Associations between Weight Loss, Food Likes, Dietary Behaviors, and Chemosensory Function in Bariatric Surgery: A Case-Control Analysis in Women



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Procedure and Measures
2.3. Statistical Analysis
2.4. Power Analysis
3. Results
3.1. Demographics of the Participants
3.2. Self-Reported Chemosensory Function
3.3. Sweet Taste, Retronasal Probe, and Sweet Liking
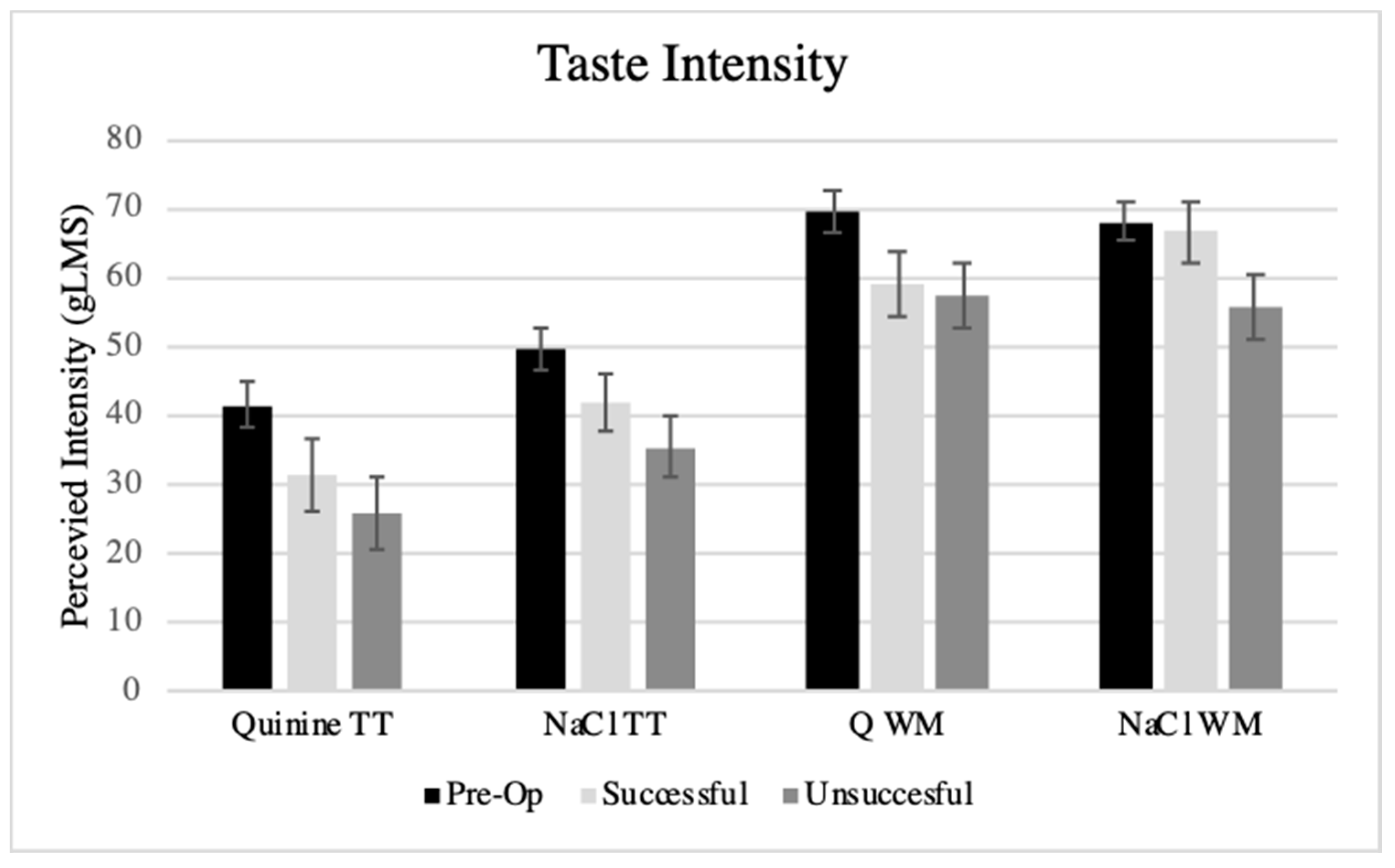
3.4. Taste Function and PROP Tasting
