
Association of Serum Vitamin B6 with All-Cause and Cause-Specific Mortality in a Prospective Study


Department of Epidemiology and Biostatistics, School of Health Sciences, Wuhan University, Wuhan 430071, China
*
Author to whom correspondence should be addressed.
Nutrients 2021, 13(9), 2977; https://doi.org/10.3390/nu13092977
Submission received: 30 June 2021
/
Revised: 22 August 2021
/
Accepted: 26 August 2021
/
Published: 27 August 2021
(This article belongs to the Section Micronutrients and Human Health)
Abstract
:There is little evidence regarding the association between serum vitamin B6 concentration and subsequent mortality. We aimed to evaluate the association of serum vitamin B6 concentration with all-cause, cardiovascular disease (CVD), and cancer mortality in the general population using data from the National Health and Nutrition Examination Survey (NHANES). Our study examined 12,190 adults participating in NHANES from 2005 to 2010 in the United States. The mortality status was linked to National Death Index (NDI) records up to 31 December 2015. Pyridoxal 5′-phosphate (PLP) is the biologically active form of vitamin B6. Vitamin B6 status was defined as deficient (PLP < 20 nmol/L), insufficient (PLP ≥ 20.0 and <30.0 nmol/L), and sufficient (PLP ≥ 30.0 nmol/L). We established Cox proportional-hazards models to estimate the associations of categorized vitamin B6 concentration and log-transformed PLP concentration with all-cause and cause-specific mortality by calculating hazard ratios (HRs) and 95% confidence intervals (95%CIs). In our study, serum vitamin B6 was sufficient in 70.6% of participants, while 12.8% of the subjects were deficient in vitamin B6. During follow-up, a total of 1244 deaths were recorded, including 294 cancer deaths and 235 CVD deaths. After multivariate adjustment in Cox regression, participants with higher serum vitamin B6 had a 15% (HR = 0.85, 95%CI = 0.77, 0.93) reduced risk of all-cause mortality and a 19% (HR = 0.81, 95%CI = 0.68, 0.98) reduced risk for CVD mortality for each unit increment in natural log-transformed PLP. A higher log-transformed PLP was not significantly associated with a lower risk for cancer mortality. Compared with sufficient vitamin B6, deficient (HR = 1.37, 95%CI = 1.17, 1.60) and insufficient (HR = 1.19, 95%CI = 1.02, 1.38) vitamin B6 level were significantly associated with a higher risk for all-cause mortality. There was no significant association for cause-specific mortality. Participants with higher levels of vitamin B6 had a lower risk for all-cause mortality. These findings suggest that maintaining a sufficient level of serum vitamin B6 may lower the all-cause mortality risk in the general population.
1. Introduction
Micronutrients, including minerals and vitamins, are important components of our bodies. However, about two billion people lack key micronutrients globally [1]. Micronutrient deficiency can result in slow growth, high anemia prevalence, increased infection rates, and even death [2]. The 2017 Global Nutrition Report showed that one million premature deaths attributable to micronutrient deficiency have occurred annually [1]. As one of the important micronutrients, the prevalence of vitamin B6 deficiency was about 11% according to the second national report of the Centers for Disease Control and Prevention (CDC) [3]. Vitamin B6 plays a role as an essential coenzyme that regulates catabolic and anabolic processes [4]. It is involved in many enzyme activities as a cofactor, including molecule synthesis, interconversion, and degradation [5]. Researchers have found that suboptimal levels of vitamin B6 were associated with increased risk of chronic diseases such as diabetes [6], cancer [7], and cardiovascular disease (CVD) [8].
There are also several epidemiological studies examining the association of vitamin B6 with all-cause and cause-specific mortality [9,10,11]. Results from cohort analyses including middle-aged and elderly individuals in Shanghai showed that a high dietary intake of vitamin B6 was inversely associated with all-cause and CVD mortality [9]. Cui et al. found that a high dietary intake of vitamin B6 was inversely associated with CVD mortality among Japanese subjects [10]. Another study demonstrated that compared with the lowest tertile of intake of vitamin B6, the highest tertile was associated with a lower risk of all-cause and cancer mortality [11]. Although many previous studies evaluated the associations of vitamin B6 intake with all-cause and cause-specific mortality, the association of serum vitamin B6 concentration with all-cause and cause-specific mortality has not attracted much attention.
Therefore, we used data from the National Health and Nutrition Examination Survey (NHANES) in this study and prospectively investigated the association of serum vitamin B6 with all-cause and cause-specific mortality in the general population of U.S. adults. Additionally, this study emphasized the importance of maintaining a sufficient level of vitamin B6 in our bodies.
2. Materials and Methods
2.1. Study Population
NHANES is a repeated nationally representative cross-sectional survey carried out by the National Center for Health Statistics (NCHS) of the CDC. Briefly, NHANES use a multistage probability sampling design to collect information on health and nutritional status in the United States. More details on survey design and methods in NHANES have been previously published elsewhere [12]. The NCHS Research Ethics Review Board has approved the NHANES, and each survey participant provided informed consent. We used information from this publicly available and deidentified NHANES database so that our study was exempt from review by the Institutional Review Board. The concentration of vitamin B6 was measured from 2003 to 2010 in four cycles of NHANES. However, due to the large difference between the method of measurement in 2003–2004 and that in 2005–2010 and no available adjustment to make them comparable, we only used NHANES data from three cycles, that is, from 2005 to 2010 in this study. Detailed information is displayed on the website of NHANES (www.cdc.gov/nchs/nhanes/index.htm; accessed on 8 April 2021). The concentration of serum vitamin B6 was measured from 2005 to 2010 in 21,281 NHANES participants. Of the 21,281 participants, we excluded 827 participants with extreme values (>Q3 + 3*IQR) of vitamin B6 concentration. Moreover, we excluded 4911 participants without information on mortality and survival status. Furthermore, we excluded 3353 participants missing data on marital status, educational level, family income, body mass index (BMI), smoking status, drinking status, physical activity level. Finally, our study included 12,190 participants.
