Association of Coffee Consumption with Hearing and Tinnitus Based on a National Population-Based Survey

Abstract
:1. Introduction
2. Materials and Methods
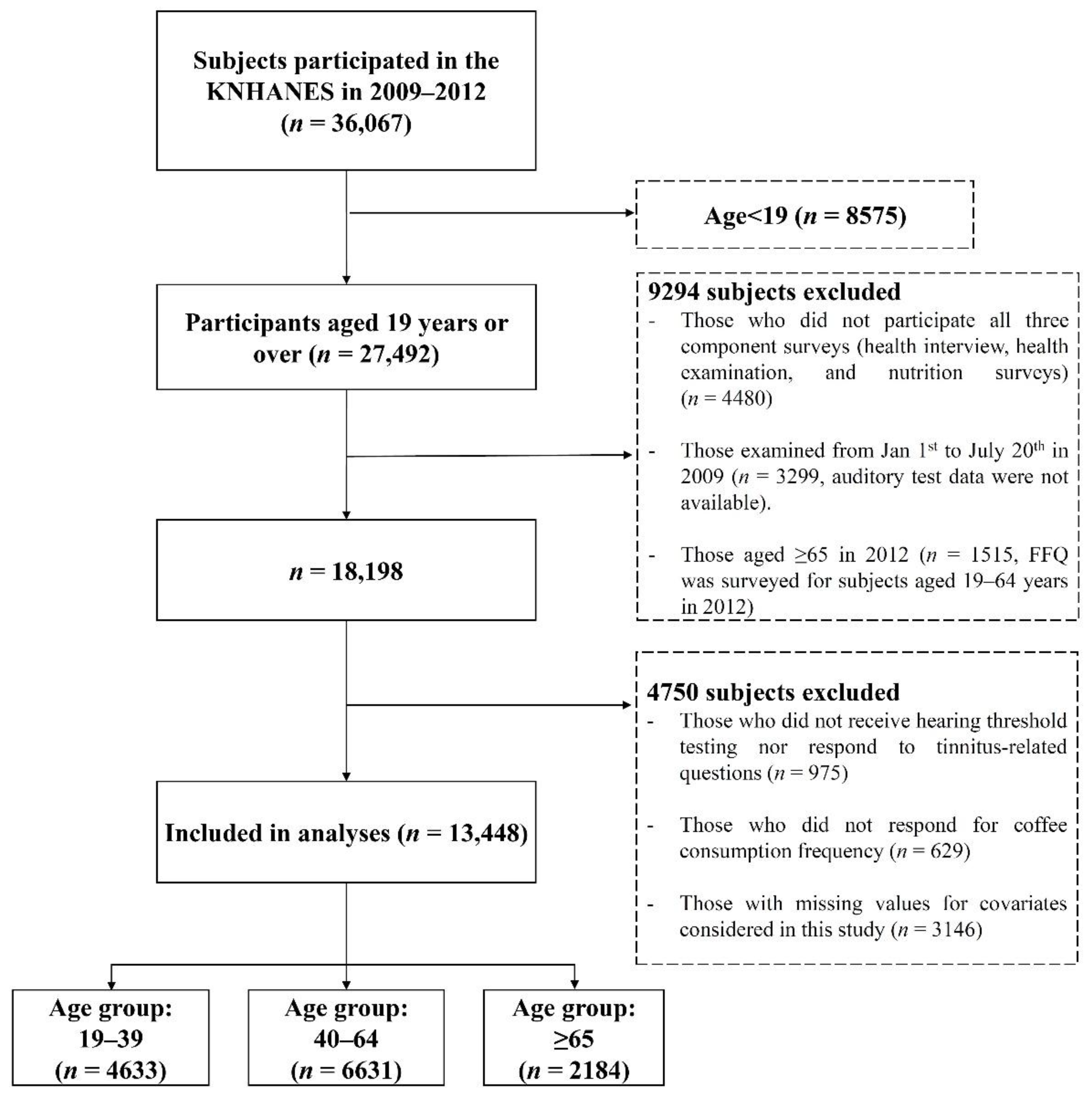
2.1. Study Population
2.2. Assessment of Coffee Consumption
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Ludwig, I.A.; Clifford, M.N.; Lean, M.E.; Ashihara, H.; Crozier, A. Coffee: Biochemistry and potential impact on health. Food Funct. 2014, 5, 1695–1717. [Google Scholar] [CrossRef] [PubMed]
- Butt, M.S.; Sultan, M.T. Coffee and its consumption: Benefits and risks. Crit. Rev. Food Sci. Nutr. 2011, 51, 363–373. [Google Scholar] [CrossRef] [PubMed]
- Bohn, S.K.; Blomhoff, R.; Paur, I. Coffee and cancer risk, epidemiological evidence and molecular mechanisms. Mol. Nutr. Food Res. 2014, 58, 915–930. [Google Scholar] [CrossRef] [PubMed]
- Santos, R.M.; Lima, D.R. Coffee consumption, obesity and type 2 diabetes: A mini-review. Eur. J. Nutr. 2016, 55, 1345–1358. [Google Scholar] [CrossRef] [PubMed]
- Qi, H.; Li, S. Dose-response meta-analysis on coffee, tea and caffeine consumption with risk of Parkinson’s disease. Geriatr. Gerontol. Int. 2014, 14, 430–439. [Google Scholar] [CrossRef] [PubMed]
- Salomone, F.; Galvano, F.; Li Volti, G. Molecular Bases Underlying the Hepatoprotective Effects of Coffee. Nutrients 2017, 9, 85. [Google Scholar] [CrossRef] [PubMed]
- Cano-Marquina, A.; Tarin, J.J.; Cano, A. The impact of coffee on health. Maturitas 2013, 75, 7–21. [Google Scholar] [CrossRef] [PubMed]
- Rhee, J.; Kim, R.; Kim, Y.; Tam, M.; Lai, Y.; Keum, N.; Oldenburg, C.E. Maternal Caffeine Consumption during Pregnancy and Risk of Low Birth Weight: A Dose-Response Meta-Analysis of Observational Studies. PLoS ONE 2015, 10, e0132334. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.R.; Lee, J.; Rota, M.; Lee, J.; Ahn, H.S.; Park, S.M.; Shin, D. Coffee consumption and risk of fractures: A systematic review and dose-response meta-analysis. Bone 2014, 63, 20–28. [Google Scholar] [CrossRef] [PubMed]
- Poole, R.; Kennedy, O.J.; Roderick, P.; Fallowfield, J.A.; Hayes, P.C.; Parkes, J. Coffee consumption and health: Umbrella review of meta-analyses of multiple health outcomes. BMJ 2017, 359, j5024. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.P.; Wu, Y.F.; Cheng, H.Y.; Xia, T.; Ding, H.; Wang, H.; Wang, Z.M.; Xu, Y. Habitual coffee consumption and risk of cognitive decline/dementia: A systematic review and meta-analysis of prospective cohort studies. Nutrition 2016, 32, 628–636. [Google Scholar] [CrossRef] [PubMed]
- Grosso, G.; Micek, A.; Castellano, S.; Pajak, A.; Galvano, F. Coffee, tea, caffeine and risk of depression: A systematic review and dose-response meta-analysis of observational studies. Mol. Nutr. Food Res. 2016, 60, 223–234. [Google Scholar] [CrossRef] [PubMed]
