Relationship between Nutrition Intake and 28-Day Mortality Using Modified NUTRIC Score in Patients with Sepsis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
Ethical Statement
2.2. Data Collection
2.3. Statistical Analysis
3. Results
3.1. Patients Characteristics
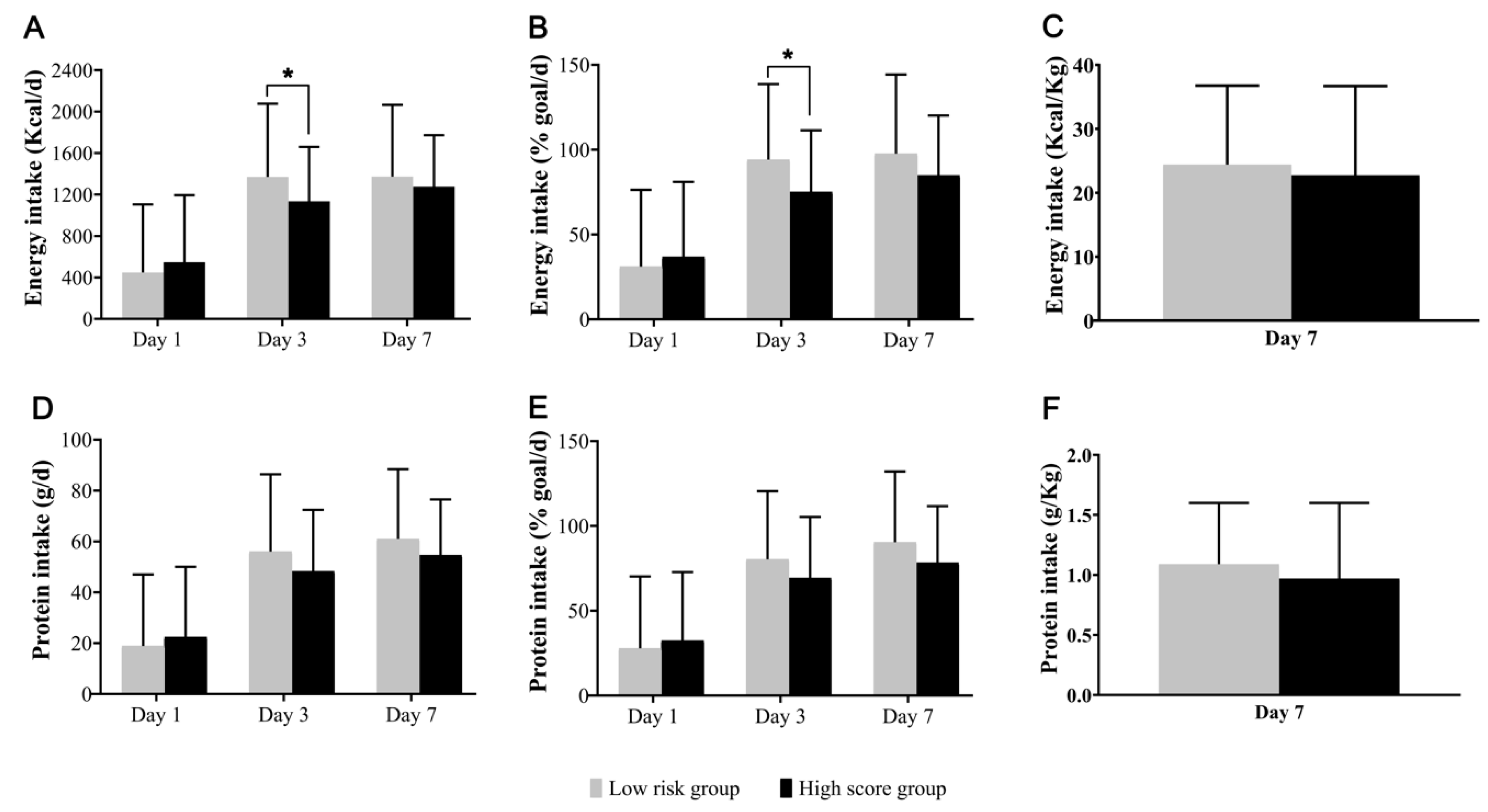
3.2. Nutritional Profiles
3.3. Nutritional Intakes and 28-Day Mortality
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Edington, J.; Boorman, J.; Durrant, E.R.; Perkins, A.; Giffin, C.V.; James, R.; Thomson, J.M.; Oldroyd, J.C.; Smith, J.C.; Torrance, A.D.; et al. Prevalence of malnutrition on admission to four hospitals in england. Clin. Nutr. 2000, 19, 191–195. [Google Scholar] [CrossRef] [PubMed]
- Kondrup, J.; Johansen, N.; Plum, L.M.; Bak, L.; Larsen, I.H.; Martinsen, A.; Andersen, J.R.; Baernthsen, H.; Bunch, E.; Lauesen, N. Incidence of nutritional risk and causes of inadequate nutritional care in hospitals. Clin. Nutr. 2002, 21, 461–468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Correia, M.I.; Campos, A.C.; Elan Cooperative Study. Prevalence of hospital malnutrition in latin america: The multicenter elan study. Nutrition 2003, 19, 823–825. [Google Scholar] [CrossRef]
- McWhirter, J.P.; Pennington, C.R. Incidence and recognition of malnutrition in hospital. BMJ 1994, 308, 945–948. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Villet, S.; Chiolero, R.L.; Bollmann, M.D.; Revelly, J.P.; Cayeux, R.N.M.; Delarue, J.; Berger, M.M. Negative impact of hypocaloric feeding and energy balance on clinical outcome in icu patients. Clin. Nutr. 2005, 24, 502–509. [Google Scholar] [CrossRef] [PubMed]
- Doig, G.S.; Simpson, F.; Finfer, S.; Delaney, A.; Davies, A.R.; Mitchell, I.; Dobb, G.; Nutrition Guidelines Investigators of the Anzics Clinical Trials Group. Effect of evidence-based feeding guidelines on mortality of critically ill adults: A cluster randomized controlled trial. JAMA 2008, 300, 2731–2741. [Google Scholar] [CrossRef] [PubMed]
- Schneider, S.M.; Veyres, P.; Pivot, X.; Soummer, A.M.; Jambou, P.; Filippi, J.; van Obberghen, E.; Hebuterne, X. Malnutrition is an independent factor associated with nosocomial infections. Br. J. Nutr. 2004, 92, 105–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kyle, U.G.; Pirlich, M.; Schuetz, T.; Lochs, H.; Pichard, C. Is nutritional depletion by nutritional risk index associated with increased length of hospital stay? A population-based study. JPEN J. Parenter. Enteral Nutr. 2004, 28, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Giner, M.; Laviano, A.; Meguid, M.M.; Gleason, J.R. In 1995 a correlation between malnutrition and poor outcome in critically ill patients still exists. Nutrition 1996, 12, 23–29. [Google Scholar] [CrossRef]
