A Mediterranean Diet with Fresh, Lean Pork Improves Processing Speed and Mood: Cognitive Findings from the MedPork Randomised Controlled Trial

 , , and
, , and
Abstract
:1. Introduction
2. Methods
2.1. Ethics
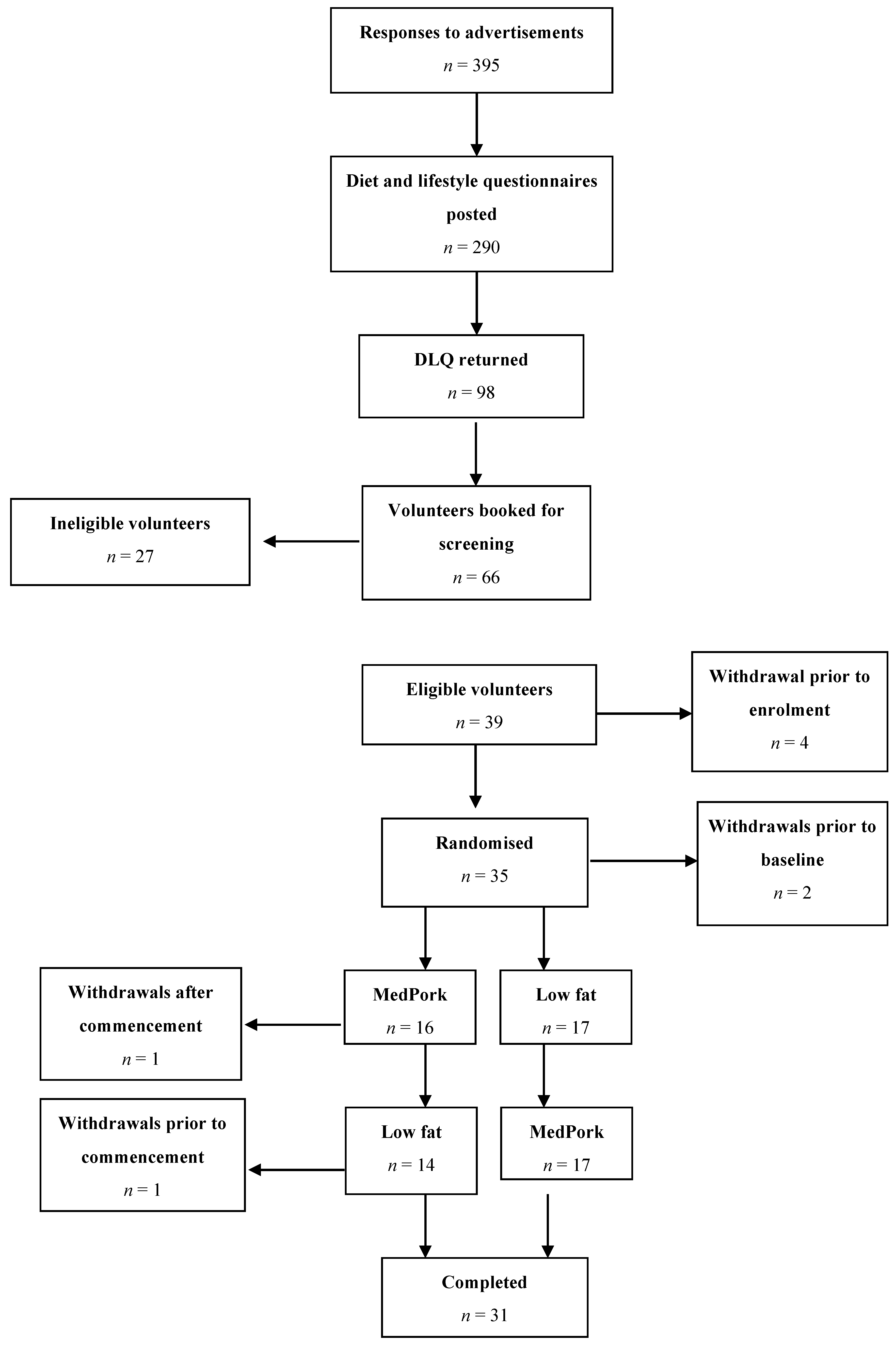
2.2. Participants and Recruitment
2.3. Design
2.4. Dietary Interventions
2.4.1. Low-Fat Diet (LF)
2.4.2. Mediterranean Diet with Pork (MedPork)
2.4.3. Dietetic Counselling
2.5. Measures
2.5.1. Cognitive Function
2.5.2. Sleep
2.5.3. Psychological Well-Being
2.5.4. Dietary Adherence
2.6. Procedure
2.7. Statistical Analysis
3. Results
3.1. Period Effects
3.2. Dietary Adherence and Nutrients
3.3. Cognitive Function
3.4. Psychological Well-Being
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Alzheimer’s Disease International. World Alzheimer Report 2015 The Global Impact of Dementia; Alzheimer’s Disease International: London, UK, 2015. [Google Scholar]
- Norton, S.; Matthews, F.E.; Barnes, D.E.; Yaffe, K.; Brayne, C. Potential for primary prevention of Alzheimer’s disease: An analysis of population-based data. Lancet Neurol. 2014, 13, 788–794. [Google Scholar] [CrossRef]
- Kivipelto, M.; Mangialasche, F.; Ngandu, T. Lifestyle interventions to prevent cognitive impairment, dementia and Alzheimer disease. Nat. Rev. Neurol. 2018, 14, 653–666. [Google Scholar] [CrossRef] [PubMed]
- Davis, C.R.; Bryan, J.; Hodgson, J.; Murphy, K. Definition of the mediterranean diet: A literature review. Nutrients 2015, 7, 9139–9153. [Google Scholar] [CrossRef] [PubMed]
- Anastasiou, C.A.; Yannakoulia, M.; Kosmidis, M.H.; Dardiotis, E.; Hadjigeorgiou, G.M.; Sakka, P.; Arampatzi, X.; Bougea, A.; Labropoulos, I.; Scarmeas, N. Mediterranean diet and cognitive health: Initial results from the Hellenic Longitudinal Investigation of Ageing and Diet. PLoS ONE 2017, 12, e0182048. [Google Scholar] [CrossRef] [PubMed]
- Scarmeas, N.; Stern, Y.; Tang, M.-X.; Luchsinger, J.A. Mediterranean diet and risk for Alzheimer’s disease. Ann. Neurol. 2011, 59, 912–921. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Lapiscina, E.H.; Clavero, P.; Toledo, E.; Estruch, R.; Salas-Salvado, J.; San Julian, B.; Sanchez-Tainta, A.; Ros, E.; Valls-Pedret, C.; Martinez-Gonzalez, M.A. Mediterranean diet improves cognition: the PREDIMED-NAVARRA randomised trial. J. Neurol. Neurosurg. Psychiatry 2013, 84, 1318–1325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valls-Pedret, C.; Sala-Vila, A.; Serra-Mir, M.; Corella, D.; de la Torre, R.; Martinez-Gonzalez, M.A.; Martinez-Lapiscina, E.H.; Fito, M.; Perez-Heras, A.; Salas-Salvado, J.; et al. Mediterranean Diet and Age-Related Cognitive Decline: A Randomized Clinical Trial. JAMA Intern. Med. 2015, 175, 1094–1103. [Google Scholar] [CrossRef] [PubMed]
- Wade, A.T.; Davis, C.R.; Dyer, K.A.; Hodgson, J.M.; Woodman, R.; Keage, H.A.; Murphy, K.J. A Mediterranean diet supplemented with dairy foods improves mood and processing speed in an Australian sample: Results from the MedDairy randomized controlled trial. Nutr. Neurosci. 2018, 1–13. [Google Scholar] [CrossRef]
