Effects of Lactobacillus plantarum PS128 on Children with Autism Spectrum Disorder in Taiwan: A Randomized, Double-Blind, Placebo-Controlled Trial

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. PS128 and Placebo Products
2.2. Study Design
2.2.1. Selection of Subjects
2.2.2. Study Protocol
2.3. Analyses
2.3.1. ABC-T
2.3.2. SRS-Taiwan Version
2.3.3. CBCL
2.3.4. CGI-S and CGI-I
2.3.5. SNAP–IV
2.4. Statistical Analyses
3. Results
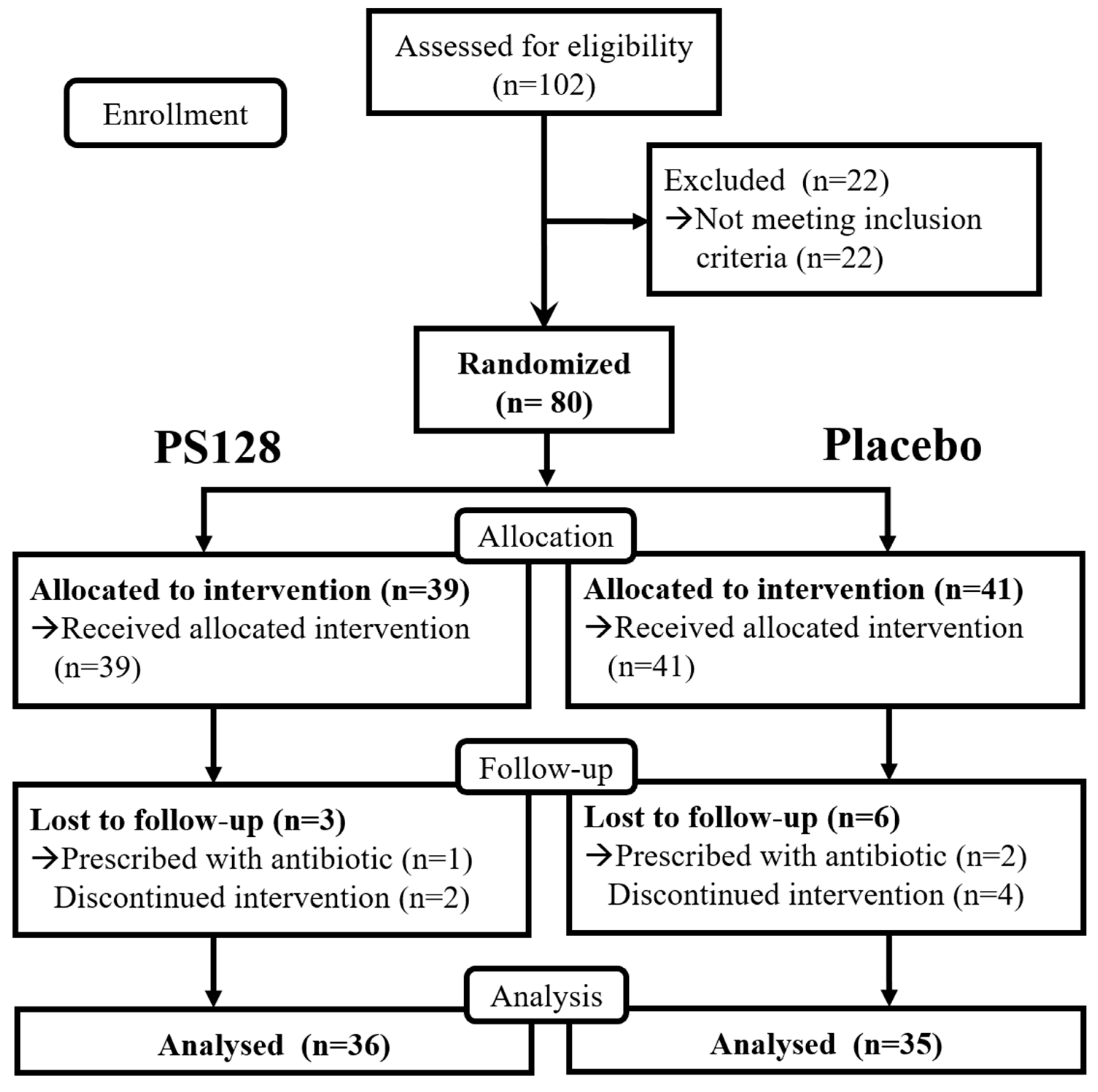
3.1. Baseline Demographics
3.2. Outcomes Measurement
3.2.1. CGI-I
3.2.2. ABC-T
3.2.3. SRS
3.2.4. CBCL
3.2.5. SNAP-IV
3.3. Analysis Stratified by Age
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®), 5th ed.; American Psychiatric Publishing: Washington, DC, USA, 2013. [Google Scholar]
- Veenstra-Vanderweele, J.; Christian, S.L.; Cook, E.H., Jr. Autism as a paradigmatic complex genetic disorder. Annu. Rev. Genom. Hum. Genet. 2004, 5, 379–405. [Google Scholar] [CrossRef] [PubMed]
- Kuo, P.H.; Chuang, L.C.; Su, M.H.; Chen, C.H.; Wu, J.Y.; Yen, C.J.; Wu, Y.Y.; Liu, S.K.; Chou, M.C.; Chou, W.J.; et al. Genome-wide association study for autism spectrum disorder in Taiwanese Han population. PLoS ONE 2015, 10, e0138695. [Google Scholar] [CrossRef] [PubMed]
- Moosa, A.; Shu, H.; Sarachana, T.; Hu, V.W. Are endocrine disrupting compounds environmental risk factors for autism spectrum disorder? Horm. Behav. 2017. [Google Scholar] [CrossRef] [PubMed]
- Strasser, L.; Downes, M.; Kung, J.; Cross, J.H.; De Haan, M. Prevalence and risk factors for autism spectrum disorder in epilepsy: A systematic review and meta-analysis. Dev. Med. Child Neurol. 2017. [Google Scholar] [CrossRef]
- Muhle, R.A.; Reed, H.E.; Stratigos, K.A.; Veenstra-VanderWeele, J. The emerging clinical neuroscience of autism spectrum disorder: A review. JAMA Psychiatry 2018. [Google Scholar] [CrossRef] [PubMed]
- Lotter, V. Epidemiology of autistic conditions in young children. Soc Psychiatry 1966, 1, 124–135. [Google Scholar] [CrossRef]
- Iwainsky, H. Mode of Action, Biotransformation and Pharmacokinetics of Antituberculosis Drugs in Animals and Man; Springer: Berlin/Heidelberg, Germany, 1988. [Google Scholar] [CrossRef]
- Prevalence of Autism Spectrum Disorders—Autism and Developmental Disabilities Monitoring Network, United States. 2006. Available online: https://www.cdc.gov/mmwr/preview/mmwrhtml/ss5810a1.htm (accessed on 28 March 2019).
