Effect of Vitamin D Treatment on Dynamics of Stones Formation in the Urinary Tract and Bone Density in Children with Idiopathic Hypercalciuria

 , and
, and
Abstract
:1. Introduction
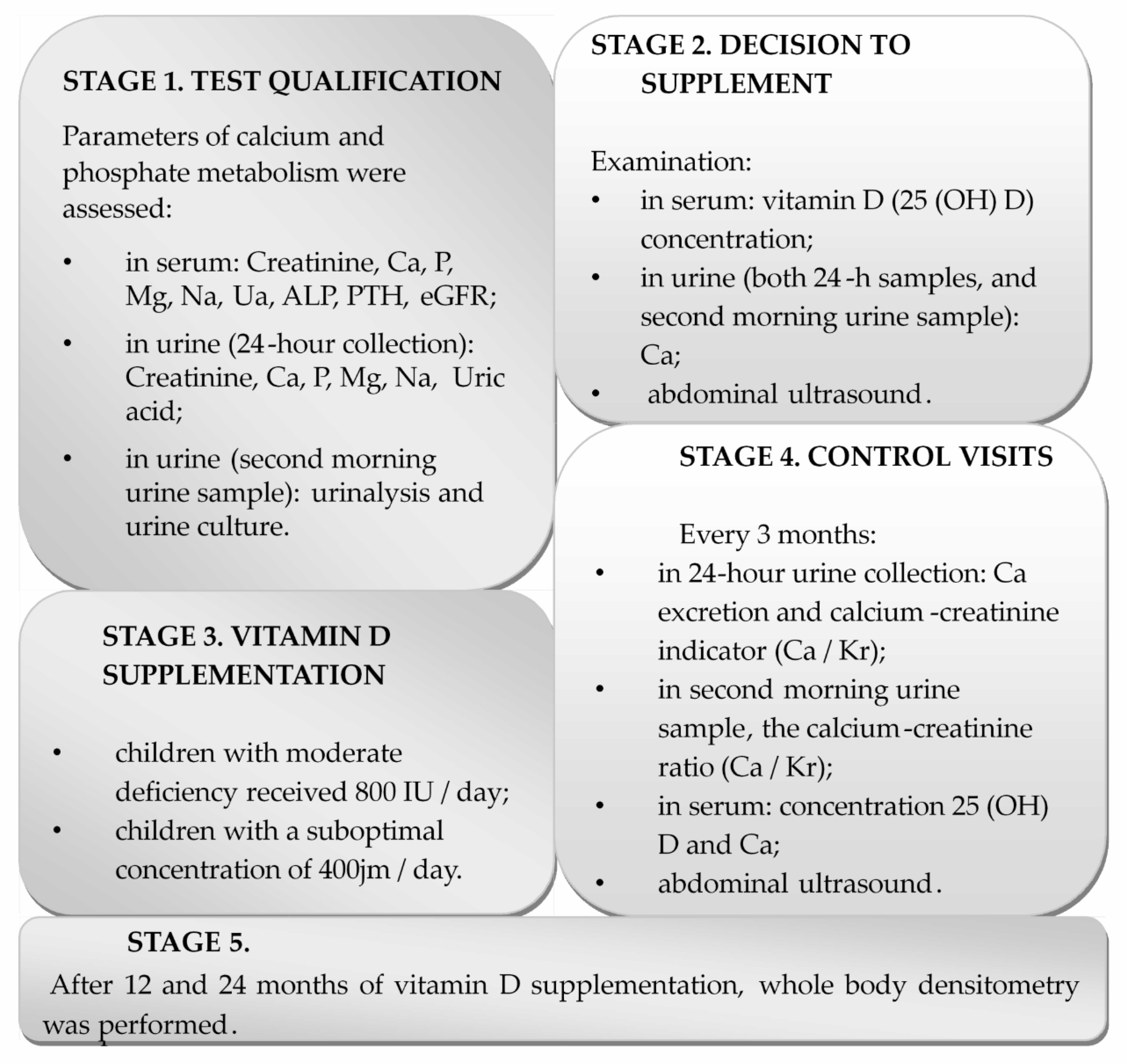
2. Materials and Methods
2.1. Patients
2.2. Experimental Study
2.3. Biochemical Parameters
