Multiple Micronutrient Supplementation Using Spirulina platensis during the First 1000 Days is Positively Associated with Development in Children under Five Years: A Follow up of A Randomized Trial in Zambia


Abstract
:1. Introduction
2. Materials and Methods
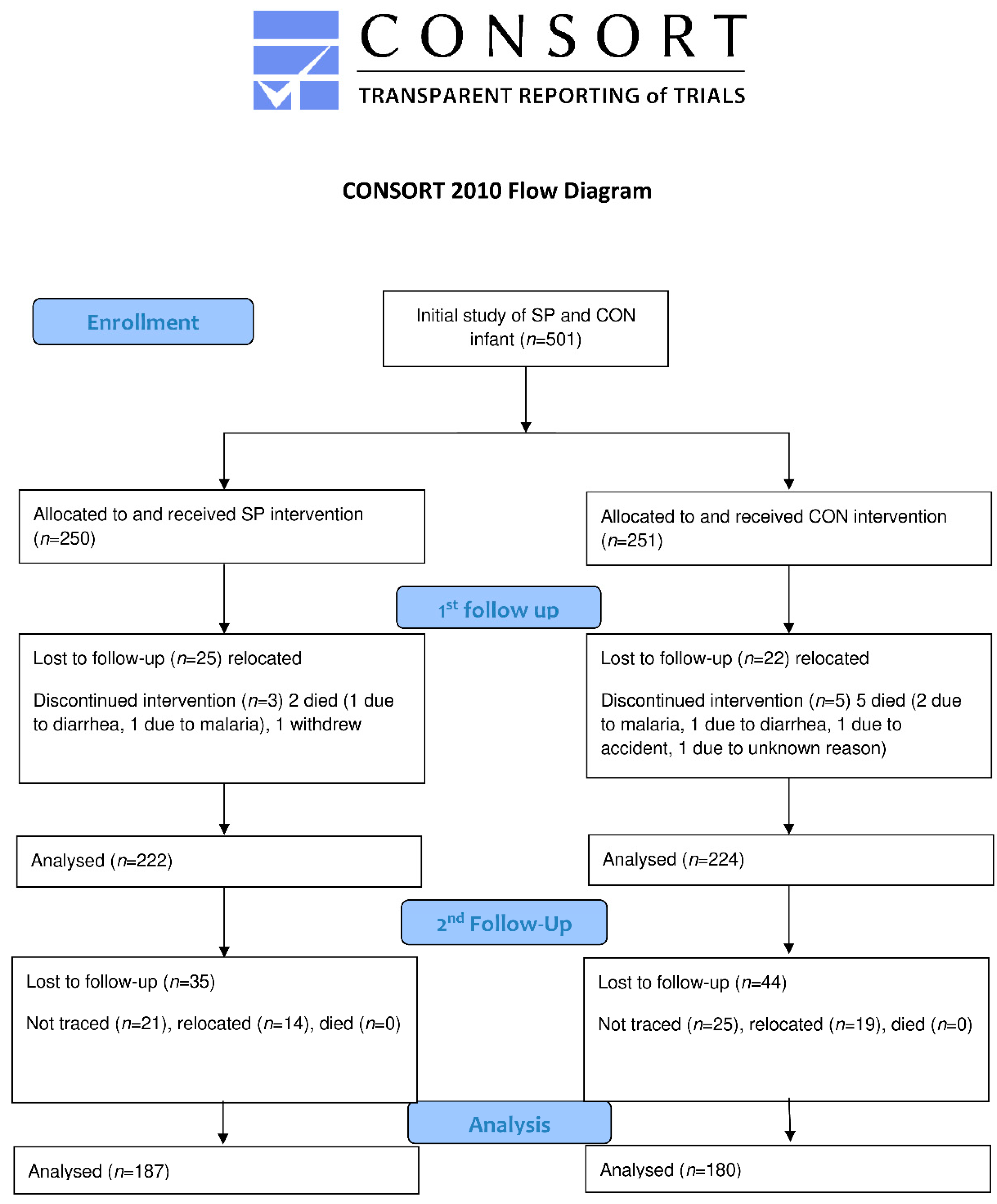
2.1. Study Design
2.2. Measurement
2.3. Ethical Statement
2.4. Statistical Analysis
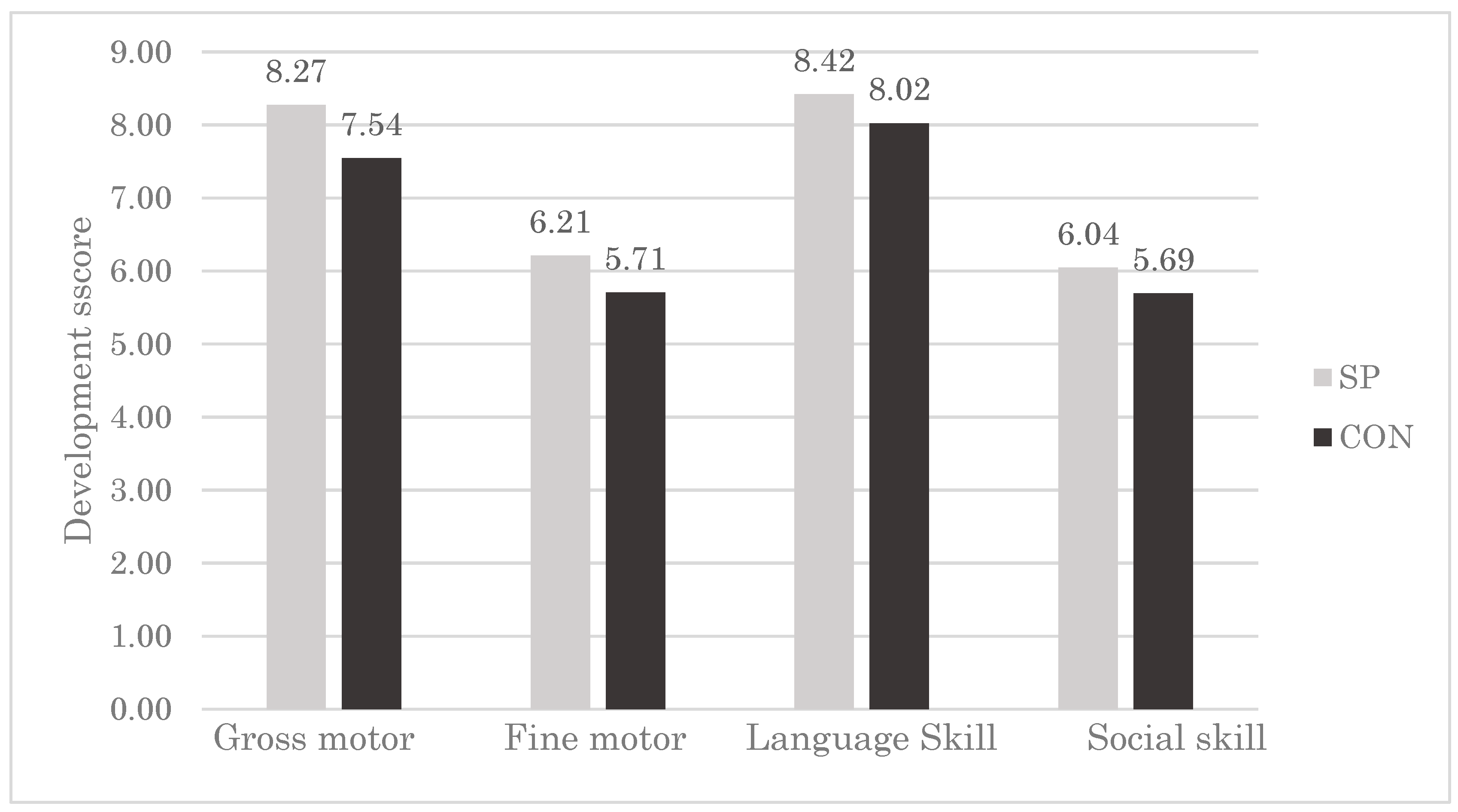
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Black, M.M.; Walker, S.P.; Fernald, L.C.; Andersen, C.T.; DiGirolamo, A.M.; Lu, C.; McCoy, D.C.; Fink, G.; Shawar, Y.R.; Shiffman, J.; et al. Lancet Early Childhood Development Series Steering Committee. Early childhood development coming of age: science through the life course. Lancet 2017, 389, 77–90. [Google Scholar] [CrossRef]
- Heckman, J.J. Skill formation and the economics of investing in disadvantaged children. Science 2006, 312, 1900–1902. [Google Scholar] [CrossRef] [PubMed]
- Grantham-McGregor, S.; Cheung, Y.B.; Cueto, S.; Glewwe, P.; Richter, L.; Strupp, B. International Child Development Steering Group. Developmental potential in the first 5 years for children in developing countries. Lancet 2007, 369, 60–70. [Google Scholar] [CrossRef]
- Sánchez, M.; Bernal-Castillo, J.; Rozo, C.; Rodríguez, I. Spirulina (Arthrospira): An edible microorganism: A review. Univ. Sci. (Bogota) 2003, 1, 7–24. [Google Scholar]