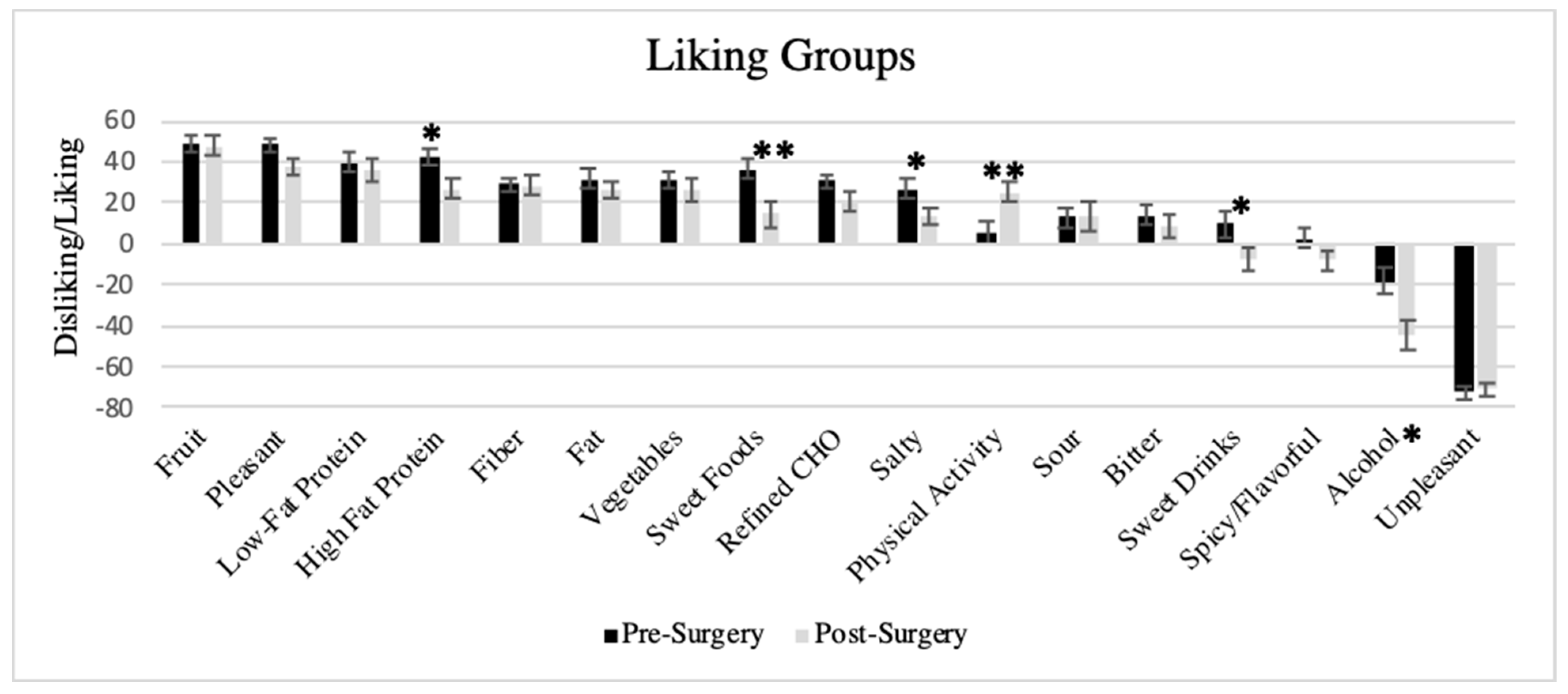
3.5. Liking Survey
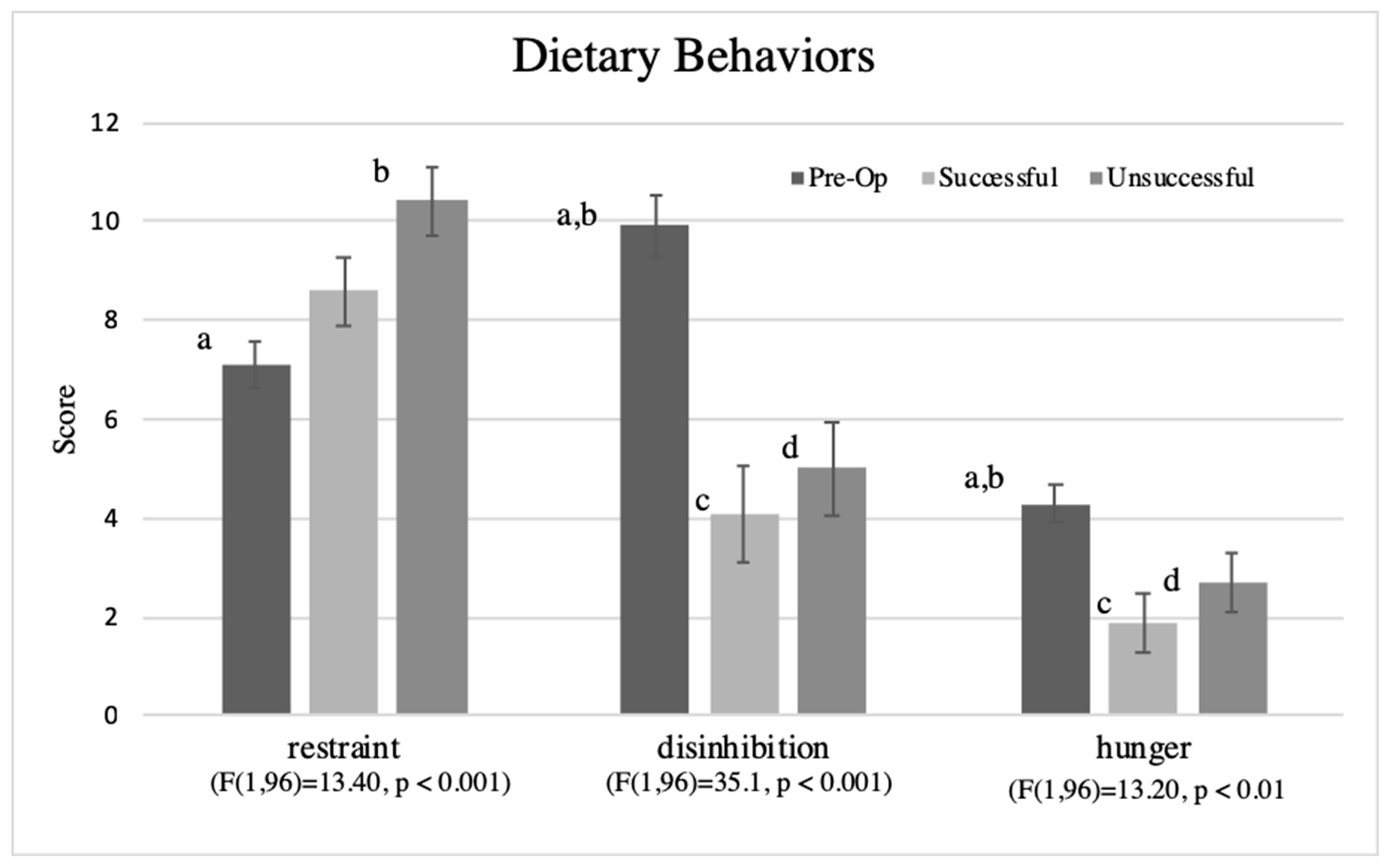
3.6. Dietary Behaviors
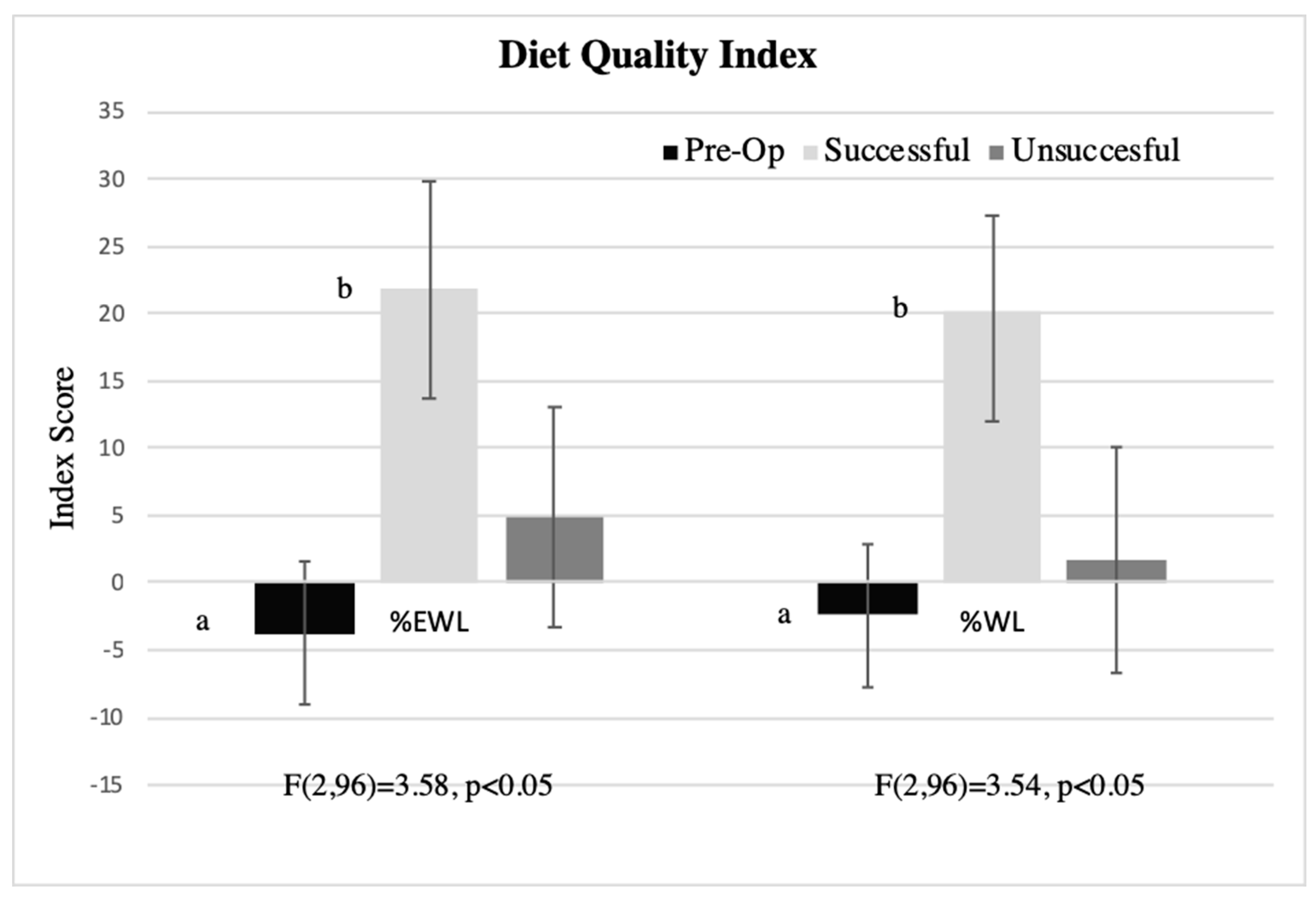
3.7. Associations between Liking-Based Indexes, Dietary Behaviors, and Percent Weight Loss in Post-Surgical Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- National Center for Health Statistics. Health, United States, 2017: With Special Feature on Mortality. Available online: https://www.cdc.gov/nchs/data/hus/hus17.pdf (accessed on 18 February 2019).
