
Nanoparticle-Mediated Photothermal Therapy Limitation in Clinical Applications Regarding Pain Management

 ,
,  , , and
, , and
Abstract
:1. Introduction
Principle of Photothermal Therapy Using AuNPs
2. Pain Management in PTT and Laser Interstitial Hyperthermia Treatments
2.1. Hepatic Cancer
2.2. Breast Cancer
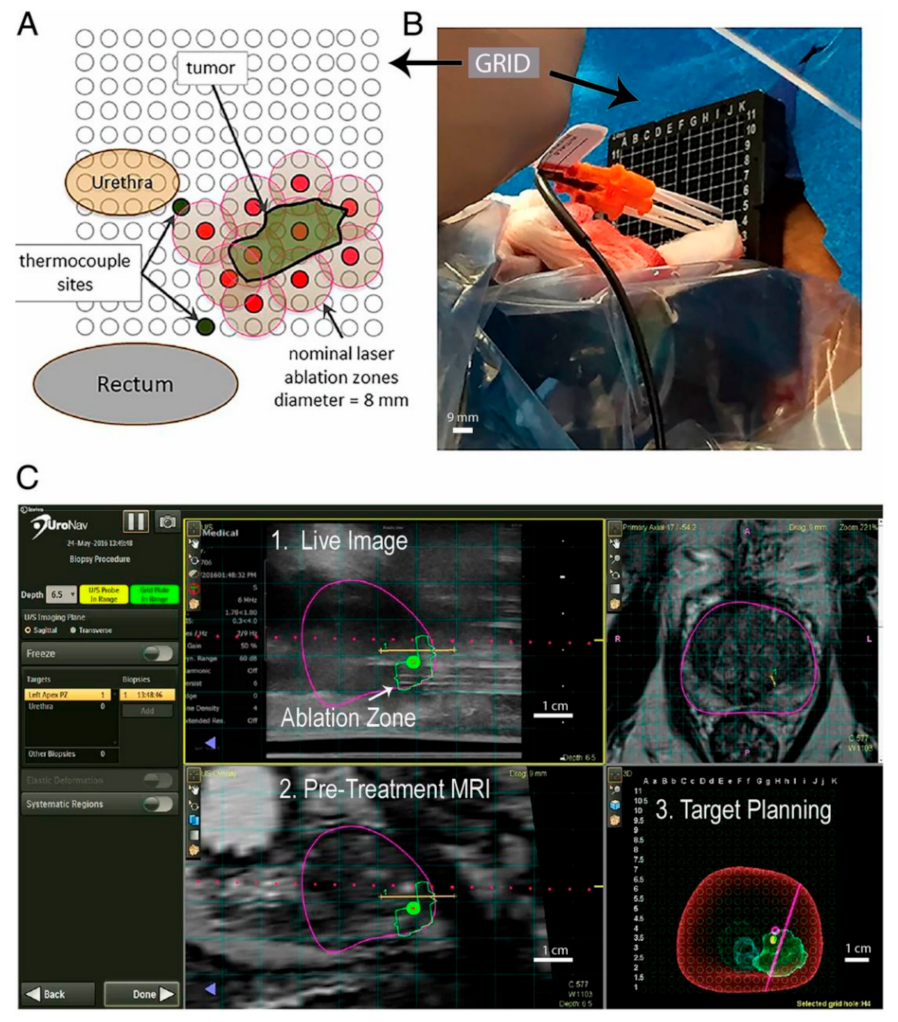
2.3. Prostate Cancer
2.4. Head and Neck Cancer
3. Skin Pain following Laser Radiation
4. Other Strategies for Pain Management in PTT
5. Temperature Monitoring during PTT
6. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ahmad, A.S.; Ormiston-Smith, N.; Sasieni, P. Trends in the lifetime risk of developing cancer in Great Britain: Comparison of risk for those born from 1930 to 1960. Br. J. Cancer 2015, 112, 943–947. [Google Scholar] [CrossRef]
- European Commission. Communication from the Commission to the European Parliament, the Council, the European Economic and Social Committee and the Committee of the Regions on European Missions. European Commission Directorate-General for Research and Innovation Directorate G—Common Policy Centre. 2021. Available online: https://op.europa.eu/en/publication-detail/-/publication/6a2cfdb8-2101-11ec-bd8e-01aa75ed71a1/language-en (accessed on 8 February 2022).
- Ferlay, J.; Ervik, M.; Lam, F.; Colombet, M.; Mery, L.; Piñeros, M.; Znaor, A.; Soerjomataram, I.; Bray, F. Global Cancer Observatory: Cancer Tomorrow; International Agency for Research on Cancer (IARC): Lion, France, 2020. [Google Scholar]
- Bao, X.; Yuan, Y.; Chen, J.; Zhang, B.; Li, D.; Zhou, D.; Jing, P.; Xu, G.; Wang, Y.; Hola, K.; et al. In vivo theranostics with near-infrared-emitting carbon dots—Highly efficient photothermal therapy based on passive targeting after intravenous administration. Light. Sci. Appl. 2018, 7, 91. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.-W.; Su, Y.-L.; Hu, S.-H.; Chen, S.-Y. Functionalized graphene nanocomposites for enhancing photothermal therapy in tumor treatment. Adv. Drug Deliv. Rev. 2016, 105, 190–204. [Google Scholar] [CrossRef] [PubMed]
- Cai, C.; Li, X.; Wang, Y.; Liu, M.; Shi, X.; Xia, J.; Shen, M. Polydopamine-coated gold core/hollow mesoporous silica shell particles as a nanoplatform for multimode imaging and photothermal therapy of tumors. Chem. Eng. J. 2019, 362, 842–850. [Google Scholar] [CrossRef]
- Lu, Y.; Wu, P.; Yin, Y.; Zhang, H.; Cai, C. Aptamer-functionalized graphene oxide for highly efficient loading and cancer cell-specific delivery of antitumor drug. J. Mater. Chem. B 2014, 2, 3849–3859. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Yuan, Z.-F.; Wang, Y.; Chen, W.-H.; Luo, G.-F.; Cheng, S.-X.; Zhuo, R.-X.; Zhang, X.-Z. Multifunctional Envelope-Type Mesoporous Silica Nanoparticles for Tumor-Triggered Targeting Drug Delivery. J. Am. Chem. Soc. 2013, 135, 5068–5073. [Google Scholar] [CrossRef]
- Ruttala, H.B.; Chitrapriya, N.; Kaliraj, K.; Ramasamy, T.; Shin, W.H.; Jeong, J.-H.; Kim, J.R.; Ku, S.K.; Choi, H.-G.; Yong, C.S.; et al. Facile construction of bioreducible crosslinked polypeptide micelles for enhanced cancer combination therapy. Acta Biomater. 2017, 63, 135–149. [Google Scholar] [CrossRef]
- Edgar, L.J.; Vellanki, R.N.; McKee, T.D.; Hedley, D.; Wouters, B.G.; Nitz, M. Isotopologous Organotellurium Probes Reveal Dynamic Hypoxia In Vivo with Cellular Resolution. Angew. Chem. 2016, 128, 13353–13357. [Google Scholar] [CrossRef]
- Brown, S.D.; Nativo, P.; Smith, J.-A.; Stirling, D.; Edwards, P.R.; Venugopal, B.; Flint, D.J.; Plumb, J.A.; Graham, D.; Wheate, N.J. Gold Nanoparticles for the Improved Anticancer Drug Delivery of the Active Component of Oxaliplatin. J. Am. Chem. Soc. 2010, 132, 4678–4684. [Google Scholar] [CrossRef]
- Deng, X.; Guan, W.; Qing, X.; Yang, W.; Que, Y.; Tan, L.; Liang, H.; Zhang, Z.; Wang, B.; Liu, X.; et al. Ultrafast Low-Temperature Photothermal Therapy Activates Autophagy and Recovers Immunity for Efficient Antitumor Treatment. ACS Appl. Mater. Interfaces 2020, 12, 4265–4275. [Google Scholar] [CrossRef]
- Zhou, L.; Xi, Y.; Xue, Y.; Wang, M.; Liu, Y.; Guo, Y.; Lei, B. Injectable self-healing antibacterial bioactive polypeptide-based hybrid nanosystems for efficiently treating multidrug resistant infection, skin-tumor therapy, and enhancing wound healing. Adv. Funct. Mater. 2019, 29, 1806883. [Google Scholar] [CrossRef]
- Chen, W.R.; Adams, R.L.; Carubelli, R.; Nordquist, R.E. Laser-photosensitizer assisted immunotherapy: A novel modality for cancer treatment. Cancer Lett. 1997, 115, 25–30. [Google Scholar] [CrossRef]
- Jolesz, F.A.; Hynynen, K. Magnetic resonance image-guided focused ultrasound surgery. Cancer J. 2002, 8, S100-12. [Google Scholar] [PubMed]
- Gazelle, G.S.; Goldberg, S.N.; Solbiati, L.; Livraghi, T. Tumor Ablation with Radio-frequency Energy. Radiology 2000, 217, 633–646. [Google Scholar] [CrossRef]
- O’Neal, D.P.; Hirsch, L.R.; Halas, N.J.; Payne, J.D.; West, J.L. Photo-thermal tumor ablation in mice using near infrared-absorbing nanoparticles. Cancer Lett. 2004, 209, 171–176. [Google Scholar] [CrossRef]
- Vogel, A.A.; Venugopalan, V. Mechanisms of Pulsed Laser Ablation of Biological Tissues. Chem. Rev. 2003, 103, 577–644. [Google Scholar] [CrossRef] [Green Version]
- Conde, J.; Oliva-Jorge, N.; Zhang, Y.; Artzi, N. Local triple-combination therapy results in tumour regression and prevents recurrence in a colon cancer model. Nat. Mater. 2016, 15, 1128–1138. [Google Scholar] [CrossRef]
- Zeng, X.; Luo, M.; Liu, G.; Wang, X.; Tao, W.; Lin, Y.; Ji, X.; Nie, L.; Mei, L. Polydopamine-Modified Black Phosphorous Nanocapsule with Enhanced Stability and Photothermal Performance for Tumor Multimodal Treatments. Adv. Sci. 2018, 5, 1800510. [Google Scholar] [CrossRef] [Green Version]
- Wu, P.; Deng, D.; Gao, J.; Cai, C. Tubelike Gold Sphere–Attapulgite Nanocomposites with a High Photothermal Conversion Ability in the Near-Infrared Region for Enhanced Cancer Photothermal Therapy. ACS Appl. Mater. Interfaces 2016, 8, 10243–10252. [Google Scholar] [CrossRef]
- Qin, Z.; Bischof, J.C. Thermophysical and biological responses of gold nanoparticle laser heating. Chem. Soc. Rev. 2012, 41, 1191–1217. [Google Scholar] [CrossRef]
- Yang, X.; Yang, M.; Pang, B.; Vara, M.; Xia, Y. Gold Nanomaterials at Work in Biomedicine. Chem. Rev. 2015, 115, 10410–10488. [Google Scholar] [CrossRef] [PubMed]
- Lin, T.-C.; Lin, F.-H.; Lin, J.-C. In vitro feasibility study of the use of a magnetic electrospun chitosan nanofiber composite for hyperthermia treatment of tumor cells. Acta Biomater. 2012, 8, 2704–2711. [Google Scholar] [CrossRef] [PubMed]
- Bettaieb, A.; Wrzal, P.K.; Averill-Bates, D.A. Hyperthermia: Cancer treatment and beyond. Cancer treatment-conventional and innovative approaches. In Cancer Treatment: Conventional and Innovative Approaches; Books on Demand: Norderstedt, Germany, 2013; pp. 257–283. [Google Scholar]
- Takada, T.; Yamashita, T.; Sato, M.; Sato, A.; Ono, I.; Tamura, Y.; Sato, N.; Miyamoto, A.; Ito, A.; Honda, H.; et al. Growth Inhibition of Re-Challenge B16 Melanoma Transplant by Conjugates of Melanogenesis Substrate and Magnetite Nanoparticles as the Basis for Developing Melanoma-Targeted Chemo-Thermo-Immunotherapy. J. Biomed. Biotechnol. 2009, 2009, 457936. [Google Scholar] [CrossRef] [PubMed]
- Babbs, C.F.; DeWitt, D.P. Physical principles of local heat therapy for cancer. Med. Instrum. 1981, 15, 367–373. [Google Scholar]
