Effect of Lupin-Enriched Biscuits as Substitute Mid-Meal Snacks on Post-Prandial Interstitial Glucose Excursions in Post-Surgical Hospital Patients with Type 2 Diabetes

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Participants
2.3. Intervention
2.4. Nutrient Composition and Ingredients in the Study Biscuits
2.5. Socio-Demographic and Medical History Data
2.6. Adherence to Biscuit Intervention and Plate Wastage
2.7. Anthropometric Measurements
2.8. Rating Hunger, Fullness and Palatability
2.9. Bowel Function
2.10. Continuous Glucose Monitoring
2.11. Statistical Analysis
3. Results
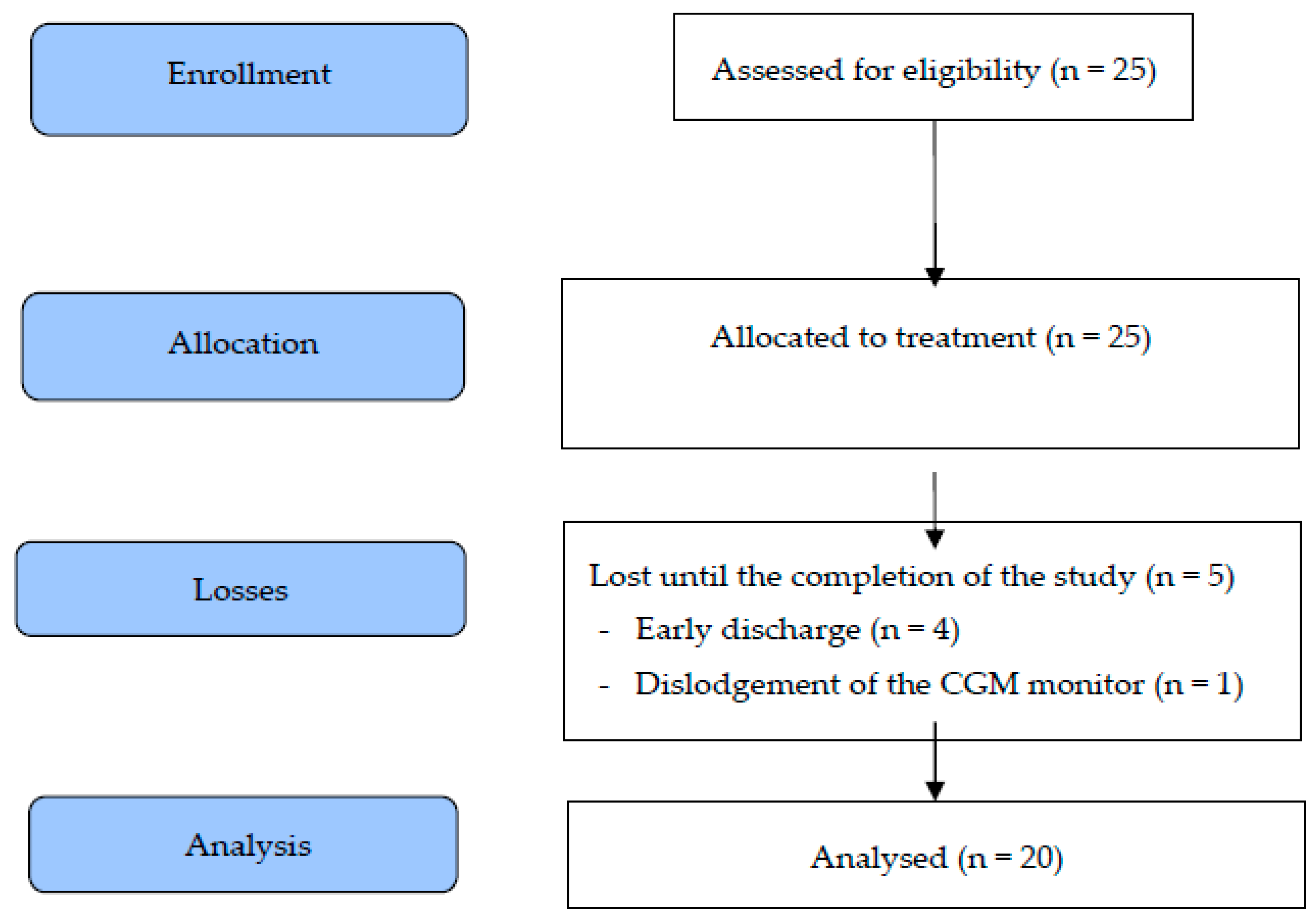
3.1. Participant Study Flow and Baseline Characteristics of the Pilot Study Cohort
3.2. Satiety and Palatability and Visual Appeal Properties of the Biscuit Treatments
3.3. Adherence to Biscuit Regime and Total Carbohydrate Intake
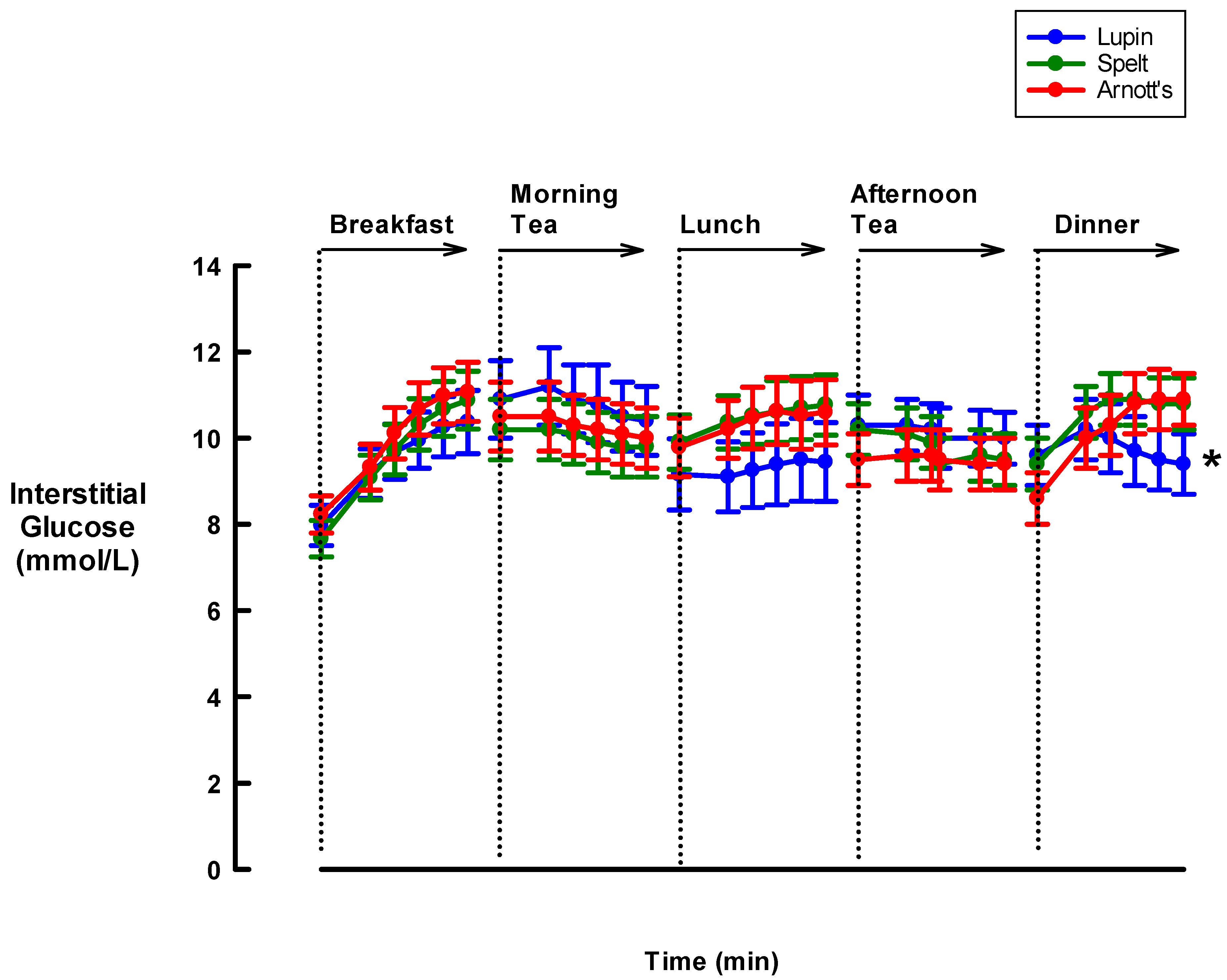
3.4. Effect of Biscuits on Interstitial Glucose Levels
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Australian Bureau of Statistics. National Health Survey: First Results, 2017–2018; Australian Bureau of Statistics: Canberra, Australia, 2017.
