Hydrolyzed Chicken Extract (ProBeptigen®) on Cognitive Function in Healthy Middle-Aged People: A Randomized Double-Blind Trial

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
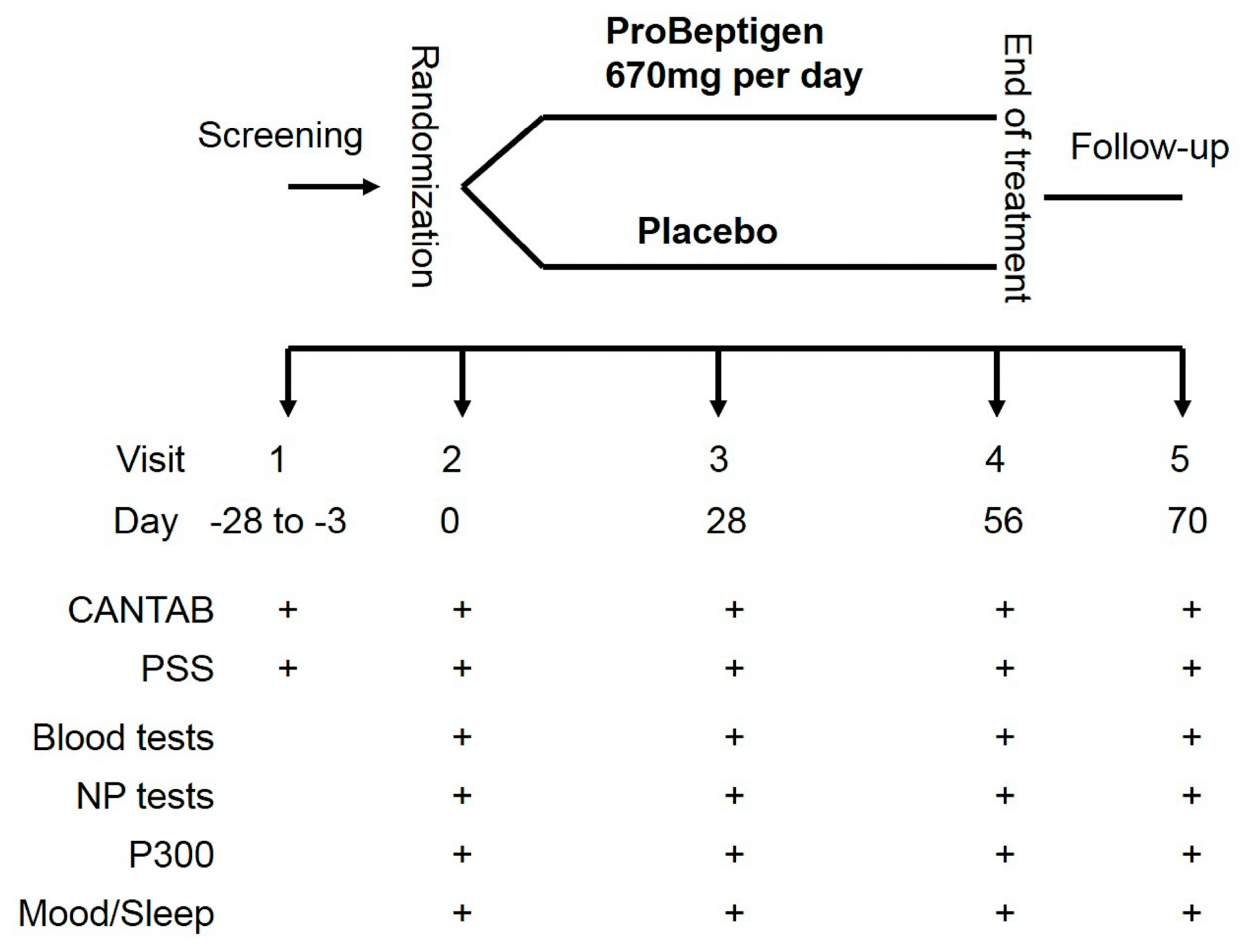
2.2. Study Procedure
2.3. ProBeptigen® and Placebo
2.4. Measurements
2.4.1. Neurocognitive Tests
2.4.2. Self-Reported Instruments
2.4.3. Blood Tests
2.4.4. ERPs
2.5. Statistical Analysis
2.6. Ethical Approval and Trial Registration
3. Results
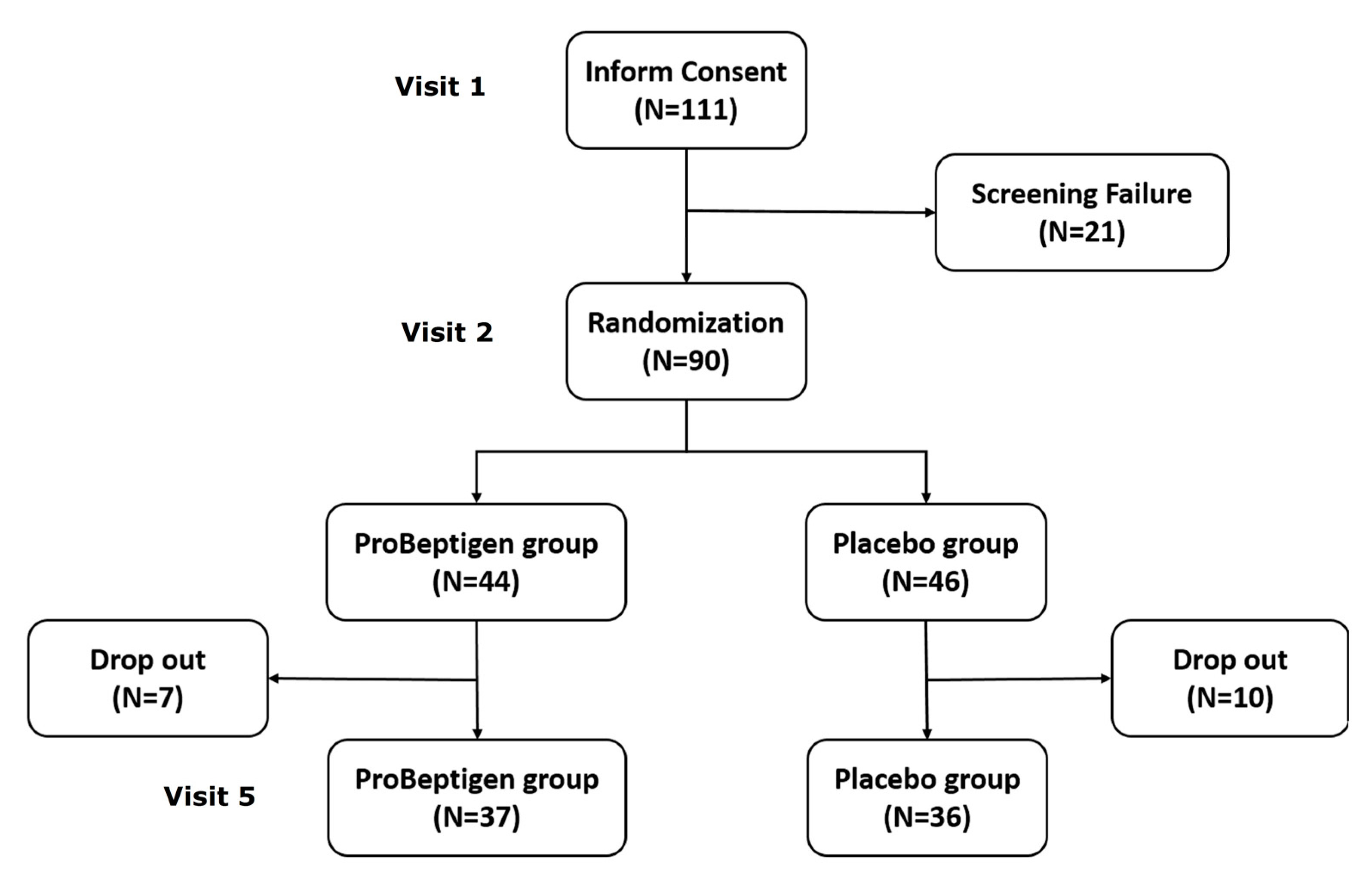
3.1. Participant Charateristics
3.2. Neurocognitive Outcomes
3.2.1. WMS-III
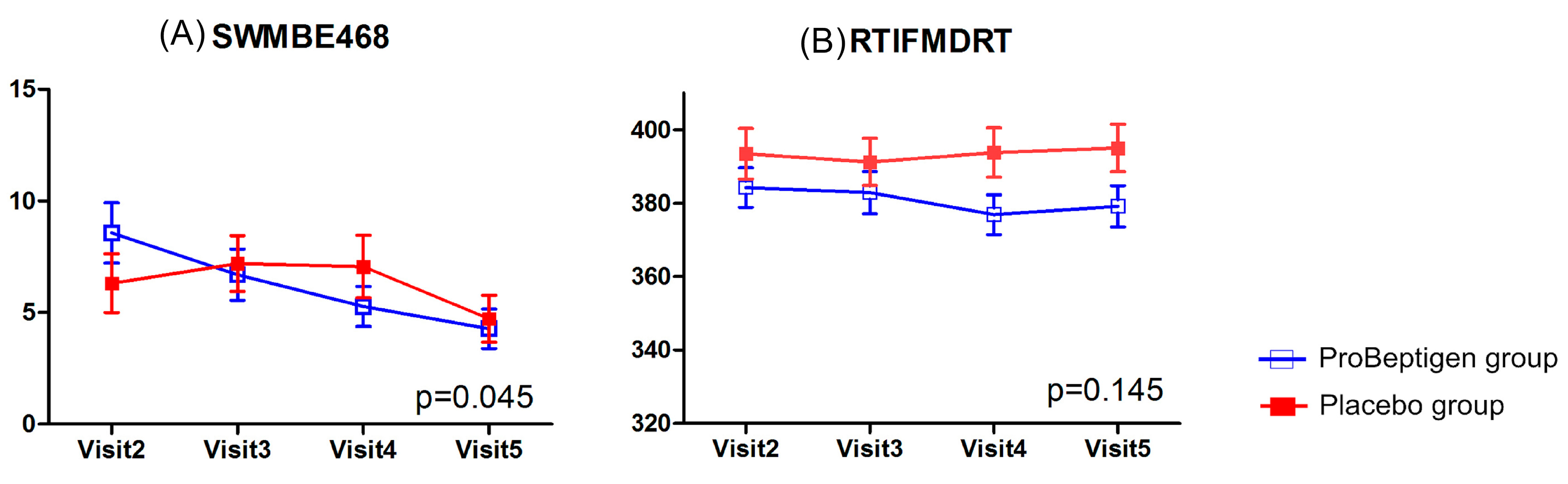
3.2.2. CANTAB
3.3. Self-reported Measurements
3.4. Physiological Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Barnes, D.E.; Yaffe, K. The projected effect of risk factor reduction on Alzheimer’s disease prevalence. Lancet Neurol. 2011, 10, 819–828. [Google Scholar] [CrossRef] [Green Version]
- Deary, I.J.; Corley, J.; Gow, A.J.; Harris, S.E.; Houlihan, L.M.; Marioni, R.E.; Penke, L.; Rafnsson, S.B.; Starr, J.M. Age-associated cognitive decline. Br. Med. Bull. 2009, 92, 135–152. [Google Scholar] [CrossRef]
- Salthouse, T.A. When does age-related cognitive decline begin? Neurobiol. Aging 2009, 30, 507–514. [Google Scholar] [CrossRef] [Green Version]
- Singh-Manoux, A.; Kivimaki, M.; Glymour, M.M.; Elbaz, A.; Berr, C.; Ebmeier, K.P.; Ferrie, J.E.; Dugravot, A. Timing of onset of cognitive decline: Results from Whitehall II prospective cohort study. BMJ 2012, 344, d7622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karlamangla, A.S.; Lachman, M.E.; Han, W.; Huang, M.; Greendale, G.A. Evidence for Cognitive Aging in Midlife Women: Study of Women’s Health Across the Nation. PLoS ONE 2017, 12, e0169008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walker, K.A.; Gottesman, R.F.; Wu, A.; Knopman, D.S.; Gross, A.L.; Mosley, T.H., Jr.; Selvin, E.; Windham, B.G. Systemic inflammation during midlife and cognitive change over 20 years: The ARIC Study. Neurology 2019, 92, e1256–e1267. [Google Scholar] [CrossRef] [PubMed]