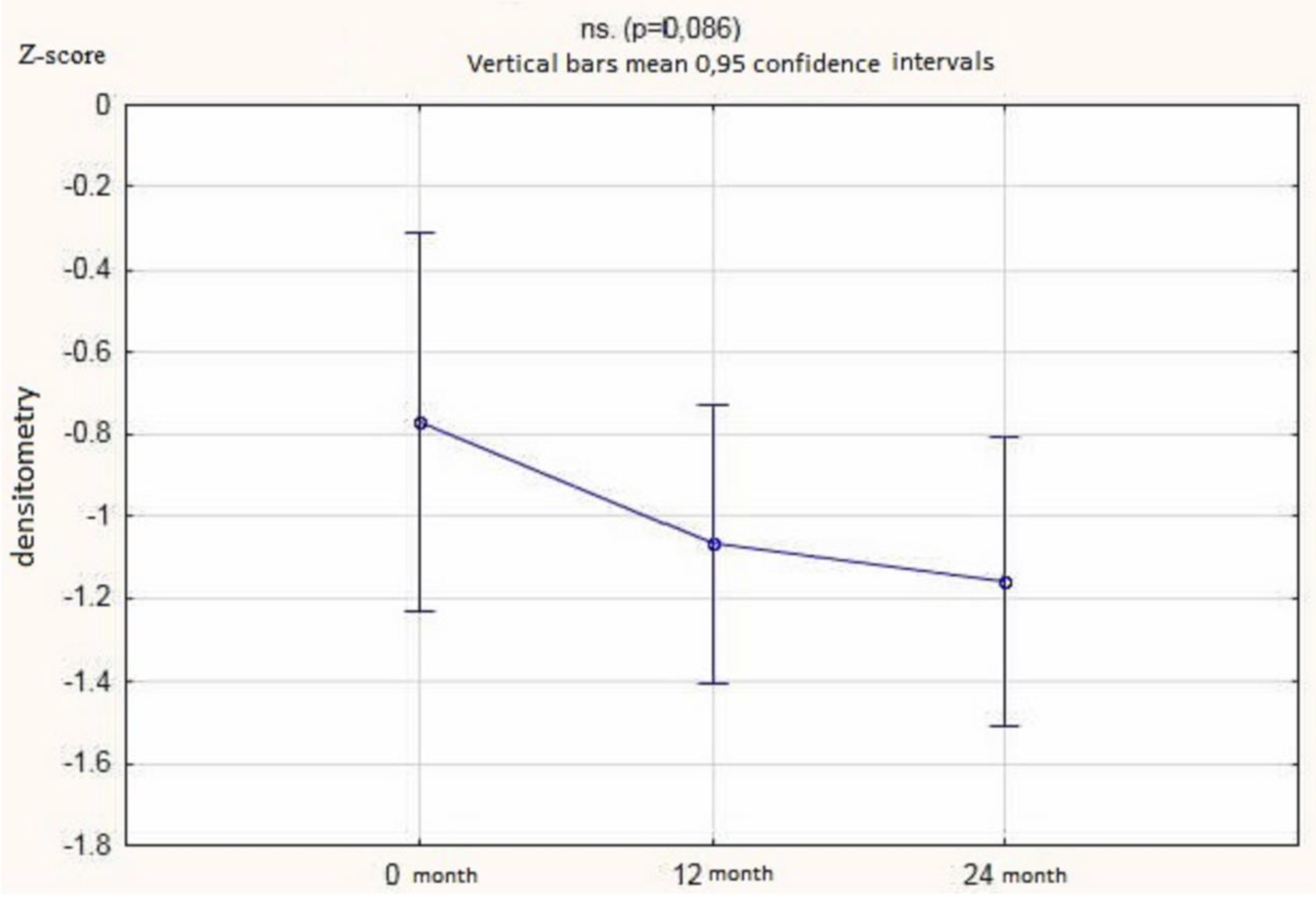
2.4. Ultrasonography and Densitometry
2.5. Statistical Analysis
3. Results
3.1. Study Population
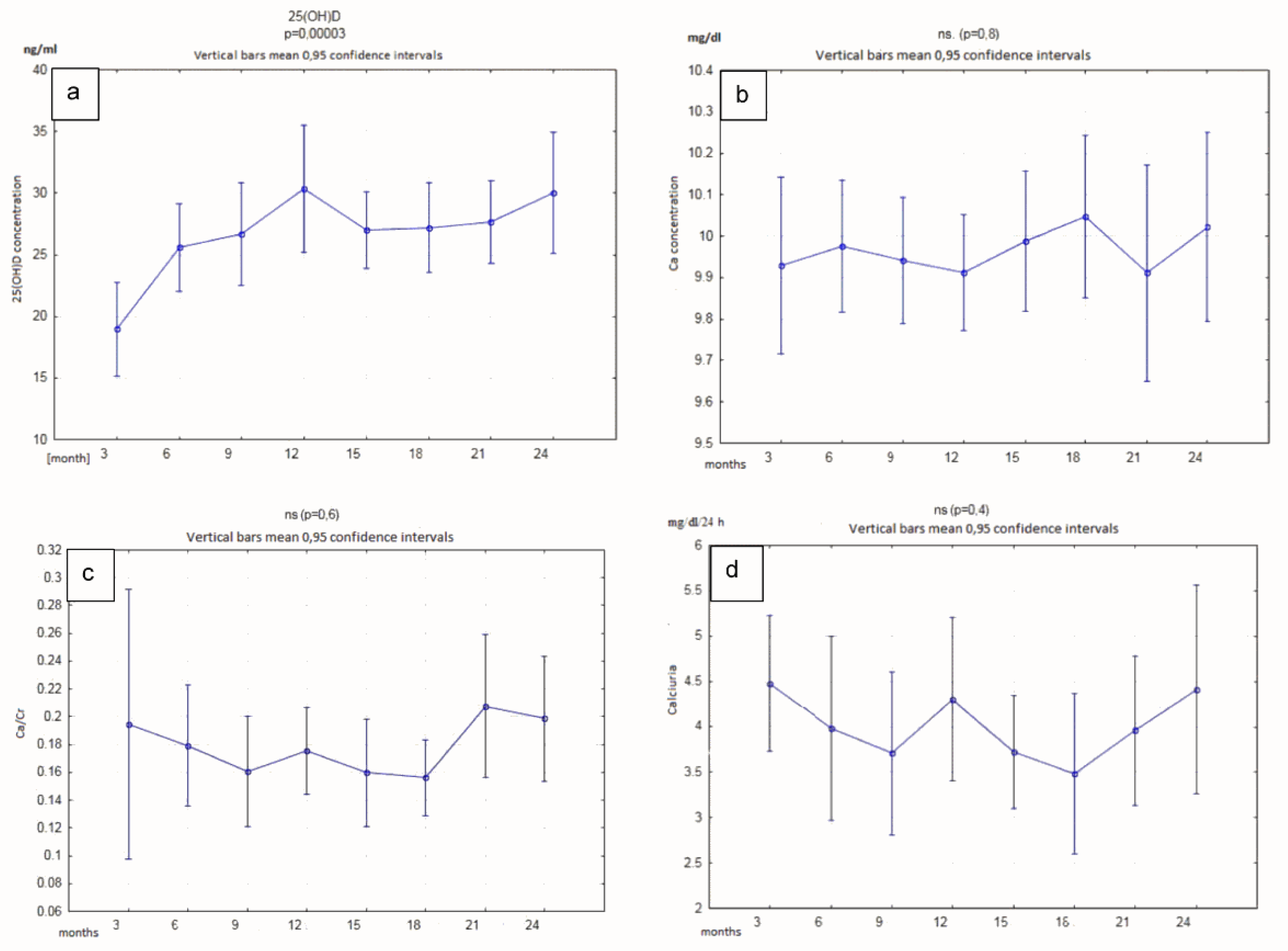
3.2. Vitamin D Level
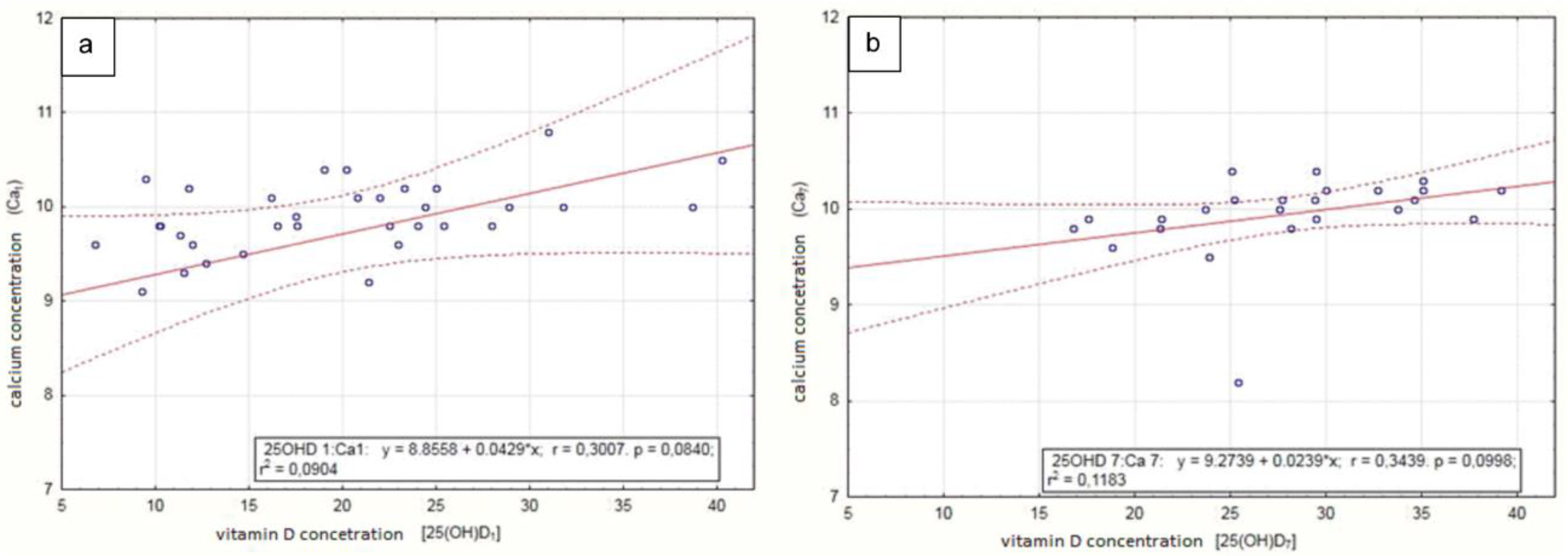
3.3. Correlations
4. Discussion
5. Limitation
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Zerwekh, J.E. Vitamin D Metabolism and Stones. In Urinary Tract Stone Disease; Rao, N.P., Preminger, G.M., Kavanagh, J.P., Eds.; Springer: London, UK, 2011; pp. 169–179. ISBN 978-1-84800-362-0. [Google Scholar]
- Holick, M.F.; Chen, T.C.; Lu, Z.; Sauter, E. Vitamin D and skin physiology: A D-lightful story. J. Bone Miner. Res. Off. J. Am. Soc. Bone Miner. Res. 2007, 22 (Suppl. 2), V28–V33. [Google Scholar] [CrossRef] [PubMed]
- Wytyczne dla lekarzy rodzinnych dotyczące suplementacji witaminy D. Available online: https://www.tvmed.pl/tresci/layout_min/11431/Wytyczne-dla-lekarzy-rodzinnych-dotyczace-suplementacji-witaminy-D (accessed on 28 June 2020).
