Salt Taste Genotype, Dietary Habits and Biomarkers of Health: No Associations in an Elderly Cohort

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Anthropometric Measures
2.3. Blood Pressure Readings
2.4. Collection of Biological Samples
2.5. Genotyping
2.6. Dietary Assessment
2.7. Medical History and Medication Status
2.8. Statistical Analysis
3. Results
3.1. Participant Characteristics
3.2. Genotype Distributions
3.3. Sodium Intake by Genotype
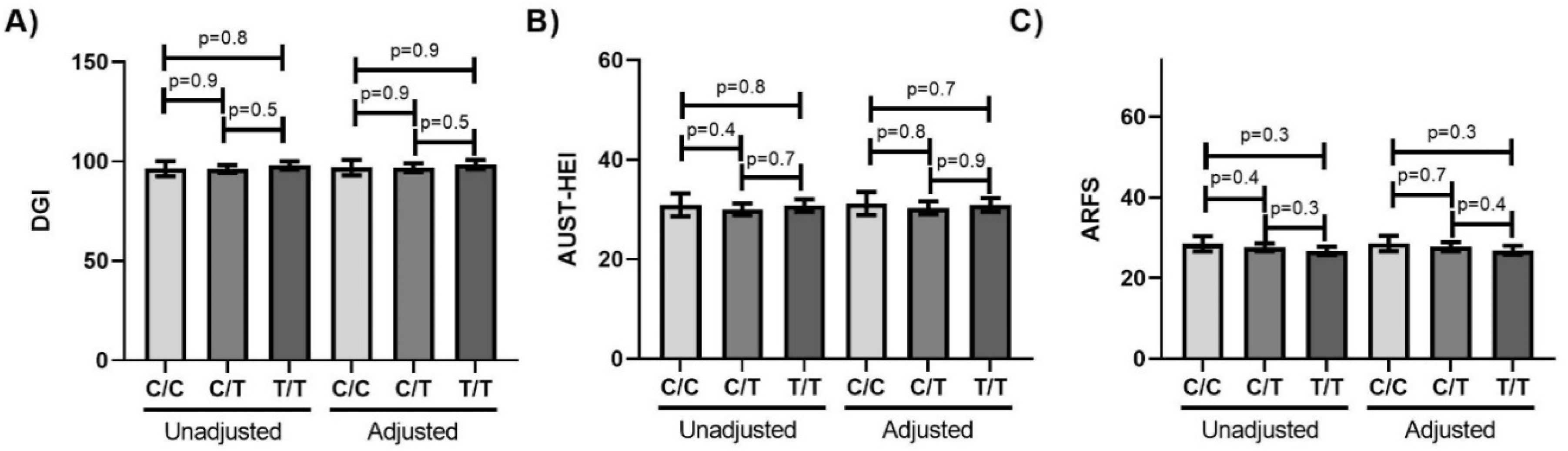
3.4. Diet Quality by Genotype
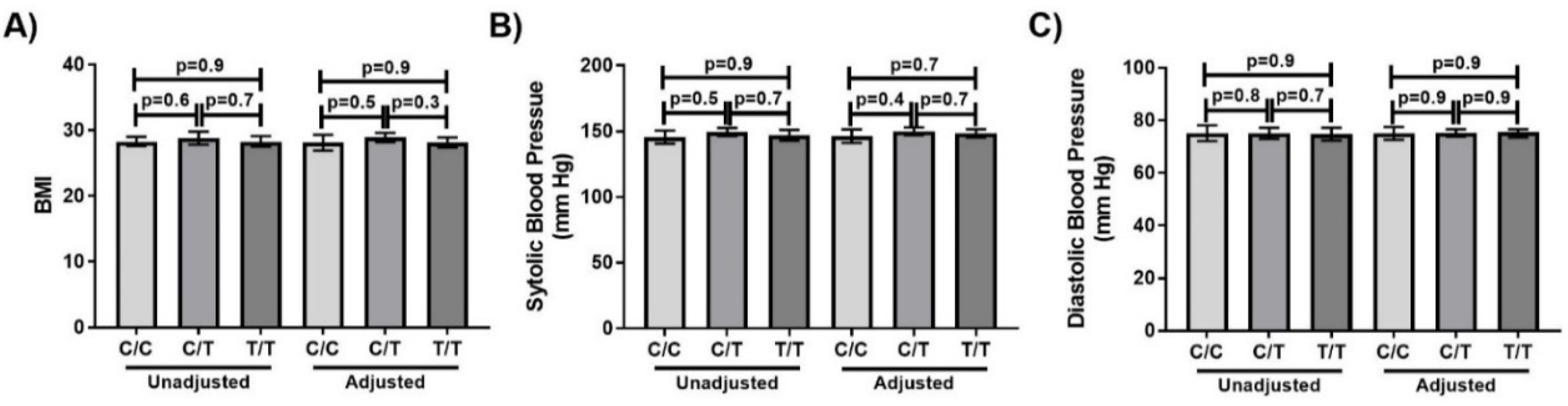
3.5. Markers of Health by Genotype
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Australian Bureau of Statistics. Twenty Years of Population Change; ABS: Canberra, Australia, 2019. Available online: https://www.abs.gov.au/ausstats/[email protected]/0/1CD2B1952AFC5E7ACA257298000F2E76 (accessed on 2 February 2020).
- Australian Institute of Health and Welfare. Nutrition Across the Life Stages; AIHW: Canberra, Australia, 2018. Available online: https://www.aihw.gov.au/getmedia/fc5ad42e-08f5-4f9a-9ca4-723cacaa510d/aihw-phe-227.pdf.aspx?inline=true (accessed on 21 January 2020).
- Strazzullo, P.; D’Elia, L.; Kandala, N.-B.; Cappuccio, F.P. Salt intake, stroke, and cardiovascular disease: Meta-analysis of prospective studies. BMJ 2009, 339, b4567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frassetto, L.A.; Morris, R.C., Jr.; Sellmeyer, D.E.; Sebastian, A. Adverse effects of sodium chloride on bone in the aging human population resulting from habitual consumption of typical American diets. J. Nutr. 2008, 138, 419S–422S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, W.G.; Chen, C.B.; Wang, Z.X.; Liu, Y.P.; Wen, X.Y.; Zhang, S.F.; Sun, T.W. A case-control study on the relationship between salt intake and salty taste and risk of gastric cancer. World J. Gastroenterol. 2011, 17, 2049–2053. [Google Scholar] [CrossRef] [PubMed]
