
Does the Combined Effect of Resistance Training with EPO and Iron Sulfate Improve Iron Metabolism in Older Individuals with End-Stage Renal Disease?

 , ,
, ,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
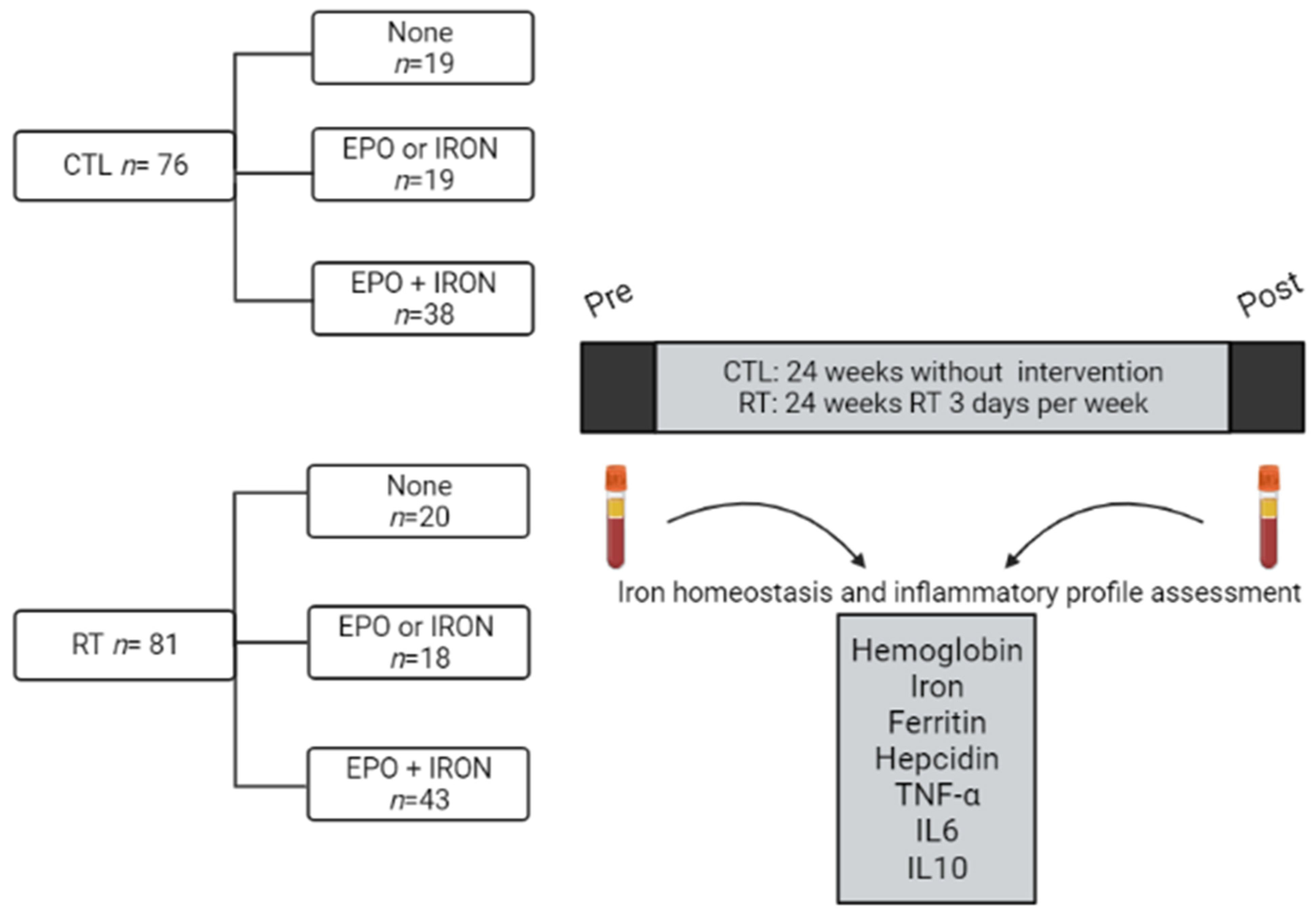
2.1. Procedures
2.2. Iron and ESA Treatments
2.3. Biochemical Analysis
2.4. Statistical Analysis
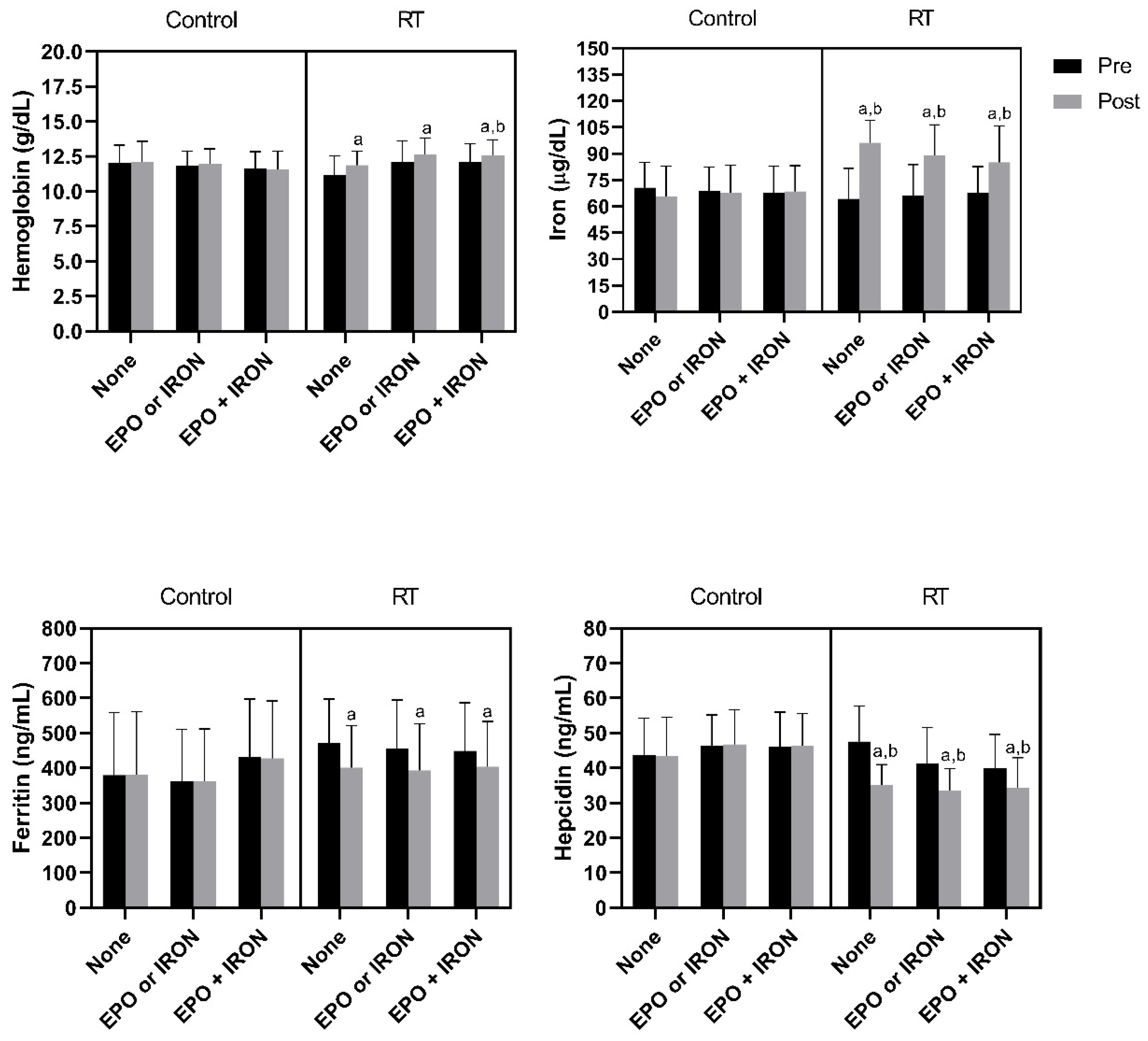
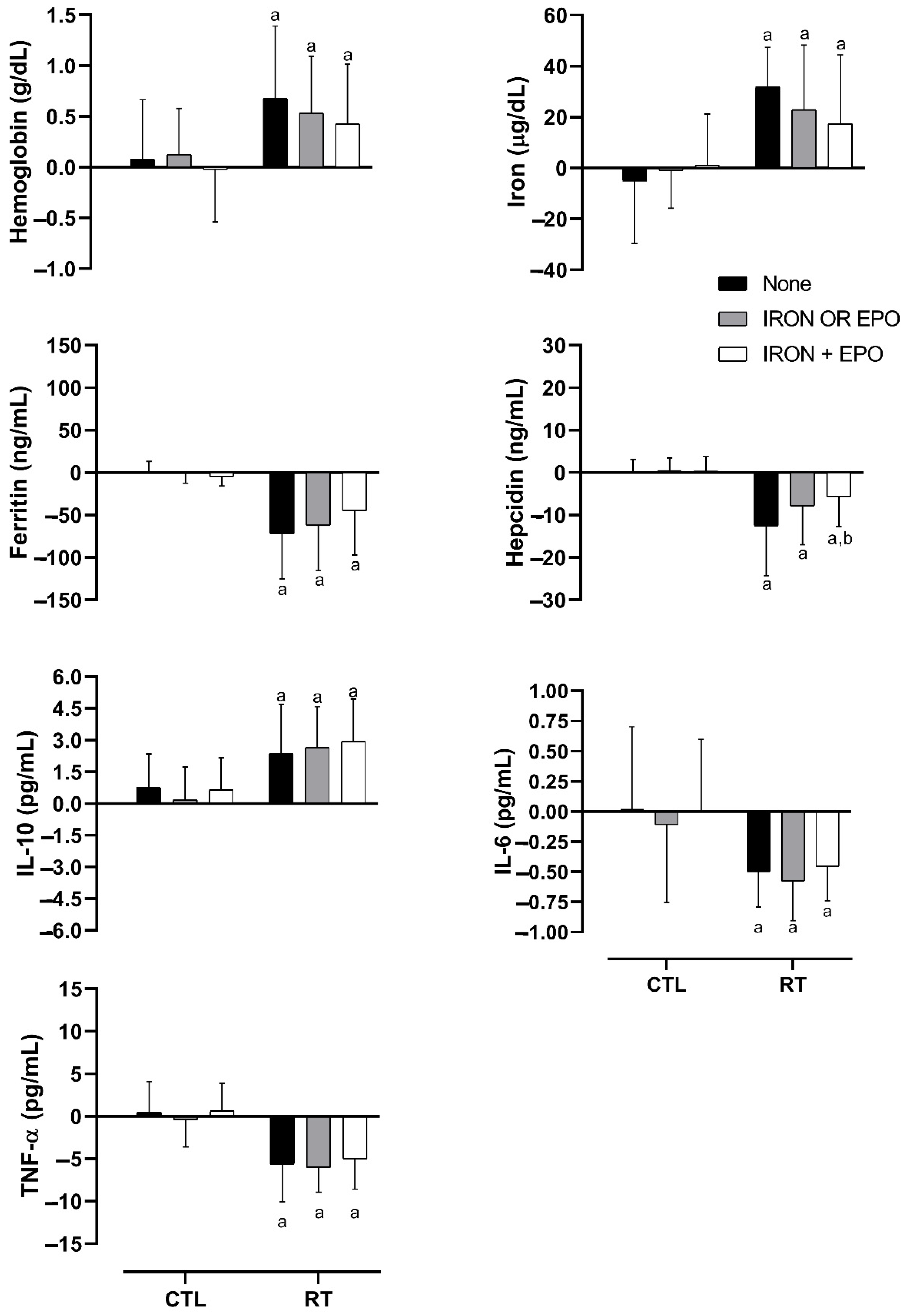
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Collister, D.; Rigatto, C.; Tangri, N. Anemia management in chronic kidney disease and dialysis: A narrative review. Curr. Opin. Nephrol. Hypertens. 2017, 26, 214–218. [Google Scholar] [CrossRef] [PubMed]
- Hörl, W.H. Clinical aspects of iron use in the anemia of kidney disease. J. Am. Soc. Nephrol. 2007, 18, 382–393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Besarab, A.; Coyne, D.W. Iron supplementation to treat anemia in patients with chronic kidney disease. Nat. Rev. Nephrol. 2010, 6, 699–710. [Google Scholar] [CrossRef] [PubMed]
- Babitt, J.L.; Eisenga, M.F.; Haase, V.H.; Kshirsagar, A.V.; Levin, A.; Locatelli, F.; Małyszko, J.; Swinkels, D.W.; Tarng, D.C.; Cheung, M.; et al. Controversies in optimal anemia management: Conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Conference. Kidney Int. 2021, 99, 1280–1295. