Cardiovascular Health Benefits of Specific Vegetable Types: A Narrative Review

 , , , , ,
, , , , ,
Abstract
:1. Introduction
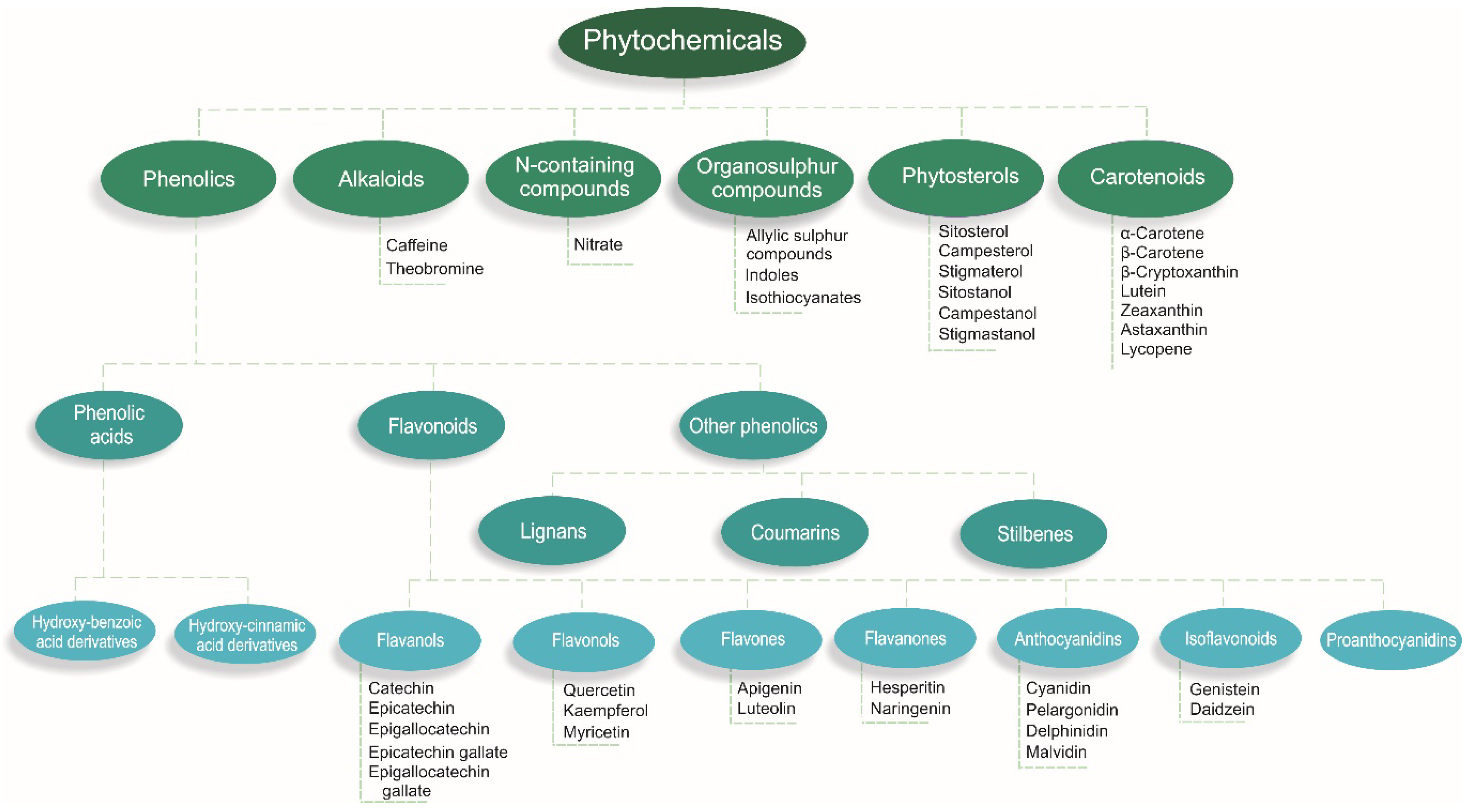
2. Nutrients and Phytochemicals in Vegetables
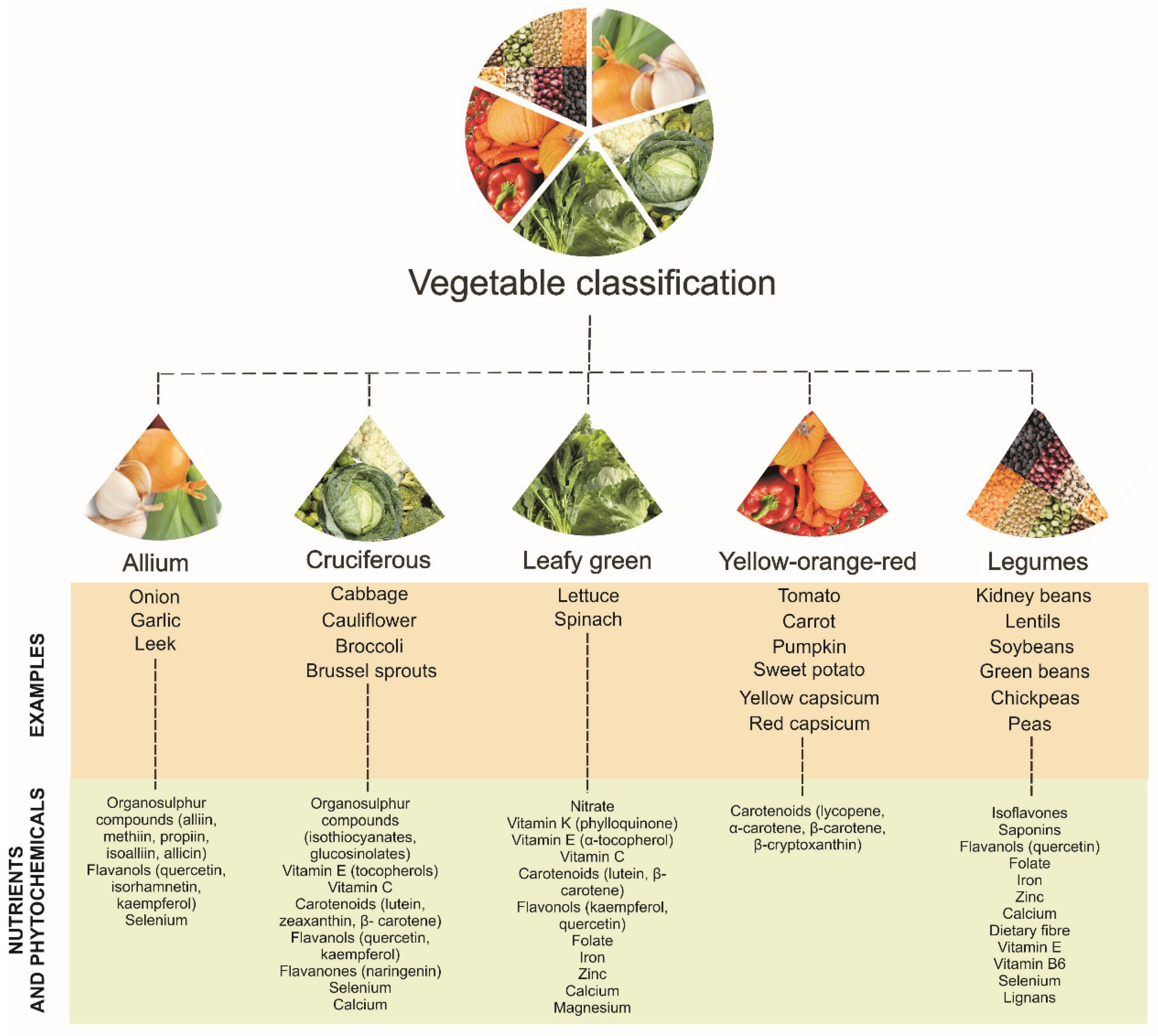
3. Classification of Vegetables
4. Subclinical Measures of Atherosclerosis
5. Cardiovascular Disease Clinical Endpoints
5.1. Leafy Green Vegetables
5.2. Cruciferous Vegetables
5.3. Allium Vegetables
5.4. Yellow-Orange-Red Vegetables
5.5. Legumes
6. Limitations and Future Directions
7. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Australian Institute of Health and Welfare. Australia’s Health 2014. Available online: http://www.aihw.gov.au/WorkArea/DownloadAsset.aspx?id=60129548150 (accessed on 25 January 2018).