- Thout, S.R.; Santos, J.A.; McKenzie, B.; Trieu, K.; Johnson, C.; McLean, R.; Arcand, J.; Campbell, N.R.C.; Webster, J. The science of salt: Updating the evidence on global estimates of salt intake. J. Clin. Hypertens. 2019, 21, 710–721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garcia-Bailo, B.; Toguri, C.; Eny, K.M.; El-Sohemy, A. Genetic variation in taste and its influence on food selection. J. Int. Biol. 2008, 13, 69–80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chamoun, E.; Mutch, D.M.; Allen-Vercoe, E.; Buchholz, A.C.; Duncan, A.M.; Spriet, L.L.; Haines, J.; Ma, D.W.L. A review of the associations between single nucleotide polymorphisms in taste receptors, eating behaviors, and health. Crit. Rev. Food Sci. Nutr. 2018, 58, 194–207. [Google Scholar] [CrossRef] [Green Version]
- Dias, A.G.; Rousseau, D.; Duizer, L.; Cockburn, M.; Chiu, W.; Nielsen, D.; El-Sohemy, A. Genetic variation in putative salt taste receptors and salt taste perception in humans. Chem. Sens. 2012, 38, 137–145. [Google Scholar] [CrossRef]
- Pilic, L.; Mavrommatis, Y. Genetic predisposition to salt-sensitive normotension and its effects on salt taste perception and intake. Br. J. Nutr. 2018, 120, 721–731. [Google Scholar] [CrossRef] [Green Version]
- Roper, S.D. The taste of table salt. Euro. J. Phys. 2015, 467, 457–463. [Google Scholar] [CrossRef] [Green Version]
- Desimone, J.A.; Lyall, V. Taste receptors in the gastrointestinal tract III. Salty and sour taste: Sensing of sodium and protons by the tongue. Am. J. Physiol. Gastro. Liver. Physiol. 2006, 291, G1005–G1010. [Google Scholar] [CrossRef]
- National Center for Biotechnology Information. Database of Single Nucleotide Polymorphisms (dbSNP). Available online: https://www.ncbi.nlm.nih.gov/snp/ (accessed on 7 January 2019).
