
Association of Preoperative Prognostic Nutritional Index and Postoperative Acute Kidney Injury in Patients with Colorectal Cancer Surgery


Abstract
:1. Introduction
2. Materials and Methods
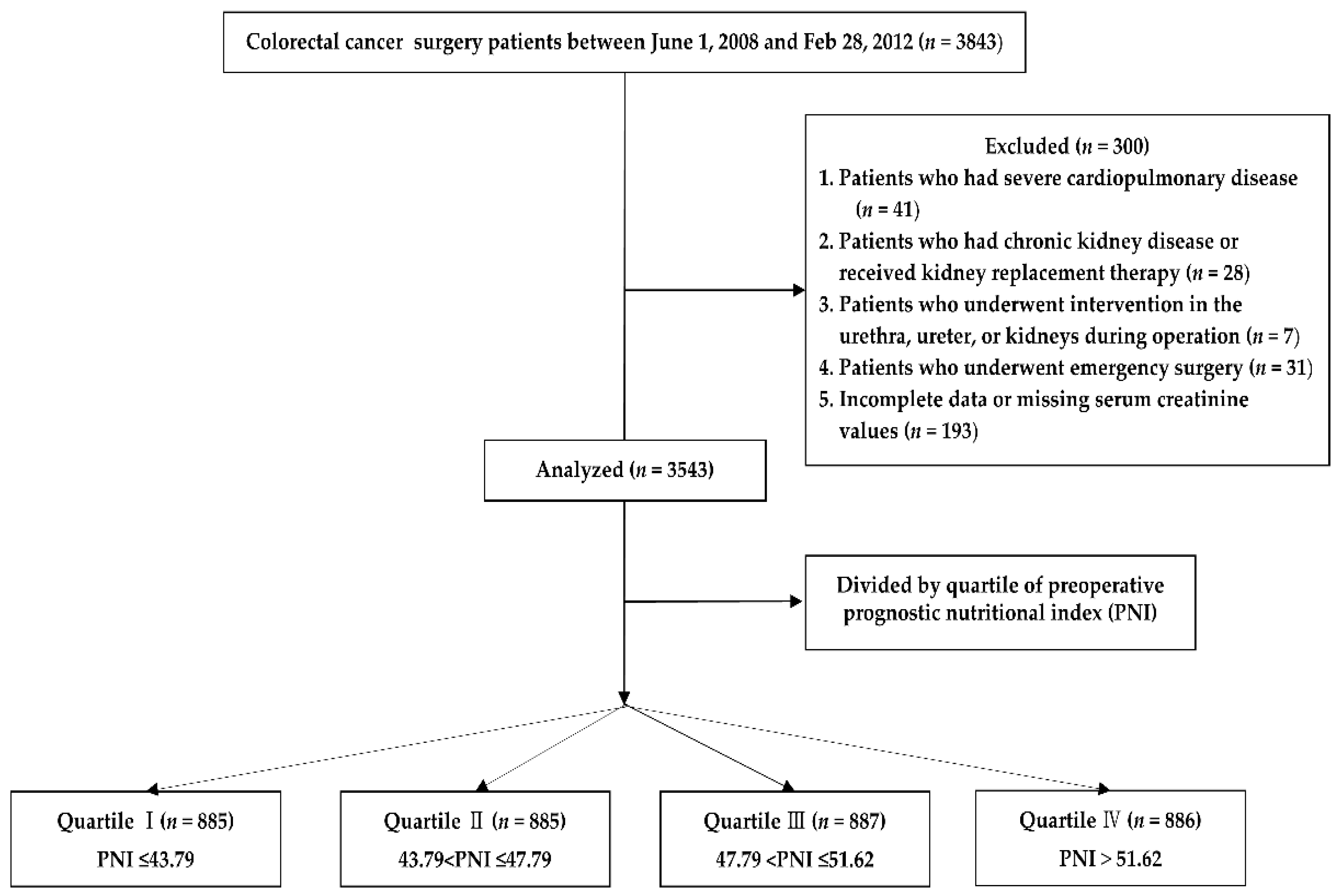
2.1. Study Design and Patient Population
2.2. General Anesthesia and Surgical Technique
2.3. Clinical Data Collection and Outcome Assessments
2.4. Primary and Secondary Outcomes
2.5. Statistical Analysis
3. Results
3.1. Primary Outcomes
3.2. Secondary Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lim, S.Y.; Lee, J.Y.; Yang, J.H.; Na, Y.J.; Kim, M.G.; Jo, S.K.; Cho, W.Y. Predictive factors of acute kidney injury in patients undergoing rectal surgery. Kidney Res. Clin. Pract. 2016, 35, 160–164. [Google Scholar] [CrossRef] [Green Version]
- Slagelse, C.; Gammelager, H.; Iversen, L.H.; Sørensen, H.T.; Christiansen, C.F. Acute kidney injury and 1-year mortality after colorectal cancer surgery: A population-based cohort study. BMJ Open 2019, 9, e024817. [Google Scholar] [CrossRef] [Green Version]
- Hsu, R.K.; Hsu, C.Y. The Role of Acute Kidney Injury in Chronic Kidney Disease. Semin. Nephrol. 2016, 36, 283–292. [Google Scholar] [CrossRef] [Green Version]
- Chertow, G.M.; Burdick, E.; Honour, M.; Bonventre, J.V.; Bates, D.W. Acute kidney injury, mortality, length of stay, and costs in hospitalized patients. J. Am. Soc. Nephrol. 2005, 16, 3365–3370. [Google Scholar] [CrossRef] [Green Version]
- Uchino, S.; Kellum, J.A.; Bellomo, R.; Doig, G.S.; Morimatsu, H.; Morgera, S.; Schetz, M.; Tan, I.; Bouman, C.; Macedo, E.; et al. Acute renal failure in critically ill patients: A multinational, multicenter study. JAMA 2005, 294, 813–818. [Google Scholar] [CrossRef] [Green Version]
- Kee, Y.K.; Kim, H.; Jhee, J.H.; Han, S.H.; Yoo, T.H.; Kang, S.W.; Park, J.T. Incidence of and risk factors for delayed acute kidney injury in patients undergoing colorectal surgery. Am. J. Surg. 2019, 218, 907–912. [Google Scholar] [CrossRef]
- Zorrilla-Vaca, A.; Mena, G.E.; Ripolles-Melchor, J.; Lorente, J.V.; Ramirez-Rodriguez, J.J.M.; Grant, M.C. Risk factors for acute kidney injury in an enhanced recovery pathway for colorectal surgery. Surg. Today 2021, 51, 537–544. [Google Scholar] [CrossRef]
- Onodera, T.; Goseki, N.; Kosaki, G. Prognostic nutritional index in gastrointestinal surgery of malnourished cancer patients. Nihon Geka Gakkai Zasshi 1984, 85, 1001–1005. [Google Scholar]
- Hong, X.; Cui, B.; Wang, M.; Yang, Z.; Wang, L.; Xu, Q. Systemic Immune-inflammation Index, Based on Platelet Counts and Neutrophil-Lymphocyte Ratio, Is Useful for Predicting Prognosis in Small Cell Lung Cancer. Tohoku J. Exp. Med. 2015, 236, 297–304. [Google Scholar] [CrossRef] [Green Version]
- Zencirkiran Agus, H.; Kahraman, S. Prognostic nutritional index predicts one-year outcome in heart failure with preserved ejection fraction. Acta Cardiol. 2020, 75, 450–455. [Google Scholar] [CrossRef]
