Nutrition Risk Assessment Using the Modified NUTRIC Score in Cirrhotic Patients with Acute Gastroesophageal Variceal Bleeding: Prevalence of High Nutrition Risk and its Independent Prognostic Value

Abstract
:1. Introduction
2. Materials and Methods
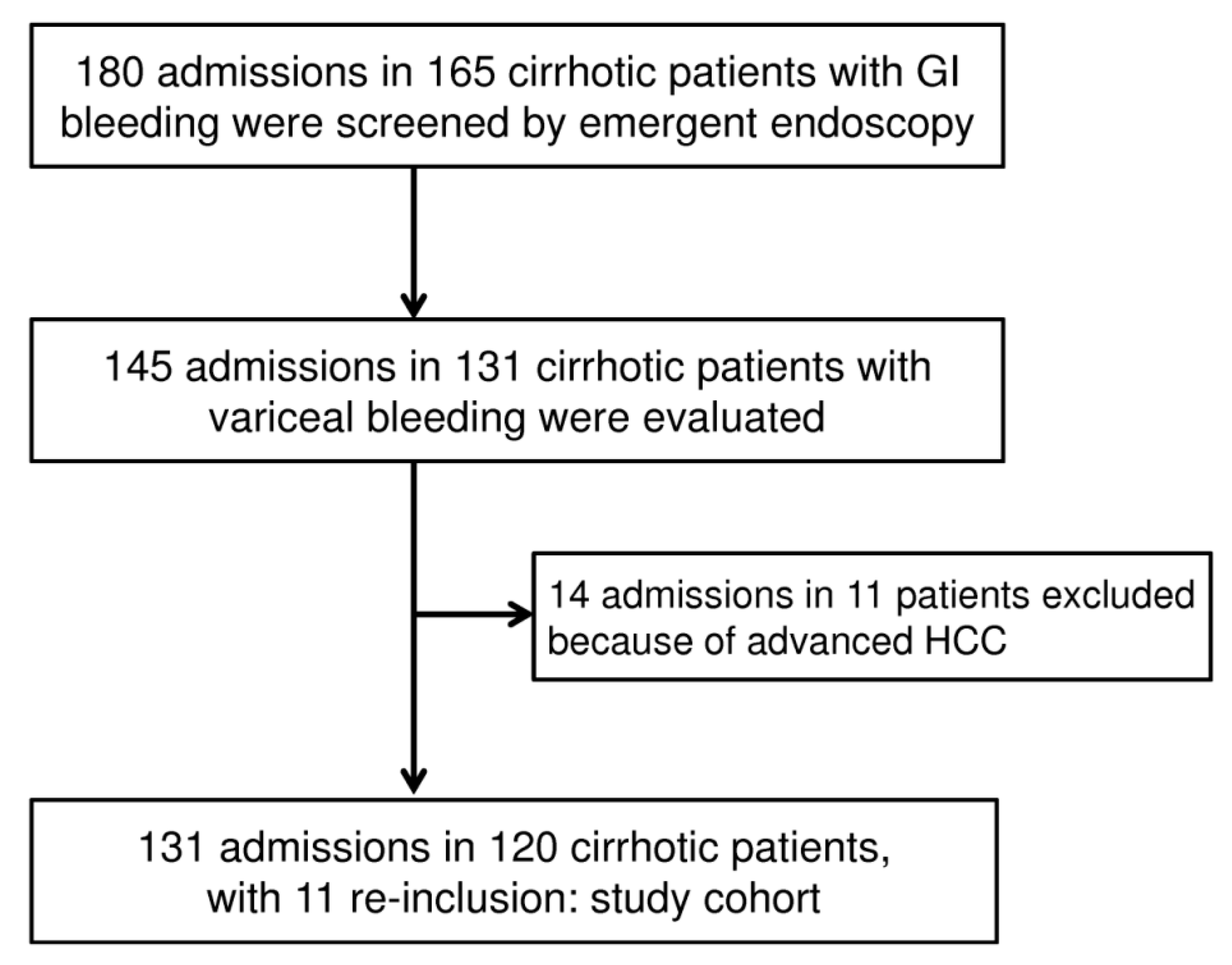
2.1. Patient Information, Data Collection, and Definitions
2.2. Laboratory Investigations
2.3. Nutrition Risk Assessment and Disease Severity Scores
2.4. Statistical Analysis
3. Results
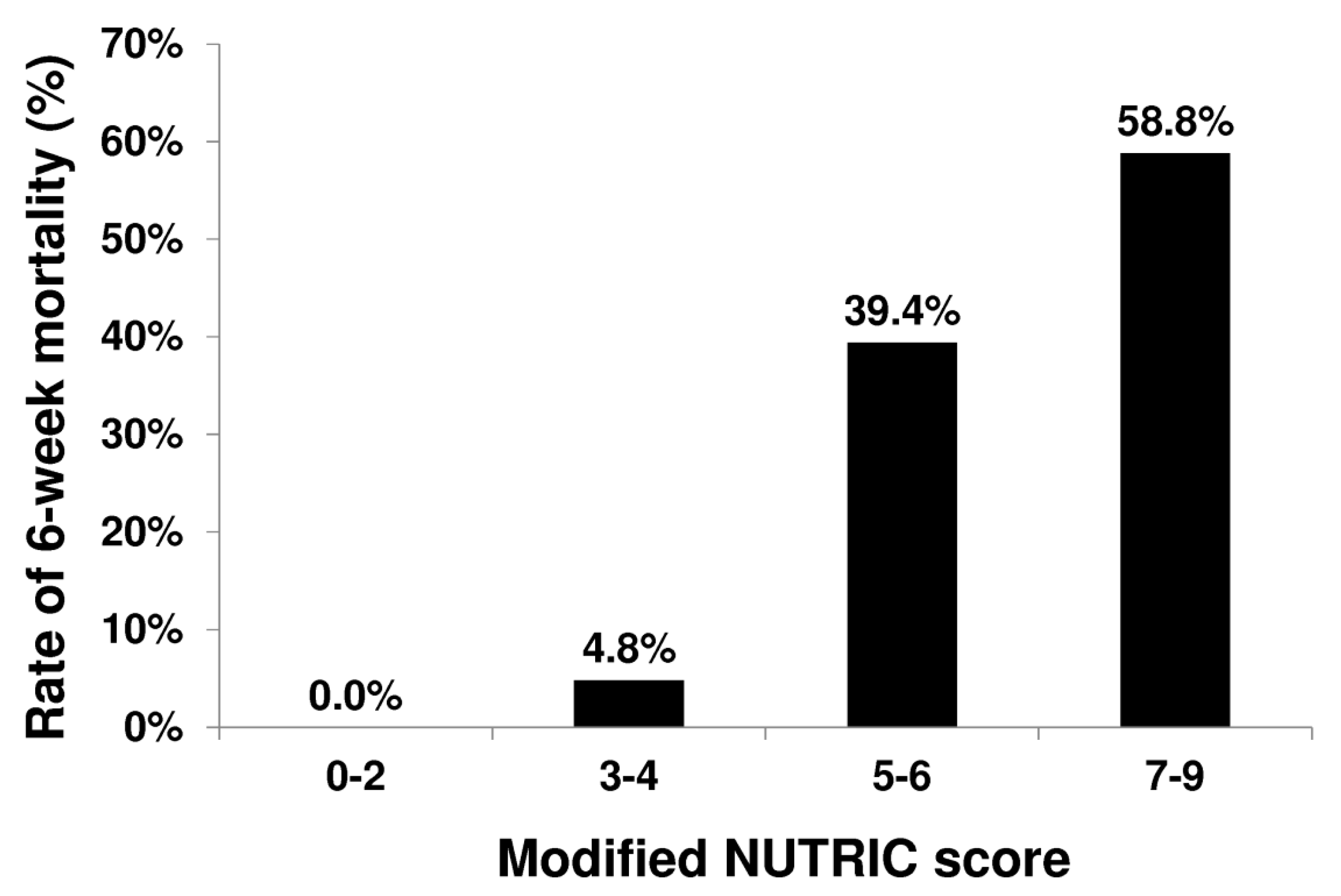
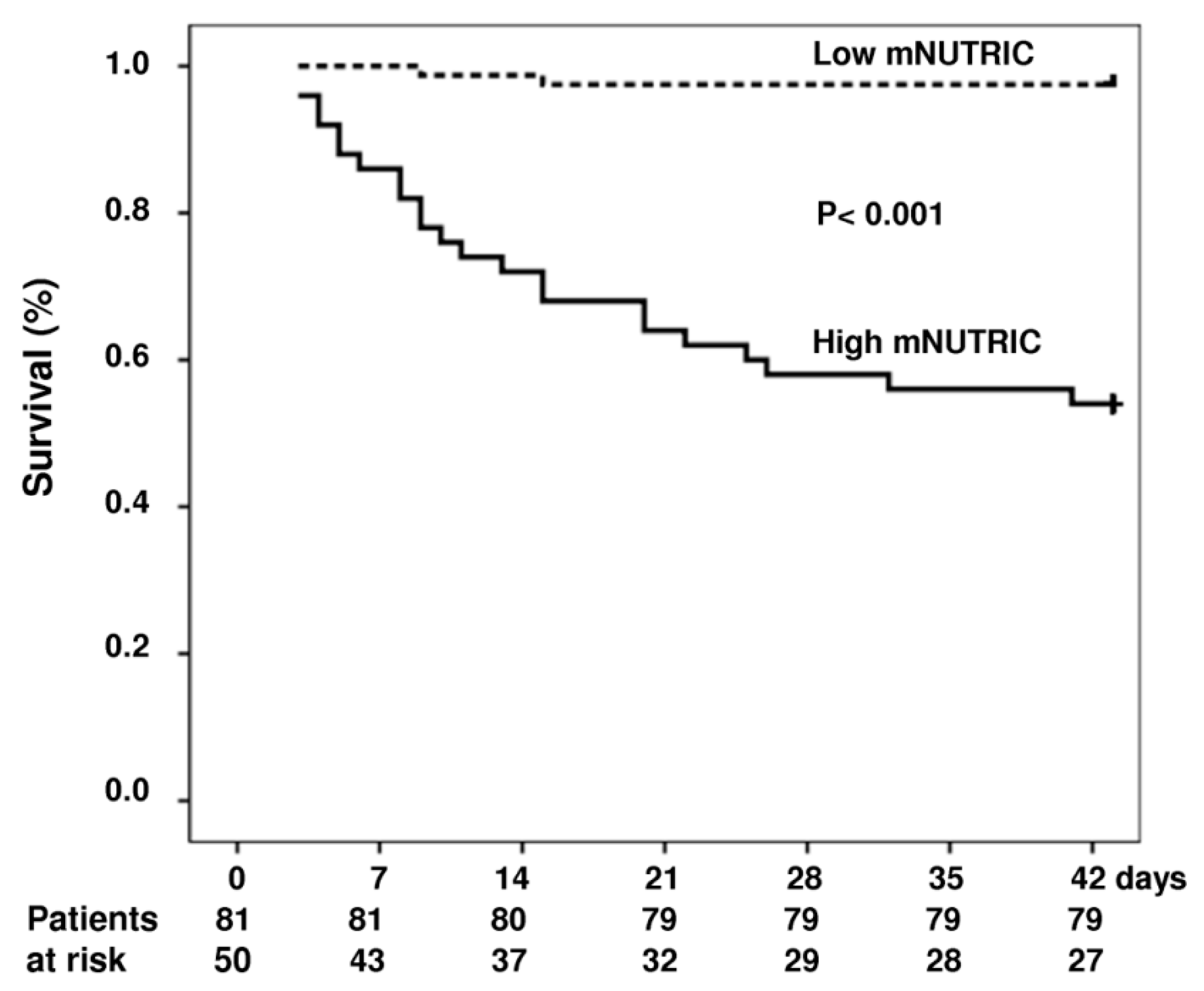
mNUTRIC Score and Outcomes
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Preiser, J.-C.; Van Zanten, A.R.; Berger, M.M.; Biolo, G.; Casaer, M.P.; Doig, G.S.; Griffiths, R.D.; Heyland, D.K.; Hiesmayr, M.; Iapichino, G.; et al. Metabolic and nutritional support of critically ill patients: Consensus and controversies. Crit. Care 2015, 19, 35. [Google Scholar] [CrossRef]
- Heyland, D.K.; Dhaliwal, R.; Jiang, X.; Day, A.G. Identifying critically ill patients who benefit the most from nutrition therapy: The development and initial validation of a novel risk assessment tool. Crit. Care 2011, 15, R268. [Google Scholar] [CrossRef]
- Kondrup, J. Nutritional risk screening (NRS 2002): A new method based on an analysis of controlled clinical trials. Clin. Nutr. 2003, 22, 321–336. [Google Scholar] [CrossRef]
- Rahman, A.; Hasan, R.M.; Agarwala, R.; Martin, C.; Day, A.G.; Heyland, D.K. Identifying critically-ill patients who will benefit most from nutritional therapy: Further validation of the “modified NUTRIC” nutritional risk assessment tool. Clin. Nutr. 2016, 35, 158–162. [Google Scholar] [CrossRef]
- Kruizenga, H.; Seidell, J.; De Vet, H.; Wierdsma, N. Development and validation of a hospital screening tool for malnutrition: The short nutritional assessment questionnaire (SNAQ©). Clin. Nutr. 2005, 24, 75–82. [Google Scholar] [CrossRef]
- Ferguson, M.; Capra, S.; Bauer, J.; Banks, M. Development of a valid and reliable malnutrition screening tool for adult acute hospital patients. Nutrition 1999, 15, 458–464. [Google Scholar] [CrossRef]