- Samoggia, A.; Riedel, B. Coffee consumption and purchasing behavior review: Insights for further research. Appetite 2018, 129, 70–81. [Google Scholar] [CrossRef] [PubMed]
- Jeszka-Skowron, M.; Zgola-Grzeskowiak, A.; Waskiewicz, A.; Stepien, L.; Stanisz, E. Positive and negative aspects of green coffee consumption–antioxidant activity versus mycotoxins. J. Sci. Food. Agric. 2017, 97, 4022–4028. [Google Scholar] [CrossRef] [PubMed]
- Moreira, A.S.P.; Nunes, F.M.; Simoes, C.; Maciel, E.; Domingues, P.; Domingues, M.R.M.; Coimbra, M.A. Data on coffee composition and mass spectrometry analysis of mixtures of coffee related carbohydrates, phenolic compounds and peptides. Data Brief 2017, 13, 145–161. [Google Scholar] [CrossRef] [PubMed]
- Park, M.K.; Im, G.J.; Chang, J.; Chae, S.W.; Yoo, J.; Han, W.G.; Hwang, G.H.; Jung, J.Y.; Choi, J.; Jung, H.H.; et al. Protective effects of caffeic acid phenethyl ester (CAPE) against neomycin-induced hair cell damage in zebrafish. Int. J. Pediatr. Otorhinolaryngol. 2014, 78, 1311–1315. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.; Kim, S.H.; Rah, Y.C.; Chae, S.W.; Lee, J.D.; Md, B.D.; Park, M.K. Effects of caffeic acid on cisplatin-induced hair cell damage in HEI-OC1 auditory cells. Int. J. Pediatr. Otorhinolaryngol. 2014, 78, 2198–2204. [Google Scholar] [CrossRef] [PubMed]
- Chadha, S.; Cieza, A. Promoting global action on hearing loss: World hearing day. Int. J. Audiol. 2017, 56, 145–147. [Google Scholar] [CrossRef] [PubMed]
- Graydon, K.; Waterworth, C.; Miller, H.; Gunasekera, H. Global burden of hearing impairment and ear disease. J. Laryngol. Otol. 2018, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Stevens, G.; Flaxman, S.; Brunskill, E.; Mascarenhas, M.; Mathers, C.D.; Finucane, M.; Global Burden of Disease Hearing Loss Expert Group. Global and regional hearing impairment prevalence: An analysis of 42 studies in 29 countries. Eur. J. Public Health 2013, 23, 146–152. [Google Scholar] [CrossRef] [PubMed]
- WHO. The Global Burden of Disease: 2004 Update; World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
- Gomaa, M.A.; Elmagd, M.H.; Elbadry, M.M.; Kader, R.M. Depression, Anxiety and Stress Scale in Patients with Tinnitus and Hearing Loss. Eur. Arch. Otorhinolaryngol. 2014, 271, 2177–2184. [Google Scholar] [CrossRef] [PubMed]
- Peracino, A. Hearing loss and dementia in the aging population. Audiol. Neurootol. 2014, 19, 6–9. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Lee, H.J.; An, S.Y.; Sim, S.; Park, B.; Kim, S.W.; Lee, J.S.; Hong, S.K.; Choi, H.G. Analysis of the prevalence and associated risk factors of tinnitus in adults. PLoS ONE 2015, 10, e0127578. [Google Scholar] [CrossRef] [PubMed]