- Wang, D.; Hu, X.; Xiao, L.; Long, G.; Yao, L.; Wang, Z.; Zhou, L. Prognostic Nutritional Index and Systemic Immune-Inflammation Index Predict the Prognosis of Patients with HCC. J. Gastrointest. Surg. 2021, 25, 421–427. [Google Scholar] [CrossRef] [Green Version]
- Salati, M.; Filippi, R.; Vivaldi, C.; Caputo, F.; Leone, F.; Salani, F.; Cerma, K.; Aglietta, M.; Fornaro, L.; Sperti, E.; et al. The prognostic nutritional index predicts survival and response to first-line chemotherapy in advanced biliary cancer. Liver Int. 2020, 40, 704–711. [Google Scholar] [CrossRef]
- Hu, Y.; Cao, Q.; Wang, H.; Yang, Y.; Xiong, Y.; Li, X.; Zhou, Q. Prognostic nutritional index predicts acute kidney injury and mortality of patients in the coronary care unit. Exp. Ther. Med. 2021, 21, 123. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.L.; Sung, S.H.; Cheng, H.M.; Hsu, P.F.; Guo, C.Y.; Yu, W.C.; Chen, C.H. Prognostic Nutritional Index and the Risk of Mortality in Patients With Acute Heart Failure. J. Am. Heart Assoc. 2017, 6, e004876. [Google Scholar] [CrossRef] [PubMed]
- Cao, X.; Zhao, G.; Yu, T.; An, Q.; Yang, H.; Xiao, G. Preoperative Prognostic Nutritional Index Correlates with Severe Complications and Poor Survival in Patients with Colorectal Cancer Undergoing Curative Laparoscopic Surgery: A Retrospective Study in a Single Chinese Institution. Nutr. Cancer 2017, 69, 454–463. [Google Scholar] [CrossRef]
- Tokunaga, R.; Sakamoto, Y.; Nakagawa, S.; Miyamoto, Y.; Yoshida, N.; Oki, E.; Watanabe, M.; Baba, H. Prognostic Nutritional Index Predicts Severe Complications, Recurrence, and Poor Prognosis in Patients With Colorectal Cancer Undergoing Primary Tumor Resection. Dis. Colon Rectum 2015, 58, 1048–1057. [Google Scholar] [CrossRef]
- Shibutani, M.; Maeda, K.; Nagahara, H.; Ohtani, H.; Iseki, Y.; Ikeya, T.; Sugano, K.; Hirakawa, K. The prognostic significance of the postoperative prognostic nutritional index in patients with colorectal cancer. BMC Cancer 2015, 15, 521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, B.K.; Park, J.W.; Han, E.C.; Ryoo, S.B.; Han, S.W.; Kim, T.Y.; Chie, E.K.; Jeong, S.Y.; Park, K.J. Systemic inflammatory markers as prognostic factors in stage IIA colorectal cancer. J. Surg. Oncol. 2016, 114, 216–221. [Google Scholar] [CrossRef]
- Kang, S.B.; Park, J.W.; Jeong, S.Y.; Nam, B.H.; Choi, H.S.; Kim, D.W.; Lim, S.B.; Lee, T.G.; Kim, D.Y.; Kim, J.S.; et al. Open versus laparoscopic surgery for mid or low rectal cancer after neoadjuvant chemoradiotherapy (corean trial): Short-term outcomes of an open-label randomised controlled trial. Lancet Oncol. 2010, 11, 637–645. [Google Scholar] [CrossRef]
- Levey, A.S.; Eckardt, K.U.; Tsukamoto, Y.; Levin, A.; Coresh, J.; Rossert, J.; De Zeeuw, D.; Hostetter, T.H.; Lameire, N.; Eknoyan, G. Definition and classification of chronic kidney disease: A position statement from Kidney Disease: Improving Global Outcomes (KDIGO). Kidney Int. 2005, 67, 2089–2100. [Google Scholar] [CrossRef] [Green Version]