2.2. Measurement of Vitamin B6
From 2005 to 2010, serum vitamin B6 concentration was measured in NHANES participants by reversed-phase high-performance liquid chromatography (HPLC) using fluorometric detection, in which post-column introduction of a sodium chlorite derivatization was incorporated to improve the signal. The detection limit of HPLC was 0.3 nmol/L. Samples were stored at −70 °C and were stable for at least 5 years. Refrigerated samples could be used if they were brought promptly from the site of collection within 2 h.
2.3. Ascertainment of Mortality
Ascertainment of all-cause and cause-specific mortality was performed through linkage to National Death Index (NDI) records until 31 December 2015. The cause of death was determined according to the 10th revision of the International Classification of Disease (ICD-10). The main outcomes in our study were all-cause, CVD, and cancer mortality. CVD mortality was defined as ICD-10 codes I00–I09, I11, I13, I20–I51, and I60–I69, and cancer mortality was defined as ICD-10 codes C00–C97.
2.4. Assessment of Covariates
Information on sociodemographic factors and lifestyle factors at baseline was obtained via examination and questionnaire-based interviews. Sociodemographic factors included age, sex, race/ethnicity, marital status, education level, family income. Lifestyle factors included BMI, consumption of cigarettes and alcohol, and physical activity level. Race/ethnicity was categorized as Hispanic, non-Hispanic white, non-Hispanic black, or other non-Hispanic. Education level was separated into three levels: less than high school; high school or equivalent; college or above. Marital status was classified into three levels: married or living with partner; widowed, divorced, or separated; never married. Family income-to-poverty ratio was divided into three levels: 0–1.0; 1.1–3.0; >3.0 BMI was equal to weight (kilogram) divided by height (meter) squared and categorized as normal weight or underweight (<25 kg/m2), pre-obese (25–29.9 kg/m2), obese (≥30 kg/m2). Drinking status was classified as never drinker, former drinker, or current drinker. Smoking status was separated as never smoker, former smoker, or current smoker. Physical activity was categorized as whether the participants met or not the recommendation to perform at least 150 min of moderate to vigorous physical activity (MVPA) (75 min of vigorous physical activity or 150 min of moderate physical activity) each week as reported in the 2020 World Health Organization (WHO) Physical Activity Guidelines [13].
2.5. Data Analysis
Due to the complex design of NHANES, sample weights, clustering, and stratification were taken into consideration in all analyses. Survival time was calculated from the date of measurement of serum vitamin B6 concentration to the time of death or the end of the study period (31 December 2015), whichever came first. Age was described as mean value with standard error (SE). Categorized variables were shown as frequency with percentage. One-way analysis of variance (ANOVA) with Bonferroni test was used to examine age differences between three groups, while the chi-square test was implemented to test the difference of categorized variables between three groups. Cox proportional hazards regression models were established to examine the association of serum vitamin B6 with all-cause and cause-specific mortality by calculating hazard ratios (HRs) and 95% confidence intervals (CIs). Pyridoxal 5′-phosphate (PLP) was the biologically active form of vitamin B6 and was used to reflect the level of vitamin B6 in our body [14,15]. According to the definition of vitamin B6 status, serum vitamin B6 was categorized as deficient (PLP < 20 nmol/L), insufficient (PLP ≥ 20.0 and <30.0 nmol/L), and sufficient (PLP ≥ 30.0 nmol/L) [16]. Serum PLP concentrations were log-transformed due to non-normal distribution and analyzed as the continuous variable. We used three models to investigate the association of serum vitamin B6 with all-cause and cause-specific mortality. In model 1, we only adjusted for age (<60 years; ≥60 years) and sex (male; female). In model 2, we further adjusted for race/ethnicity (Hispanic; non-Hispanic white; non-Hispanic black; other non-Hispanic), marital status (married or living with partner; widowed, divorced, or separated; never married), education level (less than high school; high school or equivalent; college or above), family income/poverty ratio (0–1.0; 1.1–3.0; >3.0). In model 3, we further adjusted for BMI (normal weight or underweight [<25 kg/m2]; pre-obese [25–29.9 kg/m2]; obese [≥30 kg/m2]), smoking status (never smoker; former smoker; current smoker), drinking status (never drinker; former drinker; current drinker), physical activity level (<150 min MVPA/week; ≥150 min MVPA/week). We also calculated the E-value, which was the minimum strength of association of unmeasured confounders with treatment and outcome on the risk ratio scale [17]. In addition, we explored potential nonlinear associations between log-transformed PLP concentrations and mortality using restricted cubic spline regression with four knots (5th, 35th, 65th, 95th) after multivariate adjustment as mentioned above.
To test the robustness of the results, we conducted several sensitivity analyses in our study. First, we examined the associations after excluding participants who died in the first two years of follow-up to reduce the potential role of reverse causation. Second, as renal dysfunction may influence circulating vitamin B6 levels and cardiovascular events, we estimated renal function by calculating glomerular filtration rate (eGFR) according to the CKD-EPI Creatinine Equation (2009) [18] and further adjusted for renal function (eGFR ≥ 60 mL/min·1.73 m2; eGFR < 60 mL/min·1.73 m2). Third, repeated analyses were performed according to tertiles of serum vitamin B6. All data analyses were conducted using Stata version 15 (Stata Corp, College Station, TX, USA). Two-sided p < 0.05 was considered statistically significant.