- Echouffo-Tcheugui, J.B.; Conner, S.C.; Himali, J.J.; Maillard, P.; DeCarli, C.S.; Beiser, A.S.; Vasan, R.S.; Seshadri, S. Circulating cortisol and cognitive and structural brain measures: The Framingham Heart Study. Neurology 2018, 91, e1961–e1970. [Google Scholar] [CrossRef]
- Goodnite, P.M. Stress: A concept analysis. Nurs. Forum. 2014, 49, 71–74. [Google Scholar] [CrossRef]
- McGrath, J.E. Stress and behavior in organizations. In Handbook of Industrial and Organizational Psychology; Dunnette, M.D., Ed.; Rand Mcnally: Chicago, IL, USA, 1976; pp. 1351–1395. [Google Scholar]
- AbuAlRub, R.F. Job stress, job performance, and social support among hospital nurses. J. Nurs. Scholarsh. 2004, 36, 73–78. [Google Scholar] [CrossRef]
- Gandi, J.C.; Wai, P.S.; Karick, H.; Dagona, Z.K. The role of stress and level of burnout in job performance among nurses. Ment. Health Fam. Med. 2011, 8, 181–194. [Google Scholar]
- Lue, B.H.; Chen, H.J.; Wang, C.W.; Cheng, Y.; Chen, M.C. Stress, personal characteristics and burnout among first postgraduate year residents: A nationwide study in Taiwan. Med. Teach. 2010, 32, 400–407. [Google Scholar] [CrossRef] [PubMed]
- Sandström, A.; Peterson, J.; Sandstrom, E.; Lundberg, M.; Nystrom, I.L.; Nyberg, L.; Olsson, T. Cognitive deficits in relation to personality type and hypothalamic-pituitary-adrenal (HPA) axis dysfunction in women with stress-related exhaustion. Scand. J. Psychol. 2011, 52, 71–82. [Google Scholar] [CrossRef] [PubMed]
- Wade, A.T.; Elias, M.F.; Murphy, K.J. Adherence to a Mediterranean diet is associated with cognitive function in an older non-Mediterranean sample: Findings from the Maine-Syracuse Longitudinal Study. Nutr. Neurosci. 2019, 1–12. [Google Scholar] [CrossRef]