- Zerwekh, J.E. Bone disease and hypercalciuria in children. Pediatr. Nephrol. Berl. Ger. 2010, 25, 395–401. [Google Scholar] [CrossRef] [PubMed]
- Worcester, E.M.; Coe, F.L. New insights into the pathogenesis of idiopathic hypercalciuria. Semin. Nephrol. 2008, 28, 120–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamińska, A.; Bieroza, I. Hiperkalciuria–najczęstsze zaburzenie metaboliczne u dzieci z kamicą nerkową. Nowa Pediatria 2011, 2, 49–52. [Google Scholar]
- Milart, J.; Jobs, K.; Anna, J. Hiperkalciuria idiopatyczna. Pediatr. Med. Rodz. 2016, 12, 22–27. [Google Scholar] [CrossRef]
- Kamica układu moczowego u dzieci/Urolithiasis in children-Standardy Medyczne. Available online: http://www.standardy.pl/artykuly/id/873 (accessed on 28 June 2020).
- Jobs, K.; Jung, A. Gęstość kości u pacjentów z hiperkalciurią idiopatyczną–przegląd piśmiennictwa w aspekcie bezpieczeństwa stosowania witaminy D. Pediatr. Med. Rodz. 2013, 9, 245–249. [Google Scholar]
- Rakowska, M.; Królikowska, K.; Jobs, K.; Placzyńska, M.; Kalicki, B. Pathophysiology and symptoms of renal colic in children-a case report. Dev. Period Med. 2018, 22, 265–269. [Google Scholar]
- Jobs, K.; Rakowska, M.; Paturej, A. Urolithiasis in the pediatric population-current opinion on epidemiology, patophysiology, diagnostic evaluation and treatment. Dev. Period Med. 2018, 22, 201–208. [Google Scholar]
- López, M.; Hoppe, B. History, epidemiology and regional diversities of urolithiasis. Pediatr Nephrol. 2010, 25, 49–59. [Google Scholar] [CrossRef] [Green Version]
- Iwańczak, B.; Krzesiek, E.; Iwańczak, F. Osteoporoza i osteopenia u dzieci i młodzieży–przyczyny, diagnostyka i leczenie. Adv. Clin. Exp. Med. 2004, 13, 177–184. [Google Scholar]
- Arrabal-Polo, M.Á.; Sierra Girón-Prieto, M.; Orgaz-Molina, J.; Zuluaga-Gómez, A.; Arias-Santiago, S.; Arrabal-Martín, M. Calcium renal lithiasis and bone mineral density. Importance of bone metabolism in urinary lithiasis. Actas Urol. Esp. 2013, 37, 362–367. [Google Scholar] [CrossRef] [PubMed]
- Cediel, G.; Pacheco-Acosta, J.; CastiUo-Durdn, C. Vitamin D deficiency in pediatric clinical practice. Arch. Argent. Pediatr. 2018, 116, e75–e81. [Google Scholar] [CrossRef] [PubMed]
- Povoroznyuk, V.V.; Balatska, N.I.; Muts, V.Y.; Klymovytsky, F.V.; Synenky, O.V. Vitamin D deficiency in Ukraine: A demographic and seasonal analysis. Gerontologija 2012, 13, 191–198. [Google Scholar]
- Zakharova, I.N.; Mal’tsev, S.V.; Borovik, T.E.; Yatsyk, G.V.; Malyavskaya, S.I.; Vakhlova, I.V.; Shumatova, Т.А.; Romantsova, Y.B.; Romanyuk, F.P.; Klimov, L.Y.; et al. Vitamin d Insufficiency in Children of Tender years in Russia: The Results of a Multi-Centre Cohort Study Rodnichok (2013–2014). Available online: https://vsp.spr-journal.ru/jour/article/view/98 (accessed on 21 July 2020).
- Vitamin D Deficiency/Insufficiency from Childhood to Adulthood: Insights from a Sunny Country. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5296623/ (accessed on 21 July 2020).