3. Results
Of the 12,190 participants (6010 men [49.0%]; mean age [SE], 46.6 [0.4] years), 1244 died, including 294 cancer deaths and 235 CVD deaths. Table 1 shows the characteristics of the study population at baseline. Overall, the participants in our study were more likely to be women, Non-Hispanic White, and married. They tended to consume alcohol, never smoke, and met the recommendation of 150 min/week of MVPA. Most participants had high family income, educational level, and BMI. Vitamin B6 was sufficient in the majority of participants (70.6%), and only 12.8% of the participants were deficient in vitamin B6. Participants with higher PLP levels, in general, were more likely to be younger, married, non-Hispanic White, current drinkers, and less likely to smoke cigarettes and be obese and they tended to have higher education level and family income and perform more than 150 min MVPA each week.
After multivariate adjustment for sociodemographic factors and lifestyle factors in a cox proportional hazards model, deficient and insufficient vitamin B6 were significantly associated with a higher risk for all-cause mortality. There was no significant association of serum vitamin B6 level with cancer and CVD mortality. Compared with those with sufficient serum vitamin B6, participants with deficient serum vitamin B6 had a 37% (HR = 1.37, 95%CI = 1.17, 1.60) higher risk for all-cause mortality. A high risk for all-cause mortality was also observed among those insufficient in vitamin B6 (HR = 1.19, 95%CI = 1.02, 1.38). The magnitude of unmeasured confounding needed to explain away these associations was 2.08 for deficient vitamin B6 and 1.67 for insufficient vitamin B6. For the association with cancer mortality, HR was 1.22 (95%CI = 0.85, 1.74) for deficient vitamin B6 and 1.38 (95%CI = 0.95, 2.02) for insufficient vitamin B6. Participants deficient and insufficient in vitamin B6 had HRs of at least 1.74 and 2.10 beyond the measured confounders, respectively. For the association with CVD mortality, the participants deficient and insufficient in vitamin B6 had a 26% (HR = 1.26, 95%CI = 0.89, 1.77) and a 7% (HR = 1.07, 95%CI = 0.65, 1.78) increased risk, respectively. The corresponding E-values were 1.83 for deficient vitamin B6 and 1.34 for insufficient vitamin B6. Our results also indicated a significant association of log-transformed PLP concentration with all-cause and CVD mortality. A per unit increment in the log-transformed PLP concentration was associated with a 15% (HR = 0.85, 95%CI = 0.77, 0.93) reduced risk for all-cause mortality and a 19% (HR = 0.81, 95%CI = 0.68, 0.98) reduced risk for CVD mortality. No significant association was observed between PLP concentration and CVD mortality (HR = 0.81, 95%CI = 0.66, 1.01). The association of serum vitamin B6 with all-cause and cause-specific mortality and E-value is shown in Table 2 and Table 3, respectively. The detailed association of serum vitamin B6 with all-cause and cause-specific mortality is shown in Tables S1–S3.
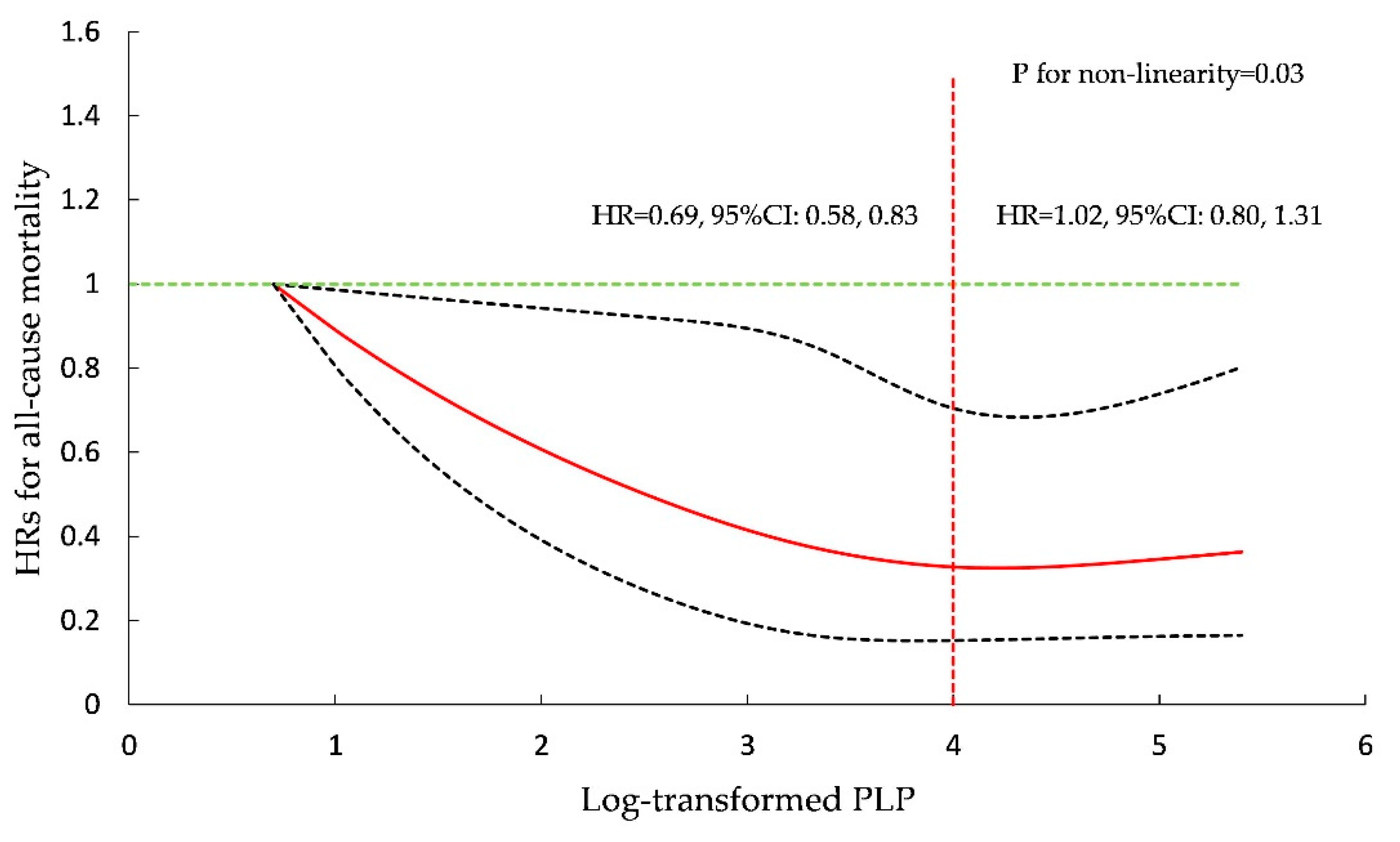
In further analysis, restricted cubic spline regression with four knots (5th, 35th, 65th, 95th) after multivariate adjustment as mentioned above demonstrated a non-linear relationship between serum PLP and all-cause mortality (p for non-linearity = 0.03). Figure 1 shows the HRs for all-cause mortality in restricted cubic spline regression with three knots. The HR for all-cause mortality decreased steadily as PLP concentration increased and almost did not change when log-transformed PLP concentration was >4. A per unit increment in log-transformed PLP could reduce by 31% (HR = 0.69, 95%CI = 0.58, 0.83) the risk for all-cause mortality among participants with log-transformed PLP ≤ 4, while for log-transformed PLP concentration >4, the HR for the association of log-transformed PLP with all-cause mortality was 1.02 (95%CI = 0.80, 1.31). The HRs for cause-specific mortality are shown in Figures S1 and S2.
In sensitivity analyses, the majority of the results were consistent with our primary results. When excluding deaths within 2 years of follow-up, an association of deficient and insufficient vitamin B6 with all-cause mortality was observed but was not statistically significant (Table S4). After further adjustment for eGFR, consistent results were obtained (Table S5). Furthermore, when serum vitamin B6 was classified as tertiles, the participants with lower serum vitamin B6 had lower all-cause and cancer mortality (Table S6).