- Baio, J.; Wiggins, L.; Christensen, D.L.; Maenner, M.J.; Daniels, J.; Warren, Z.; Kurzius-Spencer, M.; Zahorodny, W.; Robinson Rosenberg, C.; White, T.; et al. Prevalence of autism spectrum disorder among children aged 8 years—Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2014. Morb. Mortal. Wkly. Rep. Surveill. Summ. 2018, 67, 1–23. [Google Scholar] [CrossRef]
- Chien, Y.L.; Chou, M.C.; Chiu, Y.N.; Chou, W.J.; Wu, Y.Y.; Tsai, W.C.; Gau, S.S. ADHD-related symptoms and attention profiles in the unaffected siblings of probands with autism spectrum disorder: Focus on the subtypes of autism and Asperger’s disorder. Mol. Autism 2017, 8, 37. [Google Scholar] [CrossRef]
- Taurines, R.; Schwenck, C.; Westerwald, E.; Sachse, M.; Siniatchkin, M.; Freitag, C. ADHD and autism: Differential diagnosis or overlapping traits? A selective review. ADHD Atten. Deficit Hyperact. Disord. 2012, 4, 115–139. [Google Scholar] [CrossRef]
- De Boo, G.M.; Prins, P.J. Social incompetence in children with ADHD: Possible moderators and mediators in social-skills training. Clin. Psychol. Rev. 2007, 27, 78–97. [Google Scholar] [CrossRef]
- Gau, S.S.; Shang, C.Y.; Liu, S.K.; Lin, C.H.; Swanson, J.M.; Liu, Y.C.; Tu, C.L. Psychometric properties of the Chinese version of the Swanson, Nolan, and Pelham, version IV scale—Parent form. Int. J. Methods Psychiatr. Res. 2008, 17, 35–44. [Google Scholar] [CrossRef]
- Autism: Beware of Potentially Dangerous Therapies and Products. Available online: https://www.fda.gov/ForConsumers/ConsumerUpdates/ucm394757.htm (accessed on 24 March 2019).
- Label for Risperdal—FDA. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2009/020272s056,020588s044,021346s033,021444s03lbl.pdf (accessed on 24 March 2019).
- Ospina, M.B.; Krebs Seida, J.; Clark, B.; Karkhaneh, M.; Hartling, L.; Tjosvold, L.; Vandermeer, B.; Smith, V. Behavioural and developmental interventions for autism spectrum disorder: A clinical systematic review. PLoS ONE 2008, 3, e3755. [Google Scholar] [CrossRef]
- Sharma, S.R.; Gonda, X.; Tarazi, F.I. Autism spectrum disorder: Classification, diagnosis and therapy. Pharmacol. Ther. 2018. [Google Scholar] [CrossRef]
- El-Rashidy, O.; El-Baz, F.; El-Gendy, Y.; Khalaf, R.; Reda, D.; Saad, K. Ketogenic diet versus gluten free casein free diet in autistic children: A case-control study. Metab. Brain Dis. 2017, 32, 1935–1941. [Google Scholar] [CrossRef]
- Mychasiuk, R.; Rho, J.M. Genetic modifications associated with ketogenic diet treatment in the BTBRT+Tf/J mouse model of autism spectrum disorder. Autism Res. 2017, 10, 456–471. [Google Scholar] [CrossRef]
- Mazahery, H.; Camargo, C.A., Jr.; Conlon, C.; Beck, K.L.; Kruger, M.C.; von Hurst, P.R. Vitamin D and autism spectrum disorder: A literature review. Nutrients 2016, 8, 236. [Google Scholar] [CrossRef]
- Cheng, Y.S.; Tseng, P.T.; Chen, Y.W.; Stubbs, B.; Yang, W.C.; Chen, T.Y.; Wu, C.K.; Lin, P.Y. Supplementation of omega 3 fatty acids may improve hyperactivity, lethargy, and stereotypy in children with autism spectrum disorders: A meta-analysis of randomized controlled trials. Neuropsychiatr. Dis. Treat. 2017, 13, 2531–2543. [Google Scholar] [CrossRef]
- Ooi, Y.P.; Weng, S.J.; Jang, L.Y.; Low, L.; Seah, J.; Teo, S.; Ang, R.P.; Lim, C.G.; Liew, A.; Fung, D.S.; et al. Omega-3 fatty acids in the management of autism spectrum disorders: Findings from an open-label pilot study in Singapore. Eur. J. Clin. Nutr. 2015, 69, 969–971. [Google Scholar] [CrossRef]
- Sheppard, K.W.; Boone, K.M.; Gracious, B.; Klebanoff, M.A.; Rogers, L.K.; Rausch, J.; Bartlett, C.; Coury, D.L.; Keim, S.A. Effect of omega-3 and -6 supplementation on language in preterm toddlers exhibiting autism spectrum disorder symptoms. J. Autism Dev. Disord. 2017, 47, 3358–3369. [Google Scholar] [CrossRef]
- Bostock, E.C.; Kirkby, K.C.; Taylor, B.V. The current status of the ketogenic diet in psychiatry. Front. Psychiatry 2017, 8, 43. [Google Scholar] [CrossRef]
- Horvath, A.; Lukasik, J.; Szajewska, H. Omega-3 fatty acid supplementation does not affect autism spectrum disorder in children: A systematic review and meta-analysis. J. Nutr. 2017, 147, 367–376. [Google Scholar] [CrossRef] [PubMed]