- Davis, C.R.; Hodgson, J.M.; Woodman, R.; Bryan, J.; Wilson, C.; Murphy, K.J. A Mediterranean diet lowers blood pressure and improves endothelial function: results from the MedLey randomized intervention trial. Am. J. Clin. Nutr. 2017, 105, 1305–1313. [Google Scholar] [CrossRef]
- Martínez-González, M.A.; Salas-Salvadó, J.; Estruch, R.; Corella, D.; Fitó, M.; Ros, E. Benefits of the Mediterranean Diet: Insights From the PREDIMED Study. Prog. Cardiovasc. Dis. 2015, 58, 50–60. [Google Scholar] [CrossRef] [Green Version]
- Feart, C.; Samieri, C.; Barberger-Gateau, P. Mediterranean diet and cognitive function in older adults. Curr. Opin. Clin. Nutr. Metab. Care 2010, 13, 14–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dyall, S.C. Long-chain omega-3 fatty acids and the brain: a review of the independent and shared effects of EPA, DPA and DHA. Front. Aging Neurosci. 2015, 7, 52. [Google Scholar] [CrossRef] [PubMed]
- Australian Institute of Health and Welfare. Dementia and Australia; AIHW: Canberra, Australia, 2012. [CrossRef]
- Davis, C.R.; Bryan, J.; Hodgson, J.M.; Wilson, C.; Murphy, K.J. Older Australians can adhere to a traditional Mediterranean style diet over two weeks: a pilot dietary intervention study. BMC Nutr. 2015, 1. [Google Scholar] [CrossRef]
- Roberts, R.O.; Roberts, L.A.; Geda, Y.E.; Cha, R.H.; Pankratz, V.S.; O’Connor, H.M.; Knopman, D.S.; Petersen, R.C. Relative intake of macronutrients impacts risk of mild cognitive impairment or dementia. J. Alzheimer’s Dis. 2012, 32, 329–339. [Google Scholar] [CrossRef] [PubMed]
- Rae, C.; Digney, A.L.; McEwan, S.R.; Bates, T.C. Oral creatine monohydrate supplementation improves brain performance: a double-blind, placebo-controlled, cross-over trial. Proc. R. Soc. Biol. Sci. 2003, 270, 2147–2150. [Google Scholar] [CrossRef] [PubMed]
- Charlton, K.; Walton, K.; Batterham, M.; Brock, E.; Langford, K.; McMahon, A.; Roodenrys, S.; Koh, F.; Host, A.; Crowe, R.; et al. Pork and Chicken Meals Similarly Impact on Cognitive Function and Strength in Community-Living Older Adults: A Pilot Study. J. Nutr. Gerontol. Geriatr. 2016, 35, 124–145. [Google Scholar] [CrossRef] [PubMed]
- Organisation for Economic Cooperation and Development. Agricultural Output: Meat Consumption; OECD: Paris, France, 2016. [Google Scholar]
- Brinkworth, G.D.; Buckley, J.D.; Hodgson, J.M.; Noakes, M.; Clifton, P.M.; Wilson, C. Long-term Effects of a Very Low-Carbohydrate Diet and a Low-Fat Diet on Mood and Cognitive Function. Arch. Intern. Med. 2009, 169, 1873–1880. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murphy, K.J.; Thomson, R.L.; Coates, A.M.; Buckley, J.D.; Howe, P.R.C. Effects of eating fresh lean pork on cardiometabolic health parameters. Nutrients 2012, 4, 711–723. [Google Scholar] [CrossRef] [PubMed]