- Uhlén, M.; Fagerberg, L.; Hallström, B.M.; Lindskog, C.; Oksvold, P.; Mardinoglu, A.; Sivertsson, Å.; Kampf, C.; Sjöstedt, E.; Asplund, A.; et al. Tissue-based map of the human proteome. Science 2015, 347, 1260419. [Google Scholar] [CrossRef] [PubMed]
- Oka, Y.; Butnaru, M.; von Buchholtz, L.; Ryba, N.J.; Zuker, C.S. High salt recruits aversive taste pathways. Nature 2013, 494, 472–475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cantero-Recasens, G.; Gonzalez, J.R.; Fandos, C.; Duran-Tauleria, E.; Smit, L.A.M.; Kauffmann, F.; Antó, J.M.; Valverde, M.A. Loss of function of transient receptor potential vanilloid 1 (TRPV1) genetic variant is associated with lower risk of active childhood asthma. J. Biol. Chem. 2010, 285, 27532–27535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spradley, F.T.; Pollock, D.M.; Pollock, J.S. Dahl salt-sensitive rats on a high-fat diet develop hypertension and enhanced constriction to angiotensin II without changing endothelial-dependent vasorelaxation. FASEB J. 2010, 24, 1025–1029. [Google Scholar] [CrossRef]
- Chamoun, E.; Carroll, N.; Duizer, L.; Qi, W.; Feng, Z.; Darlington, G.; Duncan, A.; Haines, J.; Ma, D. The relationship between single nucleotide polymorphisms in taste receptor genes, taste function and dietary intake in preschool-aged children and adults in the Guelph family health study. Nutrients 2018, 10, 990. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, S.; Zhang, X.; Lee, N.R.; Jin, H.S. TRPV1 gene polymorphisms are associated with Type 2 Diabetes by their interaction with fat consumption in the Korean genome epidemiology study. J. Nutrigenet. Nutrigenom. 2016, 9, 47–61. [Google Scholar] [CrossRef]
- Er, L.-K.; Teng, M.-S.; Wu, S.; Hsu, L.-A.; Tzeng, I.S.; Cheng, C.-F.; Chang, H.-I.; Chou, H.-H.; Ko, Y.-L. Combined effect of acid-sensing ion channel 3 and transient receptor potential vanilloid 1 gene polymorphisms on blood pressure variations in Taiwanese. Ci Ji Yi Xue Za Zhi 2018, 30, 29–36. [Google Scholar] [CrossRef]
- Valdes, A.M.; De Wilde, G.; Doherty, S.A.; Lories, R.J.; Vaughn, F.L.; Laslett, L.L.; Maciewicz, R.A.; Soni, A.; Hart, D.J.; Zhang, W.; et al. The Ile585Val TRPV1 variant is involved in risk of painful knee osteoarthritis. Ann. Rheum. Dis. 2011, 70, 1556–1561. [Google Scholar] [CrossRef]
- Smit, L.A.; Kogevinas, M.; Anto, J.M.; Bouzigon, E.; Gonzalez, J.R.; Le Moual, N.; Kromhout, H.; Carsin, A.E.; Pin, I.; Jarvis, D.; et al. Transient receptor potential genes, smoking, occupational exposures and cough in adults. Respir. Res. 2012, 13, 26. [Google Scholar] [CrossRef] [Green Version]
