Contribution of Major Groups of Food Products to the Daily Intake of Selected Elements—Results from Analytical Determinations Supported by Chemometric Analysis




Abstract
:1. Introduction
2. Materials and Methods
2.1. Chemicals
2.2. Sampling
2.3. Digestion of Samples
2.4. Analytical Determination of Elements by Flame Atomic Absorption Spectrometry (F-AAS) and Inductively Coupled Plasma Optical Emission Spectrometry (ICP-OES)
2.5. Statistical Analysis
3. Results
3.1. Distribution of Food Groups
3.2. Dietary Intake of Macroelements with Major Food Groups
3.3. Dietary Intake of Trace Elements with Major Food Groups
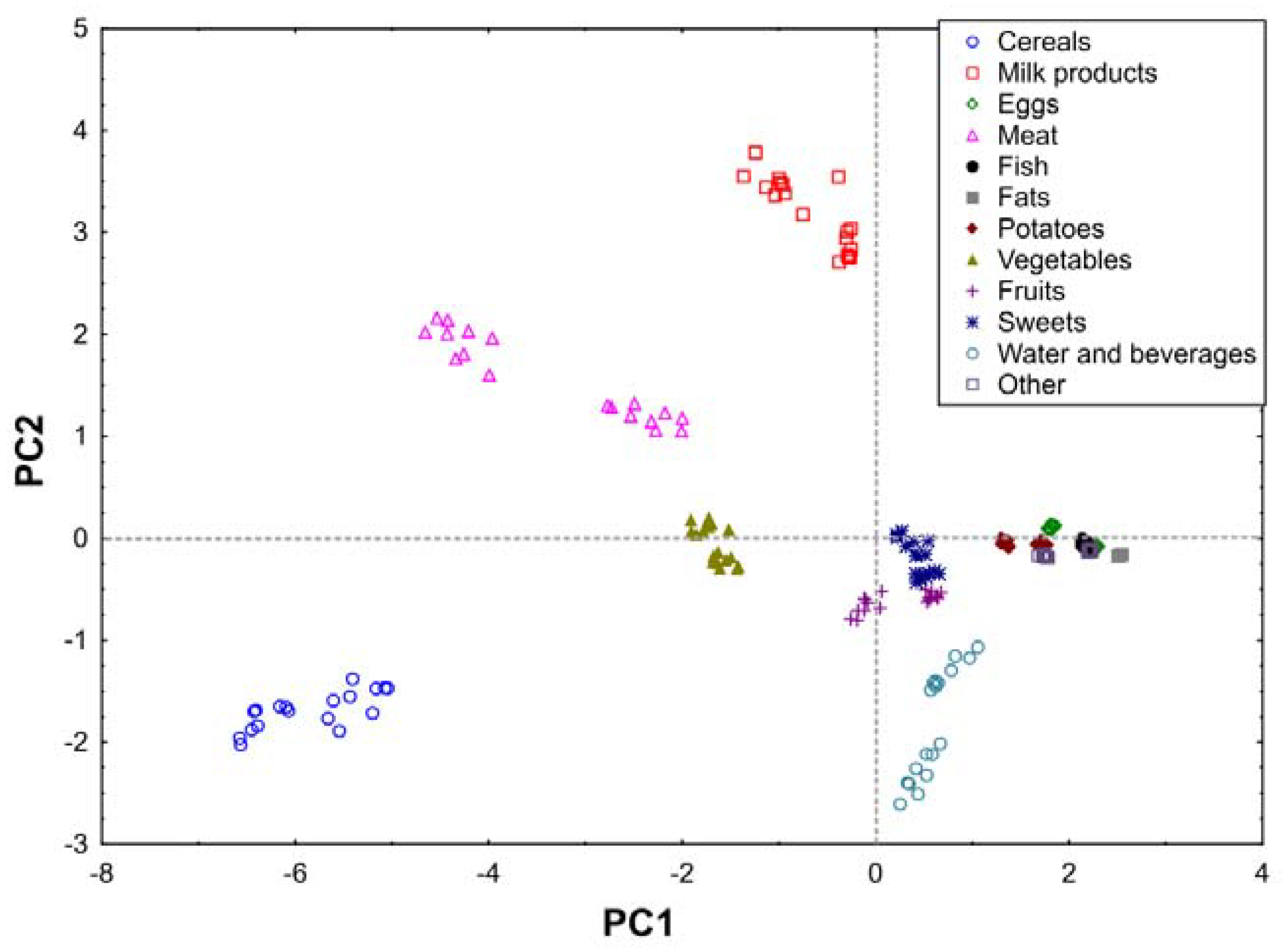
3.4. Principal Component Analysis (PCA) Analysis
4. Discussion
4.1. Dietary Intake of Macroelements with Major Food Groups
4.2. Dietary Intake of Trace Elements with Major Food Groups
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Barbaresko, J.; Koch, M.; Schulze, M.B.; Nöthlings, U. Dietary pattern analysis and biomarkers of low-grade inflammation: A systematic literature review. Nutr. Rev. 2013, 71, 511–527. [Google Scholar] [CrossRef] [PubMed]
- Bocio, A.; Nadal, M.; Domingo, J.L. Human Exposure to Metals Through the Diet in Tarragona, Spain: Temporal Trend. Biol. Trace Elem. Res. 2005, 104, 193–202. [Google Scholar] [CrossRef]
- Koch, W.; Karim, R.; Marzec, Z.; Miyataka, H.; Himeno, S.; Asakawa, Y. Dietary intake of metals by the young adult population of Eastern Poland: Results from a market basket study. J. Trace Elem. Med. Biol. 2016, 35, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Edelstein, M.; Ben-Hur, M. Heavy metals and metalloids: Sources, risks and strategies to reduce their accumulation in horticultural crops. Sci. Hortic. 2018, 234, 431–444. [Google Scholar] [CrossRef]
- Vardhan, K.H.; Kumar, P.S.; Panda, R.C. A review on heavy metal pollution, toxicity and remedial measures: Current trends and future perspectives. J. Mol. Liq. 2019, 290, 111197. [Google Scholar] [CrossRef]
- Lee, H.-S.; Cho, Y.-H.; Park, S.-O.; Kye, S.-H.; Kim, B.-H.; Hahm, T.-S.; Kim, M.; Lee, J.O.; Kim, C.-I. Dietary exposure of the Korean population to arsenic, cadmium, lead and mercury. J. Food Compos. Anal. 2006, 19, S31–S37. [Google Scholar] [CrossRef]
- Turconi, G.; Minoia, C.; Ronchi, A.; Roggi, C. Dietary exposure estimates of twenty-one trace elements from a Total Diet Study carried out in Pavia, Northern Italy. Br. J. Nutr. 2008, 101, 1200–1208. [Google Scholar] [CrossRef] [Green Version]
- Domingo, J.L.; Perelló, G.; Bordonaba, J.G. Dietary Intake of Metals by the Population of Tarragona County (Catalonia, Spain): Results from a Duplicate Diet Study. Biol. Trace Elem. Res. 2012, 146, 420–425. [Google Scholar] [CrossRef] [PubMed]
- Nasreddine, L.; Nashalian, O.; Naja, F.; Itani, L.; Parent-Massin, D.; Nabhani-Zeidan, M.; Hwalla, N. Dietary exposure to essential and toxic trace elements from a Total diet study in an adult Lebanese urban population. Food Chem. Toxicol. 2010, 48, 1262–1269. [Google Scholar] [CrossRef]
- Arnich, N.; Sirot, V.; Rivière, G.; Jean, J.; Noël, L.; Guérin, T.; Leblanc, J.-C. Dietary exposure to trace elements and health risk assessment in the 2nd French Total Diet Study. Food Chem. Toxicol. 2012, 50, 2432–2449. [Google Scholar] [CrossRef] [PubMed]
- Coelho, S.; Pastorinho, M.R.; Itai, T.; Isobe, T.; Kunisue, T.; Nogueira, A.; Tanabe, S.; Sousa, A.C. Lead in duplicate diet samples from an academic community. Sci. Total Environ. 2016, 573, 603–607. [Google Scholar] [CrossRef]
- Sousa, A.G.; Da Costa, T.H.M. Assessment of Nutrient and Food Group Intakes across Sex, Physical Activity, and Body Mass Index in an Urban Brazilian Population. Nutrients 2018, 10, 1714. [Google Scholar] [CrossRef] [Green Version]
- Dodd, K.W.; Guenther, P.M.; Freedman, L.S.; Subar, A.F.; Kipnis, V.; Midthune, D.; Tooze, J.A.; Krebs-Smith, S.M. Statistical Methods for Estimating Usual Intake of Nutrients and Foods: A Review of the Theory. J. Am. Diet. Assoc. 2006, 106, 1640–1650. [Google Scholar] [CrossRef]
- Thompson, F.E.; Kirkpatrick, S.I.; Subar, A.F.; Reedy, J.; Schap, T.E.; Wilson, M.M.; Krebs-Smith, S.M. The National Cancer Institute’s Dietary Assessment Primer: A Resource for Diet Research. J. Acad. Nutr. Diet. 2015, 115, 1986–1995. [Google Scholar] [CrossRef] [Green Version]