- Nooyens, A.C.; Milder, I.E.; van Gelder, B.M.; Bueno-de-Mesquita, H.B.; van Boxtel, M.P.; Verschuren, W.M. Diet and cognitive decline at middle age: The role of antioxidants. Br. J. Nutr. 2015, 113, 1410–1417. [Google Scholar] [CrossRef] [Green Version]
- Durga, J.; van Boxtel, M.P.; Schouten, E.G.; Kok, F.J.; Jolles, J.; Katan, M.B.; Verhoef, P. Effect of 3-year folic acid supplementation on cognitive function in older adults in the FACIT trial: A randomised, double blind, controlled trial. Lancet 2007, 369, 208–216. [Google Scholar] [CrossRef] [Green Version]
- Morris, M.C.; Evans, D.A.; Tangney, C.C.; Bienias, J.L.; Schneider, J.A.; Wilson, R.S.; Scherr, P.A. Dietary copper and high saturated and trans fat intakes associated with cognitive decline. Arch. Neurol. 2006, 63, 1085–1088. [Google Scholar] [CrossRef] [Green Version]
- Wouters-Wesseling, W.; Wagenaar, L.W.; Rozendaal, M.; Deijen, J.B.; de Groot, L.C.; Bindels, J.G.; van Staveren, W.A. Effect of an enriched drink on cognitive function in frail elderly persons. J. Gerontol. A Biol. Sci. Med. Sci. 2005, 60, 265–270. [Google Scholar] [CrossRef] [Green Version]
- Denis, I.; Potier, B.; Heberden, C.; Vancassel, S. Omega-3 polyunsaturated fatty acids and brain aging. Curr. Opin. Clin. Nutr. Metab. Care 2015, 18, 139–146. [Google Scholar] [CrossRef] [Green Version]
- Stough, C.; Downey, L.; Silber, B.; Lloyd, J.; Kure, C.; Wesnes, K.; Camfield, D. The effects of 90-day supplementation with the omega-3 essential fatty acid docosahexaenoic acid (DHA) on cognitive function and visual acuity in a healthy aging population. Neurobiol. Aging 2012, 33, 824.e821–e823. [Google Scholar] [CrossRef]
- Stonehouse, W.; Conlon, C.A.; Podd, J.; Hill, S.R.; Minihane, A.M.; Haskell, C.; Kennedy, D. DHA supplementation improved both memory and reaction time in healthy young adults: A randomized controlled trial. Am. J. Clin. Nutr. 2013, 97, 1134–1143. [Google Scholar] [CrossRef] [Green Version]
