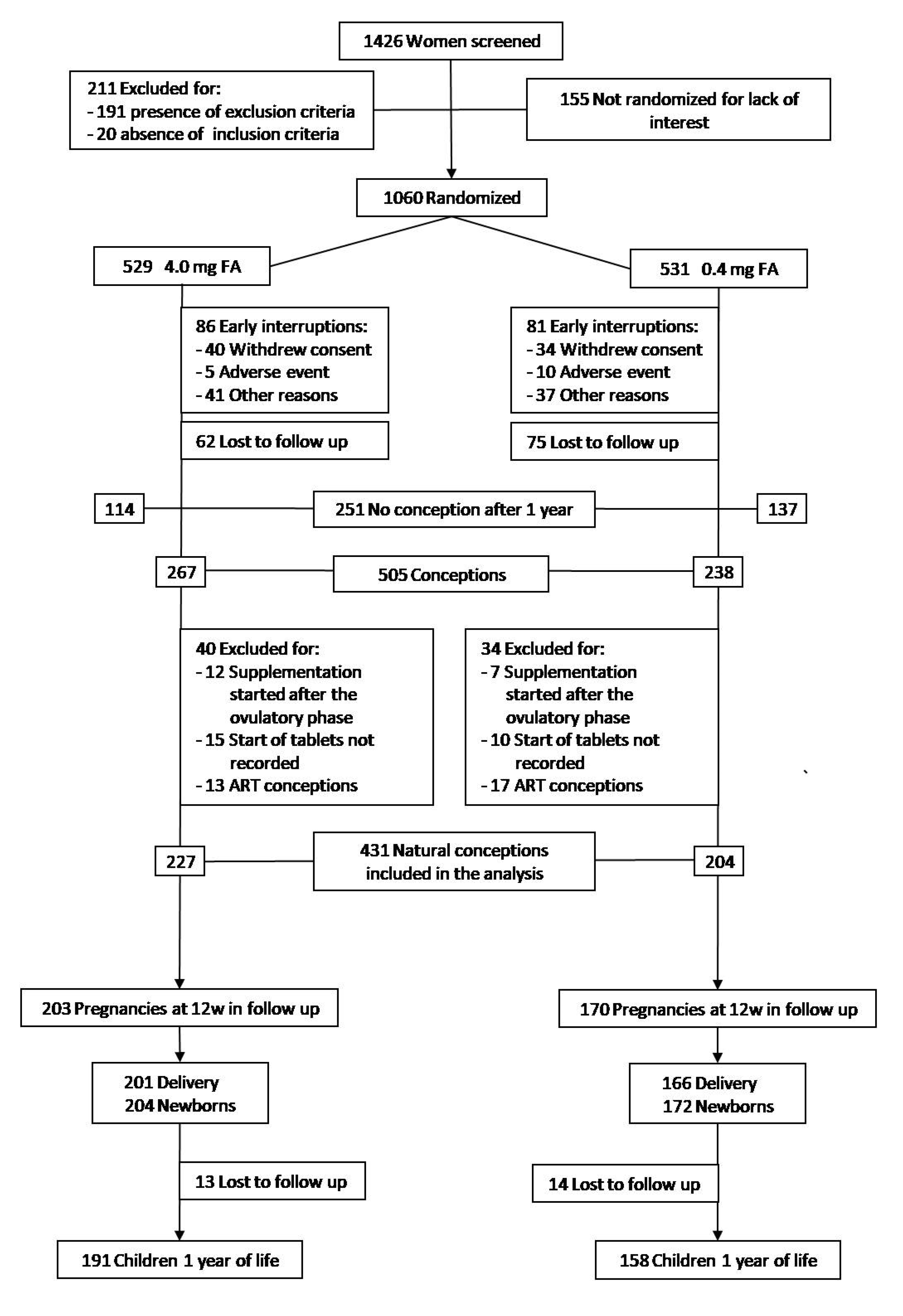
3.1. Trial Findings
3.1.1. Trial Participants
3.1.2. Study Outcomes
3.1.3. Adverse Events and Adherence
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Membership of the Italian Folic Acid Trial Study Group
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- De-Regil, L.M.; Peña-Rosas, J.P.; Fernández-Gaxiola, A.C.; Rayco-Solon, P. Effects and safety of periconceptional oral folate supplementation for preventing birth defects. Cochrane Database Syst. Rev. 2015, CD007950. [Google Scholar] [CrossRef]
- Czeizel, A.E.; Dobo, M.; Vargha, P. Hungarian cohort-controlled trial of periconceptional multivitamin supplementation shows a reduction in certain congenital abnormalities. Birth Defects Res. A Clin. Mol. Teratol. 2004, 70, 853–861. [Google Scholar] [CrossRef]
- Botto, L.D.; Olney, R.S.; Erickson, J.D. Vitamin supplements and the risk for congenital anomalies other than neural tube defects. Am. J. Med. Genet. 2004, 125C, 12–21. [Google Scholar] [CrossRef] [PubMed]
- Lassi, Z.S.; Salam, R.A.; Haider, B.A.; Bhutta, Z.A. Folic acid supplementation during pregnancy for maternal health and pregnancy outcomes. Cochrane Database Syst. Rev. 2013, CD006896. [Google Scholar] [CrossRef]
- Balogun, O.O.; Lopes, K.D.S.; Ota, E.; Takemoto, Y.; Rumbold, A.; Takegata, M.; Mori, R. Vitamin supplementation for preventing miscarriage. Cochrane Database Syst. Rev. 2016. [Google Scholar] [CrossRef]
- Fekete, K.; Berti, C.; Trovato, M.; Lohner, S.; Dullemeijer, C.; Souverein, O.W.; Cetin, I.; Decsi, T. Effect of folate intake on health outcomes in pregnancy: A systematic review and meta-analysis on birth weight, placental weight and length of gestation. Nutr. J. 2012, 11, 75. [Google Scholar] [CrossRef] [Green Version]
- Li, N.; Li, Z.; Ye, R.; Liu, J.; Ren, A. Impact of Periconceptional Folic Acid Supplementation on Low Birth Weight and Small-for-Gestational-Age Infants in China: A Large Prospective Cohort Study. J. Pediatr. 2017, 187, 105–110. [Google Scholar] [CrossRef]
- Zhang, Q.; Wang, Y.; Xin, X.; Zhang, Y.; Liu, D.; Peng, Z.; He, Y.; Xu, J.; Ma, X. Effect of folic acid supplementation on preterm delivery and small for gestational age births: A systematic review and meta-analysis. Reprod. Toxicol. 2017, 67, 35–41. [Google Scholar] [CrossRef]
- Li, B.; Zhang, X.; Peng, X.; Zhang, S.; Wang, X.; Zhu, C. Folic Acid and Risk of Preterm Birth: A Meta-Analysis. Front. Neurosci. 2019, 13, 1284. [Google Scholar] [CrossRef] [Green Version]