- Nadolna, I.; Kunachowicz, H.; Iwanow, K. Dishes, Composition and Nutritional Value; National Food and Nutrition Institute: Warsaw, Poland, 1994. [Google Scholar]
- Marzec, Z.; Koch, W.; Marzec, A.; Żukiewicz-Sobczak, W. Dietary exposure to cadmium, lead and nickel among students from the south-east region of Poland. Ann. Agric. Environ. Med. 2014, 21, 825–828. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koch, W.; Kukula-Koch, W.; Marzec, Z.; Kasperek, E.; Wyszogrodzka-Koma, L.; Szwerc, W.; Asakawa, Y. Application of Chromatographic and Spectroscopic Methods towards the Quality Assessment of Ginger (Zingiber officinale) Rhizomes from Ecological Plantations. Int. J. Mol. Sci. 2017, 18, 452. [Google Scholar] [CrossRef] [Green Version]
- Jarosz, M. Human Nutrition Recommendations for Polish Population; IZZ: Warsaw, Poland, 2017. (In Polish) [Google Scholar]
- Food and Nutrition Board. Dietary Reference Intakes: Applications in Dietary Assessment; National Academy Press: Washington, DC, USA, 2001. [Google Scholar]
- WHO. Trace Elements in Human Nutrition and Health; WHO: Geneva, Switzerland, 1996. [Google Scholar]
- Lombardi-Boccia, G.; Aguzzi, A.; Cappelloni, M.; Di Lullo, G.; Lucarini, M. Total-diet study: Dietary intakes of macro elements and trace elements in Italy. Br. J. Nutr. 2003, 90, 1117–1121. [Google Scholar] [CrossRef]
- Raghunath, R.; Tripathi, R.; Suseela, B.; Bhalke, S.; Shukla, V.; Puranik, V. Dietary intake of metals by Mumbai adult population. Sci. Total Environ. 2006, 356, 62–68. [Google Scholar] [CrossRef]
- Appel, L.J.; Foti, K. Sources of Dietary Sodium. Circulation 2017, 135, 1784–1787. [Google Scholar] [CrossRef] [Green Version]
- Marzec, Z.; Koch, W.; Marzec, A. Evaluation of selected nutrients with student daily diets in Lublin. Bromat. Chem. Toksykol. 2009, 42, 604–609. [Google Scholar]
- Myszkowska-Ryciak, J.; Harton, A. Eating Healthy, Growing Healthy: Outcome Evaluation of the Nutrition Education Program Optimizing the Nutritional Value of Preschool Menus, Poland. Nutrients 2019, 11, 2438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gowrishankar, M.; Blair, B.; Rieder, M.J. Dietary intake of sodium by children: Why it matters. Paediatr. Child Health 2020, 25, 47–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prentice, A.M.; Jebb, S.A. Fast foods, energy density and obesity: A possible mechanistic link. Obes. Rev. 2003, 4, 187–194. [Google Scholar] [CrossRef]
- Monteiro, C.A.; Levy, R.B.; Claro, R.M.; De Castro, I.R.R.; Cannon, G. Increasing consumption of ultra-processed foods and likely impact on human health: Evidence from Brazil. Public Health Nutr. 2010, 14, 5–13. [Google Scholar] [CrossRef]
- Martins, A.P.B.; Levy, R.B.; Claro, R.M.; Moubarac, J.C.; Monteiro, C.A. Participacao crescente de produtos ultraprocessados na dieta brasileira (1987–2009). Rev. Saúde Pública 2013, 47, 656–665. [Google Scholar] [CrossRef]
- Harnack, L.J.; Cogswell, M.E.; Shikany, J.M.; Gardner, C.D.; Gillespie, C.; Loria, C.M.; Zhou, X.; Yuan, K.; Steffen, L.M. Sources of Sodium in US Adults from 3 Geographic Regions. Circulation 2017, 135, 1775–1783. [Google Scholar] [CrossRef]
- Mattes, R.D.; Donnelly, D. Relative contributions of dietary sodium sources. J. Am. Coll. Nutr. 1991, 10, 383–393. [Google Scholar] [CrossRef] [PubMed]
- Anderson, C.A.M.; Appel, L.J.; Okuda, N.; Brown, I.J.; Chan, Q.; Zhao, L.; Ueshima, H.; Kesteloot, H.; Miura, K.; Curb, J.D.; et al. Dietary Sources of Sodium in China, Japan, the United Kingdom, and the United States, Women and Men Aged 40 to 59 Years: The INTERMAP Study. J. Am. Diet. Assoc. 2010, 110, 736–745. [Google Scholar] [CrossRef] [Green Version]
- Bailey, R.L.; Parker, E.A.; Rhodes, D.G.; Goldman, J.D.; Clemens, J.C.; Moshfegh, A.J.; Thuppal, S.V.; Weaver, C.M. Estimating Sodium and Potassium Intakes and Their Ratio in the American Diet: Data from the 2011–2012 NHANES. J. Nutr. 2015, 146, 745–750. [Google Scholar] [CrossRef]
- Welch, A.; Fransen, H.; Jenab, M.; Boutron-Ruault, M.C.; Tumino, R.; Agnoli, C.; Ericson, U.; Johansson, I.; Ferrari, P.; Engeset, D.; et al. Variation in intakes of calcium, phosphorus, magnesium, iron and potassium in 10 countries in the European Prospective Investigation into Cancer and Nutrition study. Eur. J. Clin. Nutr. 2009, 63, S101–S121. [Google Scholar] [CrossRef] [Green Version]