- World Health Organization. Global Status Report on Noncommunicable Diseases 2014; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Celermajer, D.S.; Chow, C.K.; Marijon, E.; Anstey, N.M.; Woo, K.S. Cardiovascular disease in the developing world: Prevalences, patterns, and the potential of early disease detection. J. Am. Coll. Cardiol. 2012, 60, 1207–1216. [Google Scholar] [CrossRef] [PubMed]
- Medis, S.; Puska, P.; Norrving, B. Global Atlas on Cardiovascular Disease Prevention and Control; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- World Health Organization. Fruit and Vegetables for Health: Report of a Joint fao/Who Workshop; World Health Organization: Geneva, Switzerland, 2004. [Google Scholar]
- National Health and Medical Research Council. Australian Dietary Guidelines; National Health and Medical Research Council: Canberra, Australia, 2013.
- U.S. Department of Health and Human Services; U.S. Department of Agriculture. 2015–2020 Dietary Guidelines for Americans; U.S. Department of Health and Human Services/U.S. Department of Agriculture: Washington, DC, USA, 2015.
- Carter, O.B.; Pollard, C.M.; Atkins, J.F.; Marie Milliner, J.; Pratt, I.S. ‘We’re not told why-we’re just told’: Qualitative reflections about the western australian go for 2&5(r) fruit and vegetable campaign. Public Health Nutr. 2011, 14, 982–988. [Google Scholar] [PubMed]
- National Cancer Institute. Usual Dietary Intakes: Food Intakes, Us Population, 2007-10. Available online: http://appliedresearch.Cancer.Gov/diet/usualintakes/pop/2007-10 (accessed on 31 August 2017).
- Hall, J.N.; Moore, S.; Harper, S.B.; Lynch, J.W. Global variability in fruit and vegetable consumption. Am. J. Prev. Med. 2009, 36, 402–409. [Google Scholar] [CrossRef] [PubMed]
- Australian Bureau of Statistics. National Health Survey: First Results, 2014-15; Commenwealth of Australia: Canberra, Australia, 2015.
- Aune, D.; Giovannucci, E.; Boffetta, P.; Fadnes, L.T.; Keum, N.; Norat, T.; Greenwood, D.C.; Riboli, E.; Vatten, L.J.; Tonstad, S. Fruit and vegetable intake and the risk of cardiovascular disease, total cancer and all-cause mortality: A systematic review and dose-response meta-analysis of prospective studies. Int. J. Epidemiol. 2017, 46, 1029–1056. [Google Scholar] [CrossRef] [PubMed]
- Threapleton, D.E.; Greenwood, D.C.; Evans, C.E.L.; Cleghorn, C.L.; Nykjaer, C.; Woodhead, C.; Cade, J.E.; Gale, C.P.; Burley, V.J. Dietary fibre intake and risk of cardiovascular disease: Systematic review and meta-analysis. Br. Med. J. 2013, 347, f6879. [Google Scholar] [CrossRef] [PubMed]
- Aburto, N.J.; Hanson, S.; Gutierrez, H.; Hooper, L.; Elliott, P.; Cappuccio, F.P. Effect of increased potassium intake on cardiovascular risk factors and disease: Systematic review and meta-analyses. Br. Med. J. 2013, 346, f1378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Del Gobbo, L.C.; Imamura, F.; Wu, J.H.Y.; de Oliveira Otto, M.C.; Chiuve, S.E.; Mozaffarian, D. Circulating and dietary magnesium and risk of cardiovascular disease: A systematic review and meta-analysis of prospective studies. Am. J. Clin. Nutr. 2013, 98, 160–173. [Google Scholar] [CrossRef] [PubMed]
- Borgi, L.; Muraki, I.; Satija, A.; Willett, W.C.; Rimm, E.B.; Forman, J.P. Fruit and vegetable consumption and the incidence of hypertension in three prospective cohort studies. Hypertension 2016, 67, 288–293. [Google Scholar] [CrossRef] [PubMed]
- Borgi, L.; Rimm, E.B.; Willett, W.C.; Forman, J.P. Potato intake and incidence of hypertension: Results from three prospective us cohort studies. BMJ 2016, 353, i2351. [Google Scholar] [CrossRef] [PubMed]
- Liu, R.H. Health-promoting components of fruits and vegetables in the diet. Adv. Nutr. 2013, 4, 384S–392S. [Google Scholar] [CrossRef] [PubMed]
- Van Breda, S.G.J.; de Kok, T.M.C.M. Smart combinations of bioactive compounds in fruits and vegetables may guide new strategies for personalized prevention of chronic diseases. Mol. Nutr. Food Res. 2018, 62, 1700597. [Google Scholar] [CrossRef] [PubMed]
- Scalbert, A.; Andres-Lacueva, C.; Arita, M.; Kroon, P.; Manach, C.; Urpi-Sarda, M.; Wishart, D. Databases on food phytochemicals and their health-promoting effects. J. Agric. Food Chem. 2011, 59, 4331–4348. [Google Scholar] [CrossRef] [PubMed]
- Liu, R.H. Health benefits of fruit and vegetables are from additive and synergistic combinations of phytochemicals. Am. J. Clin. Nutr. 2003, 78, 517S–520S. [Google Scholar] [CrossRef] [PubMed]
- Liu, R.H. Potential synergy of phytochemicals in cancer prevention: Mechanism of action. J. Nutr. 2004, 134, 3479s–3485s. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Je, Y. Flavonoid intake and mortality from cardiovascular disease and all causes: A meta-analysis of prospective cohort studies. Clin. Nutr. ESPEN 2017, 20, 68–77. [Google Scholar] [CrossRef] [PubMed]
- Cheng, H.M.; Koutsidis, G.; Lodge, J.K.; Ashor, A.; Siervo, M.; Lara, J. Tomato and lycopene supplementation and cardiovascular risk factors: A systematic review and meta-analysis. Atherosclerosis 2017, 257, 100–108. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Song, Y.; Zhang, L. Effect of lycopene supplementation on oxidative stress: An exploratory systematic review and meta-analysis of randomized controlled trials. J. Med. Food 2013, 16, 361–374. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Xu, J. Dietary and circulating lycopene and stroke risk: A meta-analysis of prospective studies. Sci. Rep. 2014, 4, 5031. [Google Scholar] [CrossRef] [PubMed]
- Leermakers, E.T.M.; Darweesh, S.K.L.; Baena, C.P.; Moreira, E.M.; Melo van Lent, D.; Tielemans, M.J.; Muka, T.; Vitezova, A.; Chowdhury, R.; Bramer, W.M.; et al. The effects of lutein on cardiometabolic health across the life course: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2016, 103, 481–494. [Google Scholar] [CrossRef] [PubMed]