- Tilman, D.; Clark, M. Global diets link environmental sustainability and human health. Nature 2014, 515, 518–522. [Google Scholar] [CrossRef]
- Wade, A.T.; Davis, C.R.; Dyer, K.A.; Hodgson, J.M.; Woodman, R.; Murphy, K. Effects of Mediterranean diet supplemented with lean pork on blood pressure and markers of cardiovascular risk: Findings from the MedPork trial. Br. J. Nutr. 2019, June 2019, 1–41. [Google Scholar] [CrossRef]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.-I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary prevention of cardiovascular disease with a Mediterranean diet. N. Engl. J. Med. 2013, 368, 1279–1290. [Google Scholar] [CrossRef] [PubMed]
- Wade, A.T.; Davis, C.R.; Dyer, K.A.; Hodgson, J.M.; Woodman, R.J.; Keage, H.A.; Murphy, K.J. A Mediterranean Diet to Improve Cardiovascular and Cognitive Health: Protocol for a Randomised Controlled Intervention Study. Nutrients 2017, 9, 145. [Google Scholar] [CrossRef] [PubMed]
- Wade, A.T.; Davis, C.R.; Dyer, K.A.; Hodgson, J.M.; Woodman, R.J.; Keage, H.A.D.; Murphy, K.J. Including pork in the Mediterranean diet for an Australian population: Protocol for a randomised controlled trial assessing cardiovascular risk and cognitive function. Nutr. J. 2017, 16. [Google Scholar] [CrossRef] [PubMed]
- National Vascular Disease Prevention Alliance. Absolute Cardiovascular Disease Risk. Guidelines for the Management of Absolute Cardiovascular Disease Risk; National Vascular Disease Prevention Alliance: Melbourne, Australia, 2012. [Google Scholar]
- Scheltens, P.; Twisk, J.W.R.; Blesa, R.; Scarpini, E.; Von Arnim, C.A.F.; Bongers, A.; Harrison, J.; Swinkels, S.H.N.; Stam, C.J.; De Waal, H.; et al. Efficacy of souvenaid in mild alzheimer’s disease: Results from a randomized, controlled trial. J. Alzheimer’s Dis. 2012, 31, 225–236. [Google Scholar] [CrossRef] [PubMed]
- Mastroiacovo, D.; Kwik-Uribe, C.; Grassi, D.; Necozione, S.; Raffaele, A.; Pistacchio, L.; Righetti, R.; Bocale, R.; Lechiara, M.C.; Marini, C.; et al. Cocoa flavanol consumption improves cognitive function, blood pressure control, and metabolic profile in elderly subjects: The Cocoa, Cognition, and Aging (CoCoA) Study—A randomized controlled trial 1–4. Am. J. Clin. Nutr. 2015, 101, 538–548. [Google Scholar] [CrossRef] [PubMed]
- Desideri, G.; Kwik-Uribe, C.; Grassi, D.; Necozione, S.; Ghiadoni, L.; Mastroiacovo, D.; Raffaele, A.; Ferri, L.; Bocale, R.; Lechiara, M.C.; et al. Benefits in cognitive function, blood pressure, and insulin resistance through cocoa flavanol consumption in elderly subjects with mild cognitive impairment: The cocoa, cognition, and aging (CoCoA) study. Hypertension 2012, 60, 794–801. [Google Scholar] [CrossRef] [PubMed]
- Mioshi, E.; Dawson, K.; Mitchell, J.; Arnold, R.; Hodges, J.R. The Addenbrooke’s Cognitive Examination Revised (ACE-R): a brief cognitive test battery for dementia screening. Int. J. Geriatr. Psychiatry 2006, 21, 1078–1085. [Google Scholar] [CrossRef]