- Cogswell, M.E.; Zhang, Z.; Carriquiry, A.L.; Gunn, J.P.; Kuklina, E.V.; Saydah, S.H.; Yang, Q.; Moshfegh, A.J. Sodium and potassium intakes among US adults: NHANES 2003–2008. Am. J. Clin. Nutr. 2012, 96, 647–657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Centre for Chronic Disease Prevention and Health Promotion. Highlights: Sodium and potassium intakes among us infants and preschool children, 2003–2010. Am. J. Clin. Nutr. 2013, 98, 1113–1122. [Google Scholar] [CrossRef]
- Zamora, D.; Gordon-Larsen, P.; He, K.; Jacobs, D.R.; Shikany, J.M.; Popkin, B.M. Are the 2005 Dietary Guidelines for Americans Associated with Reduced Risk of Type 2 Diabetes and Cardiometabolic Risk Factors? Diabetes Care 2011, 34, 1183–1185. [Google Scholar] [CrossRef] [Green Version]
- Public Health England. Food Standards Agency. National Diet and Nutrition Survey: Results from Years 1, 2, 3 and 4 (Combined) of the Rolling Programme (2008/2009–2011/2012); Public Health England: London, UK, 2014.
- Yang, Q.; Liu, T.; Kuklina, E.V.; Flanders, W.D.; Hong, Y.; Gillespie, C.; Chang, M.-H.; Gwinn, M.; Dowling, N.; Khoury, M.J.; et al. Sodium and Potassium Intake and Mortality Among US Adults. Arch. Intern. Med. 2011, 171, 1183–1191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bailey, R.L.; Fulgoni, V.L.; Keast, D.R.; Dwyer, J.T. Dietary supplement use is associated with higher intakes of minerals from food sources. Am. J. Clin. Nutr. 2011, 94, 1376–1381. [Google Scholar] [CrossRef] [Green Version]
- Jodral-Segado, A.M.; Navarro-Alarcón, M.; De La Serrana, H.L.-G.; López-Martínez, M.C. Magnesium and calcium contents in foods from SE Spain: Influencing factors and estimation of daily dietary intakes. Sci. Total Environ. 2003, 312, 47–58. [Google Scholar] [CrossRef]
- Becker, W.; Kumpulainen, J. Contents of essential and toxic mineral elements in Swedish market-basket diets in 1987. Br. J. Nutr. 1991, 66, 151–160. [Google Scholar] [CrossRef]
- Ford, E.S.; Li, C.; McGuire, L.C.; Mokdad, A.H.; Liu, S. Intake of Dietary Magnesium and the Prevalence of the Metabolic Syndrome among U.S. Adults*. Obesity 2007, 15, 1139–1146. [Google Scholar] [CrossRef] [PubMed]
- Ettinger, B.; Pak, C.Y.; Citron, J.T.; Thomas, C.; Adams-Huet, B.; Vangessel, A. Potassium-magnesium citrate is an effective prophylaxis against recurrent calcium oxalate nephrolithiasis. J. Urol. 1997, 158, 2069–2073. [Google Scholar] [CrossRef]
- Schwalfenberg, G.K.; Genuis, S.J. The Importance of Magnesium in Clinical Healthcare. Science 2017, 2017, 1–14. [Google Scholar] [CrossRef]
- Institute of Medicine (IOM). Food and Nutrition Board. Dietary Reference Intakes: Calcium, Phosphorus, Magnesium, Vitamin D and Fluoride; National Academy Press: Washington, DC, USA, 1997. [Google Scholar]
- Rude, R.K. Magnesium. In Modern Nutrition in Health and Disease, 11th ed.; Ross, A.C., Caballero, B., Cousins, R.J., Tucker, K.L., Ziegler, T.R., Eds.; Lippincott Williams & Wilkins: Baltimore, MA, USA, 2012; pp. 159–175. [Google Scholar]
- Azoulay, A.; Garzon, P.; Eisenberg, M.J. Comparison of the mineral content of tap water and bottled waters. J. Gen. Intern. Med. 2001, 16, 168–175. [Google Scholar] [CrossRef]
- Fenech, M.; Baghurst, P.; Luderer, W.; Turner, J.; Record, S.; Ceppi, M.; Bonassi, S. Low intake of calcium, folate, nicotinic acid, vitamin E, retinol, β-carotene and high intake of pantothenic acid, biotin and riboflavin are significantly associated with increased genome instability—results from a dietary intake and micronucleus index survey in South Australia. Carcinogenesis 2005, 26, 991–999. [Google Scholar] [CrossRef] [Green Version]
- Henderson, L.; Irving, K.; Gregory, J. The National Diet and Nutrition Survey: Adults Aged 19–64 Years. Vitamin and Mineral Intake and Urinary Analytes; The Stationery Office: London, UK, 2003; Volume 3. [Google Scholar]
- Cormick, G.; Belizán, J.M. Calcium Intake and Health. Nutrients 2019, 11, 1606. [Google Scholar] [CrossRef] [Green Version]
- Silanikove, N.; Leitner, G.; Merin, U. The Interrelationships between Lactose Intolerance and the Modern Dairy Industry: Global Perspectives in Evolutional and Historical Backgrounds. Nutrients 2015, 7, 7312–7331. [Google Scholar] [CrossRef] [Green Version]
- Huang, F.; Wang, Z.; Zhang, J.; Du, W.; Su, C.; Jiang, H.; Jia, X.; Ouyang, Y.; Wang, Y.; Li, L.; et al. Dietary calcium intake and food sources among Chinese adults in CNTCS. PLoS ONE 2018, 13, e0205045. [Google Scholar] [CrossRef]