- Abouzeid, M.; Philpot, B.; Janus, E.D.; Coates, M.J.; Dunbar, J. Type 2 diabetes prevalence varies by socio-economic status within and between migrant groups: Analysis and implications for Australia. BMC Public Health 2013, 13, 252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bach, L.; Ekinci, E.I.; Engler, D.; Gilfillan, C.; Hamblin, P.S.; MacIsaac, R.J.; Soldatos, G.; Steele, C.; Ward, G.M.; Wyatt, S. The high burden of inpatient diabetes mellitus: The Melbourne Public Hospitals Diabetes Inpatient Audit. Med. J. Aust. 2014, 201, 334–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akiboye, F.; Rayman, G. Management of Hyperglycemia and Diabetes in Orthopedic Surgery. Curr. Diabetes Rep. 2017, 17, 13. [Google Scholar] [CrossRef] [Green Version]
- Browne, J.A.; Cook, C.; Pietrobon, R.; Bethel, M.A.; Richardson, W. Diabetes and Early Postoperative Outcomes Following Lumbar Fusion. Spine 2007, 32, 2214–2219. [Google Scholar] [CrossRef] [PubMed]
- Schipper, O.N.; Jiang, J.J.; Chen, L.; Koh, J.; Toolan, B.C. Effect of Diabetes Mellitus on Perioperative Complications and Hospital Outcomes After Ankle Arthrodesis and Total Ankle Arthroplasty. Foot Ankle Int. 2014, 36, 258–267. [Google Scholar] [CrossRef]
- Toor, A.S.; Jiang, J.J.; Shi, L.L.; Koh, J. Comparison of perioperative complications after total elbow arthroplasty in patients with and without diabetes. J. Shoulder Elb. Surg. 2014, 23, 1599–1606. [Google Scholar] [CrossRef]
- Turina, M.; Fry, D.; Polk, H.C. Acute hyperglycemia and the innate immune system: Clinical, cellular, and molecular aspects. Crit. Care Med. 2005, 33, 1624–1633. [Google Scholar] [CrossRef]
- ACI Nutrition Network. Nutrition Standard for Adult Inpatients in NSW Hospitals; Agency for Clinical Innovation: Chatswood, Australia, 2011.
- ACI Nutrition Network. ACI Diet Specifications for Adult Inpatients–Diabetes–Standard; Agency for Clinical Innovation: Chatswood, Australia, 2016.
- Tay, J.; Luscombe-Marsh, N.D.; Thompson, C.H.; Noakes, M.; Buckley, J.D.; Wittert, G.A.; Yancy, W.S.; Brinkworth, G.D.; Buckley, J.D. A Very Low-Carbohydrate, Low–Saturated Fat Diet for Type 2 Diabetes Management: A Randomized Trial. Diabetes Care 2014, 37, 2909–2918. [Google Scholar] [CrossRef] [Green Version]
- Kirk, J.K.; Graves, D.E.; Craven, T.E.; Lipkin, E.W.; Austin, M.; Margolis, K. Restricted-Carbohydrate Diets in Patients with Type 2 Diabetes: A Meta-Analysis. J. Am. Diet. Assoc. 2008, 108, 91–100. [Google Scholar] [CrossRef]
- Meng, Y.; Bai, H.; Wang, S.; Li, Z.; Wang, Q.; Chen, L. Efficacy of low carbohydrate diet for type 2 diabetes mellitus management: A systematic review and meta-analysis of randomized controlled trials. Diabetes Res. Clin. Pract. 2017, 131, 124–131. [Google Scholar] [CrossRef]
- Sainsbury, E.; Kizirian, N.V.; Partridge, S.R.; Gill, T.; Colagiuri, S.; Gibson, A.A. Effect of dietary carbohydrate restriction on glycemic control in adults with diabetes: A systematic review and meta-analysis. Diabetes Res. Clin. Pract. 2018, 139, 239–252. [Google Scholar] [CrossRef] [PubMed]
- Snorgaard, O.; Poulsen, G.M.; Andersen, H.K.; Astrup, A. Systematic review and meta-analysis of dietary carbohydrate restriction in patients with type 2 diabetes. BMJ Open Diabetes Res. Care 2017, 5, e000354. [Google Scholar] [CrossRef] [PubMed]
- Department of Human Services (Victoria). Nutrition Standards for Menu Items in Victorian Hospitals and Residential Aged Care Facilities; Department of Human Services: Melbourne, Australia, 2009.