- Chen, Q.J.; Qu, H.J.; Li, D.Z.; Li, X.M.; Zhu, J.J.; Xiang, Y.; Li, L.; Ma, Y.T.; Yang, Y.N. Prognostic nutritional index predicts clinical outcome in patients with acute ST-segment elevation myocardial infarction undergoing primary percutaneous coronary intervention. Sci. Rep. 2017, 7, 3285. [Google Scholar] [CrossRef] [Green Version]
- Kanda, M.; Fujii, T.; Kodera, Y.; Nagai, S.; Takeda, S.; Nakao, A. Nutritional predictors of postoperative outcome in pancreatic cancer. Br. J. Surg. 2011, 98, 268–274. [Google Scholar] [PubMed]
- Mohri, Y.; Inoue, Y.; Tanaka, K.; Hiro, J.; Uchida, K.; Kusunoki, M. Prognostic nutritional index predicts postoperative outcome in colorectal cancer. World J. Surg. 2013, 37, 2688–2692. [Google Scholar]
- Nakatani, M.; Migita, K.; Matsumoto, S.; Wakatsuki, K.; Ito, M.; Nakade, H.; Kunishige, T.; Kitano, M.; Kanehiro, H. Prognostic significance of the prognostic nutritional index in esophageal cancer patients undergoing neoadjuvant chemotherapy. Dis. Esophagus 2017, 30, 1–7. [Google Scholar]
- Yu, J.; Hong, B.; Park, J.Y.; Hwang, J.H.; Kim, Y.K. Impact of Prognostic Nutritional Index on Postoperative Pulmonary Complications in Radical Cystectomy: A Propensity Score-Matched Analysis. Ann. Surg. Oncol. 2020, 28, 1859–1869. [Google Scholar]
- Min, J.Y.; Woo, A.; Chae, M.S.; Hong, S.H.; Park, C.S.; Choi, J.H.; Chung, H.S. Predictive Impact of Modified-Prognostic Nutritional Index for Acute Kidney Injury within 1-week after Living Donor Liver Transplantation. Int. J. Med. Sci. 2020, 17, 82. [Google Scholar]
- Dolapoglu, A.; Avci, E.; Kiris, T.; Bugra, O. The predictive value of the prognostic nutritional index for postoperative acute kidney injury in patients undergoing on-pump coronary bypass surgery. J. Cardiothorac. Surg. 2019, 14, 74. [Google Scholar] [PubMed]
- Neugarten, J.; Golestaneh, L.; Kolhe, N.V. Sex differences in acute kidney injury requiring dialysis. BMC Nephrol. 2018, 19, 131. [Google Scholar]
- Viñas, J.L.; Porter, C.J.; Douvris, A.; Spence, M.; Gutsol, A.; Zimpelmann, J.A.; Tailor, K.; Campbell, P.A.; Burns, K.D. Sex diversity in proximal tubule and endothelial gene expression in mice with ischemic acute kidney injury. Clin. Sci. 2020, 134, 1887–1909. [Google Scholar]
- James, M.T.; Grams, M.E.; Woodward, M.; Elley, C.R.; Green, J.A.; Wheeler, D.C.; de Jong, P.; Gansevoort, R.T.; Levey, A.S.; Warnock, D.G.; et al. A Meta-analysis of the Association of Estimated GFR, Albuminuria, Diabetes Mellitus, and Hypertension with Acute Kidney Injury. Am. J. Kidney Dis. 2015, 66, 602–612. [Google Scholar]
- Patschan, D.; Müller, G.A. Acute Kidney Injury in Diabetes Mellitus. Int. J. Nephrol. 2016, 2016, 6232909. [Google Scholar] [CrossRef] [Green Version]