- Khan, Z.; Bhadouria, P.; Bisen, P.S. Nutritional and therapeutic potential of spirulina. Curr. Pharm. Biotechnol. 2005, 5, 373–379. [Google Scholar] [CrossRef]
- Habib, M.A.; Parvin, M.; Huntington, T.C.; Hasan, M.R. A review on culture, production and use of spirulina as food for humans and feeds for domestic animals and fish. FAO Fish. Aquac. Circ. 2008, 1034, 33. [Google Scholar]
- Ravi, M.; De, S.L.; Azharuddin, S.; Paul, S.F. The beneficial effects of Spirulina focusing on its immunomodulatory and antioxidant properties. Nutr. Diet Suppl. 2010, 2, 73–83. [Google Scholar]
- Campanella, L.; Russo, M.V.; Avino, P. Free and total amino acid composition in blue-green algae. Ann. Chim. 2002, 4, 343–352. [Google Scholar]
- Siva Kiran, R.R.; Madhu, G.M.; Satyanarayana, S.V. Spirulina in combating protein energy malnutrition (pem) and protein energy wasting (PEW)—A review. J. Nutr. Res. 2015, 1, 62–79. [Google Scholar]
- Ötleş, S.; Pire, R. Fatty acid composition of Chlorella and spirulina microalgae species. J. AOAC Int. 2001, 6, 1708–1714. [Google Scholar]
- Sinha, S.; Patro, N.; Patro, I.K. Maternal protein malnutrition: Current and future perspectives of spirulina supplementation in neuroprotection. Front. Neurosci. 2018, 12, 966. [Google Scholar] [CrossRef] [PubMed]
- Masuda, K.; Inoue, Y.; Inoue, R.; Nakamura, A.; Chitundu, M.; Murakami, J.; Ota, Y.; Matsugami, J. Spirulina effectiveness study on child malnutrition in Zambia. IDS Res. 2014, 49–56, Special Collection. [Google Scholar]