- Stratton, R.J.; Hackston, A.; Longmore, D.; Dixon, R.; Price, S.; Stroud, M.; King, C.; Elia, M. Malnutrition in hospital outpatients and inpatients: Prevalence, concurrent validity and ease of use of the ‘malnutrition universal screening tool’ (‘MUST’) for adults. Br. J. Nutr. 2004, 92, 799–808. [Google Scholar] [CrossRef]
- Kondrup, J.; Allison, S.; Elia, M.; Vellas, B.; Plauth, M. ESPEN Guidelines for Nutrition Screening 2002. Clin. Nutr. 2003, 22, 415–421. [Google Scholar] [CrossRef]
- Baker, J.P.; Detsky, A.S.; Wesson, D.E.; Wolman, S.L.; Stewart, S.; Whitewell, J.; Langer, B.; Jeejeebhoy, K.N. Nutritional assessment: A comparison of clinical judgement and objective measurements. N. Engl. J. Med. 1982, 306, 969–972. [Google Scholar] [CrossRef]
- Taylor, B.E.; McClave, S.A.; Martindale, R.G.; Warren, M.M.; Johnson, D.R.; Braunschweig, C.; McCarthy, M.S.; Davanos, E.; Rice, T.W.; Cresci, G.A.; et al. Society of Critical Care Medicine; American Society of Parenteral and Enteral Nutrition. Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Adult Critically Ill Patient: Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutrition (A.S.P.E.N.). Crit. Care Med. 2016, 44, 390–438. [Google Scholar]
- Raman, M.; Mourtzakis, M.; Merli, M.; Tandon, P. A practical approach to nutritional screening and assessment in cirrhosis. Hepatology 2017, 65, 1044–1057. [Google Scholar] [Green Version]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines on nutrition in chronic liver disease. J. Hepatol. 2019, 70, 172–193. [Google Scholar] [CrossRef]
- Huisman, E.J.; Trip, E.J.; Siersema, P.D.; Van Hoek, B.; Van Erpecum, K.J. Protein energy malnutrition predicts complications in liver cirrhosis. Eur. J. Gastroenterol. Hepatol. 2011, 23, 982–989. [Google Scholar] [CrossRef]
- Merli, M.; Lucidi, C.; Giannelli, V.; Giusto, M.; Riggio, O.; Falcone, M.; Ridola, L.; Attili, A.F.; Venditti, M. Cirrhotic Patients Are at Risk for Health Care–Associated Bacterial Infections. Clin. Gastroenterol. Hepatol. 2010, 8, 979–985.e1. [Google Scholar] [CrossRef]