- Sathe, N.; Andrews, J.C.; McPheeters, M.L.; Warren, Z.E. Nutritional and dietary interventions for autism spectrum disorder: A systematic review. Pediatrics 2017, 139. [Google Scholar] [CrossRef] [PubMed]
- Dinan, T.G.; Cryan, J.F. Microbes, immunity, and behavior: Psychoneuroimmunology meets the microbiome. Neuropsychopharmacology 2017, 42, 178–192. [Google Scholar] [CrossRef] [PubMed]
- Zhou, L.; Foster, J.A. Psychobiotics and the gut-brain axis: In the pursuit of happiness. Neuropsychiatr. Dis. Treat. 2015, 11, 715–723. [Google Scholar] [CrossRef] [PubMed]
- Savignac, H.M.; Kiely, B.; Dinan, T.G.; Cryan, J.F. Bifidobacteria exert strain-specific effects on stress-related behavior and physiology in BALB/c mice. Neurogastroenterol. Motil. 2014, 26, 1615–1627. [Google Scholar] [CrossRef] [PubMed]
- Savignac, H.M.; Tramullas, M.; Kiely, B.; Dinan, T.G.; Cryan, J.F. Bifidobacteria modulate cognitive processes in an anxious mouse strain. Behav. Brain Res. 2015, 287, 59–72. [Google Scholar] [CrossRef]
- McVey Neufeld, K.A.; O’Mahony, S.M.; Hoban, A.E.; Waworuntu, R.V.; Berg, B.M.; Dinan, T.G.; Cryan, J.F. Neurobehavioural effects of Lactobacillus rhamnosus GG alone and in combination with prebiotics polydextrose and galactooligosaccharide in male rats exposed to early-life stress. Nutr. Neurosci. 2017. [Google Scholar] [CrossRef] [PubMed]
- Allen, A.P.; Clarke, G.; Cryan, J.F.; Quigley, E.M.M.; Dinan, T.G. Bifidobacterium infantis 35624 and other probiotics in the management of irritable bowel syndrome. Strain specificity, symptoms, and mechanisms. Curr. Med Res. Opin. 2017, 33, 1349–1351. [Google Scholar] [CrossRef] [PubMed]
- Slykerman, R.F.; Hood, F.; Wickens, K.; Thompson, J.M.D.; Barthow, C.; Murphy, R.; Kang, J.; Rowden, J.; Stone, P.; Crane, J.; et al. Effect of Lactobacillus rhamnosus HN001 in pregnancy on postpartum symptoms of depression and anxiety: A randomised double-blind placebo-controlled trial. EBioMedicine 2017, 24, 159–165. [Google Scholar] [CrossRef]
- Wang, L.W.; Tancredi, D.J.; Thomas, D.W. The prevalence of gastrointestinal problems in children across the United States with autism spectrum disorders from families with multiple affected members. J. Dev. Behav. Pediatrics JDBP 2011, 32, 351–360. [Google Scholar] [CrossRef]
- Chaidez, V.; Hansen, R.L.; Hertz-Picciotto, I. Gastrointestinal problems in children with autism, developmental delays or typical development. J. Autism Dev. Disord. 2014, 44, 1117–1127. [Google Scholar] [CrossRef] [PubMed]
- Ding, H.T.; Taur, Y.; Walkup, J.T. Gut microbiota and autism: Key concepts and findings. J. Autism Dev. Disord. 2017, 47, 480–489. [Google Scholar] [CrossRef] [PubMed]
- Strati, F.; Cavalieri, D.; Albanese, D.; De Felice, C.; Donati, C.; Hayek, J.; Jousson, O.; Leoncini, S.; Renzi, D.; Calabro, A.; et al. New evidences on the altered gut microbiota in autism spectrum disorders. Microbiome 2017, 5, 24. [Google Scholar] [CrossRef] [PubMed]
- Son, J.S.; Zheng, L.J.; Rowehl, L.M.; Tian, X.; Zhang, Y.; Zhu, W.; Litcher-Kelly, L.; Gadow, K.D.; Gathungu, G.; Robertson, C.E.; et al. Comparison of fecal microbiota in children with autism spectrum disorders and neurotypical siblings in the simons simplex collection. PLoS ONE 2015, 10, e0137725. [Google Scholar] [CrossRef]
- Kang, D.W.; Ilhan, Z.E.; Isern, N.G.; Hoyt, D.W.; Howsmon, D.P.; Shaffer, M.; Lozupone, C.A.; Hahn, J.; Adams, J.B.; Krajmalnik-Brown, R. Differences in fecal microbial metabolites and microbiota of children with autism spectrum disorders. Anaerobe 2018, 49, 121–131. [Google Scholar] [CrossRef] [PubMed]
- Tomova, A.; Husarova, V.; Lakatosova, S.; Bakos, J.; Vlkova, B.; Babinska, K.; Ostatnikova, D. Gastrointestinal microbiota in children with autism in Slovakia. Physiol. Behav. 2015, 138, 179–187. [Google Scholar] [CrossRef]
- Kang, D.W.; Adams, J.B.; Gregory, A.C.; Borody, T.; Chittick, L.; Fasano, A.; Khoruts, A.; Geis, E.; Maldonado, J.; McDonough-Means, S.; et al. Microbiota Transfer Therapy alters gut ecosystem and improves gastrointestinal and autism symptoms: An open-label study. Microbiome 2017, 5, 10. [Google Scholar] [CrossRef] [PubMed]
- FAO/WHO. Probiotics in Food. Health and Nutritional Properties and Guidelines for Evaluation; FAO: Rome, Italy, 2006. [Google Scholar]