- Argalious, M.Y.; Makarova, N.; Leone, A.; Cywinski, J.; Farag, E. Association of Body Mass Index and Postoperative Acute Kidney Injury in Patients Undergoing Laparoscopic Surgery. Ochsner. J. 2017, 17, 224–232. [Google Scholar]
- Bi, J.B.; Zhang, J.; Ren, Y.F.; Du, Z.Q.; Wu, Z.; Lv, Y.; Wu, R.Q. Neutrophil-to-lymphocyte ratio predicts acute kidney injury occurrence after gastrointestinal and hepatobiliary surgery. World J. Gastrointest. Surg. 2020, 12, 326–335. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.Y.; Kong, Y.G.; Park, J.H.; Kim, Y.K. Acute kidney injury after burn surgery: Preoperative neutrophil/lymphocyte ratio as a predictive factor. Acta Anaesthesiol. Scand. 2019, 63, 240–247. [Google Scholar] [CrossRef]
- Limaye, K.; Yang, J.D.; Hinduja, A. Role of admission serum albumin levels in patients with intracerebral hemorrhage. Acta Neurol. Belg. 2016, 116, 27–30. [Google Scholar] [CrossRef]
- Kaufmann, M.A.; Castelli, I.; Pargger, H.; Drop, L.J. Nitric oxide dose-response study in the isolated perfused rat kidney after inhibition of endothelium-derived relaxing factor synthesis: The role of serum albumin. J. Pharmacol. Exp. Ther. 1995, 273, 855–862. [Google Scholar] [PubMed]
- Lee, E.H.; Baek, S.H.; Chin, J.H.; Choi, D.K.; Son, H.J.; Kim, W.J.; Hahm, K.D.; Sim, J.Y.; Choi, I.C. Preoperative hypoalbuminemia is a major risk factor for acute kidney injury following off-pump coronary artery bypass surgery. Intensive Care Med. 2012, 38, 1478–1486. [Google Scholar] [CrossRef]
- Li, N.; Qiao, H.; Guo, J.F.; Yang, H.Y.; Li, X.Y.; Li, S.L.; Wang, D.X.; Yang, L. Preoperative hypoalbuminemia was associated with acute kidney injury in high-risk patients following non-cardiac surgery: A retrospective cohort study. BMC Anesthesiol. 2019, 19, 171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gamba, G.; Contreras, A.M.; Cortés, J.; Nares, F.; Santiago, Y.; Espinosa, A.; Bobadilla, J.; Jiménez Sánchez, G.; López, G.; Valadez, A.; et al. Hypoalbuminemia as a risk factor for amikacin nephrotoxicity. Rev. Investig. Clin. 1990, 42, 204–209. [Google Scholar]
- Dixon, R.; Brunskill, N.J. Activation of mitogenic pathways by albumin in kidney proximal tubule epithelial cells: Implications for the pathophysiology of proteinuric states. J. Am. Soc. Nephrol. 1999, 10, 1487–1497. [Google Scholar] [CrossRef]
- Weller, S.; Varrier, M.; Ostermann, M. Lymphocyte Function in Human Acute Kidney Injury. Nephron 2017, 137, 287–293. [Google Scholar] [CrossRef]
- Aghdaii, N.; Ferasatkish, R.; Mohammadzadeh Jouryabi, A.; Hamidi, S.H. Significance of preoperative total lymphocyte count as a prognostic criterion in adult cardiac surgery. Anesth. Pain Med. 2014, 4, e20331. [Google Scholar] [CrossRef] [Green Version]
- Martina, M.N.; Noel, S.; Bandapalle, S.; Hamad, A.R.; Rabb, H. T lymphocytes and acute kidney injury: Update. Nephron Clin. Pract. 2014, 127, 51–55. [Google Scholar]
