
Application of Approved Cisplatin Derivatives in Combination Therapy against Different Cancer Diseases


1
Department of Pharmaceutical Chemistry, Faculty of Pharmacy, Medical University-Sofia, Dunav Str. 2, 1000 Sofia, Bulgaria
2
Department of Pharmaceutical Chemistry and Pharmacognosy, Faculty of Pharmacy, Medical University-Pleven, Kliment Ohridski Str. 1, 5800 Pleven, Bulgaria
*
Author to whom correspondence should be addressed.
Molecules 2022, 27(8), 2466; https://doi.org/10.3390/molecules27082466
Submission received: 16 March 2022
/
Revised: 7 April 2022
/
Accepted: 8 April 2022
/
Published: 11 April 2022
(This article belongs to the Special Issue Synthesis of Organic Ligands and Their Metal Complexes in Medicinal Chemistry)
Abstract
:The problems with anticancer therapy are resistance and toxicity. From 3000 Cisplatin derivatives tested as antitumor agents, most of them have been rejected, due to toxicity. The aim of current study is the comparison of therapeutic combinations of the currently applied in clinical practice: Cisplatin, Carboplatin, Oxaliplatin, Nedaplatin, Lobaplatin, Heptaplatin, and Satraplatin. The literature data show that the strategies for the development of platinum anticancer agents and bypassing of resistance to Cisplatin derivatives and their toxicity are: combination therapy, Pt IV prodrugs, the targeted nanocarriers. The very important strategy for the improvement of the antitumor effect against different cancers is synergistic combination of Cisplatin derivatives with: (1) anticancer agents—Fluorouracil, Gemcitabine, Cytarabine, Fludarabine, Pemetrexed, Ifosfamide, Irinotecan, Topotecan, Etoposide, Amrubicin, Doxorubicin, Epirubicin, Vinorelbine, Docetaxel, Paclitaxel, Nab-Paclitaxel; (2) modulators of resistant mechanisms; (3) signaling protein inhibitors—Erlotinib; Bortezomib; Everolimus; (4) and immunotherapeutic drugs—Atezolizumab, Avelumab, Bevacizumab, Cemiplimab, Cetuximab, Durvalumab, Erlotinib, Imatinib, Necitumumab, Nimotuzumab, Nivolumab, Onartuzumab, Panitumumab, Pembrolizumab, Rilotumumab, Trastuzumab, Tremelimumab, and Sintilimab. An important approach for overcoming the drug resistance and reduction of toxicity of Cisplatin derivatives is the application of nanocarriers (polymers and liposomes), which provide improved targeted delivery, increased intracellular penetration, selective accumulation in tumor tissue, and enhanced therapeutic efficacy. The advantages of combination therapy are maximum removal of tumor cells in different phases; prevention of resistance; inhibition of the adaptation of tumor cells and their mutations; and reduction of toxicity.
1. Introduction
Malignant cancers include a group of more than 100 different types of diseases, causing mortality worldwide. Carcinogenesis is a transformation of cells into tumors. This multi-stage process consists of initiation, promotion, malignant transformation of cells and progression [1]. During tumorogenesis, various genetic and epigenetic tumor-specific mutations occur, which define the biological features of tumor growth: uncontrolled cell proliferation, invasion of neighboring tissues, and metastasis of cells to distant tissues [2]. Cancer cells are characterized by high mitotic and proliferative activity, have a shorter cell cycle duration and a lower rate of cell death [3]. The main difference between normal and formed in carcinogenesis tumor cells is continuous tumor growth, which cannot be controlled [4]. Highly differentiated cancers have slower growth, metastasize relatively less frequently and later, and are less sensitive to cytostatics. Poorly differentiated cells proliferate rapidly, metastasize to distant organs and are sensitive to cytostatics. At the molecular level, tumors are considered to occur as a result of a DNA-mutations. The main reasons for the transformation of normal cells into malignant ones are: conversion of proto-oncogenes into oncogenes, inactivation of tumor suppressor genes (p53, RAS) and dysregulation of positive and negative signals for proliferation [5,6]. Cancer treatment includes surgical methods, chemotherapy, radiotherapy, targeted therapy and immunotherapy [7]. Most cancer treatments show significant side effects and their effectiveness is affected by various factors, including tumor and drug type, stage of the disease, resistance to the drugs, and the individual characteristics of patients [8].
Platinum complexes are among the most widely used anticancer chemotherapeutics. The electronic configuration determines the use of Pt II and Pt IV compounds as antitumor agents. Upon oxidation, irradiation with light or electron bombardment of Pt II complexes, intermediates are formed, in which the platinum is in the unstable oxidation state (+III) and is stabilized by complexation with suitable ligands. Compared to Pt II and Pt IV, Pt III compounds exhibit in vivo intermediate behavior, in terms of kinetic inertness and thermodynamic stability. Mixed-valence Pt III–Pt II complexes with a polymer structure have high anticancer activity, but the inability in obtaining a precise chain length makes the creation of a drug based on this difficult. Pt III monomer complexes [9,10] and stable octahedral Pt III hematoporphyrin compounds with cytotoxic activity are promising in Cisplatin-resistant tumor cell lines [11].
2. Cisplatin Combinations for Anticancer Therapy
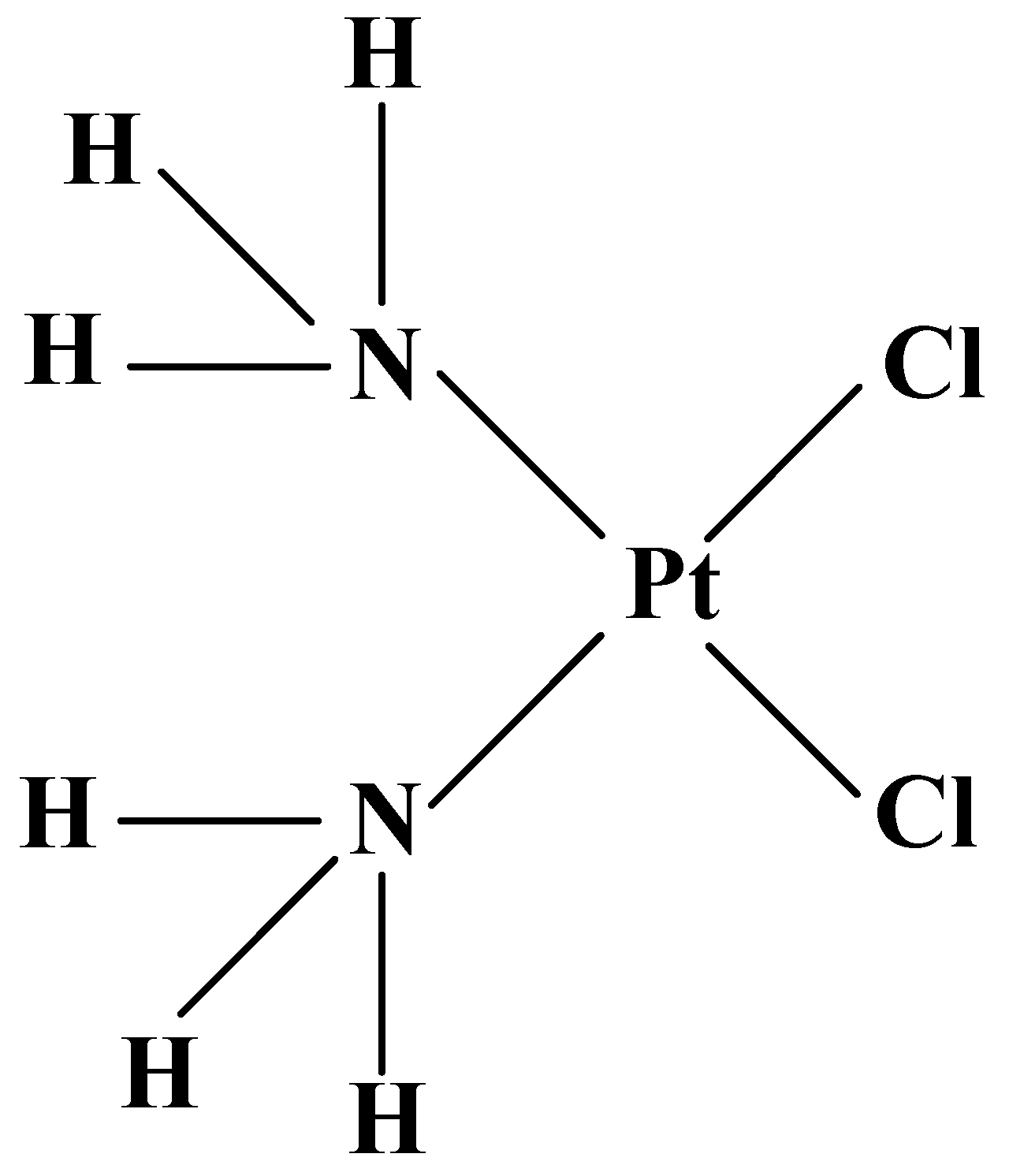
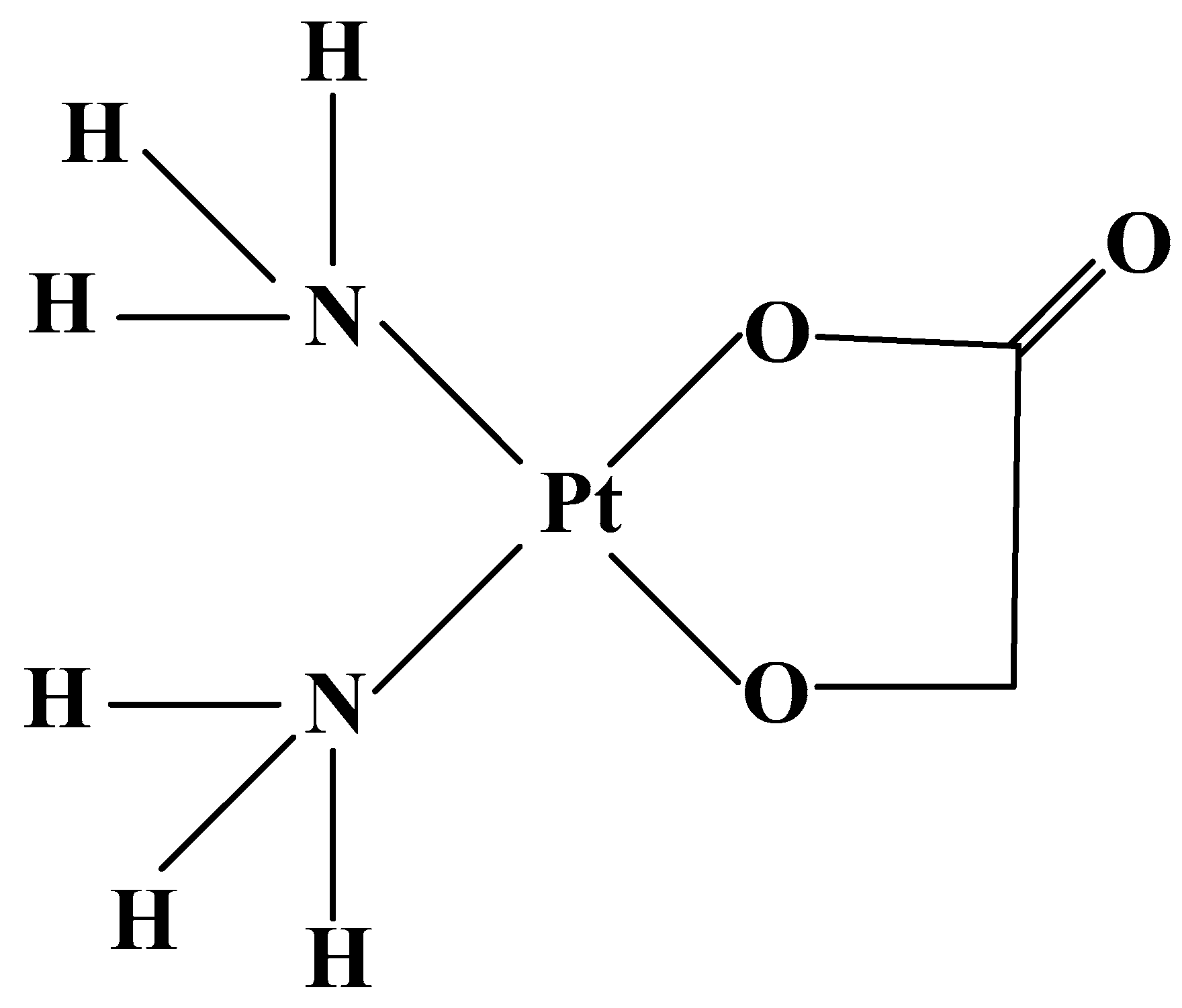
The first platinum-containing coordination complex, applied for treatment of cancer, is Cisplatin (cis-dichlorodiamineplatinum II) (Figure 1).
Cisplatin has been approved from US Food and Drug Administration (FDA) in 1978 for therapy of testicular cancer [12,13]. Cisplatin is the most studied anticancer agent in clinical trials [14,15,16] and is applied as:
- (1)
- a major component for the administration against ovarian carcinoma and testicular teratoma [17];
- (2)
- (3)
- the second cytostatic towards advanced small-cell lung cancer (SCLC) and non-small-cell lung cancer (NSCLC), breast, pancreatic, liver, kidney, and prostate cancer [17], refractory non-Hodgkin’s lymphoma, sarcoma, neuroblastoma, malignant brain multiform glioblastoma, peritoneal and pleural mesothelioma, metastatic melanoma, leukemia [19];
- (4)
- sensitization of tumor cells to radiation therapy for carcinomas of the head, neck, esophagus, lung, and gastric cancer [20].
In combination cancer treatment regimens, greater effectiveness is a result of the synergism of the different molecular mechanisms of drugs. In the therapy of first-line advanced NSCLC, the advantage of schemes is due to the inhibition of DNA-synthetic pathways, involved in the reduction of platinum-DNA adducts. Cisplatin is the most commonly used platinum-containing component in various treatment schedules, due to its synergistic effects with the following drugs: Capecitabine, Docetaxel, Epirubicin, Etoposide, Everolimus, Fluorouracil, Gemcitabine, Irinotecan, Nab-Paclitaxel, Paclitaxel, Vinorelbine, as well as with immunotherapeutic drugs such as Atezolizumab, Cemiplimab, Cetuximab, Durvalumab, Necitumumab, Rilotumumab, Trastuzumab, and with radiation therapy (Table 1).
3. Anticancer Therapy with Approved Cisplatin Derivatives in Combination Regimens
The discovery of the mechanism of action and the main structure–activity dependencies of platinum complexes create opportunities for rational synthesis of new Cisplatin analogs as potential antitumor drugs with reduced resistance and toxicity and a wider spectrum of anticancer activity. The approach to the synthesis of such compounds includes the development of new structures, based on knowledge of the biochemical mechanism of Cisplatin action. The classic structural requirements for the manifestation of antitumor activity, derived on the basis of Cisplatin structure include:
- (1)
- a flat-square Pt II complex
- (2)
- cis-position of the two “leaving” ligands
- (3)
- amino or imino ligands at the other two coordination site
- (4)
- the presence of a NH-functional group in the platinum compounds, which is important for the stability of the formed adducts, due to additional binding via H-bonds
Prospects for the creation of new platinum complexes are various ligands—amines, alkylamines, purines, pyrimidines, hydantoines, carbonyl radicals—which produce compounds with selective cytotoxicity or inhibitory effect on resistant tumors. Modifications of leaving groups (labile, hydrolyzable or exchangeable ligands) in the main classes of platinum complexes, affect the cytotoxic activity, spectrum of action and the toxicological profile of platinum analogs. Suitable ligand systems have been selected, for obtaining effective accumulation in target tissues, reduced side effects, low nephrotoxicity. Strategies for the optimization of the effectivity of antitumor agents include [15]:
- (5)
- Increasing of the therapeutic index towards Cisplatin-resistant ovarian, lung, breast, colon and prostate cancer
- (6)
- Change of the degree of oxidation of the metal ion, for kinetic and thermodynamiccontrol over the binding of the metal complex to DNA bases and ensuring oralbioavailability—Satraplatin.
The development of platinum antitumor agents has been grown exponentially in recent decades. About 3000 derivatives have been synthesized and tested against cancer cells [35]. Only about 30 compounds have shown adequate pharmacological advantages over Cisplatin and have reached clinical trials, but most have been rejected, due to toxic effects [50,51].
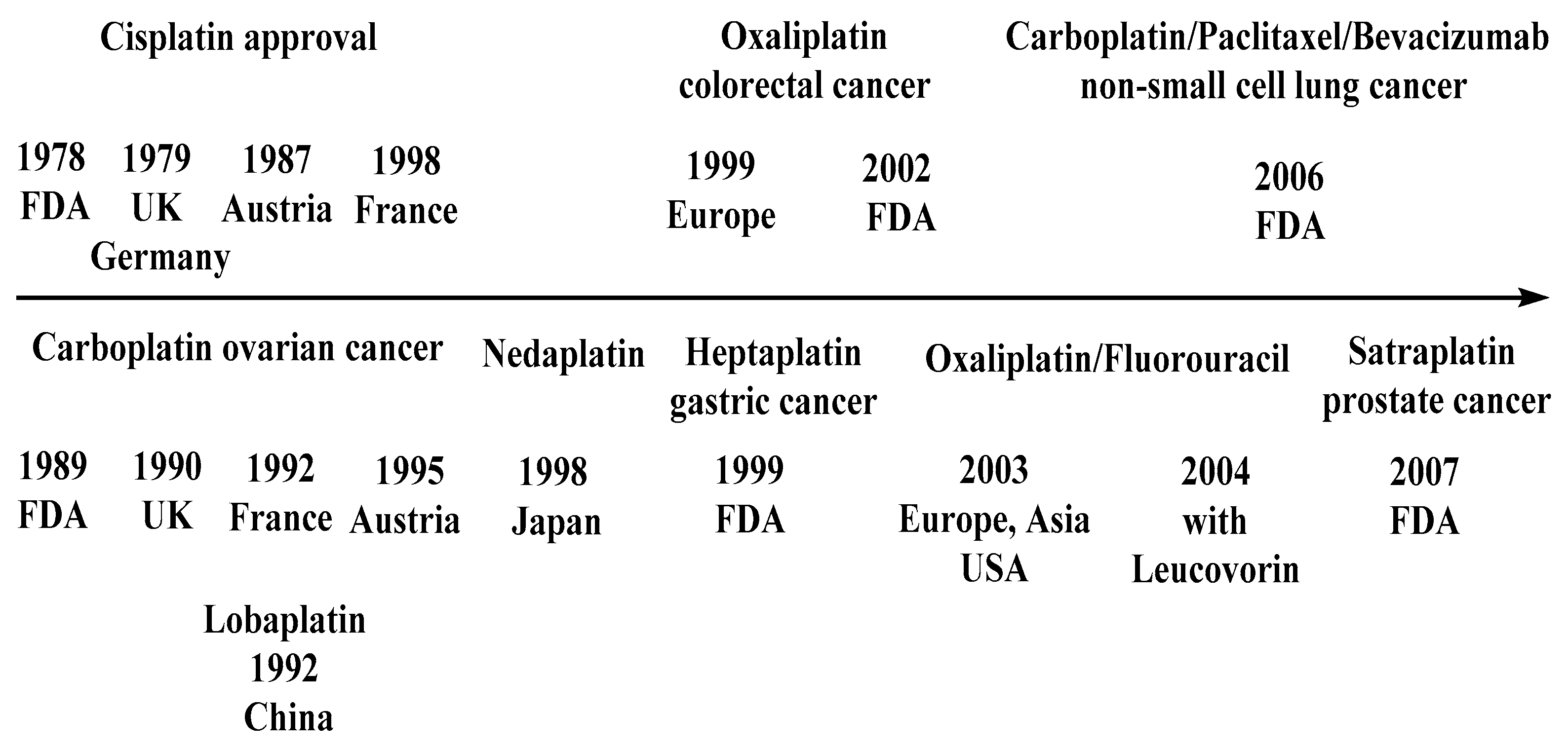
Currently applied in clinical practice worldwide are: Cisplatin and its structural analog of II generation Carboplatin, derivative of III generation Oxaliplatin, Carboplatin derivative of II generation: Nedaplatin in Japan, Oxaliplatin derivatives—III generation: Lobaplatin in China and Heptaplatin in the North Korea. To date, no analog of Cisplatin has been developed that is completely superior to it, in terms of both therapeutic effect and spectrum of action [52].
The regulations for Cisplatin and its derivatives in countries or regions are presented on Figure 2.
3.1. Cisplatin Derivatives: Carboplatin and Oxaliplatin
3.1.1. Carboplatin
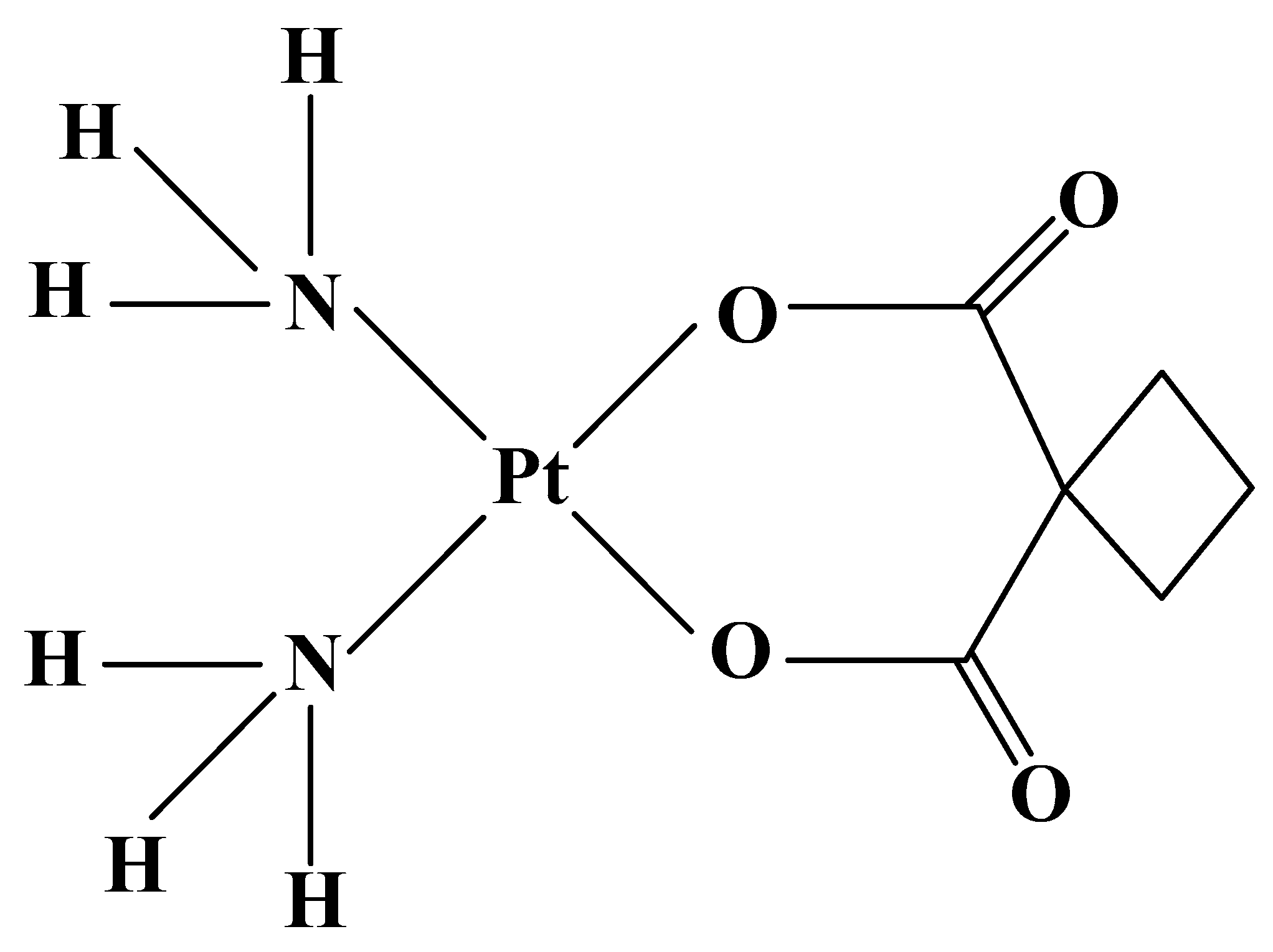
Carboplatin (Paraplatin, JM 8) (Figure 3) is the most successful platinum complex of the second generation with clinical application. In 1989, the drug was approved by the FDA for use in advanced ovarian cancer and has been recommended for treatment of ovarian and testicular carcinomas only in cases, where there are abnormalities in renal function [53]. The compound possess significant activity in sensitizing tumor cells to radiation therapy for brain, head, neck, lung, breast, esophagus, bladder, cervical and salivary gland cancer [54], retinoblastoma, neuroblastoma, and nephroblastoma [14].
For the improvement of the antitumor effect on different types of cancer, combinations of Carboplatin with different drugsare applied: Amrubicin, Capecitabine, Docetaxel, Etoposide, Fludarabine, Fluorouracil, Gemcitabine, Irinotecan, Nab-Paclitaxel, Paclitaxel, Pemetrexed, Topotecan, Vinorelbine and immunotherapeutics Atezolizumab, Avelumab, Bevacizumab, Cetuximab, Durvalumab, Imatinib, Nivolumab, Trastuzumab, and Tremelimumab [55] (Table 2).
Compared to Cisplatin, the side effects of Carboplatin—neuropathy, nephro-, oto- and gastrointestinal toxicity—are less pronounced and more easily overcome, due to the slower hydrolysis of leaving bidentate dicarboxylate ligands, compared to labile chloride ligands of Cisplatin. A limiting side effect of compound is myelosuppression, clinically manifested as severe thrombocytopenia, neutropenia and leukopenia, which requires monitoring of blood parameters or dose reduction [14]. Although the low nephrotoxicity of Carboplatin is an advantage, especially in patients with kidney disease, it is not an alternative to Cisplatin in resistant tumors, due to the presence of cross-resistance [16].