- Buchwald, H. Consensus conference statement bariatric surgery for morbid obesity: Health implications for patients, health professionals, and third-party payers. Surg. Obes. Relat. Dis. 2005, 1, 371–381. [Google Scholar] [CrossRef] [PubMed]
- Panteliou, E.; Miras, A.D. What is the role of bariatric surgery in the management of obesity? Climacteric 2017, 20, 97–102. [Google Scholar] [CrossRef] [PubMed]
- American Society for Metabolic and Bariatric Society. Estimate of Bariatric Surgery Numbers, 2011–2017. Available online: https://asmbs.org/resources/estimate-of-bariatric-surgery-numbers (accessed on 9 February 2019).
- Young, M.T.; Phelan, M.J.; Nguyen, N.T. A decade analysis of trends and outcomes of male vs female patients who underwent bariatric surgery. J. Am. Coll. Surg. 2016, 222, 226–231. [Google Scholar] [CrossRef] [PubMed]
- Sjostrom, L. Review of the key results from the Swedish Obese Subjects (SOS) trial—A prospective controlled intervention study of bariatric surgery. J. Intern Med. 2013, 273, 219–234. [Google Scholar] [CrossRef] [PubMed]
- Bonouvrie, D.S.; Uittenbogaart, M.; Luijten, A.; van Dielen, F.M.H.; Leclercq, W.K.G. Lack of standard definitions of primary and secondary (non)responders after primary gastric bypass and gastric sleeve: A systematic review. Obes. Surg. 2019, 29, 691–697. [Google Scholar] [CrossRef]
- Brethauer, S.A.; Kim, J.; el Chaar, M.; Papasavas, P.; Eisenberg, D.; Rogers, A.; Ballem, N.; Kligman, M.; Kothari, S.; Committee, A.C.I. Standardized outcomes reporting in metabolic and bariatric surgery. Surg. Obes. Relat. Dis. 2015, 11, 489–506. [Google Scholar] [CrossRef]
- Reinhold, R.B. Critical analysis of long term weight loss following gastric bypass. Surg. Gynecol. Obstet. 1982, 155, 385–394. [Google Scholar]
- Hatoum, I.J.; Kaplan, L.M. Advantages of percent weight loss as a method of reporting weight loss after Roux-en-Y gastric bypass. Obesity 2013, 21, 1519–1525. [Google Scholar] [CrossRef]
- Montero, P.N.; Stefanidis, D.; Norton, H.J.; Gersin, K.; Kuwada, T. Reported excess weight loss after bariatric surgery could vary significantly depending on calculation method: A plea for standardization. Surg. Obes. Relat. Dis. 2011, 7, 531–534. [Google Scholar] [CrossRef]
- Makaronidis, J.M.; Batterham, R.L. Potential mechanisms mediating sustained weight loss following Roux-en-Y Gastric Bypass and Sleeve Gastrectomy. Endocrinol Metab. Clin. North. Am. 2016, 45, 539–552. [Google Scholar] [CrossRef]
- Mulla, C.M.; Middelbeek, R.J.W.; Patti, M.E. Mechanisms of weight loss and improved metabolism following bariatric surgery. Ann. N. Y. Acad. Sci. 2018, 1411, 53–64. [Google Scholar] [CrossRef] [PubMed]
- Berridge, K.C.; Robinson, T.E.; Aldridge, J.W. Dissecting components of reward: ‘Liking’, ‘wanting’, and learning. Curr. Opin. Pharmacol. 2009, 9, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Bartoshuk, L.M.; Duffy, V.B.; Hayes, J.E.; Moskowitz, H.R.; Snyder, D.J. Psychophysics of sweet and fat perception in obesity: Problems, solutions and new perspectives. Philos. Trans. R. Soc. Lond. B Biol. Sci 2006, 361, 1137–1148. [Google Scholar] [CrossRef] [PubMed]
- Schultes, B.; Ernst, B.; Wilms, B.; Thurnheer, M.; Hallschmid, M. Hedonic hunger is increased in severely obese patients and is reduced after gastric bypass surgery. Am. J. Clin. Nutr. 2010, 92, 277–283. [Google Scholar] [CrossRef]
- Le Roux, C.W.; Bueter, M. The physiology of altered eating behaviour after Roux-en-Y gastric bypass. Exp. Physiol. 2014, 99, 1128–1132. [Google Scholar] [CrossRef]
- Ullrich, J.; Ernst, B.; Wilms, B.; Thurnheer, M.; Schultes, B. Roux-en Y Gastric Bypass Surgery reduces hedonic hunger and improves dietary habits in severely obese subjects. Obes. Surg. 2013, 23, 50–55. [Google Scholar] [CrossRef]
- Kapoor, N.; Al-Najim, W.; le Roux, C.W.; Docherty, N.G. Shifts in food preferences after bariatric surgery: Observational reports and proposed mechanisms. Curr. Obes. Rep. 2017, 6, 246–252. [Google Scholar] [CrossRef]
- Li, G.; Ji, G.; Hu, Y.; Liu, L.; Jin, Q.; Zhang, W.; Liu, L.; Wang, Y.; Zhao, J.; von Deneen, K.M.; et al. Reduced plasma ghrelin concentrations are associated with decreased brain reactivity to food cues after laparoscopic sleeve gastrectomy. Psychoneuroendocrinology 2019, 100, 229–236. [Google Scholar] [CrossRef]
- Gero, D.; Steinert, R.E.; le Roux, C.W.; Bueter, M. Do food preferences change after bariatric surgery? Curr. Atheroscler. Rep. 2017, 19, 38. [Google Scholar] [CrossRef]
- Primeaux, S.D.; de Silva, T.; Tzeng, T.H.; Chiang, M.C.; Hsia, D.S. Recent advances in the modification of taste and food preferences following bariatric surgery. Rev. Endocr. Metab. Dis. 2016, 17, 195–207. [Google Scholar] [CrossRef]
- Trijsburg, L.; Geelen, A.; Hollman, P.C.; Hulshof, P.J.; Feskens, E.J.; Van’t Veer, P.; Boshuizen, H.C.; de Vries, J.H. BMI was found to be a consistent determinant related to misreporting of energy, protein and potassium intake using self-report and duplicate portion methods. Pub. Health Nutr. 2016, 20, 598–607. [Google Scholar] [CrossRef]