- Martinussen, M.P.; Bracken, M.B.; Triche, E.W.; Jacobsen, G.W.; Risnes, K.R. Folic acid supplementation in early pregnancy and the risk of preeclampsia, small for gestational age offspring and preterm delivery. Eur. J. Obstet. Gynecol. Reprod. Biol. 2015, 195, 94–99. [Google Scholar] [CrossRef] [Green Version]
- Saccone, G.; Berghella, V. Folic acid supplementation in pregnancy to prevent preterm birth: A systematic review and meta-analysis of randomized controlled trials. Eur. J. Obstet. Gynecol. Reprod. Biol. 2016, 199, 76–81. [Google Scholar] [CrossRef] [Green Version]
- Gaskins, A.J.; Chavarro, J.E. Diet and fertility: A review. Am. J. Obstet. Gynecol. 2018, 218, 379–389. [Google Scholar] [CrossRef]
- Wen, S.W.; White, R.R.; Rybak, N.; Gaudet, L.M.; Robson, S.; Hague, W.; Simms-Stewart, D.; Carroli, G.; Smith, G.; Fraser, W.D.; et al. Effect of high dose folic acid supplementation in pregnancy on pre-eclampsia (FACT): Double blind, phase III, randomised controlled, international, multicentre trial. BMJ 2018, 362, k3478. [Google Scholar] [CrossRef] [Green Version]
- Bulloch, R.E.; Lovell, A.L.; Jordan, V.M.B.; McCowan, L.M.E.; Thompson, J.M.D.; Wall, C.R. Maternal folic acid supplementation for the prevention of preeclampsia: A systematic review and meta-analysis. Paediatr. Peérinat. Epidemiol. 2018, 32, 346–357. [Google Scholar] [CrossRef]
- Nilsen, R.M.; Vollset, S.E.; Rasmussen, S.A.; Ueland, P.M.; Daltveit, A.K. Folic Acid and Multivitamin Supplement Use and Risk of Placental Abruption: A Population-based Registry Study. Am. J. Epidemiol. 2008, 167, 867–874. [Google Scholar] [CrossRef] [PubMed]
- Gaskins, A.J.; Rich-Edwards, J.W.; Hauser, R.; Williams, P.L.; Gillman, M.W.; Ginsburg, E.S.; Missmer, S.A.; Chavarro, J.E. Maternal Prepregnancy Folate Intake and Risk of Spontaneous Abortion and Stillbirth. Obstet. Gynecol. 2014, 124, 23–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wald, N.J.; Morris, J.K.; Blakemore, C. Public health failure in the prevention of neural tube defects: Time to abandon the tolerable upper intake level of folate. Public Health Rev. 2018, 39, 2. [Google Scholar] [CrossRef]
- Berry, R.J. Lack of historical evidence to support folic acid exacerbation of the neuropathy caused by vitamin B12 defi-ciency. Am. J. Clin. Nutr. 2019, 110, 554–561. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cawley, S.; Mullaney, L.; McKeating, A.; Farren, M.; McCartney, D.; Turner, M.J. A review of European guidelines on periconceptional folic acid supplementation. Eur. J. Clin. Nutr. 2015, 70, 143–154. [Google Scholar] [CrossRef]