- McCormack, A.; Edmondson-Jones, M.; Somerset, S.; Hall, D. A systematic review of the reporting of tinnitus prevalence and severity. Hear Res. 2016, 337, 70–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schleuning, A.J.; Shi, Y.J.; Martin, W.H. Tinnitus. In Head and Neck Surgery—Otolaryngology; Bailey, B.J., Johnson, J.T., Newlands, S.D., Eds.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2006; p. 2241. [Google Scholar]
- Crummer, R.W.; Hassan, G.A. Diagnostic approach to tinnitus. Am. Fam. Physician 2004, 69, 120–126. [Google Scholar] [PubMed]
- Figueiredo, R.R.; Rates, M.J.; Azevedo, A.A.; Moreira, R.K.; Penido Nde, O. Effects of the reduction of caffeine consumption on tinnitus perception. Braz. J. Otorhinolaryngol. 2014, 80, 416–421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Claire, L.S.; Stothart, G.; McKenna, L.; Rogers, P.J. Caffeine abstinence: An ineffective and potentially distressing tinnitus therapy. Int. J. Audiol. 2010, 49, 24–29. [Google Scholar] [CrossRef] [PubMed]
- McCormack, A.; Edmondson-Jones, M.; Mellor, D.; Dawes, P.; Munro, K.J.; Moore, D.R.; Fortnum, H. Association of dietary factors with presence and severity of tinnitus in a middle-aged UK population. PLoS ONE 2014, 9, e114711. [Google Scholar] [CrossRef] [PubMed]
- Zawawi, F.; Bezdjian, A.; Mujica-Mota, M.; Rappaport, J.; Daniel, S.J. Association of Caffeine and Hearing Recovery after Acoustic Overstimulation Events in a Guinea Pig Model. JAMA Otolaryngol. Head Neck Surg. 2016, 142, 383–388. [Google Scholar] [CrossRef] [PubMed]
- Mujica-Mota, M.A.; Gasbarrino, K.; Rappaport, J.M.; Shapiro, R.S.; Daniel, S.J. The effect of caffeine on hearing in a guinea pig model of acoustic trauma. Am. J. Otolaryngol. 2014, 35, 99–105. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Sellero, I.; San-Roman-Rodriguez, E.; Santos-Perez, S.; Rossi-Izquierdo, M.; Soto-Varela, A. Caffeine intake and Meniere’s disease: Is there relationship? Nutr. Neurosci. 2017, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Sharon, J.D.; Trevino, C.; Schubert, M.C.; Carey, J.P. Treatment of Meniere’s Disease. Curr. Treat. Options Neurol. 2015, 17, 341. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.J.; Chang, C.K. Prevalence and risk factors of noise-induced hearing loss among liquefied petroleum gas (LPG) cylinder infusion workers in Taiwan. Ind. Health 2009, 47, 603–610. [Google Scholar] [CrossRef] [PubMed]
- Dixit, A.; Vaney, N.; Tandon, O.P. Effect of caffeine on central auditory pathways: An evoked potential study. Hear Res. 2006, 220, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Maitre, N.L.; Chan, J.; Stark, A.R.; Lambert, W.E.; Aschner, J.L.; Key, A.P. Effects of caffeine treatment for apnea of prematurity on cortical speech-sound differentiation in preterm infants. J. Child Neurol. 2015, 30, 307–313. [Google Scholar] [CrossRef] [PubMed]