- Sugahara, T.; Van Der Zee, J.; Kampinga, H.H.; Vujaskovic, Z.; Kondo, M.; Ohnishi, T.; Li, G.; Park, H.J.; Leeper, D.B.; Ostapenko, V.; et al. Kadota Fund International Forum 2004. Application of thermal stress for the improvement of health, 15–18 June 2004, Awaji Yumebutai International Conference Center, Awaji Island, Hyogo, Japan. Final Report. Int. J. Hyperth. 2008, 24, 123–140. [Google Scholar] [CrossRef] [Green Version]
- Van Rhoon, G.C.; Wust, P. Introduction: Non-invasive thermometry for thermotherapy. Int. J. Hyperth. 2005, 21, 489–495. [Google Scholar] [CrossRef]
- Cihoric, N.; Tsikkinis, A.; van Rhoon, G.; Crezee, H.; Aebersold, D.M.; Bodis, S.; Beck, M.; Nadobny, J.; Budach, V.; Wust, P.; et al. Hyperthermia-related clinical trials on cancer treatment within the ClinicalTrials. gov registry. Int. J. Hyperth. 2015, 31, 609–614. [Google Scholar] [CrossRef]
- Fan, W.; Yung, B.; Huang, P.; Chen, X. Nanotechnology for Multimodal Synergistic Cancer Therapy. Chem. Rev. 2017, 117, 13566–13638. [Google Scholar] [CrossRef]
- Weissleder, R. A clearer vision for in vivo imaging. Nat. Biotechnol. 2001, 19, 316–317. [Google Scholar] [CrossRef]
- Antaris, A.L.; Robinson, J.T.; Yaghi, O.K.; Hong, G.; Diao, S.; Luong, R.; Dai, H. Ultra-Low Doses of Chirality Sorted (6,5) Carbon Nanotubes for Simultaneous Tumor Imaging and Photothermal Therapy. ACS Nano 2013, 7, 3644–3652. [Google Scholar] [CrossRef]
- Huang, X.; Jain, P.K.; El-Sayed, I.H.; El-Sayed, M.A. Gold nanoparticles: Interesting optical properties and recent applications in cancer diagnostics and therapy. Nanomedicine 2007, 2, 681–693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Q.; Qi, H.; Ruan, L.; Ren, Y. Experimental Comparison of Photothermal Conversion Efficiency of Gold Nanotriangle and Nanorod in Laser Induced Thermal Therapy. Nanomaterials 2017, 7, 416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deng, H.; Zhong, Y.; Du, M.; Liu, Q.; Fan, Z.; Dai, F.; Zhang, X. Theranostic Self-Assembly Structure of Gold Nanoparticles for NIR Photothermal Therapy and X-Ray Computed Tomography Imaging. Theranostics 2014, 4, 904–918. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, J.; Li, Y.; Teng, Y.; Wang, S.; Guo, J.; Wang, C. NIR-controlled HSP90 inhibitor release from hollow mesoporous nanocarbon for synergistic tumor photothermal therapy guided by photoacoustic imaging. Nanoscale 2020, 12, 14775–14787. [Google Scholar] [CrossRef] [PubMed]
- Zhu, X.; Feng, W.; Chang, J.; Tan, Y.-W.; Li, J.; Chen, M.; Sun, Y.; Li, F. Temperature-feedback upconversion nanocomposite for accurate photothermal therapy at facile temperature. Nat. Commun. 2016, 7, 10437. [Google Scholar] [CrossRef]
- Huang, P.; Lin, J.; Li, W.; Rong, P.; Wang, Z.; Wang, S.; Wang, X.; Sun, X.; Aronova, M.; Niu, G.; et al. Biodegradable Gold Nanovesicles with an Ultrastrong Plasmonic Coupling Effect for Photoacoustic Imaging and Photothermal Therapy. Angew. Chem. 2013, 125, 14208–14214. [Google Scholar] [CrossRef]
- Chen, W.; Qin, M.; Chen, X.; Wang, Q.; Zhang, Z.; Sun, X. Combining photothermal therapy and immunotherapy against melanoma by polydopamine-coated Al2O3 nanoparticles. Theranostics 2018, 8, 2229–2241. [Google Scholar] [CrossRef]
- Marangon, I.; Ménard-Moyon, C.; Silva, A.K.; Bianco, A.; Luciani, N.; Gazeau, F. Synergic mechanisms of photothermal and photodynamic therapies mediated by photosensitizer/carbon nanotube complexes. Carbon 2016, 97, 110–123. [Google Scholar] [CrossRef]
- Moon, H.K.; Lee, S.H.; Choi, H.C. In Vivo Near-Infrared Mediated Tumor Destruction by Photothermal Effect of Carbon Nanotubes. ACS Nano 2009, 3, 3707–3713. [Google Scholar] [CrossRef]
- Yang, K.; Zhang, S.; Zhang, G.; Sun, X.; Lee, S.-T.; Liu, Z. Graphene in Mice: Ultrahigh In Vivo Tumor Uptake and Efficient Photothermal Therapy. Nano Lett. 2010, 10, 3318–3323. [Google Scholar] [CrossRef]
- Yang, K.; Hu, L.; Ma, X.; Ye, S.; Cheng, L.; Shi, X.; Li, C.; Li, Y.; Liu, Z. Multimodal Imaging Guided Photothermal Therapy using Functionalized Graphene Nanosheets Anchored with Magnetic Nanoparticles. Adv. Mater. 2012, 24, 1868–1872. [Google Scholar] [CrossRef] [PubMed]
- Thakur, M.; Kumawat, M.K.; Srivastava, R. Multifunctional graphene quantum dots for combined photothermal and photodynamic therapy coupled with cancer cell tracking applications. RSC Adv. 2017, 7, 5251–5261. [Google Scholar] [CrossRef] [Green Version]
- Jaque, D.; Maestro, L.M.; del Rosal, B.; Haro-Gonzalez, P.; Benayas, A.; Plaza, J.L.; Rodríguez, E.M.; Solé, J. Nanoparticles for photothermal therapies. Nanoscale 2014, 6, 9494–9530. [Google Scholar] [CrossRef] [PubMed]
- Aqel, A.; Abou El-Nour, K.M.M.; Ammar, R.A.A.; Al-Warthan, A. Carbon nanotubes, science and technology part (I) structure, synthesis and characterisation. Arab. J. Chem. 2012, 5, 1–23. [Google Scholar] [CrossRef] [Green Version]
- Zhang, B.; Wang, Y.; Zhai, G. Biomedical applications of the graphene-based materials. Mater. Sci. Eng. C 2016, 61, 953–964. [Google Scholar] [CrossRef]
- Miao, W.; Shim, G.; Lee, S.; Oh, Y.-K. Structure-dependent photothermal anticancer effects of carbon-based photoresponsive nanomaterials. Biomaterials 2014, 35, 4058–4065. [Google Scholar] [CrossRef]
- Shirshahi, V.; Hatamie, S.; Tabatabaei, S.N.; Salimi, M.; Saber, R. Enhanced Thermal Stability and Biocompatibility of Gold Nanorods by Graphene Oxide. Plasmonics 2018, 13, 1585–1594. [Google Scholar] [CrossRef]
- Terentyuk, G.S.; Maslyakova, G.; Suleymanova, L.V.; Khlebtsov, N.; Khlebtsov, B.; Akchurin, G.G.; Maksimova, I.L.; Tuchin, V. Laser-induced tissue hyperthermia mediated by gold nanoparticles: Toward cancer phototherapy. J. Biomed. Opt. 2009, 14, 021016. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Xiu, W.; Sun, Y.; Zhu, D.; Zhang, Q.; Yuwen, L.; Weng, L.; Teng, Z.; Wang, L. RGD-QD-MoS2 nanosheets for targeted fluorescent imaging and photothermal therapy of cancer. Nanoscale 2017, 9, 15835–15845. [Google Scholar] [CrossRef]
- Wang, Z.; Ma, Y.; Yu, X.; Niu, Q.; Han, Z.; Wang, H.; Li, T.; Fu, D.; Achilefu, S.; Qian, Z.; et al. Targeting CXCR4–CXCL12 axis for visualizing, predicting, and inhibiting breast cancer metastasis with theranostic AMD3100–Ag2S quantum dot probe. Adv. Funct. Mater. 2018, 28, 1800732. [Google Scholar] [CrossRef]
- Zhao, H.; Li, L.; Zhang, J.; Zheng, C.; Ding, K.; Xiao, H.; Wang, L.; Zhang, Z. C–C Chemokine Ligand 2 (CCL2) Recruits Macrophage-Membrane-Camouflaged Hollow Bismuth Selenide Nanoparticles to Facilitate Photothermal Sensitivity and Inhibit Lung Metastasis of Breast Cancer. ACS Appl. Mater. Interfaces 2018, 10, 31124–31135. [Google Scholar] [CrossRef] [PubMed]
- Cao, H.; Zou, L.; He, B.; Zeng, L.; Huang, Y.; Yu, H.; Zhang, P.; Yin, Q.; Zhang, Z.; Li, Y. Albumin Biomimetic Nanocorona Improves Tumor Targeting and Penetration for Synergistic Therapy of Metastatic Breast Cancer. Adv. Funct. Mater. 2017, 27. [Google Scholar] [CrossRef]
- Su, J.; Sun, H.; Meng, Q.; Yin, Q.; Zhang, P.; Zhang, Z.; Yu, H.; Li, Y. Bioinspired Nanoparticles with NIR-Controlled Drug Release for Synergetic Chemophotothermal Therapy of Metastatic Breast Cancer. Adv. Funct. Mater. 2016, 26, 7495–7506. [Google Scholar] [CrossRef]
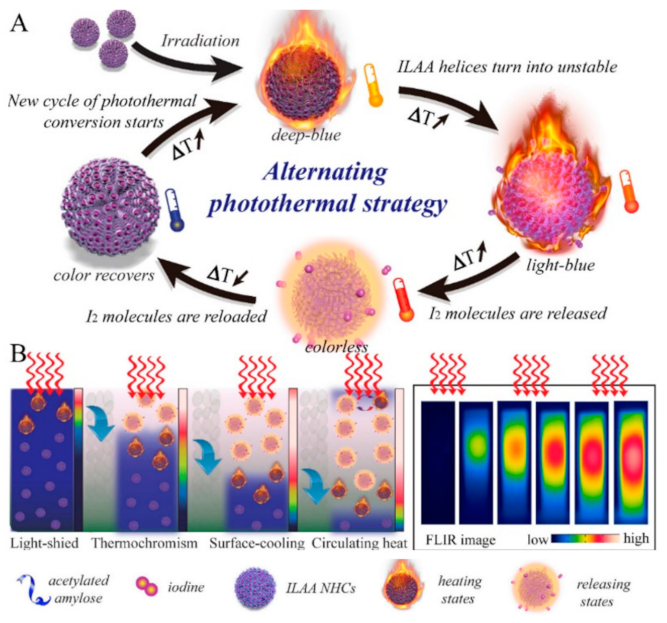
- Tang, P.; Liu, Y.; Liu, Y.; Meng, H.; Liu, Z.; Li, K.; Wu, D. Thermochromism-induced temperature self-regulation and alternating photothermal nanohelix clusters for synergistic tumor chemo/photothermal therapy. Biomaterials 2019, 188, 12–23. [Google Scholar] [CrossRef]