- Jakobsen, L.H.; Kondrup, J.; Zellner, M.; Tetens, I.; Roth, E. Effect of a high protein meat diet on muscle and cognitive functions: A randomised controlled dietary intervention trial in healthy men. Clin. Nutr. 2011, 30, 303–311. [Google Scholar] [CrossRef] [PubMed]
- Markus, C.R.; Olivier, B.; de Haan, E.H. Whey protein rich in alpha-lactalbumin increases the ratio of plasma tryptophan to the sum of the other large neutral amino acids and improves cognitive performance in stress-vulnerable subjects. Am. J. Clin. Nutr. 2002, 75, 1051–1056. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagai, H.; Harada, M.; Nakagawa, M.; Tanaka, T.; Gunadi, B.; Setiabudi, M.L.; Uktolseja, J.L.; Miyata, Y. Effects of chicken extract on the recovery from fatigue caused by mental workload. Appl. Hum. Sci. 1996, 15, 281–286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azhar, Z.M.; Syedsahiljamalulail, S. Effect of taking chicken essence on stress and cognition of human volunteers. Malays. J. Nutr. 2003, 9, 19–29. [Google Scholar]
- Azhar, Z.M.; Zubaidah, J.O.; Norjan, K.O.N. Effect of taking chicken essence on cognitive functioning of normal stressed human volunteers. Malays. J. Med. Health Sci. 2008, 4, 57–68. [Google Scholar]
- Chan, L.; Wang, H.M.; Chen, K.Y.; Lin, Y.C.; Wu, P.J.; Hsieh, W.L.; Chen, Y.R.; Liu, C.P.; Tsai, H.Y.; Chen, Y.R.; et al. Effectiveness of Essence of Chicken in Improving Cognitive Function in Young People Under Work-Related Stress: A Randomized Double-Blind Trial. Medicine 2016, 95, e3640. [Google Scholar] [CrossRef] [PubMed]
- 28-Day Repeated Dose of Oral Toxicity Study in Rats—Chicken Meat Ingredient/CE Protein Powder (Unpublished Report); MedGaea Life Sciences Ltd.: New Taipei City, Taiwan, 2015; pp. 1–168.