- Liu, M.J.; Bao, S.; Napolitano, J.R.; Burris, D.L.; Yu, L.; Tridandapani, S.; Knoell, D.L. Zinc regulates the acute phase response and serum amyloid a production in response to sepsis through jak-stat3 signaling. PLoS ONE 2014, 9, e94934. [Google Scholar] [CrossRef]
- Rhodes, A.; Evans, L.E.; Alhazzani, W.; Levy, M.M.; Antonelli, M.; Ferrer, R.; Kumar, A.; Sevransky, J.E.; Sprung, C.L.; Nunnally, M.E.; et al. Surviving sepsis campaign: International guidelines for management of sepsis and septic shock: 2016. Intensive Care Med. 2017, 43, 304–377. [Google Scholar] [CrossRef] [PubMed]
- McClave, S.A.; Taylor, B.E.; Martindale, R.G.; Warren, M.M.; Johnson, D.R.; Braunschweig, C.; McCarthy, M.S.; Davanos, E.; Rice, T.W.; Cresci, G.A.; et al. Guidelines for the provision and assessment of nutrition support therapy in the adult critically ill patient: Society of critical care medicine (sccm) and american society for parenteral and enteral nutrition (a.S.P.E.N.). JPEN J. Parenter. Enteral Nutr. 2016, 40, 159–211. [Google Scholar] [CrossRef] [PubMed]
- Weijs, P.J.; Cynober, L.; DeLegge, M.; Kreymann, G.; Wernerman, J.; Wolfe, R.R. Proteins and amino acids are fundamental to optimal nutrition support in critically ill patients. Crit. Care 2014, 18, 591. [Google Scholar] [CrossRef] [PubMed]
- Weijs, P.J.; Stapel, S.N.; de Groot, S.D.; Driessen, R.H.; de Jong, E.; Girbes, A.R.; Strack van Schijndel, R.J.; Beishuizen, A. Optimal protein and energy nutrition decreases mortality in mechanically ventilated, critically ill patients: A prospective observational cohort study. JPEN J. Parenter. Enteral Nutr. 2012, 36, 60–68. [Google Scholar] [CrossRef] [PubMed]
- Allingstrup, M.J.; Esmailzadeh, N.; Wilkens Knudsen, A.; Espersen, K.; Hartvig Jensen, T.; Wiis, J.; Perner, A.; Kondrup, J. Provision of protein and energy in relation to measured requirements in intensive care patients. Clin. Nutr. 2012, 31, 462–468. [Google Scholar] [CrossRef] [PubMed]
- Hurt, R.T.; McClave, S.A.; Martindale, R.G.; Ochoa Gautier, J.B.; Coss-Bu, J.A.; Dickerson, R.N.; Heyland, D.K.; Hoffer, L.J.; Moore, F.A.; Morris, C.R.; et al. Summary points and consensus recommendations from the international protein summit. Nutr. Clin. Pract. 2017, 32, 142S–151S. [Google Scholar] [CrossRef] [PubMed]
- Charles, E.J.; Petroze, R.T.; Metzger, R.; Hranjec, T.; Rosenberger, L.H.; Riccio, L.M.; McLeod, M.D.; Guidry, C.A.; Stukenborg, G.J.; Swenson, B.R.; et al. Hypocaloric compared with eucaloric nutritional support and its effect on infection rates in a surgical intensive care unit: A randomized controlled trial. Am. J. Clin. Nutr. 2014, 100, 1337–1343. [Google Scholar] [CrossRef]