3.1.2. Oxaliplatin
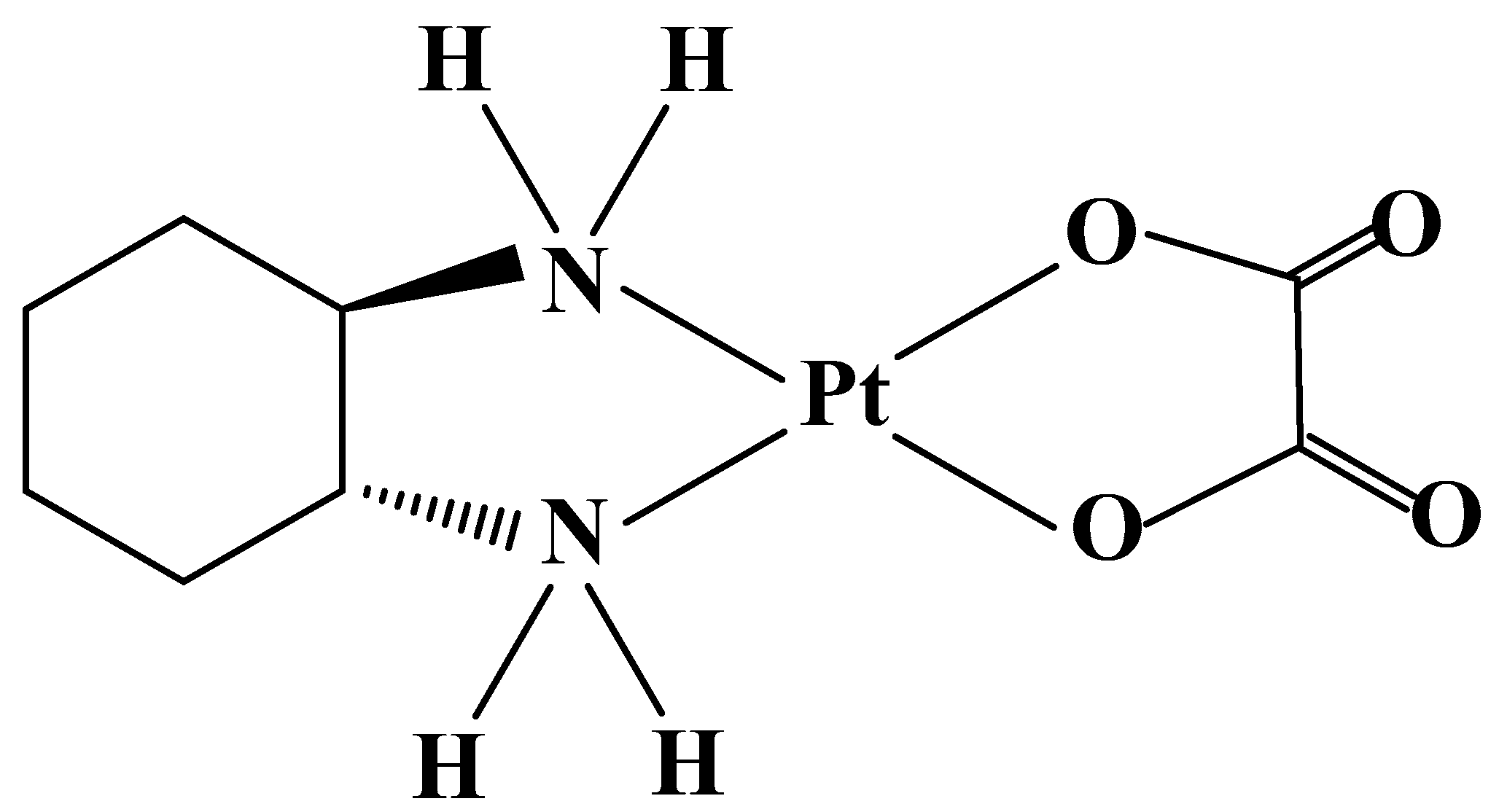
Oxaliplatin (Figure 4) was synthesized in 1970 in Japan from Nagoya University [77]. The drug was approved by the FDA in the United States in 2002. The compound has a higher efficacy than Cisplatin, due to the additional inhibition of protein synthesis, which stops cell division. Oxaliplatin has been used in ovarian and breast cancers, non-Hodgkin’s lymphoma [78], glioblastoma, malignant melanoma, non-small-cell lung cancer [79], head and neck cancer [80], and neuroendocrine tumors [81].
Compared to Cisplatin and Carboplatin, the drug shows stronger activity, and an improved therapeutic index in colorectal tumors. The mechanism for this specificity is related to differences in absorption. The overexpressed in tumor cells transporting membrane proteins: human organic cationic transporters (OCTs) 1 and 2 (SLC22A1 and SLC22A2) are the major determinants of anticancer activity and contribute to antitumor specificity, and significantly increase the accumulation and cytotoxicity in cell lines of Oxaliplatin, but not of Cisplatin or Carboplatin. The compound in regimens with Fluorouracil has been approved in Europe, Asia, Latin America, and later in the United States (2003) for the treatment of metastatic colorectal cancer.
It has been reported that the antitumor efficacy of Oxaliplatin has been improved in schemes with the following drugs: Capecitabine, Cytarabine, Docetaxel, Epirubicin, Fludarabine, Fluorouracil, Irinotecan, Leucovorin, Trifluridine, and immunotherapeutic drugs Atezolizumab, Avelumab, Bevacizumab, Bortezomib, Durvalumab, Nivolumab, Onartuzumab, Panitumumab, Pembrolizumab, Rilotumumab, Sintilimab, Trastuzumab, and Tremelimumab (Table 3).
Oxaliplatin has less pronounced side effects, such as neutropenia, than Cisplatin, and the dose-limiting factors are significant neurotoxicity and tubular necrosis [103]. Neurotoxicity is: (1) initial transient peripheral sensory neuropathy, manifesting as paresthesias and dysesthesia in limbs and muscle contractions of the jaw; (2) long-term neuropathy, manifested by profound sensory loss, sensory ataxia, and functional impairment resulting from the ability to alter the potential of the outer surface membrane [104].
3.2. Carboplatin Derivatives: Nedaplatin
Nedaplatin (Figure 5) gives better results than Cisplatin in preclinical studies, and official indications in Japan are for the treatment of head, neck, esophagus [105], non-small-cell lung [106], cervical, testicular, and prostate cancer [105]. The drug does not demonstrate superiority over Cisplatin and Carboplatin, but shows a significantly better antitumor activity in the resected gynecologic carcinoma compared to Cisplatin. A synergistic effect towards cancer has been proven with drug combinations and with radiation therapy (Table 4) [107].
3.3. Oxaliplatin Derivatives—III Generation: Heptaplatin, Lobaplatin
3.3.1. Heptaplatin
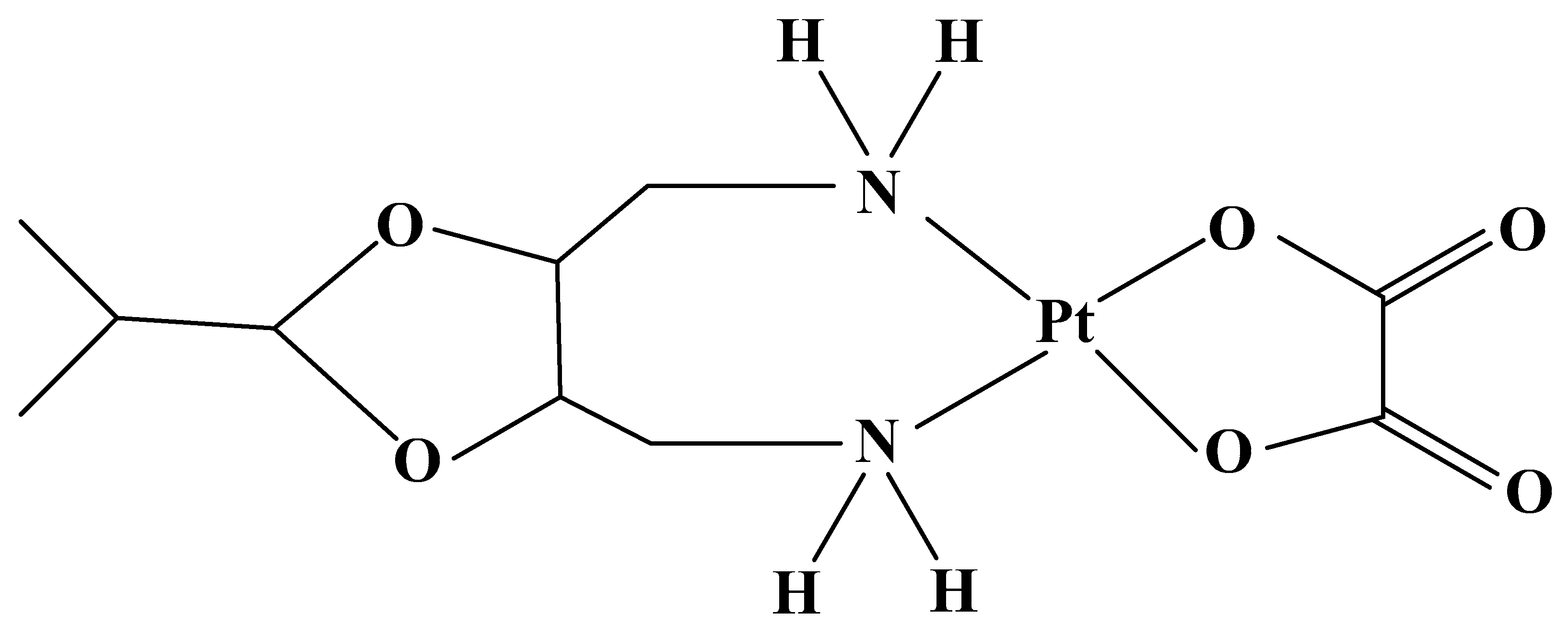
Heptaplatin (Figure 6) has been developed by the Sunkyong Industry Research Center (SK Chemicals, Kyungki-Do) in South Korea under the name SKI 2053 R [138]. The drug was entered in clinical trials in 1990 and was approved by the Korean Food and Drug Administration in 1999 under the name Sun Pla for the treatment of gastric cancer. The compound has greater antitumor activity in Cisplatin-resistant human gastric cell lines [139], and a weaker in vivo effect in small-cell lung cancer. Heptaplatin forms adducts, affecting DNA transcription and replication, and leading to cell death [140]. The drug has been studied in schedules with the following drugs:
Heptaplatin has a lower effect than Cisplatin, but registration is based on its profile of lower nephrotoxicity and less frequent leukopenia, thrombocytopenia, neuro-, hepato-, and embryotoxicity [144].
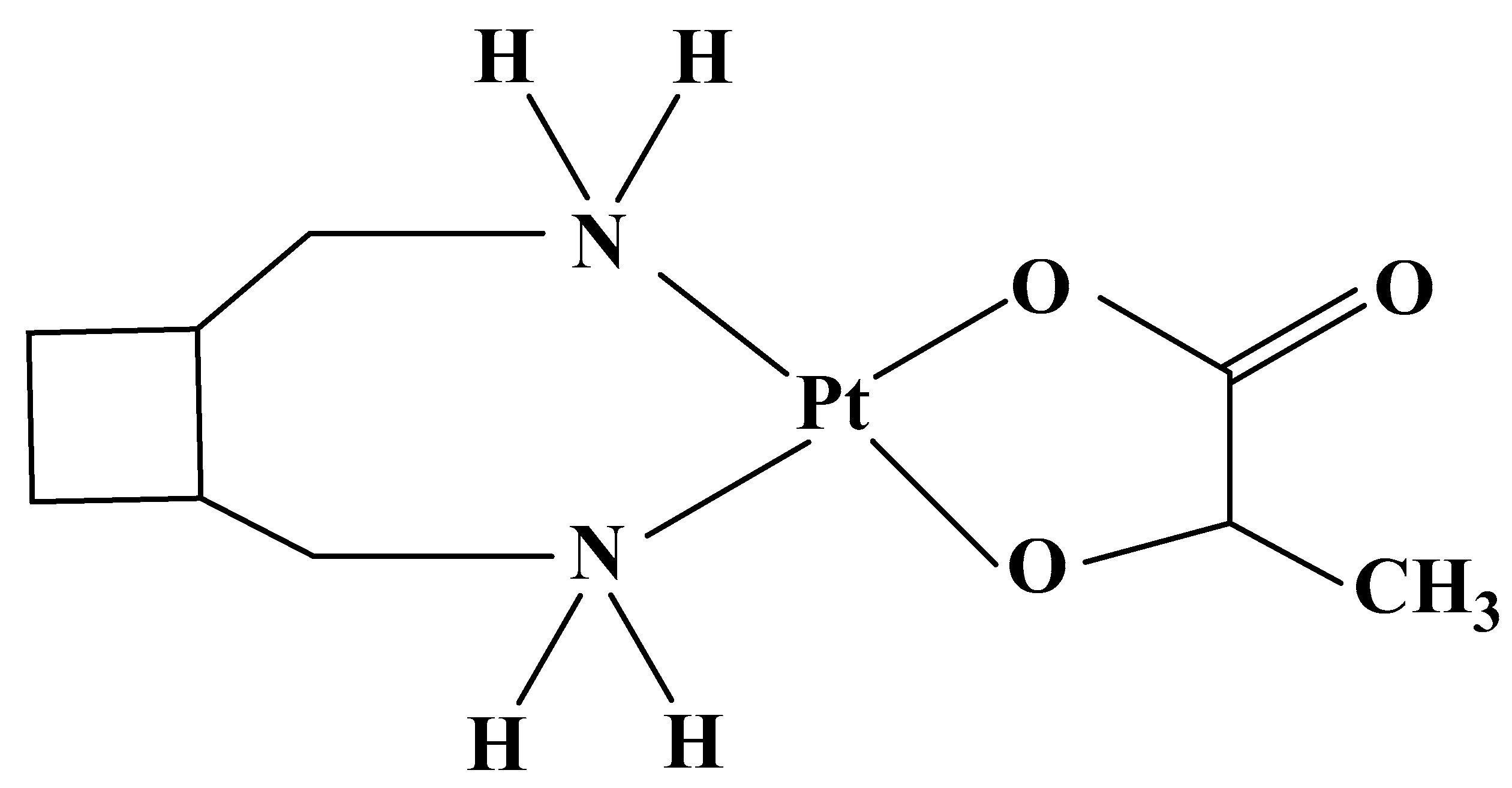
3.3.2. Lobaplatin
Lobaplatin (Figure 7) has been approved in China for the treatment of chronic myelocytic leukemia [145], hypopharyngeal carcinoma [146], esophageal squamous cell carcinoma [147], small-cell lung cancer [148].
The compound shows activity in various preclinical tumor models and has been observed to show potentialfor overcoming the resistance of some tumors to Cisplatin and Carboplatin. A second clinical phase has been completed in Australia, the EU, Brazil, and South Africa in studies of metastatic breast [149] andgastric cancer [150], and osteosarcoma [151]. By forming DNA adducts, the drug is active against Cisplatin- and Carboplatin-resistant tumors [152], and against a lung squamous cell line [153], cholangiocarcinoma cell line RBE [154], cervical cancer cell Line CaSki [155].
For improving the antitumor effect, Lobaplatin has been studied in regimens with the following drugs: Capecitabine, Docetaxel, Etoposide, Fluorouracil, Gemcitabine, Irinotecan, Leucovorin, Paclitaxel, Pemetrexed, and immunotherapeutics Bevacizumab, Temozolomide (Table 5).
Despite in vitro efficacy, in clinical trials in ovarian cancer with recurrence after first-line treatment with Cisplatin, the lower activity than Cisplatin has been reported. The approval of Lobaplatin is based mainly on reduced side effects: no nephro-, neuro-, and ototoxicity. The main side effects are thrombocytopenia, leucopenia, neutropenia, granulocytopenia, and anemia [167].
3.4. Derivatives of Cisplatin—Pt IV Complexes: III generation: Satraplatin
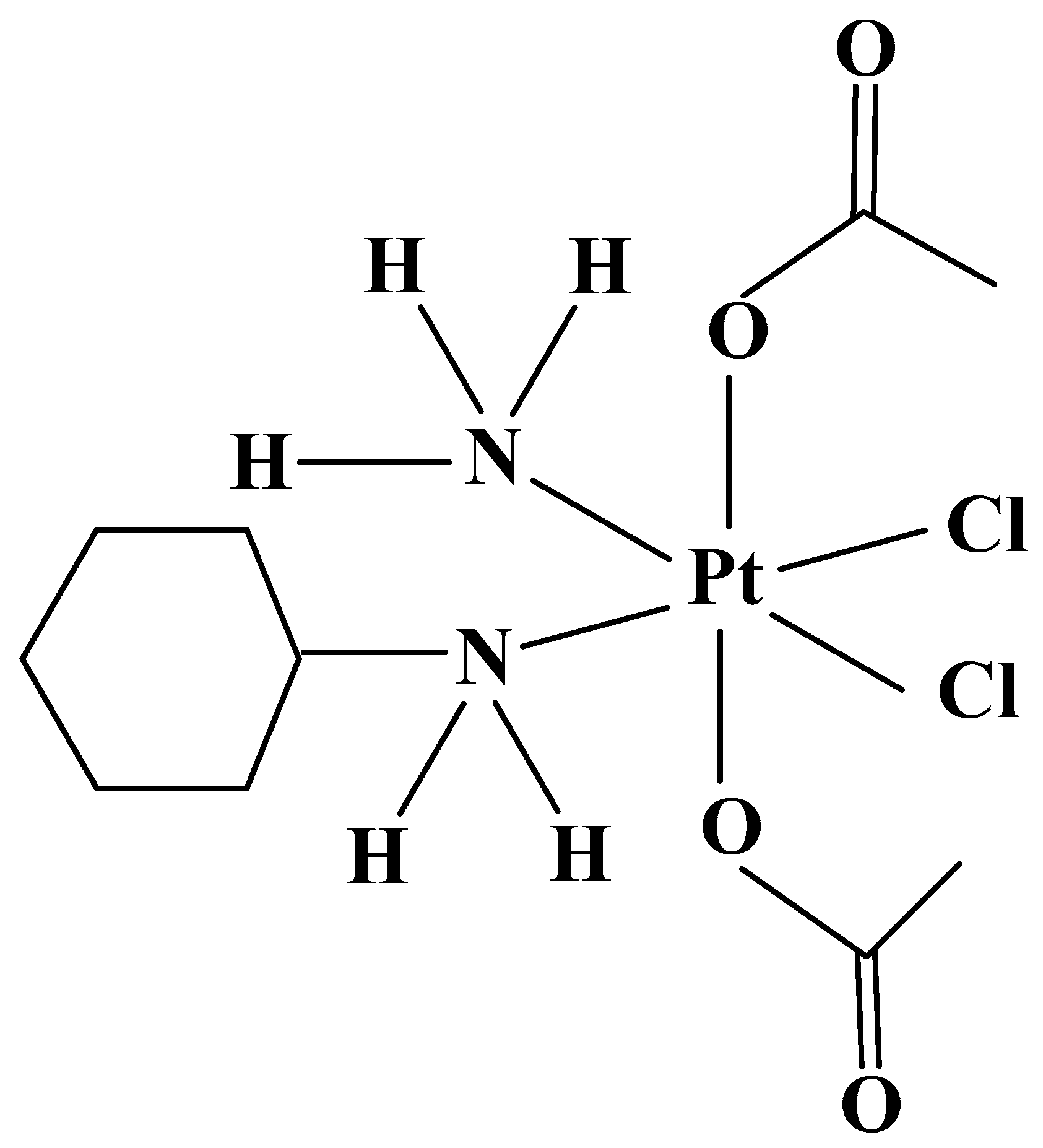
Satraplatin (JM 216) (Figure 8) was developed by the Institute for Cancer Research in London and Johnson Matthey/AnorMed in 1992. The chemical structure differs with Cisplatin with two acetate groups and a cyclohexyl group, which increases lipophilicity and allows oral administration. Unlike the intravenous platinum analogs Cisplatin, Carboplatin, and Oxaliplatin, Satraplatin is the first orally active Pt IV chemotherapeutic drug [168] towards cell lines of cervical, prostate, and ovarian cancer. Satraplatin is not recognized by DNA repair proteins due to various adducts, DNA cannot be replicated and apoptosis occurs. Preclinical in vitro and in vivo studies have shown that the compound has good antitumor activity, comparable to intravenous Cisplatin or Carboplatin in breast, lung, prostate, ovarian [169], and brain cancer [170].
The drug has activity in cancer cells with Cisplatin resistance due to reduced platinum transport. Satraplatin synergistic combinations are with:
Studies with Satraplatin have revealed dose-limiting toxicities similar to those of Carboplatin with observed myelosuppression (thrombocytopenia and neutropenia), but no marked nephro-, neuro-, and ototoxicity have been reported [175].
4. Combination Therapy for Overcoming of Toxicity and Resistance to Cisplatin Derivatives
4.1. Toxicity of Cisplatin Derivatives
The toxicity is problem with chemotherapy with Cisplatin derivatives. Antitumor drugs have no selectivity for tumor cells, but also can kill normal cells with high proliferative activity: cells of the bone-marrow hematopoiesis, and in a gastrointestinal tract. Myelosuppression leads to a risk of infection. Despite its significant therapeutic efficacy, the clinical application of Cisplatin in effective high-dose courses is limited by the manifestation of severe dose-limiting side effects, as a result of an interaction with other biomolecules in the body, and the development of resistance, due to inefficient accumulation in tumor tissue.
In comparison with Cisplatin, the advantages for its derivatives are less pronounced side effects than Cisplatin, as follows [51,176]:
- (1)
- (2)
- (3)
- (4)
- (5)
- (6)
- neutropenia: Oxaliplatin [103].
Dose-limiting effects of approved Cisplatin analogs are presented in Table 6.
4.2. Resistance to Platinum Compounds
Anticancer chemotherapy with Cisplatin analogs is based on inhibition of the growth of the tumor cells, with DNA being the main target molecule, and is associated with growth inhibition of the tumor cells, due to suppression of DNA synthesis and repair as a result from modification of the three-dimensional structure of DNA, induced by metal adducts. The antitumor effect of Pt-containing drugs has been best studied for Cisplatin, which acts as a bifunctional alkylating agent on DNA. Cisplatin preferably binds to the N7 atom of the imidazole ring of the purine base guanine (G) of DNA and with N3 and 4-NH2 of cytosine and N1 and 6-NH2 adenine. Adducts cause disturbances in the structure of DNA: inhibit cellular processes of replication and transcription, cause prolonged G2 phase of cell cycle and lead to programmed cell death (apoptosis) [181]. Due toslower hydrolysis and the stability of carboxylate (Carboplatin) and oxalate (Oxaliplatin) ligands, these drugs bind to DNA more slowly [182].
Similar to Carboplatin, Nedaplatin is a precursor of Cisplatin, due to the formation of intermediate derivatives: monochloro-diamine platinum and dichloro-diamine platinum. The drug has 10 times greater solubility in water than Cisplatin, and is hydrolysed by double hydration to the same active metabolite as with Cisplatin: diaqudiamine-platinum. Nedaplatin binds to guanine in the DNA. In attempts of mismatch repair protein complex for repairing of the DNA by removing of the platinum cross-links, this complex forms single strand breaks and induces apoptosis after the repair attempt has failed. In combination with radiation treatment, the radiosensitizing effect of Nedaplatin is due to the formation of lethal double strand breaks [183]. For Heptaplatin, the platination processes is characterized by the binding to the guanine and adenine bases of DNA, forming the DNA-aducts. The binding of Heptaplatin hydrolytic products to guanine occurs more often in comparison with adenine, due to more favorable hydrogenbonds [184]. In the hydrolysis mechanism of Lobaplatin in aqueous medium under neutral conditions, the ring-opening reaction is found to be the rate limiting. The completely hydrolysed Lobaplatin reacts with the DNA purine base [185].
The problem with the chemotherapy is the resistance, which varies with different tumors: some, such as melanoma, adrenal, and lung tumors are difficult to respond to, and others become resistant during the treatment cycles, especially in cases of suboptimal doses. As a multifactorial process, the platinum drug resistance can occur through different mechanisms: decreased platinum drug uptake, improved drug efflux, intracellular detoxification by glutathione and metallothioneins, enhanced DNA repair, defective apoptosis, and modulation of signaling pathways. The mechanisms of tumor resistance to Cisplatin and its analogs can be summarized as caused by inhibition of platinum binding to DNA and mediated after DNA binding [186].
(A) Resistance, caused by inhibition of platinum binding to DNA is a result of the following:
- (1)
- Insufficient influx and reduced cellular accumulation of Pt-compounds in cells, as a result of reduced transport across the cell membrane, and altered level of expression, localization or activity of multiple transporters, involved in the active transport of antitumor agents. The approach to overcoming of the resistance is the higher lipophilicity, which leads to greater accumulation of Pt-compounds in cells. Due to the interactions of Cisplatin with the copper transporters [187,188]: CTR1 [189,190], CTR2 [191], the overcoming of platinum resistance can be obtained using a copper-lowering agent [192];
- (2)
- Increased efflux of the drug outside the cells.
Platinum drug resistance is dominated by improved extracellular transport through the participation of transporters: ATP7A, ATP7B, MDR1, and pumps for ATP-dependent glutathione S-conjugate: MRP1 (ABCC1), GS-X (MRP2, CMOAT, ABCC2), MRP3 (ABCC3), and MRP5 (ABCC5) [186].
- (3)
- Enhanced system for the detoxification of Pt-compounds, by binding in the cytoplasm to complexes with reducing agents: glutathione, Methionine and metallothioneins, and prevention of the formation of DNA-Pt-adducts.
Dihydroxy-active metabolites have a high affinity for molecules with reducing properties, containing a thiol group: the tripeptide glutathione, Methionine, Cysteine, metallothioneins, and thioredoxin. The most common causes of resistance are high concentrations in the cytoplasm of glutathione and metallothioneins, which through sulfur-containing aminoacids Cysteine and Methionine react with activated aqua compounds to dysfunctional metabolites, reducing the possibility of interaction with DNA and leading to resistance.
(B) Resistance, mediated after DNA binding by the following:
- (1)
- Increased capacity for recognition and removal from specific proteins of DNA-adducts and resynthesis of the damaged areas of DNA molecules;
- (2)
- Modification of gene expression;
- (3)
- Modulation of signaling pathways;
- (4)
- Reduced apoptosis by inhibition of apoptotic genes or activation of anti-apoptotic genes [193];
- (5)
Antitumor treatment may not be effective, due to low sensitivity of malignant cells to drugs or due to the adaptation of the cancer cells to the drug occurring during treatment. The adducts are recognized by cellular signal transduction proteins: p53 [198,199,200,201], p73, amino-terminal kinase JUN (JNK, MAPK8), which control cell growth and differentiation and participate in the repair of the damaged DNA. Cells respond to the structural deformation of DNA, caused by Pt-adducts, through protective and repair mechanisms, that regulate drug accumulation or detoxification, and lead to resistance to Pt-complexes. Cells with improved DNA repair activity are Cisplatin-resistant. The leaving group is important for the spectrum of platinum cytostatics and in the order: Cl-, oxalato-, cyclobutanedicarboxylato-, reduces cross-resistance in Cisplatin-resistant tumors [202].
Resistance in cancer cells might be either intrinsic to the tumors, as has been observed in pancreatic and colorectal carcinoma or might be developed during therapy, as has been for ovarian cancer [203]. p53-controlled apoptotic signaling plays an important role in the response of cancer types to chemotherapeutic drugs. The correlation between the p53 status and response of tumors to platinumanticancer drugs has been indicated. Better Cisplatin effect has been observed in patients with p53 wild-type tumors, and a poor response to the drug has been connected with the inactivation of p53 [204]. In contrast to most human cancers, p53 mutations are rare in testicular tumors, and this lack of p53 mutations is the reason for the better therapeutic response to therapy, due to the sensitivity of testicular tumors against Cisplatin [205]. In contrast, in 50% of colorectal cancers, mutations in the p53 gene have been identified [206] which lead to inactivation of p53, and due to this lack of function of p53 it has been observed that tumors with mutant p53 are more chemotherapy-resistant than those with wild-type p53 [207]. The development of Cisplatin resistance during the first-line treatment arises after prolonged use and causes cancer relapse, and results from alterations in DNA methylation, the inhibition of apoptotic genes, or the activation of antiapoptotic genes. Cisplatin resistance is mainly caused by the disruption of p53-mediated DNA damage. The resistance of pleural mesothelioma cells towards Cisplatin is promoted by the overexpression of inhibitors of apoptosis proteins [208]. The factors contributing to the formation of resistance to Carboplatin are enhanced efflux and reduced uptake of the drug, intracellular detoxification by glutathione, increased DNA repair, and defective apoptotic mechanisms [209].