- Wald, N.; Law, M.R.; Morris, J.; Wald, D. Quantifying the effect of folic acid. Lancet 2001, 358, 2069–2073. [Google Scholar] [CrossRef]
- Dhonukshe-Rutten, R.A.M.; de Vries, J.H.M.; de Bree, A.; van der Put, N.; van Staveren, W.A.; de Groot, L.C.P.G.M. Dietary in-take and status of folate and vitamin B12 and their association with homocysteine and cardiovascular disease in European populations. Eur. J. Clin. Nutr. 2009, 63, 18–30. [Google Scholar] [CrossRef] [Green Version]
- Pastor-Valero, M.; Navarrete-Munoz, E.M.; Rebagliato, M.; Iñiguez, C.; Murcia, M.; Marco, A.; Ballester, F.; Vioque, J. Pericon-ceptional folic acid supplementation and anthropometric measures at birth in a cohort of pregnant women in Valencia, Spain. Br. J. Nutr. 2011, 105, 1352–1360. [Google Scholar] [CrossRef] [Green Version]
- Papadopoulou, E.; Stratakis, N.; Roumeliotaki, T.; Sarri, K.; Merlo, D.F.; Kogevinas, M.; Chatzi, L. The effect of high doses of folic acid and iron supplementation in early-to-mid pregnancy on prematurity and fetal growth retardation: The mother–child cohort study in Crete, Greece (Rhea study). Eur. J. Nutr. 2012, 52, 327–336. [Google Scholar] [CrossRef]
- Murray, L.K.; Smith, M.J.; Jadavji, N.M. Maternal oversupplementation with folic acid and its impact on neurodevelopment of offspring. Nutr. Rev. 2018, 76, 708–721. [Google Scholar] [CrossRef]
- Yajnik, C.S.; Deshpande, S.S.; Jackson, A.A.; Refsum, H.; Rao, S.; Fisher, D.J.; Bhat, D.S.; Naik, S.S.; Coyaji, K.J.; Joglekar, C.V.; et al. Vitamin B12 and folate concentrations during pregnancy and insulin resistance in the offspring: The Pune Maternal Nutrition Study. Diabetologia 2007, 51, 29–38. [Google Scholar] [CrossRef] [Green Version]
- MRC Vitamin Study Research Group. Prevention of neural tube defects: Results of the MRC Vitamin Study. Lancet 1991, 338, 131–137. [Google Scholar] [CrossRef]
- Czeizel, A.E.; Bánhidy, F. Folic acid supplementation and risk reduction in preterm birth. Am. J. Clin. Nutr. 2011, 94, 1651–1652. [Google Scholar] [CrossRef]
- Vila-Nova, C.; Wehby, G.L.; Queirós, F.C.; Chakraborty, H.; Félix, T.M.; Goco, N.; Moore, J.; Gewehr, E.V.; Lins, L.; Affonso, C.M.; et al. Periconceptional use of folic acid and risk of miscarriage–findings of the Oral Cleft Prevention Program in Brazil. J. Peérinat. Med. 2013, 41, 461–466. [Google Scholar] [CrossRef]
- Overview: What is Preconception Health and Health Care? Available online: https://www.cdc.gov/preconception/overview.html (accessed on 12 October 2021).
