
Obesity and Circulating Levels of Vitamin D before and after Weight Loss Induced by a Very Low-Calorie Ketogenic Diet

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Diet Intervention αnd Habitual Intake οf Vitamin D
2.3. Anthropometric αnd Clinical Measurements
2.4. Laboratory Analysis
2.5. Statistical Analysis
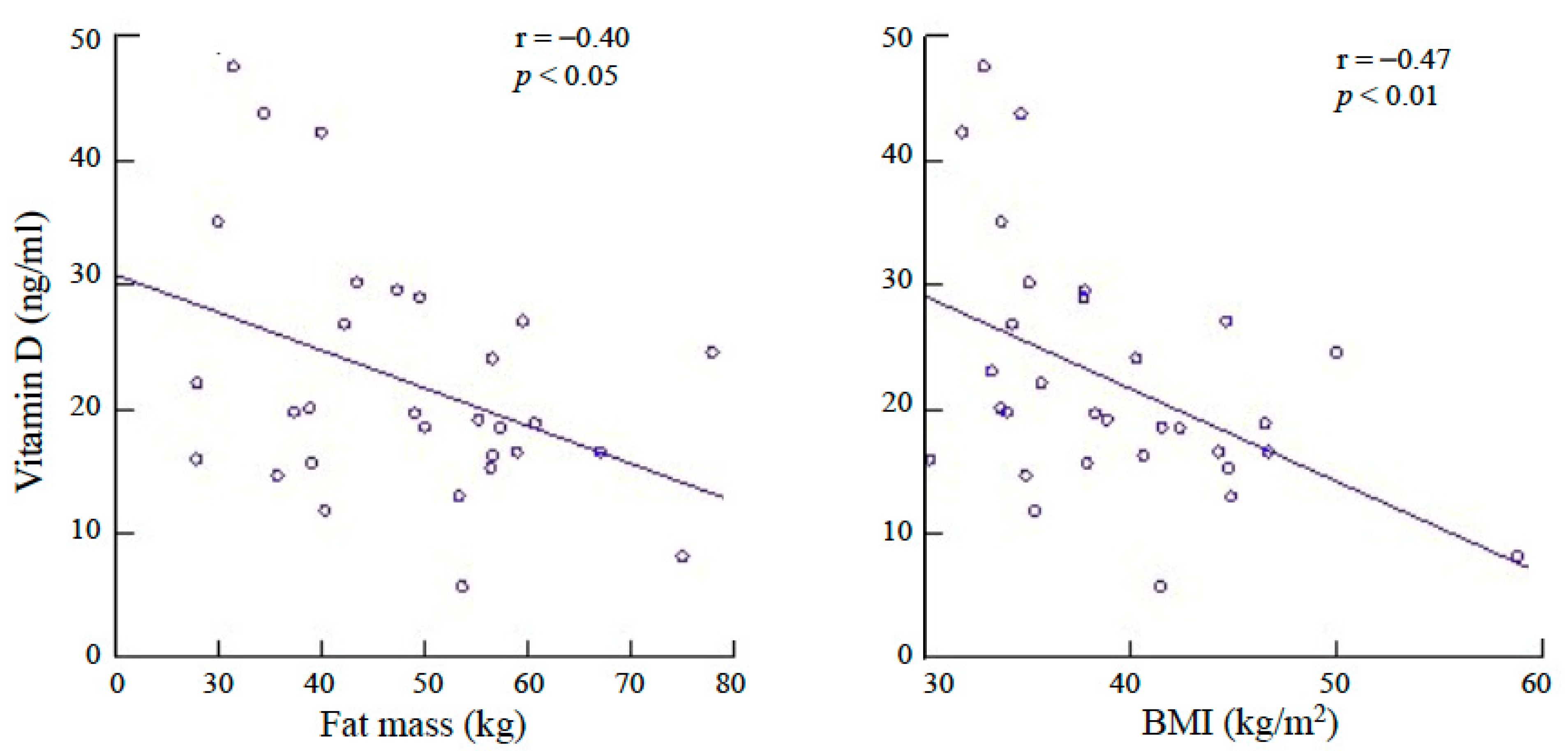
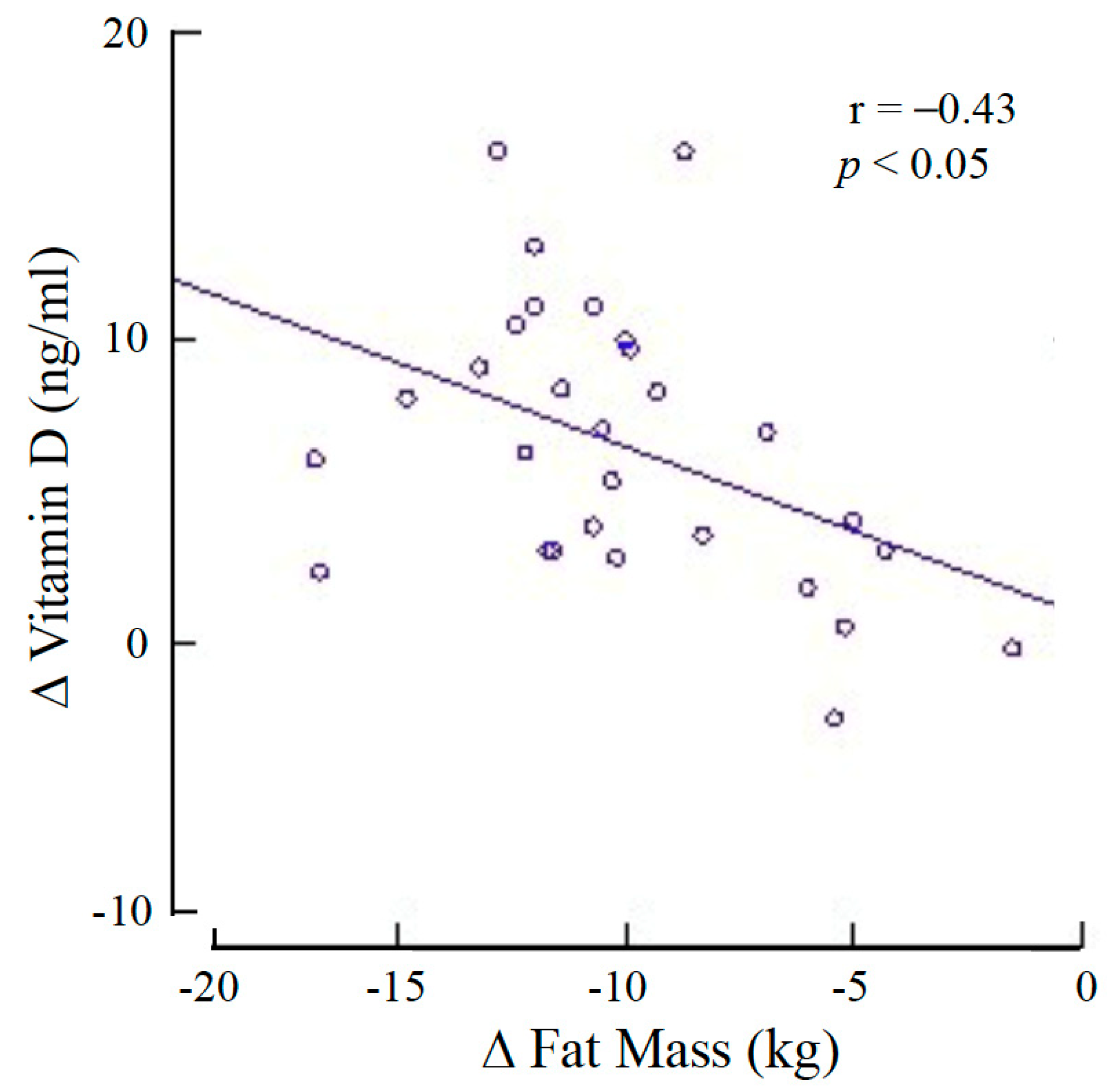
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Reid, I.R.; Bolland, M.J.; Grey, A. Effects of vitamin D supplements on bone mineral density: A systematic review and meta-analysis. Lancet 2014, 383, 146–155. [Google Scholar] [CrossRef]
- Zupo, R.; Castellana, F.; Sardone, R.; Lampignano, L.; Di Noia, C.; Savastano, S.; Giannelli, G.; De Pergola, G. Hydroxyvitamin D serum levels are negatively associated with platelet number in a cohort of subjects affected by overweight and obesity. Nutrients 2020, 12, 474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Pergola, G.; Triggiani, V.; Bartolomeo, N.; Giagulli, V.A.; Anelli, M.; Masiello, M.; Candita, V.; De Bellis, D.; Silvestris, F. Low 25 hydroxyvitamin D levels are independently associated with autoimmune thyroiditis in a cohort of apparently healthy overweight and obese subjects. Endocr. Metab. Immune Disord. Drug Targets 2018, 18, 646–652. [Google Scholar] [CrossRef]
- Holick, M.F. Vitamin D deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef]
- Walsh, J.S.; Evans, A.L.; Bowles, S.; Naylor, K.E.; Jones, K.S.; Schoenmakers, I.; Jacques, R.M.; Eastell, R. Free 25-hydroxyvitamin D is low in obesity, but there are no adverse associations with bone health. Am. J. Clin. Nutr. 2016, 103, 1465–1471. [Google Scholar] [CrossRef] [Green Version]
- Samuel, L.; Borrell, L.N. The effect of body mass index on optimal vitamin D status in U.S. adults: The national health and nutrition examination survey 2001–2006. Ann. Epidemiol. 2013, 23, 409–414. [Google Scholar] [CrossRef]
- Walsh, J.S.; Bowles, S.; Evans, A.L. Vitamin D in obesity. Curr. Opin. Endocrinol. Diabetes Obes. 2017, 24, 389–394. [Google Scholar] [CrossRef] [PubMed]