- Sanson-Fisher, R.W.; Perkins, J.J. Adaptation and validation of the SF-36 Health Survey for use in Australia. J. Clin. Epidemiol. 1998, 51, 961–967. [Google Scholar] [CrossRef]
- Ware, J.E. SF-36 Physical and Mental Health Summary Scales: A User’s Manual; New England Medical Center Hospital Health Institute: Boston, UK, 1994. [Google Scholar]
- McNair, D.M.; Lorr, M.; Droppleman, L.F. Manual for the Profile of Mood States; Educational and Industrial Testing Services: San Diego, CA, USA, 1971. [Google Scholar]
- Stonehouse, W.; Conlon, C.A.; Podd, J.; Hill, S.R.; Minihane, A.M.; Haskell, C.; Kennedy, D. DHA supplementation improved both memory and reaction time in healthy young adults: A randomized controlled trial. Am. J. Clin. Nutr. 2013, 97, 1134–1143. [Google Scholar] [CrossRef]
- Amen, D.G.; Taylor, D.V.; Ojala, K.; Kaur, J.; Willeumier, K. Effects of brain-directed nutrients on cerebral blood flow and neuropsychological testing: A randomized, double-blind, placebo-controlled, crossover trial. Adv. Mind-Body Med. 2013, 27, 24–33. [Google Scholar]
- Jacobs, H.I.L.; Leritz, E.C.; Williams, V.J.; Van Boxtel, M.P.J.; Elst, W.V.D.; Jolles, J.; Verhey, F.R.J.; McGlinchey, R.E.; Milberg, W.P.; Salat, D.H. Association between white matter microstructure, executive functions, and processing speed in older adults: The impact of vascular health. Hum. Brain Mapp. 2013, 34, 77–95. [Google Scholar] [CrossRef] [PubMed]
- Penke, L.; Maniega, S.M.; Murray, C.; Gow, A.J.; Valdes Hernandez, M.C.; Clayden, J.D.; Starr, J.M.; Wardlaw, J.M.; Bastin, M.E.; Deary, I.J. A General Factor of Brain White Matter Integrity Predicts Information Processing Speed in Healthy Older People. J. Neurosci. 2010, 30, 7569–7574. [Google Scholar] [CrossRef] [PubMed]
- Kochan, N.A.; Bunce, D.; Pont, S.; Crawford, J.D.; Brodaty, H.; Sachdev, P.S. Reaction Time Measures Predict Incident Dementia in Community-Living Older Adults: The Sydney Memory and Ageing Study. Am. J. Geriatr. Psychiatry 2016, 24, 221–231. [Google Scholar] [CrossRef] [PubMed]
- Salthouse, T.A. The processing-speed theory of adult age differences in cognition. Psychol. Rev. 1996, 103, 403–428. [Google Scholar] [CrossRef] [PubMed]
- Salthouse, T.A.; Ferrer-Caja, E. What needs to be explained to account for age-related effects on multiple cognitive variables? Psychol. Aging 2003, 18, 91–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gorus, E.; De Raedt, R.; Lambert, M.; Lemper, J.; Mets, T. Reaction times and performance variability in normal aging, mild cognitive impairment, and Alzheimer’s disease. J. Geriatr. Psychiatry 2008, 21, 204–218. [Google Scholar] [CrossRef]
- Abbott, R.A.; Skirrow, C.; Jokisch, M.; Timmers, M.; Streffer, J.; van Nueten, L.; Krams, M.; Winkler, A.; Pundt, N.; Nathan, P.J.; et al. Normative data from linear and nonlinear quantile regression in CANTAB: Cognition in mid-to-late life in an epidemiological sample. Alzheimer’s Dement. 2019, 11, 36–44. [Google Scholar] [CrossRef]