- Hong, B.N.; Yi, T.H.; Park, R.; Kim, S.Y.; Kang, T.H. Coffee improves auditory neuropathy in diabetic mice. Neurosci. Lett. 2008, 441, 302–306. [Google Scholar] [CrossRef] [PubMed]
- Hong, B.N.; Yi, T.H.; Kim, S.Y.; Kang, T.H. High-dosage pyridoxine-induced auditory neuropathy and protection with coffee in mice. Biol. Pharm. Bull. 2009, 32, 597–603. [Google Scholar] [CrossRef] [PubMed]
- Nehlig, A.; Daval, J.L.; Debry, G. Caffeine and the central nervous system: Mechanisms of action, biochemical, metabolic and psychostimulant effects. Brain Res. Brain Res. Rev. 1992, 17, 139–170. [Google Scholar] [CrossRef]
- Bagueley D, A.G.; McFerran, D.; McKenna, L. Tinnitus: Consequences and Moderating Factors; Wiley-Blackwell: West Sussex, UK, 2013; p. 100. [Google Scholar]
- Miller, B.; O’Connor, H.; Orr, R.; Ruell, P.; Cheng, H.L.; Chow, C.M. Combined caffeine and carbohydrate ingestion: Effects on nocturnal sleep and exercise performance in athletes. Eur. J. Appl. Physiol. 2014, 114, 2529–2537. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Han, J.W.; Lee, J.R.; Byun, S.; Suh, S.W.; Kim, T.; Yoon, I.Y.; Kim, K.W. Lifetime Coffee Consumption, Pineal Gland Volume and Sleep Quality in Late Life. Sleep 2018. [Google Scholar] [CrossRef] [PubMed]
- Miguel, G.S.; Yaremchuk, K.; Roth, T.; Peterson, E. The effect of insomnia on tinnitus. Ann. Otol. Rhinol. Laryngol. 2014, 123, 696–700. [Google Scholar] [CrossRef] [PubMed]
- Glicksman, J.T.; Curhan, S.G.; Curhan, G.C. A prospective study of caffeine intake and risk of incident tinnitus. Am. J. Med. 2014, 127, 739–743. [Google Scholar] [CrossRef] [PubMed]
- Mazurek, B.; Szczepek, A.J.; Hebert, S. Stress and tinnitus. HNO 2015, 63, 258–265. [Google Scholar] [CrossRef] [PubMed]
- Schaaf, H.; Flohre, S.; Hesse, G.; Gieler, U. Chronic stress as an influencing factor in tinnitus patients. HNO 2014, 62, 108–114. [Google Scholar] [CrossRef] [PubMed]
- Roland, L.T.; Lenze, E.J.; Hardin, F.M.; Kallogjeri, D.; Nicklaus, J.; Wineland, A.M.; Fendell, G.; Peelle, J.E.; Piccirillo, J.F. Effects of mindfulness based stress reduction therapy on subjective bother and neural connectivity in chronic tinnitus. Otolaryngol. Head Neck Surg. 2015, 152, 919–926. [Google Scholar] [CrossRef] [PubMed]
- Caprioli, G.; Cortese, M.; Sagratini, G.; Vittori, S. The influence of different types of preparation (espresso and brew) on coffee aroma and main bioactive constituents. Int J. Food Sci. Nutr. 2015, 66, 505–513. [Google Scholar] [CrossRef] [PubMed]