- Merli, M.; Giusto, M.; Lucidi, C.; Giannelli, V.; Pentassuglio, I.; Di Gregorio, V.; Lattanzi, B.; Riggio, O. Muscle depletion increases the risk of overt and minimal hepatic encephalopathy: Results of a prospective study. Metab. Brain Dis. 2013, 28, 281–284. [Google Scholar] [CrossRef]
- Gunsar, F.; Raimondo, M.L.; Jones, S.; Terreni, N.; Wong, C.; Patch, D.; Sabin, C.; Burroughs, A.K. Nutritional status and prognosis in cirrhotic patients. Aliment. Pharmacol. Ther. 2006, 24, 563–572. [Google Scholar] [CrossRef]
- Tandon, P.; Ney, M.; Irwin, I.; Ma, M.M.; Gramlich, L.; Bain, V.G.; Esfandiari, N.; Baracos, V.; Myers, R.P.; Montano-Loza, A.J.; et al. Severe muscle depletion in patients on the liver transplant wait list: Its prevalence and independent prognostic value. Liver Transpl. 2012, 18, 1209–1216. [Google Scholar] [CrossRef]
- De Franchis, R. Revising consensus in portal hypertension: Report of the Baveno V consensus workshop on methodology of diagnosis and therapy in portal hypertension. J. Hepatol. 2010, 53, 762–768. [Google Scholar] [CrossRef] [Green Version]
- García-Tsao, G.; Bosch, J. Management of Varices and Variceal Hemorrhage in Cirrhosis. N. Engl. J. Med. 2010, 362, 823–832. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Tsao, G.; Bosch, J.; Groszmann, R.J. Portal hypertension and variceal bleeding—Unresolved issues. Hepatology 2008, 47, 1764–1772. [Google Scholar] [CrossRef]
- Colomo, A.; Bosch, A.; Concepción, M.; Aracil, C.; Álvarez-Urturi, C.; Santaló, M.; Muñiz, E.; Villanueva, C.; Hernández-Gea, V.; Graupera, I.; et al. Transfusion Strategies for Acute Upper Gastrointestinal Bleeding. N. Engl. J. Med. 2013, 368, 11–21. [Google Scholar]
- Pugh, R.N.; Murray-Lyon, I.M.; Dawson, J.L.; Pietroni, M.C.; Williams, R. Transection of the esophagus in the bleeding esophageal varices. Br. J. Surg. 1973, 60, 646–649. [Google Scholar] [CrossRef]
- Kamath, P.S.; Wiesner, R.H.; Malinchoc, M.; Kremers, W.K.; Therneau, T.M.; D’Amico, G.; Kosberg, C.L.; Dickson, E.; Kim, W. A model to predict survival in patients with end-stage liver disease. Hepatology 2001, 120, A76–A77. [Google Scholar]