- Radd-Vagenas, S.; Duffy, S.L.; Naismith, S.L.; Brew, B.J.; Flood, V.M.; Fiatarone Singh, M.A. Effect of the Mediterranean diet on cognition and brain morphology and function: A systematic review of randomized controlled trials. Am. J. Clin. Nutr. 2018, 107, 389–404. [Google Scholar] [CrossRef]
- Strike, S.C.; Carlisle, A.; Gibson, E.L.; Dyall, S.C. A high omega-3 fatty acid multinutrient supplement benefits cognition and mobility in older women: A randomized, double-blind, placebo-controlled pilot study. J. Gerontol. Ser. A Biol. Sci. Med Sci. 2016, 71, 236–242. [Google Scholar] [CrossRef]
- Gomez-Pinilla, F. Brain foods: the effects of nutrients on the brain. Nat. Rev. Neurosci. 2008, 9, 568–578. [Google Scholar] [CrossRef]
- Albaladejo-Blazquez, N.; Ferrer-Cascales, R.; Ruiz-Robledillo, N.; Sanchez-Sansegundo, M.; Clement-Carbonell, V.; Zaragoza-Marti, A. Poor Dietary Habits in Bullied Adolescents: The Moderating Effects of Diet on Depression. Int J Env. Res Public Health 2018, 15, 1569. [Google Scholar] [CrossRef] [PubMed]
- Ferrer-Cascales, R.; Albaladejo-Blázquez, N.; Ruiz-Robledillo, N.; Clement-Carbonell, V.; Sánchez-SanSegundo, M.; Zaragoza-Martí, A. Higher Adherence to the Mediterranean Diet is Related to More Subjective Happiness in Adolescents: The Role of Health-Related Quality of Life. Nutrients 2019, 11, 698. [Google Scholar] [CrossRef] [PubMed]
- Henriquez Sanchez, P.; Ruano, C.; de Irala, J.; Ruiz-Canela, M.; Martinez-Gonzalez, M.A.; Sanchez-Villegas, A. Adherence to the Mediterranean diet and quality of life in the SUN Project. Eur. J. Clin. Nutr. 2012, 66, 360–368. [Google Scholar] [CrossRef] [PubMed]
- Crichton, G.E.; Bryan, J.; Hodgson, J.M.; Murphy, K.J. Mediterranean diet adherence and self-reported psychological functioning in an Australian sample. Appetite 2013, 70, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Parletta, N.; Zarnowiecki, D.; Cho, J.; Wilson, A.; Bogomolova, S.; Villani, A.; Itsiopoulos, C.; Niyonsenga, T.; Blunden, S.; Meyer, B.; et al. A Mediterranean-style dietary intervention supplemented with fish oil improves diet quality and mental health in people with depression: A randomized controlled trial (HELFIMED). Nutr. Neurosci. 2017, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Jacka, F.N.; O’Neil, A.; Opie, R.; Itsiopoulos, C.; Cotton, S.; Mohebbi, M.; Castle, D.; Dash, S.; Mihalopoulos, C.; Chatterton, M.L.; et al. A randomised controlled trial of dietary improvement for adults with major depression (the ‘SMILES’ trial). BMC Med. 2017, 15. [Google Scholar] [CrossRef] [PubMed]
- Miller, A.H.; Maletic, V.; Raison, C.L. Inflammation and Its Discontents: The Role of Cytokines in the Pathophysiology of Major Depression. Biol. Psychiatry 2009, 65, 732–741. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lai, J.S.; Hiles, S.; Bisquera, A.; Hure, A.J.; McEvoy, M.; Attia, J. A systematic review and meta-analysis of dietary patterns and depression in community-dwelling adults. Am. J. Clin. Nutr. 2014, 99, 181–197. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Total (n = 33) | Group 1 (n = 16) | Group 2 (n = 17) | |