- Wrzosek, M.; Woźniak, J.; Kozioł-Kaczorek, D.; Włodarek, D. The Assessment of the Supply of Calcium and Vitamin D in the Diet of Women Regularly Practicing Sport. J. Osteoporos. 2019, 2019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, J.; Chonchol, M.B. Vitamin D and kidney stone disease. Curr. Opin. Nephrol. Hypertens. 2013, 22, 383–389. [Google Scholar] [CrossRef] [PubMed]
- Taheri, M.; Tavasoli, S.; Shokrzadeh, F.; Amiri, F.B.; Basiri, A.; Taheri, M.; Tavasoli, S.; Shokrzadeh, F.; Amiri, F.B.; Basiri, A. Effect of vitamin D supplementation on 24-hour urine calcium in patients with calcium Urolithiasis and vitamin D deficiency. Int. Braz. J. Urol. 2019, 45, 340–346. [Google Scholar] [CrossRef] [PubMed]
- Ticinesi, A.; Nouvenne, A.; Ferraro, P.M.; Folesani, G.; Lauretani, F.; Allegri, F.; Guerra, A.; Cerundolo, N.; Aloe, R.; Lippi, G.; et al. Idiopathic Calcium Nephrolithiasis and Hypovitaminosis D: A Case-control Study. Urology 2016, 87, 40–45. [Google Scholar] [CrossRef]
- Malihi, Z.; Wu, Z.; Stewart, A.W.; Lawes, C.M.; Scragg, R. Hypercalcemia, hypercalciuria, and kidney stones in long-term studies of vitamin D supplementation: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2016, 104, 1039–1051. [Google Scholar] [CrossRef] [Green Version]
- Cranney, A.; Horsley, T.; O’Donnell, S.; Weiler, H.; Puil, L.; Ooi, D.; Atkinson, S.; Ward, L.; Moher, D.; Hanley, D.; et al. Effectiveness and Safety of Vitamin D in Relation to Bone Health. Evid. Rep. Technol. Assess (Full Rep). 2007, 158, 1–235. [Google Scholar]
- Avenell, A.; Mak, J.C.S.; O’Connell, D. Vitamin D and vitamin D analogues for preventing fractures in post-menopausal women and older men. Cochrane Database Syst. Rev. 2014, CD000227. [Google Scholar] [CrossRef]
- Bjelakovic, G.; Gluud, L.L.; Nikolova, D.; Whitfield, K.; Wetterslev, J.; Simonetti, R.G.; Bjelakovic, M.; Gluud, C. Vitamin D supplementation for prevention of mortality in adults. Cochrane Database Syst. Rev. 2011, CD007470. [Google Scholar] [CrossRef]
- Bjelakovic, G.; Gluud, L.L.; Nikolova, D.; Whitfield, K.; Krstic, G.; Wetterslev, J.; Gluud, C. Vitamin D supplementation for prevention of cancer in adults. Cochrane Database Syst. Rev. 2014, CD007469. [Google Scholar] [CrossRef] [PubMed]
- Kearns, M.D.; Alvarez, J.A.; Tangpricha, V. Large, single-dose, oral vitamin D supplementation in adult populations: A systematic review. Endocr. Pract. Off. J. Am. Coll. Endocrinol. Am. Assoc. Clin. Endocrinol. 2014, 20, 341–351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leaf, D.E.; Korets, R.; Taylor, E.N.; Tang, J.; Asplin, J.R.; Goldfarb, D.S.; Gupta, M.; Curhan, G.C. Effect of vitamin D repletion on urinary calcium excretion among kidney stone formers. Clin. J. Am. Soc. Nephrol. CJASN 2012, 7, 829–834. [Google Scholar] [CrossRef]
- Johri, N.; Jaeger, P.; Ferraro, P.M.; Shavit, L.; Nair, D.; Robertson, W.G.; Gambaro, G.; Unwin, R.J. Vitamin D deficiency is prevalent among idiopathic stone formers, but does correction pose any risk? Urolithiasis 2017, 45, 535–543. [Google Scholar] [CrossRef] [Green Version]