- Arabi, Y.M.; Aldawood, A.S.; Haddad, S.H.; Al-Dorzi, H.M.; Tamim, H.M.; Jones, G.; Mehta, S.; McIntyre, L.; Solaiman, O.; Sakkijha, M.H.; et al. Permissive underfeeding or standard enteral feeding in critically ill adults. N. Engl. J. Med. 2015, 372, 2398–2408. [Google Scholar] [CrossRef] [PubMed]
- Arabi, Y.M.; Haddad, S.H.; Tamim, H.M.; Rishu, A.H.; Sakkijha, M.H.; Kahoul, S.H.; Britts, R.J. Near-target caloric intake in critically ill medical-surgical patients is associated with adverse outcomes. JPEN J. Parenter. Enteral Nutr. 2010, 34, 280–288. [Google Scholar] [CrossRef]
- Petros, S.; Horbach, M.; Seidel, F.; Weidhase, L. Hypocaloric vs normocaloric nutrition in critically ill patients: A prospective randomized pilot trial. JPEN J. Parenter. Enteral Nutr. 2016, 40, 242–249. [Google Scholar] [CrossRef]
- Compher, C.; Chittams, J.; Sammarco, T.; Nicolo, M.; Heyland, D.K. Greater protein and energy intake may be associated with improved mortality in higher risk critically ill patients: A multicenter, multinational observational study. Crit. Care Med. 2017, 45, 156–163. [Google Scholar] [CrossRef] [PubMed]
- Rahman, A.; Hasan, R.M.; Agarwala, R.; Martin, C.; Day, A.G.; Heyland, D.K. Identifying critically-ill patients who will benefit most from nutritional therapy: Further validation of the “modified nutric” nutritional risk assessment tool. Clin. Nutr. 2016, 35, 158–162. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, M.C.; Bielemann, R.M.; Kruschardt, P.P.; Orlandi, S.P. Complementarity of nutric score and subjective global assessment for predicting 28-day mortality in critically ill patients. Clin. Nutr. 2018. [Google Scholar] [CrossRef] [PubMed]
- Reignier, J.; Boisrame-Helms, J.; Brisard, L.; Lascarrou, J.B.; Ait Hssain, A.; Anguel, N.; Argaud, L.; Asehnoune, K.; Asfar, P.; Bellec, F.; et al. Enteral versus parenteral early nutrition in ventilated adults with shock: A randomised, controlled, multicentre, open-label, parallel-group study (nutrirea-2). Lancet 2018, 391, 133–143. [Google Scholar] [CrossRef]
- Heidegger, C.P.; Berger, M.M.; Graf, S.; Zingg, W.; Darmon, P.; Costanza, M.C.; Thibault, R.; Pichard, C. Optimisation of energy provision with supplemental parenteral nutrition in critically ill patients: A randomised controlled clinical trial. Lancet 2013, 381, 385–393. [Google Scholar] [CrossRef]
- Arabi, Y.M.; Tamim, H.M.; Dhar, G.S.; Al-Dawood, A.; Al-Sultan, M.; Sakkijha, M.H.; Kahoul, S.H.; Brits, R. Permissive underfeeding and intensive insulin therapy in critically ill patients: A randomized controlled trial. Am. J. Clin. Nutr. 2011, 93, 569–577. [Google Scholar] [CrossRef] [PubMed]