The major way for the development of the resistance to Cisplatin and to its derivatives, is through a mammalian nucleotide excision repair pathway, which repairs the damaged DNA. A strategy for the reduction of the overall toxicity and resistance is the use of prodrugs, that can be activated locally and, being kinetically more inert than Pt II complexes, are expected to present fewer side effects [202].
The activation of Pt IV complexes is accomplished by reduction to Pt II, which is a necessary condition for achieving antitumor activity [14]. The reduction of Pt IV to Pt II is a necessary condition for achieving antitumor activity, as six-coordinate octahedral Pt IV compounds can minimize unwanted side reactions with biomolecules and are more kinetically inert and less reactive and more resistant to ligand substitution than four-coordinate Pt II [10]. In vitro studies have indicated that Pt IV complexes are characterized by higher efficacy than analogical Pt II complexes. From this class of platinum complexes is the first clinically administered oral drug: Satraplatin [210,211].
In comparison to other platinum anti-cancer drugs, due to the different adducts on the molecule (cyclohexamine), Satraplatin is not recognized by the DNA repair proteins, the DNA remains damaged, and DNA can not be replicated, resistance is solved. By binding to guanine residues, Satraplatin inhibits DNA replication and transcription, which leads to apoptosis [212].
4.3. Combination Therapy
Combination therapy is an important trend in the development of platinum anticancer agents and for bypassing of resistance to Cisplatin derivatives [55]. The need for the development of different cytostatics is a result ofthe data on the kinetics of tumor growth and from the comparative analysis of clinical outcomes in mono- and combination treatment. Today, the monotarget strategy is being replaced by a polytarget one, which achieves greater clinical efficacy in tumors. The administration of multiple anticancer regimens is a major strategy in oncology, and it is important to exploit the synergy between the drugs for a better outcome than monotherapy. The molecular mechanisms of drugs may differ; and their different schemes will combat cancer cells more effectively because they hit two or three different targets.
The development of drug schedules against malignant tumors is based on certaincriteria and principles:
- (1)
- Simultaneous application of drugs with different mechanisms and targets to achieve a more pronounced cytotoxic effect on cancer cells and prevention of resistance, based on clinical observations that tumors resistant to one cytostatic may be sensitive to another type;
- (2)
- Combinations for influencing different phases of the cell cycle, which enhances cytostatic activity by affecting many more cancer cells at different stages of development;
- (3)
- Synergism of action of drugs in regimens on the same signaling pathway for the obtaining of a greater efficacy and more pronounced selectivity to the target, better outcome in more patients, eliminating to a greater extent the risk of rapid development of resistance, and achieving an impact on primary resistant tumor clones;
- (4)
- Schemes of classical cytostatics with monoclonal antibodies for the improvement of the therapeutic response, higher frequency of remissions, and delay of progression.
The data reported in Table 1, Table 2, Table 3, Table 4 and Table 5 show that the more commonly applied therapeutic schedules of Cisplatin derivatives are with the following drugs: DNA alkylators, antimetabolites, topoisomerase inhibitors, steroids, tubuline inhibitors, DNA demethylating agent Decitabine). These are used for overcoming resistance in ovarian cancer, caused by hypermethylation of the MutL homolog-1 (MLH1) gene [213].
The different molecular mechanisms of anticancer drugs give the possibilities for obtaining synergistic effectsbetween drugs in a specific schedule, due to them simultaneously affecting DNA breaks or their associated processes (related proteins, specific genes) as targets for cancer therapy [214]. Combinations provide more effective treatment due to drugs affecting more than one different targets. Other anticancer mechanisms include the affecting of tumour cell membrane receptors and intracellular pathways (Table 7) [215].
The below tables summarize the most common regimens of Cisplatin and its derivatives with antimetabolites (Table 8), DNA topoisomerase inhibitors (Table 9), and tuboline inhibitors (Table 10).
Gimeracil is included in S-1 and is a reversible inhibitor of the liver enzyme dihydropyrimidine dehydrogenase and, due to this, it supresses the degradati on of Fluorouracil into inactive metabolites. Potassium oxonate preferentially localizes in the gut and inhibits the enzyme orotate phosphoribosyl-transferase [223].
The advantage of schemes of Cisplatin derivatives with antimetabolites is the synergistic effect, due to different molecular targets. Capecitabine is a prodrug that is selectively tumor-activated to its cytotoxic derivative Fluorouracil by thymidine phosphorylase, an enzyme found in higher concentrations in many tumors compared to normal tissues or plasma. Within normal and tumor cells, Fluorouracil is further metabolized to active metabolites: 5-fluoro-2′-deoxyuridine 5′-monophosphate and 5-fluorouridine triphosphate, which causes cell injury by the following mechanisms [244]: (1) 5-fluoro-2′-deoxyuridine 5′-monophosphate and the folate cofactor, N5-10-methylenetetrahydrofolate, form a covalently bound ternary complex, by binding to thymidylate synthase, which inhibites the formation of thymidylate from 2′-deaxyuridylate—thymidylate is a necessary precursor of thymidine triphosphate, and by its deficiency suppresses DNA replication and cell division [245]; (2) during the synthesis of RNA, nuclear transcriptional enzymes mistakenly incorporate 5-fluorouridine triphosphate in place of uridine triphosphate, and this metabolic error interferes with RNA processing and protein synthesis [244]. Pemetrexed is recommended in schedules with Carboplatin towards advanced non-small-cell lung cancer. By blocking the formation of precursor purine and pyrimidine nucleotides, the drug prevents the obtaining of DNA and RNA, which are required for the growth and survival of both normal and cancer cells. Pemetrexed disturbs enzymes, used in purine and pyrimidine synthesis: thymidylate synthase, dihydrofolate reductase, and glycinamide ribonucleotide formyltransferase [246].

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 9.
Combinations of Cisplatin and its derivatives with DNA topoisomerase inhibitors.
| DNA Topoisomerase Inhibitors | Cisplatin and Derivatives |
|---|---|
| Cisplatin | |
| Benotecan | small-cell lung cancer [247] |
| Irinotecan | esophageal [216], and penile carcinoma [248] |
| Topotecan | squamous and non-squamous cervix carcinoma [209,222] |
| Etoposide | non-small-cell lung [249], small-cell lung [247], prostate [250], and germ-cell cancer [251] |
| Doxorubicin | endometrial cancer [252] |
| Epirubicin | prostate [250], and germ-cell cancer [253] |
| Carboplatin | |
| Irinotecan | small-cell lung cancer [65], esophageal carcinoma [216] |
| Topotecan | ovarian cancer [231], rhabdomyosarcoma [254] |
| Etoposide | small-cell lung [66], non-small-cell lung [249], and prostate cancer [250], esophageal carcinoma [216] |
| Amrubicin | small-cell lung cancer [65] |
| Doxorubicin | ovarian [231], and endometrial cancer [252] |
| Epirubicin | prostate cancer [250] |
| Nedaplatin | |
| Irinotecan | non-small-cell lung [111], small-cell lung [255], and testicular cancer [209], lung squamous cell [128], neuroendocrine lung [114], and endometrial carcinoma [133] |
| Topotecan | small-cell lung cancer [255] |
| Etoposide | lung carcinoma [114] |
| Lobaplatin | |
| Irinotecan | small-cell lung cancer [159] |
| Etoposide | small-cell lung cancer [158] |
Etoposide forms a ternary complex with DNA and the topoisomerase II enzyme. Topoisomerase II normally forms a double-stranded break in one DNA double-strand, allows another to pass through, and relegates the broken strands. Etoposide’s binding prevents topoisomerase II from re-ligating the broken DNA strands. This results in a double-strand break in the DNA, errors in DNA synthesis, and promotes apoptosis of the cancer cell [256]. The inhibition of topoisomerase by the active metabolite SN-38 of camptothecin derivative Irinotecan leads to the suppression of both DNA replication and transcription [257]. Irinotecan stabilizes topoisomerase 1–DNA covalent complexes, leading to DNA strand breaks and cytotoxic damage in cells and, due to this mechanism, increases the effect of platinum drug/Etoposide [258].
Table 10.
Combinations of Cisplatin derivatives with tuboline inhibitors.
| Tubuline Inhibitors | Cisplatin and Derivatives |
|---|---|
| Cisplatin | |
| Docetaxel | non-small-cell lung [30], and breast cancer [259] |
| Paclitaxel | non-small-cell lung [249], bladder [221], cervical [222], and endometrial cancer [252], esophageal squamous cell carcinoma [31] |
| Vinorebine | non-squamous non-small-cell lung [24], small-cell lung [27], breast [260], and cervicar cancer [222], esophageal squamous cell carcinoma [216] |
| Carboplatin | |
| Docetaxel | non−small-cell lung [249], breast [261], ovarian [227], and prostate cancer [250] |
| Paclitaxel | non-small-cell lung [59,216], gastric [74], breast [262], bladder [221], ovarian [231], endometrial [252], and prostate cancer [263], urotelial [70], and esophageal squamous cell carcinoma [72,216], |
| Nab-Paclitaxel | breast cancer [264] |
| Cabazitaxel | prostate cancer [265] |
| Vinorebine | non-small-cell lung [64], and breast cancer [260] |
| Oxaliplatin | |
| Docetaxel | pancreatic adenocarcinoma [266] |
| Paclitaxel | non-small-cell lung [267], and ovarian cancer [268] |
| Vinorelbine | breast cancer [269] |
| Nedaplatin | |
| Docetaxel | non-small-cell lung [109], and breast cancer [260], squamous cellcarcinomas: oral [209], esophageal [116], and lung [126] |
| Paclitaxel | ovarian [131], cervical [134,135], and testicular cancer [209], esophageal squamous cell carcinoma [120] |
| Nab-Paclitaxel | non-small-cell lung cancer [112] |
| Vinorebine | non-small-cell lung [270], and breast cancer [260] |
| Lobaplatin | |
| Docetaxel | breast cancer [162] |
| Paclitaxel | gastric cancer [166], esophageal carcinoma [166] |
| Vinorelbine | breast cancer [260] |
| Satraplatin | |
| Docetaxel | prostate cancer [173] |
| Paclitaxel | non-small-cell lung cancer [271] |
Tubuline contributes to mitosis, intracellular transport, and cell shape. The taxanes stabilize microtubules and, as a result, disturb the normal microtubule reorganization. The advantages of regimens of Cisplatin derivatives with tubulin inhibitors are in the application of drugs with different mechanisms of action. Docetaxel binds to the microtubules reversibly, leading to their stabilization. Paclitaxel binds to the beta-tubulin subunits of microtubules, and blocks spindle function by inhibition of microtubule dynamics and microtubule detachment from centrosomes. Paclitaxel stabilizes the microtubule polymer and protects it from disassembly. Chromosomes are unable to achieve a metaphase spindle configuration and this suppresses the progression of mitosis and cell division [272]. By binding to the specific sites on tubulin, the vinca alkaloids prevent polymerization of tubulin dimers, and disrupt the formation of microtubules. Vinca alkaloid Vinorelbine suppresses microtubule dynamics, resulting in mitotic block and apoptosis.
The advantages of double-drug schemes with Cisplatin derivatives is the increasing of effectivity and reduction of the dose of combined components. From the summarized data, it is obvious that other very-often-applied schedules are between Cisplatin derivatives and targeted drugs—signaling protein inhibitors and monoclonal antibodies. Specific targets for the development of new drugs are related to the specifics of tumor development, which determine their malignant phenotype: constant signals of continuous tumor growth, avoidance of antiproliferative control, tissue invasion and metastasis, and dysregulation of cellular metabolism. Targeted drugs affect post-genomic-specific targets—intracellular proteins, genes, or enzymes—that are involved in signaling continuous and uncontrolled cell growth, and correct cell dysregulation and genomic instability. Targeted inhibitors help for the achievement of better therapeutic results in malignant tumors that are difficult to treat with other therapies and are more suitable for maintenance therapy than cytostatics. Inhibitors of post-genomic signal transduction suppress proteins, that carry signals for the continuous and uncontrolled growth of cancer cells. They interact with growth protein receptors, containing tyrosine kinase, or with other molecules in the post-genomic signaling pathway. Their effect is in correction and normalization of cell function and contributes to stopping the progression of tumor growth. They are effective only in certain types of tumors with specific expression of the target molecule.
Tyrosine kinase inhibitors are a future direction for overcoming resistance. More than 700 tyrosine kinases, entering the structure of the kinase domain of growth factor receptors, have been identified in cells. These enzymes are important regulators of intracellular signaling pathways because they are involved in cell differentiation, intercellular communication, and phosphorylate tyrosine residues. The enhanced activity of tyrosine kinases and the mitogen-activated transduction protein kinase cascade is due to mutations, which are the main factors for uncontrolled tumor growth. Tyrosine kinase inhibitors interact with the ATP-binding region of the tyrosine kinase domain of growth factor receptors and interfere with the transmission of pathological signals. The proteasome is a complex of intracellular enzymes that break down tumor suppressor proteins in cancer cells, causing cell death, and this leads to the long-term vitality of tumor cells. Proteasome inhibitors stop this process by inhibiting the activity of the 20 S proteasome and tumor suppressor proteins, inducing apoptosis. The more-often-applied therapeutic regimens of Cisplatin derivatives are with the following targeted drugs:
- (1)
- Erlotinib—monotarget tyrosine kinase inhibitor of BCR-ABL-protein receptors encoded by the Bcr-abl abnormal gene: Imatinib and of human epidermal growth factor type 1 EGFR (HER1);
- (2)
- Bortezomib—proteasome inhibitor (apoptosis-inducing drugs);
- (3)
- Everolimus—monotarget inhibitor of mTOR—target of rapamycin in mammals;
- (4)
- Erlotinib—an epidermal growth factor receptor inhibitor and specifically binds reversibly to the adenosine triphosphate binding site of the epidermal growth factor receptor tyrosine kinase, which is highly expressed and occasionally mutated in various forms of cancer [257].
The boron atom in Bortezomib binds the catalytic site of the 26S proteasome with high affinity and specificity. In normal cells, the proteasome regulates protein expression and function by degradation of ubiquitylated proteins. Proteasome inhibition prevents the degradation of pro-apoptotic factors, thereby triggering programmed cell death in neoplastic cells [273].
Preclinical data suggest that platinum may be fully combined with the mammalian target of rapamycin inhibitors, such as Everolimus, which sensitizes cancer cells to Cisplatin by increasing Cisplatin-induced apoptosis.
Monoclonal antibodies are a human variants of large protein molecules of the immune system, that are designed to attack a specific target of a malignant cell. The first antitumor antibodies were directed against lymphoid antigens CD20 and CD52 (Alemtuzumab). Monoclonal antibodies are without much activity as monotherapy, but with an optimal effect in schemes with platinum drugs. The humanized monoclonal antibody Bevacizumab has not marked antitumor efficacy, but in 2006, was approved by the FDA in schedules for application with Carboplatin and Paclitaxel in recurrent or metastatic non-small-cell lung cancer. In advanced breast cancer, Trastuzumab in combination with Cisplatin, Carboplatin and Docetaxel has shown promising clinical activity.
A very important strategy for the improvement of the antitumor effect towards different cancer types is the application of the more effective synergistic regimens of Cisplatin derivatives with immunotherapeutic drugs such as: Atezolizumab, Avelumab, Bevacizumab, Cemiplimab, Cetuximab, Durvalumab, Erlotinib, Imatinib, Necitumumab, Nimotuzumab, Nivolumab, Panitumumab, Pembrolizumab, Rilotumumab, Trastuzumab, Tremelimumab, and Sintilimab [55]. The advantage of the application of Cisplatin derivatives in triples schemes or tetra-schedules is connected with more effective treatment, due to different mechanisms of drugs affecting different tumor targets.
Lung cancer is the most commonly diagnosed cancer (11.6%) and the leading cause of cancer death (18.4%) in both sexes, followed by breast (11.6%), prostate (7.1%), and colorectal cancer (6.1%) for incidence and colorectal (9.2%), stomach (8.2%), and liver cancer (8.2%) for mortality. Lung, breast, and colorectal cancers make upone third of worldwide cancer incidence and mortality and are the respective top three cancers in terms of incidence and within the top fivein terms of mortality: lung (first), colorectal (second), breast (fifth). Among males, lung cancer is the most frequent and the leading cause of death, followed by prostate and colorectal cancer (for incidence) and liver and stomach cancer (for mortality) [274].
Lung cancer is the leading cause of cancer incidence and mortality in men and women internationally and cases have increased two- to four-fold and have been found to be more aggressive in the HIV-infected population. Non-small-cell lung cancer (NSCLC) accounts for approximately 85%–90% of lung cancer diagnoses. Up to1990, squamous cell lung carcinoma was the most common subtype of lung cancers among men. Since 1990, due to genetic and hormonal factors, as well as oncogenic viruses, lung cancer incidences have risen and doubled in women; especially the higher are rates of adenocarcinoma relative to squamous and small-cell lung cancer. This is the reason why adenocarcinoma is the most common subtype of lung cancer in men and women today [275].
4.3.1. Non-Small-Cell Lung Cancer (NSCLC)
For the first-line treatment of advanced NSCLC the most commonly applied double combinations leading to enhanced survival include platinum derivatives with one of the following drugs:
- (1)
- alkylating agents: Ifosfamide, Mitomycin C;
- (2)
- antimetabolites: Fluorouracil, Gemcitabine, Pemetrexed;
- (3)
- inhibitors of topoisomerase I (Irinotecan), and topoisomerase II (Etoposide);
- (4)
- microtubule stabilizers: Docetaxel, Paclitaxel, Nab-Paclitaxel;
- (5)
- inhibitors of microtubule polymerization: Vinblastine, Vinorelbine [209].
Important double regimens for stage III of NSCLC are:
- (1)
- (2)
- (3)
The targeted therapy against stage III NSCLC depends on the type of genetic mutation found during diagnosis. The angiogenesis inhibitor Bevacizumab targets a protein vascular endothelial growth factor (VEGF), which helps new blood vessels grow [249]. In a phase 3 trial for advanced stage III NSCLC, the enhanced effectsof theaddition of the antibody Bevacizumab to Carboplatin/Paclitaxel have been reported [61]. Very promising is simultaneous administration of Nedaplatin/Paclitaxel with Docetaxel [83] or Sintilimab [113].
The following schemes have been approved for both stage III and IV of NSCLC:
- (1)
- (2)
- (3)
- Cisplatin/Gemcitabine/Necitumumab [23].
The most important schedules for stage IV are: Cisplatin/Gemcitabine [234] and Carboplatin/Gemcitabine [57]. Different types of triple and tetra-drug combinations with addition of one or more drugs have been designed:
- (1)
- Cisplatin/Ifosfamide with Etoposide or Vinblastine [278];
- (2)
- Cisplatin/Mitomycin C with Ifosfamide or Vinblastine [276];
- (3)
- (4)
- (5)
- Cisplatin/Docetaxel/Durvalumab [286];
- (6)
- Cisplatin/Vinorelbine/Cetuximab [281];
- (7)
- (8)
- (9)
- (10)
- (11)
- Oxaliplatin/Cytarabin/Docetaxel [83].
- (12)
- Nedaplatin/Paclitaxel/Sintilimab [113].
Non-Squamos Non-Small-Cell Lung Cancer (NS-NSCLC)
As first-line treatment in stage IV for metastatic non-squamous NSCLC, for obtaining an improved effect, is appropriate to adda monoclonal antibody to drug regimens, as follows:
Squamous Non-Small-Cell Lung Cancer (S-NSCLC)
In patients with stage IV squamous NSCLC, the important role of additional drugs has been observed from the results of clinical trial. These drugs include Atezolizumab [297], Ipilimumab [298], Necitumumab [23], Pembrolizumab [299], Tislelizumab [300], Veliparib [301] for the greater anticancer activity of triple schemes in comparison with double schedules, as follows:
4.3.2. Small-Cell Lung Cancer (SCLC)
Cisplatin/Vinorebine is applied both towards NSCLC [24], and SCLC [27]. For therapy of SCLC, the most often applied are:
(A) double combinations:
- (1)
- (2)
(B) triple and multiple regimens:
- (1)
- (2)
- (3)
- Carboplatin/Paclitaxel/Ipilimumab [304].
The effectivity of double scheme Cisplatin/Etoposide is improved by simultaneous application of Irinotecan [25] or Durvalumab [26]. In the first-line treatment of the extensivestage of SCLC, the addition of Atezolizumab [303] to Carboplatin/Etoposide [26,67] increases the survival compared to monotherapy alone [67]. The effect of Carboplatin/Etoposide is improved from Durvalumab [26,66] and the efficacy of Carboplatin/Etoposide/Durvalumab is enhanced by combination with Tremelimumab [66].
For lung adenocarcinoma, the following importantschedules have been developed:
4.3.3. Esophageal Carcinoma
Gastric and esophageal cancer belongs to the most commonly diagnosed malignancies worldwide and are associated with a high disease-related mortality. Approximately 70% of cases of esophageal cancer occur in men [305]. Triple combination Fluorouracil/Leucovorin (Folinic acid): FOLFOX is applied for esophageal [82], gastroesophagealadenocarcinoma [86], and gastric cancer [94].
For the treatment of esophageal carcinoma, the administered double regimens are:
- (1)
- (2)
- (3)
- Oxaliplatin/Capecitabine [72];
- (4)
- (5)
Antiproliferative activity against esophageal squamous cell carcinoma of the following double schemes has beenreported to be enhanced by simultaneous application of a third or fourth drug, as follows [216]:
- (1)
- (2)
- Cisplatin/Paclitaxel/Cetuximab [216];
- (3)
- Carboplatin/Capecitabine with Paclitaxel or Docetaxel [216];
- (4)
- Oxaliplatin/Capecitabine/Epirubicin (EOX) or EOX/Panitumumab [216];
- (5)
- Oxaliplatin/Fluorouracil with Epirubicin (EOF); or Leucovorin (FOLFOX) [84];
- (6)
- (7)
- (8)
- Nedaplatin/Paclitaxel/Nimotuzumab [121].
4.3.4. Gastroesophageal Adenocarcinoma
The most common triple schedule for the therapy of gastroesophageal adenocarcinoma isOxaliplatin/Fluorouracil/Leucovorin (FOLFOX) [86]. The increased effect has been obtained in simultaneousl application of Epirubicin with Cisplatin/Fluorouracil [34]. Docetaxel [33], or Epirubicin [34] with Cisplatin/Capecitabine. The survival of patients is enhanced in addition to Cisplatin/Capecitabine/Epirubicin of Rilotumumab [35], or Matuzumab [307]. Very promising is Carboplatin/Doxetacel/Capecitabine [73] and a triple combination in which Doxetacel [73], Epirubicin [73], or Sintilimab [85] enhance the effectivity of Oxaliplatin/Capecitabine. Targeted therapy drugs may be used towards stage IV adenocarcinoma tumors at the gastroesophageal junction. Trastuzumab is used against HER2-positive tumors in combination with Cisplatin/Capecitabine or Cisplatin/Fluorouracil [308]. Pembrolizumab improves the Oxaliplatin/S-1 therapy [88]. The more effective is Oxaliplatin/Fluorouracil/Leucovorin [86] with the addition of Docetaxel [34,95], or of antibodies Onartuzumab [86], Panitumumab [87], Rilotumumab [87].
4.3.5. Gastric Cancer
Gastric cancer is the fifth most frequently diagnosed cancer and the third leading cause of cancer death, with rates two-fold higher in men than in women [305]. Different double regimens for the therapy of gastric cancer has been introduced in clinical practice:
For the treatment of gastric cancer, the additional drug leads to the improvement of the efficacy of double schemes and the survival of patients. The most commonly applied triple schedules for gastric cancer are:
For an advanced gastric cancer, the reference combination is Cisplatin/Fluorouracil [220]. In a phase III study, it was proved that the addition of Doxetacel or Epirubicin [220], or Epirubicin/Leucovorin is more effective than the reference Cisplatin/Fluorouracil alone. The simultaneous use of Epirubicin increases the therapeutic effect of Cisplatin or Carboplatin with Capecitabine or Fluorouracil [220]. The survival efficacy of Oxaliplatin/Fluorouracil is enhanced from the application of Epirubicin [91], Leucovorin [94], Avelumab [96]. A better effect is obtained from the addition to Oxaliplatin/Capecitabine of Epirubicin [220], Docetaxel [90,91], Sintilimab [85], or Trastuzumab [92]. Promising results are achieved by the addition to Oxaliplatin/(S-1) [97] of Paclitaxel [311,312], Pembrolizumab [88], or Capecitabine/Nivolumab [93] and by the improvement the effect of Oxaliplatin/Fluorouracil by the addition of Leucovorin/Docetaxel [95].
4.3.6. Colon Cancer
For stages II and III of colon cancer, the types of chemotherapy include the following regimens: CAPOX, SOX, FOLFOX:
The anticancer effect of CAPOX is optimized from simultaneous use of Erlotinib orBevacizumab [313]. For stage IV of colon cancer, better results than FOLFOX and FOLFIRI have been obtained from FOLFOXIRI, which is a scheme obtained from the addition of Irinotecan to FOLFOX or of Oxaliplatin to FOLFIRI [232]:
4.3.7. Colorectal Cancer
Colorectal cancer is one of the most common malignant neoplasms, showing, year by year, an increasing tendency in terms of both morbidity and deaths. In terms of incidence in the world and depending on the location, type of cancer, or gender, the disease is the third most commonly occurring cancer in men, the second most commonly occurring cancer in women, and is the second most common cause of death from cancer (9.2%) [314].
The effectivity of Oxaliplatin towards metastatic colorectal cancer is improved from the addition of Capecitabine [233], Capecitabine/Bevacizumab [233], Fluorouracil [234], or human–mouse monoclonal antibody Cetuximab (inhibitor of tumor growth and metastasis) [315]. As first-line therapy, CAPOX [233], SOX [316], (FOLFOX, FLOX), [316,317,318], or FOLFOXIRI [317] are applied. The anticancer effect obtained from FOLFOX is enhanced by simultianeous application with Irinotecan (FOLFOXIRI, FOLFIRINOX) [317], Atezolizumab [99], Bevacizumab [316,317,318], Tremelimumab or Panitumumab [100]. The activity of SOX [316] is improved by Bevacizumab [317]. Anticancer activity of Oxaliplatin/Fluorouracil/Leucovorin/Irinotecan (FOLFOXIRI) is improved by the addition of Bevacizumab [99,317] and Atezolizumab/Bevacizumab [99].
4.3.8. Pancreatic Adenocarcinoma
Pancreatic cancer is one of the leading causes of cancer death worldwide and its global burden has more than doubled over the past 25 years, with the highest incidence in North America, Europe, and Australia [319]. Different chemotherapy schedules in treating of advanced or metastatic pancreatic cancer have been reported:
The combination of Oxaliplatin with Fluorouracil results in higher response rates and longer survival thanwith either Oxaliplatin or Fluorouracil alone. The addition of Irinotecan to Oxaliplatin/Fluorouracil [235] improves outcomes in the treatment of patients and FOLFIRINOX has better short- and long-term efficacy [226].