- Willemse, J.P.M.M.; Meertens, L.J.E.; Scheepers, H.C.J.; Achten, N.M.J.; Eussen, S.J.; Van Dongen, M.C.; Smits, L.J.M. Calcium intake from diet and supplement use during early pregnancy: The Expect study I. Eur. J. Nutr. 2019, 59, 167–174. [Google Scholar] [CrossRef] [Green Version]
- Catling, L.A.; Abubakar, I.; Lake, I.R.; Swift, L.; Hunter, P. A systematic review of analytical observational studies investigating the association between cardiovascular disease and drinking water hardness. J. Water Health 2008, 6, 433–442. [Google Scholar] [CrossRef] [Green Version]
- Leoni, V.; Fabiani, L.; Ticchiarelli, L. Water Hardness and Cardiovascular Mortality Rate in Abruzzo, Italy. Arch. Environ. Health Int. J. 1985, 40, 274–278. [Google Scholar] [CrossRef]
- Institute of Medicine (US) Panel on Micronutrients. Dietary Reference Intakes for Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc; National Academy Press: Washington, DC, USA, 2001. [Google Scholar]
- Cuadrado, C.; Kumpulainen, J.; Moreiras, O. Contaminants and nutrients in total diets in Spain. Eur. J. Clin. Nutr. 1995, 49, 767–778. [Google Scholar]
- Ysart, G.; Miller, P.; Crews, H.; Robb, P.; Baxter, M.; De L’Argy, C.; Lofthouse, S.; Sargent, C.; Harrison, N. Dietary exposure estimates of 30 elements from the UK Total Diet Study. Food Addit. Contam. 1999, 16, 391–403. [Google Scholar] [CrossRef]
- Chen, J.; Gao, J. The Chinese Total Diet Study in 1990. Part II. Nutrients. J. AOAC Int. 1993, 76, 1206–1213. [Google Scholar] [CrossRef]
- Iyengar, G.V.; Kawamura, H.; Parr, R.M.; Miah, F.K.; Wang, J.-X.; Dang, H.S.; Djojosubroto, H.; Cho, S.-Y.; Akher, P.; Natera, E.S.; et al. Dietary Intake of Essential Minor and Trace Elements from Asian Diets. Food Nutr. Bull. 2002, 23, 124–128. [Google Scholar] [CrossRef] [PubMed]
- Products, N.A.A.; Nda, E.P.O.D. Scientific Opinion on Dietary Reference Values for copper. EFSA J. 2015, 13, 4253. [Google Scholar] [CrossRef]
- De Romaña, D.L.; Olivares, M.; Uauy, R.; Araya, M. Risks and benefits of copper in light of new insights of copper homeostasis. J. Trace Elem. Med. Biol. 2011, 25, 3–13. [Google Scholar] [CrossRef]
- EFSA. NDA Panel (EFSA Panel on Dietetic Products, Nutrition and Allergies), 2015. Scientific opinion on dietary reference values of zinc. EFSA J. 2014, 12, 3844. [Google Scholar]
- Gibson, R.S.; Bailey, K.B.; Gibbs, M.; Ferguson, E.L. A Review of Phytate, Iron, Zinc, and Calcium Concentrations in Plant-Based Complementary Foods Used in Low-Income Countries and Implications for Bioavailability. Food Nutr. Bull. 2010, 31, S134–S146. [Google Scholar] [CrossRef]
- Hunt, J.R.; Beiseigel, J.M.; Johnson, L.K. Adaptation in human zinc absorption as influenced by dietary zinc and bioavailability. Am. J. Clin. Nutr. 2008, 87, 1336–1345. [Google Scholar] [CrossRef] [Green Version]
- King, J.C.; Brown, K.H.; Gibson, R.S.; Krebs, N.F.; Lowe, N.M.; Siekmann, J.H.; Raiten, D.J. Biomarkers of Nutrition for Development (BOND)—Zinc Review. J. Nutr. 2015, 146, 858S–885S. [Google Scholar] [CrossRef] [Green Version]
- Egan, S.K.; Tao, S.S.-H.; Pennington, J.A.T.; Bolger, P.M. US Food and Drug Administration’s Total Diet Study: Intake of nutritional and toxic elements, 1991–1996. Food Addit. Contam. 2002, 19, 103–125. [Google Scholar] [CrossRef]
- EFSA. NDA Panel (EFSA Panel on Dietetic Products, Nutrition and Allergies). Scientific Opinion on Dietary Reference Values for manganese. EFSA J. 2013, 11, 3419. [Google Scholar] [CrossRef] [Green Version]
- ANSES. (Agence nationale de sécurité sanitaire de l’alimentation, de l’environnement, et du travail). Total Diet Study 2 (TDS 2), Report 1, Inorganic Contaminants, Minerals, Persistent Organic Pollutants, Mycotoxins and Phytoestrogens; ANSES: Paris, France, 2011.
- Rose, M.; Baxter, M.; Brereton, N.; Baskaran, C. Dietary exposure to metals and other elements in the 2006 UK Total Diet Study and some trends over the last 30 years. Food Addit. Contam. Part A 2010, 27, 1380–1404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brzezicha-Cirocka, J.; Grembecka, M.; Szefer, P. Monitoring of essential and heavy metals in green tea from different geographical origins. Environ. Monit. Assess. 2016, 188, 183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peng, C.-Y.; Zhu, X.-H.; Hou, R.; Ge, G.-F.; Hua, R.; Wan, X.; Cai, H.-M. Aluminum and Heavy Metal Accumulation in Tea Leaves: An Interplay of Environmental and Plant Factors and an Assessment of Exposure Risks to Consumers. J. Food Sci. 2018, 83, 1165–1172. [Google Scholar] [CrossRef]