- De Pergola, G.; Martino, T.; Zupo, R.; Caccavo, D.; Pecorella, C.; Paradiso, S.; Silvestris, F.; Triggiani, V. 25-hydroxyvitamin D levels are negatively and independently associated with fat mass in a cohort of healthy overweight and obese subjects. Endocr. Metab. Immune Disord. Drug Targets 2019, 19, 838–844. [Google Scholar] [CrossRef] [PubMed]
- Worstman, J.; Matsuoka, L.Y.; Chen, T.C.; Lu, Z.; Holick, M.F. Decreased bioavailability of vitamin D in obesity. Am. J. Clin. Nutr. 2000, 72, 690–693. [Google Scholar]
- Roizen, J.D.; Long, C.; Casella, A.; O’Lear, L.; Caplan, I.; Lai, M.; Sasson, I.; Singh, R.; Makowski, A.J.; Simmons, R.; et al. Obesity decreases hepatic 25-hydroxylase activity causing low serum 25-hydroxyvitamin D. J. Bone Miner. Res. 2019, 34, 1068–1073. [Google Scholar] [CrossRef] [PubMed]
- Pannu, P.K.; Zhao, Y.; Soares, M.J. Reductions in body weight and percent fat mass increase the vitamin D status of obese subjects: A systematic review and metaregression analysis. Nutr. Res. 2016, 36, 201–213. [Google Scholar] [CrossRef]
- Mallard, S.R.; Howe, A.S.; Houghton, L.A. Vitamin D status and weight loss: A systematic review and meta-analysis of randomized and nonrandomized controlled weight-loss trials. Am. J. Clin. Nutr. 2016, 104, 1151–1159. [Google Scholar] [CrossRef] [Green Version]
- Lean, M.E.; Leslie, W.S.; Barnes, A.C.; Brosnahan, N.; Thom, G.; McCombie, L.; Peters, C.; Zhyzhneuskaya, S.; Al-Mrabeh, A.; Hollingsworth, K.G.; et al. Primary care-led weight management for remission of type 2 diabetes (DiRECT): An open-label, cluster-randomised trial. Lancet 2018, 391, 541–551. [Google Scholar] [CrossRef] [Green Version]
- Buscemi, S.; Rosafio, G.; Vasto, S.; Massenti, F.M.; Grosso, G.; Galvano, F.; Rini, N.; Barile, A.M.; Maniaci, V.; Cosentino, L.; et al. Validation of a food frequency questionnaire for use in Italian adults living in Sicily. Int. J. Food Sci. Nutr. 2015, 66, 426–438. [Google Scholar] [CrossRef] [PubMed]