4.3.9. Ovarian and Endometrial Cancer
Ovarian cancer is the third most-frequent gynecological cancer and ranks fifth among cancer-related deaths in women. Malignant epithelial ovarian neoplasms are most ovarian tumors, the most common malignant ovarian neoplasm and are the eighth leading cause of cancer deaths worldwide, with 5-year survival rates below 45% [321].
For the improvement of the effect, for the first-line therapy of ovarian cancer, simultaneous application of Carboplatin [227], Oxaliplatin [268], or Nedaplatin [131] with Paclitaxel has been accepted as the standard treatment. Tubulin contributes to the mitosis, intracellular transport and cell shape. By binding to the specific sites on tubulin, Paclitaxel stabilizes microtubules, and as a result inhibits the normal microtubule reorganization and increases the effect of platinum drugs. The most common chemotherapy drug regimens against epithelial ovarian cancer are Cisplatin or Carboplatin with one of the following drugs: Cyclophosphamide [322], Gemcitabine, Docetaxel, Paclitaxel, Doxorubicin [227]. The most commondrug schemes for stromal cell ovarian cancer is Carboplatin/Paclitaxel [323]. For germ cell ovarian cancer, Carboplatin/Etoposideis administered [324]. For both stromal cell and germ cell ovarian cancer, Cisplatin/Etoposide/Bleomycin is applied [323,324].
In ovarian cancer, the advantage is the synergism between Cisplatin and nucleoside analog Gemcitabine [209], which increases platinum-DNA adduct formation and suppression of DNA synthesis by incorporation into DNA [209]. The oxazaphosphorine DNA-alkylating agent Cyclophosphamide is a prodrug, metabolized in the liver by CYP450 enzymes to active metabolites, binds to DNA to form interstrand and intrastrand crosslinks with lethal effect for cells. Through this mechanism, Cyclophosphamide improves the effectivity of the platinun drugs. The increased therapeutic effect has been reported with targeted or immunotherapy in addition to a platinum drug such as the following:
The most often adminisitered regimens for the treatment of endometrial cancer inlcude:
4.3.10. Breast and Cervical Cancer
Breast cancer is one of the leading causes cause of cancer in both sexes (11.6%), and occupies the fifth position in terms of mortality. Among females, this disease is the most commonly diagnosed cancer and the leading cause of cancer death, followed by colorectal and lung cancer (for incidence), and vice versa (for mortality). Cervical cancer ranks fourth for both incidence and mortality [274]. Both for breast and cervical cancer, the most often applied are different schemes between platinum agents and antimetabolite Gemcitabine [69,225,228], or with tuboline inhibitors: Paclitaxel [134,135,222,262] and Vinorebine [222,260,269] and the most common equal triple schedules are Carboplatin/Paclitaxel/Bevacizumab [329,330] and Carboplatin/Paclitaxel/Pembrolizumab [330,331] (Table 11).
For breast cancer-specific combinations, the following have been approved (Table 11):
- (1)
- (2)
- (3)
- (4)
- Carboplatin/Docetaxel/Trastuzumab/Pertuzumab [71].
For cervical cancer specific regimens, thereare (Table 11):
4.3.11. Prostate and Germ Cell Cancer
Prostate cancer is the most frequently diagnosed cancer among men in 105 countries of the world, and is the leading cause of cancer death among men in 46 countries. Germ cancer is common in the male population. Different schemes for treatment of prostate cancer have been designed (Table 12), which consist of a platinum drug and:
- (1)
- (2)
- (3)
- (4)
- (5)
- vascular endothelial growth factor receptors inhibitor Bevacizumab [172].
For the treatment of germ cell cancer, the following common schedules have been developed:
- (1)
- (2)
- Cisplatin/Bleomycin/Vincristine with Carboplatin [338];
- (3)
Table 12.
Combinations of Cisplatin derivatives for therapy of prostate and germ cell cancers.
| Prostate Cancer [250] | |
|---|---|
| (1) Cisplatin/Epirubicin [250] (2) Cisplatin/Etoposide [250] (3) Cisplatin/Prednisone [334] (4) Carboplatin/Epirubicin [250] (5) Carboplatin/Etoposide [250] (6) Carboplatin/Cabazitaxel [265] (7) Carboplatin/Docetaxel [250] (8) Carboplatin/Paclitaxel [263] | (9) Oxaliplatin/Fluorouracil [236] (10) Oxaliplatin/Gemcitabine [238] (11) Oxaliplatin/Gemcitabine/Prednisolone [238] (12) Oxaliplatin/Pemetrexed [242] (13) Satraplatin/Gemcitabine [174] (14) Satraplatin/Docetaxel [173] (15) Satraplatin/Prednisone [175] (16) Satraplatin/Bevacizumab [172] |
| Germ Cell Cancers | |
| (1) Csplatin/Epirubicin [253] (2) Cisplatin/Etoposide [251] (3) Cisplatin/Peplomycin/Methotrexate/Etoposide/Vincristine [253] (4) Cisplatin/Cyclophosphamide/Doxorubicin [339] (5) Cisplatin/Cyclophosphamide/Bleomycin/ Dactinomycin/Vinblastine [251] (6) Cisplatin/Ifosfamide/Gemcitabine (GIP) [335] (7) Cisplatin/Ifosfamide/Methotrexate/Paclitaxel (M-TIP) [337] (8) Cisplatin/Ifosfamide/Etoposide (VIP) [253] (9) Cisplatin/Ifosfamide/Paclitaxel [336] (10) Cisplatin/Ifosfamide/Vinblastine (VeIP) [253] (11) Cisplatin/Bleomycin/Vincristine (BOP) [338] | (12) Cisplatin/Bleomycin/Vincristine/Carboplatin [338] (13) Cisplatin/Bleomycin/Etoposide (BEP) [338,339,340] (14) Cisplatin/Bleomycin/Etoposide/Vincristine [253] (15) Cisplatin/Bleomycin/Etoposide/Paclitaxel [341] (16) Carboplatin/Etoposide [253] (17) Carboplatin/Ifosfamide/Etoposide/Paclitaxel) [253] (18) Carboplatin/Gemcitabine/Veliparib [342] (19) Oxaliplatin and gemcitabine [239] (20) Oxaliplatin/Gemcitabine/Paclitaxel [343] (21) Oxaliplatin/Bevacizumab [344] (22) Satraplatin/Gemcitabine [174] |
4.3.12. Bladder Cancer
The administered therapeutic regimens against germ cell cancer are:
4.3.13. Lymphoma, Carcinoma, Sarcoma, Blastoma, Mesothelioma, Melanoma
Other more common types of cancer include:
- (1)
- Lymphomas: non-Hodgkin lymphoma (type: refractory diffuse large B-cell lymphoma); peripheral T-cell lymphoma (type: anaplastic large cell lymphoma);
- (2)
- Carcinomas: conjunctival and oral squamous cell carcinomas; nasopharyngeal, salivary gland, neuroendocrine lung, head and neck, thymic, sarcomatoid, basaloid, mucoepidermoid, papillary, undifferentiated; hepatocellular, cervical. endometrial, urothelial, anal squamous cell, and penile carcinoma;
- (3)
- Sarcomas: osteosarcoma, rhabdomyosarcoma;
- (4)
- Multiple myeloma, mesothelioma;
- (5)
- Blastomas: neuro-, retino-, and hepatoblastoma.
5. Lymphomas
Relapsed or refractory diffuse large B-cell lymphoma (DLBCL) is the most common and aggressive subtype of non-Hodgkin lymphoma, against which the following common treatment schemes have been introduced [346,347] (Table 13):
- (1)
- Cisplatinor Oxaliplatin with Gemcitabine (GEMOX R);
- (2)
- (3)
- (4)
- Carboplatin/Ifosfamide/Etoposide (ICE) [349] with Rituximab (R-ICE), or Dexamethasone (DICE).
The addition to all of these schemes of Rituximab, increases the anticancer effect. Decitabine is a specific DNA methyltransferase inhibitor that exerts antitumor effects by re-expressing tumor suppressor genes. The survival of patients after treatment with Decitabine to Cisplatin/Cytarabine/Dexamethasone (DHAP) is enhanced after the addition of Rituximab to DHAP [346]. Based on in vitro synergism, the combination of Cisplatin/Cytarabine (Ara-C) is the basis of many schedules for patients with aggressive non-Hodgkin lymphoma. It is suggested that the addition of Fludarabine as a potential biochemical modulator and may enhance the activity of Cisplatin/Ara-C [350]. Mitoxantrone increases the activity of DHAP and Cisplatin/Cytarabine/Fludarabine, promising combination is Carboplatin/Docetaxel/Trastuzumab/Pertuzumab (TCH).
The primary systemic type of anaplastic large cell lymphoma (ALCL) is a common subtype of the heterogeneous group of peripheral T-cell lymphomas (PTCL), which is characterized by large pleomorphic cells with strong expression of CD30. A regimens, consisting of the anti-CD30 drug Brentuximab vedotin, and classical lymphoma scheduleDHAP (Cisplatin/Cytarabine/Dexamethasone), show considerable cancer regression [351].
Table 13.
Combinations of Cisplatin derivatives for therapy of lymphomas.
| Non-Hodgkin lymphoma [352] (1) Cisplatin/Gemcitabine/Dexamethasone (GDP) (2) Cisplatin/Gemcitabine/Dexamethasone/Rituximab (R-GDP) (3) Cisplatin/Cytarabine/Fludarabine (4) Cisplatin/Cytarabine/Rituximab [348] (5) Cisplatin/Cytarabine/Dexamethasone (DHAP) [348] (6) Cisplatin/Cytarabine/Dexamethasone (DHAP) [348] with Rituximab (R-DHAP) [348] (7) Cisplatin/Cytarabine/Dexamethasone/Decitabine [346] (8) Cisplatin/Cytarabine/Dexamethasone/Mitoxantrone [352] (9) Cisplatin/Cytarabine/Etoposide/Methylprednisolone (ESHAP) (10) Cisplatin/Cytarabine/Etoposide/Methylprednisolone/Rituximab (R-ESHAP) (11) Cisplatin/Cytarabine/Fludarabine/Mitoxantrone (MIFAP) (12) Carboplatin/Ifosfamide/Etoposide (ICE) [349] (13) Carboplatin/Ifosfamide/Etoposide/Rituximab (R-ICE) (14) Carboplatin/Ifosfamide/Etoposide/Dexamethasone (DICE) (15) Carboplatin/Docetaxel/Trastuzumab/Pertuzumab (16) Oxaliplatin/Gemcitabine (GEMOX R) (17) Oxaliplatin/Gemcitabine/Rituximab |
| Peripheral T-cell lymphoma—type: anaplastic large cell lymphoma (1) Cisplatin/Gemcitabine/Dexamethasone [353] (2) Cisplatin/Gemcitabine/Dexamethasone/Pegaspargase [354] (3) Cisplatin/Cytarabine/Dexamethasone) (DHAP) [353] (4) Cisplatin/Cytarabine/Dexamethasone/Brentuximab vedotin [351] |
| Lymphoepithelioma (1) Nedaplatin/Paclitaxel/Nivolumab [115] |
6. Carcinomas
In a phase III study of advanced head and neck carcinoma, the comparison of Cisplatin/Fluorouracil with Cisplatin/Fluorouracil/Paclitaxel induction chemotherapy shows that the addition of Paclitaxel leads to more beneficial results than the double standard schedule, and inclusion of radiation improves the effect of the triple combination and is the more effective [217]. Improved therapeutic effect is obtained with addition to Cisplatin/Fluorouracil of Docetaxel [355], Paclitaxel [217], Cetuximab [21], Cetuximab/Docetaxel [21], or in addition to Carboplatin/Fluorouracil [56] of Docetaxel [355] or Cetuximab [21]. Nedaplatin regimens with Capecitabine [243], Fluorouracil [123], Gemcitabine [122], or Paclitaxel/S-1 [124] are the most often double schemes for nasopharyngeal carcinoma (Table 14).
Thymic carcinoma is a rare neoplasm that often disseminates or metastasizes. Various histopathological subtypes have been described, which include epidermoid keratinizing and non-keratinizing carcinoma, clear cell carcinoma, lymphoepithelioma-like carcinoma, sarcomatoid, basaloid, mucoepidermoid, and papillary carcinoma. An effective treatment for advanced thymic carcinoma consists of Carboplatin/Paclitaxel [356] or addition to Cisplatin/Doxorubicin of Cyclophosphamide [357], or Etoposide/Vincristine [358].
Liver cancer is the sixth most commonly diagnosed and the fourth leading cause of cancer death worldwide with rates of both incidence and mortality two to three times higher among men in most world regions. Liver cancer ranks fifth in terms of global cases and second in terms of deaths for males.
For cholangiocarcinoma treatment, the most important schedules used are:
The therapeutic effect of Oxaliplatin/Capecitabine against hepatocellular carcinoma is enhanced by the addition of Bevacizumab [367]. For the obtaining of improved results are applied combinations: FOLFOX) [368] alone or with Sorafenib [369] or GEMOX alone [370] or with Sorafenib [371].
As the standard treatment for advanced urothelial carcinoma currently the preferred first-line chemotherapy is Cisplatin/Gemcitabine, due this regimens leads to long-term survival results and is less toxic than the other applied MVAC regimen Cisplatin/Methotrexate/Doxorubicin/Vinblastine [372]. New current data suggests that, for effective and safe control of urothelial carcinoma, thecompensatory scheme of Cisplatin/Gemcitabine/Romidepsin [373].
Towards penile carcinoma very often schedules applied are:
- (1)
- (2)
- Cisplatin/Fluorouracil with Doxetacel or Paxlitacel [374].
Table 14.
Combinations of Cisplatin derivatives for therapy of carcinomas.
| Head and neck squamous cell carcinoma (1) Cisplatin/Fluorouracil [56,217,355] (2) Cisplatin/Fluorouracil/Docetaxel [355] (3) Cisplatin/Fluorouracil/Docetaxel/Cetuximab [21] (4) Cisplatin/Fluorouracil/Paclitaxel [217] (5) Cisplatin/Fluorouracil/Cetuximab [21] (6) Carboplatin/Fluorouracil [56] (7) Carboplatin/Fluorouracil/Docetaxel [355] (8) Carboplatin/Fluorouracil/Cetuximab [21] (9) Carboplatin/Paclitaxel/Cetuximab [21] (10) Nedaplatin/Fluorouracil [209] (11) Nedaplatin/S-1 [108] | Cholangiocarcinoma (biliary-tract cancer) (1) Cisplatin/Fluorouracil/Epirubicin [361] (2) Cisplatin/Capecitabine [40] (3) Cisplatin/Gemcitabine [40,359] (4) Cisplatin/Gemcitabine/S-1 (GCS) [359] (5) Cisplatin/Gemcitabine/Nab-Paclitaxel [360] (6) Oxaliplatin/Capecitabine [362] (7) Oxaliplatin/Fluorouracil/Leucovorin (FOLFOX) [366] (8) Oxaliplatin/Gemcitabine [362,363,364] (9) Oxaliplatin/Gemcitabine/Bevacizumab [365] (10) Oxaliplatin/Gemcitabine/Erlotinib [364] |
| tNasopharyngeal carcinoma (1) Cisplatin/Bleomycin/Methotrexate (BMP) (2) Cisplatin/Fluorouracil [219] (3) Cisplatin/Fluorouracil/Docetaxel [219] (4) Nedaplatin Capecitabine [243] (5) Nedaplatin/Fluorouracil [123] (6) Nedaplatin/Gemcitabine [122] (7) Nedaplatin/Paclitaxel/S-1 [124] (8) Lobaplatin/Fluorouracil [156,157] | Hepatocellularcarcinoma (1) Oxaliplatin/Capecitabine/Bevacizumab [367] (2) Oxaliplatin/Fluorouracil/Leucovorin (FOLFOX) [368] (3) Oxaliplatin/Fluorouracil/Leucovorin/Sorafenib [369] (4) Oxaliplatin/S-1 [102] (5) Oxaliplatin/Gemcitabine (GEMOX) [370] (6) Oxaliplatin/Gemcitabine/Sorafenib [371] (7) Satraplatin/Gemcitabine [174] |
| Thymic carcinoma (1) Cisplatin/Cyclophosphamide/Doxorubicin [357] (2) Cisplatin/Etoposide/Doxorubicin/Vincristine [358] (3) Carboplatin/Paclitaxel [356] Conjunctival squamous cell carcinoma (1) Cisplatin/Fluorouracil [218] Oral squamous cellcarcinoma (1) Nedaplatin/Docetaxel [209] Salivary gland carcinoma (1) Carboplatin/Gemcitabine [54] Neuroendocrine lung carcinoma (1) Nedaplatin/Irinotecan [114] Cutaneous cell carcinoma (1) Cisplatin/Bleomycin (2) Cisplatin/Doxorubicin (3) Cisplatin/Paclitaxel [375] | Urothelial carcinoma (1) Cisplatin/Gemcitabine [229] (2) Cisplatin/Gemcitabine/Everolimus [41] (3) Cisplatin/Gemcitabine/Romidepsin [373] (4) Cisplatin/Methotrexate/Doxorubicin/Vinblastine [372] (5) Carboplatin/Paclitaxel [70] (6) Carboplatin/Paclitaxel/Trastuzumab [76] (7) Nedaplatin/Gemcitabine [129] (8) Nedaplatin/Paclitaxel/Ifosfamide [130] Penilecarcinoma (1) Cisplatin/Ifosfamide/Paclitaxel [374] (2) Cisplatin/Fluorouracil/Doxetael [374] (3) Cisplatin/Fluorouracil/Paxlitacel [374] (4) Cisplatin/Irinotecan [248] (5) Cisplatin/Cemiplimab [44] Anal squamous cell carcinoma (1) Cisplatin/Capecitabine/radiation therapy [42] (2) Cisplatin/Fluorouracil/Docetaxel [43] (3) Cisplatin/Fluorouracil/Docetaxel/Atezolizumab [43] |
7. Sarcoma
The development and prognosis of osteosarcoma are pathological processes, involving multiple genes and factors [376]. For the treatment of osteosarcoma the standard multidrug chemotherapy consists of Cisplatin/Methotrexate/Doxorubicin [377,378], theactivity of which is enhanced in addition of Ifosfamide [379] or Etoposide [378]. Another important regimen is Cisplatin/Ifosfamide/Epirubicin [380].
8. Blastoma
Therapy schemes for pediatric solid tumors have been developed:
- (1)
- Neuroblastoma: Cisplatin/Etoposide/Cyclophosphamide/Doxorubicin/Vincristine;
- (2)
- Retinoblastoma: Carboplatin/Etoposide/Vincristine (VEC);
- (3)
- Hepatoblastoma: Cisplatin/Fluorouracil/Vincristine with or without Doxorubicin [381].
9. Mesothelioma
10. Melanoma
For melanoma therapy, the following schedules are administered:
In different cancers, the optimized effect of mono– and double combinations with radiotherapy have been observed:
- (1)
- Cisplatin/Capecitabine—anal squamous cell carcinoma [42];
- (2)
- Cisplatin/Fluorouracil/Docetaxel—head and neck cancer [217];
- (3)
- Cisplatin/Fluorouracil/Paclitaxel—head and neck cancer [217];
- (4)
- Carboplatin/Gemcitabine; Carboplatin/Vinorelbine—NSCLC [206];
- (5)
- Carboplatin/Irinotecan;
- (6)
- Carboplatin/Fluorouracil/Paclitaxel—esophageal cancer [209];
- (7)
- Nedaplatin—nasopharyngeal carcinoma [125].
Melanoma represents the most aggressive skin cancer [393] and is responsible for most cutaneous malignancy-related deaths. An intracellular enzyme paraoxonase-2 posseses a protective role toward reactive oxygen formation within mitochondrial respiratory chain and could be a novel biomarker for the targeted anticancer therapy against melanoma [394] and bladder cancer [395].
Combinations with encapsulated Cisplatin derivatives are very promising. Nanocarriers provide improved delivery of platinum anticancer drugs, reduced drug influx, improvement of intracellular penetration, increased concentration of platinum drugs in cancer cells. The development of new nanotechnological drug systems for the targeted delivery of cytotoxic drugs and selective accumulation in tumor tissue leads to enhanced cytotoxicity, enhancement of therapeutic efficacy, overcomimg the drug resistance, and reduction of the toxicity of the anticancer agents [396]. Nanocarriers are:
- I.
- II.
- Liposomally encapsulated Oxaliplatin [398].Combinations of Lipoplatin have been investigated with the following drugs:
- (1)
- Gemcitabine in metastatic pancreatic cancer, bladder, neck, head, non-small-cell lung cancer [397], malignant pleural mesothelioma;
- (2)
- Fluorouracil in phase III in squamous cell carcinoma of the head and neck and in advanced gastric cancer [399] with 80% efficiency;
- (3)
- Docetaxel or Navelbine in metastatic breast cancer;
- (4)
- Paclitaxel in non-small-cell lung cancer—the response rate is similar, but nephrotoxicity, neurotoxicity and myelotoxicity are significantly lower. The main dose-limiting toxicity is myelosuppression (neutropenia and thrombocytopenia);
- (5)
- Lipoplatin/Gemcitabine; Lipoplatin/Docetaxel for NSCLC;
- (6)
- Lipoplatin/Docetaxel against metastatic breast cancer;
- (7)
- Lipoplatin/radiation towards head and neck cancers.
SPI-77 is a sterically stabilized liposome Cisplatin, used in osteosarcoma of the head and neck, and with Vinorelbine has been applied against non-small-cell lung cancer, with minimal granulocytopenia and thrombocytopenia, oto-, neuro- and nephrotoxicity. The main toxicity is neutropenia [400].
Combination chemotherapy involves simultaneously treatment with many different drugs, with different mechanisms and side-effects. This fact provides the biggest advantages of combination regiments such as minimizing the resistance development to any one agent and the application at lower doses, which resulted in a reduction of toxicity.
11. Conclusions
The problems with anticancer therapy are resistance and toxicity. The trend for the improvement of the anticancer effect is a synergistic combination of different drug molecular mechanisms. In various treatment regimens, applied platinum agents with radiation or in combination with the following drugs are applied:
- (1)
- Anticancer agents: Fluorouracil, Gemcitabine, Fludarabine, Pemetrexed, Ifosfamide, Irinotecan, Topotecan, Etoposide, Amrubicin, Doxorubicin, Epirubicin, Vinorelbine, Docetaxel, Paclitaxel, and Nab-Paclitaxel;
- (2)
- Modulators of resistant mechanisms;
- (3)
- Signaling protein inhibitors: Erlotinib; Bortezomib; and Everolimus;
- (4)
- Immunotherapeutic drugs: Atezolizumab, Avelumab, Bevacizumab, Cemiplimab, Cetuximab, Durvalumab, Erlotinib, Imatinib, Necitumumab, Nimotuzumab, Nivolumab, Onartuzumab, Panitumumab, Pembrolizumab, Rilotumumab, Trastuzumab, Tremelimumab, and Sintilimab.
The advantages of the reported drug regimens and the rationality of combination therapy at the molecular level are:
- (1)
- Achieving the maximum possible removal of tumor cells within the permissible toxicity;
- (2)
- Affecting the cells located in different phases of the cell cycle;
- (3)
- Realization of prevention or delay of the development of resistant cell branches;
- (4)
- Slowing the process of adaptation of tumor cells and delay of cell mutations, due to using more drugs that have different molecular targets;
- (5)
- Reduction of dose of combined components with one and the same dose-limiting effects;
- (6)
- Schemes with components with different toxicity to normal tissues, allowing the application of optimal doses of each drug in the absence of superimposition of toxic effects on an organ or cell system.
An important approach for overcoming the drug resistance and for the reduction of toxicityis the combibation therapy of liposomally encapsulated Cisplatin and Oxaliplatinwith other anticancer agents, which provide improved targeted delivery, improved intracellular penetration, selective accumulation in tumor tissue, and enhanced therapeutic efficacy.