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, R.; Kusek, J.W.; Pappas, M.K. A randomized trial of intravenous and oral iron in chronic kidney disease. Kidney Int. 2015, 88, 905–914. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moura, S.R.G.; Corrêa, H.L.; Neves, R.V.P.; Santos, C.A.R.; Neto, L.S.S.; Silva, V.L.; Souza, M.K.; Deus, L.A.; Reis, A.L.; Simões, H.G.; et al. Effects of resistance training on hepcidin levels and iron bioavailability in older individuals with end-stage renal disease: A randomized controlled trial. Exp. Gerontol. 2020, 139, 111017. [Google Scholar] [CrossRef] [PubMed]
- Corrêa, H.L.; Moura, S.R.G.; Neves, R.V.P.; Tzanno-Martins, C.; Souza, M.K.; Haro, A.S.; Costa, F.; Silva, J.A.B.; Stone, W.; Honorato, F.S.; et al. Resistance training improves sleep quality, redox balance and inflammatory profile in maintenance hemodialysis patients: A randomized controlled trial. Sci. Rep. 2020, 10, 11708. [Google Scholar] [CrossRef] [PubMed]
- da Silva, V.; Corrêa, H.; Neves, R.; Deus, L.; Reis, A.; Souza, M.; dos Santos, C.; de Castro, D.; Honorato, F.; Simões, H.; et al. Impact of Low Hemoglobin on Body Composition, Strength, and Redox Status of Older Hemodialysis Patients Following Resistance Training. Front. Physiol. 2021, 12, 619054. [Google Scholar] [CrossRef] [PubMed]