- Fan, X.; Chen, G.; Li, Y.; Shi, Z.; He, L.; Zhou, D.; Lin, H. The Preoperative Prognostic Nutritional Index in Hepatocellular Carcinoma after Curative Hepatectomy: A Retrospective Cohort Study and Meta-Analysis. J. Investig. Surg. 2019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiao, F.K.; Wang, L.; Zhang, W.C.; Wang, L.D.; Zhao, L.S. Preoperative Prognostic Nutritional Index is a Significant Predictor of Survival in Esophageal Squamous Cell Carcinoma Patients. Nutr. Cancer 2020, 1–6. [Google Scholar]



{kind=link}
{kind=link}
| Prognostic Nutritional Index | |||||
|---|---|---|---|---|---|
| Quartile Ⅰ (n = 885) | Quartile Ⅱ (n = 885) | Quartile Ⅲ (n = 887) | Quartile Ⅳ (n = 886) | SMD | |
| Preoperative variables | |||||
| Age; year | 62.60 ± 11.83 | 60.73 ± 10.64 | 59.08 ± 10.32 | 56.69 ± 10.92 | 0.293 |
| Sex; male | 512 (57.9) | 528 (59.7) | 551 (62.1) | 585 (66.0) | 0.093 |
| Weight; kg | 59.56 ± 9.84 | 62.09 ± 9.87 | 64.43 ± 10.33 | 65.36 ± 10.84 | 0.322 |
| Height; cm | 1.61 ± 0.08 | 1.62 ± 0.09 | 1.63 ± 0.08 | 1.63 ± 0.09 | 0.143 |
| BMI; kg m−2 | 22.90 ± 3.17 | 23.71 ± 3.01 | 24.25 ± 2.92 | 24.42 ± 3.06 | 0.276 |
| DM | 136 (15.4) | 119 (13.4) | 134 (15.1) | 134 (15.1) | 0.027 |
| HTN | 288 (32.5) | 270 (30.5) | 296 (33.4) | 320 (36.1) | 0.063 |
| CVA | 26 (2.9) | 23 (2.6) | 11 (1.2) | 11 (1.2) | 0.076 |
| Smoking | 513 (58.0) | 504 (56.9) | 481 (54.2) | 439 (49.5) | 0.144 |
| ASA status | 0.197 | ||||
| ASA 1 | 148 (16.7) | 210 (23.7) | 227 (25.6) | 255 (28.8) | |
| ASA 2 | 694 (78.4) | 660 (74.6) | 650 (73.3) | 624 (70.4) | |
| ASA 3 | 43 (4.9) | 15 (1.7) | 10 (1.1) | 7 (0.8) | |
| Laboratory variables | |||||
| White blood cell | 5.85 ± 2.32 | 5.69 ± 1.85 | 6.03 ± 1.69 | 6.95 ± 1.72 | 0.357 |
| Hemoglobin | 11.20 ± 1.80 | 12.21 ± 1.75 | 12.63 ± 1.77 | 13.12 ± 1.64 | 0.591 |
| Albumin; g dL−1 | 3.31 ± 0.40 | 3.80 ± 0.26 | 4.02 ± 0.25 | 4.24 ± 0.26 | 1.626 |
| Creatinine; mg dL−1 | 0.74 ± 0.18 | 0.79 ± 0.18 | 0.81 ± 0.18 | 0.83 ± 0.17 | 0.284 |
| eGFR; mL.min−1.1.73 m−2 | 75.52 ± 13.63 | 75.96 ± 13.18 | 74.56 ± 12.98 | 74.47 ± 12.95 | 0.069 |
| NLR | 3.59 ± 3.21 | 2.42 ± 1.37 | 1.95 ± 0.91 | 1.59 ± 0.69 | 0.607 |
| PLR | 226.50 ± 124.76 | 165.69 ± 62.47 | 135.97 ± 47.84 | 107.72 ± 36.53 | 0.487 |
| RDW | 15.20 ± 3.37 | 14.19 ± 2.63 | 13.55 ± 2.13 | 13.15 ± 1.79 | 0.436 |
| PNI | 39.37 ± 3.88 | 45.87 ± 1.17 | 49.69 ± 1.10 | 54.79 ± 2.73 | 3.421 |
| Intraoperative variables | |||||
| Tumor location | 0.025 | ||||
| colon | 624 (70.51) | 640 (72.32) | 633 (71.36) | 623 (70.32) | |
| rectum | 261 (29.49) | 245 (27.68) | 254 (28.64) | 263 (29.68) | |
| Tumor invasion | 0.288 | ||||
| Tis, T1, T2 | 129 (14.58) | 181 (20.45) | 233 (26.27) | 329 (37.13) | |
| T3, T4 | 756 (85.42) | 704 (79.55) | 654 (73.73) | 557 (62.87) | |
| Lymph node invasion | 0.291 | ||||
| N0 | 310 (35.03) | 408 (46.10) | 481 (54.23) | 538 (60.72) | |