- Eisner, B.H.; Thavaseelan, S.; Sheth, S.; Haleblian, G.; Pareek, G. Relationship Between Serum Vitamin D and 24-Hour Urine Calcium in Patients With Nephrolithiasis. Urology 2012, 80, 1007–1010. [Google Scholar] [CrossRef]
- Sorkhi, H.; Aahmadi, M.H. Urinary calcium to creatinin ratio in children. Indian J. Pediatr. 2005, 72, 1055–1056. [Google Scholar] [CrossRef]
- Letavernier, E.; Verrier, C.; Goussard, F.; Perez, J.; Huguet, L.; Haymann, J.-P.; Baud, L.; Bazin, D.; Daudon, M. Calcium and vitamin D have a synergistic role in a rat model of kidney stone disease. Kidney Int. 2016, 90, 809–817. [Google Scholar] [CrossRef] [Green Version]
- Penniston, K.L.; Jones, A.N.; Nakada, S.Y.; Hansen, K.E. Vitamin D repletion does not alter urinary calcium excretion in healthy postmenopausal women. BJU Int. 2009, 104, 1512–1516. [Google Scholar] [CrossRef] [Green Version]
- Ferraro, P.M.; Taylor, E.N.; Gambaro, G.; Curhan, G.C. Vitamin D Intake and the Risk of Incident Kidney Stones. J. Urol. 2017, 197, 405–410. [Google Scholar] [CrossRef]
- Nieradko-Iwanicka, B.; Borzęcki, A. Osteoporoza jako problem pediatryczny. Probl. Hig. Epidemiol. 2009, 90, 27–31. [Google Scholar]
- Lorenc, R.; Karczmarewicz, E. Znaczenie wapnia i witaminy D w optymalizacji masy kostnej oraz zapobieganiu i leczeniu osteoporozy u dzieci. Pediat. Współcz. 2001, 3, 105–109. [Google Scholar]
- Pfau, A.; Knauf, F. Update on Nephrolithiasis: Core Curriculum 2016. Am. J. Kidney Dis. Off. J. Natl. Kidney Found. 2016, 68, 973–985. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moreira Guimarães Penido, M.G.; de Sousa Tavares, M.; Campos Linhares, M.; Silva Barbosa, A.C.; Cunha, M. Longitudinal study of bone mineral density in children with idiopathic hypercalciuria. Pediatr. Nephrol. 2012, 27, 123–130. [Google Scholar] [CrossRef]
- Penido, M.-G.M.G.; Lima, E.M.; Souto, M.F.O.; Marino, V.S.P.; Tupinambá, A.-L.F.; França, A. Hypocitraturia: A risk factor for reduced bone mineral density in idiopathic hypercalciuria? Pediatr. Nephrol. Berl. Ger. 2006, 21, 74–78. [Google Scholar] [CrossRef]
- Schwaderer, A.L.; Cronin, R.; Mahan, J.D.; Bates, C.M. Low bone density in children with hypercalciuria and/or nephrolithiasis. Pediatr. Nephrol. Berl. Ger. 2008, 23, 2209–2214. [Google Scholar] [CrossRef]
- Artemiuk, I.; Pańczyk-Tomaszewska, M.; Adamczuk, D.; Przedlacki, J.; Roszkowska-Blaim, M. Bone mineral density in children with idiopathic hypercalciuria. Dev. Period Med. 2015, 19, 356–361. [Google Scholar]
- Gambaro, G.; Croppi, E.; Coe, F.; Lingeman, J.; Moe, O.; Worcester, E.; Buchholz, N.; Bushinsky, D.; Curhan, G.C.; Ferraro, P.M.; et al. Metabolic diagnosis and medical prevention of calcium nephrolithiasis and its systemic manifestations: A consensus statement. J. Nephrol. 2016, 29, 715–734. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age | mg Calcium/mg Creatinine |
|---|---|
| <1 year | <0.81 |
| 1–3 years | <0.53 |
| 3–5 years | <0.39 |
| 5–7 years | <0.28 |
| >7 years | <0.21 |
| Parameter | N | Mean ± SD | Units | Median (q25–q75) |
|---|---|---|---|---|
| 25-hydroxy-vitamin D | 35 | 20.02 ± 8.52 | ng/mL | 20.2 (11.8–25.00) |