- Kittrell, H.; Graber, W.; Mariani, E.; Czaja, K.; Hajnal, A.; Di Lorenzo, P.M. Taste and odor preferences following Roux-en-Y surgery in humans. PLoS ONE 2018, 13, e0199508. [Google Scholar] [CrossRef]
- Pepino, M.Y.; Bradley, D.; Eagon, J.C.; Sullivan, S.; Abumrad, N.A.; Klein, S. Changes in taste perception and eating behavior after bariatric surgery-induced weight loss in women. Obesity 2014, 22, E13–E20. [Google Scholar] [CrossRef]
- Nance, K.; Eagon, J.C.; Klein, S.; Pepino, M.Y. Effects of Sleeve Gastrectomy vs. Roux-en-Y Gastric Bypass on eating behavior and sweet taste perception in subjects with obesity. Nutrients 2017, 10, 18. [Google Scholar] [CrossRef]
- Miras, A.D.; Jackson, R.N.; Jackson, S.N.; Goldstone, A.P.; Olbers, T.; Hackenberg, T.; Spector, A.C.; le Roux, C.W. Gastric bypass surgery for obesity decreases the reward value of a sweet-fat stimulus as assessed in a progressive ratio task. Am. J. Clin. Nutr. 2012, 96, 467–473. [Google Scholar] [CrossRef]
- Nielsen, M.S.; Christensen, B.J.; Ritz, C.; Rasmussen, S.; Hansen, T.T.; Bredie, W.L.P.; le Roux, C.W.; Sjodin, A.; Schmidt, J.B. Roux-En-Y Gastric Bypass and Sleeve Gastrectomy does not affect food preferences when assessed by an ad libitum buffet meal. Obes. Surg. 2017, 27, 2599–2605. [Google Scholar] [CrossRef] [PubMed]
- Sondergaard Nielsen, M.; Rasmussen, S.; Just Christensen, B.; Ritz, C.; le Roux, C.W.; Berg Schmidt, J.; Sjodin, A. Bariatric surgery does not affect food preferences, but individual changes in food preferences may predict weight loss. Obesity 2018, 26, 1879–1887. [Google Scholar] [CrossRef]
- U.S. Department of Health and Human Services; Agriculture, U.S.D.o. 2015–2020 Dietary Guidelines For Americans. Available online: https://health.gov/dietaryguidelines/2015/guidelines/ (accessed on 18 February 2019).
- Molin Netto, B.D.; Earthman, C.P.; Farias, G.; Landi Masquio, D.C.; Grotti Clemente, A.P.; Peixoto, P.; Bettini, S.C.; von Der Heyde, M.E.; Damaso, A.R. Eating patterns and food choice as determinant of weight loss and improvement of metabolic profile after RYGB. Nutrition 2017, 33, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Keskitalo, K.; Knaapila, A.; Kallela, M.; Palotie, A.; Wessman, M.; Sammalisto, S.; Peltonen, L.; Tuorila, H.; Perola, M. Sweet taste preferences are partly genetically determined: Identification of a trait locus on chromosome 16. Am. J. Clin. Nutr. 2007, 86, 55–63. [Google Scholar] [CrossRef] [PubMed]
- Duffy, V.; Peterson, J.; Dinehart, M.; Bartoshuk, L. Genetic and environmental variation in taste: Associations with sweet intensity, preference, and intake. Top. Clin. Nutr. 2003, 18, 209–220. [Google Scholar] [CrossRef]
- Hayes, J.E.; Sullivan, B.S.; Duffy, V.B. Explaining variability in sodium intake through oral sensory phenotype, salt sensation and liking. Physiol. Behav. 2010, 100, 369–380. [Google Scholar] [CrossRef] [PubMed]
- Sharafi, M.; Hayes, J.E.; Duffy, V.B. Masking vegetable bitterness to improve palatability depends on vegetable type and taste phenotype. Chemosens. Percept. 2013, 6, 8–19. [Google Scholar] [CrossRef] [PubMed]
- Tuorila, H.; Huotilainen, A.; Lähteenmäki, L.; Ollila, S.; Tuomi-Nurmi, S.; Urala, N. Comparison of affective rating scales and their relationship to variables reflecting food consumption. Food Qual. Pref. 2008, 19, 51–61. [Google Scholar] [CrossRef]
- Pallister, T.; Sharafi, M.; Lachance, G.; Pirastu, N.; Mohney, R.P.; MacGregor, A.; Feskens, E.J.; Duffy, V.; Spector, T.D.; Menni, C. Food preference patterns in a UK twin cohort. Twin Res. Hum. Genet. 2015, 18, 793–805. [Google Scholar] [CrossRef] [PubMed]
- Sharafi, M.; Rawal, S.; Fernandez, M.L.; Huedo-Medina, T.B.; Duffy, V.B. Taste phenotype associates with cardiovascular disease risk factors via diet quality in multivariate modeling. Physiol. Behav. 2018, 194, 103–112. [Google Scholar] [CrossRef]
- Guenther, P.M.; Kirkpatrick, S.I.; Reedy, J.; Krebs-Smith, S.M.; Buckman, D.W.; Dodd, K.W.; Casavale, K.O.; Carroll, R.J. The Healthy Eating Index-2010 is a valid and reliable measure of diet quality according to the 2010 Dietary Guidelines for Americans. J. Nutr. 2014, 144, 399–407. [Google Scholar] [CrossRef]
- Sharafi, M.; Duffy, V.B.; Miller, R.J.; Winchester, S.B.; Sullivan, M.C. Dietary behaviors of adults born prematurely may explain future risk for cardiovascular disease. Appetite 2016, 99, 157–167. [Google Scholar] [CrossRef]
- Zoghbi, M.; Stone, A.; Papsavas, P.; Swede, H.; Hubert, P.; Tisher, D.; Duffy, V.B. Evaluating taste preferences and dietary quality with a simple liking survey: Application in bariatric treatment settings. Bariatr. Surg. Pract. Patient Care 2017, 11. [Google Scholar] [CrossRef]