Author Contributions
Conceptualization, D.T., S.I.; writing—original draft preparation, D.T.; drawing figures—D.T.; summarizing information in tables and tables formatting—D.T.; references formating, D.T.; writing abstract and conclusion—D.T., S.I.; writing—editing, D.T., S.I. writing—final review, D.T., S.I. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Blagosklonny, M. Carcinogenesis, cancer therapy and chemoprevention. Cell Death Differ. 2005, 12, 592–602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Brien, R.M.; Cannon, A.; Reynolds, J.V.; Lysaght, J.; Lynam-Lennon, N. Complement in tumourigenesis and the response to cancer therapy. Cancers 2021, 13, 1209. [Google Scholar] [CrossRef] [PubMed]
- Hanahan, D.; Weinberg, R.A. The hallmarks of cancer. Cell 2000, 100, 57–70. [Google Scholar] [CrossRef] [Green Version]
- Hickman, J.A. Apoptosis and tumourigenesis. Curr. Opin. Genet. Dev. 2002, 12, 67–72. [Google Scholar] [CrossRef]
- Liu, J.; Zhang, C.; Hu, W.; Feng, Z. Tumor suppressor p53 and metabolism. J. Mol. Cell Biol. 2019, 11, 284–292. [Google Scholar] [CrossRef] [Green Version]
- D’Orazi, G.; Cirone, M. Mutant p53 and cellular stress pathways: A criminal alliance that promotes cancer progression. Cancers 2019, 11, 614. [Google Scholar] [CrossRef] [Green Version]
- Wyld, L.; Audisio, R.A.; Poston, G.J. The evolution of cancer surgery and future perspectives. Nat. Rev. Clin. Oncol. 2015, 12, 115–124. [Google Scholar] [CrossRef]
- Caley, A.; Jones, R. The principles of cancer treatment by chemotherapy. Surgery 2012, 30, 186–190. [Google Scholar] [CrossRef]
- Momekov, G.; Momekova, D. Recent developments in antitumor platinum coordination compounds. Expert Opin. Ther. Pat. 2006, 16, 1383–1403. [Google Scholar] [CrossRef]
- Momekov, G.; Bakalova, A.; Karaivanova, M. Novel approaches towards development of non-classical platinum-based antineoplastic agents: Design of platinum complexes characterized by an alternative DNA-binding pattern and/or tumor-targeted cytotoxicity. Curr. Med. Chem. 2005, 12, 2177–2191. [Google Scholar] [CrossRef]
- Momekov, G.; Karaivanova, M.; Ugrinova, I.; Pasheva, E.; Gencheva, G.; Tsekova, D.; Arpadjan, S.; Bontchev, P. In vitro pharmacological study of monomeric platinum (III) hematoporphyrin IX complexes. Investig. New Drugs 2010, 29, 742–751. [Google Scholar] [CrossRef] [PubMed]
- Kostova, I. Platinum complexes as anticancer agents. Recent Pat. Anti-Cancer Drug Discov. 2006, 1, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, B.; Van Camp, L.; Trosko, J.E.; Mansour, V.H. Platimum compounds: A new class of potent antitumour agents. Nature 1969, 222, 385–386. [Google Scholar] [CrossRef] [PubMed]
- Johnstone, T.C.; Suntharalingam, K.; Lippard, S.J. The next generation of platinum drugs: Targeted Pt (II) agents, nanoparticle delivery, and Pt (IV) prodrugs. Chem. Rev. 2016, 116, 3436–3486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krishant, M.D.; Ang, D.L.; McGhie, B.; Rajamanickam, A.; Dhiman, A.; Khoury, A.; Holland, J.; Bjelosevic, A.; Pages, B.; Gordon, C.; et al. Platinum coordination compounds with potent anticancer activity. Coord. Chem. Rev. 2018, 375, 148–163. [Google Scholar]
- Zhou, J.; Kang, Y.; Chen, L.; Wang, H.; Liu, J.; Zeng, S.; Yu, L. The drug-resistance mechanisms of five platinum-based antitumor agents. Front. Pharmacol. 2020, 11, 343. [Google Scholar] [CrossRef] [Green Version]
- Aldossary, S.A. Review on pharmacology of Cisplatin: Clinical use, toxicity and mechanism of resistance of Cisplatin. Biomed. Pharmacol. J. 2019, 12, 7–15. [Google Scholar] [CrossRef]
- Martens-de Kemp, S.R.; Brink, A.; Van der Meulen, I.H.; de Menezes, R.X.; Te Beest, D.E.; Leemans, C.R.; Van Beusechem, V.W.; Braakhuis, B.J.M.; Brakenhoff, R.H. The FA/BRCA pathway identified as the major predictor of Cisplatin response in head and neck cancer by functional genomics. Mol. Cancer Ther. 2017, 16, 540–550. [Google Scholar] [CrossRef] [Green Version]
- Tchounwou, P.B.; Dasari, S.; Noubissi, F.K.; Ray, P.; Kumar, S. Advances in our understanding of the molecular mechanisms of action of Cisplatin in cancer therapy. J. Exp. Pharmacol. 2021, 13, 303–328. [Google Scholar] [CrossRef]
- Ghosh, S. Cisplatin: The first metal based anticancer drug. Bioorg. Chem. 2019, 88, 102925. [Google Scholar] [CrossRef]
- Haddad, R.I.; Massarelli, E.; Lee, J.J.; Lin, H.Y.; Hutcheson, K.; Lewis, J.; Garden, A.S.; Blumenschein, G.R.; William, W.N.; Pharaon, R.R.; et al. Weekly Paclitaxel, Carboplatin, Cetuximab, and Cetuximab, Docetaxel, Cisplatin, and Fluorouracil, followed by local therapy in previously untreated, locally advanced head and neck squamous cell carcinoma. Ann. Oncol. 2019, 30, 471–477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ikeda, S.; Yoshioka, H.; Kaneda, T.; Yokoyama, T.; Niwa, T.; Sone, N.; Ishida, T.; Morita, M.; Tomioka, H.; Komaki, C.; et al. A phase II study of Cisplatin plus Gemcitabine followed by maintenance Gemcitabine for advanced squamous non-small-cell lung cancer: Kyoto Thoracic Oncology Research Group 1302. Oncology 2019, 97, 327–333. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, S.; Yoshioka, H.; Sakai, H.; Hotta, K.; Takenoyama, M.; Yamada, K.; Sugawara, S.; Takiguchi, Y.; Hosomi, Y.; Tomii, K.; et al. Necitumumab plus Gemcitabine and Cisplatin versus Gemcitabine and Cisplatin alone as first-line treatment for stage IV squamous non-small cell lung cancer: A phase 1b and randomized, open-label, multicenter, phase 2 trial in Japan. Lung Cancer 2019, 129, 55–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bennouna, J.; Havel, L.; Krzakowski, M.; Kollmeier, J.; Gervais, R.; Dansin, E.; Serke, M.; Favaretto, A.; Szczesna, A.; Cobo, M.; et al. Oral Vinorelbine plus Cisplatin as first-line chemotherapy in nonsquamous non–small-cell lung cancer: Final results of an international randomized phase II study (NAVotrial 01). Clin. Lung Cancer 2014, 15, 258–265. [Google Scholar] [CrossRef]
- Goto, K.; Ohe, Y.; Shibata, T.; Seto, T.; Takahashi, T.; Nakagawa, K.; Tanaka, H.; Takeda, K.; Nishio, M.; Mori, K.; et al. Combined chemotherapy with Cisplatin, Etoposide, and Irinotecan versus Topotecan alone as second-line treatment for patients with sensitive relapsed small-cell lung cancer (JCOG0605): A multicentre, open-label, randomised phase 3 trial. Lancet Oncol. 2016, 17, 1147–1157. [Google Scholar] [CrossRef]
- Mathieu, L.; Shah, S.; Pai-Scherf, L.; Larkins, E.; Vallejo, J.; Li, X.; Rodriguez, L.; Mishra-Kalyani, P.; Goldberg, K.B.; Kluetz, P.G.; et al. FDA approval summary: Atezolizumab and Durvalumab in combination with platinum-based chemotherapy in extensive stage small cell lung cancer. Oncologist 2021, 26, 433–438. [Google Scholar] [CrossRef]
- Drąg-Zalesińska, M.; Saczko, J.; Choromańska, A.; Szewczyk, A.; Rembialkowska, N.; Kulbacka, J.; Rzechonek, A. Cisplatin and Vinorelbine-mediated electrochemotherapeutic approach against multidrug resistant small cell lung cancer (H69AR) in vitro. Anticancer Res. 2019, 39, 3711–3718. [Google Scholar] [CrossRef]
- Li, Q.; Li, Q.; Zhang, P.; Yuan, P.; Wang, J.; Ma, F.; Luo, Y.; Fan, Y.; Cai, R.; Xu, B. A phase II study of Capecitabine plus Cisplatin in metastatic triple-negative breast cancer patients pretreated with anthracyclines and taxanes. Cancer Biol. Ther. 2015, 16, 1746–1753. [Google Scholar] [CrossRef] [Green Version]
- Baselga, J.; Gómez, P.; Greil, R.; Braga, S.; Climent, M.A.; Wardley, A.M.; Kaufman, B.; Stemmer, S.M.; Pêgo, A.; Chan, A.; et al. Randomized phase II study of the anti-epidermal growth factor receptor monocloncal antibody Cetuximab with Cisplatin versus Cisplatin in patients with metastatic triple-negative breast cancer. J. Clin. Oncol. 2013, 31, 2586–2592. [Google Scholar] [CrossRef]
- Zhao, T.; Chen, H.; Zhang, T. Docetaxel and Cisplatin concurrent with radiotherapy versus 5-Fluorouracil and Cisplatin concurrent with radiotherapy in treatment for locally advanced oesophageal squamous cell carcinoma: A randomized clinical study. Med. Oncol. 2012, 29, 3017–3023. [Google Scholar] [CrossRef]
- Zhu, H.T.; Ai, D.S.; Tang, H.R.; Badakhshi, H.; Fan, J.H.; Deng, J.Y.; Zhang, J.H.; Chen, Y.; Zhang, Z.; Xia, Y.; et al. Long-term results of Paclitaxel plus Cisplatin with concurrent radiotherapy for loco-regional esophageal squamous cell carcinoma. World J. Gastroenterol. 2017, 23, 540–546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, H.; Shin, S.K.; Cho, B.C.; Lee, C.G.; Kim, C.B.; Kim, D.J.; Lee, J.G.; Hur, J.; Lee, C.Y.; Bae, M.K.; et al. A prospective phase II trial of S-1 and Cisplatin-based chemoradiotherapy for locoregionally advanced esophageal cancer. Cancer Chemother. Pharmacol. 2014, 73, 665–671. [Google Scholar] [CrossRef]
- Thuss-Patience, P.C.; Hofheinz, R.D.; Arnold, D.; Florschütz, A.; Daum, S.; Kretzschmar, A.; Mantovani-Löffler, L.; Bichev, D.; Breithaupt, K.; Kneba, M.; et al. Perioperative chemotherapy with Docetaxel, Cisplatin and Capecitabine (DCX) in gastro-oesophageal adenocarcinoma: A phase II study of the Arbeitsgemeinschaft Internistische Onkologie (AIO). Ann. Oncol. 2012, 23, 2827–2834. [Google Scholar] [CrossRef] [PubMed]
- Al-Batran, S.E.; Homann, N.; Pauligk, C.; Goetze, T.O.; Meiler, J.; Kasper, S.; Kopp, H.G.; Mayer, F.; Haag, G.M.; Luley, K.; et al. Perioperative chemotherapy with Fluorouracil plus Leucovorin, Oxaliplatin, and Docetaxel versus Fluorouracil or Capecitabine plus Cisplatin and Epirubicin for locally advanced, resectable gastric or gastro-oesophageal junction adenocarcinoma (FLOT4): A randomised, phase 2/3 trial. Lancet 2019, 393, 1948–1957. [Google Scholar] [CrossRef] [PubMed]
- Iveson, T.; Donehower, R.C.; Davidenko, I.; Tjulandin, S.; Deptala, A.; Harrison, M.; Nirni, S.; Lakshmaiah, K.; Thomas, A.; Jiang, Y.; et al. Rilotumumab in combination with Epirubicin, Cisplatin, and Capecitabine as first-line treatment for gastric or oesophagogastric junction adenocarcinoma: An open-label, dose deescalation phase 1b study and a double-blind, randomised phase 2 study. Lancet Oncol. 2014, 15, 1007–1018. [Google Scholar] [CrossRef]
- Kawakami, H.; Fujitani, K.; Matsuyama, J.; Akamaru, Y.; Tamura, S.; Endo, S.; Kimura, Y.; Makari, Y.; Tamura, T.; Sugimoto, N.; et al. Comparison of S-1–Cisplatin every 5 weeks with Capecitabine-Cisplatin every 3 weeks for HER2-negative gastric cancer (recurrent after S-1 adjuvant therapy or chemotherapy-naïve advanced): Pooled analysis of HERBIS-2 (OGSG 1103) and HERBIS-4A (OGSG 1105) trials. Int. J. Clin. Oncol. 2020, 25, 1635–1643. [Google Scholar] [CrossRef] [PubMed]
- Vatandoust, S.; Bright, T.; Roy, A.C.; Watson, D.; Gan, S.; Bull, J.; Abbas, M.N.; Karapetis, C.S. Phase I openlabel trial of intraperitoneal Paclitaxel in combination with intravenous Cisplatin and oral Capecitabine in patients with advanced gastric cancer and peritoneal metastases (IPGP study): Study protocol. BMJ Open 2019, 9, e026732. [Google Scholar] [CrossRef]
- Kurokawa, Y.; Sugimoto, N.; Miwa, H.; Tsuda, M.; Nishina, S.; Okuda, H.; Imamura, H.; Gamoh, M.; Sakai, D.; Shimokawa, T.; et al. Phase II study of Trastuzumab in combination with S-1 plus Cisplatin in HER2-positive gastric cancer (HERBIS-1). Br. J. Cancer 2014, 110, 1163–1168. [Google Scholar] [CrossRef] [Green Version]
- Reni, M.; Zanon, S.; Peretti, U.; Chiaravalli, M.; Barone, D.; Pircher, C.; Balzano, G.; Macchini, M.; Romi, S.; Gritti, E.; et al. Nab-Paclitaxel plus Gemcitabine with or without Capecitabine and Cisplatin in metastatic pancreatic adenocarcinoma (PACT-19): A randomised phase 2 trial. Lancet Gastroenterol. Hepatol. 2018, 10, 691–697. [Google Scholar] [CrossRef]
- Park, K.; Kim, K.P.; Park, S.; Chang, H.M. Comparison of Gemcitabine plus Cisplatin versus Capecitabine plus Cisplatin as first-line chemotherapy for advanced biliary tract cancer. Asia-Pac. J. Clin. Oncol. 2016, 13, 13–20. [Google Scholar] [CrossRef]
- Abida, W.; Milowsky, M.I.; Ostrovnaya, I.; Gerst, S.R.; Rosenberg, J.E.; Voss, M.H.; Apolo, A.B.; Regazzi, A.M.; McCoy, A.S.; Boyd, M.E.; et al. Phase I study of Everolimus in combination with Gemcitabine and split-dose Cisplatin in advanced urothelial carcinoma. Bladder Cancer 2016, 2, 111–117. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; Xu, H.; Zou, J.; Wang, X.; Li, Z.; Shen, Y. Cisplatin/Capecitabine with intensity modulated radiation therapy in anal squamous cell carcinoma: A preliminary study. Scand. J. Gastroenterol. 2021, 56, 432–436. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Buecher, B.; André, T.; Jary, M.; Bidard, F.; Ghiringhelli, F.; François, É.; Taieb, J.; Smith, D.; de la Fouchardière, C.; et al. Atezolizumab plus modified Docetaxel-Cisplatin-5-Fluorouracil (mDCF) regimen versus mDCF in patients with metastatic or unresectable locally advanced recurrent anal squamous cell carcinoma: A randomized, non-comparative phase II SCARCE GERCOR trial. BMC Cancer 2020, 20, 352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Denis, C.; Sakalihasan, S.; Frères, P.; Withofs, N.; Sautois, B. Cemiplimab for Cisplatin resistant metastatic penile cancer. Case Rep. Oncol. 2021, 14, 972–976. [Google Scholar] [CrossRef] [PubMed]
- Duffy, E.A.; Fitzgerald, W.; Boyle, K.; Rohatgi, R. Nephrotoxicity: Evidence in patients receiving Cisplatin therapy. Clin. J. Oncol. Nurs. 2018, 22, 175–183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crona, D.J.; Faso, A.; Nishijima, T.F.; McGraw, K.A.; Galsky, M.D.; Milowsky, M.I. A systematic review of strategies to prevent Cisplatin-induced nephrotoxicity. Oncologist 2017, 22, 609–619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Imig, J.D.; Hye-Khan, M.A.; Burkhan, A.; Chen, G.; Adebesin, A.M.; Falck, J.R. Kidney-targeted epoxyeicosatrienoic acid analog, EET-F01, reduces inflammation, oxidative stress, and Cisplatin-induced nephrotoxicity. Int. J. Mol. Sci. 2021, 22, 2793. [Google Scholar] [CrossRef]
- Manohar, S.; Leung, N. Cisplatin nephrotoxicity: A review of the literature. J. Nephrol. 2018, 31, 15–25. [Google Scholar] [CrossRef]
- dos Santos, N.A.G.; Ferreira, R.S.; dos Santos, A.C. Overview of Cisplatin-induced neurotoxicity and ototoxicity, and the protective agents. Food Chem. Toxicol. 2020, 136, 111079. [Google Scholar] [CrossRef]
- Wheate, N.J.; Walker, S.; Craig, G.E.; Oun, R. The status of platinum anticancer drugs in the clinic and in clinical trials. Dalton Trans. 2010, 39, 8113–8127. [Google Scholar] [CrossRef] [Green Version]
- Oun, R.; Moussa, Y.E.; Wheate, N.J. The side effects of platinum-based chemotherapy drugs: A review for chemists. Dalton Trans. 2018, 47, 6645–6653. [Google Scholar] [CrossRef] [PubMed]
- Ndagi, U.; Mhlongo, N.; Soliman, M.E. Metal complexes in cancer therapy—An update from drug design perspective. Drug Design Devel. Ther. 2017, 11, 599–616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ho, G.Y.; Woodward, N.; Coward, J.I.G. Cisplatin versus Carboplatin: Comparative review of therapeutic management in solid malignancies. Crit. Rev. Oncol. Hematol. 2016, 102, 37–46. [Google Scholar] [CrossRef] [Green Version]
- Laurie, S.A.; Siu, L.L.; Winquist, E.; Maksymiuk, A.; Harnett, E.L.; Walsh, W.; Tu, D.; Parulekar, W.R. A phase 2 study of platinum and Gemcitabine in patients with advanced salivary gland cancer: A trial of the NCIC clinical trials group. Cancer 2010, 116, 362–368. [Google Scholar] [CrossRef]
- Bailly, C.; Thuru, X.; Quesnel, B. Combined cytotoxic chemotherapy and immunotherapy of cancer: Modern times. NAR Cancer 2020, 2, zcaa002. [Google Scholar] [CrossRef] [Green Version]
- Hanemaaijer, S.H.; Kok, I.C.; Fehrmann, R.S.N.; Van der Vegt, B.; Gietema, J.A.; Plaat, B.E.C.; Van Vugt, M.A.T.M.; Vergeer, M.R.; Leemans, C.R.; Langendijk, J.A.; et al. Comparison of Carboplatin with 5-Fluorouracil vs. Cisplatin as concomitant chemoradiotherapy for locally advanced head and neck squamous cell carcinoma. Front. Oncol. 2020, 10, 761. [Google Scholar] [CrossRef]
- Takayama, K.; Ichiki, M.; Matsumoto, T.; Ebi, N.; Akamine, S.; Tokunaga, S.; Yamada, T.; Uchino, J.; Nakanishi, Y. Phase II study on biweekly combination therapy of Gemcitabine plus Carboplatin for the treatment of elderly patients with advanced non-small cell lung cancer. Oncologist 2020, 25, e208–e417. [Google Scholar] [CrossRef] [Green Version]
- Tfayli, A.; Al-Assaad, M.; Fakhri, G.; Akel, R.; Atwi, H.; Ghanem, H.; El-Karak, F.; Farhat, F.; Al-Rabi, K.; Sfeir, P.; et al. Neoadjuvant chemotherapy and Avelumab in early stage resectable nonsmall cell lung cancer. Cancer Med. 2020, 9, 8406–8411. [Google Scholar] [CrossRef]
- Volk, V.; Cathomas, R.; Mark, M.; Von Moos, R.; Klingbiel, D.; Brossart, P.; Mey, U. Weekly Carboplatin in combination with weekly Paclitaxel in the treatment of metastatic non-small cell lung cancer: A single center 10-year experience. Support. Care Cancer 2016, 24, 2119–2128. [Google Scholar] [CrossRef]
- West, H.; Mc Cleod, M.; Hussein, M.; Morabito, A.; Rittmeyer, A.; Conter, H.J.; Kopp, H.G.; Daniel, D.; Mc Cune, S.; Mekhail, T.; et al. Atezolizumab in combination with Carboplatin plus Nab-Paclitaxel chemotherapy compared with chemotherapy alone as first-line treatment for metastatic non-squamous non-small-cell lung cancer (IMpower130): A multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. 2019, 20, 924–937. [Google Scholar] [CrossRef]
- Zinner, R.G.; Obasaju, C.K.; Spigel, D.R.; Weaver, R.W.; Beck, J.T.; Waterhouse, D.M.; Modiano, M.R.; Hrinczenko, B.; Nikolinakos, P.G.; Liu, J.Y.; et al. PRONOUNCE: Randomized, open-label, phase III study of first-line Pemetrexed plus Carboplatin followed by maintenance Pemetrexed versus Paclitaxel plus Carboplatin plus Bevacizumab followed by maintenance Bevacizumab in patients with advanced non-squamous non-small-cell lung cancer. J. Thoracic Oncol. 2015, 10, 134–142. [Google Scholar] [CrossRef] [Green Version]
- Rizvi, N.A.; Hellmann, M.D.; Brahmer, J.R.; Juergens, R.A.; Borghaei, H.; Gettinger, S.; Chow, L.Q.; Gerber, D.E.; Laurie, S.A.; Goldman, J.W.; et al. Nivolumab in combination with platinum-based doublet chemotherapy for first-line treatment of advanced non-small-cell lung cancer. J. Clin. Oncol. 2016, 34, 2969–2979. [Google Scholar] [CrossRef] [PubMed]
- Yoshioka, H.; Okamoto, I.; Morita, S.; Ando, M.; Takeda, K.; Seto, T.; Yamamoto, N.; Saka, H.; Atagi, S.; Hirashima, T.; et al. Efficacy and safety analysis according to histology for S-1 in combination with Carboplatin as first-line chemotherapy in patients with advanced non-small-cell lung cancer: Updated results of the West Japan Oncology Group LETS study. Ann. Oncol. 2013, 24, 1326–1331. [Google Scholar] [CrossRef]
- Kolek, V.; Grygárková, I.; Koubková, L.; Skřičková, J.; Švecová, J.; Sixtová, D.; Bartoš, J.; Tichopád, A. Carboplatin with intravenous and subsequent oral administration of Vinorelbine in resected nonsmall-cell-lung cancer in real-world set-up. PLoS ONE 2017, 12, e0181803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morikawa, N.; Inoue, A.; Sugawara, S.; Maemondo, M.; Harada, T.; Harada, M.; Fujita, Y.; Katoh, T.; Yokouchi, H.; Watanabe, H.; et al. Randomized phase II study of Carboplatin plus Irinotecan versus Carboplatin plus Amrubicin in patients with chemo-naïve extensive-stage small-cell lung cancer: North Japan Lung Cancer Study Group (NJLCG) 0901. Lung Cancer 2017, 111, 38–42. [Google Scholar] [CrossRef] [PubMed]
- Goldman, J.W.; Dvorkin, M.; Chen, Y.; Reinmuth, N.; Hotta, K.; Trukhin, D.; Statsenko, G.; Hochmair, M.J.; Özgüroğlu, M.; Ji, J.H.; et al. CASPIAN investigators.Durvalumab, with or without Tremelimumab, plus platinum-Etoposide versus platinum-etoposide alone in first-line treatment of extensive-stage small-cell lung cancer (CASPIAN): Updated results from a randomised, controlled, open-label, phase 3 trial. Lancet Oncol. 2021, 22, 51–65. [Google Scholar] [CrossRef] [PubMed]
- Horn, L.; Mansfield, A.S.; Szczęsna, A.; Havel, L.; Krzakowski, M.; Hochmair, M.J.; Huemer, F.; Losonczy, G.; Johnson, M.L.; Nishio, M.; et al. First-line Atezolizumab plus chemotherapy in extensive-stage small-cell lung Cancer. N. Engl. J. Med. 2018, 379, 2220–2229. [Google Scholar] [CrossRef]
- Langer, C.I.; Albert, I.; Ross, H.; Kovacs, P.; Blakely, L.; Pajkos, G.; Somfay, A.; Zatloukal, P.; Kazarnowicz, A.; Moezi, M.; et al. Randomized phase II study of Carboplatin and Etoposide with or without Obatoclax mesylate in extensive-stage small cell lung cancer. Lung Cancer 2014, 85, 420–428. [Google Scholar] [CrossRef]
- O’Shaughnessy, J.; Schwartzberg, L.; Danso, M.A.; Miller, K.D.; Rugo, H.S.; Neubauer, M.; Robert, N.; Hellerstedt, B.; Saleh, M.; Richards, P.; et al. Phase III study of Iniparib plus Gemcitabine and Carboplatin versus Gemcitabine and Carboplatin in patients with metastatic triple-negative breast cancer. J. Clin. Oncol. 2014, 32, 3840–3847. [Google Scholar] [CrossRef]
- Cortes, J.; Cescon, D.W.; Rugo, H.S.; Nowecki, Z.; Im, S.A.; Yusof, M.M.; Gallardo, C.; Lipatov, O.; Barrios, C.H.; Holgado, E.; et al. KEYNOTE-355 Investigators. Pembrolizumab plus chemotherapy versus placebo plus chemotherapy for previously untreated locally recurrent Inoperable or metastatic triple-negative breast cancer (KEYNOTE-355): A randomised, placebo-controlled, double-blind, phase 3 clinical trial. Lancet 2020, 396, 1817–1828. [Google Scholar] [CrossRef]
- Wu, D.; Xiong, L. Efficacy analysis of Trastuzumab, Carboplatin and Docetaxel in HER-2-positive breast cancer patients. Oncol. Lett. 2020, 19, 2539–2546. [Google Scholar] [CrossRef] [PubMed]
- Mukherjee, S.; Hurt, C.; Radhakrishna, G.; Gwynne, S.; Bateman, A.; Gollins, S.; Hawkins, M.A.; Canham, J.; Grabsch, H.I.; Falk, S.; et al. Oxaliplatin/Capecitabine or Carboplatin/Paclitaxel-based preoperative chemoradiation for resectable oesophageal adenocarcinoma (neoscope): Long-term results of a randomised controlled trial. Eur. J. Cancer 2021, 153, 153–161. [Google Scholar] [CrossRef] [PubMed]
- Petersen, P.C.; Petersen, L.N.; Vogelius, I.; Bjerregaard, J.K.; Baeksgaard, L. A randomized phase 2 trial of first-line Docetaxel, Carboplatin, Capecitabine (CTX) and Epirubicin, Oxaliplatin, Capecitabine (EOX) in advanced esophagogastric adenocarcinoma. Acta Oncol. 2021, 60, 948–953. [Google Scholar] [CrossRef] [PubMed]