- Shea, M.K.; Booth, S.L.; Weiner, D.E.; Brinkley, T.E.; Kanaya, A.M.; Murphy, R.A.; Simonsick, E.M.; Wassel, C.L.; Vermeer, C.; Kritchevsky, S.B. Circulating vitamin k is inversely associated with incident cardiovascular disease risk among those treated for hypertension in the health, aging, and body composition study (health abc). J. Nutr. 2017, 147, 888–895. [Google Scholar] [CrossRef] [PubMed]
- Moser, M.; Chun, O. Vitamin c and heart health: A review based on findings from epidemiologic studies. Int. J. Mol. Sci. 2016, 17, 1328. [Google Scholar] [CrossRef] [PubMed]
- Blekkenhorst, L.C.; Bondonno, C.P.; Lewis, J.R.; Devine, A.; Woodman, R.J.; Croft, K.D.; Lim, W.H.; Wong, G.; Beilin, L.J.; Prince, R.L.; et al. Association of dietary nitrate with atherosclerotic vascular disease mortality: A prospective cohort study of older adult women. Am. J. Clin. Nutr. 2017, 106, 207–216. [Google Scholar] [CrossRef] [PubMed]
- Bondonno, C.P.; Blekkenhorst, L.C.; Prince, R.L.; Ivey, K.L.; Lewis, J.R.; Devine, A.; Woodman, R.J.; Lundberg, J.O.; Croft, K.D.; Thompson, P.L.; et al. Association of vegetable nitrate intake with carotid atherosclerosis and ischemic cerebrovascular disease in older women. Stroke 2017, 48, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Vazquez-Prieto, M.A.; Miatello, R.M. Organosulfur compounds and cardiovascular disease. Mol. Aspects Med. 2010, 31, 540–545. [Google Scholar] [CrossRef] [PubMed]
- Tang, G.; Meng, X.; Li, Y.; Zhao, C.; Liu, Q.; Li, H. Effects of vegetables on cardiovascular diseases and related mechanisms. Nutrients 2017, 9, 857. [Google Scholar] [CrossRef] [PubMed]
- Maiani, G.; Periago Castón, M.J.; Catasta, G.; Toti, E.; Cambrodón, I.G.; Bysted, A.; Granado-Lorencio, F.; Olmedilla-Alonso, B.; Knuthsen, P.; Valoti, M.; et al. Carotenoids: Actual knowledge on food sources, intakes, stability and bioavailability and their protective role in humans. Mol. Nutr. Food Res. 2009, 53, 194S–218S. [Google Scholar] [CrossRef] [PubMed]
- Kaulmann, A.; Bohn, T. Carotenoids, inflammation, and oxidative stress—Implications of cellular signaling pathways and relation to chronic disease prevention. Nutr. Res. 2014, 34, 907–929. [Google Scholar] [CrossRef] [PubMed]
- Blekkenhorst, L.C.; Prince, R.L.; Ward, N.C.; Croft, K.D.; Lewis, J.R.; Devine, A.; Shinde, S.; Woodman, R.J.; Hodgson, J.M.; Bondonno, C.P.C. Development of a reference database for assessing dietary nitrate in vegetables. Mol. Nutr. Food Res. 2017, 61. [Google Scholar] [CrossRef] [PubMed]
- Napoli, C.; Ignarro, L.J. Nitric oxide and pathogenic mechanisms involved in the development of vascular diseases. Arch. Pharm. Res. 2009, 32, 1103–1108. [Google Scholar] [CrossRef] [PubMed]
- Förstermann, U.; Münzel, T. Endothelial nitric oxide synthase in vascular disease. Circulation 2006, 113, 1708–1714. [Google Scholar] [CrossRef] [PubMed]
- Sturm, C.; Wagner, A.E. Brassica-derived plant bioactives as modulators of chemopreventive and inflammatory signaling pathways. Int. J. Mol. Sci. 2017, 18, 1890. [Google Scholar] [CrossRef] [PubMed]
- Beretta, H.V.; Bannoud, F.; Insani, M.; Berli, F.; Hirschegger, P.; Galmarini, C.R.; Cavagnaro, P.F. Relationships between bioactive compound content and the antiplatelet and antioxidant activities of six allium vegetable species. Food Technol. Biotechnol. 2017, 55, 266–275. [Google Scholar] [CrossRef] [PubMed]
- Pennington, J.A.T.; Fisher, R.A. Classification of fruits and vegetables. J. Food Compost. Anal. 2009, 22, 23S–31S. [Google Scholar] [CrossRef]
- Birt, D.F.; Boylston, T.; Hendrich, S.; Jane, J.-L.; Hollis, J.; Li, L.; McClelland, J.; Moore, S.; Phillips, G.J.; Rowling, M.; et al. Resistant starch: Promise for improving human health. Adv. Nutr. 2013, 4, 587–601. [Google Scholar] [CrossRef] [PubMed]
- Battson, M.L.; Lee, D.M.; Weir, T.L.; Gentile, C.L. The gut microbiota as a novel regulator of cardiovascular function and disease. J. Nutr. Biochem. 2017, 56, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Weitzberg, E.; Lundberg, J.O. Novel aspects of dietary nitrate and human health. Annu. Rev. Nutr. 2013, 33, 129–159. [Google Scholar] [CrossRef] [PubMed]
- Bondonno, C.P.; Croft, K.D.; Hodgson, J.M. Dietary nitrate, nitric oxide, and cardiovascular health. Crit. Rev. Food Sci. Nutr. 2016, 56, 2036–2052. [Google Scholar] [CrossRef] [PubMed]
- Dinkova-Kostova, A.T.; Kostov, R.V. Glucosinolates and isothiocyanates in health and disease. Trends Mol. Med. 2012, 18, 337–347. [Google Scholar] [CrossRef] [PubMed]
- Raiola, A.; Errico, A.; Petruk, G.; Monti, D.M.; Barone, A.; Rigano, M.M. Bioactive compounds in brassicaceae vegetables with a role in the prevention of chronic diseases. Molecules 2017, 23, 15. [Google Scholar] [CrossRef] [PubMed]
- Voutilainen, S.; Nurmi, T.; Mursu, J.; Rissanen, T.H. Carotenoids and cardiovascular health. Am. J. Clin. Nutr. 2006, 83, 1265–1271. [Google Scholar] [CrossRef] [PubMed]
- Messina, M.J. Legumes and soybeans: Overview of their nutritional profiles and health effects. Am. J. Clin. Nutr. 1999, 70, 439s–450s. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Casado, A. The health potential of fruits and vegetables phytochemicals: Notable examples. Crit. Rev. Food Sci. Nutr. 2016, 56, 1097–1107. [Google Scholar] [CrossRef] [PubMed]
- Bondonno, N.P.; Bondonno, C.P.; Hodgson, J.M.; Ward, N.C.; Croft, K.D. The efficacy of quercetin in cardiovascular health. Curr. Nutr. Rep. 2015, 4, 290–303. [Google Scholar] [CrossRef]
- Bhagwat, S.; Haytowitz, D.B.; Holden, J.M. Usda Database for the Flavonoid Content of Selected Foods Release 3.1; U.S. Department of Agriculture: Beltsville, MD, USA, 2014.
- Bhagwat, S.; Haytowitz, D.B.; Holden, J.M. Usda Database for the Isoflavone Content of Selected Foods Release 2.0; U.S. Department of Agriculture: Beltsville, MD, USA, 2008.