- Bortolus, R.; Blom, F.; Filippini, F.; van Poppel, M.N.M.; Leoncini, E.; de Smit, D.J.; Benetollo, P.P.; Cornel, M.C.; de Walle, H.E.K.; Mas-troiacovo, P.; et al. Prevention of congenital malformations and other adverse pregnancy outcomes with 4.0 mg of folic acid: Community-based randomized clinical trial in Italy and the Netherlands. BMC Pregnancy Childbirth 2014, 14, 166. [Google Scholar] [CrossRef] [Green Version]
- EUROCAT Guide 1.4 and Reference Documents. Available online: https://eu-rd-platform.jrc.ec.europa.eu/sites/default/files/JRC-EUROCAT-Full-Guide-1.4-version-26-SEP-2019.pdf (accessed on 10 October 2019).
- National Guideline Alliance (UK). Hypertension in pregnancy: Diagnosis and management. Manchester: National Institute for Health and Care Excellence (UK). 2010. Available online: www.nice.org.uk/guidance/cg107 (accessed on 12 October 2021).
- Parazzini, F.; Cortinovis, I.; Bortolus, R.; Fedele, L.; DeCarli, A. Weight at birth by gestational age in Italy. Hum. Reprod. 1995, 10, 1862–1863. [Google Scholar] [CrossRef]
- Parazzini, F.; Cortinovis, I.; Bortolus, R.; Soliani, A.; Fedele, L. Weight at birth of singleton live births between the 23rd and 27th week of gestation delivered vaginally or by cesarean section. Acta Paediatr. 1994, 83, 1206–1208. [Google Scholar] [CrossRef]
- Czeizel, A.E.; Dudas, I. Prevention of the first occurrence of neural-tube defects by periconceptional vitamin supplemen-tation. N. Engl. J. Med. 1992, 327, 1832–1835. [Google Scholar] [CrossRef] [PubMed]
- Tolarova, M.; Harris, J. Reduced recurrence of orofacial clefts after periconceptional supplementation with high dose folic acid and multivitamins. Teratology 1995, 51, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Czeizel, A.E.; Timar, L.; Sárközi, A. Dose-dependent effect of folic acid on the prevention of orofacial clefts. Pediatrics 1999, 104, e66. [Google Scholar] [CrossRef] [Green Version]
- Czeizel, A.E.; Puhó, E. Maternal use of nutritional supplements during the first month of pregnancy and decreased risk of Down’s syndrome: Case-control study. Nutrition 2005, 21, 698–704. [Google Scholar] [CrossRef]
- Ahmed, T.; Fellus, I.; Gaudet, J.; MacFarlane, A.J.; Fontaine-Bisson, B.; Bainbridge, S.A. Effect of folic acid on human tropho-blast health and function in vitro. Placenta 2016, 37, 7–15. [Google Scholar] [CrossRef]
- Mills, J.L.; Von Kohorn, I.; Conley, M.R.; Zeller, J.A.; Cox, C.; Williamson, R.E.; Dufour, D.R. Low vitamin B-12 concentrations in patients without anemia: The effect of folic acid fortification of grain. Am. J. Clin. Nutr. 2003, 77, 1474–1477. [Google Scholar] [CrossRef]
- Qi, Y.P.; Do, A.N.; Hamner, H.C.; Pfeiffer, C.M.; Berry, R. The Prevalence of Low Serum Vitamin B-12 Status in the Absence of Anemia or Macrocytosis Did Not Increase among Older U.S. Adults after Mandatory Folic Acid Fortification. J. Nutr. 2014, 144, 170–176. [Google Scholar] [CrossRef]