|---|---|---|---|
| Age (years) | 61.0 ± 7.1 | 60.2 ± 8.7 | 61.6 ± 5.7 |
| Gender | |||
| Males (%) | 10 (30.3) | 6 (40.0) | 4 (22.2) |
| Females (%) | 23 (69.7) | 9 (60.0) | 14 (77.8) |
| Education (years) | 16.7 ± 4.4 | 15.7 ± 3.5 | 17.5 ± 4.9 |
| Home SBP (mmHg) | 128.9 ± 12.1 | 129.2 ± 14.0 | 128.5 ± 10.4 |
| BMI (kg/m2) | 30.6 ± 5.1 | 31.6 ± 5.7 | 29.8 ± 4.6 |
| ACE-R | 95.1 ± 3.8 | 93.7 ± 4.2 | 96.4 ± 2.8 * |
| MedPork Diet | LF Diet | Estimated Mean Difference between Interventions (MedPork vs LF) at 8 Weeks 2 | p3 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Nutrients | Baseline | Week 8 | Baseline | Week 8 | ||||||
| Mean | SE | Mean | SE | Mean | SE | Mean | SE | (95% CI) | ||
| Energy (MJ/day) | 8.96 ± 0.33 | 8.33 ± 0.33 | 9.00 ± 0.33 | 7.86 ± 0.34 | 0.47 (−0.32, 1.27) | 0.24 | ||||
| % en from protein | 18.40 ± 0.65 | 19.71 ± 0.67 | 19.45 ± 0.66 | 22.21 ± 0.68 | −2.51 (−4.10, 0.91) | <0.01 | ||||
| % en from total fat | 34.08 ± 1.25 | 36.84 ± 0.67 | 34.59 ± 1.27 | 27.52 ± 1.31 | 9.32 (5.91, 12.74) | <0.001 | ||||
| % en from SFA | 12.07 ± 0.57 | 9.18 ± 0.58 | 12.24 ± 0.57 | 9.23 ± 0.59 | −0.05 (−1.41, 1.31) | 0.94 | ||||
| % en from MUFA | 5.41 ± 0.34 | 7.61 ± 0.35 | 5.53 ± 0.35 | 5.05 ± 0.36 | 2.56 (1.61, 3.51) | <0.001 | ||||
| % en from PUFA | 13.89 ± 0.76 | 17.37 ± 0.79 | 14.16 ± 0.077 | 10.68 ± 0.80 | 6.69 (4.55, 8.83) | <0.001 | ||||
| MUFA:SFA 4 | 1.24 ± 0.09 | 1.99 ± 0.09 | 1.19 ± 0.09 | 1.18 ± 0.09 | 1.69 (1.46, 1.95) | <0.001 | ||||
| % en from CHO | 39.50 ± 1.37 | 35.23 ± 1.37 | 38.59 ± 1.35 | 41.23 ± 1.39 | −6.00 (−9.22, −2.79) | <0.001 | ||||
| % en from alcohol | 4.41 ± 0.81 | 3.45 ± 0.82 | 3.54 ± 0.82 | 3.99 ± 0.83 | −0.55 (−1.75, 0.65) | 0.37 | ||||
| Cholesterol (mg/MJ) 4 | 37.76 ± 0.34 | 33.64 ± 3.48 | 43.57 ± 3.44 | 38.97 ± 3.58 | 0.82 (0.68, 1.01) | 0.06 | ||||
| Fibre (g/MJ) | 3.03 ± 0.19 | 3.98 ± 0.19 | 3.06 ± 0.19 | 3.84 ± 0.20 | 0.14 (−0.31, 0.59) | 0.54 | ||||
| Vitamin C (mg/MJ) 4 | 11.34 ± 0.39 | 21.53 ± 1.56 | 12.53 ± 1.51 | 17.26 ± 1.58 | 0.81 (0.96, 1.59) | 0.10 | ||||
| Vitamin E (mg/MJ) 4 | 1.64 ± 0.11 | 2.14 ± 0.12 | 1.47 ± 0.12 | 1.40 ± 0.12 | 1.57 (1.33, 1.85) | <0.001 | ||||
| Total vit A equiv. (mg/MJ) 4 | 0.11 ± 0.01 | 0.13 ± 0.01 | 0.12 ± 0.01 | 0.12 ± 0.01 | 0.01(−0.01, 0.01) | 0.96 | ||||
| Total folate (µg/MJ) | 61.65 ± 3.56 | 68.28 ± 3.68 | 63.94 ± 3.63 | 81.11 ± 3.74 | −12.83 (−21.57, 4.09) | <0.01 | ||||
| β-carotene equiv. (mg/MJ) 4 | 0.49 ± 0.08 | 0.67 ± 0.08 | 0.51 ± 0.08 | 0.58 ± 0.08 | 0.01 (−0.01, 0.01) | 0.45 | ||||
| Sodium (g/MJ) | 0.28 ± 0.02 | 0.24 ± 0.02 | 0.32 ± 0.02 | 0.28 ± 0.02 | −0.04 (−0.08, 0.01) | 0.06 | ||||
| Calcium (g/MJ) | 0.10 ± 0.01 | 0.11 ± 0.01 | 0.11 ± 0.01 | 0.12 ± 0.01 | −0.01 (−0.02, 0.01) | 0.14 | ||||
| Iron (mg/MJ) 4 | 1.48 ± 0.07 | 1.48 ± 0.07 | 1.39 ± 0.07 | 1.63 ± 0.07 | 0.93 (0.82, 1.05) | 0.21 | ||||