- Chapman, M.; Peake, S.L.; Bellomo, R.; Davies, A.; Deane, A.; Horowitz, M.; Hurford, S.; Lange, K.; Little, L.; et al.; TARGET Investigators, for the ANZICS Clinical Trials Group Energy-dense versus routine enteral nutrition in the critically ill. N. Engl. J. Med. 2018, 379, 1823–1834. [Google Scholar] [CrossRef]
- Alberda, C.; Gramlich, L.; Jones, N.; Jeejeebhoy, K.; Day, A.G.; Dhaliwal, R.; Heyland, D.K. The relationship between nutritional intake and clinical outcomes in critically ill patients: Results of an international multicenter observational study. Intensive Care Med. 2009, 35, 1728–1737. [Google Scholar] [CrossRef]
- Wei, X.; Day, A.G.; Ouellette-Kuntz, H.; Heyland, D.K. The association between nutritional adequacy and long-term outcomes in critically ill patients requiring prolonged mechanical ventilation: A multicenter cohort study. Crit. Care Med. 2015, 43, 1569–1579. [Google Scholar] [CrossRef]
- Nicolo, M.; Heyland, D.K.; Chittams, J.; Sammarco, T.; Compher, C. Clinical outcomes related to protein delivery in a critically ill population: A multicenter, multinational observation study. JPEN J. Parenter. Enteral Nutr. 2016, 40, 45–51. [Google Scholar] [CrossRef]
- Weijs, P.J.; Looijaard, W.G.; Beishuizen, A.; Girbes, A.R.; Oudemans-van Straaten, H.M. Early high protein intake is associated with low mortality and energy overfeeding with high mortality in non-septic mechanically ventilated critically ill patients. Crit. Care 2014, 18, 701. [Google Scholar] [CrossRef] [PubMed]
- Perner, A.; Rhodes, A.; Venkatesh, B.; Angus, D.C.; Martin-Loeches, I.; Preiser, J.C.; Vincent, J.L.; Marshall, J.; Reinhart, K.; Joannidis, M.; et al. Sepsis: Frontiers in supportive care, organisation and research. Intensive Care Med. 2017, 43, 496–508. [Google Scholar] [CrossRef] [PubMed]
- Artinian, V.; Krayem, H.; DiGiovine, B. Effects of early enteral feeding on the outcome of critically ill mechanically ventilated medical patients. Chest 2006, 129, 960–967. [Google Scholar] [CrossRef] [PubMed]
- Heyland, D.K.; Dhaliwal, R.; Jiang, X.; Day, A.G. Identifying critically ill patients who benefit the most from nutrition therapy: The development and initial validation of a novel risk assessment tool. Crit. Care 2011, 15, R268. [Google Scholar] [CrossRef] [PubMed]
- Mukhopadhyay, A.; Henry, J.; Ong, V.; Leong, C.S.; Teh, A.L.; van Dam, R.M.; Kowitlawakul, Y. Association of modified nutric score with 28-day mortality in critically ill patients. Clin. Nutr. 2017, 36, 1143–1148. [Google Scholar] [CrossRef] [PubMed]
- Arabi, Y.M.; Aldawood, A.S.; Al-Dorzi, H.M.; Tamim, H.M.; Haddad, S.H.; Jones, G.; McIntyre, L.; Solaiman, O.; Sakkijha, M.H.; Sadat, M.; et al. Permissive underfeeding or standard enteral feeding in high- and low-nutritional-risk critically ill adults. Post hoc analysis of the permit trial. Am. J. Respir. Crit. Care Med. 2017, 195, 652–662. [Google Scholar] [CrossRef]