4. Discussion
In the analysis of this nationally representative prospective cohort study of U.S. adults, we found that deficient and insufficient serum vitamin B6 were significantly associated with a higher risk for all-cause mortality. Participants deficient and insufficient in serum vitamin B6 had a higher risk for cancer mortality and CVD mortality, but these associations were not statistically significant. We also found a significant association of PLP as a continuous variable with all-cause and CVD mortality.
The prevalence of deficiency in serum vitamin B6 was 12.8% in our study, which was almost the same as that in a previous study (11%) [3]. This may be partly due to the fact that many common foods, such as various meats and vegetables, are rich in vitamin B6 and thus contribute to maintaining a sufficient vitamin B6 status [15]. To our knowledge, only a few studies investigated the association of serum vitamin B6 concentration with all-cause and cause-specific mortality [19,20,21,22,23]. A prospective cohort study examined the association of serum vitamin B6 concentration with all-cause mortality and found that vitamin B6 concentration, whether as a continuous variable or categorized variable, was significantly associated with all-cause mortality [19]. Meanwhile, Huang et.al. investigated the effects of the vitamin B group on all-cause mortality in elderly individuals in Taiwan and found that participants with sufficient vitamin B6 had a lower risk for all-cause mortality, which is almost consistent with our results [21]. Moreover, a prospective case–cohort Study also found that renal cell carcinoma patients with high PLP had a significantly lower risk for all-cause mortality, which supports our results [22].
In addition, a previous epidemiological study showed a significant association between serum continuous vitamin B6 and CVD mortality and an association of deficient vitamin B6 with CVD mortality [19]. Our study also found that vitamin B6, as a continuous variable, was significantly associated with CVD mortality. A research demonstrated that vitamin B6 is linked to cardiovascular events [24]. Vitamin B6 could reduce the concentration of serum homocysteine [25], which is a risk factor for cardiovascular disease [26]. As categorized variables, deficient and insufficient vitamin B6 corresponded to a higher risk for CVD mortality in our study, but the association was not significant for both vitaminB6 status. This may because that epidemiological study was conducted among renal transplant recipients. It was estimated that low circulating concentrations of PLP were common in renal disease patients [27]. A low PLP concentration and renal disease could both increase the risk for CVD [8,28]. Another study found that renal transplant recipients deficient in vitamin B6 had a worse functional vitamin B6 status than healthy people and renal transplant recipients sufficient in vitamin B6 [20]. Compared with the low vitamin B6 concentration common in renal disease patients, vitamin B6 level varied widely, and the majority of participants had a high concentration in our study. Consequently, although a low level of vitamin B6 could increase the risk for CVD mortality, a significant association of deficient vitamin B6 level with CVD mortality was more likely to be observed among renal disease patients than among the general population in our study.
In terms of cancer mortality, David et.al. found that PLP concentration was significantly associated with renal cell carcinoma mortality [22]. However, we did not observe a significant association between PLP level and cancer mortality. It was reported that vitamin B6 level is related to cancer events [29]. Vitamin B6 deficiency could lead to changes affecting genes, such as chromosome breaks and alterations in gene expression [30], which would increase the risk of cancer occurrence. The non-significant association in our study may be partly because the PLP concentration was lower in David’s study than in ours. In that study, only less than 50% of participants had sufficient vitamin B6 concentration, and 30% of them would be considered deficient in vitamin B6. However, in our study, 70.6% of participants had sufficient vitamin B6, and only 12.8% of them were deficient in vitamin B6.