- Vollset, S.E.; Clarke, R.; Lewington, S.; Ebbing, M.; Halsey, J.; Lonn, E.; Armitage, J.; Manson, J.E.; Hankey, G.J.; Spence, J.D.; et al. Effects of folic acid supplementation on overall and site-specific cancer incidence during the randomised trials: Meta-analyses of data on 50000 individuals. Lancet 2013, 381, 1029–1036. [Google Scholar] [CrossRef] [Green Version]
- Chen, H.; Qin, L.; Gao, R.; Jin, X.; Cheng, K.; Zhang, S.; Hu, X.; Xu, W.; Wang, H. Neurodevelopmental effects of maternal folic acid supplementation: A systematic review and meta-analysis. Crit. Rev. Food Sci. Nutr. 2021, 21, 1–17. [Google Scholar] [CrossRef]
- Liu, H.-Y.; Liu, S.-M.; Zhang, Y.-Z. Maternal Folic Acid Supplementation Mediates Offspring Health via DNA Methylation. Reprod. Sci. 2020, 27, 963–976. [Google Scholar] [CrossRef]
- Vollset, S.E.; Refsum, H.; Irgens, L.M.; Emblem, B.M.; Tverdal, A.; Gjessing, H.K.; Monsen, A.L.B.; Ueland, P.M. Plasma total homocysteine, pregnancy complications, and adverse pregnancy outcomes: The Hordaland Homocysteine Study. Am. J. Clin. Nutr. 2000, 71, 962–968. [Google Scholar] [CrossRef]
- Bergen, N.E.; Jaddoe, V.W.; Timmermans, S.; Hofman, A.; Lindemans, J.; Russcher, H.; Raat, H.; Steegers-Theunissen, R.P.; Steegers, E.A. Homocysteine and folate concentrations in early pregnancy and the risk of adverse pregnancy outcomes: The Genera-tion R Study. BJOG 2012, 119, 739–751. [Google Scholar] [CrossRef] [PubMed]
- Bortolus, R.; Filippini, F.; Udali, S.; Rinaldi, M.; Genesini, S.; Gandini, G.; Montagnana, M.; Chiaffarino, F.; Lippi, G.; Pattini, P.; et al. B vitamin blood concentrations and one-carbon metabolism polymorphisms in a sample of Italian women and men attending a unit of transfusion medicine: A cross-sectional study. Eur. J. Nutr. 2020, 60, 2643–2654. [Google Scholar] [CrossRef] [PubMed]
- Zappacosta, B.; Persichilli, S.; Iacoviello, L.; Di Castelnuovo, A.; Graziano, M.; Gervasoni, J.; Leoncini, E.; Cimino, G.; Mastroiacovo, P. Folate, vitamin B12 and homocysteine status in an Italian blood donor population. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 473–480. [Google Scholar] [CrossRef]
- Keenan, K.; Hipwell, A.; McAloon, R.; Hoffmann, A.; Mohanty, A.; Magee, K. Concordance between maternal recall of birth complications and data from obstetrical records. Early Hum. Dev. 2017, 105, 11–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Characteristic | 4.0 mg FA Group (n = 227) | 0.4 mg FA Group (n = 204) |
|---|---|---|
| Sociodemographic characteristics | ||
| Maternal age, years | ||
| Mean age (SD) | 32.2 (4.4) | 32.3 (4.0) |
| <30-no. (%) | 67 (29.5) | 54 (26.5) |
| 30–34 | 88 (38.8) | 85 (41.7) |
| 35–39 | 63 (27.8) | 59 (28.9) |
| ≥40 | 9 (4.0) | 6 (2.9) |
| Missing | - | - |
| Education, years | ||
| ≤8-no. (%) | 18 (7.9) | 14 (6.9) |
| 9–13 | 85 (37.4) | 90 (44.1) |
| 14–18 | 88 (38.8) | 81 (39.7) |
| ≥19 | 35 (15.4) | 19 (9.3) |
| Missing | 1 | - |
| Marital status, no. (%) | ||