- Iatridi, V.; Hayes, J.E.; Yeomans, M.R. Quantifying sweet taste liker phenotypes: Time for some consistency in the classification criteria. Nutrients 2019, 11, 129. [Google Scholar] [CrossRef]
- Shoar, S.; Naderan, M.; Shoar, N.; Modukuru, V.R.; Mahmoodzadeh, H. Alteration pattern of taste perception after bariatric surgery: A systematic review of four taste domains. Obes. Surg. 2019. [Google Scholar] [CrossRef]
- Tichansky, D.S.; Boughter, J.D., Jr.; Madan, A.K. Taste change after laparoscopic Roux-en-Y gastric bypass and laparoscopic adjustable gastric banding. Surg. Obes. Relat. Dis. 2006, 2, 440–444. [Google Scholar] [CrossRef] [PubMed]
- Graham, L.; Murty, G.; Bowrey, D.J. Taste, smell and appetite change after Roux-en-Y gastric bypass surgery. Obes. Surg. 2014, 24, 1463–1468. [Google Scholar] [CrossRef]
- Makaronidis, J.M.; Neilson, S.; Cheung, W.H.; Tymoszuk, U.; Pucci, A.; Finer, N.; Doyle, J.; Hashemi, M.; Elkalaawy, M.; Adamo, M.; et al. Reported appetite, taste and smell changes following Roux-en-Y gastric bypass and sleeve gastrectomy: Effect of gender, type 2 diabetes and relationship to post-operative weight loss. Appetite 2016, 107, 93–105. [Google Scholar] [CrossRef]
- Holinski, F.; Menenakos, C.; Haber, G.; Olze, H.; Ordemann, J. Olfactory and gustatory function after bariatric surgery. Obes. Surg. 2015, 25, 2314–2320. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, H.J.; Rawal, S.; Li, C.M.; Duffy, V.B. New chemosensory component to the U.S. National Health and Nutrition Examination Survey (NHANES), first-year results for measured olfactory dysfunction. Rev. Endocr. Metab. Disord. 2016, 17, 221–240. [Google Scholar] [CrossRef]
- Rawal, S.; Huedo-Medina, T.B.; Hoffman, H.J.; Swede, H.; Duffy, V.B. Structural equation modeling of associations among taste-related risk factors, taste functioning, and adiposity. Obesity 2017, 25, 781–787. [Google Scholar] [CrossRef] [PubMed]
- Tepper, B.J.; Banni, S.; Melis, M.; Crnjar, R.; Tomassini Barbarossa, I. Genetic sensitivity to the bitter taste of 6-n-propylthiouracil (PROP) and its association with physiological mechanisms controlling body mass index (BMI). Nutrients 2014, 6, 3363–3381. [Google Scholar] [CrossRef]
- Brockmeyer, T.; Hamze Sinno, M.; Skunde, M.; Wu, M.; Woehning, A.; Rudofsky, G.; Friederich, H.C. Inhibitory control and hedonic response towards food interactively predict success in a weight loss programme for adults with obesity. Obes. Facts 2016, 9, 299–309. [Google Scholar] [CrossRef] [PubMed]
- Hays, N.P.; Roberts, S.B. Aspects of eating behaviors “disinhibition” and “restraint” are related to weight gain and BMI in women. Obesity 2008, 16, 52–58. [Google Scholar] [CrossRef]
- Thomas, J.G.; Bond, D.S.; Phelan, S.; Hill, J.O.; Wing, R.R. Weight-loss maintenance for 10 years in the National Weight Control Registry. Am. J. Prev. Med. 2014, 46, 17–23. [Google Scholar] [CrossRef]
- Neumann, M.; Holzapfel, C.; Muller, A.; Hilbert, A.; Crosby, R.D.; de Zwaan, M. Features and trajectories of eating behavior in weight-loss maintenance: Results from the German Weight Control Registry. Obesity 2018, 26, 1501–1508. [Google Scholar] [CrossRef]
- Figura, A.; Rose, M.; Ordemann, J.; Klapp, B.F.; Ahnis, A. Changes in self-reported eating patterns after laparoscopic sleeve gastrectomy: A pre-post analysis and comparison with conservatively treated patients with obesity. Surg. Obes. Relat. Dis. 2017, 13, 129–137. [Google Scholar] [CrossRef] [PubMed]
- Rieber, N.; Giel Ke Fau-Meile, T.; Meile T Fau-Enck, P.; Enck P Fau-Zipfel, S.; Zipfel S Fau-Teufel, M.; Teufel, M. Psychological dimensions after laparoscopic sleeve gastrectomy: Reduced mental burden, improved eating behavior, and ongoing need for cognitive eating control. Surg. Obes. Relat. Dis. 2013, 9, 569–573. [Google Scholar] [CrossRef] [PubMed]
- Kalarchian, M.A.; Wilson, G.T.; Brolin, R.E.; Bradley, L. Effects of bariatric surgery on binge eating and related psychopathology. Eat Weight Disord. 1999, 4, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Burgmer, R.; Grigutsch, K.; Zipfel, S.; Wolf, A.M.; de Zwaan, M.; Husemann, B.; Albus, C.; Senf, W.; Herpertz, S. The influence of eating behavior and eating pathology on weight loss after gastric restriction operations. Obes. Surg. 2005, 15, 684–691. [Google Scholar] [CrossRef] [PubMed]
- Bartoshuk, L.M.; Duffy, V.B.; Green, B.G.; Hoffman, H.J.; Ko, C.W.; Lucchina, L.A.; Marks, L.E.; Snyder, D.J.; Weiffenbach, J.M. Valid across-group comparisons with labeled scales: The gLMS versus magnitude matching. Physiol. Behav. 2004, 82, 109–114. [Google Scholar] [CrossRef] [PubMed]
- CDC. National Health and Nutrition Examination Survey (NHANES) Taste and Smell Examination Component Manual [Internet]. Centers for Disease Control and Prevention (CDC), National Center for Health Statistics (NCHS). Available online: http://www.cdc.gov/nchs/data/nhanes/nhanes_13_14/Taste_Smell.pdf. (accessed on 18 February 2019).