| Ca | 35 | 9.72 ± 1.19 | mg/dL | 9.8 (9.6–10.20) |
| Calciuria | 36 | 4.28 ± 1.85 | mg/kg/24 h | 4.515 (2.94–5.37) |
| Ca/Creatinine | 33 | 0.19 ± 0.16 | mg/mg | 0.198 (0.13–0.26) |
| Z-score | 36 | −0.73 ± 0.87 | - | −0.855 ((−)1.26–(−)0.36) |
| Parameter | N | Mean ± SD | Units | Median (q25–q75) |
|---|---|---|---|---|
| 25-hydroxy-vitamin D | 22 | 29.85 ± 9.65 | ng/mL | 29.25 (21.5–35.5) |
| Ca | 21 | 10.02 ± 0.41 | mg/dL | 9.9 (9.8–10.20) |
| Calciuria | 21 | 4.5 ± 2.24 | mg/kg/24h | 4.06 (3.30–5.43) |
| Ca/Creatinine | 22 | 0.2 ± 0.09 | mg/mg | 0.185 (0.13–0.26) |
| Z-score | 23 | −1.05 ± 0.77 | - | −0.96 ((−)1.7–(−)0.56) |
| Variables | Time | R Spearman | p |
|---|---|---|---|
| 25-hydroxy-vitamin D and calcium (Ca) | 3 months | 0.451871 | 0.007301 |
| 6 months | 0.215881 | 0.220112 | |
| 9 months | 0.216470 | 0.226283 | |
| 12 months | 0.037120 | 0.834899 | |
| 15 months | 0.297773 | 0.103748 | |
| 18 months | 0.068840 | 0.743692 | |
| 21 months | 0.560887 | 0.004355 | |
| 24 months | 0.237260 | 0.300404 | |
| 25-hydroxy-vitamin D and calciuria | 3 months | 0.093781 | 0.592064 |
| 6 months | −0.040049 | 0.822074 | |
| 9 months | −0.016993 | 0.921642 | |
| 12 months | 0.223403 | 0.204067 | |
| 15 months | 0.059459 | 0.754959 | |
| 18 months | 0.087581 | 0.670520 | |
| 21 months | −0.142049 | 0.507896 | |
| 24 months | −0.059740 | 0.797001 | |
| 25-hydroxy-vitamin D and Ca/creatinine ratio | 3 months | −0.039043 | 0.831986 |
| 6 months | −0.040196 | 0.821432 | |
| 9 months | −0.006245 | 0.971165 | |
| 12 months | −0.133705 | 0.450932 | |
| 15 months | 0.176983 | 0.332539 | |
| 18 months | −0.098432 | 0.647248 | |
| 21 months | −0.235857 | 0.267205 | |
| 24 months | −0.206331 | 0.356917 | |
| 25-hydroxy-vitamin D and densitometry | 12 months | 0.104499 | 0.575855 |
| 24 months | −0.314512 | 0.153997 |
| Time | p Value | Odds Ratio | Confidence OR −95% | Confidence OR +95% | |
|---|---|---|---|---|---|
| 25-hydroxy-vitamin D and urolithiasis activity | 3 months | 0.761 | 0.987 | 0.909 | 1.072 |
| 12 months | 0.498 | 1.027 | 0.952 | 1.108 | |
| 24 months | 0.509 | 1.039 | 0.927 | 1.164 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Milart, J.; Lewicka, A.; Jobs, K.; Wawrzyniak, A.; Majder-Łopatka, M.; Kalicki, B. Effect of Vitamin D Treatment on Dynamics of Stones Formation in the Urinary Tract and Bone Density in Children with Idiopathic Hypercalciuria. Nutrients 2020, 12, 2521. https://doi.org/10.3390/nu12092521
Milart J, Lewicka A, Jobs K, Wawrzyniak A, Majder-Łopatka M, Kalicki B. Effect of Vitamin D Treatment on Dynamics of Stones Formation in the Urinary Tract and Bone Density in Children with Idiopathic Hypercalciuria. Nutrients. 2020; 12(9):2521. https://doi.org/10.3390/nu12092521
Chicago/Turabian StyleMilart, Joanna, Aneta Lewicka, Katarzyna Jobs, Agata Wawrzyniak, Małgorzata Majder-Łopatka, and Bolesław Kalicki. 2020. "Effect of Vitamin D Treatment on Dynamics of Stones Formation in the Urinary Tract and Bone Density in Children with Idiopathic Hypercalciuria" Nutrients 12, no. 9: 2521. https://doi.org/10.3390/nu12092521