- 28-Day Repeated Dose of Oral Toxicity Study in Rats—Chicken meat ingredient (Unpublished Report); MedGaea Life Sciences Ltd.: New Taipei City, Taiwan, 2016; pp. 2–76.
- A Human Tolerance, Safety, and Quality of Life Study on a Protein-Peptide Extract Health Supplement (Unpublished Report); Asia Global Research Co., Ltd.: Bangkok, Thailand, 2019; pp. 1–56.
- Tsai, S.F.; Chang, C.Y.; Yong, S.M.; Lim, A.L.; Nakao, Y.; Chen, S.J.; Kuo, Y.M. A Hydrolyzed Chicken Extract CMI-168 Enhances Learning and Memory in Middle-Aged Mice. Nutrients 2018, 11, 27. [Google Scholar] [CrossRef] [Green Version]
- Chou, M.Y.; Chen, Y.J.; Lin, L.H.; Nakao, Y.; Lim, A.L.; Wang, M.F.; Yong, S.M. Protective Effects of Hydrolyzed Chicken Extract (Probeptigen(R)/Cmi-168) on Memory Retention and Brain Oxidative Stress in Senescence-Accelerated Mice. Nutrients 2019, 11, 1870. [Google Scholar] [CrossRef] [Green Version]
- Azhar, Z.M.; Zubaidah, J.O.; Norjan, K.O.N.; Zhuang, C.Y.; Tsang, F. A pilot placebo-controlled, double-blind, and randomized study on the cognition-enhancing benefits of a proprietary chicken meat ingredient in healthy subjects. Nutr. J. 2013, 12, 121. [Google Scholar] [CrossRef] [Green Version]
- Ni, Y.; Ni, L.; Ma, L.; Wang, Z.; Zhao, Y.; Hu, L.; Zheng, L.; Fu, Z. Neuroprotective Effects of ProBeptigen/CMI-168 on Aging-Induced Cognitive Decline and Neuroinflammation in Mice: A Comparison with Essence of Chicken; College of Biotechnology and Bioengineering, Zhejiang University of Technology: Hangzhou, China, 2020. [Google Scholar]
- Cambridge Cognition CANTAB®. Cognitive Assessment Software; Cambridge Cognition: Cambridge, UK, 2016. [Google Scholar]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef]
- Beck, A.T.; Steer, R.A.; Brown, G.K. Manual for the Beck Depression Inventory-II; Psychological Corporation: San Antonio, TX, USA, 1996. [Google Scholar]
- Spielberger, C.D.; Gorsuch, R.L.; Lushene, R.; Vagg, P.R.; Jacobs, G.A. Manual for the State-Trait. Anxiety Inventory (STAI); Consulting Psychologists Press: Palo Alto, CA, USA, 1983. [Google Scholar]
- Buysse, D.J.; Reynolds, C.F., 3rd; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Faden, A.I.; Knoblach, S.M.; Movsesyan, V.A.; Cernak, I. Novel small peptides with neuroprotective and nootropic properties. J. Alzheimers Dis. 2004, 6, S93–S97. [Google Scholar] [CrossRef] [PubMed]
- Tsuruoka, N.; Beppu, Y.; Koda, H.; Doe, N.; Watanabe, H.; Abe, K. A DKP cyclo(L-Phe-L-Phe) found in chicken essence is a dual inhibitor of the serotonin transporter and acetylcholinesterase. PLoS ONE 2012, 7, e50824. [Google Scholar] [CrossRef] [PubMed]