| married | 160 (70.5) | 146 (71.6) |
| common-low wife | 51 (22.5) | 39 (19.1) |
| unmarried | 16 (7.0) | 19 (9.3) |
| Lifestyle/Personal habits | ||
| Cigarette smokers, no. (%) | ||
| No | 195 (85.9) | 176 (86.3) |
| Yes: | 32 (14.1) | 28 (13.7) |
| ≤10 cig/day | 26 (11.5) | 25 (12.3) |
| >10 cig/day | 6 (2.6) | 3 (1.5) |
| Alcohol drinkers, no. (%) | ||
| No | 120 (52.9) | 95 (46.6) |
| Yes: | 107 (47.1) | 109 (53.4) |
| ≤7 drinks/week | 101 (44.5) | 101 (49.5) |
| >7 drinks/week | 6 (2.6) | 8 (3.9) |
| BMI and current medical conditions | ||
| BMI a | ||
| Mean (SD) | 22.1 (2.8) | 21.9 (2.8) |
| <18.50 kg/m2, no. (%) | 15 (6.6) | 14 (6.9) |
| 18.50–24.99 kg/m2 | 180 (79.3) | 158 (77.5) |
| ≥25.00 kg/m2 | 32 (14.1) | 32 (15.7) |
| Current medical conditions, no. (%) | ||
| No | 183 (80.6) | 163 (79.9) |
| Yes: | 44 (19.4) | 41 (20.1) |
| hypertension | 1 (0.4) | 0 (0.0) |
| thyroid diseases | 11 (4.8) | 14 (6.9) |
| rheumatic diseases | 1 (0.4) | 2 (1.0) |
| urinary tract infections | 3 (1.3) | 3 (1.5) |
| genital tract infections | 8 (3.5) | 5 (2.5) |
| other diseases | 24 (10.6) | 21 (10.3) |
| Reproductive history | ||
| Previous pregnancies, no. (%) | ||
| 0 | 117 (51.5) | 107 (52.5) |
| 1 | 72 (31.8) | 67 (32.8) |
| ≥2 | 38 (16.7) | 30 (14.7) |
| Livebirth b, no. (%) | ||
| 0 | 38 (34.5) | 38 (39.2) |
| 1 | 66 (60.0) | 54 (55.7) |
| ≥2 | 6 (5.5) | 5 (5.2) |
| Spontaneous abortion b, no. (%) | ||
| 0 | 50 (45.5) | 44 (45.4) |
| 1 | 46 (41.8) | 46 (47.4) |
| ≥2 | 14 (12.7) | 7 (7.2) |
| Perinatal death b, no. (%) | ||
| No | 109 (99.1) | 93 (95.9) |
| Yes | 1 (0.9) | 4 (4.1) |
| Fetus/child with malformation or genetic disease b, no. (%) | ||
| No | 108 (98.2) | 94 (96.9) |
| Yes | 2 (1.8) | 3 (3.1) |
| Current pregnancy | ||
| Planned pregnancy, months | ||
| Mean (SD) | 5.36 (11.1) | 6.35 (11.3) |
| <4-no. (%) | 159 (70.7) | 131 (64.3) |
| 4–7 | 29 (12.9) | 26 (12.7) |
| ≥8 | 37 (16.4) | 47 (23.0) |
| Missing | 2 | - |
| Use of supplements before randomization, no. (%) | ||
| No | 146 (64.3) | 124 (60.8) |
| Yes | 81 (35.7) | 80 (39.2) |
| Use of FA after the 12th week of gestation, no. (%) | ||
| No | 155 (76.7) | 131 (79.4) |
| Yes | 31 (15.4) | 19 (11.5) |
| Missing | 16 (7.9) | 15 (9.1) |
| Outcome | 4.0 mg FA Group (n = 227) | 0.4 mg FA Group (n = 204) | RR (95%CI) | p Value | Adjusted RR (95%CI) | p Value |
|---|---|---|---|---|---|---|
| Major CMs, no. (%) | 8 (3.5) | 9 (4.4) | 0.80 (0.31 to 2.03) | 0.64 | 0.76 (0.30 to 1.92) a | 0.56 a |
| Composite outcome b, no. (%) | ||||||
| No | 184 (81.1) | 129 (63.2) | Ref. cat. | Ref. cat. | ||
| Yes | 43 (18.9) | 75 (36.8) | 0.51 (0.40 to 0.68) | <0.0001 | 0.52 (0.38 to 0.72) c | 0.0001 c |
| Spontaneous abortion, no. (%) | 21 (9.3) | 34 (16.7) | 0.56 (0.33 to 0.92) | 0.02 | 0.56 (0.34 to 0.93) d | 0.02 d |
| Intrauterine fetal death e, no. (%) | 1 (0.4) | 1 (0.5) | 0.90 (0.06 to 14.27) | 0.94 | - | - |