- El-Sayed, I.H.; Huang, X.; El-Sayed, M.A. Selective laser photo-thermal therapy of epithelial carcinoma using anti-EGFR antibody conjugated gold nanoparticles. Cancer Lett. 2006, 239, 129–135. [Google Scholar] [CrossRef]
- Zhang, C.; Yong, Y.; Song, L.; Dong, X.; Zhang, X.; Liu, X.; Gu, Z.; Zhao, Y.; Hu, Z. Multifunctional WS2@ Poly (ethylene imine) Nanoplatforms for Imaging Guided Gene-Photothermal Synergistic Therapy of Cancer. Adv. Healthc. Mater. 2016, 5, 2776–2787. [Google Scholar] [CrossRef]
- Pan, L.; Liu, J.; Shi, J. Nuclear-Targeting Gold Nanorods for Extremely Low NIR Activated Photothermal Therapy. ACS Appl. Mater. Interfaces 2017, 9, 15952–15961. [Google Scholar] [CrossRef]
- Treede, R.-D. The International Association for the Study of Pain definition of pain: As valid in 2018 as in 1979, but in need of regularly updated footnotes. Pain Rep. 2018, 3, e643. [Google Scholar] [CrossRef]
- Merskey, H. Pain terms: A list with definitions and notes on usage. Recommended by the IASP Subcommittee on Taxonomy. Pain 1979, 6, 249–252. [Google Scholar]
- Raja, S.N.; Carr, D.B.; Cohen, M.; Finnerup, N.B.; Flor, H.; Gibson, S.; Keefe, F.J.; Mogil, J.S.; Ringkamp, M.; Sluka, K.A.; et al. The revised International Association for the Study of Pain definition of pain: Concepts, challenges, and compromises. Pain 2020, 161, 1976–1982. [Google Scholar] [CrossRef]
- Anand, K.J.; Craig, K.D. New perspectives on the definition of pain. Pain 1996, 67, 3–6. [Google Scholar]
- Williams, A.C.d.C.; Craig, K.D. Updating the definition of pain. Pain 2016, 157, 2420–2423. [Google Scholar] [CrossRef] [PubMed]
- Cohen, M.; Quintner, J.; Van Rysewyk, S. Reconsidering the International Association for the Study of Pain definition of pain. Pain Rep. 2018, 3, e634. [Google Scholar] [CrossRef] [PubMed]
- Aydede, M. Does the IASP definition of pain need updating? Pain Rep. 2019, 4, e777. [Google Scholar] [CrossRef] [PubMed]
- Wells, J.; Kao, C.; Mariappan, K.G.; Albea, J.; Jansen, E.D.; Konrad, P.; Mahadevan-Jansen, A. Optical stimulation of neural tissue in vivo. Opt. Lett. 2005, 30, 504–506. [Google Scholar] [CrossRef]
- Wells, J.; Kao, C.; Jansen, E.D.; Konrad, P.; Mahadevan-Jansen, A. Application of infrared light for in vivo neural stimulation. J. Biomed. Opt. 2005, 10, 064003. [Google Scholar] [CrossRef] [Green Version]
- Loeser, J.D.; Treede, R.-D. The Kyoto protocol of IASP basic pain Terminology. Pain 2008, 137, 473–477. [Google Scholar] [CrossRef]
- Argoff, C.E.; Dubin, A.; Pilitsis, J.; McCleane, G. Pain Management Secrets E-Book; Elsevier Health Sciences: Oxford, UK, 2009. [Google Scholar]
- Von Ungern-Sternberg, B.S.; Habre, W. Pediatric anesthesia—Potential risks and their assessment: Part I. Pediatric Anesth. 2007, 17, 206–215. [Google Scholar] [CrossRef]
- UnicStojanovic, D.; Babic, S.; Jovic, M. Benefits, Risks and Complications of Perioperative Use of Epidural Anesthesia. Med. Arch. 2012, 66, 340–343. [Google Scholar] [CrossRef] [Green Version]
- Wernli, K.J.; Brenner, A.; Rutter, C.M.; Inadomi, J. Risks Associated with Anesthesia Services During Colonoscopy. Gastroenterology 2016, 150, 888–894. [Google Scholar] [CrossRef] [Green Version]
- Maestro, L.M.; Camarillo, E.; Sánchez-Gil, J.A.; Rodríguez-Oliveros, R.; Ramiro-Bargueño, J.; Caamaño, A.J.; Jaque, F.; Solé, J.G.; Jaque, D. Gold nanorods for optimized photothermal therapy: The influence of irradiating in the first and second biological windows. RSC Adv. 2014, 4, 54122–54129. [Google Scholar] [CrossRef] [Green Version]
- Riley, R.S.; Day, E.S. Gold nanoparticle-mediated photothermal therapy: Applications and opportunities for multimodal cancer treatment. WIREs Nanomed. Nanobiotechnol. 2017, 9, e1449. [Google Scholar] [CrossRef] [PubMed]
- Loo, C.; Lin, A.; Hirsch, L.; Lee, M.-H.; Barton, J.; Halas, N.; West, J.; Drezek, R. Nanoshell-Enabled Photonics-Based Imaging and Therapy of Cancer. Technol. Cancer Res. Treat. 2004, 3, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Bickford, L.; Sun, J.; Fu, K.; Lewinski, N.; Nammalvar, V.; Chang, J.; Drezek, R. Enhanced multi-spectral imaging of live breast cancer cells using immunotargeted gold nanoshells and two-photon excitation microscopy. Nanotechnology 2008, 19, 315102. [Google Scholar] [CrossRef] [PubMed]
- Hwang, S.; Nam, J.; Jung, S.; Song, J.; Doh, H.; Kim, S. Gold nanoparticle-mediated photothermal therapy: Current status and future perspective. Nanomedicine 2014, 9, 2003–2022. [Google Scholar] [CrossRef] [PubMed]
- Melamed, J.; Edelstein, R.S.; Day, E. Elucidating the Fundamental Mechanisms of Cell Death Triggered by Photothermal Therapy. ACS Nano 2015, 9, 6–11. [Google Scholar] [CrossRef]
- Pérez-Hernández, M.; Del Pino, P.; Mitchell, S.G.; Moros, M.; Stepien, G.; Pelaz, B.; Parak, W.J.; Gálvez, E.M.; Pardo, J.; De La Fuente, J.M. Dissecting the Molecular Mechanism of Apoptosis during Photothermal Therapy Using Gold Nanoprisms. ACS Nano 2015, 9, 52–61. [Google Scholar] [CrossRef]
- Lee, J.; Chatterjee, D.K.; Lee, M.H.; Krishnan, S. Gold nanoparticles in breast cancer treatment: Promise and potential pitfalls. Cancer Lett. 2014, 347, 46–53. [Google Scholar] [CrossRef] [Green Version]
- Jiang, K.; Smith, D.A.; Pinchuk, A. Size-Dependent Photothermal Conversion Efficiencies of Plasmonically Heated Gold Nanoparticles. J. Phys. Chem. C 2013, 117, 27073–27080. [Google Scholar] [CrossRef]
- Miyako, E.; Kono, K.; Yuba, E.; Hosokawa, C.; Nagai, H.; Hagihara, Y. Carbon nanotube–liposome supramolecular nanotrains for intelligent molecular-transport systems. Nat. Commun. 2012, 3, 1226. [Google Scholar] [CrossRef] [Green Version]
- Baffou, G.; Quidant, R. Thermo-plasmonics: Using metallic nanostructures as nano-sources of heat. Laser Photon-Rev. 2013, 7, 171–187. [Google Scholar] [CrossRef]
- Ansari, M.A.; Erfanzadeh, M.; Mohajerani, E. Mechanisms of Laser-Tissue Interaction: II. Tissue Thermal Properties. J. Lasers Med. Sci. 2013, 4, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Almada, M.; Leal-Martínez, B.; Hassan, N.; Kogan, M.; Burboa, M.; Topete, A.; Valdez, M.; Juárez, J. Photothermal conversion efficiency and cytotoxic effect of gold nanorods stabilized with chitosan, alginate and poly(vinyl alcohol). Mater. Sci. Eng. C 2017, 77, 583–593. [Google Scholar] [CrossRef] [PubMed]
- Roper, D.K.; Ahn, W.; Hoepfner, M. Microscale Heat Transfer Transduced by Surface Plasmon Resonant Gold Nanoparticles. J. Phys. Chem. C 2007, 111, 3636–3641. [Google Scholar] [CrossRef] [Green Version]
- Rashidi-Huyeh, M.; Palpant, B. Thermal response of nanocomposite materials under pulsed laser excitation. J. Appl. Phys. 2004, 96, 4475. [Google Scholar] [CrossRef]
- Wilson, O.M.; Hu, X.; Cahill, D.G.; Braun, P.V. Colloidal metal particles as probes of nanoscale thermal transport in fluids. Phys. Rev. B 2002, 66, 224301. [Google Scholar] [CrossRef] [Green Version]
- Plech, A.; Kotaidis, V.; Grésillon, S.; Dahmen, C.; von Plessen, G. Laser-induced heating and melting of gold nanoparticles studied by time-resolved x-ray scattering. Phys. Rev. B 2004, 70, 195423. [Google Scholar] [CrossRef]
- Chen, H.; Shao, L.; Ming, T.; Sun, Z.; Zhao, C.; Yang, B.; Wang, J. Understanding the Photothermal Conversion Efficiency of Gold Nanocrystals. Small 2010, 6, 2272–2280. [Google Scholar] [CrossRef]