- Prithviraj, G.K.; Baksh, K.; Fulp, W.; Meredith, K.; Hoffe, S.; Shridhar, R.; Almhanna, K. Carboplatin and Paclitaxel as first-line treatment of unresectable or metastatic esophageal or gastric cancer. Dis. Esophagus 2014, 28, 782–787. [Google Scholar] [CrossRef] [PubMed]
- Al-Eisawi, Z.; Beale, P.; Chan, C.; Yu, J.Q.; Huq, F. Carboplatin and Oxaliplatin in sequenced combination with Bortezomib in ovarian tumour models. J. Ovarian Res. 2013, 6, 78. [Google Scholar] [CrossRef] [Green Version]
- Fader, A.N.; Roque, D.M.; Siegel, E.; Buza, N.; Hui, P.; Abdelghany, O.; Chambers, S.K.; Secord, A.A.; Havrilesky, L.; O’Malley, D.M.; et al. Randomized phase II trial of Carboplatin-Paclitaxel versus Carboplatin-Paclitaxel-Trastuzumab in uterine serous carcinomas that overexpress human epidermal growth factor receptor 2/Neu. J. Clin. Oncol. 2018, 36, 2044–2051. [Google Scholar] [CrossRef]
- Kidani, Y.; Inagaki, K.; Iigo, M.; Hoshi, A.; Kuretani, K. Antitumor activity of 1,2-diaminocyclohexane-platinum complexes against sarcoma-180 ascites form. J.Med. Chem. 1978, 21, 1315–1318. [Google Scholar] [CrossRef]
- Alcindor, T.; Beauger, N. Oxaliplatin: A review in the era of molecularly targeted therapy. Curr. Oncol. 2011, 18, 18–25. [Google Scholar] [CrossRef] [Green Version]
- Perego, P.; Robert, J. Oxaliplatin in the era of personalized medicine: From mechanistic studies to clinical efficacy. Cancer Chemother. Pharmacol. 2015, 77, 5–18. [Google Scholar] [CrossRef]
- Park, S.J.; Ye, W.; Xiao, R.; Silvin, C.; Padget, M.; Hodge, J.W.; Van Waes, C.; Schmitt, N.C. Cisplatin and Oxaliplatin induce similar immunogenic changes in preclinical models of head and neck cancer. Oral Oncol. 2019, 95, 127–135. [Google Scholar] [CrossRef]
- Spada, F.; Antonuzzo, L.; Marconcini, R.; Radice, D.; Antonuzzo, A.; Ricci, S.; Di Costanzo, F.; Fontana, A.; Gelsomino, F.; Luppi, G.; et al. Oxaliplatin-based chemotherapy in advanced neuroendocrine tumors: Clinical outcomes and preliminary correlation with biological factors. Neuroendocrinology 2016, 103, 806–814. [Google Scholar] [CrossRef] [PubMed]
- Tsimberidou, A.M.; Keating, M.J.; Jabbour, E.J.; Ravandi-Kashani, F.; O’Brien, S.; Estey, E.; Bekele, N.; Plunkett, W.K.; Kantarjian, H.; Borthakur, G. A phase I study of Fludarabine, Cytarabine, and Oxaliplatin therapy in patients with relapsed or refractory acute myeloid leukemia. Clin. Lymphoma Myeloma Leuk. 2014, 14, 395–400.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, K.; Qin, H.; Pan, F.; Liu, E.; Liang, H.; Ruan, Z. Nedaplatin or Oxaliplatin combined with Paclitaxel and Docetaxel as first-line treatment for patients with advanced non-small cell lung cancer. Med. Sci. Monit. 2014, 20, 2830–2836. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitani, S.; Kadowaki, S.; Kato, K.; Masuishi, T.; Muro, K. Combination of Oxaliplatin and 5-Fluorouracil/Leucovorin for advanced esophageal squamous cell carcinoma refractory or Iintolerant to standard therapies. Case Rep. Oncol. 2019, 12, 304–310. [Google Scholar] [CrossRef] [PubMed]
- Jiang, H.; Zheng, Y.; Qian, J.; Mao, C.; Xu, X.; Li, N.; Xiao, C.; Wang, H.; Teng, L.; Zhou, H.; et al. Safety and efficacy of Sintilimab combined with Oxaliplatin/Capecitabine as first-line treatment in patients with locally advanced or metastatic gastric/gastroesophageal junction adenocarcinoma in a phase Ib clinical trial. BMC Cancer 2020, 20, 760. [Google Scholar] [CrossRef]
- Shah, M.A.; Bang, Y.J.; Lordick, F.; Alsina, M.; Chen, M.; Hack, S.P.; Bruey, J.; Smith, D.; McCaffery, I.; Shames, D.; et al. Effect of Fluorouracil, Leucovorin, and Oxaliplatin with or without Onartuzumab in HER2-negative, MET-positive gastroesophageal adenocarcinoma. JAMA Oncol. 2017, 3, 620–627. [Google Scholar] [CrossRef]
- Malka, D.; François, E.; Penault-Llorca, F.; Castan, F.; Bouché, O.; Bennouna, J.; Ghiringhelli, F.; de la Fouchardière, C.; Borg, C.; Samalin, E.; et al. FOLFOX alone or combined with Rilotumumab or Panitumumab as first-line treatment for patients with advanced gastroesophageal adenocarcinoma (PRODIGE 17-ACCORD 20-MEGA): A randomised, open-label, three-arm phase II trial. Eur. J. Cancer 2019, 115, 97–106. [Google Scholar] [CrossRef]
- Kawazoe, A.; Yamaguchi, K.; Yasui, H.; Negoro, Y.; Azuma, M.; Amagai, K.; Hara, H.; Baba, H.; Tsuda, M.; Hosaka, H.; et al. Safety and efficacy of Pembrolizumab in combination with S-1 plus Oxaliplatin as a first-line treatment in patients with advanced gastric/gastroesophageal junction cancer: Cohort 1 data from the KEYNOTE-659 phase IIb study. Eur. J. Cancer 2020, 129, 97–106. [Google Scholar] [CrossRef] [Green Version]
- Cheng, X.; Wu, D.; Xu, N.; Chen, L.; Yan, Z.; Chen, P.; Zhou, L.; Yu, J.; Cui, J.; Li, W.; et al. Adjuvant albumin-bound Paclitaxel combined with S-1 vs. Oxaliplatin combined with Capecitabine after D2 gastrectomy in patients with stage III gastric adenocarcinoma: A phase III multicenter, open-label, randomized controlled clinical trial protocol. BMC Cancer 2021, 21, 56. [Google Scholar] [CrossRef]
- Monti, M.; Morgagni, P.; Nanni, O.; Framarini, M.; Saragoni, L.; Marrelli, D.; Roviello, F.; Petrioli, R.; Romario, U.F.; Rimassa, L.; et al. Preoperative or perioperative Docetaxel, Oxaliplatin, and Capecitabine (GASTRODOC Regimen) in patients with locally-advanced eesectable gastric cancer: A randomized phase-II trial. Cancers 2020, 12, 2790. [Google Scholar] [CrossRef]
- Petrioli, R.; Marrelli, D.; Roviello, F.; D’Ignazio, A.; Torre, P.; Chirra, M.; Savelli, V.; Ambrosio, M.R.; Francini, G.; Calomino, N.; et al. Pathological response and outcome after neoadjuvant chemotherapy with DOC (Docetaxel, Oxaliplatin, Capecitabine) or EOF (Epirubicin, Oxaliplatin, 5-Fluorouracil) for clinical T3-T4 non-metastatic gastric cancer. Surg. Oncol. 2020, 32, 2–7. [Google Scholar] [CrossRef] [PubMed]
- Rivera, F.; Romero, C.; Jimenez-Fonseca, P.; Izquierdo-Manuel, M.; Salud, A.; Martínez, E.; Jorge, M.; Arrazubi, V.; Méndez, J.C.; García-Alfonso, P.; et al. Phase II study to evaluate the efficacy of Trastuzumab in combination with Capecitabine and Oxaliplatin in first-line treatment of HER2-positive advanced gastric cancer: HERXO trial. Cancer Chemother. Pharmacol. 2019, 83, 1175–1181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boku, N.; Ryu, M.H.; Kato, K.; Chung, H.C.; Minashi, K.; Lee, K.W.; Cho, H.; Kang, W.K.; Komatsu, Y.; Tsuda, M.; et al. Safety and efficacy of Nivolumab in combination with S-1/Capecitabine plus Oxaliplatin in patients with previously untreated, unresectable, advanced, or recurrent gastric/gastroesophageal junction cancer: Interim results of a randomized, phase II trial (ATTRACTION-4). Annals Oncol. 2019, 30, 250–258. [Google Scholar] [CrossRef] [Green Version]
- Kondoh, C.; Kadowaki, S.; Komori, A.; Narita, Y.; Taniguchi, H.; Ura, T.; Ando, M.; Muro, K. Salvage chemotherapy with the combination of Oxaliplatin, Leucovorin, and 5-Fluorouracil in advanced gastric cancer refractory or intolerant to fluoropyrimidines, platinum, taxanes, and Irinotecan. Gastric Cancer 2018, 21, 1050–1057. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sah, B.K.; Zhang, B.; Zhang, H.; Li, J.; Yuan, F.; Ma, T.; Shi, M.; Xu, W.; Zhu, Z.; Liu, W.; et al. Neoadjuvant FLOT versus SOX phase II randomized clinical trial for patients with locally advanced gastric cancer. Nature Commun. 2020, 11, 6093. [Google Scholar] [CrossRef] [PubMed]
- Moehler, M.; Dvorkin, M.; Boku, N.; Özgüroğlu, M.; Ryu, M.H.; Muntean, A.S.; Lonardi, S.; Nechaeva, M.; Bragagnoli, A.C.; Coşkun, H.S.; et al. Phase III trial of Avelumab maintenance after first-line induction chemotherapy versus continuation of chemotherapy in patients with gastric cancers: Results from JAVELIN Gastric 100. J. Clin. Oncol. 2021, 39, 966–977. [Google Scholar] [CrossRef]
- Tan, S.; Xie, J.; Wei, J.; Liu, Q.; Du, J.; Liu, B.; Yang, Y. Concurrent Docetaxel and S-1 compared with Oxaliplatin and S-1 as first-line therapy for advanced gastric adenocarcinoma: A eetrospective study. J. Clin. Oncol. 2020, 38 (Suppl. S15), 16540. [Google Scholar] [CrossRef]
- Matsumoto, T.; Kurioka, Y.; Okazaki, U.; Matsuo, Y.; Kimura, S.; Miura, K.; Tsuduki, T.; Takagi, S.; Takatani, M.; Morishita, H. FOLFIRINOX for advanced pancreatic cancer patients after Nab-Paclitaxel plus Gemcitabine failure. Pancreas 2020, 49, 574–578. [Google Scholar] [CrossRef]
- Antoniotti, C.; Borelli, B.; Rossini, D.; Pietrantonio, F.; Morano, F.; Salvatore, L.; Lonardi, S.; Marmorino, F.; Tamberi, S.; Corallo, S.; et al. AtezoTRIBE: A randomised phase II study of FOLFOXIRI plus Bevacizumab alone or in combination with Atezolizumab as initial therapy for patients with unresectable metastatic colorectal cancer. BMC Cancer 2020, 20, 683. [Google Scholar] [CrossRef]
- Fumet, J.D.; Isambert, N.; Hervieu, A.; Zanetta, S.; Guion, J.F.; Hennequin, A.; Rederstorff, E.; Bertaut, A.; Ghiringhelli, F. Phase Ib/II trial evaluating the safety, tolerability and immunological activity of Durvalumab (MEDI4736) (anti-PD-L1) plus Tremelimumab (anti-CTLA-4) combined with FOLFOX in patients with metastatic colorectal cancer. ESMO Open 2018, 3, e000375. [Google Scholar] [CrossRef] [Green Version]
- Limagne, E.; Thibaudin, M.; Nuttin, L.; Spill, A.; Derangère, V.; Fumet, J.D.; Amellal, N.; Peranzoni, E.; Cattan, V.; Ghiringhelli, F. Trifluridine/Tipiracil plus Oxaliplatin improves PD-1 blockade in colorectal cancer by inducing immunogenic cell death and depleting macrophages. Cancer Immunol. Res. 2019, 7, 1958–1969. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.W.; Lee, K.H.; Kim, H.J.; Kim, T.Y.; Kim, J.S.; Han, S.W.; Oh, D.Y.; Kim, J.H.; Im, S.A.; Kim, T.Y. A phase II trial of S-1 and Oxaliplatin in patients with advanced hepatocellular carcinoma. BMC Cancer 2018, 18, 252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drott, J.R.; Fomichov, V.; Starkhammar, H.; Börjeson, S.; Kjellgren, K.; Berterö, C. Oxaliplatin-induced neurotoxic side effects and their impact on daily activities. A longitudinal study among patients with colorectal cancer. Cancer Nurs. 2018, 42, 40–48. [Google Scholar] [CrossRef] [Green Version]
- Gebremedhn, E.G.; Shortland, P.J.; Mahns, D.A. The incidence of acute Oxaliplatin-induced neuropathy and its impact on treatment in the first cycle: A systematic review. BMC Cancer 2018, 18, 410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shimada, M.; Itamochi, H.; Kigawa, J. Nedaplatin: A Cisplatin derivative in cancer chemotherapy. Cancer Manag. Res. 2013, 5, 67–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y.; Yu, S.; Liu, S.; Cao, H.; Ma, R.; Wu, J.; Feng, J. Comparison of Nedaplatin-based versus Cisplatin-based chemotherapy for advanced non-small cell lung cancer among East Asian populations: A meta-analysis. Sci. Rep. 2015, 5, 10516. [Google Scholar] [CrossRef]
- Zhu, H.; Ge, X.; Lu, Y.; Zuo, Y.; Qin, Q.; Sun, X.; Yang, M. Nedaplatin-based chemotherapy regimens combined with concurrent radiotherapy as first-line treatment for stage II-III esophageal squamous cell carcinoma. Oncol. Lett. 2018, 17, 594–602. [Google Scholar] [CrossRef] [Green Version]
- Okuda, H.; Ohnishi, M.; Takahashi, H.; Takagi, C.; Takada, N.; Ohashi, T. Long-term efficacy and toxicity of concurrent chemoradiotherapy with Nedaplatin and S-1 for head and neck squamous cell carcinomaCarcinoma. Auris Nasus Larynx 2019, 46, 882–888. [Google Scholar] [CrossRef]
- Teramoto, K.; Asada, Y.; Ozaki, Y.; Suzumura, Y.; Nakano, Y.; Sawai, S.; Tezuka, N.; Inoue, S.; Fujino, S. A phase II study of Docetaxel plus Nedaplatin in patients with metastatic non-small-cell lung cancer. Cancer Chemother. Pharmacol. 2012, 70, 531–537. [Google Scholar] [CrossRef]
- Yang, S. A pooled study on combination of Gemcitabine and Nedaplatin for treating patients with non-small cell lung cancer. Asian Pac. J. Cancer Prevent. 2015, 16, 5963–5966. [Google Scholar] [CrossRef] [Green Version]
- Fu, J.; Fang, S.; Wen, Y.; Wang, Y.; Yin, X.; Wang, D. The efficacy and safety of Irinotecan combined with Nedaplatin in the treatment of small cell lung cancer. J. Buon 2020, 25, 1707–1713. [Google Scholar] [PubMed]
- Igawa, S.; Otani, S.; Nakahara, Y.; Ryuge, S.; Hiyoshi, Y.; Fukui, T.; Mitsufuji, H.; Kubota, M.; Katagiri, M.; Sato, Y.; et al. Phase I study of Nedaplatin, a platinum based antineoplastic drug, combined with Nab-Paclitaxel in patients with advanced squamous non-small cell lung cancer. Investig. New Drugs 2017, 36, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Mai, W.; Hao, B.; Jiang, W.; Geng, Q. Promising response to a PD-1 inhibitor (Sintilimab) in non-small cell lung cancer: A case report. Medicine 2020, 99, e19790. [Google Scholar] [CrossRef] [PubMed]
- Kenmotsu, Y.; Oshita, F.; Sugiura, M.; Murakami, S.; Kondo, T.; Saito, H.; Yamada, K. Nedaplatin and Irinotecan in patients with large-cell neuroendocrine carcinoma of the lung. Anticancer Res. 2012, 32, 1453–1456. [Google Scholar]
- Tang, Z.; Fang, R.; Tong, G.; Liu, P.; Ou, Z.; Tang, Y. Overcoming resistance to anti-PD-1 immunotherapy in lymphoepithelioma-like carcinoma: A case report and review of the literature. Lung Cancer 2020, 146, 335–340. [Google Scholar] [CrossRef]
- Fujita, Y.; Hiramatsu, M.; Kawai, M.; Sumiyoshi, K.; Nishimura, H.; Tanigawa, N. Evaluation of combined Docetaxel and Nedaplatin chemotherapy for recurrent esophageal cancer compared with conventional chemotherapy using Cisplatin and 5-Fluorouracil: A retrospective study. Dis. Esophagus 2008, 21, 496–501. [Google Scholar] [CrossRef]
- Miyazaki, T.; Ojima, H.; Fukuchi, M.; Sakai, M.; Sohda, M.; Tanaka, N.; Suzuki, S.; Ieta, K.; Saito, K.; Sano, A.; et al. Phase II study of Docetaxel, Nedaplatin, and 5-Fluorouracil combined chemotherapy for advanced esophageal cancer. Annals Surgic. Oncol. 2015, 22, 3653–3658. [Google Scholar] [CrossRef]
- Tanaka, Y.; Yoshida, K.; Tanahashi, T.; Okumura, N.; Matsuhashi, N.; Yamaguchi, K. Phase II trial of neoadjuvant chemotherapy with Docetaxel, Nedaplatin, and S1 for advanced esophageal squamous cell carcinoma. Cancer Sci. 2016, 107, 764–772. [Google Scholar] [CrossRef] [Green Version]
- Yamashita, H.; Abe, O.; Nakagawa, K. Involved-field irradiation concurrently combined with Nedaplatin/5-Fluorouracil for inoperable esophageal cancer on basis of 18FDG-PET scans: A long follow-up results of phase II study. Radiother. Oncol. 2017, 123, 488. [Google Scholar] [CrossRef]
- Wang, Z.Q.; Wang, D.S.; Wang, F.H.; Ren, C.; Tan, Q.; Li, Y.H. Recombinant human endostatin plus Paclitaxel/ Nedaplatin for recurrent or metastatic advanced esophageal squamous cell carcinoma: A prospective, single-arm, open-label, phase II study. Investig. New Drugs 2020, 39, 516–523. [Google Scholar] [CrossRef]
- Jing, W.; Yan, W.; Liu, Y.; Li, J.; Yu, J.; Zhu, H. Slight advantages of Nimotuzumab versus Cetuximab plus concurrent chemoradiotherapy in locally advanced esophageal squamous cell carcinoma. Cancer Biol. Ther. 2019, 20, 1121–1126. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.; Fu, J.T.; Shi, D.; Feng, B.; Shi, Z. Clinical efficacy and safety of Gemcitabine plus Nedaplatin in the treatment of advanced nasopharyngeal carcinoma. J. Cancer Res. Ther. 2016, 12, 252–255. [Google Scholar] [CrossRef]
- Liu, T.; Sun, Q.; Chen, J.; Li, B.; Qin, W.; Wang, F.; Ye, Z.; Hu, F. Neoadjuvant chemotherapy with Fluorouracil plus Nedaplatin or Cisplatin for locally advanced nasopharyngeal carcinoma: A retrospective study. J. Cancer 2018, 9, 3676–3682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peng, P.J.; Lv, B.J.; Wang, Z.H.; Liao, H.; Liu, Y.M.; Lin, Z.; Con, Y.Y.; Huang, P.Y. Multi-institutional prospective study of Nedaplatin plus S-1 chemotherapy in recurrent and metastatic nasopharyngeal carcinoma patients after failure of platinum-containing regimens. Ther. Adv. Med. Oncol. 2016, 9, 68–74. [Google Scholar] [CrossRef]
- Zhan, Z.J.; Tao, H.Y.; Qiu, W.Z.; Liu, Z.Y.; Zhang, R.X.; Liao, K.; Li, G.; Yuan, Y.W.; Yuan, T.Z.; Zheng, R.H. Clinical value of Nedaplatin-based chemotherapy combined with radiotherapy for locoregional advanced nasopharyngeal carcinoma: A retrospective, propensity score-matched analysis. J. Cancer 2020, 11, 6782–6789. [Google Scholar] [CrossRef]
- Shukuya, T.; Yamanaka, T.; Seto, T.; Daga, H.; Goto, K.; Saka, H.; Sugawara, S.; Takahashi, T.; Yokota, S.; Kaneda, H.; et al. Nedaplatin plus Docetaxel versus Cisplatin plus Docetaxel for advanced or relapsed squamous cell carcinoma of the lung (WJOG5208L): A randomised, open-label, phase 3 trial. Lancet Oncol. 2015, 16, 1630–1638. [Google Scholar] [CrossRef]
- Masago, K.; Fujita, S.; Kim, Y.H.; Hatachi, Y.; Fukuhara, A.; Irisa, K.; Nagai, H.; Sakamori, Y.; Togashi, Y.; Mio, T.; et al. Phase I study of the combination of Nedaplatin and Gemcitabine in previously untreated advanced squamous cell lung cancer. Cancer Chemother. Pharmacol. 2010, 67, 325–330. [Google Scholar] [CrossRef]
- Yamada, K.; Saito, H.; Kondo, T.; Murakami, S.; Masuda, N.; Yamamoto, M.; Igawa, S.; Katono, K.; Takiguchi, Y.; Iwasawa, S.; et al. Multicenter phase II study of Nedaplatin and Irinotecan for patients with squamous cell carcinoma of the lung: Thoracic oncology research group 0910. Anticancer Res. 2015, 35, 6705–6711. [Google Scholar]
- Matsumoto, K.; Mochizuki, K.; Hirayama, T.; Ikeda, M.; Nishi, M.; Tabata, K.; Okazaki, M.; Fujita, T.; Taoka, Y.; Iwamura, M. Gemcitabine plus Nedaplatin as salvage therapy is a favorable option for patients with progressive metastatic urothelial carcinoma after two lines of chemotherapy. Asian Pac. J. Cancer Prev. 2015, 16, 2483–2487. [Google Scholar] [CrossRef] [Green Version]
- Kitamura, H.; Taguchi, K.; Kunishima, Y.; Yanase, M.; Takahashi, A.; Shigyo, M.; Tanaka, T.; Mutoh, M.; Fukuta, F.; Masumori, N.; et al. Paclitaxel, Ifosfamide, and Nedaplatin as second-line treatment for patients with metastatic urothelial carcinoma: A phase II study of the SUOC group. Cancer Sci. 2011, 102, 1171–1175. [Google Scholar] [CrossRef]
- Li, L.; Zhuang, Q.; Cao, Z.; Yin, R.; Zhu, Y.; Zhu, L.; Xie, X.; Zhang, Y.; Li, L.; Wu, Q.; et al. Paclitaxel plus Nedaplatin vs. Paclitaxel plus Carboplatin in women with epithelial ovarian cancer: A multi-center, randomized, open-label, phase III trial. Oncol. Lett. 2018, 15, 3646–3652. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Chen, C.; Wang, S.; Li, X.; Fan, T. Efficacy of Bevacizumab combined with Nedaplatin in the treatment of ovarian cancer and it’s effects on tumor markers and immunity of patients. J. Buon 2020, 25, 80–86. [Google Scholar] [PubMed]
- Miyamoto, M.; Takano, M.; Kuwahara, M.; Soyama, H.; Kato, K.; Matuura, H.; Sakamoto, T.; Takasaki, K.; Aoyama, T.; Yoshikawa, T.; et al. Efficacy of combination chemotherapy using Irinotecan and Nedaplatin for patients with recurrent and refractory endometrial carcinomas: Preliminary analysis and literature review. Cancer Chemother. Pharmacol. 2017, 81, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Zeng, J.; Huang, M.; An, J.; Bai, P.; Wu, L.; Zhang, R. A phase 2 study of nanoparticle albumin-bound Paclitaxel plus Nedaplatin for patients with advanced, recurrent, or metastatic cervical carcinoma. Cancer 2016, 123, 420–425. [Google Scholar] [CrossRef]
- Takekuma, M.; Shimokawa, M.; Nishio, S.; Omi, H.; Tabata, T.; Takei, Y.; Nasu, K.; Takahashi, Y.; Toyota, S.; Ichikawa, Y.; et al. Phase II study of adjuvant chemotherapy with Paclitaxel and Nedaplatin for uterine cervical cancer with lymph node metastasis. Cancer Sci. 2018, 109, 1602–1608. [Google Scholar] [CrossRef] [Green Version]
- Uehara, T.; Yamate, J.; Torii, M.; Maruyama, T. Comparative nephrotoxicity of Cisplatin and Nedaplatin: Mechanisms and histopathological characteristics. J. Toxicol. Pathol. 2011, 24, 87–94. [Google Scholar] [CrossRef] [Green Version]
- Zhong, L.Z.; Xu, H.Y.; Zhao, Z.M.; Zhang, G.M.; Lin, F.W. Comparison of efficacy and toxicity between Nedaplatin and Cisplatin in treating malignant pleural effusion. OncoTargets Ther. 2018, 11, 5509–5512. [Google Scholar] [CrossRef] [Green Version]
- Chen, X.; Wu, Y.; Dong, H.; Zhang, C.; Zhang, Y. Platinum-based agents for individualized cancer treatment. Curr. Molecul. Med. 2013, 13, 1603–1612. [Google Scholar] [CrossRef]
- Brown, A.; Kumar, S.; Tchounwou, P.B. Cisplatin-based chemotherapy of human cancers. J. Cancer Sci. Ther. 2019, 11, 97. [Google Scholar]
- Zhang, H.Y.; Liu, Y.R.; Li, W.; Li, H.; Dou, S.X.; Xie, P.; Wang, W.C.; Wang, P.V. Condensations of single DNA molecules induced by Heptaplatin and its chiral isomer. AIP Adv. 2014, 4, 087128. [Google Scholar] [CrossRef]
- Lee, K.H.; Hyun, M.S.; Kim, H.K.; Jin, H.M.; Yang, J.; Song, H.S.; Do, Y.R.; Ryoo, H.M.; Chung, J.S.; Zang, D.Y.; et al. Randomized, multicenter, phase III trial of Heptaplatin 1-hour infusion and 5-Fluorouracil combination chemotherapy comparing with Cisplatin and 5-Fluorouracil combination chemotherapy in patients with advanced gastric cancer. CancerRes. Treat. 2009, 41, 12–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, W.S.; Lee, G.W.; Kim, H.W.; Lee, O.J.; Lee, Y.J.; Ko, G.H.; Lee, J.S.; Jang, J.S.; Ha, W.S. A phase II trial of Heptaplatin/5-FU and Leucovorin for advanced stomach cancer. Cancer Res. Treat. 2005, 37, 208–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, X.; Zhou, H.; Jiao, R.; Liu, H.; Qin, C.; Xu, L.; Chen, Y. Supramolecular chemotherapy: Host–guest complexes of Heptaplatin-Cucurbit [7]uril toward colorectal normal and tumor cells. Langmuir 2021, 37, 5475–5482. [Google Scholar] [CrossRef] [PubMed]
- Park, M.S.; Kang, M.H.; Lim, S.C.; Choi, S.O.; Lee, B.K.; Lee, M.K. Retrospective evaluation of Heptaplatin toxicities in patients with advanced gastric cancer. Korean J. Clin. Pharm. 2006, 16, 131–138. [Google Scholar]
- Muggia, F.M.; Bonetti, A.; Hoeschele, J.D.; Rozencweig, M.; Howell, S.B. Platinum antitumor complexes: 50 years since Barnett Rosenberg’s discovery. J. Clin. Oncol. 2015, 33, 4219–4226. [Google Scholar] [CrossRef]