- Koch, W.; Kukula-Koch, W.; Komsta, Ł.; Marzec, Z.; Szwerc, W.; Głowniak, K. Green Tea Quality Evaluation Based on Its Catechins and Metals Composition in Combination with Chemometric Analysis. Molecules 2018, 23, 1689. [Google Scholar] [CrossRef] [Green Version]
- Rusinek-Prystupa, E.; Marzec, Z.; Sembratowicz, I.; Samolińska, W.; Kiczorowska, B.; Kwiecień, M. Content of Selected Minerals and Active Ingredients in Teas Containing Yerba Mate and Rooibos. Biol. Trace Elem. Res. 2015, 172, 266–275. [Google Scholar] [CrossRef]
- Linder, M.C. Mobilization of stored iron in mammals: A Review. Nutrients 2013, 5, 4022–4050. [Google Scholar] [CrossRef] [Green Version]
- Looker, A.C.; Dallman, P.R.; Carroll, M.D.; Gunter, E.W.; Johnson, C.L. Prevalence of iron deficiency in the United States. JAMA 1997, 277, 973–976. [Google Scholar] [CrossRef]
- International Nutritional Anemia Consultative Group, WHO and UNICEF. Guidelines for the Use of Iron Supplements to Prevent and Treat Iron Deficiency Anemia; International Life Sciences Institute: Washington, DC, USA, 1998. [Google Scholar]
- Broniecka, A.; Wyka, J.; Bronkowska, M.; Piotrowska, E.; Biernat, J. Assessment of intake of iron and nutrients that affect bioavailability of daily food rations of girls. Ann. Agric. Environ. Med. 2014, 21, 327–330. [Google Scholar] [CrossRef] [Green Version]
- Grajeta, H. Wpływ składników pokarmowych na wchłanianie żelaza (The effect of foodstuffs on the absorption of iron). Bromat. Chem. Toksykol. 2006, 39, 111–119. (In Polish) [Google Scholar]
- Ziemlański, Ś. Human Nutrition Recommendations. Physiological Basis; PZWL: Warsaw, Poland, 2001. (In Polish) [Google Scholar]
- Guthrie, B.; Picciano, M.F. Macronutrient minerals. In Human Nutrition; Mosby Year Book: St. Louis, MO, USA, 1995; pp. 334–351. [Google Scholar]
- Vincent, J.B. Elucidating a biological role for chromium at a molecular level. Accounts Chem. Res. 2000, 33, 503–510. [Google Scholar] [CrossRef]
- Di Bona, K.R.; Love, S.; Rhodes, N.R.; McAdory, D.; Sinha, S.H.; Kern, N.; Kent, J.; Strickland, J.; Wilson, A.; Beaird, J.; et al. Chromium is not an essential trace element for mammals: Effects of a “low-chromium” diet. J. Biol. Inorg. Chem. 2010, 16, 381–390. [Google Scholar] [CrossRef]
- Vincent, J.B. New evidence against chromium as an essential trace element. J. Nutr. 2017, 147, 2212–2219. [Google Scholar] [CrossRef] [Green Version]
- Roussel, A.-M.; Andriollo-Sanchez, M.; Ferry, M.; Bryden, N.A.; Anderson, R.A. Food chromium content, dietary chromium intake and related biological variables in French free-living elderly. Br. J. Nutr. 2007, 98, 326–331. [Google Scholar] [CrossRef] [Green Version]
- Noel, L.; Leblanc, J.-C.; Guérin, T. Determination of several elements in duplicate meals from catering establishments using closed vessel microwave digestion with inductively coupled plasma mass spectrometry detection: Estimation of daily dietary intake. Food Addit. Contam. 2003, 20, 44–56. [Google Scholar] [CrossRef]
- Marzec, Z. Alimentary chromium, nickel, and selenium intake of adults in Poland estimated by analysis and calculations using the duplicate portion technique. Food/Nahrung 2004, 48, 47–52. [Google Scholar] [CrossRef]
- Ysart, G.; Miller, P.; Croasdale, M.; Crews, H.; Robb, P.; Baxter, M.; De L’Argy, C.; Harrison, N. 1997 UK Total Diet Study dietary exposures to aluminium, arsenic, cadmium, chromium, copper, lead, mercury, nickel, selenium, tin and zinc. Food Addit. Contam. 2000, 17, 775–786. [Google Scholar] [CrossRef]
- Puccinelli, M.; Malorgio, F.; Pezzarossa, B. Selenium enrichment of horticultural crops. Molecules 2017, 22, 933. [Google Scholar] [CrossRef]
- Qin, H.-B.; Zhu, J.-M.; Liang, L.; Wang, M.-S.; Su, H. The bioavailability of selenium and risk assessment for human selenium poisoning in high-Se areas, China. Environ. Int. 2013, 52, 66–74. [Google Scholar] [CrossRef] [PubMed]
- Gao, J.; Liu, Y.; Huang, Y.; Lin, Z.-Q.; Bañuelos, G.S.; Lam, M.H.-W.; Yin, X. Daily selenium intake in a moderate selenium deficiency area of Suzhou, China. Food Chem. 2011, 126, 1088–1093. [Google Scholar] [CrossRef]