| N1, N2 | 575 (64.97) | 477 (53.90) | 406 (45.77) | 348 (39.28) | |
| Distant metastasis | 0.098 | ||||
| M0 | 765 (86.44) | 794 (89.72) | 799 (90.08) | 818 (92.33) | |
| M1 | 120 (13.56) | 91 (10.28) | 88 (9.92) | 68 (7.67) | |
| Operation time; min | 180.05 ± 66.45 | 169.48 ± 57.67 | 167.83 ± 60.13 | 166.86 ± 58.35 | 0.111 |
| Lowest MBP; mmHg | 69.33 ± 9.05 | 70.91 ± 8.47 | 71.65 ± 9.02 | 72.27 ± 8.80 | 0.180 |
| Laparoscopic surgery | 159 (18.0) | 217 (24.5) | 260 (29.3) | 338 (38.1) | 0.247 |
| Total fluids; mL kg−1 | 30.93 ± 15.72 | 27.41 ± 12.51 | 26.04 ± 10.36 | 25.74 ± 9.86 | 0.218 |
| Crystalloid; mL kg−1 h−1 | 24.45 ± 14.05 | 21.44 ± 11.57 | 19.85 ± 9.55 | 19.69 ± 9.03 | 0.226 |
| Colloid; mL kg−1 h−1 | 6.42 ± 5.33 | 5.96 ± 4.81 | 6.19 ± 4.25 | 6.05 ± 4.25 | 0.054 |
| Colloid use | 616 (69.6) | 604 (68.2) | 671 (75.6) | 660 (74.5) | 0.101 |
| RBC transfusion | 51 (5.8) | 20 (2.3) | 18 (2.0) | 10 (1.1) | 0.134 |
| Unit of infused RBC | 0.11 ± 0.53 | 0.04 ± 0.33 | 0.05 ± 0.38 | 0.03 ± 0.36 | 0.094 |
| Urine output; mL kg−1 h−1 | 1.88 ± 1.74 | 1.88 ± 1.79 | 1.84 ± 1.44 | 2.00 ± 1.59 | 0.052 |
| Diuretics | 8 (0.9) | 2 (0.2) | 4 (0.5) | 4 (0.5) | 0.046 |
| Surgical outcomes | |||||
| AKI | 119 (13.4) | 81 (9.2) | 83 (9.4) | 78 (8.8) | 0.075 |
| Hospital days | 9.45 ± 9.28 | 8.01 ± 5.51 | 7.69 ± 4.37 | 7.41 ± 5.69 | 0.154 |
| ICU admission | 54 (6.1) | 25 (2.8) | 22 (2.5) | 18 (2.0) | 0.117 |
| ICU stay (≥2 days) | 20 (2.3) | 4 (0.5) | 6 (0.7) | 6 (0.7) | 0.153 |
| Postoperative complication | 10 (1.1) | 9 (1.0) | 8 (0.9) | 6 (0.7) | |
| Cardiac | 1 (0.1) | 2 (0.2) | 1 (0.1) | 2 (0.2) | |
| Pulmonary | 4 (0.5) | 6 (0.7) | 5 (0.6) | 2 (0.2) | |
| Bleeding | 5 (0.6) | 1 (0.1) | 2 (0.2) | 2 (0.2) | |
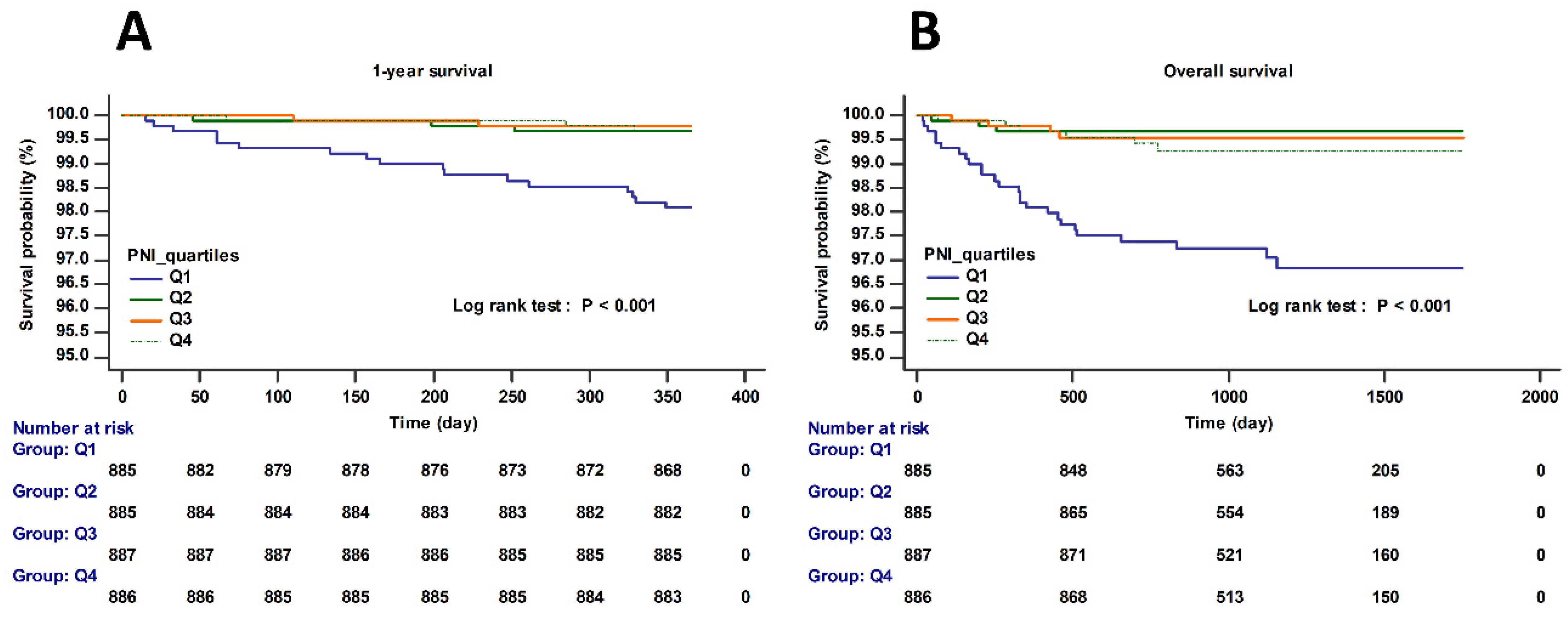
| 1-year mortality | 17 (1.9) | 3 (0.3) | 2 (0.2) | 3 (0.3) | 0.085 |
| Overall mortality | 26 (2.9) | 3 (0.3) | 4 (0.5) | 6 (0.7) | 0.111 |
| Univariate | Multivariate | |||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| PNI | 0.97 | 0.96–0.99 | 0.003 | 0.96 | 0.93–0.99 | 0.003 |
| Age | 1.01 | 1.00–1.02 | 0.018 | 1.00 | 0.99–1.02 | 0.465 |
| Sex (male) | 1.65 | 1.30–1.21 | <0.001 | 1.60 | 1.19–2.14 | <0.001 |
| BMI | 1.04 | 1.00–1.07 | 0.042 | 1.06 | 1.02–1.11 | 0.003 |
| DM | 1.83 | 1.40–2.38 | <0.001 | 1.48 | 1.10–1.98 | 0.009 |
| HTN | 1.50 | 1.20–1.87 | <0.001 | 1.46 | 1.12–1.91 | 0.006 |
| CVA | 1.29 | 0.63–2.61 | 0.485 | |||
| Smoking | 1.43 | 1.13–1.80 | 0.003 | 1.09 | 0.81–1.45 | 0.573 |
| ASA | 0.010 | 0.130 | ||||
| ASA status 1 | 1.00 | 1.00 | ||||
| ASA status 2 | 1.20 | 0.91–1.56 | 0.195 | 0.80 | 0.58–1.11 | 0.189 |
| ASA status 3 | 2.59 | 1.40–4.78 | 0.002 | 1.36 | 0.68–2.73 | 0.388 |
| Tumor location | ||||||
| colon | 1.00 | 1.00 | ||||
| rectum | 0.90 | 0.70–1.14 | 0.376 | |||
| Tumor invasion | ||||||
| Tis, T1, T2 | 1.00 | 1.00 | ||||
| T3, T4 | 1.21 | 0.93–1.58 | 0.153 | 1.12 | 0.81–1.54 | 0.497 |