- Jensen, G.L.; Hsiao, P.Y.; Wheeler, D. Adult nutrition assessmenttutorial. JPEN J. Parenter Enter. Nutr. 2012, 36, 267–274. [Google Scholar] [CrossRef]
- Hébuterne, X.; Vanbiervliet, G. Feeding the patients with upper gastrointestinal bleeding. Curr. Opin. Clin. Nutr. Metab. Care 2011, 14, 197–201. [Google Scholar] [CrossRef]
- McClave, S.A.; Chang, W.-K. When to feed the patient with gastrointestinal bleeding. Nutr. Clin. Pract. 2005, 20, 544–550. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| All (n = 131) | 6-Week Mortality (n = 25) | 6-Week Survival (n = 106) | p-value | |
|---|---|---|---|---|
| Age | 54.45 ± 14.20 | 53.88 ± 13.66 | 54.58 ± 14.39 | NS (0.842) |
| Sex (male/female) | 109/22 | 20/5 | 89/17 | NS (0.634) |
| Etiology (alcohol/virus/mixed type/others) | 51/67/12/1 | 13/10/2/0 | 38/57/10/1 | NS (0.550) |
| mNUTRIC score | 3.88 ± 2.22 | 6.27 ± 1.39 | 3.32 ± 2.01 | <0.001 |
| High mNUTRIC score | 50/131 (38.2) | 23/25 (92.0) | 27/106 (25.5) | <0.001 |
| BMI | 24.12 ± 4.24 | 24.41 ± 5.01 | 24.05 ± 4.06 | NS (0.729) |
| Child–Pugh score | 9.65 ± 2.34 | 12.48 ± 1.74 | 8.98 ± 1.93 | <0.001 |
| Child A/B/C | 12/51/68 | 0/1/24 | 12/50/44 | <0.001 |
| SOFA score | 7.57 ± 3.55 | 9.84 ± 3.83 | 6.65 ± 2.98 | <0.001 |
| APACHE II | 20.57 ± 8.34 | 29.68 ± 8.76 | 18.42 ± 6.64 | <0.001 |
| MELD | 18.92 ± 10.23 | 31.88 ± 11.48 | 15.86 ± 7.07 | <0.001 |
| CRP (mg/L) | 37.30 ± 38.00 | 60.41 ± 52.82 | 32.00 ± 31.84 | 0.003 |
| Albumin (g/dL) | 2.59 ± 0.55 | 2.42 ± 0.61 | 2.63 ± 0.52 | NS (0.080) |
| Bilirubin (mg/dL) | 5.28 ± 7.62 | 13.49 ± 13.08 | 3.35 ± 3.61 | <0.001 |
| INR | 1.81 ± 1.18 | 2.90 ± 2.15 | 1.55 ± 0.38 | <0.001 |
| Serum creatinine (mg/dL) | 1.68 ± 1.49 | 2.82 ± 1.83 | 1.41 ± 1.27 | <0.001 |
| Hemoglobulin (g/dL) | 8.43 ± 1.55 | 8.58 ± 1.96 | 8.41 ± 1.48 | NS (0.673) |
| Platelet (×109/L) | 65.02 ± 35.49 | 56.08 ± 32.66 | 67.15 ± 35.95 | NS (0.162) |
| Leukocytes (×109/L) | 9.43 ± 6.08 | 12.25 ± 9.01 | 8.75 ± 4.96 | 0.009 |
| Blood transfusion (unit) | 4.56 ± 4.01 | 8.75 ± 5.04 | 3.65 ± 3.13 | <0.001 |
| Mean arterial pressure (mmHg) | 73.91 ± 12.87 | 64.22 ± 11.12 | 76.31 ± 12.17 | 0.003 |