- Binder, A.; May, D.; Baron, R.; Maier, C.; Tolle, T.R.; Treede, R.D.; Berthele, A.; Faltraco, F.; Flor, H.; Gierthmuhlen, J.; et al. Transient receptor potential channel polymorphisms are associated with the somatosensory function in neuropathic pain patients. PLoS ONE 2011, 6, e17387. [Google Scholar] [CrossRef]
- Kim, H.; Neubert, J.K.; San Miguel, A.; Xu, K.; Krishnaraju, R.K.; Iadarola, M.J.; Goldman, D.; Dionne, R.A. Genetic influence on variability in human acute experimental pain sensitivity associated with gender, ethnicity and psychological temperament. Pain 2004, 109, 488–496. [Google Scholar] [CrossRef] [PubMed]
- Beckett, E.L.; Duesing, K.; Martin, C.; Jones, P.; Furst, J.; King, K.; Niblett, S.; Yates, Z.; Veysey, M.; Lucock, M. Relationship between methylation status of vitamin D-related genes, vitamin D levels, and methyl-donor biochemistry. J. Nutri. Intemed. Met. 2016, 6, 8–15. [Google Scholar] [CrossRef] [Green Version]
- Travers, C.; Dixon, A.; Laurence, A.; Niblett, S.; King, K.; Lewis, P.; Owen, N.; Veysey, M. Retirement Health and Lifestyle Study: Australian neighborhood environments and physical activity in older adults. Environ. Beh. 2018, 50, 426–453. [Google Scholar] [CrossRef]
- Beckett, E.L.; Martin, C.; Boyd, L.; Porter, T.; King, K.; Niblett, S.; Yates, Z.; Veysey, M.; Lucock, M. Reduced plasma homocysteine levels in elderly Australians following mandatory folic acid fortification—A comparison of two cross-sectional cohorts. J. Nutri. Intermed. Met. 2017, 8, 14–20. [Google Scholar] [CrossRef]
- Marfell-Jones, M.; Norton, K.; Carter, L.; Olds, T. International Standards for Anthropometric Assessment; International Society for the Advancement of Kinanthropometry: South Australia, 2001. Available online: https://docplayer.net/25335980-International-standards-for-anthropometric-assessment.html (accessed on 28 January 2020).
- QIAGEN. QIAamp® DNA Mini and Blood Mini Handbook, 3rd ed. 2012. Available online: https://www.qiagen.com/au/resources/resourcedetail?id=62a200d6-faf4-469b-b50f-2b59cf738962&lang=en (accessed on 18 February 2020).
- ThermoFisher Scientific. QuantStudio 7 Flex Real-Time PCR System. Available online: https://www.thermofisher.com/au/en/home/life-science/pcr/real-time-pcr/real-time-pcr-instruments/quantstudio-7-flex-real-time-pcr-system.html?icid=QuantStudioqPCRFamily-QuantStudio7flex-100915-IPAC (accessed on 23 January 2020).
- Duffy, V.B.; Hayes, J.E.; Davidson, A.C.; Kidd, J.R.; Kidd, K.K.; Bartoshuk, L.M. Vegetable intake in college-aged adults Is explained by oral sensory phenotypes and TAS2R38 genotype. Chemosens. Percept. 2010, 3, 137–148. [Google Scholar] [CrossRef] [Green Version]
- Xyris Software. FoodWorks, Brisbane, QLD, Australia. 2019. Available online: https://xyris.com.au (accessed on 18 February 2020).