- Kouris-Blazos, A.; Belski, R. Health benefits of legumes and pulses with a focus on Australian sweet lupins. Asia Pac. J. Clin. Nutr. 2016, 25, 1–17. [Google Scholar] [PubMed]
- Jenkins, D.J.; Wolever, T.M.; Taylor, R.H.; Griffiths, C.; Krzemińska, K.; Lawrie, J.A.; Bennett, C.M.; Goff, D.V.; Sarson, D.L.; Bloom, S.R. Slow release dietary carbohydrate improves second meal tolerance. Am. J. Clin. Nutr. 1982, 35, 1339–1346. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J. Whole Grains, Legumes, and the Subsequent Meal Effect: Implications for Blood Glucose Control and the Role of Fermentation. J. Nutr. Metab. 2011, 2012, 1–7. [Google Scholar] [CrossRef]
- Winham, D.M.; Hutchins, A.; Thompson, S.V. Glycemic Response to Black Beans and Chickpeas as Part of a Rice Meal: A Randomized Cross-Over Trial. Nutrients 2017, 9, 1095. [Google Scholar] [CrossRef] [Green Version]
- Flint, A.; Raben, A.; Blundell, J.; Astrup, A. Reproducibility, power and validity of visual analogue scales in assessment of appetite sensations in single test meal studies. Int. J. Obes. 2000, 24, 38–48. [Google Scholar] [CrossRef] [Green Version]
- Blake, M.R.; Raker, J.M.; Whelan, K. Validity and reliability of the Bristol Stool Form Scale in healthy adults and patients with diarrhoea-predominant irritable bowel syndrome. Aliment. Pharmacol. Ther. 2016, 44, 693–703. [Google Scholar] [CrossRef] [Green Version]
- Poolsup, N.; Suksomboon, N.; Kyaw, A.M. Systematic review and meta-analysis of the effectiveness of continuous glucose monitoring (CGM) on glucose control in diabetes. Diabetol. Metab. Syndr. 2013, 5, 39. [Google Scholar] [CrossRef] [Green Version]
- Kerr, D.; Fayers, K. Continuous real-time glucose monitoring systems: Time for a closer look. Pract. Diabetes Int. 2008, 25, 37–41. [Google Scholar] [CrossRef]
- Maran, A.; Crepaldi, C.; Tiengo, A.; Grassi, G.; Vitali, E.; Pagano, G.; Bistoni, S.; Calabrese, G.; Santeusanio, F.; Leonetti, F.; et al. Continuous subcutaneous glucose monitoring in diabetic patients: A multicenter analysis. Diabetes Care 2002, 25, 347–352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mollard, R.; Wong, C.L.; Luhovyy, B.L.; Anderson, G.H. First and second meal effects of pulses on blood glucose, appetite, and food intake at a later meal. Appl. Physiol. Nutr. Metab. 2011, 36, 634–642. [Google Scholar] [CrossRef] [PubMed]
- Hall, R.S.; Thomas, S.J.; Johnson, S.K. Australian sweet lupin flour addition reduces the glycaemic index of a white bread breakfast without affecting palatability in healthy human volunteers. Asia Pac. J. Clin. Nutr. 2005, 14, 91–97. [Google Scholar] [PubMed]
- Hodgson, J.M.; Lee, Y.P.; Puddey, I.B.; Sipsas, S.; Ackland, T.; Beilin, L.J.; Belski, R.; Mori, T.A. Effects of increasing dietary protein and fibre intake with lupin on body weight and composition and blood lipids in overweight men and women. Int. J. Obes. 2010, 34, 1086–1094. [Google Scholar] [CrossRef] [Green Version]