In further analysis, regression with restricted cubic spline showed that a high PLP concentration was inversely associated with all-cause mortality and provided no more additional benefits. Another study reported similar results, indicating that the HR for all-cause mortality decreased with a moderate increase of PLP concentration, and the risk for all-cause mortality did not decrease with a high level of PLP [23]. Generally, adults in the United States take vitamin B6-containing supplements regularly [31]. High PLP concentrations would be observed shortly after taking vitamin B6-containing supplements, which would lead to a right-skewed distribution of vitamin B6 concentrations. Consequently, the risk associations at higher concentrations of vitamin B6 could be expected to tend toward the mean risk.
After excluding participants who died within 2 years of follow-up, it was observed that deficient and insufficient vitamin B6 levels were associated with an increased risk for mortality, but this association was not statistically significant. Of those 241 participants who died in the first 2 years of follow-up, 32.3% and 17.1% had deficient and insufficient vitamin B6, respectively. Moreover, 109 adult participants died from cancer and CVD. Compared with the proportion of deficient (12.8%) and insufficient (16.6%) vitamin B6, the proportion of participants deficient for vitamin B6 among those 241 adults was larger. This could reduce the HRs for mortality after excluding participants who died within 2 years of follow-up, especially for the association of deficient vitamin B6, and even lead to non-significant associations of deficient and insufficient vitamin B6 with all-cause mortality. Additionally, it is suggested that upcoming death or diseases may lead to reduced vitamin B6 concentration. Future studies can investigate the prospective effect of disease on vitamin B6 concentration.
This study has several strengths. First, we used data from a large national database, which is representative of the general population. Second, we investigated associations considering PLP both as a categorized variable and as a continuous variable. Third, we adjusted for many sociodemographic factors and lifestyle factors to estimate the association of serum vitamin B6 with all-cause and cause-specific mortality. However, there are still a few limitations in this study. First, our study has the common limitations of observational studies. Therefore, a random control trial is needed to explore the examined associations in the future. Second, we did not investigate the association of vitamin B6 with mortality in groups stratified by covariates. Future studies could evaluate this association in subgroups stratified by covariates and examine whether interactions exist. Third, considering the limitations of PLP as a biomarker, the ratio 4-pyridoxic acid (PA)/(pyridoxal + PLP) (PAr) was proposed to reflect the vitamin B6 status [32,33]. The association of PAr with all-cause and cause-specific mortality could be investigated in further analyses.
5. Conclusions
This study revealed that as a categorized variable, vitamin B6 was inversely associated with all-cause mortality after multivariate adjustment, including sociodemographic factors and lifestyle factors. Meanwhile, a higher log-transformed PLP concentration was associated with a lower risk of all-cause and CVD mortality. Hence, to reduce the risk of mortality, it is essential to address vitamin B6 and increase the concentration of PLP.
Supplementary Materials
The following are available online at https://www.mdpi.com/article/10.3390/nu13092977/s1. Figure S1: Association of pyridoxal 5′-phosphate (PLP) with cancer mortality in restricted cubic regression with four knots (5th, 35th, 65th, 95th) in NHANES participants from 2005 to 2010. Figure S2: Association of pyridoxal 5′-phosphate (PLP) with cardiovascular disease (CVD) mortality in restricted cubic regression with four knots (5th, 35th, 65th, 95th) in NHANES participants from 2005 to 2010. Table S1: Associations between serum vitamin B6 and all-cause mortality in adults from the NHANES. Table S2: Associations between serum vitamin B6 and cancer mortality in adults from the NHANES. Table S3: Associations between serum vitamin B6 and CVD mortality in adults from the NHANES. Table S4: HRs (95% CIs) of all-cause and specific-cause mortality according to serum vitamin B6 concentrations after excluding participants who died within 2 years of follow-up in NHANES participants from 2005 to 2010. Table S5: HRs (95% CIs) of all-cause and specific cause mortality according to serum vitamin B6 concentrations after further adjustment for estimated glomerular filtration rate (eGFR) in NHANES participants from 2005 to 2010. Table S6: HRs (95% CIs) of all-cause and specific cause mortality according to tertiles of serum pyridoxal 5′-phosphate (PLP) concentrations in NHANES participants from 2005 to 2010.
Author Contributions
Conceptualization, D.Y., Y.W. and C.Y.; methodology, D.Y. and Y.L.; software, D.Y.; validation, D.Y. and Y.L.; formal analysis, D.Y.; investigation, D.Y.; resources, D.Y. and C.Y.; data curation, D.Y.; writing—original draft preparation, D.Y.; writing—review and editing, D.Y., Y.L., Y.M. and J.B.; visualization, D.Y., Y.M. and J.B.; funding acquisition, C.Y. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the National Natural Science Foundation of China (Grant No. 81773552) and the National Key Research and Development Program of China (Grant No. 2018YFC1315302).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Publicly available datasets were analyzed in this study. Data can be found here: www.cdc.gov/nchs/nhanes/index.htm (accessed on 8 April 2021).
Conflicts of Interest
The authors declare no conflict of interest.