- Li, J.; Zhang, W.; Ji, W.; Wang, J.; Wang, N.; Wu, W.; Wu, Q.; Hou, X.; Hu, W.; Li, L. Near infrared photothermal conversion materials: Mechanism, preparation, and photothermal cancer therapy applications. J. Mater. Chem. B 2021, 9, 7909–7926. [Google Scholar] [CrossRef]
- Hessel, C.M.; Pattani, V.P.; Rasch, M.; Panthani, M.G.; Koo, B.; Tunnell, J.W.; Korgel, B.A. Copper Selenide Nanocrystals for Photothermal Therapy. Nano Lett. 2011, 11, 2560–2566. [Google Scholar] [CrossRef] [Green Version]
- Lyu, Y.; Xie, C.; Chechetka, S.A.; Miyako, E.; Pu, K. Semiconducting Polymer Nanobioconjugates for Targeted Photothermal Activation of Neurons. J. Am. Chem. Soc. 2016, 138, 9049–9052. [Google Scholar] [CrossRef] [PubMed]
- Cole, J.R.; Mirin, N.A.; Knight, M.W.; Goodrich, G.P.; Halas, N.J. Photothermal Efficiencies of Nanoshells and Nanorods for Clinical Therapeutic Applications. J. Phys. Chem. C 2009, 113, 12090–12094. [Google Scholar] [CrossRef]
- Tian, Q.; Jiang, F.; Zou, R.; Liu, Q.; Chen, Z.; Zhu, M.; Yang, S.; Wang, J.; Wang, J.; Hu, J. Hydrophilic Cu9S5 Nanocrystals: A Photothermal Agent with a 25.7% Heat Conversion Efficiency for Photothermal Ablation of Cancer Cells in Vivo. ACS Nano 2011, 5, 9761–9771. [Google Scholar] [CrossRef] [PubMed]
- Maestro, L.M.; Gonzalez, P.H.; Sánchez-Iglesias, A.; Liz-Marzán, L.M.; Solé, J.G.; Jaque, D. Quantum Dot Thermometry Evaluation of Geometry Dependent Heating Efficiency in Gold Nanoparticles. Langmuir 2014, 30, 1650–1658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, Q.; Zeng, W.; Zhang, C.; Meng, Z.; Wu, J.; Zhu, Q.; Wu, D.; Zhu, H. Broadband absorption and enhanced photothermal conversion property of octopod-like Ag@Ag2S core@shell structures with gradually varying shell thickness. Sci. Rep. 2017, 7, 17782. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, X.; Yang, K.; Chen, X.; Li, W. Black hollow silicon oxide nanoparticles as highly efficient photothermal agents in the second near-infrared window for in vivo cancer therapy. Biomaterials 2017, 143, 120–129. [Google Scholar] [CrossRef] [PubMed]
- Marin, R.; Skripka, A.; Besteiro, L.V.; Benayas, A.; Wang, Z.; Govorov, A.O.; Canton, P.; Vetrone, F. Highly Efficient Copper Sulfide-Based Near-Infrared Photothermal Agents: Exploring the Limits of Macroscopic Heat Conversion. Small 2018, 14, e1803282. [Google Scholar] [CrossRef]
- Feng, W.; Chen, L.; Qin, M.; Zhou, X.; Zhang, Q.; Miao, Y.; Qiu, K.; Zhang, Y.; He, C. Flower-like PEGylated MoS2 nanoflakes for near-infrared photothermal cancer therapy. Sci. Rep. 2015, 5, 17422. [Google Scholar] [CrossRef] [Green Version]
- Szuplewska, A.; Kulpińska, D.; Dybko, A.; Jastrzębska, A.M.; Wojciechowski, T.; Rozmysłowska, A.; Chudy, M.; Grabowska-Jadach, I.; Ziemkowska, W.; Brzózka, Z.; et al. 2D Ti2C (MXene) as a novel highly efficient and selective agent for photothermal therapy. Mater. Sci. Eng. C 2019, 98, 874–886. [Google Scholar] [CrossRef]
- Wang, J.; Li, Y.; Deng, L.; Wei, N.; Weng, Y.; Dong, S.; Qi, D.; Qiu, J.; Chen, X.; Wu, T. High-Performance Photothermal Conversion of Narrow-Bandgap Ti2O3 Nanoparticles. Adv. Mater. 2016, 29, e1603730. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Wang, H.; Yang, Y.; Jin, L.; Liu, Y.; Wang, Y.; Yan, X.; Xu, J.; Gao, R.; Lei, P.; et al. Plasmonic Pt Superstructures with Boosted Near-Infrared Absorption and Photothermal Conversion Efficiency in the Second Biowindow for Cancer Therapy. Adv. Mater. 2019, 31, e1904836. [Google Scholar] [CrossRef] [PubMed]
- Savchuk, O.A.; Carvajal, J.J.; Massons, J.; Aguiló, M.; Díaz, F. Determination of photothermal conversion efficiency of graphene and graphene oxide through an integrating sphere method. Carbon 2016, 103, 134–141. [Google Scholar] [CrossRef]
- Guan, Q.; Zhou, L.-L.; Zhou, L.-N.; Li, M.; Qin, G.-X.; Li, W.-Y.; Li, Y.-A.; Dong, Y.-B. A carbon nanomaterial derived from a nanoscale covalent organic framework for photothermal therapy in the NIR-II biowindow. Chem. Commun. 2020, 56, 7793–7796. [Google Scholar] [CrossRef] [PubMed]
- Maestro, L.M.; Haro-González, P.; del Rosal, B.; Ramiro, J.; Caamaño, A.J.; Carrasco, E.; Juarranz, A.; Sanz-Rodríguez, F.; Solé, J.G.; Jaque, D. Heating efficiency of multi-walled carbon nanotubes in the first and second biological windows. Nanoscale 2013, 5, 7882–7889. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Lu, Z.; Zhu, X.; Wang, X.; Liao, Y.; Ma, Z.; Li, F. NIR photothermal therapy using polyaniline nanoparticles. Biomaterials 2013, 34, 9584–9592. [Google Scholar] [CrossRef]
- Liu, Z.; Cheng, L.; Zhang, L.; Yang, Z.; Liu, Z.; Fang, J. Sub-100 nm hollow Au–Ag alloy urchin-shaped nanostructure with ultrahigh density of nanotips for photothermal cancer therapy. Biomaterials 2014, 35, 4099–4107. [Google Scholar] [CrossRef]
- Sebastian, V.; Lee, S.-K.; Jensen, K.F. Engineering the synthesis of silica–gold nano-urchin particles using continuous synthesis. Nanoscale 2014, 6, 13228–13235. [Google Scholar] [CrossRef] [Green Version]
- Nolsøe, C.P.; Torp-Pedersen, S.; Burcharth, F.; Horn, T.; Christensen, N.E.; Olldag, E.S.; Andersen, P.H.; Karstrup, S.; Lorentzen, T. Interstitial hyperthermia of colorectal liver metastases with a US-guided Nd-YAG laser with a diffuser tip: A pilot clinical study. Radiology 1993, 187, 333–337. [Google Scholar] [CrossRef]
- Amin, Z.; Donald, J.J.; Masters, A.; Kant, R.; Steger, A.C.; Bown, S.G.; Lees, W.R. Hepatic metastases: Interstitial laser photocoagulation with real-time US monitoring and dynamic CT evaluation of treatment. Radiology 1993, 187, 339–347. [Google Scholar] [CrossRef]
- Masters, A.; Steger, A.; Lees, W.; Walmsley, K.; Bown, S. Interstitial laser hyperthermia: A new approach for treating liver metastases. Br. J. Cancer 1992, 66, 518–522. [Google Scholar] [CrossRef] [Green Version]
- Vogl, T.J.; Straub, R.; Eichler, K.; Woitaschek, D.; Mack, M.G. Malignant Liver Tumors Treated with MR Imaging–guided Laser-induced Thermotherapy: Experience with Complications in 899 Patients (2520 lesions). Radiology 2002, 225, 367–377. [Google Scholar] [CrossRef] [PubMed]
- Harries, S.A.; Amin, Z.; Smith, M.E.F.; Lees, W.R.; Cooke, J.; Cook, M.G.; Scurr, J.H.; Kissin, M.W.; Bown, S.G. Interstitial laser photocoagulation as a treatment for breast cancer. Br. J. Surg. 1994, 81, 1617–1619. [Google Scholar] [CrossRef] [PubMed]
- Robinson, D.S.; Parel Ing, J.-M.; Denham, D.B.; González-Cirre, X.; Schachner, R.D.; Herron, A.J.; Comander, J.; Hauptmann, G. Interstitial laser hyperthermia model development for minimally invasive therapy of breast carcinoma. J. Am. Coll. Surg. 1998, 186, 284–292. [Google Scholar] [CrossRef]
- Dowlatshahi, K.; Francescatti, D.S.; Bloom, K.J. Laser therapy for small breast cancers. Am. J. Surg. 2002, 184, 359–363. [Google Scholar] [CrossRef]
- Rastinehad, A.R.; Anastos, H.; Wajswol, E.; Winoker, J.S.; Sfakianos, J.P.; Doppalapudi, S.K.; Carrick, M.R.; Knauer, C.J.; Taouli, B.; Lewis, S.C.; et al. Gold nanoshell-localized photothermal ablation of prostate tumors in a clinical pilot device study. Proc. Natl. Acad. Sci. USA 2019, 116, 18590–18596. [Google Scholar] [CrossRef] [Green Version]
- Staves, B. Pilot Study of AurolaseTM Therapy in Refractory and/or Recurrent Tumors of the Head and Neck. ClinicalTrials. gov Identifier: NCT00848042. 2010. Available online: https://clinicaltrials.gov/ct2/show/NCT00848042 (accessed on 8 February 2022).