- Buscemi, S.; Verga, S.; Batsis, J.A.; Cottone, S.; Mattina, A.; Re, A.; Arnone, M.; Citarda, S.; Cerasola, G. Intra-renal hemodynamics and carotid intima-media thickness in the metabolic syndrome. Diabetes Res. Clin. Pract. 2009, 86, 177–185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buscemi, S.; Blunda, G.; Maneri, R.; Verga, S. Bioelectrical characteristics of type 1 and type 2 diabetic subjects with reference to body water compartments. Acta Diabetol. 1998, 35, 220–223. [Google Scholar] [CrossRef]
- Friedewald, W.T.; Levy, R.I.; Fredrickson, D.S. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin. Chem. 1972, 18, 499–502. [Google Scholar] [CrossRef] [PubMed]
- Florez, H.; Martinez, R.; Chacra, W.; Strickman-Stein, N.; Levis, S. Outdoor exercise reduces the risk of hypovitaminosis D in the obese. J. Steroid Biochem. Mol. Biol. 2007, 103, 679–681. [Google Scholar] [CrossRef]
- Ernst, B.; Thurnheer, M.; Schmid, S.M.; Wilms, B.; Schultes, B. Seasonal variation in the deficiency of 25-hydroxyvitamin D(3) in mildly to extremely obese subjects. Obes. Surg. 2009, 19, 180–183. [Google Scholar] [CrossRef] [Green Version]
- Himbert, C.; Ose, J.; Delphan, M.; Ulrich, C.M. A systematic review of the interrelation between diet- and surgery-induced weight loss and vitamin D status. Nutr. Res. 2017, 38, 13–26. [Google Scholar] [CrossRef]
- Beckman, L.M.; Earthman, C.P.; Thomas, W.; Compher, C.W.; Muniz, J.; Horst, R.L.; Ikramuddin, S.; Kellogg, T.A.; Sibley, S.D. Serum 25(OH) vitamin D concentration changes after Roux-en-Y gastric bypass surgery. Obes. Silver Spring 2013, 21, E599–E606. [Google Scholar] [CrossRef] [PubMed]
- Switzer, N.J.; Marcil, G.; Prasad, S.; Debru, E.; Church, N.; Mitchell, P.; Billington, E.O.; Gill, R.S. Long-term hypovitaminosis D and secondary hyperparathyroidism outcomes of the Roux-en-Y gastric bypass: A systematic review. Obes. Rev. 2017, 18, 560–566. [Google Scholar] [CrossRef]