- Stoffaneller, R.; Morse, N.L. A Review of dietary seleniumintake and selenium status in Europe and the Middle East. Nutrients 2015, 7, 1494–1537. [Google Scholar] [CrossRef]
- Van Dokkum, W. The intake of selected minerals and trace elements in European countries. Nutr. Res. Rev. 1995, 8, 271–302. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Parameter | Women (N = 274) | Men (N = 305) |
|---|---|---|
| Age (years) | 24 ± 4 | 24 ± 4 |
| Physical activity | Moderate | Moderate |
| Height (m) | 1.58 ± 0.17 | 1.74 ± 0.19 |
| Weight (kg) | 58 ± 6.4 | 74 ± 8.5 |
| BMI (kg/m2) | 23.2 ± 1.90 | 24.4 ± 2.75 |
| Parameter | Element | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Na | K | Mg | Ca | Cu | Zn | Mn | Fe | Cr | Se | |
| Reference value (mg/kg) | 6300 | 10,260 | 752.3 | 3522 | 2.94 | 24.0 | 9.02 | 22.9 | 0.15 | 0.20 |
| Determined value (mg/kg) | 6178 | 10,722 | 754.2 | 3452 | 2.97 | 23.1 | 8.80 | 20.7 | 0.17 | 0.21 |
| SD | 249.4 | 884 | 39.3 | 202.6 | 0.15 | 1.97 | 0.36 | 1.76 | 0.017 | 0.017 |
| RSD (%) | 4.04 | 8.24 | 5.21 | 5.87 | 5.05 | 8.53 | 4.09 | 8.50 | 10.0 | 8.10 |
| Recovery (%) | 98.1 | 104.5 | 100.3 | 98.0 | 101.0 | 96.3 | 97.6 | 90.4 | 113.3 | 105 |
| LOD (µg/kg) | 82.0 | 65.0 | 37.0 | 182 | 182 | 40.0 | 171.0 | 161.0 | 1.2 | 2.2 |
| LOQ (µg/kg) | 295 | 279.5 | 135.7 | 600.6 | 637.5 | 148.4 | 607.3 | 536.3 | 4.3 | 7.5 |
| Food Group | Women | Men | ||||
|---|---|---|---|---|---|---|
| Amount (g) | Energy (kcal) | Composition (%) | Amount (g) | Energy (kcal) | Composition (%) | |
| Cereals | 224.1 ± 20.8 | 653.6 ± 79.2 | baking 51.5 cereal flakes 14.7 grits 12.5 rice 11.5 pasta 9.80 | 284.8 ± 25.3 | 770.1 ± 84.2 | baking 66.6 rice 12.9 pasta 9.40 cereal flakes 6.35 grits 4.75 |
| Milk and diary | 276.9 ± 25.7 | 303.9 ± 35.4 | milk 45.1 cheese 30.4 yogurts 23.2 sour cream 1.3 | 232.3 ± 22.4 | 327.1 ± 29.8 | cheese 47.0 milk 31.2 yogurts 18.9 sour cream 2.90 |
| Eggs | 18.2 ± 2.11 | 21.4 ± 1.92 | scrambled eggs 48.1 boiled eggs 38.7 omelette 13.2 | 45.5 ± 5.17 | 53.1 ± 7.12 | scrambled eggs 60.9 boiled eggs 33.2 omelette 5.90 |
| Meat and meat products | 191.7 ± 20.8 | 406.5 ± 47.2 | pork 39.0 poultry 37.6 beef 23.4 | 283.5 ± 31.4 | 621.5 ± 56.4 | pork 42.0 beef 30.4 poultry 27.6 |
| Fish | 17.5 ± 2.14 | 21.4 ± 2.72 | tuna 44.2 cod 38.6 salmon 12.0 herring 4.0 pike 1.2 | 20.0 ± 3.18 | 36.7 ± 4.12 | mackerel 47.0 salmon 35.3 tuna 8.90 sardine 8.80 |
| Fats and oils | 14.0 ± 1.34 | 116.7 ± 11.4 | butter 35.2 rapeseed oil 32.5 sunflower oil 15.7 olive oil 11.1 margarine 3.29 linseed oil 2.21 | 25.1 ± 2.91 | 209.7 ± 18.4 | rapeseed oil 38.2 butter 32.6 sunflower oil 20,2 lard 6.90 olive oil 2.10 |
| Potatoes | 50.1 ± 6.55 | 38.6 ± 4.22 | 82.5 ± 9.52 | 63.5 ± 7.48 | ||
| Vegetables | 384.1 ± 45.2 | 90.9 ± 12.5 | tomatoes 30.1 pepper 19.4 carrot 10.9 cabbage 9.95 beetroot 7.85 cauliflower 6.82 broccoli 6.64 lettuce 2.17 celery 1.16 others 5 | 343.8 ± 38.4 | 72.6 ± 9.15 | tomatoes 32.2 carrot 22.3 pepper 15.6 cucumber 11.2 onion 4.05 cabbage 3.58 broccoli 2.50 pumpkin 1.30 leek 1.27 lettuce 1.05 others 5 |
| Fruits | 227.2 ± 35.6 | 140.5 ± 18.8 | apples 34.2 bananas 33.6 oranges 7.65 mandarins 5.92 pears 4.14 peaches 3.42 raspberries 3.05 watermelons 1.86 kiwi 1.48 raisins 1.32 nectarines 1.25 others 1.44 | 192.2 ± 26.2 | 114.4 ± 17.8 | apples 40.5 bananas 28.9 oranges 10.1 mandarins 5.92 pears 5.56 grapefruit 3.10 grapes 1.55 red currants 1.85 dried dates 1.36 others 1.16 |
| Sweets and sugars | 62.4 ± 10.2 | 236.9 ± 31.8 | cakes and cookies 53.4 bars 14.3 sugar 13.4 chocolate 12.5 honey 1.70 others 4.70 | 69.1 ± 12.4 | 251 ± 40.8 | cakes and cookies 60.5 sugar 23.4 bars 10.6 chocolate 4.80 honey 0.70 |
| Water and beverages | 638.7 ± 75.4 | 33.8 ± 4.52 | black tea (infusion) 56.8 soups (only water) 18.8 fruit juices 11.1 coffee (infusion) 11.0 sweet beverages 2.30 | 713.1 ± 100.2 | 52.3 ± 6.18 | black tea (infusion) 53.4 coffee (infusion) 17.0 soups (only water) 13.2 fruit juices 11.8 sweet beverages 3.27 bear 1.33 |
| Other products | 34.5 ± 5.52 | 139 ± 15.8 | jams (no added sugar) 32.4 sauces 22.8 hooves 16.9 seeds (pumpkin/sunflower) 10.6 nuts 5.50 snacks 4.24 pudding 2.56 almonds 2.11 tomato concentrate 1.94 cocoa 0.95 | 18.4 ± 3.11 | 98.7 ± 10.2 | sauces 56.3 jams (no added sugar) 22.0 pancakes 13.4 almonds 2.78 nuts 2.25 pudding 1.68 cocoa 1.10 others 0.49 |