- Dove, E.R.; Mori, T.A.; Chew, G.T.; Barden, A.E.; Woodman, R.J.; Puddey, I.B.; Sipsas, S.; Hodgson, J.M. Lupin and soya reduce glycaemia acutely in type 2 diabetes. Br. J. Nutr. 2011, 106, 1045–1051. [Google Scholar] [CrossRef]
- Lee, Y.P.; Mori, T.; Sipsas, S.; Barden, A.; Puddey, I.; Burke, V.; Hall, R.S.; Hodgson, J.M. Lupin-enriched bread increases satiety and reduces energy intake acutely. Am. J. Clin. Nutr. 2006, 84, 975–980. [Google Scholar] [CrossRef] [Green Version]
- Welch, R.W.; Antoine, J.M.; Berta, J.L.; Bub, A.; de Vries, J.; Guarner, F.; Hasselwander, O.; Hendriks, H.; Jakel, M.; Koletzko, B.V.; et al. Guidelines for the design, conduct and reporting of human intervention studies to evaluate the health benefits of foods. Br. J. Nutr. 2011, 106 (Suppl. 2), S3–S15. [Google Scholar] [CrossRef]
- Brighenti, F.; Benini, L.; del Rio, D.; Casiraghi, C.; Pellegrini, N.; Scazzina, F.; Jenkins, D.J.; Vantini, I. Colonic fermentation of indigestible carbohydrates contributes to the second-meal effect. Am. J. Clin. Nutr. 2006, 83, 817–822. [Google Scholar] [CrossRef] [Green Version]
- Pingitore, A.; Chambers, E.S.; Hill, T.; Maldonado, I.R.; Liu, B.; Bewick, G.; Morrison, D.J.; Preston, T.; Wallis, G.A.; Tedford, C.; et al. The diet-derived short chain fatty acid propionate improves beta-cell function in humans and stimulates insulin secretion from human islets in vitro. Diabetes. Obes. Metab. 2017, 19, 257–265. [Google Scholar] [CrossRef] [Green Version]
- Ropert, A.; Cherbut, C.; Roze, C.; le Quellec, A.; Holst, J.J.; Fu-Cheng, X.; Varannes, S.B.d.; Galmiche, J.P. Colonic fermentation and proximal gastric tone in humans. Gastroenterology 1996, 111, 289–296. [Google Scholar] [CrossRef]
- Sievenpiper, J.L.; Kendall, C.W.C.; Esfahani, A.; Wong, J.M.W.; Carleton, A.J.; Jiang, H.Y.; Bazinet, R.P.; Vidgen, E.; Jenkins, D.J.A. Effect of non-oil-seed pulses on glycaemic control: A systematic review and meta-analysis of randomised controlled experimental trials in people with and without diabetes. Diabetologia 2009, 52, 1479–1495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dagogo-Jack, S. Preventing diabetes-related morbidity and mortality in the primary care setting. J. Natl. Med. Assoc. 2002, 94, 549–560. [Google Scholar] [PubMed]
- Chrastil, J.; Anderson, M.; Stevens, V.; Anand, R.; Peters, C.L.; Pelt, C.E. Is Hemoglobin A1c or Perioperative Hyperglycemia Predictive of Periprosthetic Joint Infection or Death Following Primary Total Joint Arthroplasty? J. Arthroplast. 2015, 30, 1197–1202. [Google Scholar] [CrossRef] [PubMed]