- Perticone, M.; Maio, R.; Sciacqua, A.; Suraci, E.; Pinto, A.; Pujia, R.; Zito, R.; Gigliotti, S.; Sesti, G.; Perticone, F. Ketogenic diet-induced weight loss is associated with an increase in vitamin D levels in obese adults. Molecules 2019, 24, 2499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Snijder, M.B.; van Dam, R.M.; Visser, M.; Deeg, D.J.; Dekker, J.M.; Bouter, L.M.; Seidell, J.C.; Lips, P. Adiposity in relation to vitamin D status and parathyroid hormone levels: A population-based study in older men and women. J. Clin. Endocrinol. Metab. 2005, 90, 4119–4123. [Google Scholar] [CrossRef] [Green Version]
- Roy, B.; Curtis, M.E.; Fears, L.S.; Nahashon, S.N.; Fentress, H.M. Molecular mechanisms of obesity-induced osteoporosis and muscle atrophy. Front. Physiol. 2016, 7, 439. [Google Scholar] [CrossRef] [Green Version]
- Abbas, M.A. Physiological functions of Vitamin D in adipose tissue. J. Steroid Biochem. Mol. Biol. 2017, 165, 369–381. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Control Group | pa | VLCKD (n = 31) | pb | ||
|---|---|---|---|---|---|
| (n = 20) | Before | After | |||
| Age (years) | 46 ± 8 | 0.29 | 43 ± 11 | ||
| Males (%) | 25.0 | 25.6 | |||
| Body weight (kg) | 71.2 ± 14.8 | <0.001 | 104.3 ± 16.8 | 89.2 ± 15.5 | <0.001 |
| BMI (kg/m2) | 24.1 ± 2.9 | <0.001 | 39.4 ± 6.3 | 33.7 ± 5.9 | <0.001 |
| Circumferences | |||||
| waist (cm) | 93.0 ± 10.1 | <0.001 | 119.5 ± 11.9 | 107.1 ± 13.2 | <0.001 |
| hip (cm) | 104.3 ± 7.7 | <0.001 | 124.8 ± 13.0 | 115.8 ± 12.0 | <0.001 |
| WHR | 0.89 ± 0.05 | <0.001 | 0.96 ± 0.08 | 0.93 ± 0.10 | <0.005 |
| BIA | |||||
| fat mass (%) | 29.6 ± 5.7 | <0.001 | 45.8 ± 7.8 | 41.3 ± 8.3 | <0.001 |
| fat-free mass (kg) | 49.8 ± 9.7 | <0.05 | 56.2 ± 8.6 | 52.4 ± 9.3 | <0.001 |
| phase angle (°) | 6.8 ± 0.7 | 0.62 | 6.9 ± 0.7 | 6.8 ± 0.8 | 0.20 |
| Ultrasound thickness | |||||
| cutis-rectis (cm) | 3.2 ± 0.6 | <0.001 | 4.5 ± 1.2 | 4.2 ± 1.2 | <0.001 |
| rectis-aorta (cm) | 4.2 ± 1.7 | <0.001 | 8.9 ± 3.6 | 5.6 ± 2.7 | <0.001 |
| Blood pressure | |||||
| systolic (mmHg) | 119 ± 16 | 0.55 | 122 ± 18 | 115 ± 10 | <0.05 |
| diastolic (mmHg) | 81 ± 10 | 0.19 | 85 ± 11 | 78 ± 8 | <0.001 |
| Heart rate (beats/min) | 70 ± 10 | <0.005 | 81 ± 12 | 78 ± 11 | 0.18 |