- Narita, Y.; Inouye, K. Decrease in the acrylamide content in canned coffee by heat treatment with the addition of cysteine. J. Agric. Food Chem. 2014, 62, 12218–12222. [Google Scholar] [CrossRef] [PubMed]
- Maas, I.L.; Bruggemann, P.; Requena, T.; Bulla, J.; Edvall, N.K.; Hjelmborg, J.V.B.; Szczepek, A.J.; Canlon, B.; Mazurek, B.; Lopez-Escamez, J.A.; et al. Genetic susceptibility to bilateral tinnitus in a Swedish twin cohort. Genet. Med. 2017, 19, 1007–1012. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Symptoms by Group | Frequency of Coffee Consumption | ||||
|---|---|---|---|---|---|
| Total | Rarely | Monthly | Weekly | Daily | |
| Age group (19–39) | n = 4633 | n = 634 | n = 304 | n = 873 | n = 2822 |
| Hearing loss *, n (%) | |||||
| Unilateral | 55 (1.19%) | 11 (1.74%) | 2 (0.66%) | 6 (0.69%) | 36 (1.28%) |
| Bilateral | 8 (0.17%) | 1 (0.16%) | 0 (0.00%) | 3 (0.34%) | 4 (0.14%) |
| Tinnitus, n (%) | 837 (18.07%) | 130 (20.50%) | 62 (20.39%) | 177 (20.27%) | 468 (16.58%) |
| Tinnitus-related annoyance, n (%) | 179 (3.86%) | 33 (5.21%) | 13 (4.28%) | 26 (2.98%) | 107 (3.79%) |
| Age group (40–64) | n = 6631 | n = 656 | n = 308 | n = 899 | n = 4768 |
| Hearing loss *, n (%) | |||||
| Unilateral | 332 (5.01%) | 40 (6.1%) | 15 (4.87%) | 47 (5.23%) | 230 (4.82%) |
| Bilateral | 192 (2.90%) | 31 (4.73%) | 18 (5.84%) | 33 (3.67%) | 110 (2.31%) |
| Tinnitus, n (%) | 1321 (19.92%) | 149 (22.71%) | 64 (20.78%) | 191 (21.25%) | 917 (19.23%) |
| Tinnitus-related annoyance, n (%) | 414 (6.24%) | 50 (7.62%) | 18 (5.84%) | 66 (7.34%) | 280 (5.87%) |
| Age group (≥65) | n = 2184 | n = 429 | n = 122 | n = 383 | n = 1250 |
| Hearing loss *, n (%) | |||||
| Unilateral | 311 (14.24%) | 71 (16.55%) | 18 (14.75%) | 58 (15.14%) | 164 (13.12%) |
| Bilateral | 458 (20.97%) | 99 (23.08%) | 20 (16.39%) | 79 (20.63%) | 260 (20.80%) |
| Tinnitus, n (%) | 611 (27.98%) | 135 (31.47%) | 38 (31.15%) | 95 (24.80%) | 343 (27.44%) |
| Tinnitus-related annoyance, n (%) | 280 (12.82%) | 73 (17.02%) | 18 (14.75%) | 47 (12.27%) | 142 (11.36%) |
| Univariable Analysis | Multivariable Analysis * | |||||||
|---|---|---|---|---|---|---|---|---|
| Frequency of Coffee Consumption | Hearing Loss (Unilateral) | Hearing Loss (Bilateral) | Hearing Loss (Unilateral) | Hearing Loss (Bilateral) | ||||
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Age 19–39 | ||||||||
| Rarely | Reference | Reference | Reference | Reference | ||||
| Monthly | 0.38 (0.08, 1.70) | 0.2039 | 0.69 (0.03, 17.15) | 0.8231 | 0.42 (0.09, 1.99) | 0.2768 | 0.59 (0.06, 6.35) | 0.6656 |
| Weekly | 0.39 (0.14, 1.07) | 0.0664 | 1.70 (0.25, 11.55) | 0.5880 | 0.45 (0.16, 1.28) | 0.1338 | 1.53 (0.37, 6.32) | 0.5607 |
| Daily | 0.73 (0.37, 1.45) | 0.3688 | 0.67 (0.11, 4.29) | 0.6765 | 0.76 (0.36, 1.59) | 0.4595 | 0.74 (0.19, 2.94) | 0.6715 |