| Shock (%) | 59/131 (45.0) | 22/25 (88.0) | 37/106 (34.9) | <0.001 |
| Ascites (%) | 83/131 (63.4) | 24/25 (96.0) | 59/106 (55.7) | 0.001 |
| Hepatic encephalopathy (%) | 73/131 (55.7) | 20/25 (80.0) | 53/106 (50.0) | 0.007 |
| Hepatocellular carcinoma (%) | 33/131 (25.2) | 9/25 (36.0) | 24/106 (22.6) | NS (0.166) |
| Bacterial infection at inclusion (%) | 42/131 (32.1) | 19/25 (76.0) | 23/106 (21.7) | <0.001 |
| Treatment failure (%) | 38/131 (29.0) | 20/25 (80.0%) | 18/106 (17.0%) | <0.001 |
| ICU stay (days) | 8.05 ± 8.54 | 12.76 ± 11.04 | 6.91 ± 7.47 | 0.002 |
| Parameter | Beta Coefficient | Standard Error | Odds Ratios (95%CI) | p |
|---|---|---|---|---|
| Univariate logistic regression | ||||
| mNUTRIC score | 0.849 | 0.175 | 2.338 (1.658–3.296) | <0.001 |
| High mNUTRIC score | 3.516 | 0.770 | 33.648 (7.437–152.243) | <0.001 |
| Child–Pugh score | 1.007 | 0.200 | 2.738 (1.850–4.053) | <0.001 |
| SOFA score | 0.586 | 0.115 | 1.796 (1.434–2.250) | <0.001 |
| APACHE II | 0.176 | 0.036 | 1.192 (1.112–1.278) | <0.001 |
| MELD | 0.175 | 0.033 | 1.191 (1.116–1.272) | <0.001 |
| CRP (mg/L) | 0.017 | 0.006 | 1.017 (1.005–1.030) | 0.007 |
| Bilirubin (mg/dL) | 0.180 | 0.044 | 1.197 (1.098–1.305) | <0.001 |
| INR | 3.044 | 0.625 | 20.980 (6.157–71.481) | <0.001 |
| Serum creatinine (mg/dL) | 0.528 | 0.138 | 1.695 (1.293–2.223) | <0.001 |
| Leukocytes (×109/L) | 0.082 | 0.035 | 1.085 (1.014–1.162) | 0.0185 |
| Blood transfusion (unit) | 0.291 | 0.079 | 1.337 (1.146–1.561) | <0.001 |
| Mean arterial pressure (mmHg) | −0.096 | 0.025 | 0.908 (0.865–0.953) | <0.001 |
| Shock (%) | 2.616 | 0.648 | 13.676 (3.838–48.730) | <0.001 |
| Ascites (%) | 2.951 | 1.039 | 19.119 (2.494–146.557) | 0.005 |
| Hepatic encephalopathy (%) | 1.386 | 0.536 | 4.000 (1.398–11.446) | 0.010 |
| Bacterial infection at inclusion (%) | 2.436 | 0.524 | 11.428 (4.090–31.929) | <0.001 |
| Treatment failure (%) | 2.973 | 0.563 | 19.556 (6.488–58.947) | 0.001 |
| ICU stay (days) | 0.064 | 0.024 | 1.066 (1.017–1.117) | 0.007 |
| Multivariate logistic regression (Model 1) | ||||
| mNUTRIC score | 0.770 | 0.238 | 2.160 (1.355–3.445) | 0.001 |