- Neves, R.V.P.; Corrêa, H.L.; Deus, L.A.; Reis, A.L.; Souza, M.K.; Simões, H.G.; Navalta, J.W.; Moraes, M.R.; Prestes, J.; Rosa, T.S. Dynamic not isometric training blunts osteo-renal disease and improves the sclerostin/FGF23/Klotho axis in maintenance hemodialysis patients: A randomized clinical trial. J. Appl. Physiol. 2021, 130, 508–516. [Google Scholar] [CrossRef] [PubMed]
- Beltrame, A. Portaria Nº 224, de 10 de Maio de 2010; Ministério da Saúde: Rio de Janeiro, Brazil, 2010. [Google Scholar]
- Bay, M.L.; Pedersen, B.K. Muscle-Organ Crosstalk: Focus on Immunometabolism. Front. Physiol. 2020, 11, 567881. [Google Scholar] [CrossRef] [PubMed]
- Xiao, X.; Alfaro-Magallanes, V.M.; Babitt, J.L. Bone morphogenic proteins in iron homeostasis. Bone 2020, 138, 115495. [Google Scholar] [CrossRef] [PubMed]
- Babitt, J.L.; Lin, H.Y. Mechanisms of anemia in CKD. J. Am. Soc. Nephrol. 2012, 23, 1631–1634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fudin, R.; Jaichenko, J.; Shostak, A.; Bennett, M.; Gotloib, L. Correction of uremic iron deficiency anemia in hemodialyzed patients: A prospective study. Nephron 1998, 79, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Macdougall, I.C.; Tucker, B.; Thompson, J.; Tomson, C.R.; Baker, L.R.; Raine, A.E. A randomized controlled study of iron supplementation in patients treated with erythropoietin. Kidney Int. 1996, 50, 1694–1699. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Markowitz, G.S.; Kahn, G.A.; Feingold, R.E.; Coco, M.; Lynn, R.I. An evaluation of the effectiveness of oral iron therapy in hemodialysis patients receiving recombinant human erythropoietin. Clin. Nephrol. 1997, 48, 34–40. [Google Scholar] [PubMed]