- Li, Y.; Yang, G.; Li, M.; Tong, X. Nursing observation on the clinical efficacy and toxicity of Lobaplatin compared with Cisplatin in the treatment of locally advanced hypopharyngeal carcinoma based on intelligent CT imaging. J. Healthc. Eng. 2021, 2021, 9982888. [Google Scholar] [CrossRef]
- Pan, S.; Sun, Y.; Sui, D.; Yang, T.; Fu, S.; Wang, J.; Hui, B.; Xi, R.; He, C.; Zhang, X. Lobaplatin promotes radiosensitivity, induces apoptosis, attenuates cancer stemness and inhibits proliferation through PI3K/AKT pathway in esophageal squamous cell carcinoma. Biomed. Pharmacother. 2018, 102, 567–574. [Google Scholar] [CrossRef]
- Zhou, N.N.; Zhao, Y.Y.; Zhai, L.Z.; Ruan, C.M.; Yang, Y.P.; Huang, Y.; Hou, X.; Chen, L.K.; Zhou, T.; Zhang, L. The efficacy and toxicity of Lobaplatin-contained chemotherapy in extensive-stage small-cell lung cancer. J. Cancer 2018, 9, 2232–2236. [Google Scholar] [CrossRef]
- Wang, Z.; Xu, L.; Wang, H.; Li, Z.; Lu, L.; Li, X.; Zhang, Q. Lobaplatin-based regimens outperform Cisplatin for metastatic breast cancer after anthracyclines and taxanes treatment. Saudi J. Biol. Sci. 2018, 25, 909–916. [Google Scholar] [CrossRef]
- Li, Y.; Liu, B.; Yang, F.; Yu, Y.; Zeng, A.; Ye, T.; Yin, W.; Xie, Y.; Fu, Z.; Zhao, C. Lobaplatin induces BGC-823 human cell apoptosis via ROS-mitochondrial apoptotic pathway and impairs cell migration gastric carcinoma and invasion. Biomed. Pharmacother. 2016, 83, 1239–1246. [Google Scholar] [CrossRef]
- Wang, H.; Li, B.; Yan, K.; Wu, Y.; Wen, Y.; Liu, Y.; Fan, P.; Ma, Q. Protein and signaling pathway responses to rhIL-6 intervention before Lobaplatin treatment in osteosarcoma cells. Front. Oncol. 2021, 11, 602712. [Google Scholar] [CrossRef] [PubMed]
- Makovec, T. Cisplatin and beyond: Molecular mechanisms of action and drug resistance development in cancer chemotherapy. Radiol. Oncol. 2019, 53, 148–158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, B.; Zhang, H.; Chen, R.; Yang, S.; Liu, W.; Li, K.; Zhang, H.; Zhu, X. Lobaplatin for the treatment of SK-MES-1 lung squamous cell line in vitro and in vivo. OncoTargets Ther. 2016, 9, 4215–4224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Z.; Tang, X.; Zhang, Y.; Qi, R.; Li, Z.; Zhang, K.; Liu, Z.; Yang, X. Lobaplatin induces apoptosis and arrests cell cycle progression in human cholangiocarcinoma cell line RBE. Biomed. Pharmacother. 2012, 66, 161–166. [Google Scholar] [CrossRef]
- Li, X.; Ran, L.; Fang, W.; Wang, D. Lobaplatin arrests cell cycle progression, induces apoptosis and alters the proteome in human cervical cancer cell Line CaSki. Biomed. Pharmacother. 2014, 68, 291–297. [Google Scholar] [CrossRef]
- Lv, X.; Cao, X.; Xia, W.X.; Liu, K.Y.; Qiang, M.Y.; Guo, L.; Qian, C.N.; Cao, K.J.; Mo, H.Y.; Li, X.M.; et al. Induction chemotherapy with Lobaplatin and Fluorouracil versus Cisplatin and Fluorouracil followed by chemoradiotherapy in patients with stage III–IVB nasopharyngeal carcinoma: An open-label, non-inferiority, randomised, controlled, phase 3 trial. Lancet Oncol. 2021, 22, 716–726. [Google Scholar] [CrossRef]
- Ke, L.R.; Xia, W.X.; Qiu, W.Z.; Huang, X.J.; Yang, J.; Yu, Y.H.; Liang, H.; Liu, G.Y.; Ye, Y.F.; Xiang, Y.Q.; et al. Safety and efficacy of Lobaplatin combined with 5-Fluorouracil as first-line induction chemotherapy followed by Lobaplatin-radiotherapy in locally advanced nasopharyngeal carcinoma: Preliminary results of a prospective phase II trial. BMC Cancer 2017, 17, 134. [Google Scholar] [CrossRef] [Green Version]
- Cheng, Y.; Fan, Y.; Liu, X.; Liu, Y.; Liu, J.; Wang, D.; Yu, Y.; Qin, S.; Liu, W.; Huang, C.; et al. Randomized controlled trial of Lobaplatin plus Etoposide vs.Cisplatin plus Etoposide as first-line therapy in patients with extensive-stage small cell lung cancer. Oncol. Lett. 2019, 17, 4701–4709. [Google Scholar] [CrossRef]
- Zhang, H.; Zhang, Y.; Wang, C.; Fang, S.; Xu, B.; Wang, C.; Wu, J.; Liu, D. Clinical research on therapeutic effect of combined application of Lobaplatin and Irinotecan in treating recurrant small cell lung cancer. Pak. J. Pharm. Sci. 2018, 31 (Suppl. S5), 2295–2298. [Google Scholar]
- Zhong, R.; Li, H.; Liu, Y.; Zhang, S.; Liu, J.; Huang, Z.; Cheng, Y. Chemotherapy combined with Bevacizumab for the treatment of advanced lung adenocarcinoma cancer harboring EGFR-ANXA2, EGFR-RAD51, ATR and BRCA2 mutations: A case report. Thorac. Cancer 2019, 11, 456–460. [Google Scholar] [CrossRef] [Green Version]
- Yuan, Y.; Zhang, L.; Zhang, Z.; Qian, Y.; Teng, Y. A study of the efficacy and tolerability of Capecitabine and Lobaplatin in advanced HER-2 negative breast cancer patients. Ann. Transl. Med. 2021, 9, 1151. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Wang, B.; He, M.; Chang, J.; Li, J.; Shan, L.; Wang, H.; Hong, W.; Luo, D.; Song, Y.; et al. Pilot study of Docetaxel combined with Lobaplatin or Gemcitabine for recurrent and metastatic breast cancer. Medicine 2019, 98, e18513. [Google Scholar] [CrossRef] [PubMed]
- Jia, X.J.; Huang, J.Z. Clinical study on Lobaplatin combined with 5-Fu and concurrent radiotherapy in treating patients with inoperable esophageal cancer. Asian Pac. J. Cancer Prev. 2015, 16, 6595–6597. [Google Scholar] [CrossRef] [PubMed]
- Li, X.Y.; Zhou, F.; Ren, Z.H.; Zhao, Y.F.; Lu, P.; Wang, J.S.; Zhen, A.P.; Ku, J.W. Phase trail of Lobaplatin, Leucovorin and Fluorouracil in patient s with advanced carcinoma of the esophagus. Chin. J. Cancer. Prev. Treat. 2007, 14, 64–66. [Google Scholar]
- Chen, M.Q.; Chen, C.; Lu, H.J.; Xu, B.H. The efficacy and toxicities of combined Lobaplatin with Paclitaxel as a first-line chemotherapy for advanced esophageal squamous cell carcinoma. J. Thorac. Dis. 2015, 7, 1749–1755. [Google Scholar] [CrossRef]
- Hua, S.; Kong, X.; Chen, B.; Zhuang, W.; Sun, Q.; Yang, W.; Liu, W.; Zhang, Y. Anticancer mechanism of Lobaplatin as monotherapy and in combination with Paclitaxel in human gastric cancer. Curr. Mol. Pharmacol. 2018, 11, 316–325. [Google Scholar] [CrossRef]
- Wu, Y.; Xu, X.Y.; Yan, F.; Sun, W.L.; Zhang, Y.; Liu, D.L.; Shen, B. Retrospective study of the efficacy and toxicity of Lobaplatin in combined chemotherapy for metastatic breast cancer. OncoTargets Ther. 2019, 12, 4849–4857. [Google Scholar] [CrossRef] [Green Version]
- Nagyal, L.; Kumar, A.; Sharma, R.; Yadav, R.; Chaudhary, P.; Singh, R. Bioinorganic chemistry of platinum (IV) complexes as platforms for anticancer agents. Curr. Bioact. Compd. 2020, 16, 726–737. [Google Scholar] [CrossRef]
- Doshi, G.; Sonpavde, G.; Sternberg, C. Clinical and pharmacokinetic evaluation of Satraplatin. Expert Opin. Drug Metabol. Toxicol. 2011, 8, 103–111. [Google Scholar] [CrossRef]
- Akshintala, S.; Marcus, L.; Warren, K.E.; Murphy, R.; Sissung, T.; Srivastava, A.; Goodspeed, W.; Goodwin, A.; Brewer, C.; Zalewski, C.; et al. Phase 1 trial and pharmacokinetic study of the oral platinum analog Satraplatin in children and young adults with refractory solid tumors including brain tumors. Pediatr. Blood Cancer 2015, 62, 603–610. [Google Scholar] [CrossRef] [Green Version]
- Avan, A.; Adema, A.D.; Hoebe, E.K.; Huijts, C.M.; Avan, A.; Veal, G.J.; Ruijtenbeek, R.; Wosikowski, K.; Peters, G.J. Modulation of signaling enhances the efficacy of the combination of Satraplatin and Erlotinib. Curr. Drug Targets 2014, 15, 1312–1321. [Google Scholar] [CrossRef] [PubMed]
- Vaishampayan, U.N.; Fontana, J.; Heilbrun, L.K.; Smith, D.; Heath, E.; Dickow, B.; Figg, W.D. Phase II trial of Bevacizumab and Satraplatin in Docetaxel-pretreated metastatic castrate-resistant prostate cancer. Urol. Oncol.Semin. Orig. Investig. 2014, 32, 31–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cetnar, J.; Wilding, G.; McNeel, D.; Loconte, N.K.; McFarland, T.A.; Eickhoff, J.; Liu, G. A phase 1/1b study of Satraplatin (JM-216) in combination with Docetaxel in patients with advanced solid tumors and metastatic castrate-resistant prostate cancer. Urol. Oncol. Semin. Orig. Investig. 2013, 31, 436–441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Figg, W.D.; Chau, C.H.; Madan, R.A.; Gulley, J.L.; Gao, R.; Sissung, T.M.; Spencer, S.; Beatson, M.; Aragon-Ching, J.; Steinberg, S.M.; et al. Phase II study of Satraplatin and Prednisone in patients with metastatic castration-resistant prostate cancer: A pharmacogenetic assessment of outcome and toxicity. Clin. Genitourin. Cancer 2013, 11, 229–237. [Google Scholar] [CrossRef] [Green Version]
- Di Paola, E.D.; Alonso, S.; Giuliani, R.; Calabrò, F.; D’Alessio, A.; Regine, G.; Cerbone, L.; Bianchi, L.; Mancuso, A.; Sperka, S.; et al. An open-label, dose-finding study of the combination of Satraplatin and Gemcitabine in patients with advanced solid tumors. Front. Oncol. 2012, 2, 175. [Google Scholar] [CrossRef] [Green Version]
- Qi, L.; Luo, Q.; Zhang, Y.; Jia, F.; Zhao, Y.; Wang, F. Advances in toxicological research of the anticancer drug Cisplatin. Chem. Res. Toxicol. 2019, 32, 1469–1486. [Google Scholar] [CrossRef]
- Chung, M.K.; Kim, J.C.; Roh, J.K. Embryotoxic effects of SKI 2053R, a new potential anticancer agent, in rats. Reprod. Toxicol. 1998, 12, 375–381. [Google Scholar] [CrossRef]
- Miller, R.P.; Tadagavadi, R.K.; Ramesh, G.; Reeves, W.B. Mechanisms of Cisplatin nephrotoxicity. Toxins 2010, 2, 2490–2518. [Google Scholar] [CrossRef] [Green Version]
- Ahn, J.H.; Kang, Y.K.; Kim, T.W.; Bahng, H.; Chang, H.M.; Kang, W.C.; Kim, W.K.; Lee, J.S.; Park, J.S. Nephrotoxicity of Heptaplatin: A randomized comparison with Cisplatin in advanced gastric cancer. Cancer Chemother. Pharmacol. 2002, 50, 104–110. [Google Scholar] [CrossRef]
- Waissbluth, S.; Daniel, S.J. Cisplatin-induced ototoxicity: Transporters playing a role in Cisplatintoxicity. Heart Res. 2013, 299, 37–45. [Google Scholar] [CrossRef]
- Basu, A.; Krishnamurthy, S. Cellular responses to Cisplatin-induced DNA damage. J. Nucleic Acids 2010, 2010, 201367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sawant, A.; Kothandapani, A.; Zhitkovich, A.; Sobol, R.W.; Patrick, S.M. Role of mismatch repair proteins in the processing of Cisplatin interstrand cross-links. DNA Repair 2015, 35, 126–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dilruba, S.; Kalayda, G.V. Platinum-based drugs: Past, present and future. Cancer Chemother. Pharmacol. 2016, 77, 1103–1124. [Google Scholar] [CrossRef] [PubMed]
- Apps, M.G.; Choi, E.H.Y.; Wheate, N.J. The state-of-play and future of platinum drugs. Endocr. Relat. Cancer 2015, 22, 219–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, J.; Wei, Q.; Zhou, Y.; Wang, J.; Liu, Q.; Xu, H. A systematic analysis of FDA-approved anticancer drugs. BMC Syst. Biol. 2017, 11, 28–43. [Google Scholar] [CrossRef] [PubMed]
- De Luca, A.; Parker, L.J.; Ang, W.H.; Rodolfo, C.; Gabbarini, V.; Hancock, N.C.; Palone, F.; Mazzetti, A.P.; Menin, L.; Morton, C.J.; et al. A structure-based mechanism of cisplatin resistance mediated by glutathione transferase P1-1. Proc. Natl. Acad. Sci. USA 2019, 116, 13943–13951. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abada, P.; Howell, S.B. Regulation of Cisplatin cytotoxicity by Cu-influx transporters. Met.-Based Drugs. 2010, 2010, 317581. [Google Scholar] [CrossRef] [Green Version]
- Bompiani, K.M.; Tsai, C.Y.; Achatz, F.P.; Liebig, J.K.; Howell, S.B. Copper transporters and chaperones CTR1, CTR2, ATOX1, and CCS as determinants of Cisplatin sensitivity. Metallomics 2016, 8, 951–962. [Google Scholar] [CrossRef] [Green Version]
- Akerfeldt, M.C.; Tran, C.M.N.; Shen, C.; Hambley, T.W.; New, E.J. Interactions of Cisplatin and the copper transporter CTR1 in human colon cancer cells. J. Biol. Inorg. Chem. 2017, 22, 765–774. [Google Scholar] [CrossRef]
- Buss, I.; Hamacher, A.; Sarin, N.; Kassack, M.U.; Kalayda, G.V. Relevance of copper transporter 1 and organic cation transporters 1-3 for oxaliplatin uptake and drug resistance in colorectal cancer cells. Metallomics 2018, 10, 414–425. [Google Scholar] [CrossRef]
- Blair, B.G.; Larson, C.A.; Safaei, R.; Howell, S.B. Copper transporter 2 regulates the cellular accumulation and cytotoxicity of Cisplatin and Carboplatin. Clin. Cancer Res. 2009, 15, 4312–4321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fu, S.; Naing, A.; Fu, C.; Kuo, M.T.; Kurzrock, R. Overcoming platinum resistance through the use of a copper-lowering agent. Mol. Cancer Ther. 2012, 11, 1221–1225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shen, D.W.; Pouliot, L.M.; Hall, M.D.; Gottesman, M.M. Cisplatin resistance: A cellular self-defense mechanism resulting from multiple epigenetic and genetic changes. Pharmacol. Rev. 2012, 64, 706–721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan, H.; Cai, N.; Li, M.; Liu, G.H.; Izpisua-Belmonte, J.C. Autophagic control of cell ‘stemness’. EMBO Mol. Med. 2013, 5, 327–331. [Google Scholar] [CrossRef]
- Ma, L.; Xu, Y.; Su, J.; Yu, H.; Kang, J.; Li, H.; Li, X.; Xie, Q.; Yu, C.; Sun, L.; et al. Autophagic flux promotes Cisplatin resistance in human ovarian carcinoma cells through ATP mediated lysosomal function. Int. J. Oncol. 2015, 47, 1890–1900. [Google Scholar] [CrossRef] [Green Version]
- Yu, L.; Gu, C.; Zhong, D.; Shi, L.; Kong, Y.; Zhou, Z.; Liu, S. Induction of autophagy counteracts the anticancer effect of Cisplatin in human esophageal cancer cells with acquired drug resistance. Cancer Lett. 2014, 355, 34–45. [Google Scholar] [CrossRef]
- Yang, H.Z.; Ma, Y.; Zhou, Y.; Xu, L.M.; Chen, X.J.; Ding, W.B.; Zou, H. Autophagy contributes to the enrichment and survival of colorectal cancer stem cells under Oxaliplatin treatment. Cancer Lett. 2015, 361, 128–136. [Google Scholar] [CrossRef]
- Suntharalingam, K.; Wilson, J.J.; Lin, W.; Lippard, S.J. A dual-targeting, p53-independent, apoptosis-inducing platinum (II) anticancer complex, [Pt(BDI(QQ))]Cl. Metallomics 2014, 6, 437–443. [Google Scholar] [CrossRef] [Green Version]
- Goh, A.M.; Coffill, C.R.; Lane, D.P. The role of mutant p53 in human cancer. J. Pathol. 2011, 223, 116–126. [Google Scholar] [CrossRef]
- Xie, X.; He, G.; Siddik, Z.H. Functional activation of mutant P53 by platinum analogues in Cisplatin-resistant cells is dependent on phosphorylation. Mol. Cancer Res. 2016, 15, 328–339. [Google Scholar] [CrossRef] [Green Version]
- Bykov, V.J.N.; Eriksson, S.E.; Bianchi, J.; Wiman, K.G. Targeting mutant p53 for efficient cancer therapy. Nat. Rev.Cancer 2018, 18, 89–102. [Google Scholar] [CrossRef] [PubMed]
- Mi, Q.; Shu, S.; Yang, C.; Gao, C.; Zhang, X.; Luo, X.; Bao, C.; Zhang, X.; Niu, J. Current status for oral platinum (IV) anticancer drug development. Int. J. Med. Phys. Clin. Eng. Radiat. Oncol. 2018, 7, 231–247. [Google Scholar] [CrossRef] [Green Version]
- Kelland, L.R. Overcoming resistance to platinum therapy in patients with advances cancer. Am. J. Cancer 2002, 1, 247–255. [Google Scholar] [CrossRef]
- Dempke, W.; Voigt, W.; Grothey, A.; Hill, B.T.; Schmoll, H.J. Cisplatin resistance and oncogenes—A review. Anti-Cancer Drugs 2000, 11, 225–236. [Google Scholar] [CrossRef] [PubMed]
- Feldman, D.R.; Bosl, G.J.; Sheinfeld, J.; Motzer, R.J. Medical treatment of advanced testicular cancer. JAMA 2008, 299, 672–684. [Google Scholar] [CrossRef] [Green Version]
- Wolff, R.K.; Hoffman, M.D.; Wolff, E.C.; Herrick, J.S.; Sakoda, L.C.; Samowitz, W.S.; Slattery, M.L. Mutation analysis of adenomas and carcinomas of the colon: Early and late drivers. Genes Chromosomes Cancer 2018, 57, 366–376. [Google Scholar] [CrossRef]
- Köberle, B.; Schoch, S. Platinum complexes in colorectal cancer and other solid tumors. Cancers 2021, 13, 2073. [Google Scholar] [CrossRef]
- Amable, L. Cisplatin resistance and opportunities for precision medicine. Pharm. Res. 2016, 106, 27–36. [Google Scholar] [CrossRef]
- Boulikas, T.; Pantos, A.; Bellis, E.; Christofis, P. Designing platinum compounds in cancer: Structures and mechanisms. Cancer Ther. 2007, 5, 537–583. [Google Scholar]
- Johnstone, T.C.; Wilson, J.J.; Lippard, S.J. Monofunctional and higher-valent platinum anticancer agents. Inorg. Chem. 2013, 52, 12234–12249. [Google Scholar] [CrossRef] [Green Version]
- Gibson, D. Platinum (IV) anticancer prodrugs–hypotheses and facts. Dalton. Trans. 2016, 45, 12983–12991. [Google Scholar] [CrossRef] [PubMed]
- Yao, M. Current status and future prospects for Satraplatin, an oral platinum analogue. Clin. Cancer Res. 2008, 14, 1633–1638. [Google Scholar] [CrossRef] [Green Version]
- Gifford, G.; Paul, J.; Vasey, P.A.; Kaye, S.B.; Brown, R. The acquisition of hMLH1 methylation in plasma DNA after chemotherapy predicts poor survival for ovarian cancer patients. Clin. Cancer Res. 2004, 10, 4420–4426. [Google Scholar] [CrossRef] [Green Version]
- Hurley, L.H. DNA and it’s associated processes as targets for cancer therapy. Nat. Rev. Cancer 2002, 2, 188–200. [Google Scholar] [CrossRef] [PubMed]
- Espinosa, E.; Zamora, P.; Feliu, J.; Baron, M.G. Classification of anticancer drugs–a new system based on therapeutic targets. Cancer Treat. Rev. 2003, 29, 515–523. [Google Scholar] [CrossRef]
- Eyck, B.M.; van Lanschot, J.J.B.; Hulshof, M.C.C.M.; van der Wilk, B.J.; Shapiro, J.; van Hagen, P.; van Berge-Henegouwen, M.I.; Wijnhoven, B.P.L.; van Laarhoven, H.W.M.; Nieuwenhuijzen, G.A.P.; et al. Ten-year outcome of neoadjuvant chemoradiotherapy plus surgery for esophageal cancer: The randomized controlled CROSS. Trial. J. Clin. Oncol. 2021, 39, 1995–2004. [Google Scholar] [CrossRef] [PubMed]
- Hitt, R.; López-Pousa, A.; Martínez-Trufero, J.; Escrig, V.; Carles, J.; Rizo, A.; Isla, D.; Vega, M.E.; Martí, J.L.; Lobo, F.; et al. Phase III study comparing Cisplatin plus Fluorouracil to Paclitaxel, Cisplatin, and Fluorouracil induction chemotherapy followed by chemoradiotherapy in locally advanced head and neck cancer. J. Clin. Oncol. 2005, 23, 8636–8645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nair, A.G.; Kaliki, S.; Mishra, D.K.; Reddy, V.A.; Naik, M.N. Neoadjuvant chemotherapy for invasive squamous cell carcinoma of the conjunctiva: A case report. Indian J. Ophthalmol. 2015, 63, 927–929. [Google Scholar] [CrossRef]
- Jin, T.; Qin, W.F.; Jiang, F.; Jin, Q.F.; Wei, Q.C.; Jia, Y.S.; Sun, X.N.; Li, W.F.; Chen, X.Z. Cisplatin and Fluorouracil induction chemotherapy with or without Docetaxel in locoregionally advanced nasopharyngeal carcinoma. Transl. Oncol. 2019, 12, 633–639. [Google Scholar] [CrossRef]
- Celio, L.; Sternberg, C.N.; Labianca, R.; La Torre, I.; Amoroso, V.; Barone, C.; Pinotti, G.; Cascinu, S.; Di Costanzo, F.; Cetto, G.L.; et al. Pemetrexed in combination with Oxaliplatin as a first-line therapy for advanced gastric cancer: A multi-institutional phase II study. Ann. Oncol. 2009, 20, 1062–1067. [Google Scholar] [CrossRef]
- Zapatero, A.; de Vidales, M.C.; Arellano, R.; Ibañez, Y.; Bocardo, G.; Perez, M.; Rabadan, M.; García, V.F.; Cruz, C.J.A.; Olivier, C. Long-term results of two prospective bladder-sparing trimodality approaches for invasive bladder cancer: Neoadjuvant chemotherapy and concurrent radio-chemotherapy. Urology 2012, 80, 1056–1062. [Google Scholar] [CrossRef] [PubMed]
- Klopp, A.H.; Eifel, P.J.; Berek, J.S.; Konstantinopoulos, P.A. Cancer of the cervix, vagina and vulva. In Cancer: Principles and Practice of Oncology, 10th ed.; De Vita, V.T., Lawrence, T.S., Rosenberg, S.A., Eds.; Wolters Kluwer Health/Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2015; Volume 72, pp. 1013–1047. [Google Scholar]
- Ishigami, H.; Fujiwara, Y.; Fukushima, R.; Nashimoto, A.; Yabusaki, H.; Imano, M.; Imamoto, H.; Kodera, Y.; Uenosono, Y.; Amaga, K.; et al. Phase III trial comparing Intraperitoneal and intravenous Paclitaxel plus S-1 versus Cisplatin plus S-1 in patients with gastric cancer with peritoneal metastasis: PHOENIX-GCtrial. J. Clin. Oncol. 2018, 36, 1922–1929. [Google Scholar] [CrossRef] [PubMed]
- Aoki, Y.; Ochiai, K.; Lim, S.; Aoki, D.; Kamiura, S.; Lin, H.; Katsumata, N.; Cha, S.D.; Kim, J.H.; Kim, B.G.; et al. PhaseIIIstudyofCisplatinwithorwithoutS-1 inpatientswithstageIVB, recurrent, orpersistentcervicalcancer. Br. J. Cancer 2018, 119, 530–537. [Google Scholar] [CrossRef] [PubMed]
- Hu, X.C.; Zhang, J.; Xu, B.H.; Cai, L.; Ragaz, J.; Wang, Z.H.; Wang, B.Y.; Teng, Y.E.; Tong, Z.S.; Pan, Y.Y.; et al. Cisplatin plus Gemcitabine versus Paclitaxel plus Gemcitabine as first-line therapy for metastatic triple-negative breast cancer (CBCSG006): A randomised, open-label, multicentre, phase 3 trial. Lancet Oncol. 2015, 16, 436–446. [Google Scholar] [CrossRef]
- Liu, G.F.; Li, G.J.; Zhao, H. Efficacy and toxicity of different chemotherapy regimens in the treatment of advanced or metastatic pancreatic cancer: A network meta-analysis. J. Cell Biochem. 2018, 119, 511–523. [Google Scholar] [CrossRef] [PubMed]
- Kehoe, S.; Hook, J.; Nankivell, M.; Jayson, G.C.; Kitchener, H.; Lopes, T.; Luesley, D.; Perren, T.; Bannoo, S.; Mascarenhas, M.; et al. Primary chemotherapy versus primary surgery for newly diagnosed advanced ovarian cancer (CHORUS): An open-label, randomised, controlled, non-inferiority trial. Lancet 2015, 386, 249–257. [Google Scholar] [CrossRef]
- Dueñas-González, A.; Zarbá, J.J.; Patel, F.; Alcedo, J.C.; Beslija, S.; Casanova, L.; Pattaranutaporn, P.; Hameed, S.; Blair, J.M.; Barraclough, H.; et al. Phase III, open-label, randomized study comparing concurrent Gemcitabine plus Cisplatin and radiation followed by adjuvant Gemcitabine and Cisplatin versus concurrent Cisplatin and radiation in patients with stage IIB to IVA carcinoma of the cervix. J. Clin. Oncol. 2011, 29, 1678–1685. [Google Scholar] [CrossRef]
- Birtle, A.; Johnson, M.; Chester, J.; Jones, R.; Dolling, D.; Bryan, R.T.; Harris, C.; Winterbottom, A.; Blacker, A.; Catto, J.W.F.; et al. Adjuvant chemotherapy in upper tract urothelial carcinoma (thePOUTtrial): A phase 3, open-label, randomised controlled trial. Lancet 2020, 395, 1268–1277. [Google Scholar] [CrossRef]