- Compher, C.; Chittams, J.; Sammarco, T.; Higashibeppu, N.; Higashiguchi, T.; Heyland, D.K. Greater nutrient intake is associated with lower mortality in western and eastern critically ill patients with low bmi: A multicenter, multinational observational study. JPEN J. Parenter. Enteral Nutr. 2019, 43, 63–69. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Modified NUTRIC Score (n = 248) | ||
|---|---|---|---|
| Low Score | High Score | p-Value | |
| (n = 28) | (n = 220) | ||
| Age, years | 54 (42–70) | 68 (58–75) | 0.001 |
| Height, cm | 164 (160–170) | 163 (155–170) | 0.375 |
| Weight, kg | 57 (49–61) | 60 (51–67) | 0.548 |
| BMI, kg/m2 | 21 (18–24) | 23 (19–25) | 0.156 |
| Female, n (%) | 7 (25.0) | 68 (30.9) | 0.521 |
| APACHE II score | 15 (13–18) | 24 (20–28) | <0.001 |
| SOFA score | 6 (4–8) | 12 (9–14) | <0.001 |
| Days from hospital to ICU | 0 (0–2) | 0 (0–6) | 0.510 |
| Co-morbidities | 1 (1–2) | 2 (1–3) | 0.013 |
| LOS in ICU, days | 11 (9–19) | 14 (9–25) | 0.586 |
| MV | 21 (75.0) | 196 (89.1) | 0.034 |
| Vasopressor use | 22 (78.6) | 204 (92.7)) | 0.013 |
| RRT | 4 (14.3) | 100 (45.5) | 0.002 |
| Diagnosis | 0.434 | ||
| Respiratory disease | 19 (62.9) | 119 (54.1) | |
| Liver/GI disease | 3 (10.7) | 35 (15.9) | |
| Cardiovascular disease | 0 (0) | 8 (3.6) | |
| Renal disease | 1 (3.6) | 14 (6.4) | |
| Febrile neutropenia | 0 (0) | 11 (5.0) | |
| SSTI | 0 (0) | 8 (3.6) | |
| Other | 5 (17.9) | 25 (11.4) | |
| VAP | 0 (0) | 19 (8.6) | 0.106 |
| Bacteremia | 8 (28.6) | 77 (35.0) | 0.500 |
| Sepsis severity | <0.001 | ||
| Sepsis | 0 (0) | 6 (2.7) | |
| Severe sepsis | 19 (67.9) | 65 (29.5) | |
| Septic shock | 9 (32.1) | 149 (67.7) | |
| 28-day mortality | 5 (17.9) | 80 (36.4) | 0.052 |
| Sepsis related deaths | 4 (80) | 40 (50) | 0.193 |
| Low Score (n = 28) | p-Value | High Score (n = 220) | p-Value | |||||
|---|---|---|---|---|---|---|---|---|
| Energy intake (kcal/kg) | <20 | 20 to <25 | ≥25 | <20 | 20 to <25 | ≥25 | ||
| No. of patients | 10 | 3 | 15 | 90 | 53 | 77 | ||
| Deaths | 3 (30.0) | 0 (0) | 2 (13.3) | 0.323 | 39 (43.3) | 19 (35.8) | 22 (28.6) | 0.048 |
| Protein intake (g/kg) | <1.0 | 1.0 to <1.2 | ≥1.2 | <1.0 | 1.0 to <1.2 | ≥1.2 | ||
| No. of patients | 12 | 5 | 11 | 128 | 40 | 52 | ||
| Deaths | 3 (25.0) | 1 (20.0) | 1 (9.1) | 0.330 | 52 (40.6) | 13 (32.5) | 15 (28.8) | 0.117 |
| Variables | Unadjusted | Adjusted | ||
|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Age | 1.008 (0.992–1.015) | 0.334 | 1.015 (0.998–1.032) | 0.091 |
| Sex | 1.823 (1.177–2.826) | 0.007 | 2.009 (1.285–3.140) | 0.002 |
| BMI | 1.051 (1.007–1.098) | 0.024 | .. | .. |