- Valentine, R.M.; Ibbotson, S.H.; Brown, C.T.A.; Wood, K.; Moseley, H. A quantitative comparison of 5-aminolaevulinic acid-and methyl aminolevulinate-induced fluorescence, photobleaching and pain during photodynamic therapy. Photochem. Photobiol. 2011, 87, 242–249. [Google Scholar] [CrossRef]
- Ang, J.M.; bin Riaz, I.; Kamal, M.U.; Paragh, G.; Zeitouni, N.C. Photodynamic therapy and pain: A systematic review. Photodiagnosis Photodyn. Ther. 2017, 19, 308–344. [Google Scholar] [CrossRef]
- Fink, C.; Enk, A.; Gholam, P. Photodynamic therapy–aspects of pain management. J. Dtsch. Dermatol. Ges. 2015, 13, 15–22. [Google Scholar] [CrossRef] [Green Version]
- Haimi-Cohen, R.; Cohen, A.; Carmon, A. A model for the temperature distribution in skin noxiously stimulated by a brief pulse of CO2 laser radiation. J. Neurosci. Methods 1983, 8, 127–137. [Google Scholar] [CrossRef]
- Spiegel, J.; Hansen, C.; Treede, R.-D. Clinical evaluation criteria for the assessment of impaired pain sensitivity by thulium-laser evoked potentials. Clin. Neurophysiol. 2000, 111, 725–735. [Google Scholar] [CrossRef]
- Arits, A.; Van De Weert, M.; Nelemans, P.; Kelleners-Smeets, N. Pain during topical photodynamic therapy: Uncomfortable and unpredictable. J. Eur. Acad. Dermatol. Venereol. 2010, 24, 1452–1457. [Google Scholar] [CrossRef] [PubMed]
- Borelli, C.; Herzinger, T.; Merk, K.; Berking, C.; Kunte, C.; Plewig, G.; Degitz, K. Effect of Subcutaneous Infiltration Anesthesia on Pain in Photodynamic Therapy: A Controlled Open Pilot Trial. Dermatol. Surg. 2007, 33, 314–318. [Google Scholar] [CrossRef]
- Tyrrell, J.; Campbell, S.; Curnow, A. The effect of air cooling pain relief on protoporphyrin IX photobleaching and clinical efficacy during dermatological photodynamic therapy. J. Photochem. Photobiol. B Biol. 2011, 103, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Apalla, Z.; Sotiriou, E.; Panagiotidou, D.; Lefaki, I.; Goussi, C.; Ioannides, D. The impact of different fluence rates on pain and clinical outcome in patients with actinic keratoses treated with photodynamic therapy. Photodermatol. Photoimmunol. Photomed. 2011, 27, 181–185. [Google Scholar] [CrossRef] [PubMed]
- Babilas, P.; Knobler, R.; Hummel, S.; Gottschaller, C.; Maisch, T.; Koller, M.; Landthaler, M.; Szeimies, R.-M. Variable pulsed light is less painful than light-emitting diodes for topical photodynamic therapy of actinic keratosis: A prospective randomized controlled trial. Br. J. Dermatol. 2007, 157, 111–117. [Google Scholar] [CrossRef]
- Stangeland, K.; Kroon, S. Cold air analgesia as pain reduction during photodynamic therapy of actinic keratoses. J. Eur. Acad. Dermatol. Venereol. 2012, 26, 849–854. [Google Scholar] [CrossRef]
- Chaves, Y.N.; Torezan, L.A.; Niwa, A.B.M.; Sanches, A.S., Jr.; Neto, C.F. Pain in photodynamic therapy: Mechanism of action and management strategies. Anais Bras. Dermatol. 2012, 87, 521–529. [Google Scholar] [CrossRef] [Green Version]
- Halldin, C.; Paoli, J.; Sandberg, C.; Gonzalez, H.; Wennberg, A.-M. Nerve blocks enable adequate pain relief during topical photodynamic therapy of field cancerization on the forehead and scalp. Br. J. Dermatol. 2009, 160, 795–800. [Google Scholar] [CrossRef]
- Serra-Guillén, C.; Hueso, L.; Nagore, E.; Vila, M.; Llombart, B.; Caballero, C.R.; Botella-Estrada, R.; Sanmartín, O.; Alfaro-Rubio, A. Comparative study between cold air analgesia and supraorbital and supratrochlear nerve block for the management of pain during photodynamic therapy for actinic keratoses of the frontotemporal zone. Br. J. Dermatol. 2009, 161, 353–356. [Google Scholar] [CrossRef]
- Lumpkin, E.A.; Caterina, M.J. Mechanisms of sensory transduction in the skin. Nature 2007, 445, 858–865. [Google Scholar] [CrossRef]
- Beissner, F.; Brandau, A.; Henke, C.; Felden, L.; Baumgärtner, U.; Treede, R.-D.; Oertel, B.G.; Lotsch, J. Quick Discrimination of Adelta and C Fiber Mediated Pain Based on Three Verbal Descriptors. PLoS ONE 2010, 5, e12944. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, X.; Naylor, M.F.; Le, H.; Nordquist, R.E.; Teague, T.K.; Howard, C.A.; Murray, C.; Chen, W.R. Clinical effects of in situ photoimmunotherapy on late-stage melanoma patients: A preliminary study. Cancer Biol. Ther. 2010, 10, 1081–1087. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barge, J.; Glanzmann, T.; Zellweger, M.; Salomon, D.; Bergh, H.V.D.; Wagnières, G. Correlations between photoactivable porphyrins’ fluorescence, erythema and the pain induced by PDT on normal skin using ALA-derivatives. Photodiagn. Photodyn. Ther. 2013, 10, 683–693. [Google Scholar] [CrossRef] [PubMed]
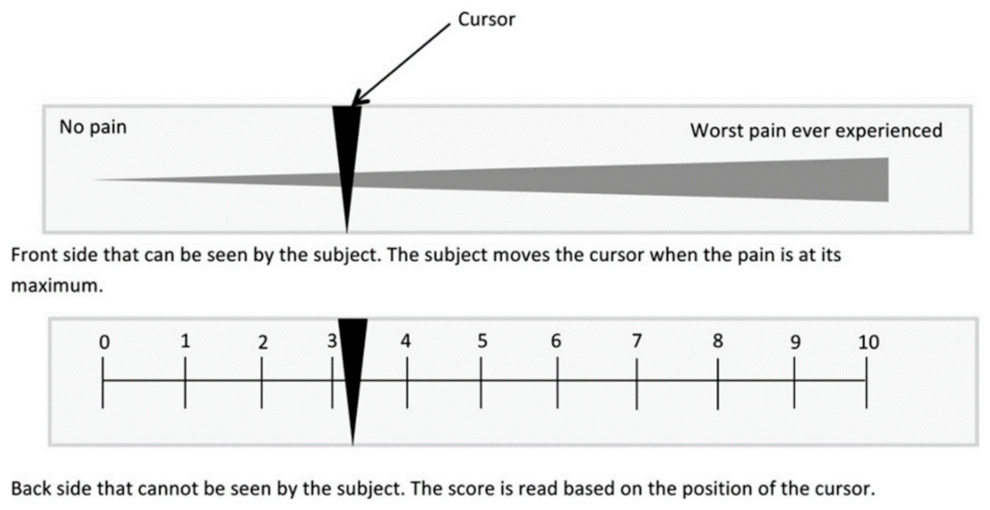
- Johnson, C. Measuring pain. Visual analog scale versus numeric pain scale: What is the difference? J. Chiropr. Med. 2005, 4, 43. [Google Scholar] [CrossRef] [Green Version]
- Langley, G.B.; Sheppeard, H. The visual analogue scale: Its use in pain measurement. Rheumatol. Int. 1985, 5, 145–148. [Google Scholar] [CrossRef]
- Duncan, K.J. Laser based power transmission: Component selection and laser hazard analysis. In Proceedings of the 2016 IEEE PELS Workshop on Emerging Technologies: Wireless Power Transfer (WoW), Knoxville, TN, USA, 4–6 October 2016. [Google Scholar]
- Jung, B.-K.; Lee, Y.K.; Hong, J.; Ghandehari, H.; Yun, C.-O. Mild Hyperthermia Induced by Gold Nanorod-Mediated Plasmonic Photothermal Therapy Enhances Transduction and Replication of Oncolytic Adenoviral Gene Delivery. ACS Nano 2016, 10, 10533–10543. [Google Scholar] [CrossRef]
- Kaneti, Y.V.; Chen, C.; Liu, M.; Wang, X.; Yang, J.L.; Taylor, R.A.; Jiang, X.; Yu, A. Carbon-Coated Gold Nanorods: A Facile Route to Biocompatible Materials for Photothermal Applications. ACS Appl. Mater. Interfaces 2015, 7, 25658–25668. [Google Scholar] [CrossRef]