- Morris, M.C.; Wang, Y.; Barnes, L.L.; Bennett, D.A.; Dawson-Hughes, B.; Booth, S.L. Nutrients and bioactives in green leafy vegetables and cognitive decline: Prospective study. Neurology 2018, 90, e214–e222. [Google Scholar] [CrossRef] [PubMed]
- Papandreou, C.; Becerra-Tomás, N.; Bulló, M.; Martínez-González, M.Á.; Corella, D.; Estruch, R.; Ros, E.; Arós, F.; Schroder, H.; Fitó, M.; et al. Legume consumption and risk of all-cause, cardiovascular, and cancer mortality in the predimed study. Clin. Nutr. 2018. [Google Scholar] [CrossRef] [PubMed]
- Hansson, G.K. Inflammation, atherosclerosis, and coronary artery disease. N. Engl. J. Med. 2005, 352, 1685–1695. [Google Scholar] [CrossRef] [PubMed]
- Manduteanu, I.; Simionescu, M. Inflammation in atherosclerosis: A cause or a result of vascular disorders? J. Cell. Mol. Med. 2012, 16, 1978–1990. [Google Scholar] [CrossRef] [PubMed]
- Ebrahim, S.; Papacosta, O.; Whincup, P.; Wannamethee, G.; Walker, M.; Nicolaides, A.N.; Dhanjil, S.; Griffin, M.; Belcaro, G.; Rumley, A.; et al. Carotid plaque, intima media thickness, cardiovascular risk factors, and prevalent cardiovascular disease in men and women. Stroke 1999, 30, 841–850. [Google Scholar] [CrossRef] [PubMed]
- Lorenz, M.W.; Markus, H.S.; Bots, M.L.; Rosvall, M.; Sitzer, M. Prediction of clinical cardiovascular events with carotid intima-media thickness: A systematic review and meta-analysis. Circulation 2007, 115, 459–467. [Google Scholar] [CrossRef] [PubMed]
- Touboul, P.J.; Hennerici, M.G.; Meairs, S.; Adams, H.; Amarenco, P.; Bornstein, N.; Csiba, L.; Desvarieux, M.; Ebrahim, S.; Hernandez Hernandez, R.; et al. Mannheim carotid intima-media thickness and plaque consensus (2004–2006–2011). Cerebrovasc. Dis. 2012, 34, 290–296. [Google Scholar] [CrossRef] [PubMed]
- Johnsen, S.H.; Mathiesen, E.B. Carotid plaque compared with intima-media thickness as a predictor of coronary and cerebrovascular disease. Curr. Cardiol. Rep. 2009, 11, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Plichart, M.; Celermajer, D.S.; Zureik, M.; Helmer, C.; Jouven, X.; Ritchie, K.; Tzourio, C.; Ducimetière, P.; Empana, J.-P. Carotid intima-media thickness in plaque-free site, carotid plaques and coronary heart disease risk prediction in older adults. Atherosclerosis 2011, 219, 917–924. [Google Scholar] [CrossRef] [PubMed]
- Murie-Fernandez, M.; Irimia, P.; Toledo, E.; Martínez-Vila, E.; Buil-Cosiales, P.; Serrano-Martínez, M.; Ruiz-Gutiérrez, V.; Ros, E.; Estruch, R.; Martínez-González, M.Á. Carotid intima-media thickness changes with mediterranean diet: A randomized trial (predimed-navarra). Atherosclerosis 2011, 219, 158–162. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.-Y.; Li, X.-J.; Zhang, W.; Liu, C.-Q.; Zhang, H.-J.; Lin, J.-R.; Yan, B.; Yu, Y.-X.; Shi, X.-L.; Li, C.-D.; et al. Chinese lacto-vegetarian diet exerts favorable effects on metabolic parameters, intima-media thickness, and cardiovascular risks in healthy men. Nutr. Clin. Pract. 2012, 27, 392–398. [Google Scholar] [CrossRef] [PubMed]
- Sala-Vila, A.; Romero-Mamani, E.-S.; Gilabert, R.; Núñez, I.; de la Torre, R.; Corella, D.; Ruiz-Gutiérrez, V.; López-Sabater, M.-C.; Pintó, X.; Rekondo, J.; et al. Changes in ultrasound-assessed carotid intima-media thickness and plaque with a mediterranean diet: A substudy of the predimed trial. Arterioscler. Thromb. Vasc. Biol. 2014, 34, 439–445. [Google Scholar] [CrossRef] [PubMed]
- Petersen, K.S.; Clifton, P.M.; Keogh, J.B. The association between carotid intima media thickness and individual dietary components and patterns. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 495–502. [Google Scholar] [CrossRef] [PubMed]
- Blekkenhorst, L.C.; Bondonno, C.P.; Lewis, J.R.; Woodman, R.J.; Devine, A.; Bondonno, N.P.; Lim, W.H.; Zhu, K.; Beilin, L.J.; Thompson, P.L.; et al. Cruciferous and total vegetable intakes are inversely associated with subclinical atherosclerosis in older adult women. J. Am. Heart. Assoc. 2018, 7, e008391. [Google Scholar] [CrossRef] [PubMed]
- Hung, H.-C.; Joshipura, K.J.; Jiang, R.; Hu, F.B.; Hunter, D.; Smith-Warner, S.A.; Colditz, G.A.; Rosner, B.; Spiegelman, D.; Willett, W.C. Fruit and vegetable intake and risk of major chronic disease. J. Natl. Cancer Inst. 2004, 96, 1577–1584. [Google Scholar] [CrossRef] [PubMed]
- Takachi, R.; Inoue, M.; Ishihara, J.; Kurahashi, N.; Iwasaki, M.; Sasazuki, S.; Iso, H.; Tsubono, Y.; Tsugane, S. Fruit and vegetable intake and risk of total cancer and cardiovascular disease: Japan public health center-based prospective study. Am. J. Epidemiol. 2007, 167, 59–70. [Google Scholar] [CrossRef] [PubMed]
- Buil-Cosiales, P.; Toledo, E.; Salas-Salvadó, J.; Zazpe, I.; Farràs, M.; Basterra-Gortari, F.J.; Diez-Espino, J.; Estruch, R.; Corella, D.; Ros, E.; et al. Association between dietary fibre intake and fruit, vegetable or whole-grain consumption and the risk of cvd: Results from the prevención con dieta mediterránea (predimed) trial. Br. J. Nutr. 2016, 116, 534–546. [Google Scholar] [CrossRef] [PubMed]
- Gaziano, J.M.; Manson, J.E.; Branch, L.G.; Colditz, G.A.; Willett, W.C.; Buring, J.E. A prospective study of consumption of carotenoids in fruits and vegetables and decreased cardiovascular mortality in the elderly. Ann. Epidemiol. 1995, 5, 255–260. [Google Scholar] [CrossRef]
- Blekkenhorst, L.C.; Bondonno, C.P.; Lewis, J.R.; Devine, A.; Zhu, K.; Lim, W.H.; Woodman, R.J.; Beilin, L.J.; Prince, R.L.; Hodgson, J.M. Cruciferous and allium vegetable intakes are inversely associated with 15-year atherosclerotic vascular disease deaths in older adult women. J. Am. Heart. Assoc. 2017, 6, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Bhupathiraju, S.N.; Wedick, N.M.; Pan, A.; Manson, J.E.; Rexrode, K.M.; Willett, W.C.; Rimm, E.B.; Hu, F.B. Quantity and variety in fruit and vegetable intake and risk of coronary heart disease. Am. J. Clin. Nutr. 2013, 98, 1514–1523. [Google Scholar] [CrossRef] [PubMed]
- Bendinelli, B.; Masala, G.; Saieva, C.; Salvini, S.; Calonico, C.; Sacerdote, C.; Agnoli, C.; Grioni, S.; Frasca, G.; Mattiello, A.; et al. Fruit, vegetables, and olive oil and risk of coronary heart disease in italian women: The epicor study. Am. J. Clin. Nutr. 2011, 93, 275–283. [Google Scholar] [CrossRef] [PubMed]