- McNaughton, S.A.; Ball, K.; Crawford, D.; Mishra, G.D. An index of diet and eating patterns is a valid measure of diet quality in an Australian population. J. Nutr. 2008, 138, 86–93. [Google Scholar] [CrossRef] [Green Version]
- Collins, C.E.; Young, A.F.; Hodge, A. Diet quality is associated with higher nutrient intake and self-rated health in mid-aged women. J. Am. Col. Nutr. 2008, 27, 146–157. [Google Scholar] [CrossRef]
- Collins, C.E.; Burrows, T.L.; Rollo, M.E.; Boggess, M.M.; Watson, J.F.; Guest, M.; Duncanson, K.; Pezdirc, K.; Hutchesson, M.J. The comparative validity and reproducibility of a diet quality index for adults: The Australian Recommended Food Score. Nutrients 2015, 7, 785–798. [Google Scholar] [CrossRef] [Green Version]
- Australian Institute of Health and Welfare. Australian Diet Quality index Project. Available online: https://www.aihw.gov.au/getmedia/2b8340a0-b694-4eb6-b5c2-21419e06fa49/adqip.pdf.aspx?inline=true (accessed on 27 January 2020).
- Wiltgren, A.R.; Booth, A.O.; Kaur, G.; Cicerale, S.; Lacy, K.E.; Thorpe, M.G.; Keast, R.S.; Riddell, L.J. Micronutrient supplement use and diet quality in university students. Nutrients 2015, 7, 1094–1107. [Google Scholar] [CrossRef]
- National Health and Medical Research Council. Eat for Health. Australian Dietary Guidelines; NHMRC: Canberra, Australia, 2013. Available online: https://eatforhealth.govcms.gov.au/sites/default/files/content/n55_australian_dietary_guidelines.pdf (accessed on 16 February 2020).
- Viñuela, A.; Brown, A.A.; Buil, A.; Tsai, P.C.; Davies, M.N.; Bell, J.T.; Dermitzakis, E.T.; Spector, T.D.; Small, K.S. Age-dependent changes in mean and variance of gene expression across tissues in a twin cohort. Hum. Mol. Gen. 2018, 27, 732–741. [Google Scholar] [CrossRef]
- Lu, P.; Zhang, C.-H.; Lifshitz, L.M.; ZhuGe, R. Extraoral bitter taste receptors in health and disease. J. Gen. Physiol. 2017, 149, 181–197. [Google Scholar] [CrossRef] [Green Version]
- Aburto, N.J.; Ziolkovska, A.; Hooper, L.; Elliott, P.; Cappuccio, F.P.; Meerpohl, J.J. Effect of lower sodium intake on health: Systematic review and meta-analyses. BMJ 2013, 346, f1326. [Google Scholar] [CrossRef] [Green Version]
- Australian Bureau of Statistics. National Health Survey: First Results 2017-18. Available online: https://www.ausstats.abs.gov.au/ausstats/subscriber.nsf/0/4B3976684C09F43FCA258399001CE630/$File/4364.0.55.001%20-%20national%20health%20survey,%20first%20results,%202017-18.pdf (accessed on 2 February 2020).
- Australian Bureau of Statistics. National Nutrition and Physical Activity Survey; ABS: Canberra, ACT, Australia, 2011–2012. Available online: https://www.abs.gov.au/ausstats/[email protected]/mf/4364.0.55.007 (accessed on 18 February 2020).