| Total | 2139 ± 264 | 2203 ± 331 | 2310 ± 351 | 2671 ± 355 | ||
| Food Group | Na (mg) | K (mg) | Mg (mg) | Ca (mg) | ||||
|---|---|---|---|---|---|---|---|---|
| Women | Men | Women | Men | Women | Men | Women | Men | |
| Cereals | 588 ± 31.3 g 550–642 | 634 ± 32.6 f 590–674 | 290 ± 17.3 e 261–311 | 253 ± 12.4 d 236–270 | 63.9 ± 4.93 g 58.3–71.7 | 66.8 ± 4.78 g 58.4–73.2 | 11.4 ± 1.67 a 9.22–14.2 | 13.8 ± 0.52 cd 13.0–14.7 |
| Milk and diary | 219 ± 10.5 e 205–234 | 324 ± 20.2 d 293–356 | 289 ± 19.1 e 262–316 | 201 ± 20.3 c 170–230 | 22.5 ± 1.32 e 20.1–24.5 | 20.9 ± 2.97 d 17.3–26.5 | 284 ± 34.0 c 247–359 | 322 ± 16.1 f 301–354 |
| Eggs | 18.0 ± 1.56 abc 15.1–20.3 | 37.6 ± 1.73 ab 34.9–39.5 | 17.8 ± 2.01 a 15.6–21.5 | 46.0 ± 4.99 b 37.4–52.3 | 1.23 ± 0.18 b 1.00–1.55 | 3.26 ± 0.60 a 2.32–3.96 | 3.02 ± 0.46 a 2.55–3.92 | 21.0 ± 2.87 d 18.1–26.6 |
| Meat and meat products | 671 ± 66.7 h 582–760 | 1012 ± 69.6 g 912–1125 | 460 ± 60.0 f 356–523 | 672 ± 39.8 h 612–719 | 37.9 ± 6.03 d 29.5–46.2 | 36.5 ± 3.73 f 31.1–42.2 | 9.62 ± 0.49 a 9.14–10.2 | 7.50 ± 0.49 abc 6.76–8.06 |
| Fish | 39.6 ± 1.55 bc 37.2–42.5 | 53.1 ± 3.93 b 46.2–57.4 | 26.0 ± 1.69 ab 24.1–28.9 | 32.5 ± 3.25 ab 28.1–36.8 | 2.37 ± 0.21 bc 1.98–2.68 | 3.21 ± 0.30 a 2.82–3.72 | 0.67 ± 0.09 a 0.55–0.82 | 0.49 ± 0.04 a 0.42–0.53 |
| Fats and oils | 0.08 ± 0.01 a 0.06–0.10 | 0.05 ± 0.01 a 0.04–0.07 | 0.32 ± 0.03 a 0.28–0.35 | 1.50 ± 0.21 a 1.14–1.78 | 0.03 ± 0.01 b 0.02–0.05 | 0.08 ± 0.01 a 0.06–0.09 | 0.15 ± 0.02 a 0.11–0.17 | 0.90 ± 0.04 a 0.84–1.00 |
| Potatoes | 104 ± 10.1 d 88.3–118 | 162 ± 9.48 c 152–178 | 123 ± 12.0 d 105–141 | 195 ± 19.0 c 160–219 | 6.30 ± 0.35 ac 5.72–6.79 | 10.0 ± 0.37 e 9.55–10.7 | 1.02 ± 0.11 a 0.82–1.18 | 1.48 ± 0.1 ab 1.34–1.63 |
| Vegetables | 360 ± 22.4 f 320–390 | 372 ± 25.0 e 333–415 | 650 ± 36.4 g 608–705 | 456 ± 44.1 g 410–528 | 34.2 ± 3.45 d 28.5–40.1 | 21.5 ± 2.10 d 18.8–24.1 | 43.1 ± 2.56 b 38.7–47.1 | 31.0 ± 1.40 e 28.1–32.9 |
| Fruits | 3.70 ± 0.26 ab 3.29–4.12 | 1.08 ± 0.19 a 0.84–1.34 | 465 ± 35.8 f 406–512 | 273 ± 17.8 d 250–303 | 30.0 ± 2.39 f 26.2–33.5 | 17.2 ± 1.22 c 15.6–18.9 | 5.79 ± 0.57 a 5.12–6.84 | 6.36 ± 0.64 abc 5.34–6.98 |
| Sweets and sugars | 48.1 ± 4.91 c 40.7–56.1 | 55.9 ± 7.91 b 42.5–67.6 | 68.7 ± 5.28 c 58.2–75.6 | 84.8 ± 10.8 e 70.3–105 | 8.18 ± 0.19 a 7.87–8.55 | 14.7 ± 0.73 bc 13.6–15.7 | 9.87 ± 1.38 a 8.31–12.6 | 8.43 ± 0.40 bc 7.65–8.86 |
| Water and beverages | 4.16 ± 0.14 ab 3.94–4.29 | 4.52 ± 0.35 a 3.91–5.03 | 113 ± 10.3 d 101–132 | 159 ± 21.3 f 132–198 | 9.88 ± 1.34 a 8.11–12.3 | 13.8 ± 1.00 b 12.6–15.9 | 8.90 ± 0.30 a 8.39–9.25 | 13.1 ± 1.32 c 11.7–15.1 |
| Other products | 47.6 ± 4.81 c 41.2–55.7 | 21.6 ± 2.24 ab 17.9–24.6 | 60.5 ± 3.15 bc 56.0–65.6 | 21.6 ± 2.08 ab 18.1–24.6 | 7.89 ± 0.85 a 6.92–9.34 | 2.49 ± 0.27 a 2.05–2.82 | 7.89 ± 0.37 a 7.46–8.56 | 2.49 ± 0.19 ab 2.28–2.80 |
| Total | 2103 ± 94.0 | 2679 ± 87.0 | 2564 ± 99.0 | 2396 ± 89.0 | 224 ± 3.00 | 210 ± 7.00 | 385 ± 36.0 | 429 ± 18.0 |
| EAR/AI [22] | 1500 | 1500 | 3500 | 3500 | 255 | 330 | 800 | 800 |
| Food Group | Cu (mg) | Zn (mg) | Mn (mg) | Fe (mg) | Cr (µg) | Se (µg) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Women | Men | Women | Men | Women | Men | Women | Men | Women | Men | Women | Men | |
| Cereals | 0.331 ± 0.035 h 0.291–0.376 | 0.377 ± 0.028 h 0.331–0.412 | 2.15 ± 0.21 g 1.85–2.46 | 2.32 ± 0.14 d 2.09–2.45 | 1.68 ± 0.11 g 1.52–1.87 | 1.57 ± 0.09 e 1.41–1.68 | 4.70 ± 0.33 g 4.22–5.15 | 6.95 ± 0.44 i 6.16–7.51 | 34.3 ± 3.49 d 28.2–38.9 | 41.4 ± 3.89 d 35.6–47.2 | 29.9 ± 5.45 h 25.2–42.4 | 31.0 ± 5.32 h 22.8–38.5 |
| Milk and diary | 0.034 ± 0.004 cd 0.028–0.038 | 0.030 ± 0.005 a 0.024–0.039 | 1.92 ± 0.13 f 1.71–2.14 | 2.24 ± 0.08 d 2.14–2.35 | 0.04 ± 0.003 ab 0.03–0.04 | 0.032 ± 0.004 ab 0.027–0.038 | 0.30 ± 0.05 ab 0.24–0.36 | 0.568 ± 0.060 cde 0.450–0.650 | 19.1 ± 1.61 f 17.0–21.8 | 36.0 ± 4.44 e 28.9–42.5 | 4.99 ± 0.55 bc 4.11–5.72 | 9.18 ± 0.77 be 8.28–10.4 |
| Eggs | 0.010 ± 0.002 ab 0.008–0.013 | 0.022 ± 0.002 acd 0.018–0.025 | 0.20 ± 0.03 abc 0.16–0.25 | 0.41 ± 0.03 c 0.360–0.450 | 0.004 ± 0.001 a 0.003–0.006 | 0.018 ± 0.004 a 0.014–0.025 | 0.26 ± 0.03 a 0.21–0.29 | 0.530 ± 0.056 cd 0.440–0.590 | 1.47 ± 0.25 bc 1.06–1.75 | 5.64 ± 0.43 a 5.12–6.26 | 0.60 ± 0.08 a 0.47–0.70 | 2.13 ± 0.27 ac 1.62–2.36 |