| Preeclampsia, no. (%) | 2 (0.9) | 3 (1.5) | 0.60 (0.10 to 3.55) | 0.57 | - | - |
| Abruptio placentae, no. (%) | 0 (0.0) | 2 (1.0) | 0.18 (0.01 to 3.72) | 0.22 f | - | - |
| SGA (<10°) g, no. (%) | 8 (3.5) | 17 (8.3) | 0.42 (0.19 to 0.96) | 0.04 | 0.43 (0.19 to 0.97) a | 0.04 a |
| Preterm delivery, no. (%) | 9 (4.0) | 18 (8.8) | 0.45 (0.21 to 0.98) | 0.04 | 0.44 (0.20 to 0.95) a | 0.04 a |
| Outcome | 4.0 mg FA Group (n = 227) | 0.4 mg FA Group (n = 204) | RR (95% CI) or MD (95% CI) | p Value | Adjusted RR (95% CI) or MD (95% CI) | p Value |
|---|---|---|---|---|---|---|
| Ectopic pregnancy, no. (%) | 3 (1.3) | 2 (1.0) | 1.35 (0.23 to 7.99) | 0.74 | - | - |
| Voluntary abortion, no. (%) | 1 (0.4) | 1 (0.5) | 0.90 (0.06 to 14.27) | 0.94 | - | - |
| LBW a, no. (%) | 9 (4.0) | 21 (10.3) | 0.39 (0.18 to 0.82) | 0.01 | - | - |
| Birthweight a, mean (SD) | 3357 (470.4) | 3213 (597.5) | 144 (34 to 254) | 0.01 | 145 (35 to 255) b | 0.01 b |
| Twin delivery, no. (%) | 3 (1.3) | 6 (2.9) | 0.45 (0.11 to 1.77) | 0.25 | - | - |
| Characteristic | 4.0 mg FA Group | 0.4 mg FA Group | p Value |
|---|---|---|---|
| Mode of Delivery, no. (%) | n = 201 | n = 166 | 0.21 |
| Spontaneous vaginal delivery | 99 (50.3) | 77 (47.2) | |
| Induced vaginal delivery | 37 (18.8) | 30 (18.4) | |
| Operative vaginal delivery | 12 (6.1) | 12 (7.4) | |
| Elective caesarean section | 26 (13.2) | 13 (8.0) | |
| Emergency caesarean section | 23 (11.7) | 31 (19.0) | |
| Missing | 4 | 3 | |
| Admission to NICU, no. (%) | n = 204 | n = 172 | 0.38 |
| No | 173 (88.3) | 140 (84.8) | |
| Yes, for observation | 18 (9.2) | 18 (10.9) | |
| Yes, for intensive care | 5 (2.5) | 7 (4.2) | |
| Missing | 8 | 7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bortolus, R.; Filippini, F.; Cipriani, S.; Trevisanuto, D.; Cavallin, F.; Zanconato, G.; Somigliana, E.; Cesari, E.; Mastroiacovo, P.; Parazzini, F., on behalf of the Italian Folic Acid Trial Study Group. Efficacy of 4.0 mg versus 0.4 mg Folic Acid Supplementation on the Reproductive Outcomes: A Randomized Controlled Trial. Nutrients 2021, 13, 4422. https://doi.org/10.3390/nu13124422
Bortolus R, Filippini F, Cipriani S, Trevisanuto D, Cavallin F, Zanconato G, Somigliana E, Cesari E, Mastroiacovo P, Parazzini F on behalf of the Italian Folic Acid Trial Study Group. Efficacy of 4.0 mg versus 0.4 mg Folic Acid Supplementation on the Reproductive Outcomes: A Randomized Controlled Trial. Nutrients. 2021; 13(12):4422. https://doi.org/10.3390/nu13124422
Chicago/Turabian StyleBortolus, Renata, Francesca Filippini, Sonia Cipriani, Daniele Trevisanuto, Francesco Cavallin, Giovanni Zanconato, Edgardo Somigliana, Elena Cesari, Pierpaolo Mastroiacovo, and Fabio Parazzini on behalf of the Italian Folic Acid Trial Study Group. 2021. "Efficacy of 4.0 mg versus 0.4 mg Folic Acid Supplementation on the Reproductive Outcomes: A Randomized Controlled Trial" Nutrients 13, no. 12: 4422. https://doi.org/10.3390/nu13124422