| Zinc (mg/MJ) | 1.32 ± 0.06 | 1.27 ± 0.06 | 1.30 ± 0.06 | 1.40 ± 0.06 | −0.12 (−0.26, 0.01) | 0.07 | ||||
| Linoleic acid (g/MJ) | 1.18 ± 0.08 | 1.69 ± 0.08 | 1.23 ± 0.08 | 1.11 ± 0.09 | 0.59 (0.36, 0.81) | <0.001 | ||||
| α-linolenic acid (g/MJ) 4 | 0.17 ± 0.01 | 0.23 ± 0.02 | 0.16 ± 0.02 | 0.16 ± 0.02 | 1.49 (1.19, 1.86) | <0.001 | ||||
| Servings/day | ||||||||||
| Whole grains 4 | 2.14 ± 0.26 | 2.44 ± 0.27 | 1.70 ± 0.26 | 2.03 ± 0.27 | 1.49 (0.88, 2.54) | 0.14 | ||||
| Refined grains 4 | 3.61 ± 0.37 | 1.96 ± 0.38 | 3.84 ± 0.38 | 3.45 ± 0.38 | 0.65 (0.49, 0.85) | <0.01 | ||||
| Fruits | 1.30 ± 0.17 | 2.20 ± 0.18 | 1.57 ± 0.18 | 1.74 ± 0.18 | 0.46 (0.05, 0.86) | 0.03 | ||||
| Vegetables 4 | 4.39 ± 0.60 | 5.83 ± 0.62 | 3.66 ± 0.61 | 5.02 ± 0.64 | 1.25 (0.95, 1.62) | 0.10 | ||||
| Legumes 4 | 0.19 ± 0.09 | 0.63 ± 0.09 | 0.23 ± 0.09 | 0.35 ± 0.09 | 1.90 (1.19, 3.04) | <0.01 | ||||
| Meat/meat altern. | 2.71 ± 0.19 | 3.43 ± 0.20 | 2.95 ± 0.20 | 2.62 ± 0.20 | 0.81 (0.34, 1.27) | <0.001 | ||||
| Red meat 4 | 0.64 ± 0.13 | 0.85 ± 0.13 | 0.78 ± 0.13 | 0.71 ± 0.13 | 1.09 (0.95, 1.25) | 0.24 | ||||
| Fresh pork 4 | 0.09 ± 0.05 | 0.44 ± 0.06 | 0.16 ± 0.05 | 0.13 ± 0.05 | 1.13 (1.06, 1.20) | <0.001 | ||||
| Seafood 4 | 0.38 ± 0.08 | 0.64 ± 0.08 | 0.30 ± 0.08 | 0.39 ± 0.08 | 1.19 (1.05, 1.36) | <0.01 | ||||
| Nuts and seeds 4 | 0.47 ± 0.08 | 0.96 ± 0.08 | 0.50 ± 0.08 | 0.22 ± 0.08 | 1.61 (1.42, 1.84) | <0.001 | ||||
| Total dairy 4 | 1.80 ± 0.20 | 1.60 ± 0.20 | 1.92 ± 0.20 | 1.93 ± 0.20 | 0.85 (0.64, 1.11) | 0.23 | ||||
| EVOO (tsp/day) 4 | 1.14 ± 0.39 | 4.51 ± 0.39 | 1.15 ± 0.39 | 0.68 ± 0.39 | 2.83 (2.20, 3.65) | <0.001 | ||||
| MedPork Diet | LF Diet | Estimated Mean Difference between Interventions (MedPork vs LF) at 8 Weeks 2 | p3 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | Week 8 | Baseline | Week 8 | |||||||
| Mean | SE | Mean | SE | Mean | SE | Mean | SE | (95% CI) | ||
| Attention | −0.14 ± 0.11 | 0.17 ± 0.11 | −0.06 ± 0.11 | 0.14 ± 0.11 | 0.04 (−0.14, 0.21) | 0.70 | ||||
| Processing speed | −0.04 ± 0.16 | 0.13 ± 0.16 | 0.01 ± 0.16 | −0.19 ± 0.16 | 0.32 (0.08, 0.57) | 0.01 | ||||
| Memory | 0.04 ± 0.09 | -0.08 ± 0.09 | 0.03 ± 0.09 | 0.07 ± 0.09 | −0.15 (−0.31, 0.01) | 0.06 | ||||
| Planning | −0.18 ± 0.11 | 0.15 ± 0.11 | −0.05 ± 0.11 | 0.09 ± 0.11 | 0.06 (−0.14, 0.26) | 0.56 | ||||
| ACE-R | 95.98 ± 0.52 | 96.19 ± 0.53 | 95.13 ± 0.52 | 96.37 ± 0.53 | −0.18 (−1.12, 0.76) | 0.71 | ||||
| MedPork Diet | LF Diet | Estimated Mean Difference between Interventions (MedPork vs LF) at 8 Weeks 3 | p4 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Normative Data 2 | Baseline | Week 8 | Baseline | Week 8 | |||||||
| Mean (SD) | Mean + SE | Mean + SE | Mean + SE | Mean + SE | (95% CI) | ||||||
| SF-36 Health Survey | |||||||||||
| Physical functioning 5 | 92.5 (13.4) | 81.57 ± 2.88 | 85.82 ± 2.96 | 83.56 ± 2.96 | 83.47 ± 2.95 | 0.95 (0.64, 1.38) | 0.80 | ||||