- Oude Griep, L.M.; Verschuren, W.M.; Kromhout, D.; Ocke, M.C.; Geleijnse, J.M. Colours of fruit and vegetables and 10-year incidence of chd. Br. J. Nutr. 2011, 106, 1562–1569. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.-B.; Fan, J.-H.; Dawsey, S.M.; Sinha, R.; Freedman, N.D.; Taylor, P.R.; Qiao, Y.-L.; Abnet, C.C. Dietary components and risk of total, cancer and cardiovascular disease mortality in the linxian nutrition intervention trials cohort in china. Sci. Rep. 2016, 6, 22619. [Google Scholar] [CrossRef] [PubMed]
- Larsson, S.C.; Virtamo, J.; Wolk, A. Total and specific fruit and vegetable consumption and risk of stroke: A prospective study. Atherosclerosis 2013, 227, 147–152. [Google Scholar] [CrossRef] [PubMed]
- Joshipura, K.J.; Ascherio, A.; Manson, J.E.; Stampfer, M.J.; Rimm, E.B.; Speizer, F.E.; Hennekens, C.H.; Spiegelman, D.; Willett, W.C. Fruit and vegetable intake in relation to risk of ischemic stroke. J. Am. Med. Assoc. 1999, 282, 1233–1239. [Google Scholar] [CrossRef]
- Johnsen, S.P.; Overvad, K.; Stripp, C.; Tjonneland, A.; Husted, S.E.; Sorensen, H.T. Intake of fruit and vegetables and the risk of ischemic stroke in a cohort of danish men and women. Am. J. Clin. Nutr. 2003, 78, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Shu, X.-O.; Xiang, Y.-B.; Yang, G.; Li, H.; Gao, J.; Cai, H.; Gao, Y.-T.; Zheng, W. Cruciferous vegetable consumption is associated with a reduced risk of total and cardiovascular disease mortality. Am. J. Clin. Nutr. 2011, 91, 240–246. [Google Scholar] [CrossRef] [PubMed]
- Mink, P.J.; Scrafford, C.G.; Barraj, L.M.; Harnack, L.; Hong, C.P.; Nettleton, J.A.; Jacobs, D.R., Jr. Flavonoid intake and cardiovascular disease mortality: A prospective study in postmenopausal women. Am. J. Clin. Nutr. 2007, 85, 895–909. [Google Scholar] [CrossRef] [PubMed]
- Genkinger, J.M.; Platz, E.A.; Hoffman, S.C.; Comstock, G.W.; Helzlsouer, K.J. Fruit, vegetable, and antioxidant intake and all-cause, cancer, and cardiovascular disease mortality in a community-dwelling population in washington county, maryland. Am. J. Epidemiol. 2004, 160, 1223–1233. [Google Scholar] [CrossRef] [PubMed]
- Yu, D.; Zhang, X.; Gao, Y.-T.; Li, H.; Yang, G.; Huang, J.; Zheng, W.; Xiang, Y.-B.; Shu, X.-O. Fruit and vegetable intake and risk of chd: Results from prospective cohort studies of chinese adults in shanghai. Br. J. Nutr. 2013, 111, 353–362. [Google Scholar] [CrossRef] [PubMed]
- Mizrahi, A.; Knekt, P.; Montonen, J.; Laaksonen, M.A.; Heliovaara, M.; Jarvinen, R. Plant foods and the risk of cerebrovascular diseases: A potential protection of fruit consumption. Br. J. Nutr. 2009, 102, 1075–1083. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.; Rexrode, K.M.; Hu, F.; Albert, C.M.; Chae, C.U.; Rimm, E.B.; Stampfer, M.J.; Manson, J.E. Dietary intakes of flavonols and flavones and coronary heart disease in us women. Am. J. Epidemiol. 2007, 165, 1305–1313. [Google Scholar] [CrossRef] [PubMed]
- Knekt, P.; Jarvinen, R.; Reunanen, A.; Maatela, J. Flavonoid intake and coronary mortality in finland: A cohort study. Br. Med. J. 1996, 312, 478–481. [Google Scholar] [CrossRef]
- Hertog, M.G.; Sweetnam, P.M.; Fehily, A.M.; Elwood, P.C.; Kromhout, D. Antioxidant flavonols and ischemic heart disease in a welsh population of men: The caerphilly study. Am. J. Clin. Nutr. 1997, 65, 1489–1494. [Google Scholar] [CrossRef] [PubMed]
- Knekt, P.; Isotupa, S.; Rissanen, H.; Heliovaara, M.; Jarvinen, R.; Hakkinen, S.; Aromaa, A.; Reunanen, A. Quercetin intake and the incidence of cerebrovascular disease. Eur. J. Clin. Nutr. 2000, 54, 415–417. [Google Scholar] [CrossRef] [PubMed]
- Jacques, P.F.; Lyass, A.; Massaro, J.M.; Vasan, R.S.; D’Agostino, R.B., Sr. Relationship of lycopene intake and consumption of tomato products to incident cvd. Br. J. Nutr. 2013, 110, 545–551. [Google Scholar] [CrossRef] [PubMed]
- Buijsse, B.; Feskens, E.J.M.; Kwape, L.; Kok, F.J.; Kromhout, D. Both α- and β-carotene, but not tocopherols and vitamin c, are inversely related to 15-year cardiovascular mortality in dutch elderly men. J. Nutr. 2008, 138, 344–350. [Google Scholar] [CrossRef] [PubMed]
- Nagura, J.; Iso, H.; Watanabe, Y.; Maruyama, K.; Date, C.; Toyoshima, H.; Yamamoto, A.; Kikuchi, S.; Koizumi, A.; Kondo, T.; et al. Fruit, vegetable and bean intake and mortality from cardiovascular disease among japanese men and women: The jacc study. Br. J. Nutr. 2009, 102, 285–292. [Google Scholar] [CrossRef] [PubMed]
- Martínez-González, M.A.; García-López, M.; Bes-Rastrollo, M.; Toledo, E.; Martínez-Lapiscina, E.H.; Delgado-Rodriguez, M.; Vazquez, Z.; Benito, S.; Beunza, J.J. Mediterranean diet and the incidence of cardiovascular disease: A spanish cohort. Nutr. Metab. Cardiovasc. Dis. 2011, 21, 237–244. [Google Scholar] [CrossRef] [PubMed]
- Bazzano, L.A.; He, J.; Ogden, L.G.; Loria, C.; Vupputuri, S.; Myers, L.; Whelton, P.K. Legume consumption and risk of coronary heart disease in us men and women: Nhanes i epidemiologic follow-up study. Arch. Intern. Med. 2001, 161, 2573–2578. [Google Scholar] [CrossRef] [PubMed]
- Nouri, F.; Sarrafzadegan, N.; Mohammadifard, N.; Sadeghi, M.; Mansourian, M. Intake of legumes and the risk of cardiovascular disease: Frailty modeling of a prospective cohort study in the iranian middle-aged and older population. Eur. J. Clin. Nutr. 2016, 70, 217. [Google Scholar] [CrossRef] [PubMed]
- Kokubo, Y.; Iso, H.; Ishihara, J.; Okada, K.; Inoue, M.; Tsugane, S. Association of dietary intake of soy, beans, and isoflavones with risk of cerebral and myocardial infarctions in japanese populations: The japan public health center–based (jphc) study cohort i. Circulation 2007, 116, 2553–2562. [Google Scholar] [CrossRef] [PubMed]
- Kelemen, L.E.; Kushi, L.H.; Jacobs, J.D.R.; Cerhan, J.R. Associations of dietary protein with disease and mortality in a prospective study of postmenopausal women. Am. J. Epidemiol. 2005, 161, 239–249. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, A.M.; Sun, Q.; Hu, F.B.; Stampfer, M.J.; Manson, J.E.; Willett, W.C. Major dietary protein sources and risk of coronary heart disease in women. Circulation 2010, 122, 876–883. [Google Scholar] [CrossRef] [PubMed]
- Buckland, G.; González, C.A.; Agudo, A.; Vilardell, M.; Berenguer, A.; Amiano, P.; Ardanaz, E.; Arriola, L.; Barricarte, A.; Basterretxea, M.; et al. Adherence to the mediterranean diet and risk of coronary heart disease in the spanish epic cohort study. Am. J. Epidemiol. 2009, 170, 1518–1529. [Google Scholar] [CrossRef] [PubMed]