| Bacterial infection at inclusion | 1.980 | 0.819 | 7.240 (1.453–36.071) | 0.016 |
| Child–Pugh score | 0.954 | 0.274 | 2.596 (1.518–4.439) | <0.001 |
| Multivariate logistic regression (Model 2) | ||||
| mNUTRIC score | 0.875 | 0.292 | 2.399 (1.353–4.256) | 0.003 |
| Bacterial infection at inclusion | 3.155 | 0.948 | 23.443 (3.659–150.178) | 0.001 |
| MELD score | 0.184 | 0.052 | 1.202 (1.086–1.330) | <0.001 |
| All (n = 131) | High mNUTRIC (n = 50) | Low mNUTRIC (n = 81) | p-value | |
|---|---|---|---|---|
| Age | 54.45 ± 14.20 | 60.62 ± 13.51 | 50.64 ± 13.33 | <0.001 |
| Sex (male/female) | 109/22 | 38/12 | 71/10 | NS (0.083) |
| Etiology (alcohol/virus/mixed type/others) | 51/67/12/1 | 17/30/3/0 | 34/37/9/1 | NS (0.359) |
| BMI | 24.12 ± 4.24 | 24.51 ± 4.21 | 23.87 ± 4.27 | NS (0.448) |
| Child–Pugh score | 9.65 ± 2.34 | 11.00 ± 2.28 | 8.81 ± 1.97 | <0.001 |
| Child A/B/C | 12/51/68 | 1/12/37 | 11/39/31 | <0.001 |
| SOFA score | 7.57 ± 3.55 | 10.40 ± 3.42 | 5.83 ± 2.29 | <0.001 |
| APACHE II | 20.57 ± 8.34 | 27.90 ± 7.47 | 16.05 ± 4.95 | <0.001 |
| MELD | 18.92 ± 10.23 | 26.22 ± 11.04 | 14.41 ± 6.44 | <0.001 |
| CRP (mg/L) | 37.30 ± 38.00 | 53.97 ± 43.46 | 26.09 ± 29.21 | <0.001 |
| Albumin (g/dL) | 2.59 ± 0.55 | 2.49 ± 0.53 | 2.65 ± 0.55 | NS (0.091) |
| Bilirubin (mg/dl) | 5.28 ± 7.62 | 7.69 ± 9.88 | 3.80 ± 5.37 | 0.004 |
| INR | 1.81 ± 1.18 | 2.24 ± 1.67 | 1.54 ± 0.38 | <0.001 |
| Serum creatinine (mg/dL) | 1.68 ± 1.49 | 2.68 ± 1.84 | 1.06 ± 0.72 | <0.001 |
| Hemoglobulin (g/dL) | 8.43 ± 1.55 | 8.45 ± 1.51 | 8.42 ± 1.59 | NS (0.924) |
| Platelet (x109/L) | 65.02 ± 35.49 | 63.53 ± 33.08 | 65.92 ± 37.04 | NS (0.711) |
| Leukocytes (x109/L) | 9.43 ± 6.08 | 11.57 ± 7.76 | 8.12 ± 4.32 | 0.002 |
| Blood transfusion (unit) | 4.56 ± 4.01 | 5.17 ± 4.71 | 4.15 ± 3.44 | NS (0.243) |
| Mean arterial pressure (mmHg) | 73.91 ± 12.87 | 68.24 ± 11.82 | 77.41 ± 12.30 | <0.001 |
| Shock (%) | 59/131 (45.0) | 28/50 (56.0) | 31/81 (38.3) | 0.048 |
| Ascites (%) | 83/131 (63.4) | 39/50 (78.0) | 44/81 (54.3) | 0.006 |
| Hepatic encephalopathy (%) | 73/131 (55.7) | 33/50 (66.0) | 40/81 (49.4) | NS (0.063) |