- Simpore, J.; Kabore, F.; Zongo, F.; Dansou, D.; Bere, A.; Pignatelli, S.; Biondi, D.M.; Ruberto, G.; Musumeci, S. Nutrition rehabilitation of undernourished children utilizing spiruline and misola. Nutr. J. 2006, 1, 3. [Google Scholar] [CrossRef] [PubMed]
- Simpore, J.; Zongo, F.; Kabore, F.; Dansou, D.; Bere, A.; Nikiema, J.B.; Pignatelli, S.; Biondi, D.M.; Ruberto, G.; Musumeci, S. Nutrition rehabilitation of HIV-infected and HIV-negative undernourished children utilizing spirulina. Ann. Nutr. Metab. 2005, 6, 373–380. [Google Scholar] [CrossRef]
- Abed, E.; Ihab, A.N.; Suliman, E.; Mahmoud, A. Impact of spirulina on nutritional status, haematological profile and anaemia status in malnourished children in the Gaza Strip: randomized clinical trial. Matern. Pediatr. Nutr. 2016, 110, 2. [Google Scholar]
- Masuda, K.; Chitundu, M. Multiple micronutrient supplementation using spirulina platensis and infant growth, morbidity, and motor development: evidence from a randomized trial in Zambia. PLoS ONE 2019, 14, e0211693. [Google Scholar] [CrossRef]
- Masuda, K.; Chitundu, M. Post Intervention Morbidity and Growth Among Zambian Children Who Received Multiple Micronutrient Supplementation Using Spirulina Platensis: Evidence From A Randomized Trial in Zambia. Available online: http://cei.ier.hit-u.ac.jp/Japanese/WP2018-21.pdf (accessed on 16 February 2019).