- Dilis, V.; Katsoulis, M.; Lagiou, P.; Trichopoulos, D.; Naska, A.; Trichopoulou, A. Mediterranean diet and chd: The greek european prospective investigation into cancer and nutrition cohort. Br. J. Nutr. 2012, 108, 699–709. [Google Scholar] [CrossRef] [PubMed]
- Haring, B.; Gronroos, N.; Nettleton, J.A.; Von Ballmoos, M.C.W.; Selvin, E.; Alonso, A. Dietary protein intake and coronary heart disease in a large community based cohort: Results from the atherosclerosis risk in communities (aric) study. PLoS ONE 2014, 9, e109552. [Google Scholar] [CrossRef] [PubMed]
- Misirli, G.; Benetou, V.; Lagiou, P.; Bamia, C.; Trichopoulos, D.; Trichopoulou, A. Relation of the traditional mediterranean diet to cerebrovascular disease in a mediterranean population. Am. J. Epidemiol. 2012, 176, 1185–1192. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, A.M.; Pan, A.; Rexrode, K.M.; Stampfer, M.; Hu, F.B.; Mozaffarian, D.; Willett, W.C. Dietary protein sources and the risk of stroke in men and women. Stroke 2012, 43, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Haring, B.; Misialek, J.R.; Rebholz, C.M.; Petruski-Ivleva, N.; Gottesman, R.F.; Mosley, T.H.; Alonso, A. Association of dietary protein consumption with incident silent cerebral infarcts and stroke: The atherosclerosis risk in communities (aric) study. Stroke 2015, 46, 3443–3450. [Google Scholar] [CrossRef] [PubMed]
- Langseth, L. Nutritional Epidemiology: Possibilities and Limitations; International Life Sciences Institute Europe: Brussels, Belgium, 1996. [Google Scholar]
- Rollo, M.E.; Williams, R.L.; Burrows, T.; Kirkpatrick, S.I.; Bucher, T.; Collins, C.E. What are they really eating? A review on new approaches to dietary intake assessment and validation. Curr. Nutr. Rep. 2016, 5, 307–314. [Google Scholar] [CrossRef]
- Lachat, C.; Hawwash, D.; Ocké, M.C.; Berg, C.; Forsum, E.; Hörnell, A.; Larsson, C.L.; Sonestedt, E.; Wirfält, E.; Åkesson, A.; et al. Strengthening the reporting of observational studies in epidemiology—Nutritional epidemiology (strobe-nut): An extension of the strobe statement. Nutr. Bull. 2016, 41, 240–251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, T.; Yang, B.; Zheng, J.; Li, G.; Wahlqvist, M.L.; Li, D. Cardiovascular disease mortality and cancer incidence in vegetarians: A meta-analysis and systematic review. Ann. Nutr. Metab. 2012, 60, 233–240. [Google Scholar] [CrossRef] [PubMed]
- Crowe, F.L.; Appleby, P.N.; Travis, R.C.; Key, T.J. Risk of hospitalization or death from ischemic heart disease among british vegetarians and nonvegetarians: Results from the epic-oxford cohort study. Am. J. Clin. Nutr. 2013, 97, 597–603. [Google Scholar] [CrossRef] [PubMed]
- Bazzano, L.A.; Serdula, M.K.; Liu, S. Dietary intake of fruits and vegetables and risk of cardiovascular disease. Curr. Atheroscler. Rep. 2003, 5, 492–499. [Google Scholar] [CrossRef] [PubMed]
- Eckel, R.H.; Jakicic, J.M.; Ard, J.D.; de Jesus, J.M.; Houston Miller, N.; Hubbard, V.S.; Lee, I.-M.; Lichtenstein, A.H.; Loria, C.M.; Millen, B.E.; et al. 2013 aha/acc guideline on lifestyle management to reduce cardiovascular risk: A report of the american college of cardiology/american heart association task force on practice guidelines. J. Am. Coll. Cardiol. 2014, 63, 2960–2984. [Google Scholar] [CrossRef] [PubMed]
- Wood, A.M.; Kaptoge, S.; Butterworth, A.S.; Willeit, P.; Warnakula, S.; Bolton, T.; Paige, E.; Paul, D.S.; Sweeting, M.; Burgess, S.; et al. Risk thresholds for alcohol consumption: Combined analysis of individual-participant data for 599 912 current drinkers in 83 prospective studies. Lancet 2018, 391, 1513–1523. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Study Cohort (Country) | Sample Number | Sex | Age (years) | Dietary Assessment Method | Outcome | Follow-up (years) | Results | First Author, Year (ref) |
|---|---|---|---|---|---|---|---|---|
| NHS and HPFS (USA) | 109,635 | M and F | 30–75 | FFQ | CVD (fatal or nonfatal MI or stroke) | 12–15 | 11% ↓ RR (per serving/day) | Hung, 2004 [68] |
| JPHCPS (Japan) | 77,891 | M and F | 45–74 | FFQ | CVD (fatal or nonfatal MI or stroke) | 5–8 | No association | Takachi, 2007 [69] |
| PREDIMED (Spain) | 7216 | M and F | 55–80 | FFQ | CVD (cardiovascular death, MI or stroke) | 7 | No association | Buil-Cosiales, 2016 [70] |
| MHCPS (USA) | 1273 | M and F | ≥66 | FFQ | CVD (death) | 4.75 | 51% ↓ RR (≥1 vs. <1 serving/day) | Gaziano, 1995 [71] |
| PLSAW (Australia) | 1226 | F | ≥70 | FFQ | ASVD (fatal ischemic heart disease, heart failure, cerebrovascular disease excluding hemorrhage, or peripheral heart disease) | 15 | No association | Blekkenhorst, 2017 [72] |
| NHS (USA) | 71,141 | F | 50 ± 7 | FFQ | CHD (fatal CHD or nonfatal MI) | 24 | 22% ↓ RR (high vs. low intake) | Bhupathiraju, 2013 [73] |
| HPFS (USA) | 42,135 | M | 53 ± 10 | FFQ | CHD (fatal CHD or nonfatal MI) | 22 | 12% ↓ RR (high vs. low intake) | Bhupathiraju, 2013 [73] |
| EPICOR (Italy) | 29,689 | F | 35–74 | FFQ | CHD (fatal or nonfatal MI or coronary revascularization) | 7.85 | 46% ↓ HR (high vs. low intake) | Bendinelli, 2011 [74] |
| MORGEN (The Netherlands) | 20,069 | M and F | 20–65 | FFQ | CHD (fatal CHD or nonfatal acute MI) | 10 | No association | Oude Griep, 2011 [75] |
| Linxian NIT (China) | 2445 | M and F | 40–69 | FFQ | Heart disease (death) | 26 | No association | Wang, 2016 [76] |
| SMC and COSM (Sweden) | 74,961 | M and F | 45–83 | FFQ | Stroke (cerebral infarction, hemorrhagic stroke or unspecified stroke) | 10.2 | No association | Larsson, 2013 [77] |
| Linxian NIT (China) | 2445 | M and F | 40–69 | FFQ | Stroke (death) | 26 | 38% ↓ HR (per twice/week) | Wang, 2016 [76] |
| NHS and HPFS (USA) | 114,279 | M and F | 34–59 | FFQ | Ischemic stroke (embolic or thrombotic) | 14 | 84% ↓ RR (high vs. low intake) | Joshipura, 1999 [78] |
| DDCHS (Denmark) | 54,506 | M and F | 50–64 | FFQ | Ischemic stroke (ischemic infarction, intracerebral hemorrhage or subarachnoid hemorrhage) | 3.09 | No association | Johnsen, 2003 [79] |
| Study Cohort (Country) | Sample Number | Sex | Age (years) | Dietary Assessment Method | Outcome | Follow-up (years) | Results | First Author, Year (ref) |
|---|---|---|---|---|---|---|---|---|
| NHS and HPFS (USA) | 109,635 | M and F | 30–75 | FFQ | CVD (fatal or nonfatal MI or stroke) | 12–15 | No association | Hung, 2004 [68] |
| JPHCPS (Japan) | 77,891 | M and F | 45–74 | FFQ | CVD (fatal or nonfatal MI or stroke) | 5–8 | No association | Takachi, 2007 [69] |