- Ewe, J.A.; Wan-Abdullah, W.N.; Liong, M.T. Viability and growth characteristics of Lactobacillus in soymilk supplemented with B-vitamins. Int. J. Food Sci. Nutr. 2010, 61, 87–107. [Google Scholar] [CrossRef]
- Liong MT, S.N. Bile salt deconjugation and BSH activity of five bifidobacterial strains and their cholesterol co-precipitating properties. Food Res. Int. 2005, 38, 135–142. [Google Scholar] [CrossRef]
- Dinan, T.G.; Stanton, C.; Cryan, J.F. Psychobiotics: A novel class of psychotropic. Biol. Psychiatry 2013, 74, 720–726. [Google Scholar] [CrossRef]
- Desbonnet, L.; Garrett, L.; Clarke, G.; Bienenstock, J.; Dinan, T.G. The probiotic Bifidobacteria infantis: An assessment of potential antidepressant properties in the rat. J. Psychiatr. Res. 2008, 43, 164–174. [Google Scholar] [CrossRef]
- Liu, Y.W.; Liu, W.H.; Wu, C.C.; Juan, Y.C.; Wu, Y.C.; Tsai, H.P.; Wang, S.; Tsai, Y.C. Psychotropic effects of Lactobacillus plantarum PS128 in early life-stressed and naive adult mice. Brain Res. 2016, 1631, 1–12. [Google Scholar] [CrossRef]
- Liang, S.; Wang, T.; Hu, X.; Luo, J.; Li, W.; Wu, X.; Duan, Y.; Jin, F. Administration of Lactobacillus helveticus NS8 improves behavioral, cognitive, and biochemical aberrations caused by chronic restraint stress. Neuroscience 2015, 310, 561–577. [Google Scholar] [CrossRef]
- Bravo, J.A.; Forsythe, P.; Chew, M.V.; Escaravage, E.; Savignac, H.M.; Dinan, T.G.; Bienenstock, J.; Cryan, J.F. Ingestion of Lactobacillus strain regulates emotional behavior and central GABA receptor expression in a mouse via the vagus nerve. Proc. Natl. Acad. Sci. USA 2011, 108, 16050–16055. [Google Scholar] [CrossRef]
- Liu, W.H.; Chuang, H.L.; Huang, Y.T.; Wu, C.C.; Chou, G.T.; Wang, S.; Tsai, Y.C. Alteration of behavior and monoamine levels attributable to Lactobacillus plantarum PS128 in germ-free mice. Behav. Brain Res. 2016, 298, 202–209. [Google Scholar] [CrossRef]
- Desbonnet, L.; Garrett, L.; Clarke, G.; Kiely, B.; Cryan, J.F.; Dinan, T.G. Effects of the probiotic Bifidobacterium infantis in the maternal separation model of depression. Neuroscience 2010, 170, 1179–1188. [Google Scholar] [CrossRef]
- Gareau, M.G.; Wine, E.; Rodrigues, D.M.; Cho, J.H.; Whary, M.T.; Philpott, D.J.; Macqueen, G.; Sherman, P.M. Bacterial infection causes stress-induced memory dysfunction in mice. Gut 2011, 60, 307–317. [Google Scholar] [CrossRef]
- Jeong, J.J.; Kim, K.A.; Ahn, Y.T.; Sim, J.H.; Woo, J.Y.; Huh, C.S.; Kim, D.H. Probiotic mixture KF attenuates age-dependent memory deficit and lipidemia in Fischer 344 rats. J. Microbiol. Biotechnol. 2015, 25, 1532–1536. [Google Scholar] [CrossRef]
- Davari, S.; Talaei, S.A.; Alaei, H.; Salami, M. Probiotics treatment improves diabetes-induced impairment of synaptic activity and cognitive function: Behavioral and electrophysiological proofs for microbiome-gut-brain axis. Neuroscience 2013, 240, 287–296. [Google Scholar] [CrossRef]
- Hsiao, E.Y.; McBride, S.W.; Hsien, S.; Sharon, G.; Hyde, E.R.; McCue, T.; Codelli, J.A.; Chow, J.; Reisman, S.E.; Petrosino, J.F.; et al. Microbiota modulate behavioral and physiological abnormalities associated with neurodevelopmental disorders. Cell 2013, 155, 1451–1463. [Google Scholar] [CrossRef]
- Chao, S.H.; Wu, R.J.; Watanabe, K.; Tsai, Y.C. Diversity of lactic acid bacteria in suan-tsai and fu-tsai, traditional fermented mustard products of Taiwan. Int. J. Food Microbiol. 2009, 135, 203–210. [Google Scholar] [CrossRef]
- Mahdavi, M.; Kheirollahi, M.; Riahi, R.; Khorvash, F.; Khorrami, M.; Mirsafaie, M. Meta-analysis of the association between GABA receptor polymorphisms and autism spectrum disorder (ASD). J. Mol. Neurosci. MN 2018. [Google Scholar] [CrossRef] [PubMed]
- Israelyan, N.; Margolis, K.G. Serotonin as a link between the gut-brain-microbiome axis in autism spectrum disorders. Pharmacol. Res. 2018, 132, 1–6. [Google Scholar] [CrossRef]
- Hamilton, P.J.; Campbell, N.G.; Sharma, S.; Erreger, K.; Herborg Hansen, F.; Saunders, C.; Belovich, A.N.; Sahai, M.A.; Cook, E.H.; Gether, U.; et al. De novo mutation in the dopamine transporter gene associates dopamine dysfunction with autism spectrum disorder. Mol. Psychiatry 2013, 18, 1315–1323. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.H.; Yang, C.H.; Lin, C.T.; Li, S.W.; Cheng, W.S.; Jiang, Y.P.; Wu, C.C.; Chang, C.H.; Tsai, Y.C. Genome architecture of Lactobacillus plantarum PS128, a probiotic strain with potential immunomodulatory activity. Gut Pathog. 2015, 7, 22. [Google Scholar] [CrossRef] [PubMed]