| Meat and meat products | 0.132 ± 0.016 e 0.116–0.158 | 0.138 ± 0.010 e 0.122–0.151 | 2.46 ± 0.22 h 2.11–2.74 | 3.39 ± 0.39 f 2.80–3.82 | 0.14 ± 0.007 c 0.13–0.15 | 0.101 ± 0.014 ab 0.075–0.118 | 1.80 ± 0.26 f 1.45–2.26 | 2.20 ± 0.153 h 1.88–2.34 | 23.8 ± 2.09 g 19.8–26.2 | 40.6 ± 4.13 d 34.7–46.2 | 6.70 ± 0.93 cd 5.33–8.22 | 17.3 ± 1.19 f 15.3–18.5 |
| Fish | 0.006 ± 0.001 ab 0.004–0.007 | 0.009 ± 0.001 bc 0.007–0.011 | 0.8 ± 0.01 ad 0.06–0.09 | 0.087 ± 0.015 ab 0.060–0.110 | 0.003 ± 0.0008 a 0.002–0.004 | 0.005 ± 0.0007 a 0.003–0.005 | 0.14 ± 0.02 ac 0.12–0.17 | 0.213 ± 0.027 ab 0.170–0.250 | 6.07 ± 0.65 a 5.22–7.11 | 2.65 ± 0.39 ab 2.24–3.28 | 1.52 ± 0.25 ab 1.27–1.90 | 0.91 ± 0.13 a 0.76–1.11 |
| Fats and oils | 0.0003 ± 0.0001 a 0.0002–0.0005 | 0.001 ± 0.0002 b 0.0008–0.0014 | 0.001 ± 0.0002 d 0.0008–0.001 | 0.002 ± 0.0003 a 0.002–0.003 | <LOQ | <LOQ | 0.006 ± 0.001 c 0.005–0.008 | 0.017 ± 0.003 a 0.014–0.023 | 0.30 ± 0.06 c 0.22–0.37 | 0.27 ± 0.03 b 0.22–0.32 | 0.87 ± 0.11 a 0.67–0.98 | 1.31 ± 0.14 a 1.11–1.51 |
| Potatoes | 0.023 ± 0.003 bc 0.020–0.031 | 0.033 ± 0.003 a 0.028–0.038 | 0.16 ± 0.016 ab 0.14–0.18 | 0.234 ± 0.025 bc 0.200–0.280 | 0.07 ± 0.003 b 0.06–0.07 | 0.116 ± 0.010 abc 0.102–0.128 | 0.29 ± 0.03 ab 0.25–0.35 | 0.324 ± 0.043 bc 0.260–0.380 | 4.09 ± 0.27 ab 3.75–4.48 | 3.13 ± 0.45 ab 2.47–3.78 | 2.39 ± 0.27 ab 2.02–2.78 | 4.30 ± 0.30 cd 3.82–4.67 |
| Vegetables | 0.170 ± 0.014 g 0.150–0.191 | 0.145 ± 0.007 e 0.132–0.155 | 0.88 ± 0.07 e 0.78–0.99 | 0.704 ± 0.044 e 0.620–0.770 | 0.47 ± 0.01 d 0.46–0.49 | 0.383 ± 0.024 d 0.351–0.414 | 1.30 ± 0.11 e 1.14–1.45 | 1.90 ± 0.18 g 1.60–2.15 | 12.3 ± 1.63 e 10.2–14.8 | 17.1 ± 1.85 c 14.5 - 20.2 | 15.4 ± 0.92 f 14.5–16.9 | 22.4 ± 1.52 g 20.1–25.3 |
| Fruits | 0.143 ± 0.019 e 0.121–0.172 | 0.114 ± 0.007 g 0.107–0.129 | 0.27 ± 0.03 bc 0.24–0.32 | 0.149 ± 0.020 ab 0.120–0.180 | 0.55 ± 0.002 e 0.53–0.59 | 0.145 ± 0.012 bc 0.131–0.165 | 0.48 ± 0.04 bd 0.42–0.55 | 0.790 ± 0.048 e 0.720–0.870 | 5.08 ± 0.35 a 4.45–5.46 | 5.06 ± 0.56 a 4.18–5.69 | 10.8 ± 1.29 e 9.23–12.3 | 11.6 ± 0.46 b 10.8–12.2 |
| Sweets and sugars | 0.075 ± 0.006 f 0.068–0.088 | 0.099 ± 0.012 f 0.081–0.120 | 0.33 ± 0.03 c 0.30–0.37 | 0.418 ± 0.036 c 0.370–0.480 | 0.14 ± 0.01 c 0.12–0.16 | 0.219 ± 0.011 c 0.205–0.232 | 1.39 ± 0.12 e 1.22–1.55 | 1.60 ± 0.15 f 1.40–1.89 | 31.8 ± 4.07 d 26.2–37.4 | 16.2 ± 0.51 c 15.2–16.8 | 8.83 ± 1.34 de 7.24–10.6 | 6.36 ± 0.34 de 5.88–6.75 |
| Water and beverages | 0.021 ± 0.002 abc 0.017–0.025 | 0.029 ± 0.003 ad 0.025 - 0.035 | 0.08 ± 0.014 ad 0.07–0.11 | 0.193 ± 0.041 ab 0.130–0.250 | 1.05 ± 0.06 f 0.97–1.14 | 3.03 ± 0.23 f 2.72–3.31 | 0.58 ± 0.04 d 0.52–0.63 | 0.632 ± 0.087 de 0.480–0.780 | 6.08 ± 1.03 a 4.69–7.46 | 4.88 ± 0.64 a 4.19–5.96 | 22.2 ± 5.23 g 12.4–28.3 | 11.5 ± 2.90 b 8.00–16.1 |
| Other products | 0.052 ± 0.005 d 0.047–0.061 | 0.014 ± 0.002 bcd 0.011–0.017 | 0.20 ± 0.02 abc 0.17–0.24 | 0.079 ± 0.012 ab 0.060–0.100 | 0.1 ± 0.007 bc 0.09–0.11 | 0.035 ± 0.003 ab 0.032–0.039 | 0.29 ± 0.05 ab 0.22–0.38 | 0.149 ± 0.020 ab 0.120–0.180 | 3.69 ± 0.50 ab 3.06–4.35 | 3.56 ± 0.23 ab 3.12–3.85 | 1.99 ± 0.15 ab 1.69–2.15 | 1.16 ± 0.20 a 0.90–1.51 |
| Total | 1.00 ± 0.04 | 1.01 ± 0.03 | 8.74 ± 0.37 | 10.2 ± 0.51 | 4.25 ± 0.19 | 5.66 ± 0.26 | 11.5 ± 0.55 | 15.9 ± 0.42 | 148 ± 7.00 | 177 ± 5.36 | 106 ± 8.00 | 119 ± 7.70 |
| EAR/AI | 0.7 | 0.7 | 6.8 | 9.4 | 1.8 | 2.3 | 8 | 6 | 25 | 35 | 45 | 45 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koch, W.; Czop, M.; Nawrocka, A.; Wiącek, D. Contribution of Major Groups of Food Products to the Daily Intake of Selected Elements—Results from Analytical Determinations Supported by Chemometric Analysis. Nutrients 2020, 12, 3412. https://doi.org/10.3390/nu12113412
Koch W, Czop M, Nawrocka A, Wiącek D. Contribution of Major Groups of Food Products to the Daily Intake of Selected Elements—Results from Analytical Determinations Supported by Chemometric Analysis. Nutrients. 2020; 12(11):3412. https://doi.org/10.3390/nu12113412
Chicago/Turabian StyleKoch, Wojciech, Marcin Czop, Agnieszka Nawrocka, and Dariusz Wiącek. 2020. "Contribution of Major Groups of Food Products to the Daily Intake of Selected Elements—Results from Analytical Determinations Supported by Chemometric Analysis" Nutrients 12, no. 11: 3412. https://doi.org/10.3390/nu12113412