| SWHS (China) | 74,942 | F | 40–70 | FFQ | CVD (death) | 10.2 | 20% ↓ HR (high vs. low intake) | Zhang, 2011 [80] |
| SMHS (China) | 61,500 | M | 40–74 | FFQ | CVD (death) | 4.6 | 27% ↓ HR (high vs. low intake) | Zhang, 2011 [80] |
| IWHS (USA) | 34,492 | F | 55–69 | FFQ | CVD (death) | 16 | No association | Mink, 2007 [81] |
| PREDIMED (Spain) | 7216 | M and F | 55–80 | FFQ | CVD (cardiovascular death, MI or stroke) | 7 | 36% ↓ HR (high vs. low intake) | Buil-Cosiales, 2016 [70] |
| Odyssey Cohort (USA) | 6151 | M and F | 30–93 | FFQ | CVD (death) | 14 | No association | Genkinger, 2004 [82] |
| MHCPS (USA) | 1273 | M and F | ≥66 | FFQ | CVD (death) | 4.75 | No association | Gaziano, 1995 [71] |
| PLSAW (Australia) | 1226 | F | ≥70 | FFQ | ASVD (fatal ischemic heart disease, heart failure, cerebrovascular disease excluding hemorrhage, or peripheral heart disease) | 15 | 12% ↓ HR (per 10 g/day) | Blekkenhorst, 2017 [72] |
| NHS (USA) | 71,141 | F | 50±7 | FFQ | CHD (fatal CHD or nonfatal MI) | 24 | No association | Bhupathiraju, 2013 [73] |
| SWHS (China) | 67,211 | F | 40–70 | FFQ | CHD (fatal CHD or nonfatal MI) | 9.8 | No association | Yu, 2013 [83] |
| SMHS (China) | 55,474 | M | 40–75 | FFQ | CHD (fatal CHD or nonfatal MI) | 5.4 | No association | Yu, 2013 [83] |
| HPFS (USA) | 42,135 | M | 53 ± 10 | FFQ | CHD (fatal CHD or nonfatal MI) | 22 | No association | Bhupathiraju, 2013 [73] |
| IWHS (USA) | 34,492 | F | 55–69 | FFQ | CHD (death) | 16 | No association | Mink, 2007 [81] |
| EPICOR (Italy) | 29,689 | F | 35–74 | FFQ | CHD (fatal or nonfatal MI or coronary revascularization) | 7.85 | No association | Bendinelli, 2011 [74] |
| MORGEN (The Netherlands) | 20,069 | M and F | 20–65 | FFQ | CHD (fatal CHD or nonfatal acute MI) | 10 | No association | Oude Griep, 2011 [75] |
| PLSAW (Australia) | 1226 | F | ≥70 | FFQ | IHD (death) | 15 | 17% ↓ HR (per 10 g/day) | Blekkenhorst, 2017 [72] |
| Linxian NIT (China) | 2445 | M and F | 40–69 | FFQ | Heart disease (death) | 26 | No association | Wang, 2016 [76] |
| FMCHES (Finland) | 3932 | M and F | 40–74 | FFQ | CVA (fatal or nonfatal) | 24 | 21% ↓ RR (high vs. low intake) | Mizrahi, 2009 [84] |
| PLSAW (Australia) | 1226 | F | ≥70 | FFQ | Ischemic CVA (death) | 15 | No association | Blekkenhorst, 2017 [72] |
| SMC and COSM (Sweden) | 74,961 | M and F | 45–83 | FFQ | Stroke (cerebral infarction, hemorrhagic stroke or unspecified stroke) | 10.2 | No association | Larsson, 2013 [77] |
| Linxian NIT (China) | 2445 | M and F | 40–69 | FFQ | Stroke (death) | 26 | No association | Wang, 2016 [76] |
| NHS and HPFS (USA) | 114,279 | M and F | 34–59 | FFQ | Ischemic stroke (embolic or thrombotic) | 14 | 29% ↓ RR (high vs. low intake) | Joshipura, 1999 [78] |
| DDCHS (Denmark) | 54,506 | M and F | 50–64 | FFQ | Ischemic stroke (ischemic infarction, intracerebral hemorrhage or subarachnoid hemorrhage) | 3.09 | No association | Johnsen, 2003 [79] |
| FMCHES (Finland) | 3932 | M and F | 40–74 | FFQ | Ischemic stroke (fatal or nonfatal) | 24 | 33% ↓ RR (high vs. low intake) | Mizrahi, 2009 [84] |
| FMCHES (Finland) | 3932 | M and F | 40–74 | FFQ | Intracerebral hemorrhage (fatal or nonfatal) | 24 | 51% ↓ RR (high vs. low intake) | Mizrahi, 2009 [84] |
| Study Cohort (Country) | Sample Number | Sex | Age (years) | Dietary Assessment Method | Outcome | Follow-up (years) | Results | First Author, Year (ref) |
|---|---|---|---|---|---|---|---|---|
| PLSAW (Australia) | 1226 | F | ≥70 | FFQ | ASVD (fatal ischemic heart disease, heart failure, cerebrovascular disease excluding hemorrhage, or peripheral heart disease) | 15 | 15% ↓ HR (per 5 g/day) | Blekkenhorst, 2017 [72] |
| SWHS (China) | 67,211 | F | 40–70 | FFQ | CHD (fatal CHD or nonfatal MI) | 9.8 | No association | Yu, 2013 [83] |
| NHS (USA) | 66,360 | F | 30–55 | FFQ | CHD (fatal CHD or nonfatal MI) | 12 | No association | Lin, 2007 [85] |
| SMHS (China) | 55,474 | M | 40–75 | FFQ | CHD (fatal CHD or nonfatal MI) | 5.4 | No association | Yu, 2013 [83] |
| MORGEN (The Netherlands) | 20,069 | M and F | 20–65 | FFQ | CHD (fatal CHD or nonfatal acute MI) | 10 | No association | Oude Griep, 2011 [75] |
| FSII (Finland) | 2748 | M | 30–69 | DHQ | CHD (death) | 26 | No association | Knekt, 1996 [86] |
| FSII (Finland) | 2385 | F | 30–69 | DHQ | CHD (death) | 26 | 50% ↓ RR (high vs. low intake) | Knekt, 1996 [86] |
| Caerphilly Study (UK) | 2512 | M | 45–59 | FFQ | IHD (IHD death, nonfatal MI, MI define by electrocardiogram) | 10 | No association | Hertog, 1997 [87] |
| PLSAW (Australia) | 1226 | F | ≥70 | FFQ | IHD (death) | 15 | 18% ↓ HR (per 5 g/day) | Blekkenhorst, 2017 [72] |
| FMCHES (Finland) | 9208 | M and F | ≥15 | DHQ | CVA (fatal or nonfatal) | 28 | No association | Knekt, 2000 [88] |
| PLSAW (Australia) | 1226 | F | ≥70 | FFQ | Ischemic CVA (death) | 15 | 25% ↓ HR (per 5 g/day) | Blekkenhorst, 2017 [72] |
| SMC and COSM (Sweden) | 74,961 | M and F | 45–83 | FFQ | Stroke (cerebral infarction, hemorrhagic stroke or unspecified stroke) | 10.2 | No association | Larsson, 2013 [77] |
| FMCHES (Finland) | 9208 | M and F | ≥15 | DHQ | Acute strokes | 28 | No association | Knekt, 2000 [88] |
| DDCHS (Denmark) | 54,506 | M and F | 50–64 | FFQ | Ischemic stroke (ischemic infarction, intracerebral hemorrhage or subarachnoid hemorrhage) | 3.09 | No association | Johnsen, 2003 [79] |
| FMCHES (Finland) | 9208 | M and F | ≥15 | DHQ | Intracerebral hemorrhage | 28 | No association | Knekt, 2000 [88] |
| FMCHES (Finland) | 9208 | M and F | ≥15 | DHQ | Thrombosis or embolia | 28 | No association | Knekt, 2000 [88] |
| Study Cohort (Country) | Sample Number | Sex | Age (years) | Dietary Assessment Method | Outcome | Follow-up (years) | Results | First Author, Year (ref) |
|---|---|---|---|---|---|---|---|---|
| JPHCPS (Japan) | 77,891 | M and F | 45–74 | FFQ | CVD (MI or stroke) | 5–8 | No association | Takachi, 2007 [69] |
| IWHS (USA) | 34,489 | F | 55–69 | FFQ | CVD (CHD or stroke) | 16 | No association | Mink, 2007 [81] |
| Framingham Offspring Study (USA) | 2525 | M and F | 26–79 | FFQ | CVD (fatal or nonfatal CHD, CVA, congestive heart failure or peripheral vascular disease) | 11 | 6% ↓ HR (per 1 serving/day) | Jacques, 2013 [89] |
| MHCPS (USA) | 1273 | M and F | ≥66 | FFQ | CVD (death) | 4.75 | 60% ↓ RR (≥1 vs. <1 serving) | Gaziano, 1995 [71] |
| Zutphen Elderly Study (The Netherlands) | 559 | M | 65–84 | DHQ | CVD (fatal ischemic heart disease, stroke or other diseases of the circulatory system) | 15 | 17% ↓ RR (per SD) | Buijsse, 2008 [90] |