References
- World Health Organization. Global Nutrition Report 2017: Nourishing the SDGs; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- World Health Organization. Global Health Risks: Mortality and Burden of Disease Attributable to Selected Major Risks; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Pfeiffer, C.M.; Sternberg, M.R.; Schleicher, R.L.; Haynes, B.M.; Rybak, M.E.; Pirkle, J.L. The CDC’s Second National Report on Biochemical Indicators of Diet and Nutrition in the U.S. Population is a valuable tool for researchers and policy makers. J. Nutr. 2013, 143, 938s–947s. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agnoli, C.; Grioni, S.; Krogh, V.; Pala, V.; Allione, A.; Matullo, G.; Di Gaetano, C.; Tagliabue, G.; Pedraglio, S.; Garrone, G.; et al. Plasma Riboflavin and Vitamin B-6, but Not Homocysteine, Folate, or Vitamin B-12, Are Inversely Associated with Breast Cancer Risk in the European Prospective Investigation into Cancer and Nutrition-Varese Cohort. J. Nutr. 2016, 146, 1227–1234. [Google Scholar] [CrossRef] [Green Version]
- Percudani, R.; Peracchi, A. The B6 database: A tool for the description and classification of vitamin B6-dependent enzymatic activities and of the corresponding protein families. BMC Bioinform. 2009, 10, 273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mascolo, E.; Vernì, F. Vitamin B6 and Diabetes: Relationship and Molecular Mechanisms. Int. J. Mol. Sci. 2020, 21, 3669. [Google Scholar] [CrossRef] [PubMed]
- Wu, W.; Kang, S.; Zhang, D. Association of vitamin B6, vitamin B12 and methionine with risk of breast cancer: A dose-response meta-analysis. Br. J. Cancer 2013, 109, 1926–1944. [Google Scholar] [CrossRef] [Green Version]
- Minović, I.; Kieneker, L.M.; Gansevoort, R.T.; Eggersdorfer, M.; Touw, D.J.; Voerman, A.J.; Connelly, M.A.; Boer, R.A.; Hak, E.; Bos, J.; et al. Vitamin B6, Inflammation, and Cardiovascular Outcome in a Population-Based Cohort: The Prevention of Renal and Vascular End-Stage Disease (PREVEND) Study. Nutrients 2020, 12, 2711. [Google Scholar] [CrossRef]
- Zhao, L.G.; Shu, X.O.; Li, H.L.; Gao, J.; Han, L.H.; Wang, J.; Fang, J.; Gao, Y.T.; Zheng, W.; Xiang, Y.B. Prospective cohort studies of dietary vitamin B6 intake and risk of cause-specific mortality. Clin. Nutr. (Edinb. Scotl.) 2019, 38, 1180–1187. [Google Scholar] [CrossRef]
- Cui, R.; Iso, H.; Date, C.; Kikuchi, S.; Tamakoshi, A. Dietary folate and vitamin b6 and B12 intake in relation to mortality from cardiovascular diseases: Japan collaborative cohort study. Stroke 2010, 41, 1285–1289. [Google Scholar] [CrossRef] [Green Version]
- Ricci, C.; Freisling, H.; Leitzmann, M.F.; Taljaard-Krugell, C.; Jacobs, I.; Kruger, H.S.; Smuts, C.M.; Pieters, M. Diet and sedentary behaviour in relation to cancer survival. A report from the national health and nutrition examination survey linked to the U.S. mortality registry. Clin. Nutr. (Edinb. Scotl.) 2020, 39, 3489–3496. [Google Scholar] [CrossRef]
- Iii, N. National Health and Nutrition Examination Survey (NHANES) Analytic and Reporting Guidelines; National Center for Health Statistics, Centers for Disease Control and Prevention: Hyattsville, MD, USA, 2000.
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef]
- Lamers, Y. Indicators and methods for folate, vitamin B-12, and vitamin B-6 status assessment in humans. Curr. Opin. Clin. Nutr. Metab. Care 2011, 14, 445–454. [Google Scholar] [CrossRef] [PubMed]
- Ueland, P.M.; Ulvik, A.; Rios-Avila, L.; Midttun, Ø.; Gregory, J.F. Direct and Functional Biomarkers of Vitamin B6 Status. Annu. Rev. Nutr. 2015, 35, 33–70. [Google Scholar] [CrossRef] [PubMed]
- Stover, P.J.; Field, M.S. Vitamin B-6. Adv. Nutr. (Bethesda Md.) 2015, 6, 132–133. [Google Scholar] [CrossRef]
- VanderWeele, T.J.; Ding, P. Sensitivity Analysis in Observational Research: Introducing the E-Value. Ann. Intern. Med. 2017, 167, 268–274. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Minović, I.; Riphagen, I.J.; van den Berg, E.; Kootstra-Ros, J.E.; van Faassen, M.; Gomes Neto, A.W.; Geleijnse, J.M.; Gans, R.O.; Eggersdorfer, M.; Navis, G.J.; et al. Vitamin B-6 deficiency is common and associated with poor long-term outcome in renal transplant recipients. Am. J. Clin. Nutr. 2017, 105, 1344–1350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Minović, I.; van der Veen, A.; van Faassen, M.; Riphagen, I.J.; van den Berg, E.; van der Ley, C.; Gomes-Neto, A.W.; Geleijnse, J.M.; Eggersdorfer, M.; Navis, G.J.; et al. Functional vitamin B-6 status and long-term mortality in renal transplant recipients. Am. J. Clin. Nutr. 2017, 106, 1366–1374. [Google Scholar] [CrossRef] [Green Version]
- Huang, Y.C.; Lee, M.S.; Wahlqvist, M.L. Prediction of all-cause mortality by B group vitamin status in the elderly. Clin. Nutr. (Edinb. Scotl.) 2012, 31, 191–198. [Google Scholar] [CrossRef]
- Muller, D.C.; Johansson, M.; Zaridze, D.; Moukeria, A.; Janout, V.; Holcatova, I.; Navratilova, M.; Mates, D.; Midttun, Ø.; Ueland, P.M.; et al. Circulating Concentrations of Vitamin B6 and Kidney Cancer Prognosis: A Prospective Case-Cohort Study. PLoS ONE 2015, 10, e0140677. [Google Scholar] [CrossRef] [Green Version]