- Gladstone, M.; Lancaster, G.A.; Umar, E.; Nyirenda, M.; Kayira, E.; van den Broek, N.R.; Smyth, R.L. The Malawi Developmental Assessment Tool (MDAT): The creation, validation, and reliability of a tool to assess child development in rural African settings. PLoS Med. 2010, 7, e1000273. [Google Scholar] [CrossRef]
- WHO Multicentre Growth Reference Study Group; de Onis, M. WHO Child Growth Standards based on length/height, weight and age. Acta. Paediatr. 2006, 95, 76–85. [Google Scholar]
- Larson, L.M.; Young, M.F.; Bauer, P.J.; Mehta, R.; Girard, A.W.; Ramakrishnan, U.; Verma, P.; Chaudhuri, I.; Srikantiah, S.; Martorell, R. Effectiveness of a home fortification programme with multiple micronutrients on infant and young child development: A cluster-randomised trial in rural Bihar, India. Br. J. Nutr. 2018, 120, 176–187. [Google Scholar] [CrossRef] [PubMed]
- Matias, S.L.; Mridha, M.K.; Tofail, F.; Arnold, C.D.; Khan, M.S.A.; Siddiqui, Z.; Ullah, M.B.; Dewey, K.G. Home fortification during the first 1000 d improves child development in Bangladesh: A cluster-randomized effectiveness trial–3. Am. J. Clin. Nutr. 2017, 105, 958–969. [Google Scholar] [CrossRef]
- Prado, E.L.; Abbeddou, S.; Yakes Jimenez, E.; Somé, J.W.; Ouédraogo, Z.P.; Vosti, S.A.; Dewey, K.G.; Brown, K.H.; Hess, S.Y.; Ouédraogo, J.B. Lipid- based nutrient supplements plus malaria and diarrhea treatment increase infant development scores in a cluster-randomized trial in Burkina Faso–3. J. Nutr. 2015, 146, 814–822. [Google Scholar] [CrossRef]
- Yousafzai, A.K.; Rasheed, M.A.; Rizvi, A.; Armstrong, R.; Bhutta, Z.A. Effect of integrated responsive stimulation and nutrition interventions in the Lady Health Worker programme in Pakistan on child development, growth, and health outcomes: A cluster-randomised factorial effectiveness trial. Lancet 2014, 384, 1282–1293. [Google Scholar] [CrossRef]
- Prado, E.L.; Alcock, K.J.; Muadz, H.; Ullman, M.T.; Shankar, A.H. Maternal multiple micronutrient supplements and child cognition: a randomized trial in Indonesia. Pediatrics 2012, 130, e536–e546. [Google Scholar] [CrossRef]
- Lozoff, B.; Castillo, M.; Clark, K.M.; Smith, J.B. Iron-fortified vs low-iron infant formula: Developmental outcome at 10 years. Arch. Pediatr. Adolesc. Med. 2012, 166, 208–215. [Google Scholar] [CrossRef]
- Moramarco, S.; Amerio, G.; Gozza Maradini, G.; Garuti, E. The Rainbow Project: A Model to Fight Child Malnutrition in Zambia. IDS Res. 2014, 57–61, Special Collection. [Google Scholar]
- Moramarco, S.; Amerio, G.; Kasengele Chipoma, J.; Nielsen-Saines, K.; Palombi, L.; Buonomo, E. Filling the Gaps for Enhancing the Effectiveness of Community-Based Programs Combining Treatment and Prevention of Child Malnutrition: Results from the Rainbow Project 2015–17 in Zambia. Int. J. Environ. Res Public Health 2018, 15, 1807. [Google Scholar] [CrossRef]
- Prado, E.L.; Dewey, K.G. Nutrition and brain development in early life. Nutr. Rev. 2014, 72, 267–284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levitsky, D.A.; Strupp, B.J. Malnutrition and the brain: changing concepts, changing concerns. J. Nutr. 1995, 125, 2212S–2220S. [Google Scholar] [CrossRef]
- Sika, M.K.; Adu-Afarwuah, S.; Young, R.R.; Oaks, B.M.; Tamakloe, S.M.; Ocansey, M.E.; Okronipa, H.; Prado, E.L.; Dewey, K.G. Maternal–Infant Supplementation with Small-Quantity Lipid-Based Nutrient Supplements Does Not Affect Child Blood Pressure at 4–6 Y in Ghana: Follow-up of a Randomized Trial. J. Nutr. 2019, 149, 522–531. [Google Scholar]