| PLSAW (Australia) | 1226 | F | ≥70 | FFQ | ASVD (fatal ischemic heart disease, heart failure, cerebrovascular disease excluding hemorrhage, or peripheral heart disease) | 15 | No association | Blekkenhorst, 2017 [72] |
| NHS (USA) | 66,360 | F | 30–55 | FFQ | CHD (fatal CHD or nonfatal MI) | 12 | No association | Lin, 2007 [85] |
| EPICOR (Italy) | 29,689 | F | 35–74 | FFQ | CHD (fatal or nonfatal MI or coronary revascularization) | 7.85 | No association | Bendinelli, 2011 [74] |
| MORGEN (The Netherlands) | 20,069 | M and F | 20–65 | FFQ | CHD (nonfatal acute MI or fatal CHD) | 10 | No association | Oude Griep, 2011 [75] |
| Framingham Offspring Study (USA) | 2525 | M and F | 26–79 | FFQ | CHD (MI, angina pectoris, coronary insufficiency or CHD death) | 11 | 10% ↓ HR (per 1 serving/day) | Jacques, 2013 [89] |
| Linxian NIT (China) | 2445 | M and F | 40–69 | FFQ | Heart disease (death) | 26 | 23% ↓ HR (per once/day) | Wang, 2016 [76] |
| SMC and COSM (Sweden) | 74,961 | M and F | 45–83 | FFQ | Stroke (cerebral infarction, hemorrhagic stroke or unspecified stroke) | 10.2 | No association | Larsson, 2013 [77] |
| Framingham Offspring Study (USA) | 2525 | M and F | 26–79 | FFQ | Stroke (nonfatal) | 11 | No association | Jacques, 2013 [89] |
| Linxian NIT (China) | 2445 | M and F | 40–69 | FFQ | Stroke (death) | 26 | No association | Wang, 2016 [76] |
| Study Cohort (Country) | Sample Number | Sex | Age (years) | Dietary Assessment Method | Outcome | Follow-up (years) | Results | First Author, Year (ref) |
|---|---|---|---|---|---|---|---|---|
| NHS and HPFS (USA) | 109,635 | M and F | 30–75 | FFQ | CVD (fatal or nonfatal MI or stroke) | 12–15 | No association | Hung, 2004 [68] |
| JCCS (Japan) | 59,485 | M and F | 40–79 | FFQ | CVD (death) | 12.7 | 16% ↓ HR (high vs. low intake) | Nagura, 2009 [91] |
| The SUN Project (Spain) | 13,609 | M and F | 38 | FFQ | CVD (cardiovascular death, MI, revascularization procedures, fatal or nonfatal stroke) | 4.9 | No association | Martínez-González, 2011 [92] |
| NHEFS (USA) | 9632 | M and F | 25–74 | FFQ | CVD (fatal or nonfatal) | 21 | 11% ↓ RR (≥4 vs. <1 times/week) | Bazzano, 2001 [93] |
| ICS (Iran) | 6504 | M and F | ≥35 | FFQ | CVD (fatal or nonfatal MI, sudden cardiac death, unstable angina or stroke) | 6.8 | 33% ↓ HR (>55 years only) (high vs. low intake) | Nouri, 2016 [94] |
| JPHC (Japan) | 40,462 | M and F | 40–59 | FFQ | Ischemic CVD (fatal CI or MI) | 13 | 69% ↓ HR (F only) (high vs. low intake) | Kokubo, 2007 [95] |
| PLSAW (Australia) | 1226 | F | ≥70 | FFQ | ASVD (fatal ischemic heart disease, heart failure, cerebrovascular disease excluding hemorrhage, or peripheral heart disease | 15 | No association | Blekkenhorst, 2017 [72] |
| IWHS (USA) | 99,826 | F | 55–69 | FFQ | CHD (death) | 15 | No association | Kelemen, 2005 [96] |
| NHS (USA) | 84,136 | F | 30–55 | FFQ | CHD (fatal CHD or nonfatal MI) | 26 | No association | Bernstein, 2010 [97] |
| SWHS (China) | 67,211 | F | 40–70 | FFQ | CHD (fatal CHD or nonfatal MI) | 9.8 | No association | Yu, 2013 [83] |
| JCCS (Japan) | 59,485 | M and F | 40–79 | FFQ | CHD (death) | 12.7 | No association | Nagura, 2009 [91] |
| SMHS (China) | 55,474 | M | 40–75 | FFQ | CHD (fatal CHD or nonfatal MI) | 5.4 | No association | Yu, 2013 [83] |
| EPIC (Spain) | 41,078 | M and F | 29–69 | FFQ | CHD (fatal or nonfatal) | 10.4 | No association | Buckland, 2009 [98] |
| EPIC (Greece) | 23,929 | M and F | 20–86 | FFQ | CHD (fatal or nonfatal MI, angina or other CHD) | 10 | No association | Dilis, 2012 [99] |
| The SUN Project (Spain) | 13,609 | M and F | 38 | FFQ | CHD (fatal) | 4.9 | No association | Martínez-González, 2011 [92] |
| ARIC (USA) | 12,066 | M and F | 45–64 | FFQ | CHD (fatal CHD or nonfatal MI) | 22 | No association | Haring, 2014 [100] |
| NHEFS (USA) | 9632 | M and F | 25–74 | FFQ | CHD (fatal or nonfatal) | 21 | 22% ↓ RR (≥4 vs. <1 time/week) | Bazzano, 2001 [93] |
| Linxian NIT (China) | 2445 | M and F | 40–69 | FFQ | Heart disease (death) | 26 | 37% ↓ HR (4 times/week) | Wang, 2016 [76] |
| EPIC (Greece) | 23,601 | M and F | 25–67 | FFQ | CVA (fatal or nonfatal) | 10.6 | No association | Misirli, 2012 [101] |
| FMCHES (Finland) | 3932 | M and F | 40–74 | FFQ | CVA (fatal or nonfatal) | 24 | No association | Mizrahi, 2009 [84] |
| NHS (USA) | 84,010 | F | 30–55 | FFQ | Stroke (fatal or nonfatal ischemic, hemorrhagic or other stroke) | 26 | No association | Bernstein, 2012 [102] |
| JCCS (Japan) | 59,485 | M and F | 40–79 | FFQ | Stroke (fatal ischemic or hemorrhagic stroke) | 12.7 | No association | Nagura, 2009 [91] |
| HPFS (USA) | 43,150 | M | 40–75 | FFQ | Stroke (fatal or nonfatal ischemic, hemorrhagic or other stroke) | 22 | No association | Bernstein, 2012 [102] |
| ARIC (USA) | 11,601 | M and F | 45–64 | FFQ | Stroke (fatal or nonfatal ischemic or hemorrhagic stroke) | 22.7 | No association | Haring, 2015 [103] |
| Linxian NIT (China) | 2445 | M and F | 40–69 | FFQ | Stroke (death) | 26 | No association | Wang, 2016 [76] |
| NHS and HPFS (USA) | 114,279 | M and F | 34–59 | FFQ | Ischemic stroke (embolic or thrombotic) | 14 | No association | Joshipura, 1999 [78] |
| FMCHES (Finland) | 3932 | M and F | 40–74 | FFQ | Ischemic stroke (fatal or nonfatal) | 24 | 28% ↓ RR (high vs. low intake) | Mizrahi, 2009 [84] |
| FMCHES (Finland) | 3932 | M and F | 40–74 | FFQ | Intracerebral hemorrhage (fatal or nonfatal) | 24 | No association | Mizrahi, 2009 [84] |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Blekkenhorst, L.C.; Sim, M.; Bondonno, C.P.; Bondonno, N.P.; Ward, N.C.; Prince, R.L.; Devine, A.; Lewis, J.R.; Hodgson, J.M. Cardiovascular Health Benefits of Specific Vegetable Types: A Narrative Review. Nutrients 2018, 10, 595. https://doi.org/10.3390/nu10050595
Blekkenhorst LC, Sim M, Bondonno CP, Bondonno NP, Ward NC, Prince RL, Devine A, Lewis JR, Hodgson JM. Cardiovascular Health Benefits of Specific Vegetable Types: A Narrative Review. Nutrients. 2018; 10(5):595. https://doi.org/10.3390/nu10050595
Chicago/Turabian StyleBlekkenhorst, Lauren C., Marc Sim, Catherine P. Bondonno, Nicola P. Bondonno, Natalie C. Ward, Richard L. Prince, Amanda Devine, Joshua R. Lewis, and Jonathan M. Hodgson. 2018. "Cardiovascular Health Benefits of Specific Vegetable Types: A Narrative Review" Nutrients 10, no. 5: 595. https://doi.org/10.3390/nu10050595