- Gudasheva, T.A.; Boyko, S.S.; Akparov, V.; Ostrovskaya, R.U.; Skoldinov, S.P.; Rozantsev, G.G.; Voronina, T.A.; Zherdev, V.P.; Seredenin, S.B. Identification of a novel endogenous memory facilitating cyclic dipeptide cyclo-prolylglycine in rat brain. FEBS Lett. 1996, 391, 149–152. [Google Scholar] [CrossRef] [Green Version]
- Prasad, C. Bioactive cyclic dipeptides. Peptides 1995, 16, 151–164. [Google Scholar] [CrossRef]
- Tabassum, S.; Ahmad, S.; Madiha, S.; Khaliq, S.; Shahzad, S.; Batool, Z.; Haider, S. Impact of oral supplementation of Glutamate and GABA on memory performance and neurochemical profile in hippocampus of rats. Pak. J. Pharm. Sci. 2017, 30, 1013–1021. [Google Scholar]
- Bohme, G.A.; Bon, C.; Lemaire, M.; Reibaud, M.; Piot, O.; Stutzmann, J.M.; Doble, A.; Blanchard, J.C. Altered synaptic plasticity and memory formation in nitric oxide synthase inhibitor-treated rats. Proc. Natl. Acad. Sci. USA 1993, 90, 9191–9194. [Google Scholar] [CrossRef] [Green Version]
- Calabrese, V.; Mancuso, C.; Calvani, M.; Rizzarelli, E.; Butterfield, D.A.; Stella, A.M. Nitric oxide in the central nervous system: Neuroprotection versus neurotoxicity. Nat. Rev. Neurosci. 2007, 8, 766–775. [Google Scholar] [CrossRef]
- Cooke, J.P.; Dzau, V.J. Nitric oxide synthase: Role in the genesis of vascular disease. Annu. Rev. Med. 1997, 48, 489–509. [Google Scholar] [CrossRef] [Green Version]
- Colzato, L.S.; Jongkees, B.J.; Sellaro, R.; Hommel, B. Working memory reloaded: Tyrosine repletes updating in the N-back task. Front. Behav. Neurosci. 2013, 7, 200. [Google Scholar] [CrossRef] [Green Version]
- Shurtleff, D.; Thomas, J.R.; Schrot, J.; Kowalski, K.; Harford, R. Tyrosine reverses a cold-induced working memory deficit in humans. Pharmacol. Biochem. Behav. 1994, 47, 935–941. [Google Scholar] [CrossRef]
- Thomas, J.R.; Lockwood, P.A.; Singh, A.; Deuster, P.A. Tyrosine improves working memory in a multitasking environment. Pharmacol. Biochem. Behav. 1999, 64, 495–500. [Google Scholar] [CrossRef]
- Wechsler, D. WMS-III: Wechsler Memory Scale Administration and Scoring Manual; The Psychological Corporation: San Antonio, TX, USA, 1997. [Google Scholar]
- The Psychological Corporation. WAIS-III/WMS-III Technical Manual; Harcourt Brace & Company: San Antonio, TX, USA, 1997. [Google Scholar]
- Hua, M.-S.; Chang, B.-S.; Lin, K.-N.; Yang, C.-M.; Lu, L.H.-J.; Chen, H.-Y. Wechsler Memory Scale- III (Chinese Version): Administration and Scoring Manual; Chinese Behavioral Science Corporation: Taipei, Taiwan, 2005. [Google Scholar]
- Fray, P.J.; Robbins, T.W.; Sahakian, B.J. Neuropsychiatric applications of CANTAB. Int. J. Geriatr. Psych. 1996, 11, 329–336. [Google Scholar] [CrossRef]
- Cambridge Cognition. CANTAB. Available online: http://www.cambridgecognition.com/technology (accessed on 2 October 2019).