| Co-morbidities | 1.054 (0.849–1.309) | 0.631 | .. | .. |
| Energy intake (kcal/kg) | ||||
| <20 | Reference | Reference | ||
| 20 to <25 | 0.865 (0.503–1.487) | 0.599 | 0.883 (0.513–1.520) | 0.654 |
| ≥25 | 0.562 (0.340–0.929) | 0.025 | 0.534 (0.322–0.887) | 0.015 |
| Protein intake (g/kg) | ||||
| <1.0 | Reference | Reference | ||
| 1.0 to <1.2 | 0.793 (0.441–1.427) | 0.643 | 0.860 (0.476–1.555) | 0.618 |
| ≥1.2 | 0.506 (0.289–0.886) | 0.017 | 0.475 (0.270–0.836) | 0.010 |
| Variables | Unadjusted | Adjusted | ||
|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Age | 0.993 (0.954–1.034) | 0.742 | ||
| Sex | 1.001 (0.274–3.657) | 0.999 | ||
| BMI | 1.050 (0.931–1.184) | 0.424 | 1.081 (0.927–1.260) | 0.320 |
| Co-morbidities | 0.565 (0.296–1.078) | 0.083 | ||
| Energy intake (kcal/kg) | ||||
| <20 | Reference | Reference | ||
| 20 to <25 | 0 (0) | 0.989 | 0 (0) | 0.988 |
| ≥25 | 0.400 (0.062–2.563) | 0.334 | 0.193 (0.013–2.840) | 0.231 |
| Protein intake (g/kg) | ||||
| <1.0 | Reference | Reference | ||
| 1.0 to <1.2 | 0.806 (0.079–8.187) | 0.855 | 0.021 (0.000–9.343) | 0.214 |
| ≥1.2 | 0.285 (0.028–2.909) | 0.289 | 0.256 (0.013–5.176) | 0.375 |
| Variables | Unadjusted | Adjusted | ||
|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Age | 1.009 (0.990–1.028) | 0.345 | ||
| Sex | 1.977 (1.235–3.165) | 0.005 | 1.970 (1.239–3.132) | 0.004 |
| BMI | 1.049 (1.001–1.099) | 0.044 | ||
| Co-morbidities | 1.117 (0.884–1.411) | 0.354 | ||
| Energy intake (kcal/kg) | ||||
| <20 | Reference | Reference | ||
| 20 to <25 | 0.864 (0.499–1.495) | 0.601 | 0.901 (0.520–1.561) | 0.709 |
| ≥25 | 0.582 (0.344–0.982) | 0.043 | 0.569 (0.337–0.962) | 0.035 |
| Protein intake (g/kg) | ||||
| <1.0 | Reference | Reference | ||
| 1.0 to <1.2 | 0.780 (0.425–1.432) | 0.423 | 0.857 (0.464–1.583) | 0.622 |
| ≥1.2 | 0.537 (0.301–0.956) | 0.035 | 0.502 (0.280–0.900) | 0.021 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jeong, D.H.; Hong, S.-B.; Lim, C.-M.; Koh, Y.; Seo, J.; Kim, Y.; Min, J.-Y.; Huh, J.W. Relationship between Nutrition Intake and 28-Day Mortality Using Modified NUTRIC Score in Patients with Sepsis. Nutrients 2019, 11, 1906. https://doi.org/10.3390/nu11081906
Jeong DH, Hong S-B, Lim C-M, Koh Y, Seo J, Kim Y, Min J-Y, Huh JW. Relationship between Nutrition Intake and 28-Day Mortality Using Modified NUTRIC Score in Patients with Sepsis. Nutrients. 2019; 11(8):1906. https://doi.org/10.3390/nu11081906
Chicago/Turabian StyleJeong, Dae Hyun, Sang-Bum Hong, Chae-Man Lim, Younsuck Koh, Jarim Seo, Younkyoung Kim, Ji-Yeon Min, and Jin Won Huh. 2019. "Relationship between Nutrition Intake and 28-Day Mortality Using Modified NUTRIC Score in Patients with Sepsis" Nutrients 11, no. 8: 1906. https://doi.org/10.3390/nu11081906