- Ulvik, A.; Pedersen, E.R.; Svingen, G.F.; McCann, A.; Midttun, Ø.; Nygård, O.; Ueland, P.M. Vitamin B-6 catabolism and long-term mortality risk in patients with coronary artery disease. Am. J. Clin. Nutr. 2016, 103, 1417–1425. [Google Scholar] [CrossRef]
- Dhalla, N.S.; Takeda, S.; Elimban, V. Mechanisms of the beneficial effects of vitamin B6 and pyridoxal 5-phosphate on cardiac performance in ischemic heart disease. Clin. Chem. Lab. Med. 2013, 51, 535–543. [Google Scholar] [CrossRef] [PubMed]
- Herrmann, W.; Herrmann, M.; Obeid, R. Hyperhomocysteinaemia: A critical review of old and new aspects. Curr. Drug Metab. 2007, 8, 17–31. [Google Scholar] [CrossRef] [PubMed]
- Bots, M.L.; Launer, L.J.; Lindemans, J.; Hofman, A.; Grobbee, D.E. Homocysteine, atherosclerosis and prevalent cardiovascular disease in the elderly: The Rotterdam Study. J. Intern. Med. 1997, 242, 339–347. [Google Scholar] [CrossRef]
- Hafkenscheid, J.C.; Rosier, J.G.; van Dijk, C.M. Relationship between plasma pyridoxal-5’-phosphate concentration and the apoenzyme content of serum aminotransferases in patients with a renal allograft. Clin. Chim. Acta Int. J. Clin. Chem. 1984, 144, 137–144. [Google Scholar] [CrossRef]
- Rucker, D.; Tonelli, M. Cardiovascular risk and management in chronic kidney disease. Nat. Rev. Nephrol. 2009, 5, 287–296. [Google Scholar] [CrossRef]
- Galluzzi, L.; Vacchelli, E.; Michels, J.; Garcia, P.; Kepp, O.; Senovilla, L.; Vitale, I.; Kroemer, G. Effects of vitamin B6 metabolism on oncogenesis, tumor progression and therapeutic responses. Oncogene 2013, 32, 4995–5004. [Google Scholar] [CrossRef] [Green Version]
- Selhub, J. Folate, vitamin B12 and vitamin B6 and one carbon metabolism. J. Nutr. Health Aging 2002, 6, 39–42. [Google Scholar]
- Kantor, E.D.; Rehm, C.D.; Du, M.; White, E.; Giovannucci, E.L. Trends in Dietary Supplement Use among US Adults from 1999-2012. JAMA 2016, 316, 1464–1474. [Google Scholar] [CrossRef]
- Ulvik, A.; Midttun, Ø.; Pedersen, E.R.; Eussen, S.J.; Nygård, O.; Ueland, P.M. Evidence for increased catabolism of vitamin B-6 during systemic inflammation. Am. J. Clin. Nutr. 2014, 100, 250–255. [Google Scholar] [CrossRef] [Green Version]
- Ueland, P.M.; McCann, A.; Midttun, Ø.; Ulvik, A. Inflammation, vitamin B6 and related pathways. Mol. Asp. Med. 2017, 53, 10–27. [Google Scholar] [CrossRef]
Figure 1.
Association of pyridoxal 5′-phosphate (PLP) with all-cause mortality in restricted cubic regression with four knots (5th, 35th, 65th, 95th) in NHANES participants from 2005 to 2010.
Figure 1.
Association of pyridoxal 5′-phosphate (PLP) with all-cause mortality in restricted cubic regression with four knots (5th, 35th, 65th, 95th) in NHANES participants from 2005 to 2010.


{kind=link}
Table 1.
Baseline characteristics of participants in NHANES from 2005 to 2010 a.
| Total | Vitamin B6 | p Value | |||
|---|---|---|---|---|---|
| Deficient (12.8%) | Insufficient (16.6%) | Sufficient (70.6%) | |||
| Age, mean (SE) | 46.6 (0.4) | 50.1 (0.6) | 46.5 (0.5) | 46.0 (0.4) | <0.01 |
| Sex, % | <0.01 | ||||
| Male | 49.0 | 35.3 | 39.5 | 53.8 | |
| Female | 51.0 | 64.8 | 60.6 | 46.2 | |
| Race/ethnicity, % | <0.01 | ||||
| Hispanic | 12.1 | 9.6 | 12.1 | 12.6 | |
| Non-Hispanic White | 71.8 | 70.3 | 69.3 | 72.6 | |
| Non-Hispanic Black | 10.7 | 16.8 | 13.4 | 9.0 | |
| Non-Hispanic other | 5.4 | 3.4 | 5.2 | 5.8 | |
| Educational level, % | <0.01 | ||||
| Less than high school | 18.5 | 27.3 | 20.5 | 16.3 | |
| High school or equivalent | 24.3 | 29.7 | 27.0 | 22.7 | |
| College or above | 57.2 | 43.0 | 52.4 | 60.9 | |
| Marital Status, % | <0.01 | ||||
| Married or living with partner | 64.8 | 59.2 | 62.4 | 66.5 | |
| Widowed, divorced, or separated | 18.8 | 26.8 | 21.2 | 16.8 | |
| Never married | 16.3 | 16.1 | 16.4 | 16.7 | |
| Family income-poverty ratio, % | <0.01 | ||||
| 0.0–1.0 | 13.2 | 21.4 | 15.7 | 11.1 | |
| 1.1–3.0 | 35.7 | 43.6 | 38.6 | 33.6 | |
| >3.0 | 51.1 | 35.0 | 45.7 | 55.4 | |
| BMI, kg/m2, % | <0.01 | ||||
| <25.0 | 30.7 | 24.2 | 27.4 | 32.7 | |
| 25.0–29.9 | 33.3 | 26.40 | 28.4 | 35.8 | |
| ≥30.0 | 36.0 | 49.4 | 44.2 | 31.5 | |
| Drinking status, % | <0.01 | ||||
| Never drinker | 10.8 | 14.5 | 11.9 | 9.9 | |
| Ever drinker | 16.5 | 26.0 | 17.6 | 14.5 | |
| Current drinker | 72.7 | 59.5 | 70.5 | 75.6 | |
| Smoking Status, % | <0.01 | ||||
| Never smoker | 52.2 | 38.4 | 49.4 | 55.4 | |
| Ever smoker | 24.7 | 22.1 | 22.6 | 25.7 | |
| Current smoker | 23.1 | 39.6 | 28.1 | 19.0 | |
| Physical activity, % | <0.01 | ||||
| <150 min MVPA | 46.8 | 61.3 | 50.6 | 43.2 | |
| ≥150 min MVPA | 53.2 | 38.7 | 49.4 | 56.8 | |
Abbreviation: NHANES, National Health and Nutrition Examination Survey; SE, standard error; BMI, body mass index; MVPA, moderate to vigorous physical activity. a The NHANES used a complex design. Weight was taken into consideration. Continuous variables are shown as weighted mean and SE, while categorized variables are described as frequency and weighted percentage.