- Strauss, E.; Sherman, E.M.S.; Spreen, O. A Compendium of Neuropsychological Tests: Administration, Norms, and Commentary; Oxford University Press: New York, NY, USA, 2006. [Google Scholar]
- Gerhart, K.A.; Weitzenkamp, D.A.; Kennedy, P.; Glass, C.A.; Charlifue, S.W. Correlates of stress in long-term spinal cord injury. Spinal Cord. 1999, 37, 183–190. [Google Scholar] [CrossRef] [Green Version]
- Lu, M.-L.; Che, H.; Chang, S.W.; Shen, W.W. [Reliability and Validity of the Chinese Version of the Beck Depression Inventory-II]. Taiwan J. Psychiatry 2002, 16, 301–310. [Google Scholar]
- Huang, S.-L.; Hsieh, C.-L.; Wu, R.-M.; Lu, W.-S. Test-retest reliability and minimal detectable change of the Beck Depression Inventory and the Taiwan Geriatric Depression Scale in patients with Parkinson’s disease. PLoS ONE 2017, 12, e0184823. [Google Scholar] [CrossRef] [Green Version]
- Wang, K.-C.; Chung, F.-C. An Investigation of Multidimensional Factorial Validity of the Chinese Version of State-Trait Anxiety Inventory. Psychol. Test. 2016, 63, 287–313. [Google Scholar]
- Tsai, P.S.; Wang, S.Y.; Wang, M.Y.; Su, C.T.; Yang, T.T.; Huang, C.J.; Fang, S.C. Psychometric evaluation of the Chinese version of the Pittsburgh Sleep Quality Index (CPSQI) in primary insomnia and control subjects. Qual. Life Res. 2005, 14, 1943–1952. [Google Scholar] [CrossRef]
- Squires, N.K.; Squires, K.C.; Hillyard, S.A. Two varieties of long-latency positive waves evoked by unpredictable auditory stimuli in man. Electroencephalogr. Clin. Neurophysiol. 1975, 38, 387–401. [Google Scholar] [CrossRef]
- Linden, D.E. The p300: Where in the brain is it produced and what does it tell us? Neuroscientist 2005, 11, 563–576. [Google Scholar] [CrossRef]
- Portin, R.; Kovala, T.; Polo-Kantola, P.; Revonsuo, A.; Muller, K.; Matikainen, E. Does P3 reflect attentional or memory performances, or cognition more generally? Scand. J. Psychol. 2000, 41, 31–40. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liang, K.-Y.; Zeger, S.L. Longitudinal data analysis using generalized linear models. Biometrika 1986, 73, 13–22. [Google Scholar] [CrossRef]
- Reder, L.M.; Wible, C.; Martin, J. Differential memory changes with age: Exact retrieval versus plausible inference. J. Exp. Psychol. Learn. Mem. Cogn. 1986, 12, 72–81. [Google Scholar] [CrossRef]
- Toh, D.W.K.; Wong, C.H.; Fam, J.; Kim, J.E. Daily consumption of essence of chicken improves cognitive function: A systematically searched meta-analysis of randomized controlled trials. Nutr. Neurosci. 2019, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Johnson, W.; Logie, R.H.; Brockmole, J.R. Working memory tasks differ in factor structure across age cohorts: Implications for dedifferentiation. Intelligence 2010, 38, 513–528. [Google Scholar] [CrossRef] [Green Version]
- Baddeley, A. The episodic buffer: A new component of working memory? Trends Cogn. Sci. 2000, 4, 417–423. [Google Scholar] [CrossRef]
- Salthouse, T.A. The processing-speed theory of adult age differences in cognition. Psychol. Rev. 1996, 103, 403–428. [Google Scholar] [CrossRef] [Green Version]
- Goodin, D.S.; Squires, K.C.; Starr, A. Long latency event-related components of the auditory evoked potential in dementia. Brain 1978, 101, 635–648. [Google Scholar] [CrossRef] [Green Version]
- Parra, M.A.; Ascencio, L.L.; Urquina, H.F.; Manes, F.; Ibanez, A.M. P300 and neuropsychological assessment in mild cognitive impairment and Alzheimer dementia. Front. Neurol. 2012, 3, 172. [Google Scholar] [CrossRef] [Green Version]
- Kurihara, H.; Yao, X.-S.; Nagai, H.; Tsuruoka, N.; Shibata, H.; Kiso, Y.; Fukami, H. Anti-Stress Effect of BRAND’S Essence of Chicken (BEC) on Plasma Glucose Levels in Mice Loaded with Restraint Stress. J. Health Sci. 2006, 52, 252–258. [Google Scholar] [CrossRef] [Green Version]