- Yang, Y.; Zhu, W.; Dong, Z.; Chao, Y.; Xu, L.; Chen, M.; Liu, Z. 1D Coordination Polymer Nanofibers for Low-Temperature Photothermal Therapy. Adv. Mater. 2017, 29, 1703588. [Google Scholar] [CrossRef]
- Zhang, Y.; Sha, R.; Zhang, L.; Zhang, W.; Jin, P.; Xu, W.; Ding, J.; Lin, J.; Qian, J.; Yao, G.; et al. Harnessing copper-palladium alloy tetrapod nanoparticle-induced pro-survival autophagy for optimized photothermal therapy of drug-resistant cancer. Nat. Commun. 2018, 9, 4236. [Google Scholar] [CrossRef] [Green Version]
- Ren, X.; Chen, Y.; Peng, H.; Fang, X.; Zhang, X.; Chen, Q.; Wang, X.; Yang, W.; Sha, X. Blocking Autophagic Flux Enhances Iron Oxide Nanoparticle Photothermal Therapeutic Efficiency in Cancer Treatment. ACS Appl. Mater. Interfaces 2018, 10, 27701–27711. [Google Scholar] [CrossRef]
- Tian, G.; Zhang, X.; Zheng, X.; Yin, W.; Ruan, L.; Liu, X.; Zhou, L.; Yan, L.; Li, S.; Gu, Z.; et al. Multifunctional RbxWO3 Nanorods for Simultaneous Combined Chemo-photothermal Therapy and Photoacoustic/CT Imaging. Small 2014, 10, 4160–4170. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Peng, J.; Tan, L.; Wu, J.; Shi, K.; Qu, Y.; Wei, X.; Qian, Z. Mild photothermal therapy/photodynamic therapy/chemotherapy of breast cancer by Lyp-1 modified Docetaxel/IR820 Co-loaded micelles. Biomaterials 2016, 106, 119–133. [Google Scholar] [CrossRef] [PubMed]
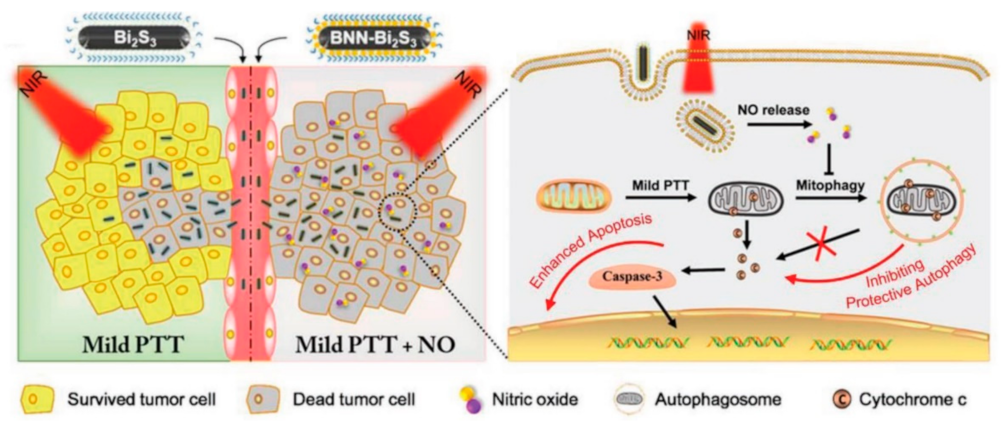
- Sarkar, S.; Korolchuk, V.I.; Renna, M.; Imarisio, S.; Fleming, A.; Williams, A.; Garcia-Arencibia, M.; Rose, C.; Luo, S.; Underwood, B.R.; et al. Complex inhibitory effects of nitric oxide on autophagy. Mol. Cell 2011, 43, 19–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, X.; Guo, Z.; Liu, J.; Tian, G.; Chen, K.; Yu, S.; Gu, Z. Near infrared light triggered nitric oxide releasing platform based on upconversion nanoparticles for synergistic therapy of cancer stem-like cells. Sci. Bull. 2017, 62, 985–996. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Du, J.; Guo, Z.; Yu, J.; Gao, Q.; Yin, W.; Zhu, S.; Gu, Z.; Zhao, Y. Efficient Near Infrared Light Triggered Nitric Oxide Release Nanocomposites for Sensitizing Mild Photothermal Therapy. Adv. Sci. 2019, 6, 1801122. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Liu, J.; Liu, Y.; Wang, L.; Cao, M.; Ji, Y.; Wu, X.; Xu, Y.; Bai, B.; Miao, Q.; et al. Gd-Hybridized Plasmonic Au-Nanocomposites Enhanced Tumor-Interior Drug Permeability in Multimodal Imaging-Guided Therapy. Adv. Mater. 2016, 28, 8950–8958. [Google Scholar] [CrossRef]
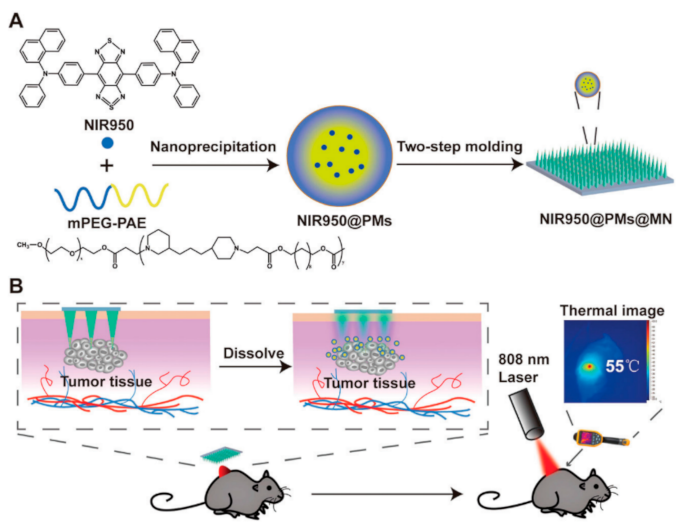
- Wei, S.; Quan, G.; Lu, C.; Pan, X.; Wu, C. Dissolving microneedles integrated with pH-responsive micelles containing AIEgen with ultra-photostability for enhancing melanoma photothermal therapy. Biomater. Sci. 2020, 8, 5739–5750. [Google Scholar] [CrossRef]
- Ma, G.; Wu, C. Microneedle, bio-microneedle and bio-inspired microneedle: A review. J. Control. Release 2017, 251, 11–23. [Google Scholar] [CrossRef] [Green Version]
- Kaushik, S.; Hord, A.H.; Denson, D.D.; McAllister, D.V.; Smitra, S.; Allen, M.G.; Prausnitz, M.R. Lack of pain associated with microfabricated microneedles. Anesth. Analg. 2001, 92, 502–504. [Google Scholar] [CrossRef] [Green Version]
- Arya, J.; Henry, S.; Kalluri, H.; McAllister, D.V.; Pewin, W.P.; Prausnitz, M.R. Tolerability, usability and acceptability of dissolving microneedle patch administration in human subjects. Biomaterials 2017, 128, 1–7. [Google Scholar] [CrossRef]
- Landry, J.; Chrétien, P.; Bernier, D.; Nicole, L.M.; Marceau, N.; Tanguay, R.M. Thermotolerance and heat shock proteins induced by hyperthermia in rat liver cells. Int. J. Radiat. Oncol. 1982, 8, 59–62. [Google Scholar] [CrossRef]
- Dombrovsky, L.A.; Timchenko, V.; Jackson, M.; Yeoh, G.H. A combined transient thermal model for laser hyperthermia of tumors with embedded gold nanoshells. Int. J. Heat Mass Transf. 2011, 54, 5459–5469. [Google Scholar] [CrossRef]
- Dombrovsky, L.A.; Timchenko, V.; Jackson, M. Indirect heating strategy for laser induced hyperthermia: An advanced thermal model. Int. J. Heat Mass Transf. 2012, 55, 4688–4700. [Google Scholar] [CrossRef]
- Davenport, J.; Manjarrez, J.R.; Peterson, L.; Krumm, B.; Blagg, B.S.J.; Matts, R.L. Gambogic Acid, a Natural Product Inhibitor of Hsp90. J. Nat. Prod. 2011, 74, 1085–1092. [Google Scholar] [CrossRef] [Green Version]
- Ju, Y.; Zhang, H.; Yu, J.; Tong, S.; Tian, N.; Wang, Z.; Wang, X.; Su, X.; Chu, X.; Lin, J.; et al. Monodisperse Au–Fe2C Janus Nanoparticles: An Attractive Multifunctional Material for Triple-Modal Imaging-Guided Tumor Photothermal Therapy. ACS Nano 2017, 11, 9239–9248. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.; Gao, S.; Dai, C.; Chen, Y.; Shi, J. A Two-Dimensional Biodegradable Niobium Carbide (MXene) for Photothermal Tumor Eradication in NIR-I and NIR-II Biowindows. J. Am. Chem. Soc. 2017, 139, 16235–16247. [Google Scholar] [CrossRef] [PubMed]
- Grobmyer, S.R.; Gutwein, L.G.; Singh, A.K.; Hahn, M.A.; Rule, M.C.; Knapik, J.A.; Moudgil, B.M.; Brown, S.C. Fractionated photothermal antitumor therapy with multidye nanoparticles. Int. J. Nanomed. 2012, 7, 351–357. [Google Scholar] [CrossRef] [Green Version]
- Hsiao, C.-W.; Chuang, E.-Y.; Chen, H.-L.; Wan, D.; Korupalli, C.; Liao, Z.-X.; Chiu, Y.-L.; Chia, W.-T.; Lin, K.-J.; Sung, H.-W. Photothermal tumor ablation in mice with repeated therapy sessions using NIR-absorbing micellar hydrogels formed in situ. Biomaterials 2015, 56, 26–35. [Google Scholar] [CrossRef]
- Ren, Y.; Qi, H.; Chen, Q.; Ruan, L. Thermal dosage investigation for optimal temperature distribution in gold nanoparticle enhanced photothermal therapy. Int. J. Heat Mass Transf. 2017, 106, 212–221. [Google Scholar] [CrossRef]
- Simón, M.; Nørregaard, K.; Jørgensen, J.T.; Oddershede, L.B.; Kjaer, A. Fractionated photothermal therapy in a murine tumor model: Comparison with single dose. Int. J. Nanomed. 2019, 14, 5369–5379. [Google Scholar] [CrossRef] [Green Version]