| Hepatocellular carcinoma (%) | 33/131 (25.2) | 21/60 (42.0) | 12/81 (14.8) | <0.001 |
| Bacterial infection at inclusion (%) | 42/131 (32.1) | 23/50 (46.0) | 19/81 (23.5) | 0.007 |
| Outcome | ||||
| Treatment failure (%) | 38/131 (29.0) | 24/50 (48.0) | 14/62 (17.3) | <0.001 |
| ICU stay (days) | 8.05 ± 8.54 | 11.20 ± 10.56 | 6.05 ± 6.26 | 0.001 |
| ICU mortality (%) | 26/131 19.8) | 23/50 (46.0) | 3/81 (3.7) | <0.001 |
| 28-day mortality (%) | 23/131 (17.6) | 21/50 (42.0) | 2/81 (2.5) | <0.001 |
| 6-week mortality (%) | 25/131 (19.1) | 23/50 (46.0) | 2/81 (2.5) | <0.001 |
| All (n = 131) | Treatment Failure (n = 38) | Treatment Success (n = 93) | p-value | |
|---|---|---|---|---|
| Age | 54.45 ± 14.20 | 52.18 ± 11.54 | 55.38 ± 15.12 | NS (0.245) |
| Sex (male/female) | 109/22 | 34/4 | 75/18 | NS (0.220) |
| Etiology (Alcohol/virus/mixed type/others) | 51/67/12/1 | 20/14/3/1 | 31/53/9/0 | NS (0.090) |
| mNUTRIC score | 3.88 ± 2.22 | 4.82 ± 2.48 | 3.49 ± 2.00 | 0.002 |
| High mNUTRIC score | 50/131 (38.2) | 24/38 (63.2) | 26/93 (28.0) | <0.001 |
| BMI | 24.12 ± 4.24 | 25.01 ± 4.29 | 23.72 ± 4.18 | NS (0.147) |
| Child–Pugh score | 9.65 ± 2.34 | 10.87 ± 2.27 | 9.15 ± 2.19 | <0.001 |
| Child A/B/C | 12/51/68 | 0/12/26 | 12/39/42 | <0.001 |
| SOFA score | 7.57 ± 3.55 | 10.40 ± 3.42 | 5.83 ± 2.29 | <0.001 |
| APACHE II | 20.57 ± 8.34 | 24.39 ± 9.88 | 19.01 ± 7.10 | 0.001 |
| MELD | 18.92 ± 10.23 | 24.58 ± 13.03 | 16.60 ± 7.80 | <0.001 |
| CRP (mg/L) | 37.30 ± 38.00 | 49.57 ± 50.26 | 31.94 ± 30.08 | 0.030 |
| Albumin (g/dL) | 2.59 ± 0.55 | 2.43 ± 0.58 | 2.65 ± 0.52 | 0.035 |
| Bilirubin (mg/dL) | 5.28 ± 7.62 | 7.71 ± 10.62 | 4.29 ± 5.78 | 0.019 |
| INR | 1.81 ± 1.18 | 2.38 ± 1.87 | 1.57 ± 0.41 | <0.001 |
| Serum creatinine (mg/dL) | 1.68 ± 1.49 | 2.25 ± 1.87 | 1.44 ± 1.25 | <0.005 |
| Hemoglobulin (g/dL) | 8.43 ± 1.55 | 8.24 ± 1.73 | 8.50 ± 1.49 | NS (0.423) |
| Platelet (x109/L) | 65.02 ± 35.49 | 57.09 ± 32.71 | 68.30 ± 36.24 | NS (0.101) |
| Leukocytes (x109/L) | 9.43 ± 6.08 | 9.72 ± 5.87 | 9.31 ± 6.19 | NS (0.728) |
| Blood transfusion (unit) | 4.56 ± 4.01 | 7.84 ± 4.76 | 3.28 ± 2.81 | <0.001 |