- Mraovic, B.; Suh, D.; Jacovides, C.; Parvizi, J. Perioperative Hyperglycemia and Postoperative Infection after Lower Limb Arthroplasty. J. Diabetes Sci. Technol. 2011, 5, 412–418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tonks, K.T.; Jones, G.R.; McGeechan, K.; Campbell, L.V. Hyperglycaemia in hospital inpatients: Still a sticky situation. Intern. Med. J. 2010, 40, 521–526. [Google Scholar] [CrossRef]
- Boden, G.; Sargrad, K.; Homko, C.; Mozzoli, M.; Stein, T.P. Effect of a low-carbohydrate diet on appetite, blood glucose levels, and insulin resistance in obese patients with type 2 diabetes. Ann. Intern. Med. 2005, 142, 403–411. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Nutrient Content | Lupin Biscuits (100 g) (Skinnybik™) | Spelt Biscuits (100 g) (Skinnybik™) | Marie Biscuits (100 g) * (Arnott’s™) | |||
|---|---|---|---|---|---|---|
| 100 g | 30 g (2 Biscuits) | 100 g | 30 g (2 Biscuits) | 100 g | 16 g (2 Biscuits) | |
| Energy (kJ) | 1590 | 477 | 1590 | 477 | 1850 | 277 |
| Protein (g) | 12.9 | 3.9 | 10.0 | 3.0 | 6.6 | 1.0 |
| Total fat (g) | 14.9 | 4.4 | 15.4 | 4.6 | 11.9 | 1.9 |
| Saturated fat (g) | 1.6 | 0.5 | 1.8 | 0.6 | 5.9 | 0.9 |
| Total carbohydrate (g) | 36.0 | 10.8 | 36.0 | 10.8 | 75.0 | 12.0 |
| Sugar (g) | 14.9 | 4.5 | 14.0 | 4.2 | 21.3 | 3.4 |
| Fibre (g) | 10.0 | 3.0 | 10.0 | 3.0 | 2.8 | 0.4 |
| Sodium (mg) | 200 | 60 | 114 | 34 | 192 | 30 |
| Descriptor | Total Sample (n = 20) |
|---|---|
| Mean (SD) | |
| Age (years) | 74.3 (11.7) |
| Height (cm) | 164.4 (7.4) |
| Weight (kg) | 82.5 (15.6) |
| BMI (kg/m2) | 30.7 (4.5) |
| Gender | N (%) |
| Female | 8 (40) |
| Male | 12 (60) |
| Ethnicity | |
| Australian | 14 (70) |
| Non-Australian | 6 (30) |
| Medication | |
| Combined Hypoglycaemic Treatment | 7 (35) |
| Biguanides | 11 (55) |
| DPP-4 Inhibitors | 1 (5) |
| Sulphonylureas | 1 (5) |
| Categories of Surgery | |
| Orthopaedic | 6 (30) |
| Gastrointestinal | 4 (20) |
| Cardiac | 9 (45) |
| Urogenital | 1 (5) |
| Weight Status | |
| Normal weight (BMI, 18.5–25 kg/m2) | 3 (15) |
| Overweight BMI, 25–30 kg/m2) | 5 (25) |
| Obese (BMI > 30 kg/m2) | 12 (60) |
| Lupin Skinnybik™ (n = 19) | Spelt Skinnybik™ (n = 19) | Marie Arnott’s™ (n = 18) | ||
|---|---|---|---|---|
| Satiety | n (%) | n (%) | n (%) | p-Value † |
| Hunger (“How hungry do you feel?”) | ||||
| Before Breakfast | ||||
| Not at all/somewhat | 13 (68.1) | 15 (78.9) | 13 (72.2) | 0.745 |
| Neutral | 3 (15.8) | 3 (15.8) | 4 (22.2) | |
| Mostly | 3 (15.8) | 1 (5.3) | 1 (5.6) | |
| Before Lunch | ||||
| Not at all/somewhat | 15 (78.9) | 11 (57.9) | 15 (83.3) | 0.444 |
| Neutral | 3 (15.8) | 5 (26.3) | 2 (11.1) | |
| Mostly | 1 (5.2) | 3 (15.8) | 1 (5.6) | |
| Before Dinner | ||||
| Not at all/somewhat | 15 (78.9) | 15 (78.9) | 13 (72.2) | 0.249 |
| Neutral | 2 (10.5) | 4 (21.0) | 5 (27.8) | |
| Mostly | 2 (10.5) | 0 (0.0) | 0 (0.0) | |
| Fullness (“How full do you feel?”) | ||||
| Before Breakfast | ||||