| Lymph node invasion | ||||||
| N0 | 1.00 | 1.00 | ||||
| N1, N2 | 1.17 | 0.94–1.46 | 0.152 | 1.02 | 0.79–1.33 | 0.862 |
| Distant metastasis | ||||||
| M0 | 1.00 | 1.00 | ||||
| M1 | 1.28 | 0.91–1.79 | 0.157 | 1.09 | 0.74–1.58 | 0.672 |
| Operation time; min | 1.00 | 1.00–1.00 | 0.333 | 1.00 | 1.00–1.00 | 0.798 |
| Laparoscopic surgery | 0.98 | 0.77–1.25 | 0.878 | 1.05 | 0.80–1.39 | 0.712 |
| Lowest MBP; mmHg | 1.00 | 0.99–1.02 | 0.625 | 1.00 | 0.99–1.02 | 0.496 |
| Total fluids; mL kg−1 | 1.00 | 0.99–1.01 | 0.565 | 1.00 | 0.99–1.02 | 0.748 |
| Crystalloid; mL kg−1 | 1.00 | 1.00–1.01 | 0.289 | |||
| Colloid; mL kg−1 | 0.99 | 0.96–1.01 | 0.244 | |||
| Synthetic Colloid use | 0.91 | 0.72–1.16 | 0.464 | 0.98 | 0.75–1.27 | 0.862 |
| Urine output; mL kg−1 h−1 | 1.03 | 0.97–1.10 | 0.372 | 1.06 | 0.99–1.13 | 0.124 |
| Diuretics | 1.77 | 0.51–6.14 | 0.369 | 1.57 | 0.35–5.19 | 0.497 |
| RBC transfusion | 1.35 | 0.74–2.44 | 0.327 | 1.04 | 0.51–2.11 | 0.922 |
| White blood cell | 1.04 | 0.98–1.09 | 0.179 | 1.10 | 1.02–1.19 | 0.016 |
| Hemoglobin | 0.98 | 0.93–1.04 | 0.560 | 0.96 | 0.89–1.04 | 0.316 |
| Albumin; g dL−1 | 0.55 | 0.44–0.69 | <0.001 | |||
| Creatinine | 0.38 | 0.21–0.71 | 0.002 | 0.05 | 0.02–0.13 | <0.001 |
| eGFR | 1.00 | 0.99–1.01 | 0.608 | |||
| NLR | 0.98 | 0.93–1.05 | 0.594 | 0.90 | 0.78–1.03 | 0.118 |
| PLR | 1.00 | 0.99–1.01 | 0.302 | 0.98 | 0.94–1.02 | 0.337 |
| RDW | 1.01 | 0.97–1.05 | 0.755 | 0.99 | 0.94–1.03 | 0.579 |
| Univariate | Multivariate | |||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| PNI | 0.87 | 0.82–0.92 | <0.001 | 0.92 | 0.86–0.98 | 0.011 |
| Age | 1.05 | 1.01–1.10 | 0.008 | 1.04 | 1.00–1.09 | 0.054 |
| Sex (male) | 1.12 | 0.49–2.54 | 0.790 | 1.50 | 0.41–5.50 | 0.545 |
| BMI | 0.90 | 0.79–1.02 | 0.111 | 1.02 | 0.89–1.18 | 0.760 |
| DM | 3.91 | 1.75–8.74 | <0.001 | 3.91 | 1.60–9.60 | 0.003 |
| HTN | 1.87 | 0.85–4.11 | 0.119 | 1.33 | 0.49–3.62 | 0.577 |
| CVA | 2.05 | 0.27–15.38 | 0.484 | |||
| Smoking | 2.96 | 1.3–6.72 | 0.009 | 4.12 | 1.28–13.31 | 0.018 |
| ASA | <0.001 | 0.130 | ||||
| ASA status 1 | 1.00 | 1.00 | ||||
| ASA status 2 | 1.82 | 0.53–6.21 | 0.342 | 0.56 | 0.14–2.28 | 0.418 |
| ASA status 3 | 19.93 | 4.67–85.13 | <0.001 | 2.93 | 0.52–16.41 | 0.221 |
| Tumor location | ||||||
| colon | 1.00 | 1.00 | ||||
| rectum | 1.39 | 0.62–3.13 | 0.430 | |||
| Tumor invasion | ||||||
| Tis, T1, T2 | 1.00 | 1.00 | ||||
| T3, T4 | 7.49 | 1.02–54.90 | 0.049 | 3.58 | 0.38–33.67 | 0.265 |
| Lymph node invasion | ||||||
| N0 | 1.00 | 1.00 | ||||
| N1, N2 | 2.89 | 1.15–7.24 | 0.025 | 1.81 | 0.69–4.78 | 0.230 |
| Distant metastasis | ||||||
| M0 | 1.00 | 1.00 | ||||
| M1 | 2.94 | 1.17–7.38 | 0.022 | 1.67 | 0.56–4.99 | 0.358 |
| Operation time; min | 1.00 | 1.00–1.01 | 0.022 | 1.01 | 1.00–1.01 | 0.116 |
| Laparoscopic surgery | 0.11 | 0.01–0.81 | 0.030 | 0.15 | 0.02–1.16 | 0.070 |
| Lowest MBP; mmHg | 0.95 | 0.90–0.99 | 0.027 | 1.00 | 0.94–1.05 | 0.853 |