- Barragán, R.; Coltell, O.; Portolés, O.; Asensio, E.M.; Sorlí, J.V.; Ortega-Azorín, C.; González, J.I.; Sáiz, C.; Fernández-Carrión, R.; Ordovas, J.M.; et al. Bitter, sweet, salty, sour and umami taste perception decreases with age: Sex-specific analysis, modulation by genetic variants and taste-preference associations in 18 to 80 year-old subjects. Nutrients 2018, 10, 1539. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variable | Mean | Minimum | Maximum | SD |
|---|---|---|---|---|
| Age (years) | 77.4 | 65 | 94 | 6.8 |
| DGI (150-point index) | 97.0 | 30.9 | 132.6 | 15.8 |
| ARFS (74-point index) | 28.9 | 6 | 50 | 7.6 |
| AUST-HEI (60-point index) | 30.2 | 5 | 50 | 9.7 |
| BMI (kg/m2) | 28.5 | 17.1 | 46.3 | 4.8 |
| Sodium intake (mg/day) | 2052 | 506 | 8250 | 843 |
| Variable | n | % |
|---|---|---|
| Sex | ||
| Males | 241 | 45.0 |
| Females | 295 | 55.0 |
| Income | ||
| <AUD 20,000 per year | 165 | 31.5 |
| AUD 20,000 to AUD 60,000 per year | 322 | 61.6 |
| >AUD 60,000 per year | 36 | 6.9 |
| Education | ||
| ≤Trade qualification | 177 | 33.1 |
| TAFE or other certificates | 295 | 55.1 |
| ≥Bachelor degree | 63 | 11.8 |
| Smoking | ||
| Current smoker | 15 | 2.8 |
| Ex-smoker | 253 | 47.2 |
| Never smoked | 268 | 50.0 |
| History of cardiovascular disease a,b | ||
| Yes | 219 | 40.9 |
| No | 317 | 59.1 |
| History of kidney disease b | ||
| Yes | 90 | 17.5 |
| No | 425 | 82.5 |
| Use of anti-hypertensive medication b | ||
| Yes | 118 | 22.0 |
| No | 418 | 78.0 |
| Regular use of any prescription medication b | ||
| Yes | 438 | 81.7 |
| No | 98 | 18.3 |
| SNP | Female n (%) | Male n (%) | Total n (%) |
|---|---|---|---|
| C/C | 33 (11.2) | 33 (13.7) | 66 (12.3) |
| C/T | 134 (45.4) | 116 (48.1) | 250 (46.6) |
| T/T | 128 (43.4) | 92 (38.2) | 220 (41.1) |
| Unadjusted (Mean ± SEM) | Adjusted (Mean ± SEM) | |||||||
|---|---|---|---|---|---|---|---|---|
| C/C | C/T | T/T | ptrend | C/C | C/T | T/T | ptrend | |
| Creat (mmol/L) | 9.3 ± 0.6 | 9.7 ± 0.3 | 9.2 ± 0.3 | 0.5 | 9.1 ± 0.7 | 9.8 ± 0.4 | 9.2 ± 0.4 | 0.4 |
| Alb/Creat Ratio (mg/mmol) | 2.5 ± 4.0 | 9.3 ± 2.0 | 3.6 ± 2.3 | 0.1 | 5.7 ± 4.0 | 9.7 ± 2.3 | 7.5 ± 2.5 | 0.2 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferraris, C.; Turner, A.; Kaur, K.; Piper, J.; Veysey, M.; Lucock, M.; Beckett, E.L. Salt Taste Genotype, Dietary Habits and Biomarkers of Health: No Associations in an Elderly Cohort. Nutrients 2020, 12, 1056. https://doi.org/10.3390/nu12041056
Ferraris C, Turner A, Kaur K, Piper J, Veysey M, Lucock M, Beckett EL. Salt Taste Genotype, Dietary Habits and Biomarkers of Health: No Associations in an Elderly Cohort. Nutrients. 2020; 12(4):1056. https://doi.org/10.3390/nu12041056
Chicago/Turabian StyleFerraris, Celeste, Alexandria Turner, Kiranjit Kaur, Jessica Piper, Martin Veysey, Mark Lucock, and Emma L. Beckett. 2020. "Salt Taste Genotype, Dietary Habits and Biomarkers of Health: No Associations in an Elderly Cohort" Nutrients 12, no. 4: 1056. https://doi.org/10.3390/nu12041056