- Coldwell, S.E.; Mennella, J.A.; Duffy, V.B.; Pelchat, M.L.; Griffith, J.W.; Smutzer, G.; Cowart, B.J.; Breslin, P.A.; Bartoshuk, L.M.; Hastings, L.; et al. Gustation assessment using the NIH Toolbox. Neurology 2013, 80, S20–S24. [Google Scholar] [CrossRef] [PubMed]
- Bartoshuk, L.M.; Duffy, V.B.; Miller, I.J., Jr. PTC/PROP Tasting: Anatomy, psychophysics, and sex effects. Physiol. Behav. 1994, 56, 1165–1171. [Google Scholar] [CrossRef]
- Hayes, J.E.; Bartoshuk, L.M.; Kidd, J.R.; Duffy, V.B. Supertasting and PROP bitterness depends on more than the TAS2R38 gene. Chem. Senses 2008, 33, 255–265. [Google Scholar] [CrossRef]
- Stunkard, A.J.; Messick, S. The three-factor eating questionnaire to measure dietary restraint, disinhibition and hunger. J. Psychosom. Res. 1985, 29, 71–83. [Google Scholar] [CrossRef]
- Westenhoefer, J.; Stunkard Albert, J.; Pudel, V. Validation of the flexible and rigid control dimensions of dietary restraint. Int. J. Eat Disord. 1999, 26, 53–64. [Google Scholar] [CrossRef]
- Robinson, A.H.; Adler, S.; Stevens, H.B.; Darcy, A.M.; Morton, J.M.; Safer, D.L. What variables are associated with successful weight loss outcomes for bariatric surgery after 1 year? Surg. Obes. Relat. Dis. 2014, 10, 697–704. [Google Scholar] [CrossRef] [PubMed]
- Sillen, L.; Andersson, E. Patient factors predicting weight loss after Roux-en-Y Gastric Bypass. J. Obes. 2017, 2017, 3278751. [Google Scholar] [CrossRef] [PubMed]
- Courcoulas, A.P.; Christian Nj Fau-Belle, S.H.; Belle Sh Fau-Berk, P.D.; Berk Pd Fau-Flum, D.R.; Flum Dr Fau-Garcia, L.; Garcia L Fau-Horlick, M.; Horlick M Fau-Kalarchian, M.A.; Kalarchian Ma Fau-King, W.C.; King Wc Fau-Mitchell, J.E.; Mitchell Je Fau-Patterson, E.J.; et al. Weight change and health outcomes at 3 years after bariatric surgery among individuals with severe obesity. JAMA 2013, 310, 2416–2425. [Google Scholar] [CrossRef] [PubMed]
- Taboada, D.; Navio M Fau-Jurado, R.; Jurado R Fau-Fernandez, V.; Fernandez V Fau-Bayon, C.; Bayon C Fau-Alvarez, M.J.; Alvarez Mj Fau-Morales, I.; Morales I Fau-Ponce, G.; Ponce G Fau-Rubio, G.; Rubio G Fau-Mingote, J.C.; Mingote Jc Fau-Cruz, F.; et al. Factor structure and psychometric properties of the TFEQ in morbid obese patients, candidates to bariatric surgery. Psicothema 2015, 27, 141–150. [Google Scholar] [PubMed]
- Tepper, B.J. Nutritional implications of genetic taste variation: The role of PROP sensitivity and other taste phenotypes. Ann. Rev. Nutr. 2008, 28, 367–388. [Google Scholar] [CrossRef] [PubMed]
- Peng, M.; Coutts, D.; Wang, T.; Cakmak, Y.O. Systematic review of olfactory shifts related to obesity. Obes. Rev. 2019, 20, 325–338. [Google Scholar] [CrossRef]
- Snyder, D.J.; Bartoshuk, L.M. Oral sensory nerve damage: Causes and consequences. Rev. Endocr. Metab. Disord. 2016, 17, 149–158. [Google Scholar] [CrossRef]
- Oor, J.E.; Roks, D.J.; Unlu, C.; Hazebroek, E.J. Laparoscopic sleeve gastrectomy and gastroesophageal reflux disease: A systematic review and meta-analysis. Am. J. Surg. 2016, 211, 250–267. [Google Scholar] [CrossRef] [PubMed]
- Althuwaini, S.; Bamehriz, F.; Aldohayan, A.; Alshammari, W.; Alhaidar, S.; Alotaibi, M.; Alanazi, A.; Alsahabi, H.; Almadi, M.A. Prevalence and predictors of gastroesophageal reflux disease after Laparoscopic Sleeve Gastrectomy. Obes. Surg. 2018, 28, 916–922. [Google Scholar] [CrossRef] [PubMed]
- Laboure, H.; Repoux, M.; Courcoux, P.; Feron, G.; Guichard, E. Inter-individual retronasal aroma release variability during cheese consumption: Role of food oral processing. Food Res. Int. 2014, 64, 692–700. [Google Scholar] [CrossRef] [PubMed]
- Canterini, C.C.; Gaubil-Kaladjian, I.; Vatin, S.; Viard, A.; Wolak-Thierry, A.; Bertin, E. Rapid eating is linked to emotional eating in obese women relieving from bariatric surgery. Obes. Surg. 2018, 28, 526–531. [Google Scholar] [CrossRef] [PubMed]
- Duffy, V.B.; Peterson, J.; Bartoshuk, L.M. Associations between taste genetics, oral sensations and alcohol intake. Physiol. Behav. 2004, 82, 435–445. [Google Scholar] [CrossRef] [PubMed]
- Dinehart, M.E.; Hayes, J.E.; Bartoshuk, L.M.; Lanier, S.L.; Duffy, V.B. Bitter taste markers explain variability in vegetable sweetness, bitterness, and intake. Physiol. Behav. 2006, 87, 304–313. [Google Scholar] [CrossRef] [PubMed]
- Fischer, M.E.; Cruickshanks, K.J.; Schubert, C.R.; Pinto, A.; Huang, G.H.; Klein, B.E.; Klein, R.; Pankow, J.S. The association of taste with change in adiposity-related health measures. J. Acad. Nutr. Diet 2014, 114, 1195–1202. [Google Scholar] [CrossRef] [PubMed]
- Ortega, F.J.; Aguera, Z.; Sabater, M.; Moreno-Navarrete, J.M.; Alonso-Ledesma, I.; Xifra, G.; Botas, P.; Delgado, E.; Jimenez-Murcia, S.; Fernandez-Garcia, J.C.; et al. Genetic variations of the bitter taste receptor TAS2R38 are associated with obesity and impact on single immune traits. Mol. Nutr. Food Res. 2016, 60, 1673–1683. [Google Scholar] [CrossRef] [PubMed]
- Coluzzi, I.; Raparelli, L.; Guarnacci, L.; Paone, E.; Del Genio, G.; le Roux, C.W.; Silecchia, G. Food intake and changes in eating behavior after Laparoscopic Sleeve Gastrectomy. Obes. Surg. 2016, 26, 2059–2067. [Google Scholar] [CrossRef] [PubMed]