- Lord, C.; Rutter, M.; Le Couteur, A. Autism diagnostic interview-revised: A revised version of a diagnostic interview for caregivers of individuals with possible pervasive developmental disorders. J. Autism Dev. Disord. 1994, 24, 659–685. [Google Scholar] [CrossRef] [PubMed]
- Krug, D.A.; Arick, J.; Almond, P. Behavior checklist for identifying severely handicapped individuals with high levels of autistic behavior. J. Child Psychol. Psychiatry 1980, 21, 221–229. [Google Scholar] [CrossRef] [PubMed]
- Constantino, J.N.; Gruber, C.P. Social Responsiveness Scale (SRS) Manual; Western Psychological Services: Los Angeles, CA, USA, 2005. [Google Scholar]
- Gau, S.S.-F.; Liu, L.-T.; Wu, Y.-Y.; Chiu, Y.-N.; Tsai, W.-C. Psychometric properties of the Chinese version of the Social Responsiveness Scale. Res. Autism Spectr. Disord. 2013, 7, 349–360. [Google Scholar] [CrossRef]
- Achenbach, T.M. Manual for the Child Behavior Checklist/4-18 and 1991 Profile; Department of Psychiatry, University of Vermont: Burlington, VT, USA, 1991. [Google Scholar]
- Kuo, P.H.; Lin, C.C.; Yang, H.J.; Soong, W.T.; Chen, W.J. A twin study of competence and behavioral/emotional problems among adolescents in Taiwan. Behav. Genet. 2004, 34, 63–74. [Google Scholar] [CrossRef]
- Wadsworth, M.E.; Hudziak, J.J.; Heath, A.C.; Achenbach, T.M. Latent class analysis of child behavior checklist anxiety/depression in children and adolescents. J. Am. Acad. Child Adolesc. Psychiatry 2001, 40, 106–114. [Google Scholar] [CrossRef]
- Guy, W. ECDEU Assessment Manual for Psychopharmacology; U.S. Department of Health, Education, and Welfare Public Health Service; Alcohol, Drug Abuse, and Mental Health Administration; National Institute of Mental Health; Psychopharmacology Research Branch; Division of Extramural Research Programs: Rockville, MD, USA, 1976. [Google Scholar]
- Swanson, J.M.; Kraemer, H.C.; Hinshaw, S.P.; Arnold, L.E.; Conners, C.K.; Abikoff, H.B.; Clevenger, W.; Davies, M.; Elliott, G.R.; Greenhill, L.L.; et al. Clinical relevance of the primary findings of the MTA: Success rates based on severity of ADHD and ODD symptoms at the end of treatment. J. Am. Acad. Child Adolesc. Psychiatry 2001, 40, 168–179. [Google Scholar] [CrossRef]
- The MTA Cooperative Group. A 14-month randomized clinical trial of treatment strategies for attention-deficit/hyperactivity disorder. The MTA cooperative group. Multimodal treatment study of children with ADHD. Arch. Gen. Psychiatry 1999, 56, 1073–1086. [Google Scholar] [CrossRef]
- Bussing, R.; Fernandez, M.; Harwood, M.; Wei, H.; Garvan, C.W.; Eyberg, S.M.; Swanson, J.M. Parent and teacher SNAP-IV ratings of attention deficit hyperactivity disorder symptoms: Psychometric properties and normative ratings from a school district sample. Assessment 2008, 15, 317–328. [Google Scholar] [CrossRef]
- Hsiao, M.N.; Tseng, W.L.; Huang, H.Y.; Gau, S.S. Effects of autistic traits on social and school adjustment in children and adolescents: The moderating roles of age and gender. Res. Dev. Disabil. 2013, 34, 254–265. [Google Scholar] [CrossRef]
- Constantino, J.N.; Davis, S.A.; Todd, R.D.; Schindler, M.K.; Gross, M.M.; Brophy, S.L.; Metzger, L.M.; Shoushtari, C.S.; Splinter, R.; Reich, W. Validation of a brief quantitative measure of autistic traits: Comparison of the social responsiveness scale with the autism diagnostic interview-revised. J. Autism Dev. Disord. 2003, 33, 427–433. [Google Scholar] [CrossRef]
- Duarte, C.S.; Bordin, I.A.; de Oliveira, A.; Bird, H. The CBCL and the identification of children with autism and related conditions in Brazil: Pilot findings. J. Autism Dev. Disord. 2003, 33, 703–707. [Google Scholar] [CrossRef]
- Chiang, H.L.; Kao, W.C.; Chou, M.C.; Chou, W.J.; Chiu, Y.N.; Wu, Y.Y.; Gau, S.S. School dysfunction in youth with autistic spectrum disorder in Taiwan: The effect of subtype and ADHD. Autism Res. 2018. [Google Scholar] [CrossRef]
- MacDonald, R.; Parry-Cruwys, D.; Dupere, S.; Ahearn, W. Assessing progress and outcome of early intensive behavioral intervention for toddlers with autism. Res. Dev. Disabil. 2014, 35, 3632–3644. [Google Scholar] [CrossRef]