| Age 40–64 | ||||||||
| Rarely | Reference | Reference | Reference | Reference | ||||
| Monthly | 0.79 (0.43, 1.45) | 0.4442 | 1.25 (0.69, 2.28) | 0.4604 | 0.80 (0.42, 1.52) | 0.4891 | 1.19 (0.62, 2.26) | 0.6051 |
| Weekly | 0.85 (0.55, 1.31) | 0.4611 | 0.77 (0.47, 1.27) | 0.3023 | 0.86 (0.54, 1.36) | 0.5141 | 0.74 (0.43, 1.26) | 0.2624 |
| Daily | 0.78 (0.55, 1.10) | 0.1603 | 0.48 (0.32, 0.72) | 0.0004 | 0.85 (0.59, 1.23) | 0.3865 | 0.50 (0.33, 0.78) | 0.0021 |
| Age ≥ 65 | ||||||||
| Rarely | Reference | Reference | Reference | Reference | ||||
| Monthly | 0.87 (0.50, 1.53) | 0.6344 | 0.65 (0.39, 1.11) | 0.1155 | 0.89 (0.48, 1.66) | 0.7070 | 0.72 (0.40, 1.29) | 0.2720 |
| Weekly | 0.90 (0.62, 1.31) | 0.5841 | 0.87 (0.62, 1.21) | 0.3997 | 0.97 (0.64, 1.47) | 0.8765 | 0.90 (0.62, 1.31) | 0.5953 |
| Daily | 0.76 (0.56, 1.03) | 0.0778 | 0.88 (0.67, 1.14) | 0.3212 | 0.85 (0.60, 1.19) | 0.3360 | 0.84 (0.62, 1.14) | 0.2669 |
| Univariable Analysis | Multivariable Analysis * | |||||||
|---|---|---|---|---|---|---|---|---|
| Frequency of Coffee Consumption | Tinnitus | Tinnitus-Related Annoyance | Tinnitus | Tinnitus-Related Annoyance | ||||
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Age 19–39 | ||||||||
| Rarely | Reference | Reference | Reference | Reference | ||||
| Monthly | 0.99 (0.71, 1.39) | 0.9688 | 0.81 (0.42, 1.57) | 0.5382 | 1.09 (0.77, 1.54) | 0.6366 | 0.94 (0.48, 1.84) | 0.8541 |
| Weekly | 0.99 (0.77, 1.27) | 0.9129 | 0.56 (0.33, 0.95) | 0.0298 | 1.05 (0.81, 1.37) | 0.7013 | 0.58 (0.34, 1.01) | 0.0529 |
| Daily | 0.77 (0.62, 0.96) | 0.0186 | 0.72 (0.48, 1.07) | 0.1043 | 0.80 (0.63 ,1.00) | 0.0548 | 0.76 (0.50, 1.16) | 0.2035 |
| Age 40–64 | ||||||||
| Rarely | Reference | Reference | Reference | Reference | ||||
| Monthly | 0.89 (0.64, 1.24) | 0.4998 | 0.75 (0.43, 1.31) | 0.3159 | 0.92 (0.65, 1.29) | 0.6210 | 0.75 (0.42, 1.35) | 0.3376 |
| Weekly | 0.92 (0.72, 1.17) | 0.4892 | 0.96 (0.66, 1.41) | 0.8349 | 0.97 (0.75, 1.25) | 0.8249 | 1.07 (0.72, 1.60) | 0.7322 |
| Daily | 0.81 (0.67, 0.99) | 0.0357 | 0.76 (0.55, 1.03) | 0.0795 | 0.90 (0.73, 1.10) | 0.3066 | 0.92 (0.66, 1.29) | 0.6464 |
| Age ≥ 65 | ||||||||
| Rarely | Reference | Reference | Reference | Reference | ||||
| Monthly | 0.99 (0.64, 1.52) | 0.9463 | 0.84 (0.48, 1.48) | 0.5530 | 1.02 (0.63, 1.65) | 0.9417 | 0.94 (0.49, 1.78) | 0.8446 |
| Weekly | 0.72 (0.53, 0.98) | 0.0357 | 0.68 (0.46, 1.01) | 0.0582 | 0.71 (0.51, 1.00) | 0.0514 | 0.74 (0.48, 1.16) | 0.1881 |
| Daily | 0.82 (0.65, 1.05) | 0.1109 | 0.63 (0.46, 0.85) | 0.0026 | 0.95 (0.72, 1.24) | 0.6899 | 0.77 (0.54, 1.09) | 0.1355 |
| Coffee Type | Hearing Loss (Unilateral) | Hearing Loss (Bilateral) | ||
|---|---|---|---|---|