| Not at all/somewhat | 9 (47.4) | 12 (63.2) | 9 (50.0) | 0.451 |
| Neutral | 6 (31.6) | 4 (21.1) | 8 (44.4) | |
| Mostly | 4 (21.1) | 3 (15.8) | 1 (5.6) | |
| Before Lunch | ||||
| Not at all/somewhat | 11 (57.9) | 10 (52.6) | 8 (44.4) | 0.155 |
| Neutral | 3 (15.8) | 7 (36.8) | 9 (50.0) | |
| Mostly | 5 (26.3) | 2 (10.5) | 1 (5.6) | |
| Before Dinner | ||||
| Not at all/somewhat | 10 (52.6) | 10 (52.6) | 9 (50) | 0.018 |
| Neutral | 2 (10.5) | 8 (42.1) | 8 (44.4) | |
| Mostly | 7 (36.8) | 1 (5.3) | 1 (5.6) | |
| Visual appeal of biscuits | ||||
| Good | 5 (26.3) | 3 (15.8) | 14 (77.8) | 0.001 |
| Neutral | 14 (73.7) | 15 (78.9) | 4 (22.2) | |
| Bad | 0 (0.0) | 1 (5.3) | 0 (0.0) | |
| Palatability of biscuits | ||||
| Good | 4 (21.1) | 0 (0.0) | 15 (83.3) | 0.001 |
| Neutral | 13 (68.4) | 19 (100.0) | 3 (16.7) | |
| Bad | 2 (10.5) | 0 (0.0) | 0 (0.0) | |
| Bowel Function (Based on Bristol Stool Chart) | ||||
| Constipation | 5 (26.3) | 3 (15) | 3 (15.8) | 0.777 |
| Normal | 14 (73.7) | 15 (78.9) | 15 (78.9) | |
| Loose Bowels | 0 (0.0) | 1 (5.3) | 1 (5.3) | |
| Lupin Skinnybik™ * (n = 20) | Spelt Skinnybik™ * (n = 20) | Marie Arnott’s™ * (n = 20) | ||
|---|---|---|---|---|
| Mean (SD) | Mean (SD) | Mean (SD) | p-Value † | |
| Adherence (Grams of Biscuit Consumed) | ||||
| Morning Tea | 27.1 (3.1) | 17.2 (3.5) | 7.0 (2.4) | <0.001 |
| Afternoon Tea | 27.1 (3.1) | 19.7 (3.4) | 7.5 (2.5) | <0.001 |
| Total Amount of Carbohydrate Consumed (Grams per Main Meal or Mid-Meal) | ||||
| Breakfast | 41.2 (6.7) | 30.2 (9.8) | 28.5 (10.8) | <0.001 |
| Morning Tea | 9.3 (1.1) | 6.1 (2.7) | 5.2 (1.8) | <0.001 |
| Lunch | 39.2 (9.5) | 21.8 (4.9) | 19.2 (7.1) | <0.001 |
| Afternoon Tea | 9.3 (1.1) | 7.1 (5.6) | 5.6 (4.1) | <0.001 |
| Dinner | 39.2 (8.1) | 25.0 (10.1) | 22.5 (9.7) | <0.001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Skalkos, S.; Moschonis, G.; Thomas, C.J.; McMillan, J.; Kouris-Blazos, A. Effect of Lupin-Enriched Biscuits as Substitute Mid-Meal Snacks on Post-Prandial Interstitial Glucose Excursions in Post-Surgical Hospital Patients with Type 2 Diabetes. Nutrients 2020, 12, 1239. https://doi.org/10.3390/nu12051239
Skalkos S, Moschonis G, Thomas CJ, McMillan J, Kouris-Blazos A. Effect of Lupin-Enriched Biscuits as Substitute Mid-Meal Snacks on Post-Prandial Interstitial Glucose Excursions in Post-Surgical Hospital Patients with Type 2 Diabetes. Nutrients. 2020; 12(5):1239. https://doi.org/10.3390/nu12051239
Chicago/Turabian StyleSkalkos, Sophie, George Moschonis, Colleen J. Thomas, Joanna McMillan, and Antigone Kouris-Blazos. 2020. "Effect of Lupin-Enriched Biscuits as Substitute Mid-Meal Snacks on Post-Prandial Interstitial Glucose Excursions in Post-Surgical Hospital Patients with Type 2 Diabetes" Nutrients 12, no. 5: 1239. https://doi.org/10.3390/nu12051239