- Shattuck, P.T.; Durkin, M.; Maenner, M.; Newschaffer, C.; Mandell, D.S.; Wiggins, L.; Lee, L.C.; Rice, C.; Giarelli, E.; Kirby, R.; et al. Timing of identification among children with an autism spectrum disorder: Findings from a population-based surveillance study. J. Am. Acad. Child Adolesc. Psychiatry 2009, 48, 474–483. [Google Scholar] [CrossRef]
- Risi, S.; Lord, C.; Gotham, K.; Corsello, C.; Chrysler, C.; Szatmari, P.; Cook, E.H., Jr.; Leventhal, B.L.; Pickles, A. Combining information from multiple sources in the diagnosis of autism spectrum disorders. J. Am. Acad. Child Adolesc. Psychiatry 2006, 45, 1094–1103. [Google Scholar] [CrossRef]
- Shaaban, S.Y.; El Gendy, Y.G.; Mehanna, N.S.; El-Senousy, W.M.; El-Feki, H.S.A.; Saad, K.; El-Asheer, O.M. The role of probiotics in children with autism spectrum disorder: A prospective, open-label study. Nutr. Neurosci. 2018, 21, 676–681. [Google Scholar] [CrossRef]
- Parracho, H.M.R.T.; Gibson, G.R.; Knott, F.; Bosscher, D.; Kleerebezem, M.; McCartney, A.L. A double-blind, placebo-controlled, crossover-designed probiotic feeding study inchildren diagnosed with autistic spectrum disorders. Int. J. Probiotics Prebiotics 2010, 5, 69–74. [Google Scholar]
- Craig, F.; Lamanna, A.L.; Margari, F.; Matera, E.; Simone, M.; Margari, L. Overlap between autism spectrum disorders and attention deficit hyperactivity disorder: searching for distinctive/common clinical features. Autism Res. 2015, 8, 328–337. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.L.; Chen, S.H.; Gau, S.S. ADHD and autistic traits, family function, parenting style, and social adjustment for Internet addiction among children and adolescents in Taiwan: A longitudinal study. Res. Dev. Disabil. 2015, 39, 20–31. [Google Scholar] [CrossRef] [PubMed]
- Havdahl, K.A.; von Tetzchner, S.; Huerta, M.; Lord, C.; Bishop, S.L. Utility of the child behavior checklist as a screener for autism spectrum disorder. Autism Res. 2016, 9, 33–42. [Google Scholar] [CrossRef]
- Snow, A.V.; Lecavalier, L.; Houts, C. The structure of the autism diagnostic interview-revised: diagnostic and phenotypic implications. J. Child Psychol. Psychiatry 2009, 50, 734–742. [Google Scholar] [CrossRef]
- Chenga, L.-H.; Liu, Y.-W.; Wu, C.-C.; Wang, S.; Tsai, Y.-C. Psychobiotics in mental health, neurodegenerative and neurodevelopmental disorders. J. Food Drug Anal. 2019. [Google Scholar] [CrossRef]
- Langella, P.; Chatel, J.M. Risk assessment of probiotics use requires clinical parameters. Nat. Rev. Gastroenterol. Hepatol. 2019. [Google Scholar] [CrossRef]
- Plaza-Diaz, J.; Ruiz-Ojeda, F.J.; Gil-Campos, M.; Gil, A. Mechanisms of action of probiotics. Adv. Nutr. 2019, 10, S49–S66. [Google Scholar] [CrossRef]
- King, B.H.; Dukes, K.; Donnelly, C.L.; Sikich, L.; McCracken, J.T.; Scahill, L.; Hollander, E.; Bregman, J.D.; Anagnostou, E.; Robinson, F.; et al. Baseline factors predicting placebo response to treatment in children and adolescents with autism spectrum disorders: A multisite randomized clinical trial. JAMA Pediatr 2013, 167, 1045–1052. [Google Scholar] [CrossRef]
- Jones, R.M.; Carberry, C.; Hamo, A.; Lord, C. Placebo-like response in absence of treatment in children with Autism. Autism Res. 2017, 10, 1567–1572. [Google Scholar] [CrossRef] [PubMed]
- Taylor, J.M. Choosing the number of controls in a matched case-control study, some sample size, power and efficiency considerations. Stat. Med. 1986, 5, 29–36. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristic | PS128 | Placebo | Total | P-Value |
|---|---|---|---|---|
| Sample size (n) | 36 | 35 | 71 | |
| Age | 10.11 (2.34) | 9.91 (2.33) | 10.01 (2.32) | 0.72 |
| Height | 144.16 (16.31) | 140.63 (15.44) | 142.39 (15.85) | 0.38 |
| Weight | 37.31 (13.56) | 35.65 (15.12) | 36.49 (14.26) | 0.65 |
| CGI-S | 4.86 (1.25) | 5.17 (1.04) | 5.01 (1.15) | 0.26 |
| Autism Diagnostic Interview-Revised (ADI-R) Scores | ||||
| Qualitative abnormalities in reciprocal social interaction | 22.81 (4.78) | 24.03 (6.55) | 23.41 (5.71) | 0.37 |
| Qualitative abnormalities in communication (Verbal) | 16.22 (4.66) | 16.20 (4.90) | 16.21 (4.75) | 0.98 |
| Qualitative abnormalities in communication (Non-verbal) | 9.19 (3.18) | 9.20 (2.92) | 9.20 (3.03) | 0.99 |