| Total fluids; mL kg−1 | 1.02 | 1.00–1.04 | 0.030 | 1.27 | 0.90–1.80 | 0.178 |
| Crystalloid; mL kg−1 | 1.03 | 1.01–1.05 | 0.005 | 0.80 | 0.56–1.13 | 0.208 |
| Colloid; mL kg−1 | 0.94 | 0.86–1.03 | 0.167 | 0.72 | 0.49–1.04 | 0.080 |
| Synthetic Colloid use | 0.42 | 0.19–0.92 | 0.030 | 0.40 | 0.16–1.02 | 0.054 |
| Urine output; mL kg−1 h−1 | 0.85 | 0.63–1.16 | 0.305 | |||
| Diuretics | * | 0.992 | ||||
| RBC transfusion | 3.07 | 0.71–13.19 | 0.132 | 0.59 | 0.09–3.93 | 0.593 |
| White blood cell | 1.13 | 0.96–1.34 | 0.142 | 1.06 | 0.87–1.30 | 0.547 |
| Hemoglobin | 0.7 | 0.58–0.85 | <0.001 | 0.92 | 0.70–1.20 | 0.534 |
| Albumin; g dL−1 | 0.19 | 0.10–0.36 | <0.001 | |||
| Creatinine | 0.11 | 0.01–1.05 | 0.05503 | 0.15 | 0.01–3.27 | 0.228 |
| eGFR | 1.00 | 0.97–1.03 | 0.930 | |||
| NLR | 1.10 | 1.02–1.18 | 0.010 | 0.98 | 0.73–1.31 | 0.888 |
| PLR | 1.02 | 1.00–1.05 | 0.003 | 1.00 | 0.92–1.09 | 0.952 |
| RDW | 1.19 | 1.09–1.31 | <0.001 | 1.08 | 0.95–1.22 | 0.256 |
| Univariate | Multivariate * | |||
|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| AKI | ||||
| Quartile Ⅰ | 1.55 (1.23–1.96) | <0.001 | 1.52 (1.18–1.95) | 0.001 |
| Quartile Ⅱ, Ⅲ, Ⅳ | 1.00 | 1.00 | ||
| Postoperative complication | ||||
| Quartile Ⅰ | 1.51 (0.73–3.12) | 0.269 | 0.86 (0.38–1.94) | 0.721 |
| Quartile Ⅱ, Ⅲ, Ⅳ | 1.00 | 1.00 | ||
| Hospital days (≥14 days) | ||||
| Quartile Ⅰ | 2.86 (2.14–3.82) | <0.001 | 2.16 (1.55–2.99) | <0.001 |
| Quartile Ⅱ, Ⅲ, Ⅳ | 1.00 | 1.00 | ||
| ICU admission | ||||
| Quartile Ⅰ | 2.59 (1.79–3.75) | <0.001 | 1.26 (0.79–2.01) | 0.327 |
| Quartile Ⅱ, Ⅲ, Ⅳ | 1.00 | 1.00 | ||
| ICU stay (≥2 days) | ||||
| Quartile Ⅰ | 3.82 (1.97–7.40) | <0.001 | 2.14 (1.01–4.53) | 0.046 |
| Quartile Ⅱ, Ⅲ, Ⅳ | 1.00 | 1.00 | ||
| 1-year mortality | ||||
| Quartile Ⅰ | 6.49 (2.79–15.09) | <0.001 | 3.83 (1.55–9.49) | 0.004 |
| Quartile Ⅱ, Ⅲ, Ⅳ | 1.00 | 1.00 | ||
| Overall mortality | ||||
| Quartile Ⅰ | 6.16 (3.15–12.04) | <0.001 | 3.81 (1.86–7.79) | <0.001 |
| Quartile Ⅱ, Ⅲ, Ⅳ | 1.00 | 1.00 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sim, J.-H.; Bang, J.-Y.; Kim, S.-H.; Kang, S.-J.; Song, J.-G. Association of Preoperative Prognostic Nutritional Index and Postoperative Acute Kidney Injury in Patients with Colorectal Cancer Surgery. Nutrients 2021, 13, 1604. https://doi.org/10.3390/nu13051604
Sim J-H, Bang J-Y, Kim S-H, Kang S-J, Song J-G. Association of Preoperative Prognostic Nutritional Index and Postoperative Acute Kidney Injury in Patients with Colorectal Cancer Surgery. Nutrients. 2021; 13(5):1604. https://doi.org/10.3390/nu13051604
Chicago/Turabian StyleSim, Ji-Hoon, Ji-Yeon Bang, Sung-Hoon Kim, Sa-Jin Kang, and Jun-Gol Song. 2021. "Association of Preoperative Prognostic Nutritional Index and Postoperative Acute Kidney Injury in Patients with Colorectal Cancer Surgery" Nutrients 13, no. 5: 1604. https://doi.org/10.3390/nu13051604