- Zoon, H.F.A.; de Bruijn, S.E.M.; Smeets, P.A.M.; de Graaf, C.; Janssen, I.M.C.; Schijns, W.; Aarts, E.O.; Jager, G.; Boesveldt, S. Altered neural responsivity to food cues in relation to food preferences, but not appetite-related hormone concentrations after RYGB-surgery. Behav. Brain Res. 2018, 353, 194–202. [Google Scholar] [CrossRef]
- Mack, I.; Olschlager, S.; Sauer, H.; von Feilitzsch, M.; Weimer, K.; Junne, F.; Peeraully, R.; Enck, P.; Zipfel, S.; Teufel, M. Does Laparoscopic Sleeve Gastrectomy improve depression, stress and eating behaviour? A 4-Year Follow-up Study. Obes. Surg. 2016, 26, 2967–2973. [Google Scholar] [CrossRef]
- Karlsson, J.; Persson, L.O.; Sjostrom, L.; Sullivan, M. Psychometric properties and factor structure of the Three-Factor Eating Questionnaire (TFEQ) in obese men and women. Results from the Swedish Obese Subjects (SOS) study. Int. J. Obes. Relat. Metab. Disord. 2000, 24, 1715–1725. [Google Scholar] [CrossRef]
- Lang, T.; Hauser, R.; Buddeberg, C.; Klaghofer, R. Impact of gastric banding on eating behavior and weight. Obes. Surg. 2002, 12, 100–107. [Google Scholar] [CrossRef]
- Roehrig, M.; Masheb Rm Fau-White, M.A.; White Ma Fau-Rothschild, B.S.; Rothschild Bs Fau-Burke-Martindale, C.H.; Burke-Martindale Ch Fau-Grilo, C.M.; Grilo, C.M. Chronic dieting among extremely obese bariatric surgery candidates. Obes. Surg. 2009, 19, 1116–1123. [Google Scholar] [CrossRef]
- Lowe, M.R.; Doshi Sd Fau-Katterman, S.N.; Katterman Sn Fau-Feig, E.H.; Feig, E.H. Dieting and restrained eating as prospective predictors of weight gain. Front. Psychol. 2013, 4, 577. [Google Scholar] [CrossRef] [PubMed]
- Schaumberg, K.; Anderson, D.A.; Anderson, L.M.; Reilly, E.E.; Gorrell, S. Dietary restraint: What’s the harm? A review of the relationship between dietary restraint, weight trajectory and the development of eating pathology. Clin. Obes. 2016, 6, 89–100. [Google Scholar] [CrossRef] [PubMed]
- Polivy, J.; Herman, C.P. Dieting and binging. A causal analysis. Am. Psychol. 1985, 40, 193–201. [Google Scholar] [CrossRef] [PubMed]
- Van de Laar, A.W.; van Rijswijk, A.S.; Kakar, H.; Bruin, S.C. Sensitivity and specificity of 50% excess weight loss (50%EWL) and twelve other bariatric criteria for weight loss success. Obes. Surg. 2018, 28, 2297–2304. [Google Scholar] [CrossRef]
- Andromalos, L.; Crowley, N.; Brown, J.; Craggs-Dino, L.; Handu, D.; Isom, K.; Lynch, A.; DellaValle, D. Nutrition Care in Bariatric Surgery: An Academy Evidence Analysis Center Systematic Review. J. Acad. Nutr. Diet. 2018, 119, 678–686. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Pre-Op n = 49 | Post-Surg n = 48 | Success %EWL n = 23 | Unsuccess %EWL n = 25 | Success %WL n = 26 | Unsuccess %WL n = 22 |
|---|---|---|---|---|---|---|
| Age † | 45.7 ± 1.6 | 48.44 ± 1.6 | 47.8 ± 1.8 | 49.0 ± 2.5 | 46.4 ± 2.2 | 50.8 ± 2.2 |
| Race ¥ | ||||||
| Black | 25 | 21 | 13 | 28 | 15 | 27 |
| Other | 4 | 10 | 17 | 4 | 15 | 5 |
| White | 71 | 69 | 70 | 68 | 70 | 68 |
| Ethnicity ¥ | ||||||
| Hispanic | 16 | 13 | 22 | 4 | 19 | 5 |
| Not-Hispanic | 84 | 87 | 78 | 96 | 82 | 95 |
| Surgery Type ¥ | ||||||
| RYGB | 51 | 50 | 48 | 52 | 59 | 38 |
| SG | 49 | 50 | 52 | 48 | 41 | 62 |
| Pre-Op † | ||||||
| Weight (lbs) | 266.5 ± 6.7 | 273.4 ± 8.8 | 238.4 ± 6.4 b | 305.6 ± 12.7 a | 277.8 ± 14.9 | 268.1 ± 7.5 |
| BMI †† | 45.7 ± 1.2 | 47.0 ± 1.6 | 41.0 ± 1.3 b | 52.6 ± 2.4 a | 48.0 ± 2.8 | 45.9 ± 1.4 |
| Post-Surgery † (1 year) | ||||||
| Weight (lbs) | 198.3 ± 7.9 | 156.1 ± 4.3 b | 240.6 ± 8.0 a | 183.7 ± 11.7 b | 219.5 ± 6.8 a | |
| BMI †† | 33.8 ± 1.4 | 26.4 ± 0.7 b | 41.2 ± 1.7 a | 31.4 ± 2.1 b | 37.3 ± 1.4 a |
| %WL | ||||
|---|---|---|---|---|
| Successful | Unsuccessful | Total | ||
| %EWL | Successful | 19 | 4 | 23 |
| Unsuccessful | 7 | 18 | 25 | |
| Total | 26 | 22 | 48 | |
| Smell † | Post-Op - %EWL | Post-Op - %WL | Pre-Op | NHANES | ||
|---|---|---|---|---|---|---|
| Successful | Unsuccessful | Successful | Unsuccessful | |||
| Problem since surgery | ||||||
| Yes | 9 | 8 | 10 | 5 | ||
| No | 87 | 92 | 85 | 95 | ||
| Don’t Know | 4 | 0 | 5 | 0 | ||
| Problem in past year | ||||||
| Yes | 9 | 8 | ||||
| No | 91 | 92 | ||||
| Description since surgery | ||||||
| Excellent | 35 | 42 | 41 | 35 | ||
| Good | 35 | 46 | 37 | 45 | ||
| Little trouble | 17 | 8 | 11 | 15 | ||
| Moderate trouble | 4 | 0 | 4 | 0 | ||
| A lot of trouble | 0 | 0 | 0 | 0 | ||
| Loss smell | 0 | 0 | 0 | 0 | ||
| Don’t Know | 9 | 4 | 7 | 5 | ||
| Change since 25 years | ||||||
| Better | 22 | 6 | ||||
| Worse | 7 | 14 | ||||
| No Change | 65 | 79 | ||||
| Don’t Know | 7 | 0 | ||||
| Change since surgery | ||||||
| Better | 22 | 24 | 30 | 14 | ||
| Worse | 4 | 4 | 4 | 5 | ||
| No Change | 74 | 68 | 67 | 76 | ||
| Don’t Know | 0 | 4 | 0 | 5 | ||
| Specific problem since surgery | ||||||
| None | 65 | 68 | 59 | 76 | ||
| less able | 0 | 8 | 0 | 9 | ||
| parosmia or phantom | 26 | 8 | 33 | 5 | ||
| smell stronger/make sick or anxious | 4 | 12 | 4 | 5 | ||
| Don’t Know | 4 | 4 | 4 | 5 | ||
| Specific problem in past year | ||||||
| None | 72 | |||||
| less able | 4 | |||||