| Restricted, repetitive, and stereotyped patterns of behavior | 7.11 (2.41) | 8.14 (2.48) | 7.62 (2.48) | 0.08 |
| Abnormality of development evident at or before 36 months | 3.86 (1.38) | 3.83 (1.49) | 3.85 (1.42) | 0.92 |
| Baseline | Week 4 | |||||
|---|---|---|---|---|---|---|
| PS128 | Placebo | P-Value | PS128 | Placebo | P-Value | |
| CGI-I | 3.64 (1.1) | 3.66 (1.00) | 0.94 | |||
| ABC-T | ||||||
| Sensory | 2.24 (1.41) | 3.03 (1.98) | 0.07 | 2.21 (1.58) | 2.75 (1.74) | 0.19 |
| Relating | 3.88 (2.77) | 3.74 (2.43) | 0.82 | 4.03 (3.08) | 3.63 (2.74) | 0.59 |
| Body and object use | 3.42 (2.62) | 3.71 (2.71) | 0.66 | 3.12 (2.59) | 3.45 (2.68) | 0.62 |
| Language | 2.47 (2.15) | 3.0 (1.77) | 0.27 | 2.15 (1.89) | 2.81 (1.84) | 0.16 |
| Social and self help | 3.24 (2.02) | 3.59 (2.11) | 0.48 | 3.15 (1.98) | 3.52 (2.45) | 0.52 |
| Total score | 15.81 (8.39) | 17 (9.31) | 0.59 | 14.67 (8.97) | 16.21 (10.11) | 0.53 |
| SRS | ||||||
| Social communication | 64.06 (14.84) | 64.0 (15.87) | 0.99 | 62.17 (12.9) | 63.34 (16.21) | 0.75 |
| Autism mannerisms | 30.82 (6.26) | 30.39 (6.58) | 0.79 | 29.97 (7.25) | 29.71 (6.53) | 0.88 |
| Social awareness | 23.29 (4.22) | 21.11 (5.27) | 0.06 | 23.21 (4.89) | 21.57 (5.25) | 0.21 |
| Social emotion | 19.74 (4.54) | 19.11 (4.34) | 0.56 | 19.24 (4.55) | 18.81 (5.14) | 0.72 |
| Total score | 138.87 (24.19) | 135.88 (26.04) | 0.64 | 132.77 (22.99) | 135.79 (25.79) | 0.63 |
| CBCL | ||||||
| Anxiety | 6.76 (4.85) | 6.0 (4.46) | 0.51 | 5.63 (4.34) | 5.84 (4.41) | 0.84 |
| Withdrawn | 4.41 (2.83) | 4.68 (3.05) | 0.71 | 4.22 (2.67) | 4.50 (3.16) | 0.7 |
| Somatic complaints | 2.38 (1.79) | 3.13 (2.92) | 0.22 | 2.5 (2.53) | 2.41 (2.72) | 0.9 |
| Internalization | 13.32 (7.98) | 13.60 (8.46) | 0.9 | 12.34 (6.83) | 12.72 (8.53) | 0.85 |
| Social problems | 7.65 (3.98) | 7.71 (3.13) | 0.95 | 7.38 (4.04) | 7.65 (3.67) | 0.78 |
| Thoughts problems | 5.73 (4.04) | 6.90 (5.57) | 0.35 | 4.84 (3.96) | 6.50 (5.28) | 0.17 |
| Attention problems | 10.61 (3.74) | 11.12 (3.92) | 0.59 | 10.87 (4.42) | 10.90 (4.28) | 0.98 |
| Rule-breaking behavior | 3.5 (3.3) | 3.84 (2.74) | 0.65 | 3.06 (3.62) | 3.31 (3.15) | 0.77 |
| Aggressive behavior | 8.27 (7.0) | 8.71 (6.21) | 0.8 | 8.06 (7.02) | 7.94 (6.02) | 0.94 |
| External | 11.73 (9.73) | 12.75 (8.64) | 0.67 | 11.1 (10.2) | 11.25 (8.47) | 0.95 |
| Total score | 49.63 (25.4) | 50.60 (25.91) | 0.89 | 44.34 (23.25) | 49.20 (24.46) | 0.53 |
| SNAP-IV | ||||||
| Inattention | 15.18 (5.83) | 15.79 (5.16) | 0.66 | 14.39 (5.91) | 15.35 (5.48) | 0.5 |
| Hyperactivity/impulsivity | 10.3 (5.51) | 10.97 (6.0) | 0.64 | 9.65 (5.23) | 10.25 (6.42) | 0.68 |
| Opposition/defiance | 8.93 (6.09) | 7.5 (5.41) | 0.32 | 7.73 (5.04) | 7.41 (5.43) | 0.8 |
| Total score | 34.03 (14.61) | 34.48 (13.39) | 0.9 | 31.87 (14.26) | 33.16 (15.58) | 0.73 |
| PS128 | Placebo | |||||
|---|---|---|---|---|---|---|
| Aged 7–15 | Aged 7–12 | Aged 13–15 | Aged 7–15 | Aged 7–12 | Aged 13–15 | |
| ABC-T | ||||||
| Sensory | 1.0 | 0.88 | 0.37 | 0.18 | 0.18 | N.C. |
| Relating | 1.0 | 0.72 | 0.21 | 0.84 | 1 | 0.39 |
| Body and object use | 0.04 * | 0.06 | 0.48 | 0.5 | 0.5 | N.C. |
| Language | 0.33 | 0.48 | 0.37 | 0.31 | 0.39 | 0.39 |
| Social and self help | 0.4 | 0.46 | 0.62 | 0.78 | 0.78 | N.C. |
| Total score | 0.28 | 0.4 | 0.28 | 0.43 | 0.49 | 0.23 |
| SRS | ||||||
| Social communication | 0.12 | 0.28 | 0.28 | 0.25 | 0.51 | 0.36 |
| Autism mannerisms | 0.08 | 0.21 | 0.13 | 0.19 | 0.19 | 0.89 |
| Social awareness | 0.93 | 0.9 | 0.7 | 0.41 | 0.62 | 0.52 |
| Social emotion | 0.09 | 0.33 | 0.08 | 0.29 | 0.38 | 0.55 |
| Total score | 0.04* | 0.13 | 0.15 | 0.2 | 0.36 | 0.4 |
| CBCL | ||||||
| Anxiety | 0.02 * | 0.01 * | 0.82 | 0.38 | 0.45 | 0.6 |
| Withdrawn | 0.43 | 0.45 | 0.85 | 0.63 | 0.63 | 1 |
| Somatic complaints | 0.85 | 0.9 | 0.7 | 0.1 | 0.16 | 0.39 |
| Internalization | 0.12 | 0.12 | 0.8 | 0.15 | 0.2 | 0.39 |
| Social problems | 0.21 | 0.32 | 0.3 | 0.66 | 0.93 | 0.18 |
| Thoughts problems | 0.05 | 0.06 | 0.62 | 0.17 | 0.22 | 0.53 |
| Attention problems | 0.46 | 0.24 | 0.46 | 0.78 | 0.7 | 0.79 |
| Rule-breaking behavior | 0.02 * | 0.01 * | 1 | 0.11 | 0.14 | 0.39 |
| Aggressive behavior | 0.41 | 0.42 | 0.85 | 0.07 | 0.13 | 0.31 |