- Terai, K.; Matsuo, A.; McGeer, P.L. Enhancement of immunoreactivity for NF-kappa B in the hippocampal formation and cerebral cortex of Alzheimer’s disease. Brain Res. 1996, 735, 159–168. [Google Scholar] [CrossRef]
- Wesnes, K.A. Moving beyond the pros and cons of automating cognitive testing in pathological aging and dementia: The case for equal opportunity. Alzheimers Res. Ther. 2014, 6, 58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leung, D.Y.; Lam, T.-H.; Chan, S.S. Three versions of Perceived Stress Scale: Validation in a sample of Chinese cardiac patients who smoke. BMC Public Health 2010, 10, 513. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables 1 | Total (N = 73) | ProBeptigen® (n = 37) | Placebo (n = 36) | p-Value |
|---|---|---|---|---|
| Demographics | ||||
| Age (year) | 42.38 ± 6.36 | 42.46 ± 6.36 | 42.31 ± 6.45 | 0.919 |
| Education (year) | 15.82 ± 1.77 | 15.62 ± 1.92 | 16.03 ± 1.59 | 0.328 |
| WMS-III 2 | ||||
| Logical Memory I | 11.16 ± 2.85 | 10.62 ± 3.14 | 11.72 ± 2.44 | 0.100 |
| Logical Memory I thematic score | 10.08 ± 3.27 | 9.54 ± 3.42 | 10.64 ± 3.05 | 0.153 |
| Logical Memory II | 11.03 ± 2.59 | 10.57 ± 2.75 | 11.50 ± 2.36 | 0.125 |
| Logical Memory II-thematic score | 9.90 ± 2.72 | 9.32 ± 2.64 | 10.50 ± 2.72 | 0.065 |
| Family Pictures I | 11.34 ± 3.00 | 10.70 ± 3.15 | 12.00 ± 2.72 | 0.064 |
| Family Pictures II | 11.27 ± 2.96 | 10.92 ± 3.09 | 11.64 ± 2.83 | 0.308 |
| Self-reported measures | ||||
| PSS | 28.07 ± 4.59 | 27.05 ± 3.64 | 29.11 ± 5.25 | 0.057 |
| BDI | 12.60 ± 8.41 | 11.24 ± 8.06 | 14.00 ± 8.64 | 0.163 |
| STAI-State | 32.01 ± 10.84 | 31.14 ± 10.15 | 32.92 ± 11.59 | 0.487 |
| STAI-Trait | 40.07 ± 8.04 | 38.30 ± 7.76 | 41.89 ± 8.03 | 0.056 |
| PSQI | 7.68 ± 3.63 | 7.43 ± 3.48 | 7.94 ± 3.81 | 0.550 |
| Event-related potentials | ||||
| P300-L (ms) | 381.60 ± 40.79 | 373.95 ± 41.10 | 389.47 ± 39.49 | 0.104 |
| P300-A (mV) | 7.00 ± 3.87 | 7.13 ± 3.99 | 6.87 ± 3.80 | 0.781 |
| Blood biochemistry | ||||
| ALT (IU/L) | 22.97 ± 15.96 | 25.14 ± 20.86 | 20.75 ± 8.13 | 0.240 |
| AST (IU/L) | 23.03 ± 9.79 | 25.14 ± 12.47 | 20.86 ± 5.25 | 0.061 |
| BUN (mg/dL) | 11.33 ± 3.40 | 11.41 ± 3.24 | 11.25 ± 3.60 | 0.847 |
| Cortisol (μg/dL) | 10.77 ± 3.51 | 10.96 ± 3.49 | 10.58 ± 3.56 | 0.645 |
| Creatinine (mg/dL) | 0.74 ± 0.16 | 0.76 ± 0.17 | 0.73 ± 0.15 | 0.342 |
| hs-CRP (mg/dL) | 0.16 ± 0.30 | 0.17 ± 0.34 | 0.15 ± 0.19 | 0.810 |
| eGFR (mL/min/1.73 m2) | 104.09 ± 18.60 | 100.39 ± 15.81 | 107.89 ± 20.63 | 0.085 |
| Glucose (mg/dL) | 97.32 ± 10.70 | 93.89 ± 9.13 | 100.83 ± 11.16 | 0.005 |
| T3 (ng/mL) | 1.07 ± 0.16 | 1.04 ± 0.17 | 1.10 ± 0.15 | 0.156 |
| Free T4 (ng/dL) | 0.87 ± 0.11 | 0.89 ± 0.11 | 0.85 ± 0.11 | 0.126 |
| TSH (μIU/mL) | 2.19 ± 1.28 | 2.23 ± 1.13 | 2.16 ± 1.44 | 0.822 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, D.; Yang, C.-C.; Chen, K.-Y.; Lin, Y.-C.; Wu, P.-J.; Hsieh, P.-H.; Nakao, Y.; Ow, M.Y.L.; Hsieh, Y.-C.; Hu, C.-J. Hydrolyzed Chicken Extract (ProBeptigen®) on Cognitive Function in Healthy Middle-Aged People: A Randomized Double-Blind Trial. Nutrients 2020, 12, 1362. https://doi.org/10.3390/nu12051362
Wu D, Yang C-C, Chen K-Y, Lin Y-C, Wu P-J, Hsieh P-H, Nakao Y, Ow MYL, Hsieh Y-C, Hu C-J. Hydrolyzed Chicken Extract (ProBeptigen®) on Cognitive Function in Healthy Middle-Aged People: A Randomized Double-Blind Trial. Nutrients. 2020; 12(5):1362. https://doi.org/10.3390/nu12051362
Chicago/Turabian StyleWu, Dean, Cheng-Chang Yang, Kuan-Yu Chen, Ying-Chin Lin, Pei-Jung Wu, Pei-Hsiu Hsieh, Yoshihiro Nakao, Mandy Y. L. Ow, Yi-Chen Hsieh, and Chaur-Jong Hu. 2020. "Hydrolyzed Chicken Extract (ProBeptigen®) on Cognitive Function in Healthy Middle-Aged People: A Randomized Double-Blind Trial" Nutrients 12, no. 5: 1362. https://doi.org/10.3390/nu12051362