- Hirsch, L.R.; Stafford, R.J.; Bankson, J.A.; Sershen, S.R.; Rivera, B.; Price, R.E.; Hazle, J.D.; Halas, N.J.; West, J.L. Nanoshell-mediated near-infrared thermal therapy of tumors under magnetic resonance guidance. Proc. Natl. Acad. Sci. USA 2003, 100, 13549–13554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Q.; Xu, L.; Liang, C.; Wang, C.; Peng, R.; Liu, Z. Photothermal therapy with immune-adjuvant nanoparticles together with checkpoint blockade for effective cancer immunotherapy. Nat. Commun. 2017, 7, 13193. [Google Scholar] [CrossRef] [PubMed]
- Piao, J.-G.; Gao, F.; Yang, L. Acid-Responsive Therapeutic Polymer for Prolonging Nanoparticle Circulation Lifetime and Destroying Drug-Resistant Tumors. ACS Appl. Mater. Interfaces 2016, 8, 936–944. [Google Scholar] [CrossRef] [PubMed]
- El-Sayed, M.A.; Ali, M.R.K.; Ibrahim, I.M.; Ali, H.R.; Selim, S.A. Treatment of natural mammary gland tumors in canines and felines using gold nanorods-assisted plasmonic photothermal therapy to induce tumor apoptosis. Int. J. Nanomed. 2016, 11, 4849–4863. [Google Scholar] [CrossRef] [Green Version]
- Sato, K.; Sato, N.; Xu, B.; Nakamura, Y.; Nagaya, T.; Choyke, P.L.; Hasegawa, Y.; Kobayashi, H. Spatially selective depletion of tumor-associated regulatory T cells with near-infrared photoimmunotherapy. Sci. Transl. Med. 2016, 8, 352ra110. [Google Scholar] [CrossRef] [Green Version]
- Mooney, R.; Roma, L.; Zhao, D.; Van Haute, D.; Garcia, E.; Kim, S.U.; Annala, A.J.; Aboody, K.S.; Berlin, J.M. Neural Stem Cell-Mediated Intratumoral Delivery of Gold Nanorods Improves Photothermal Therapy. ACS Nano 2014, 8, 12450–12460. [Google Scholar] [CrossRef]
- Gardner, B.; Matousek, P.; Stone, N. Direct monitoring of light mediated hyperthermia induced within mammalian tissues using surface enhanced spatially offset Raman spectroscopy (T-SESORS). Analyst 2019, 144, 3552–3555. [Google Scholar] [CrossRef] [Green Version]
- Bagavathiappan, S.; Lahiri, B.B.; Saravanan, T.; Philip, J.; Jayakumar, T. Infrared thermography for condition monitoring—A review. Infrared Phys. Technol. 2013, 60, 35–55. [Google Scholar] [CrossRef]
- Levick, A.; Land, D.; Hand, J. Validation of microwave radiometry for measuring the internal temperature profile of human tissue. Meas. Sci. Technol. 2011, 22, e065801. [Google Scholar] [CrossRef]
- Feddersen, T.V.; Hernandez-Tamames, J.A.; Franckena, M.; Van Rhoon, G.C.; Paulides, M.M. Clinical Performance and Future Potential of Magnetic Resonance Thermometry in Hyperthermia. Cancers 2021, 13, 31. [Google Scholar] [CrossRef]
- West, C.L.; Doughty, A.C.; Liu, K.; Chen, W.R. Monitoring tissue temperature during photothermal therapy for cancer. J. Bio-X Res. 2019, 2, 159–168. [Google Scholar] [CrossRef] [PubMed]
- Bruggmoser, G.; Bauchowitz, S.; Canters, R.; Crezee, J.; Ehmann, M.; Gellermann, J.; Lamprecht, U.; Lomax, N.; Messmer, M.B.; Ott, O.; et al. Guideline for the clinical application, documentation and analysis of clinical studies for regional deep hyperthermia. Strahlenther. Onkol. 2012, 188, 198–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van der Zee, J.; Peer-Valstar, J.N.; Rietveld, P.J.; de Graaf-Strukowska, L.; van Rhoon, G.C. Practical limitations of interstitial thermometry during deep hyperthermia. Int. J. Radiat. Oncol. Biol. Phys. 1998, 40, 1205–1212. [Google Scholar] [CrossRef]
- Wust, P.; Gellermann, J.; Harder, C.; Tilly, W.; Rau, B.; Dinges, S.; Schlag, P.; Budach, V.; Felix, R. Rationale for using invasive thermometry for regional hyperthermia of pelvic tumors. Int. J. Radiat. Oncol. 1998, 41, 1129–1137. [Google Scholar] [CrossRef]
- Hynynen, K.; McDannold, N.; Mulkern, R.V.; Jolesz, F.A. Temperature monitoring in fat with MRI. Magn. Reson. Med. 2000, 43, 901–904. [Google Scholar] [CrossRef]
- Ghita, A.; Matousek, P.; Stone, N. Sensitivity of Transmission Raman Spectroscopy Signals to Temperature of Biological Tissues. Sci. Rep. 2018, 8, 8379. [Google Scholar] [CrossRef]
- Lanka, P.; Francis, K.J.; Kruit, H.; Farina, A.; Cubeddu, R.; Sekar, S.K.V.; Manohar, S.; Pifferi, A. Optical signatures of radiofrequency ablation in biological tissues. Sci. Rep. 2021, 11, 6579. [Google Scholar] [CrossRef]
- Jaywant, S.M.; Wilson, B.C.; Patterson, M.S.; Lilge, L.D.; Flotte, T.J.; Woolsey, J.; McCulloch, C. Temperature-dependent changes in the optical absorption and scattering spectra of tissues: Correlation with ultrastructure. In Laser-Tissue Interaction IV; SPIE: Bellingham, WA, USA, 1993; pp. 218–229. [Google Scholar] [CrossRef]
- van der Meer, F.J.; Faber, D.J.; Cilesiz, I.F.; van Gemert, M.J.; van Leeuwen, T.G. Temperature-dependent optical properties of individual vascular wall components measured by optical coherence tomography. J. Biomed. Opt. 2006, 11, 041120. [Google Scholar] [CrossRef]
- Huang, B.; Tian, Y.; Li, Z.; Gao, S.; Li, Z. Temperature measurement from the intensity ratio of the Raman-scattering lines in carbon tetrachloride constituting the liquid core of an optical fiber. Instrum. Exp. Tech. 2007, 50, 282–285. [Google Scholar] [CrossRef]
- Mosca, S.; Dey, P.; Salimi, M.; Gardner, B.; Palombo, F.; Stone, N.; Matousek, P. Estimating the Reduced Scattering Coefficient of Turbid Media Using Spatially Offset Raman Spectroscopy. Anal. Chem. 2021, 93, 3386–3392. [Google Scholar] [CrossRef]
- Mosca, S.; Dey, P.; Salimi, M.; Palombo, F.; Stone, N.; Matousek, P. Non-invasive depth determination of inclusion in biological tissues using spatially offset Raman spectroscopy with external calibration. Analyst 2020, 145, 7623–7629. [Google Scholar] [CrossRef] [PubMed]
- Mosca, S.; Dey, P.; Salimi, M.; Gardner, B.; Palombo, F.; Stone, N.; Matousek, P. Spatially Offset Raman Spectroscopy—How Deep? Anal. Chem. 2021, 93, 6755–6762. [Google Scholar] [CrossRef] [PubMed]