| OR * (95% CI) | p-Value | OR * (95% CI) | p-Value | |
| Age group: 19–39 | ||||
| Brewed coffee (yes vs. no) | 0.95 (0.53, 1.69) | 0.8599 | 0.46 (0.16, 1.27) | 0.1333 |
| Instant coffee (yes vs. no) | 0.65 (0.22, 1.91) | 0.4369 | 0.64 (0.08, 4.88) | 0.6683 |
| Canned coffee (yes vs. no) | 1.02 (0.39, 2.64) | 0.9752 | 1.28 (0.32, 5.08) | 0.7223 |
| Age group: 40–64 | ||||
| Brewed coffee (yes vs. no) | 1.04 (0.81, 1.34) | 0.7414 | 0.61 (0.44, 0.84) | 0.0028 |
| Instant coffee (yes vs. no) | 1.11 (0.81, 1.51) | 0.5216 | 0.70 (0.45, 1.09) | 0.1133 |
| Canned coffee (yes vs. no) | 1.41 (0.86, 2.30) | 0.1694 | 0.63 (0.23, 1.73) | 0.3672 |
| Age group: ≥65 | ||||
| Brewed coffee (yes vs. no) | 0.84 (0.64, 1.10) | 0.2083 | 1.02 (0.80, 1.30) | 0.8886 |
| Instant coffee (yes vs. no) | 0.87 (0.60, 1.26) | 0.4472 | 0.74 (0.53, 1.04) | 0.0842 |
| Canned coffee (yes vs. no) | 1.38 (0.51, 3.74) | 0.5233 | 0.89 (0.30, 2.64) | 0.8294 |
| Tinnitus | Tinnitus-Related Annoyance | |||
| OR † (95% CI) | p-Value | OR † (95% CI) | p-Value | |
| Age group: 19–39 | ||||
| Brewed coffee (yes vs. no) | 0.82 (0.70, 0.97) | 0.0175 | 1.09 (0.80, 1.50) | 0.5821 |
| Instant coffee (yes vs. no) | 1.08 (0.84, 1.41) | 0.5439 | 1.04 (0.62, 1.74) | 0.8812 |
| Canned coffee (yes vs. no) | 0.95 (0.74, 1.23) | 0.7163 | 1.13 (0.68, 1.86) | 0.6454 |
| Age group: 40–64 | ||||
| Brewed coffee (yes vs. no) | 1.00 (0.87, 1.14) | 0.9359 | 0.96 (0.77, 1.19) | 0.6790 |
| Instant coffee (yes vs. no) | 0.96 (0.81, 1.14) | 0.6779 | 0.96 (0.72, 1.27) | 0.7660 |
| Canned coffee (yes vs. no) | 1.49 (1.17, 1.90) | 0.0011 | 1.28 (0.83, 1.95) | 0.2619 |
| Age group: ≥65 | ||||
| Brewed coffee (yes vs. no) | 0.92 (0.74, 1.14) | 0.4318 | 0.89 (0.66, 1.20) | 0.4441 |
| Instant coffee (yes vs. no) | 1.19 (0.90, 1.57) | 0.2263 | 0.95 (0.64, 1.42) | 0.7967 |
| Canned coffee (yes vs. no) | 0.85 (0.37, 1.97) | 0.7051 | 0.63 (0.14, 2.74) | 0.5328 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.-Y.; Jung, G.; Jang, M.-j.; Suh, M.-W.; Lee, J.H.; Oh, S.H.; Park, M.K. Association of Coffee Consumption with Hearing and Tinnitus Based on a National Population-Based Survey. Nutrients 2018, 10, 1429. https://doi.org/10.3390/nu10101429
Lee S-Y, Jung G, Jang M-j, Suh M-W, Lee JH, Oh SH, Park MK. Association of Coffee Consumption with Hearing and Tinnitus Based on a National Population-Based Survey. Nutrients. 2018; 10(10):1429. https://doi.org/10.3390/nu10101429
Chicago/Turabian StyleLee, Sang-Youp, Gucheol Jung, Myoung-jin Jang, Myung-Whan Suh, Jun Ho Lee, Seung Ha Oh, and Moo Kyun Park. 2018. "Association of Coffee Consumption with Hearing and Tinnitus Based on a National Population-Based Survey" Nutrients 10, no. 10: 1429. https://doi.org/10.3390/nu10101429