| Role physical 5 | 91.4 (23.2) | 84.58 ± 3.19 | 91.54 ± 3.35 | 84.88 ± 3.13 | 88.95 ± 3.33 | 0.71 (0.38, 1.32) | 0.27 | ||||
| Bodily pain | 86.3 (17.9) | 71.54 ± 3.36 | 78.66 ± 3.47 | 75.72 ± 3.33 | 74.74 ± 3.47 | 3.92 (−1.84, 9.67) | 0.18 | ||||
| General health | 78.8 (15.7) | 68.84 ± 3.39 | 74.18 ± 3.46 | 71.12 ± 3.38 | 74.99 ± 3.45 | −0.80 (−5.14, 3.54) | 0.72 | ||||
| Vitality | 64.0 (18.2) | 61.45 ± 3.05 | 65.51 ± 3.19 | 64.11 ± 3.02 | 67.89 ±3.18 | −2.37 (−8.54, 3.79) | 0.45 | ||||
| Social functioning 5 | 91.3 (15.8) | 89.96 ± 2.80 | 89.93 ± 2.97 | 89.64 ± 2.73 | 91.71 ± 2.95 | 1.05 (0.56, 2.00) | 0.87 | ||||
| Role emotional 5 | 85.6 (29.3) | 93.26 ± 2.22 | 96.87 ± 2.33 | 91.67 ± 2.18 | 91.30 ± 2.32 | 0.55 (0.32, 1.05) | 0.03 | ||||
| Mental health 5 | 75.4 (16.3) | 82.97 ±1.96 | 85.80 ±2.01 | 83.70 ±1.92 | 83.61 ±1.98 | 0.83 (0.66, 1.05) | 0.10 | ||||
| Physical component score | - | 49.60 +1.34 | 52.27 + 1.36 | 50.98 + 1.34 | 51.61 + 1.37 | 0.65 (−1.23, 2.54) | 0.47 | ||||
| Mental component score | - | 54.92 + 1.08 | 55.68 + 1.11 | 55.00 + 1.08 | 54.40 + 1.12 | 1.29 (−0.63, 3.20) | 0.19 | ||||
| POMS | |||||||||||
| Tension 5 | 7.0 (5.5) | 5.27 ±0.75 | 4.54 ±0.76 | 5.29 ±0.76 | 5.20 ±0.76 | 0.87 (0.71, 1.07) | 0.20 | ||||
| Depression 5 | 7.1 (8.4) | 3.50 ± 0.63 | 2.36 ± 0.64 | 3.21 ± 0.63 | 3.59 ± 0.63 | 0.77 (0.58, 1.02) | 0.08 | ||||
| Anger 5 | 6.6 (6.7) | 3.81 ± 0.67 | 3.01 ± 0.67 | 3.06 ± 0.67 | 3.71 ± 0.67 | 0.85 (0.68, 1.10) | 0.20 | ||||
| Confusion 5 | 5.2 (4.1) | 4.34 ± 0.57 | 3.97 ± 0.58 | 4.21 ± 0.58 | 3.89 ± 0.59 | 1.10 (0.91, 1.29) | 0.36 | ||||
| Fatigue 5 | 7.3 (5.7) | 5.85 ± 0.75 | 5.14 ± 0.77 | 6.09 ± 0.77 | 6.53 ± 0.77 | 0.87 (0.68, 1.12) | 0.31 | ||||
| Vigour | 20.2 (6.2) | 18.36 ± 1.11 | 19.15 ± 0.12 | 17.90 ± 1.12 | 18.12 ± 1.12 | 1.03 (−0.23, 2.28) | 0.11 | ||||
| Total Mood Disturbance 5 | 12.7 (29.6) | 5.81 ±0.32 | 5.41 ±0.32 | 5.77 ±0.32 | 5.80 ±0.32 | 0.87 (0.72, 1.05) | 0.12 | ||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wade, A.T.; Davis, C.R.; Dyer, K.A.; Hodgson, J.M.; Woodman, R.J.; Keage, H.A.D.; Murphy, K.J. A Mediterranean Diet with Fresh, Lean Pork Improves Processing Speed and Mood: Cognitive Findings from the MedPork Randomised Controlled Trial. Nutrients 2019, 11, 1521. https://doi.org/10.3390/nu11071521
Wade AT, Davis CR, Dyer KA, Hodgson JM, Woodman RJ, Keage HAD, Murphy KJ. A Mediterranean Diet with Fresh, Lean Pork Improves Processing Speed and Mood: Cognitive Findings from the MedPork Randomised Controlled Trial. Nutrients. 2019; 11(7):1521. https://doi.org/10.3390/nu11071521
Chicago/Turabian StyleWade, Alexandra T., Courtney R. Davis, Kathryn A. Dyer, Jonathan M. Hodgson, Richard J. Woodman, Hannah A. D. Keage, and Karen J. Murphy. 2019. "A Mediterranean Diet with Fresh, Lean Pork Improves Processing Speed and Mood: Cognitive Findings from the MedPork Randomised Controlled Trial" Nutrients 11, no. 7: 1521. https://doi.org/10.3390/nu11071521