Table 2.
HRs (95% CIs) of all-cause and specific-cause mortality according to serum vitamin B6 concentrations.
Table 2.
HRs (95% CIs) of all-cause and specific-cause mortality according to serum vitamin B6 concentrations.
| Vitamin B6 Status | Per Unit Increment in Log-Transformed PLP | |||
|---|---|---|---|---|
| Deficient | Insufficient | Sufficient | ||
| All-cause mortality | ||||
| Number of deaths/total | 296/1886 | 244/2157 | 704/8147 | 1244/12,190 |
| Model 1 | 1.83 (1.55,2.15) | 1.37 (1.17,1.60) | 1.00 | 0.72 (0.65,0.80) |
| Model 2 | 1.50 (1.28,1.75) | 1.20 (1.04,1.40) | 1.00 | 0.82 (0.74,0.90) |
| Model 3 | 1.37 (1.17,1.60) | 1.19 (1.02,1.38) | 1.00 | 0.85 (0.77,0.93) |
| Cancer mortality | ||||
| Number of deaths | 67 | 66 | 161 | 294 |
| Model 1 | 1.72 (1.19,2.49) | 1.61 (1.11,2.32) | 1.00 | 0.68 (0.54,0.85) |
| Model 2 | 1.43 (1.00,2.03) | 1.43 (0.98,2.11) | 1.00 | 0.76 (0.61,0.95) |
| Model 3 | 1.22 (0.85,1.74) | 1.38 (0.95,2.02) | 1.00 | 0.81 (0.66,1.01) |
| CVD mortality | ||||
| Number of deaths | 47 | 45 | 143 | 235 |
| Model 1 | 1.65 (1.18,2.31) | 1.29 (0.78,2.12) | 1.00 | 0.70 (0.58,0.83) |
| Model 2 | 1.31 (0.93,1.85) | 1.07 (0.66,1.73) | 1.00 | 0.80 (0.67,0.97) |
| Model 3 | 1.26 (0.89,1.77) | 1.07 (0.65,1.78) | 1.00 | 0.81 (0.68,0.98) |
Model 1: adjusted for age (<60 years; ≥60 years) and sex (male; female). Model 2: further adjusted (from Model 1) for race/ethnicity (Hispanic; non-Hispanic white; non-Hispanic black; other non-Hispanic), marital status (married or living with partner; widowed, divorced, or separated; never married), education level (less than high school; high school or equivalent; college or above), family income/poverty ratio (0–1.0; 1.1–3.0; >3.0). Model 3: further adjusted (from Model 2) for BMI (normal weight or underweight [<25 kg/m2]; pre-obese [25–29.9 kg/m2]; obese [≥30 kg/m2]), smoking status (never smoker; former smoker; current smoker), drinking status (never drinker; former drinker; current drinker), physical activity level (<150 min MVPA/week; ≥150 min MVPA/week).
Table 3.
E-values for the point estimates.
| HR (95%CI) | E-Value | |
|---|---|---|
| All-cause mortality | ||
| Deficient | 1.37 (1.17,1.60) | 2.08 |
| Insufficient | 1.19 (1.02,1.38) | 1.67 |
| Sufficient | 1.00 | NA |
| Cancer mortality | ||
| Deficient | 1.22 (0.85,1.74) | 1.74 |
| Insufficient | 1.38 (0.95,2.02) | 2.10 |
| Sufficient | 1.00 | NA |
| CVD mortality | ||
| Deficient | 1.26 (0.89,1.77) | 1.83 |
| Insufficient | 1.07 (0.65,1.78) | 1.34 |
| Sufficient | 1.00 | NA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Yang, D.; Liu, Y.; Wang, Y.; Ma, Y.; Bai, J.; Yu, C. Association of Serum Vitamin B6 with All-Cause and Cause-Specific Mortality in a Prospective Study. Nutrients 2021, 13, 2977. https://doi.org/10.3390/nu13092977
AMA Style
Yang D, Liu Y, Wang Y, Ma Y, Bai J, Yu C. Association of Serum Vitamin B6 with All-Cause and Cause-Specific Mortality in a Prospective Study. Nutrients. 2021; 13(9):2977. https://doi.org/10.3390/nu13092977
Chicago/Turabian StyleYang, Donghui, Yan Liu, Yafeng Wang, Yudiyang Ma, Jianjun Bai, and Chuanhua Yu. 2021. "Association of Serum Vitamin B6 with All-Cause and Cause-Specific Mortality in a Prospective Study" Nutrients 13, no. 9: 2977. https://doi.org/10.3390/nu13092977
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.