| parosmia or phantom | 11 | 7 | ||||
| smell stronger/make sick or anxious | 13 | |||||
| Don’t Know | 0 | |||||
| Taste † | Post-Op - EWL | Post-Op - % Wt Loss | Pre-Op | NHANES | ||
|---|---|---|---|---|---|---|
| Successful | Unsuccessful | Successful | Unsuccessful | |||
| Problem since surgery | ||||||
| Yes | 26 | 28 | 30 | 24 | ||
| No | 70 | 68 | 66 | 71 | ||
| Don’t Know | 4 | 4 | 4 | 5 | ||
| Problem in past year | ||||||
| Yes | 6 | 5 | ||||
| No | 94 | 95 | ||||
| Description since surgery | ||||||
| Excellent | 43 | 42 | 48 | 35 | ||
| Good | 39 | 33 | 33 | 40 | ||
| Little trouble | 9 | 17 | 11 | 15 | ||
| Moderate trouble | 4 | 4 | 4 | 5 | ||
| A lot of trouble | 4 | 4 | 4 | 5 | ||
| Loss smell | 0 | 0 | 0 | 0 | ||
| Don’t Know | 0 | 0 | 0 | 0 | ||
| Change since 25 yrs across each taste quality | ||||||
| Better | 21.7 to 39.1 | 8.7 to 30.4 | 42.3 | 23.8 | 17–26 | 4–8 |
| Worse | 8.7 to 21.7 | 13.0 to 17.4 | 15.4 | 19.1 | 9–13 | 7–13 |
| No Change | 52.2 to 60.9 | 60.1 to 82.6 | 42.3 | 57.1 | 60–64 | 87–92 |
| Don’t Know | 0 to 8.7 | 0 to 17.4 | 0.0 | 0.0 | 6–9 | <1 |
| Ability to taste food flavor as good as when younger | ||||||
| Yes | 85 | 92 | ||||
| No | 6 | 7 | ||||
| Don’t Know | 8 | 1 | ||||
| Change since surgery across each taste quality | ||||||
| Better | 22–44 | 8–28 | 26–44 | 0–24 | ||
| Worse | 9–22 | 12–20 | 11–19 | 14–19 | ||
| No Change | 32–61 | 56–72 | 41–59 | 57–71 | ||
| Don’t Know | 0–9 | 0–12 | 0–7 | 0–14 | ||
| Ability to taste food flavor as good since surgery | ||||||
| Yes | 82 | 88 | 89 | 81 | ||
| No | 9 | 8 | 4 | 14 | ||
| Don’t Know | 9 | 4 | 7 | 5 | ||
| Specific problem since surgery | ||||||
| None | 39 | 52 | 37 | 55 | ||
| Can’t taste some things | 0 | 8 | 4 | 5 | ||
| Things don’t taste right | 48 | 20 | 45 | 27 | ||
| taste stronger | 13 | 20 | 15 | 14 | ||
| Specific problem in past year | ||||||
| None | 87 | |||||
| less able | 0 | |||||
| dysgeusia | 7 | 6 | ||||
| stronger | 2 | |||||
| Don’t Know | 4 | |||||
| %EWL | %WL | |||||
|---|---|---|---|---|---|---|
| Pre-Op | Post-Surg | Successful | Unsuccessful | Successful | Unsuccessful | |
| Nontaster | 29 | 26 | 30 | 21 | 27 | 24 |
| Medium taster | 51 | 45 | 43 | 46 | 46 | 43 |
| Supertaster | 20 | 30 | 26 | 33 | 27 | 33 |
| Group | Cronbach’s α | Mean ± SEM |
|---|---|---|
| Physical Activity—bicycling, working up a sweat, playing sports, exercising with others, exercising alone, going to the gym, taking the stairs | 0.84 | 15.12 ± 3.8 |
| Sweet foods—cookies, cake, or pie, jam or jelly, ice cream, icing | 0.81 | 25.46 ± 4.2 |
| Alcohol—vodka, gin, or scotch, white wine, red wine, beer | 0.79 | −31.54 ± 5.2 |
| High-Fat Protein—bacon, pizza, fried chicken, sausage, fried fish, pork chops, charred meat, cheddar cheese | 0.77 | 34.52 ± 3.1 |
| Sour—sour pickles, lemon, vinegar | 0.72 | 13.0 ± 4.3 |
| Vegetable—eggplant, spinach or greens, beets, sautéed mushrooms, asparagus, raw carrots, broccoli, tomatoes | 0.71 | 28.7 ± 3.3 |
| Refined Carbohydrate—crackers, white potato, cornflakes, white rice, pasta, bagel or rolls | 0.70 | 25.2 ± 3.1 |
| Fruit—strawberries, pineapple, cherries, pear, melon, banana | 0.70 | 48.2 ± 3.0 |
| Spicy/flavorful —Tabasco sauce, raw onion, chili pepper, garlic, soy sauce, blue cheese, dark chocolate | 0.67 | −2.8 ± 3.4 |
| Fat—olive oil, salad dressing, mayonnaise, butter | 0.66 | 28.9 ± 3.3 |
| Salt—salting foods, ham, pretzels, olives, tortilla or potato chips, French fries | 0.65 | 20.2 ± 3.3 |
| Sweet Drinks—orange juice, coffee drinks, sugar-sweetened coffee or tea, soda | 0.58 | 1.43 ± 4.3 |
| Bitter—tea, grapefruit juice, black coffee, unsweetened iced tea | 0.56 | 11.2 ± 3.6 |
| Pleasant—hearing favorite music, going to a coffee shop, going to a pub or bar, smell of cut grass, cooling off on a hot day, television | 0.55 | 43.2 ± 2.7 |
| Low-Fat Protein—tuna or salmon, baked chicken, plain yogurt, shrimp | 0.52 | 38.1 ± 3.4 |
| Fiber—fiber bar, oatmeal, lentils or beans, whole wheat bread | 0.40 | 28.9 ± 3.0 |
| Unpleasant—glare of headlights, car accident, seeing a mouse at home | 0.37 | −72.0 ± 2.3 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hubert, P.A.; Papasavas, P.; Stone, A.; Swede, H.; Huedo-Medina, T.B.; Tishler, D.; Duffy, V.B. Associations between Weight Loss, Food Likes, Dietary Behaviors, and Chemosensory Function in Bariatric Surgery: A Case-Control Analysis in Women. Nutrients 2019, 11, 804. https://doi.org/10.3390/nu11040804
Hubert PA, Papasavas P, Stone A, Swede H, Huedo-Medina TB, Tishler D, Duffy VB. Associations between Weight Loss, Food Likes, Dietary Behaviors, and Chemosensory Function in Bariatric Surgery: A Case-Control Analysis in Women. Nutrients. 2019; 11(4):804. https://doi.org/10.3390/nu11040804
Chicago/Turabian StyleHubert, Patrice A., Pavlos Papasavas, Andrea Stone, Helen Swede, Tania B. Huedo-Medina, Darren Tishler, and Valerie B. Duffy. 2019. "Associations between Weight Loss, Food Likes, Dietary Behaviors, and Chemosensory Function in Bariatric Surgery: A Case-Control Analysis in Women" Nutrients 11, no. 4: 804. https://doi.org/10.3390/nu11040804