- Gadelha, A.B.; Cesari, M.; Corrêa, H.L.; Neves, R.V.P.; Sousa, C.V.; Deus, L.A.; Souza, M.K.; Reis, A.L.; Moraes, M.R.; Prestes, J.; et al. Effects of pre-dialysis resistance training on sarcopenia, inflammatory profile, and anemia biomarkers in older community-dwelling patients with chronic kidney disease: A randomized controlled trial. Int. Urol. Nephrol. 2021, in press. [Google Scholar] [CrossRef] [PubMed]
- Neves, P.; Sesso, R.C.C.; Thomé, F.S.; Lugon, J.R.; Nasicmento, M.M. Brazilian Dialysis Census: Analysis of data from the 2009–2018 decade. J. Bras. Nefrol. 2020, 42, 191–200. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | CTL | RT | p Value | Eta2 | ||||
|---|---|---|---|---|---|---|---|---|
| None | EPO or IRON | EPO + IRON | None | EPO or IRON | EPO + IRON | |||
| Age (years) | 66.16 ± 4 | 66 ± 4.14 | 66.58 ± 3.77 | 66.75 ± 3.34 | 67.83 ± 3.33 | 67.28 ± 3.19 | 0.687 | 0.005 |
| Body mass (kg) | 71.47 ± 14.72 | 72.33 ± 15.46 | 73.61 ± 14.38 | 71.38 ± 16.76 | 77.03 ± 17.31 | 73.78 ± 16.41 | 0.740 | 0.004 |
| Body mass index (kg/m2) | 26.54 ± 2.85 | 26.78 ± 3.12 | 26.98 ± 2.88 | 26.66 ± 3.75 | 27.95 ± 3.86 | 27.32 ± 3.78 | 0.769 | 0.003 |