- Null, C.; Stewart, C.P.; Pickering, A.J.; Dentz, H.N.; Arnold, B.F.; Arnold, C.D.; Benjamin-Chung, J.; Clasen, T.; Dewey, K.G.; Fernald, L.C.H.; et al. Effects of water quality, sanitation, handwashing, and nutritional interventions on diarrhoea and child growth in rural Kenya: a cluster-randomised controlled trial. The Lancet Glob. Health 2018, 6, e316–e329. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| SP | CON | |
|---|---|---|
| (n = 187) | (n = 180) | |
| Child characteristics | ||
| Age at follow up (months) | 43.0 ± 4.5 | 43.5 ± 5.0 |
| Child female (%) | 52.1 | 46.5 |
| Stunting at baseline (%) | 42.1 | 43.0 |
| Underweight at baseline (%) | 19.5 | 24.3 |
| Wasting at baseline (%) | 9.7 | 10.7 |
| Dietary diversity score (0–7) | 5.2 ± 1.0 | 5.2 ± 1.0 |
| HIV-positive at baseline (%) | 3.1 | 2.5 |
| Child exclusively breastfed for 6 months (%) | 89.5 | 90.1 |
| Length of exclusive breastfeeding (months) | 5.9 ± 0.5 | 5.8 ± 0.5 |
| Maternal characteristics | ||
| Maternal age at baseline (years) | 28.1 ± 6.5 | 27.6 ± 7.5 |
| Maternal height at baseline (cm) | 152.5 ± 12.8 | 154.1 ± 10.6 |
| Maternal weight at baseline (kg) | 49.7 ± 7.3 | 49.4 ± 8.5 |
| Maternal education at baseline (years) | 6.1 ± 4.7 | 5.9 ± 4.3 |
| Household characteristics | ||
| Farmer (%) | 61.7 | 69.1 |
| Number of household members at baseline (persons) | 5.8 ± 2.1 | 5.7 ± 2.5 |
| Number of household members under the age of 5 at baseline (persons) | 2.2 ± 0.9 | 2.2 ± 1.1 |
| Households which had access to electricity at baseline (%) | 1.1 | 1.1 |
| Outcome: Standardized z Score Measuring | Motor Development | Mental Development | Gross Motor Development | Fine Motor Development | Language Skill | Personal-Social Skills |
|---|---|---|---|---|---|---|
| All children | ||||||
| Effect size | 0.42 *** | 0.33 *** | 0.37 *** | 0.38 *** | 0.24 ** | 0.28 ** |
| 95% CI | (0.22, 0.63) | (0.12, 0.54) | (0.16, 0.58) | (0.18, 0.59) | (0.03, 0.45) | (0.06, 0.49) |
| Children with HAZ < −2.0 at baseline (n = 141) | ||||||
| Effect size | 0.57 *** | 0.37 ** | 0.55 *** | 0.46 *** | 0.22 | 0.41 ** |
| 95% CI | (0.25, 0.89) | (0.04, 0.70) | (0.23, 0.88) | (0.12, 0.80) | (−0.11, 0.55) | (0.05, 0.77) |
| Children with HAZ > −2.0 at baseline (n = 190) | ||||||
| Effect size | 0.36 ** | 0.23 | 0.25 * | 0.35 ** | 0.15 | 0.20 |
| 95% CI | (0.07, 0.64) | (−0.07, 0.52) | (−0.04, 0.54) | (0.07, 0.63) | (−0.12, 0.43) | (−0.11, 0.51) |
| Children with dietary diversity score < median at baseline (n = 128) | ||||||
| Effect size | 0.75 *** | 0.41 ** | 0.66 *** | 0.67 *** | 0.34 ** | 0.27 |
| 95% CI | (0.40, 1.09) | (0.07, 0.76) | (0.27, 1.04) | (0.36, 0.98) | (0.03, 0.66) | (−0.09, 0.62) |
| Children with dietary diversity score > median at baseline (n = 209) | ||||||
| Effect size | 0.20 | 0.27 * | 0.22 | 0.13 | 0.16 | 0.32 ** |
| 95% CI | (−0.07, 0.47) | (−0.01, 0.55) | (−0.06, 0.49) | (−0.14, 0.39) | (−0.12, 0.43) | (0.03, 0.61) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Masuda, K.; Chitundu, M. Multiple Micronutrient Supplementation Using Spirulina platensis during the First 1000 Days is Positively Associated with Development in Children under Five Years: A Follow up of A Randomized Trial in Zambia. Nutrients 2019, 11, 730. https://doi.org/10.3390/nu11040730
Masuda K, Chitundu M. Multiple Micronutrient Supplementation Using Spirulina platensis during the First 1000 Days is Positively Associated with Development in Children under Five Years: A Follow up of A Randomized Trial in Zambia. Nutrients. 2019; 11(4):730. https://doi.org/10.3390/nu11040730
Chicago/Turabian StyleMasuda, Kazuya, and Maureen Chitundu. 2019. "Multiple Micronutrient Supplementation Using Spirulina platensis during the First 1000 Days is Positively Associated with Development in Children under Five Years: A Follow up of A Randomized Trial in Zambia" Nutrients 11, no. 4: 730. https://doi.org/10.3390/nu11040730