| External | 0.11 | 0.1 | 1 | 0.02 * | 0.04 * | 0.32 |
| Total score | 0.1 | 0.09 | 0.83 | 0.3 | 0.48 | 0.4 |
| SNAP-IV | ||||||
| Inattention | 0.08 | 0.03 * | 0.49 | 0.91 | 0.86 | 0.72 |
| Hyperactivity/impulsivity | 0.04 * | 0.02 * | 0.59 | 0.32 | 0.29 | 0.72 |
| Opposition/defiance | 0.05 | 0.02 * | 0.78 | 0.77 | 0.79 | 0.33 |
| Total score | 0.02 * | 0.004 * | 0.61 | 0.86 | 0.96 | 0.46 |
| Baseline | Week 4 | Difference between PS128 and placebo | |||||
|---|---|---|---|---|---|---|---|
| PS128 | Placebo | P-Value | PS128 | Placebo | P-Value | P-Value | |
| CGI-I | 3.68 (1.14) | 3.57 (1.04) | 0.69 | ||||
| ABC-T | |||||||
| Sensory | 2.36 (1.47) | 2.9 (1.88) | 0.22 | 2.29 (1.61) | 2.68 (1.68) | 0.38 | 0.41 |
| Relating | 4.14 (2.89) | 3.66 (2.35) | 0.49 | 4.43 (3.1) | 3.77 (2.72) | 0.41 | 0.82 |
| Body and object use | 3.32 (2.75) | 3.7 (2.74) | 0.6 | 3.04 (2.67) | 3.52 (2.75) | 0.51 | 0.51 |
| Language | 2.44 (2.26) | 3.1 (1.81) | 0.23 | 2.14 (1.94) | 2.93 (1.84) | 0.13 | 0.93 |
| Social and self help | 3.28 (2.12) | 3.45 (2.06) | 0.75 | 3.21 (2.08) | 3.41 (2.44) | 0.75 | 0.71 |
| Total score | 16.22 (8.79) | 16.82 (9.08) | 0.8 | 15.11 (9.14) | 16.36 (10.16) | 0.64 | 0.95 |
| SRS | |||||||
| Social communication | 63.6 (15.54) | 64.5 (16.5) | 0.83 | 62.12 (12.89) | 64.79 (16.01) | 0.51 | 0.72 |
| Autism mannerisms | 30.53 (6.59) | 31.1 (6.77) | 0.75 | 30.04 (7.52) | 30.33 (6.47) | 0.88 | 0.82 |
| Social awareness | 23.59 (4.42) | 20.73 (4.73) | 0.02 * | 23.46 (5.29) | 20.62 (4.67) | 0.04 * | 0.74 |
| Social emotion | 19.41 (4.66) | 19.53 (4.21) | 0.92 | 19.25 (4.66) | 19.25 (4.88) | 1 | 0.98 |
| Total score | 138.23 (25.67) | 137.25 (27.28) | 0.89 | 132.72 (23.37) | 137.96 (25.98) | 0.46 | 0.43 |
| CBCL | |||||||
| Anxiety | 6.86 (5.2) | 6.14 (4.43) | 0.86 | 5.59 (4.34) | 5.82 (4.39) | 0.83 | 0.13 |
| Withdrawn | 4.45 (3.03) | 4.59 (2.95) | 0.35 | 4.26 (2.7) | 4.43 (3.02) | 0.71 | 0.81 |
| Somatic complaints | 2.44 (1.91) | 3.08 (2.88) | 0.98 | 2.63 (2.63) | 2.36 (2.51) | 0.97 | 0.65 |
| Internalization | 13.5 (8.63) | 13.56 (8.13) | 0.81 | 12.48 (6.9) | 12.56 (7.87) | 0.95 | 0.78 |
| Social problems | 7.83 (4.24) | 7.59 (3.29) | 0.32 | 7.7 (4.07) | 7.63 (3.81) | 0.2 | 0.44 |
| Thoughts problems | 5.96 (4.22) | 7.37 (5.79) | 0.59 | 5.08 (4.37) | 6.81 (5.39) | 0.95 | 0.41 |
| Attention problems | 10.54 (3.72) | 11.07 (3.73) | 0.77 | 11 (4.2) | 10.93 (4.18) | 0.98 | 0.25 |
| Rule-breaking behavior | 3.72 (3.38) | 3.96 (2.79) | 0.87 | 3.23 (3.65) | 3.25 (3.31) | 0.81 | 0.39 |
| Aggressive behavior | 8.46 (6.86) | 8.76 (6.1) | 0.73 | 8.22 (6.44) | 7.82 (6.09) | 0.89 | 0.87 |
| External | 12.08 (9.75) | 12.96 (8.56) | 0.89 | 11.42 (9.6) | 11.07 (8.67) | 0.45 | 0.83 |
| Total score | 51.04 (26.87) | 52.14 (26.9) | 0.86 | 45.17 (23.02) | 50.5 (24.42) | 0.83 | 0.29 |
| SNAP-IV | |||||||
| Inattention | 15.29 (5.58) | 15.43 (5.14) | 0.92 | 14.18 (5.72) | 15.26 (5.65) | 0.48 | 0.08 |
| Hyperactivity/impulsivity | 10.75 (5.75) | 11.41 (5.96) | 0.67 | 9.88 (5.22) | 10.82 (6.5) | 0.56 | 0.26 |
| Opposition/defiance | 9.26 (5.93) | 7.38 (5.13) | 0.21 | 7.71 (4.75) | 7.32 (5.44) | 0.77 | 0.03 * |
| Total score | 34.85 (14.46) | 34.5 (13.8) | 0.93 | 31.88 (13.83) | 33.59 (15.99) | 0.68 | 0.02 * |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, Y.-W.; Liong, M.T.; Chung, Y.-C.E.; Huang, H.-Y.; Peng, W.-S.; Cheng, Y.-F.; Lin, Y.-S.; Wu, Y.-Y.; Tsai, Y.-C. Effects of Lactobacillus plantarum PS128 on Children with Autism Spectrum Disorder in Taiwan: A Randomized, Double-Blind, Placebo-Controlled Trial. Nutrients 2019, 11, 820. https://doi.org/10.3390/nu11040820
Liu Y-W, Liong MT, Chung Y-CE, Huang H-Y, Peng W-S, Cheng Y-F, Lin Y-S, Wu Y-Y, Tsai Y-C. Effects of Lactobacillus plantarum PS128 on Children with Autism Spectrum Disorder in Taiwan: A Randomized, Double-Blind, Placebo-Controlled Trial. Nutrients. 2019; 11(4):820. https://doi.org/10.3390/nu11040820
Chicago/Turabian StyleLiu, Yen-Wenn, Min Tze Liong, Yu-Chu Ella Chung, Hui-Yi Huang, Wu-Shun Peng, Yun-Fang Cheng, Yu-Siou Lin, Yu-Yu Wu, and Ying-Chieh Tsai. 2019. "Effects of Lactobacillus plantarum PS128 on Children with Autism Spectrum Disorder in Taiwan: A Randomized, Double-Blind, Placebo-Controlled Trial" Nutrients 11, no. 4: 820. https://doi.org/10.3390/nu11040820