| Waist circumference (cm) | 94.54 ± 12.84 | 94.91 ± 12.12 | 96.27 ± 11.87 | 93.9 ± 12.24 | 98.12 ± 12.13 | 95.47 ± 11.41 | 0.680 | 0.005 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Corrêa, H.d.L.; Alfaro-Magallanes, V.M.; Moura, S.R.G.; Neves, R.V.P.; Deus, L.A.; Honorato, F.S.; Silva, V.L.; Raab, A.T.O.; Maia, B.C.H.; Padula, I.A.; et al. Does the Combined Effect of Resistance Training with EPO and Iron Sulfate Improve Iron Metabolism in Older Individuals with End-Stage Renal Disease? Nutrients 2021, 13, 3250. https://doi.org/10.3390/nu13093250
Corrêa HdL, Alfaro-Magallanes VM, Moura SRG, Neves RVP, Deus LA, Honorato FS, Silva VL, Raab ATO, Maia BCH, Padula IA, et al. Does the Combined Effect of Resistance Training with EPO and Iron Sulfate Improve Iron Metabolism in Older Individuals with End-Stage Renal Disease? Nutrients. 2021; 13(9):3250. https://doi.org/10.3390/nu13093250
Chicago/Turabian StyleCorrêa, Hugo de Luca, Víctor Manuel Alfaro-Magallanes, Sting Ray Gouveia Moura, Rodrigo Vanerson Passos Neves, Lysleine Alves Deus, Fernando Sousa Honorato, Victor Lopes Silva, Artur Temizio Oppelt Raab, Beatriz Carneiro Habbema Maia, Isabela Akaishi Padula, and et al. 2021. "Does the Combined Effect of Resistance Training with EPO and Iron Sulfate Improve Iron Metabolism in Older Individuals with End-Stage Renal Disease?" Nutrients 13, no. 9: 3250. https://doi.org/10.3390/nu13093250