| Control Group | p a | VLCKD (n = 31) | p b | ||
|---|---|---|---|---|---|
| (n = 20) | Before | After | |||
| Habitual intake of vitamin D (µg/day) | 1.12 ± 0.83 | <0.05 | 1.61 ± 0.56 | ||
| Serum concentration of: | |||||
| HbA1c (%) | 5.5 ± 0.4 | 0.07 | 6.1 ± 1.4 | 5.7 ± 0.5 | <0.05 |
| glucose (mg/dL) | 89 ± 10 | 0.09 | 108 ± 48 | 95 ± 17 | 0.07 |
| insulin (μUI/mL) | 9.1 ± 4.4 | 0.15 | 12.6 ± 10 | 7.9 ± 5.6 | <0.005 |
| HOMA-IR | 1.92 ± 0.46 | <0.001 | 3.76 ± 0.94 | 1.74 ± 0.68 | <0.001 |
| cholesterol (mg/dL) | 202 ± 51 | 0.05 | 178 ± 36 | 151 ± 25 | <0.001 |
| HDL-C (mg/dL) | 67 ± 20 | <0.05 | 55 ± 13 | 46 ± 13 | <0.05 |
| triglycerides (mg/dL) | 96 ± 51 | 0.32 | 113 ± 64 | 84 ± 35 | <0.001 |
| 25-hydroxy vitamin D (ng/mL) | 29.7 ± 6.7 | <0.005 | 21.6 ± 9.9 | 25.8 ± 10.4 | <0.001 |
| PTH (pg/mL) | 28.5 ± 8.2 | <0.001 | 41.0 ± 11.7 | 32.0 ± 13.6 | <0.01 |
| calcium (mg/dL) | 9.1 ± 0.3 | <0.01 | 9.4 ± 0.4 | 9.5 ± 0.4 | 0.06 |
| phosphorus (mg/dL) | 3.6 ± 0.5 | 0.17 | 3.4 ± 0.5 | 3.6 ± 0.4 | <0.05 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buscemi, S.; Buscemi, C.; Corleo, D.; De Pergola, G.; Caldarella, R.; Meli, F.; Randazzo, C.; Milazzo, S.; Barile, A.M.; Rosafio, G.; et al. Obesity and Circulating Levels of Vitamin D before and after Weight Loss Induced by a Very Low-Calorie Ketogenic Diet. Nutrients 2021, 13, 1829. https://doi.org/10.3390/nu13061829
Buscemi S, Buscemi C, Corleo D, De Pergola G, Caldarella R, Meli F, Randazzo C, Milazzo S, Barile AM, Rosafio G, et al. Obesity and Circulating Levels of Vitamin D before and after Weight Loss Induced by a Very Low-Calorie Ketogenic Diet. Nutrients. 2021; 13(6):1829. https://doi.org/10.3390/nu13061829
Chicago/Turabian StyleBuscemi, Silvio, Carola Buscemi, Davide Corleo, Giovanni De Pergola, Rosalia Caldarella, Francesco Meli, Cristiana Randazzo, Salvatore Milazzo, Anna Maria Barile, Giuseppe Rosafio, and et al. 2021. "Obesity and Circulating Levels of Vitamin D before and after Weight Loss Induced by a Very Low-Calorie Ketogenic Diet" Nutrients 13, no. 6: 1829. https://doi.org/10.3390/nu13061829