| Mean arterial pressure (mmHg) | 73.91 ± 12.87 | 68.56 ± 12.87 | 76.06 ± 12.30 | 0.003 |
| Shock (%) | 59/131 (45.0) | 31/38 (81.6) | 28/93 (30.1) | <0.001 |
| Ascites (%) | 83/131 (63.4) | 32/38 (84.2.0) | 51/93 (54.8) | 0.002 |
| Hepatic encephalopathy (%) | 73/131 (55.7) | 24/38 (63.2) | 49/93 (52.7) | NS (0.274) |
| Hepatocellular carcinoma (%) | 33/131 (25.2) | 13/38 (34.2) | 20/93 (21.5) | NS (0.128) |
| Bacterial infection at inclusion (%) | 42/131 (32.1) | 21/38 (55.3) | 21/93 (22.6) | <0.001 |
| Outcome | ||||
| ICU stay (days) | 8.05 ± 8.54 | 10.11 ± 10.21 | 7.22 ± 7.67 | NS (0.082) |
| ICU mortality (%) | 26/131 (19.8) | 19/38 (50.0) | 7/93 (7.5) | <0.001 |
| 28-day mortality (%) | 23/131 (17.6) | 18/38 (47.4) | 5/93 (5.4) | <0.001 |
| 6-week mortality (%) | 25/131 (19.1) | 20/38 (52.6) | 5/93 (5.4) | <0.001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsai, M.-H.; Huang, H.-C.; Peng, Y.-S.; Chen, Y.-C.; Tian, Y.-C.; Yang, C.-W.; Lien, J.-M.; Fang, J.-T.; Hou, M.-C.; Shen, C.-H.; et al. Nutrition Risk Assessment Using the Modified NUTRIC Score in Cirrhotic Patients with Acute Gastroesophageal Variceal Bleeding: Prevalence of High Nutrition Risk and its Independent Prognostic Value. Nutrients 2019, 11, 2152. https://doi.org/10.3390/nu11092152
Tsai M-H, Huang H-C, Peng Y-S, Chen Y-C, Tian Y-C, Yang C-W, Lien J-M, Fang J-T, Hou M-C, Shen C-H, et al. Nutrition Risk Assessment Using the Modified NUTRIC Score in Cirrhotic Patients with Acute Gastroesophageal Variceal Bleeding: Prevalence of High Nutrition Risk and its Independent Prognostic Value. Nutrients. 2019; 11(9):2152. https://doi.org/10.3390/nu11092152
Chicago/Turabian StyleTsai, Ming-Hung, Hui-Chun Huang, Yun-Shing Peng, Yung-Chang Chen, Ya-Chung Tian, Chih-Wei Yang, Jau-Min Lien, Ji-Tseng Fang, Ming-Chih Hou, Chien-Heng Shen, and et al. 2019. "Nutrition Risk Assessment Using the Modified NUTRIC Score in Cirrhotic Patients with Acute Gastroesophageal Variceal Bleeding: Prevalence of High Nutrition Risk and its Independent Prognostic Value" Nutrients 11, no. 9: 2152. https://doi.org/10.3390/nu11092152