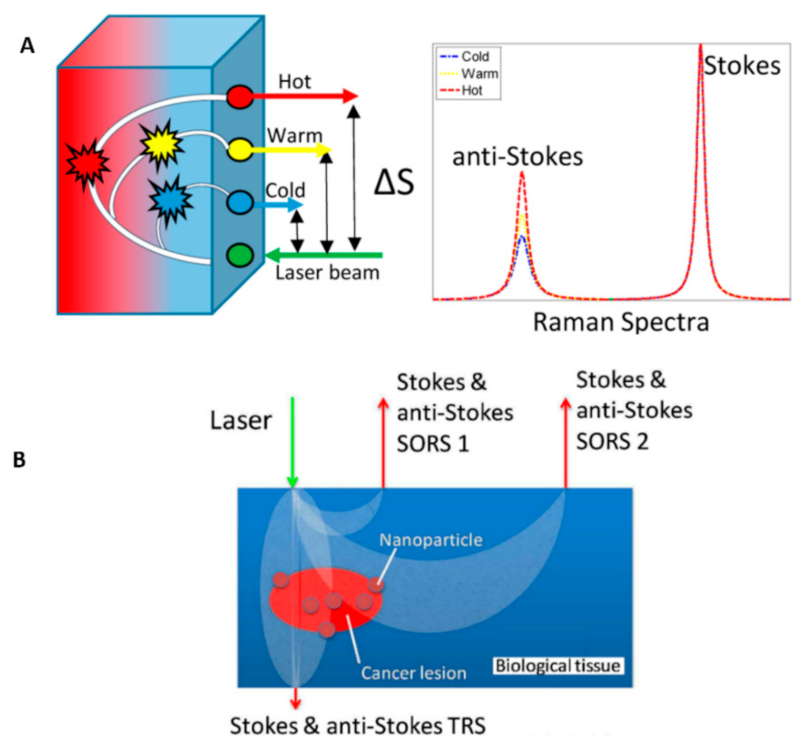
- Gardner, B.; Matousek, P.; Stone, N.; Stone, N. Temperature Spatially Offset Raman Spectroscopy (T-SORS): Subsurface Chemically Specific Measurement of Temperature in Turbid Media Using Anti-Stokes Spatially Offset Raman Spectroscopy. Anal. Chem. 2016, 88, 832–837. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gardner, B.; Stone, N.; Matousek, P. Non-invasive chemically specific measurement of subsurface temperature in biological tissues using surface-enhanced spatially offset Raman spectroscopy. Faraday Discuss. 2016, 187, 329–339. [Google Scholar] [CrossRef]
- Xie, H.; Stevenson, R.; Stone, N.; Hernandez-Santana, A.; Faulds, K.; Graham, D. Tracking Bisphosphonates through a 20 mm Thick Porcine Tissue by Using Surface-Enhanced Spatially Offset Raman Spectroscopy. Angew. Chem. Int. Ed. 2012, 51, 8509–8511. [Google Scholar] [CrossRef]
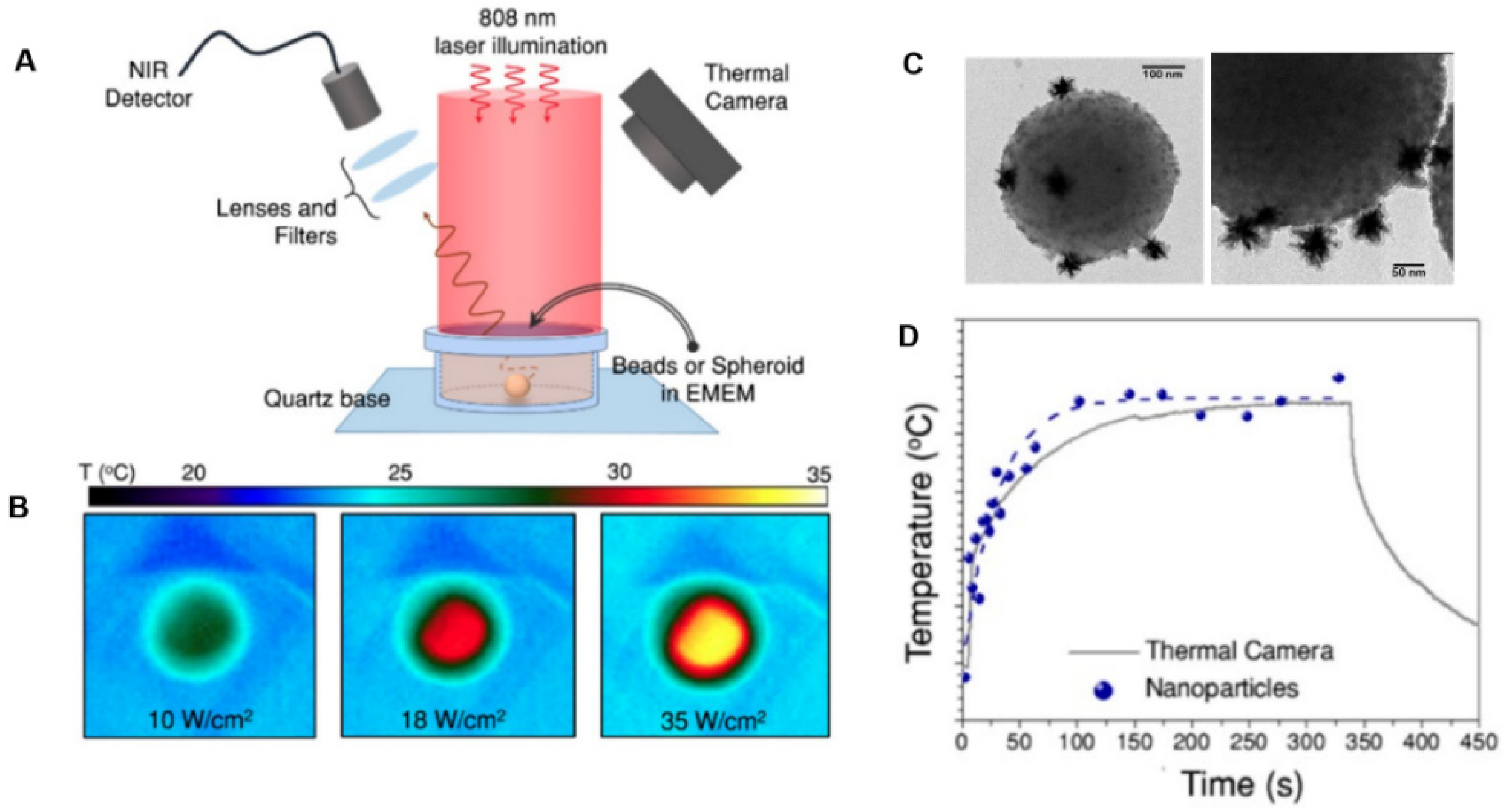
- Quintanilla, M.; García, I.; de Lázaro, I.; García-Alvarez, R.; Henriksen-Lacey, M.; Vranic, S.; Kostarelos, K.; Liz-Marzán, L.M. Thermal monitoring during photothermia: Hybrid probes for simultaneous plasmonic heating and near-infrared optical nanothermometry. Theranostics 2019, 9, 7298–7312. [Google Scholar] [CrossRef]
- Yu, Z.F.; Shi, J.P.; Li, J.L.; Li, P.H.; Zhang, H.W. Luminescence enhancement of CaF2: Nd3+ nanoparticles in the second near-infrared window for in vivo imaging through Y3+ doping. J. Mater. Chem. B 2018, 6, 1238–1243. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Terminology | Definition |
|---|---|
| Pain | A subjective unpleasant sensory and emotional experience associated with actual or potential tissue damage. |
| Noxious stimulus | Stimulus that is damaging to normal tissues and causes pain. |
| Nociceptive stimulus | An actually or potentially tissue-damaging event transduced and encoded by nociceptors. |
| Nociceptor | A receptor preferentially sensitive to a noxious stimulus or a prolonged stimulus that would become noxious. |
| Pain threshold | The minimal intensity of a stimulus that is perceived as painful. |
| Pain tolerance level | The maximum intensity of a stimulus that evokes pain and that a subject is able to tolerate in a given situation. |
| Materials | Size (nm) | Laser Wavelength (nm) | Laser Irradiance (or Power) | Reported Conversion Efficiency (%) | Ref. |
|---|---|---|---|---|---|
| Au nanorods | 5 × 27 | 800 | 2 W/cm2 | 21 | [94] |
| Au nanorods | 10 × 41 | 808 | 1 W/cm2 | 17 | [95] |
| Au nanorods | 13 × 44 | 815 | - | 62 | [96] |
| Au nanorods | 15 × 50 | 980 | 0.51 W/cm2 | 23.7 | [97] |
| Au nanostars | 36 | 808 | 2 mW | 74 | [98] |
| Au nanoshells | 65 | 800 | 2 W/cm2 | 13 | [94] |
| Au nanospheres | 5 | 532 | 228 mW | 80 | [83] |
| 15 | 78 | ||||
| 19 | 73 | ||||
| 40 | 69.4 | ||||
| 50 | 65 | ||||
| Ag@Ag2S core–shell structures | 25 | 635 | 420 mW | 63.7 | [99] |
| 808 | 64.7 | ||||
| 1064 | 79.3 | ||||
| Au-Ag2S hybrid | 88 ± 8 | 809 | 1.72 W | 64 | [92] |
| Au-ZnS hybrid | 160 ± 8 | 809 | 1.72 W | 86 | [92] |
| Au nanopolyhedrons | 3 ± 1 | 809 | 1.72 W | 18 | [92] |
| hollow silicon oxide nanoparticles (H-SiOx NPs) | 150 | 1064 | 0.6 W/cm2 | 48.6 | [100] |
| copper selenide (Cu2xSe) nanocrystals | 16 | 800 | 2 W/cm2 | 22 | [94] |
| Cu9S5 nanocrystals | 13 ×70 | 980 | 0.51 W/cm2 | 25.7 | [97] |
| PEG-coated copper sulfide nanoparticles (CuS) | 7.2 ± 0.7 | 970 | 0.18 W | 71.4 | [101] |
| MoS2 nanoflakes | 50–300 | 808 | 2 W/cm2 | 27 | [102] |
| PEG-coated Ti2C nanoflakes | 41 ± 8 | 808 | - | 87.1 | [103] |
| Ti2O3 nanoparticles | 400 | >760 | 7 kW/cm2 | 82 | [104] |
| hollow Pt nanoframes | 30 | 1120 | 1.2 W | 52.5 | [105] |
| GO | 300–700 | 808 | 200 mW | 4 | [106] |
| 980 | 2 | ||||
| carbon-based NPs | 100 | 1064 | 1.0 W/cm2 | 50.6 | [107] |
| multi-walled carbon nanotubes | 10 × 1500 | 808 | 1 W/cm2 | 53 | [108] |
| semiconducting polymer nanobioconjugates (SPN) | 25 | 808 | 1 W/cm2 | 20–30 | [95] |
| polyaniline nanoparticles (PANPs) | 48.5 ± 1.5 | 808 | 0.5 W/cm2 | 48.5 | [109] |
| Treatment Stage | Actions |
|---|---|
| Before treatment | Checking possible jaundice, fever, and common cold; complete blood count and coagulation (i.e., hematocrit, prothrombin time, partial thromboplastin time) tests |
| During treatment | Monitoring of heart rate, blood pressure, and blood oxygen level; administration of 1% mepivacaine for local anesthesia, diazepam for mild conscious sedation, single dose of antibiotics (usually, 2 g of cefotiam), and opioids (e.g., piritramide and pethidine) intravenously for pain management |
| After treatment (immediately) | Using opioids (e.g., piritramide and pethidine) intravenously for pain, antinausea medication (e.g., metoclopramide), and fluids; continuous monitoring of heart rate; monitoring of blood pressure every 30 min for 6 h |
| After treatment (delayed) | Checking possible fever, jaundice, and shortness of breath after ten days |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salimi, M.; Mosca, S.; Gardner, B.; Palombo, F.; Matousek, P.; Stone, N. Nanoparticle-Mediated Photothermal Therapy Limitation in Clinical Applications Regarding Pain Management. Nanomaterials 2022, 12, 922. https://doi.org/10.3390/nano12060922
Salimi M, Mosca S, Gardner B, Palombo F, Matousek P, Stone N. Nanoparticle-Mediated Photothermal Therapy Limitation in Clinical Applications Regarding Pain Management. Nanomaterials. 2022; 12(6):922. https://doi.org/10.3390/nano12060922
Chicago/Turabian StyleSalimi, Marzieh, Sara Mosca, Benjamin Gardner, Francesca Palombo, Pavel Matousek, and Nicholas Stone. 2022. "Nanoparticle-Mediated Photothermal Therapy Limitation in Clinical Applications Regarding Pain Management" Nanomaterials 12, no. 6: 922. https://doi.org/10.3390/nano12060922