- Paz-Ares, L.; deMarinis, F.; Dediu, M.; Thomas, M.; Pujol, J.L.; Bidoli, P.; Molinier, O.; Sahoo, T.P.; Laack, E.; Reck, M.; et al. Maintenance therapy with Pemetrexed plus best supportive care versus placebo plus best supportive care after induction therapy with Pemetrexed plus Cisplatin for advanced non-squamous non-small-cell lung cancer (PARAMOUNT): A double-blind, phase 3, randomised controlle dtrial. Lancet Oncol. 2012, 13, 247–255. [Google Scholar] [CrossRef]
- Sehouli, J.; Chekerov, R.; Reinthaller, A.; Richter, R.; Gonzalez-Martin, A.; Harter, P.; Woopen, H.; Petru, E.; Hanker, L.C.; Keil, E.; et al. Topotecan plus Carboplatin versus standard therapy with Paclitaxel plus Carboplatin (PC) or Gemcitabine plus Carboplatin (GC) or pegylated liposomal Doxorubicin plus Carboplatin (PLDC): A randomized phase III trial of the NOGGO-AGO-Study Group-AGO Austria and GEICO-ENGOT-GCIG intergroup study (HECTOR). Gynecol. Tumors 2016, 27, 2236–2241. [Google Scholar] [CrossRef]
- Souglakos, J.; Boukovinas, I.; Kakolyris, S.; Xynogalos, S.; Ziras, N.; Athanasiadis, A.; Androulakis, N.; Christopoulou, A.; Vaslamatzis, M.; Ardavanis, A.; et al. Three versus six months adjuvant FOLFOX or CAPOX for high risk stage II and stage III colon cancer patients: The efficacy results of Hellenic Oncology Research Group (HORG) participation to the InternationalDuration Evaluation of Adjuvant chemotherapy (IDEA) project. Ann. Oncol. 2019, 30, 1304–1310. [Google Scholar] [CrossRef]
- Snoeren, N.; vanHillegersberg, R.; Schouten, S.B.; Bergman, A.M.; vanWerkhoven, E.; Dalesio, O.; Tollenaar, R.A.; Verheul, H.M.; vanderSijp, J.; Borel, R.I.H.; et al. Randomized phase III study to assess efficacy and safety of adjuvant CAPOX with or without Bevacizumab in patients after resection of colorectal liver metastases: HEPATICA study. Neoplasia 2017, 19, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Iveson, T.J.; Kerr, R.S.; Saunders, M.P.; Cassidy, J.; Hollander, N.H.; Tabernero, J.; Haydon, A.; Glimelius, B.; Harkin, A.; Allan, K.; et al. 3 versus 6 months of adjuvant Oxaliplatin-fluoropyrimidine combination therapy for colorectal cancer (SCOT): An international, randomised, phase 3, non-inferiority trial. Lancet Oncol. 2018, 19, 562–578. [Google Scholar] [CrossRef] [Green Version]
- Ducreux, M.; Mitry, E.; Ould-Kaci, M.; Boige, V.; Seitz, J.F.; Bugat, R.; Breau, J.L.; Bouché, O.; Etienne, P.L.; Tigaud, J.M.; et al. Randomized phase II study evaluating Oxaliplatin alone, Oxaliplatin combined with infusional 5-FU, and infusional 5-FU alone in advanced pancreatic carcinoma patients. Ann. Oncol. 2004, 15, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Droz, J.P.; Muracciole, X.; Mottet, N.; Ould, K.M.; Vannetzel, J.M.; Albin, N.; Culine, S.; Rodier, J.M.; Misset, J.L.; Mackenzie, S.; et al. Phase II study of Oxaliplatin versus Oxaliplatin combined with infusional 5-Fluorouracil in hormone refractory metastatic prostate cancer patients. Ann. Oncol. 2003, 14, 1291–1298. [Google Scholar] [CrossRef] [PubMed]
- Sunami, E.; Kusumoto, T.; Ota, M.; Sakamoto, Y.; Yoshida, K.; Tomita, N.; Maeda, A.; Teshima, J.; Okabe, M.; Tanaka, C.; et al. S-1 and Oxaliplatin versus Tegafur-uracil and Leucovorin as postoperative adjuvant chemotherapy in patients with high-risk stage III colon cancer (ACTS-CC 02): A randomized, open-label, multicenter, phase 3, superiority trial. Clin. Colorectal Cancer 2020, 19, 22–31.e6. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.L.; Ahn, J.H.; Choi, M.K.; Kim, Y.; Hong, S.W.; Lee, K.H.; Jeong, I.G.; Song, C.; Hong, B.S.; Hong, J.H.; et al. Gemcitabine–Oxaliplatin plus Prednisolone is active in patients with castration-resistant prostate cancer for whom Docetaxel-based chemotherapy failed. Br. J. Cancer 2014, 110, 2472–2478. [Google Scholar] [CrossRef] [Green Version]
- De Giorgi, U.; Rosti, G.; Aieta, M.; Testore, F.; Burattini, L.; Fornarini, G.; Naglieri, E.; Lo-Re, G.; Zumaglini, F.; Marangolo, M. Phase II study of Oxaliplatin and Gemcitabine salvage chemotherapy in patients with Cisplatin-refractory nonseminomatous germ cell tumor. Eur. Urol. 2006, 50, 1032–1038. [Google Scholar] [CrossRef]
- Gilbert, J.; Murphy, B.; Dietrich, M.S.; Henry, E.; Jordan, R.; Counsell, A.; Wirth, P.; Yarbrough, W.G.; Slebos, R.J.; Chung, C.H. Phase 2 trial of Oxaliplatin and Pemetrexed as an induction regimen in locally advanced head and neck cancer. Cancer 2012, 118, 1007–1013. [Google Scholar] [CrossRef]
- Alberts, S.R.; Kim, G.P.; Mahoney, M.R.; Gornet, M.K.; Rubin, J.; Ames, M.; Goetz, M.P.; Weinshilboum, R.M.; Nicol, S.J.; Goldberg, R.M. Pemetrexed and Oxaliplatin for metastatic colorectal cancer: Results of a phase I Mayo Cancer Center Research Consortium trial, MC0248. Clin. Colorectal Cancer 2007, 6, 572–577. [Google Scholar] [CrossRef]
- Dorff, T.B.; Tsao-Wei, D.D.; Groshen, S.; Boswell, W.; Goldkorn, A.; Xiong, S.; Quinn, D.I.; Pinski, J.K. Efficacy of Oxaliplatin plus Pemetrexed in chemotherapy pretreated metastatic castration-resistant prostate cancer. Clin. Genitourin. Cancer 2013, 11, 416–422. [Google Scholar] [CrossRef] [PubMed]
- Peng, P.J.; Ou, X.Q.; Chen, Z.B.; Liao, H.; Peng, Y.L.; Wang, S.Y.; Zhang, H.Y.; Lin, Z. Multicenter phase II study of Capecitabine combined with Nedaplatin for recurrent and metastatic nasopharyngeal carcinoma patients after failure of Cisplatin-based chemotherapy. Cancer Chemother. Pharmacol. 2013, 72, 323–328. [Google Scholar] [CrossRef] [PubMed]
- Walko, C.M.; Lindley, C. Capecitabine: A review. Clin. Ther. 2005, 27, 23–44. [Google Scholar] [CrossRef] [PubMed]
- Longley, D.B.; Harkin, D.P.; Johnston, P.G. 5-Fluorouracil: Mechanisms of action and clinical strategies. Nat. Rev. Cancer 2003, 3, 330–338. [Google Scholar] [CrossRef] [PubMed]
- Hazarika, M.; White, R.M.; Johnson, J.R.; Pazdur, R. FDA drug approval summaries: Pemetrexed (Alimta). Oncologist 2004, 9, 482–488. [Google Scholar] [CrossRef]
- Oh, I.J.; Kim, K.S.; Park, C.K.; Kim, Y.C.; Lee, K.H.; Jeong, J.H.; Kim, S.Y.; Lee, J.E.; Shin, K.C.; Jang, T.W.; et al. Belotecan/Cisplatin versus Etoposide/Cisplatin in previously untreated patients with extensive-stage small cell lung carcinoma: A multi-center randomized phase III trial. BMC Cancer 2016, 16, 690. [Google Scholar] [CrossRef] [Green Version]
- Theodore, C.; Skoneczna, I.; Bodrogi, I.; Leahy, M.; Kerst, J.M.; Collette, L.; Ven, K.; Marréaud, S.; Oliver, R.D.T.; EORTC Genito-Urinary Tract Cancer Group. A phase II multicentre study of Irinotecan (CPT 11) in combination with Cisplatin (CDDP) in metastatic or locally advanced penile carcinoma (EORTC PROTOCOL 30992). Ann. Oncol. 2008, 19, 1304–1307. [Google Scholar] [CrossRef]
- Dong, J.; Li, B.; Lin, D.; Zhou, Q.; Huang, D. Advances in targeted therapy and immunotherapy for non–small cell lung cancer based on accurate molecular typing. Front. Pharmacol. 2019, 10, 230. [Google Scholar] [CrossRef]
- Ito, K.; Kobayashi, M.; Komiyama, M.; Naito, S.; Nishimura, K.; Yonese, J.; Hashine, K.; Saito, S.; Arai, G.; Shinohara, M.; et al. Oncological outcomes for patients with locally advanced prostate cancer treated with neoadjuvant endocrine and external-beam radiation therapy followed by adjuvant continuous/intermittent endocrine therapy in an open-label, randomized, phase 3 trial. Cancer 2020, 126, 3961–3971. [Google Scholar] [CrossRef]
- Bosl, G.J.; Geller, N.L.; Bajorin, D.; Leitner, S.P.; Yagoda, A.; Golbey, R.B.; Scher, H.; Vogelzang, N.J.; Auman, J.; Carey, R.; et al. A randomized trial of Etoposide + Cisplatin versus Vinblastine + Bleomycin + Cisplatin + Cyclophosphamide + Dactinomycin in patients with good-prognosis germ cell tumors. J. Clin. Oncol. 1988, 6, 1231–1238. [Google Scholar] [CrossRef]
- de Boer, S.M.; Powell, M.E.; Mileshkin, L.; Katsaros, D.; Bessette, P.; Haie-Meder, C.; Ottevanger, P.B.; Ledermann, J.A.; Khaw, P.; Colombo, A.; et al. Adjuvant chemoradiotherapy versus radiotherapy alone for women with high-risk endometrial cancer (PORTEC-3): Final results of an international, open-label, multicentre, randomised, phase 3 trial. Lancet Oncol. 2018, 19, 295–309. [Google Scholar] [CrossRef] [Green Version]
- Lorch, A.; Kleinhans, A.; Kramar, A.; Kollmannsberger, C.K.; Hartmann, J.T.; Bokemeyer, C.; Rick, O.; Beyer, J. Sequential versus single high-dose chemotherapy in patients with relapsed or refractory germ cell tumors: Long-term results of a prospective randomized trial. J. Clin. Oncol. 2012, 30, 800–805. [Google Scholar] [CrossRef] [PubMed]
- Compostella, A.; Affinita, M.C.; Casanova, M.; Milano, J.M.; Scagnellato, A.; Dall’Igna, P.; Chiaravalli, S.; Pierobon, M.; Manzitti, C.; Zanetti, I.; et al. Topotecan/Carboplatin regimen for refractory/recurrent rhabdomyosarcoma in children: Report from the AIEOP Soft Tissue Sarcoma Committee. Tumori J. 2019, 105, 138–143. [Google Scholar] [CrossRef] [PubMed]
- Zhaowei, Z.; Tianzi, F.; Jianxia, L. Study of the efficacy and safty of Irinotecan combined with Nedaplatin versus Topotecan combined with Nedaplatin in treatment of small lung cancer. Chin. J. Clin. Pharmacol. Ther. 2017, 22, 943–947. [Google Scholar]
- Pommier, Y.; Leo, E.; Zhang, H.; Marchand, C. DNA topoisomerases and their poisoning by anticancer and antibacterial drugs. Chem. Biol. 2010, 17, 421–433. [Google Scholar] [CrossRef] [Green Version]
- Raymond, E.; Faivre, S.; Armand, J.P. Epidermal growth factor receptor tyrosine kinase as a target for anticancer therapy. Drugs 2000, 60 (Suppl. S1), 15–23. [Google Scholar] [CrossRef]
- Bailly, C. Irinotecan: 25 years of cancer treatment. Pharmacol. Res. 2019, 148, 104398. [Google Scholar] [CrossRef]
- Fan, Y.; Xu, B.H.; Yuan, P.; Ma, F.; Wang, J.Y.; Ding, X.Y.; Zhang, P.; Li, Q.; Cai, R.G. Docetaxel-Cisplatin might be superior to Docetaxel-Capecitabine in the first-line treatment of metastatic triple-negative breast cancer. Ann. Oncol. 2013, 24, 1219–1225. [Google Scholar] [CrossRef]
- Li, M.; Fan, Y.; Li, Q.; Zhang, P.; Yuan, P.; Ma, F.; Wang, J.; Luo, Y.; Cai, R.; Chen, S.; et al. Vinorelbine plus platinum in patients with metastatic triple negative breast cancer and prior anthracycline and taxane treatment. Medicine 2015, 94, e1928. [Google Scholar] [CrossRef]
- Sharma, P.; López-Tarruella, S.; García-Saenz, J.A.; Ward, C.; Connor, C.S.; Gómez, H.L.; Prat, A.; Moreno, F.; Jerez-Gilarranz, Y.; Barnadas, A.; et al. Efficacy of neoadjuvant Carboplatin plus Docetaxel in triple-negative breast cancer: Combined analysis of two cohorts. Clin. Cancer Res. 2017, 23, 649–657. [Google Scholar] [CrossRef] [Green Version]
- Yu, K.D.; Ye, F.G.; He, M.; Fan, L.; Ma, D.; Mo, M.; Wu, J.; Liu, G.Y.; Di, G.H.; Zeng, X.H.; et al. Effect of adjuvant Paclitaxel and Carboplatin on survival in women with triple-negative breast cancer: A phase 3 randomized clinical trial. JAMA Oncol. 2020, 6, 1390–1396. [Google Scholar] [CrossRef] [PubMed]
- Kentepozidis, N.; Soultati, A.; Giassas, S.; Vardakis, N.; Kalykaki, A.; Kotsakis, A.; Papadimitraki, E.; Pantazopoulos, N.; Bozionellou, V.; Georgoulias, V.; et al. Paclitaxel in combination with Carboplatin as salvage treatment in patients with castration-resistant prostate cancer: A Hellenic Oncology Research Group multicenter phase II study. Cancer Chemother. Pharmacol. 2012, 70, 161–168. [Google Scholar] [CrossRef] [PubMed]
- Gluz, O.; Nitz, U.; Liedtke, C.; Christgen, M.; Grischke, E.M.; Forstbauer, H.; Braun, M.; Warm, M.; Hackmann, J.; Uleer, C.; et al. Comparison of neoadjuvant Nab-Paclitaxel + Carboplatin vs Nab-Paclitaxel + Gemcitabine in triple-negative breast cancer: Randomized WSG-ADAPT-TN trial results. J. Natl. Cancer Inst. 2018, 110, 628–637. [Google Scholar] [CrossRef]
- Corn, P.G.; Heath, E.I.; Zurita, A.; Ramesh, N.; Xiao, L.; Sei, E.; Li-Ning-Tapia, E.; Tu, S.M.; Subudhi, S.K.; Wang, J.; et al. Cabazitaxel plus Carboplatin for the treatment of men with metastatic castration-resistant prostate cancers: A randomised, open-label, phase 1-2 trial. Lancet Oncol. 2019, 20, 1432–1443. [Google Scholar] [CrossRef]
- Rayan, A.; Fattah, O.N.A.; Soliman, A.; Hasan, H.A.; Zahran, A.M. Efficacy of Docetaxel and Oxaliplatin regimen as a second-line therapy for patients with advanced pancreatic adenocarcinoma. J. Gastrointest. Cancer 2019, 50, 519–524. [Google Scholar] [CrossRef] [PubMed]
- Winegarden, J.D.; Mauer, A.M.; Otterson, G.A.; Rudin, C.M.; Villalona-Calero, M.A.; Lanzotti, V.J.; Szeto, L.; Kasza, K.; Hoffman, P.C.; Vokes, E.E. A phase II study of Oxaliplatin and Paclitaxel in patients with advanced non-small-cell lung cancer. Ann. Oncol. 2004, 15, 915–920. [Google Scholar] [CrossRef] [PubMed]
- Viens, P.; Bougnoux, P.; Rixe, O.; Petit, T.; Laadem, A.; Cottu, P.; Delva, R.; Burki, F.; Goupil, A.; Extra, J.M. A phase II trial of a Paclitaxel and Oxaliplatin combination in advanced ovarian cancer patients pretreated with Cisplatin or Carboplatin ± taxanes: Preliminary results. Eur. J. Cancer 2001, 37 (Suppl. S6), S323. [Google Scholar] [CrossRef]
- Zhang, J.; Wang, L.; Wang, Z.; Hu, X.; Wang, B.; Cao, J.; Lv, F.; Zhen, C.; Zhang, S.; Shao, Z. A phase II trial of biweekly Vinorelbine and Oxaliplatin in second- or third-line metastatic triple-negative breast cancer. Cancer Biol. Ther. 2015, 16, 225–232. [Google Scholar] [CrossRef] [Green Version]
- Lu, J.; Ying, H.C.; Xue, W. Clinical observation of Nedaplatin combined with Vinorelbine in the treatment of advanced non-small cell lung cancer. China Med. Herald 2009, 7, 50–51. [Google Scholar]
- Shipley, D.; Spigel, D.R.; Cavanaugh, C.; Moore, Y.; Hainsworth, J.D.; Jones, S.; Burris, H.A.; Sade, L.; Yardley, D.A.; Greco, F. Phase II trial of Satraplatin and Paclitaxel in the first-line treatment of advanced non-small cell lung cancer. J. Clin. Oncol. 2007, 25 (Suppl. S18), 18073. [Google Scholar] [CrossRef]
- Jordan, M.A.; Wilson, L. Microtubules as a target for anticancer drugs. Nat. Rev. Cancer 2004, 4, 253–265. [Google Scholar] [CrossRef] [PubMed]
- Gelman, J.S.; Sironi, J.; Berezniuk, I.; Dasgupta, S.; Castro, L.M.; Gozzo, F.C.; Ferro, E.S.; Fricker, L.D. Alterations of the intracellular peptidome in response to the proteasome inhibitor Bortezomib. PLoS ONE 2013, 8, e53263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Barta, J.A.; Powell, C.A.; Wisnivesky, J.P. Global epidemiology of lung vancer. Ann. Glob. Health 2019, 85, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Booton, R.; Lorigan, P.; Anderson, H.; Baka, S.; Ashcroft, L.; Nicolson, M.; O’Brien, M.; Dunlop, D.; O’Byrne, K.; Laurence, V.; et al. A phase III trial of Docetaxel/Carboplatin versus Mitomycin C/Ifosfamide/Cisplatin (MIC) or Mitomycin C/Vinblastine/Cisplatin (MVP) in patients with advanced non-small-cell lung cancer: A randomised multicentre trial of the British Thoracic Oncology Group (BTOG1). Ann. Oncol. 2006, 17, 1111–1119. [Google Scholar] [CrossRef] [PubMed]
- Herbst, R.S.; Redman, M.W.; Kim, E.S.; Semrad, T.J.; Bazhenova, L.; Masters, G.; Oettel, K.; Guaglianone, P.; Reynolds, C.; Karnad, A.; et al. Cetuximab plus Carboplatin and Paclitaxel with or without Bevacizumab versus Carboplatin and Paclitaxel with or without Bevacizumab in advanced NSCLC (SWOG S0819): A randomised, phase 3 study. Lancet Oncol. 2018, 19, 101–114. [Google Scholar] [CrossRef] [Green Version]
- Kosmidis, P.; Mylonakis, N.; Fountzilas, G.; Pavlidis, N.; Samantas, E.; Karabelis, A.; Kattis, K.; Skarlos, D. A prospective randomized phase III study in non-small-cell lung cancer comparing Cisplatin, Ifosfamide, Vinblastine (VIP) versus Cisplatin, Ifosfamide and Etoposide (VIP-16). Hellenic Co-Operative Oncology Group. Ann. Oncol. 1996, 7, 517–520. [Google Scholar] [CrossRef]
- Comella, P.; Filippelli, G.; De Cataldis, G.; Massidda, B.; Frasci, G.; Maiorino, L.; Putzu, C.; Mancarella, S.; Palmeri, S.; Cioffi, R.; et al. Efficacy of the combination of Cisplatin with either Gemcitabine and Vinorelbine or Gemcitabine and Paclitaxel in the treatment of locally advanced or metastatic non-small-cell lung cancer: A phase III randomised trial of the Southern Italy Cooperative Oncology Group (SICOG 0101). Ann. Oncol. 2007, 18, 324–330. [Google Scholar] [CrossRef]
- Wu, Y.L.; Lee, J.S.; Thongprasert, S.; Yu, C.J.; Zhang, L.; Ladrera, G.; Srimuninnimit, V.; Sriuranpong, V.; Sandoval-Tan, J.; Zhu, Y.; et al. Intercalated combination of chemotherapy and Erlotinib for patients with advanced stage non-small-cell lung cancer (FASTACT-2): A randomised, double-blind trial. Lancet Oncol. 2013, 14, 777–786. [Google Scholar] [CrossRef]
- Bradley, J.D.; Hu, C.; Komaki, R.R.; Masters, G.A.; Blumenschein, G.R.; Schild, S.E.; Bogart, J.A.; Forster, K.M.; Magliocco, A.M.; Kavadi, V.S.; et al. Long-term results of NRG oncology RTOG 0617: Standard-versus high-dose chemoradiotherapy with or without Cetuximab for unresectable stage III non-small-cell lung cancer. J. Clin. Oncol. 2020, 38, 706–714. [Google Scholar] [CrossRef]
- Barlesi, F.; Scherpereel, A.; Rittmeyer, A.; Pazzola, A.; Ferrer-Tur, N.; Kim, J.H.; Ahn, M.J.; Aerts, J.G.J.V.; Gorbunova, V.; Vikström, A.; et al. Randomized phase III trial of maintenance Bevacizumab with or without Pemetrexed after first-line induction with Bevacizumab, Cisplatin, and Pemetrexed in advanced nonsquamous non-small-cell lung cancer: AVAPERL (MO22089). J. Clin. Oncol. 2013, 31, 3004–3011. [Google Scholar] [CrossRef] [PubMed]
- Wakelee, H.A.; Dahlberg, S.E.; Keller, S.M.; Tester, W.J.; Gandara, D.R.; Graziano, S.L.; Adjei, A.A.; Leighl, N.B.; Aisner, S.C.; Rothman, J.M.; et al. Adjuvant chemotherapy with or without Bevacizumab in patients with resected non-small-cell lung cancer (E1505): An open-label, multicentre, randomised, phase 3 trial. Lancet Oncol. 2017, 18, 1610–1623. [Google Scholar] [CrossRef]
- Paz-Ares, L.; Ciuleanu, T.E.; Cobo, M.; Schenker, M.; Zurawski, B.; Menezes, J.; Richardet, E.; Bennouna, J.; Felip, E.; Juan-Vidal, O.; et al. First-line Nivolumab plus Ipilimumab combined with two cycles of chemotherapy in patients with non-small-cell lung cancer (CheckMate 9LA): An international, randomised, open-label, phase 3 trial. Lancet Oncol. 2021, 22, 198–211. [Google Scholar] [CrossRef]
- Reck, M.; Ciuleanu, T.E.; Cobo, M.; Schenker, M.; Zurawski, B.; Menezes, J.; Richardet, E.; Bennouna, J.; Felip, E.; Juan-Vidal, O.; et al. First-line Nivolumab plus Ipilimumab with two cycles of chemotherapy versus chemotherapy alone (four cycles) in advanced non-small-cell lung cancer: CheckMate 9LA 2-year update. ESMO Open 2021, 6, 100273. [Google Scholar] [CrossRef] [PubMed]
- Rothschild, S.I.; Zippelius, A.; Eboulet, E.I.; Savic, P.S.; Betticher, D.; Bettini, A.; Früh, M.; Joerger, M.; Lardinois, D.; Gelpke, H.; et al. SAKK 16/14: Durvalumab in addition to neoadjuvant chemotherapy in patients with stage IIIA(N2) non-small-cell lungcancer-a multicenter single-arm phase II trial. J. Clin. Oncol. 2021, 39, 2872–2880. [Google Scholar] [CrossRef]
- Paccagnella, A.; Oniga, F.; Bearz, A.; Favaretto, A.; Clerici, M.; Barbieri, F.; Riccardi, A.; Chella, A.; Tirelli, U.; Ceresoli, G.; et al. Adding Gemcitabine to Paclitaxel/Carboplatin combination increases survival in advanced non-small-cell lung cancer: Results of a phase II–III study. J. Clin. Oncol. 2006, 24, 681–687. [Google Scholar] [CrossRef]
- Soria, J.C.; Tan, D.S.; Chiari, R.; Wu, Y.L.; Paz-Ares, L.; Wolf, J.; Geater, S.L.; Orlov, S.; Cortinovis, D.; Yu, C.J.; et al. First-line Ceritinib versus platinum-based chemotherapy in advanced ALK-rearranged non-small-cell lung cancer (ASCEND-4): A randomised, open-label, phase 3 study. Lancet 2017, 389, 917–929. [Google Scholar] [CrossRef]
- Rodríguez-Abreu, D.; Powell, S.F.; Hochmair, M.J.; Gadgeel, S.; Esteban, E.; Felip, E.; Speranza, G.; De Angelis, F.; Dómine, M.; Cheng, S.Y.; et al. Pemetrexed plus platinum with or without Pembrolizumab in patients with previously untreated metastatic non-squamous NSCLC: Protocol-specified final analysis from KEYNOTE-189. Ann. Oncol. 2021, 32, 881–895. [Google Scholar] [CrossRef]
- Ramalingam, S.S.; Blais, N.; Mazieres, J.; Reck, M.; Jones, C.M.; Juhasz, E.; Urban, L.; Orlov, S.; Barlesi, F.; Kio, E.; et al. Randomized, placebo-controlled, phase II study of Veliparib in combination with Carboplatin and Paclitaxel for advanced/metastatic non-small cell lung cancer. Clin. Cancer Res. 2017, 23, 1937–1944. [Google Scholar] [CrossRef] [Green Version]
- Yang, Y.; Wang, Z.; Fang, J.; Yu, Q.; Han, B.; Cang, S.; Chen, G.; Mei, X.; Yang, Z.; Ma, R.; et al. Efficacy and safety of Sintilimab plus Pemetrexed and platinum as first-line treatment for locally advanced or metastatic non-squamous NSCLC: A randomized, double-blind, phase 3 study (Oncology pRogram by InnovENT anti-PD-1-11). J. Thorac. Oncol. 2020, 15, 1636–1646. [Google Scholar] [CrossRef]
- Zhou, C.; Chen, G.; Huang, Y.; Zhou, J.; Lin, L.; Feng, J.; Wang, Z.; Shu, Y.; Shi, J.; Hu, Y.; et al. Camrelizumab plus Carboplatin and Pemetrexed versus chemotherapy alone in chemotherapy-naive patients with advanced non-squamous non-small-cell lung cancer (CameL): A randomised, open-label, multicentre, phase 3 trial. Lancet Respir. Med. 2021, 9, 305–314. [Google Scholar] [CrossRef]
- Sugawara, S.; Lee, J.S.; Kang, J.H.; Kim, H.R.; Inui, N.; Hida, T.; Lee, K.H.; Yoshida, T.; Tanaka, H.; Yang, C.T.; et al. Nivolumab with Carboplatin, Paclitaxel, and Bevacizumab for first-line treatment of advanced non-squamous non-small-cell lung cancer. Ann. Oncol. 2021, 32, 1137–1147. [Google Scholar] [CrossRef] [PubMed]
- Kubota, K.; Yoshioka, H.; Oshita, F.; Hida, T.; Yoh, K.; Hayashi, H.; Kato, T.; Kaneda, H.; Yamada, K.; Tanaka, H.; et al. Phase III, randomized, placebo-controlled, double-blind trial of Motesanib (AMG-706) in combination with Paclitaxel and Carboplatin in East Asian patients with advanced non-squamous non-small-cell lung cancer. J. Clin. Oncol. 2017, 35, 3662–3670. [Google Scholar] [CrossRef] [PubMed]
- Nishio, M.; Barlesi, F.; West, H.; Ball, S.; Bordoni, R.; Cobo, M.; Longeras, P.D.; Goldschmidt, J.; Novello, S.; Orlandi, F.; et al. Atezolizumab plus chemotherapy for first-line treatment of non-squamous NSCLC: Results from the randomized phase 3 IMpower132 trial. J. Thorac. Oncol. 2021, 16, 653–664. [Google Scholar] [CrossRef] [PubMed]
- Lu, S.; Wang, J.; Yu, Y.; Yu, X.; Hu, Y.; Ai, X.; Ma, Z.; Li, X.; Zhuang, W.; Liu, Y.; et al. Tislelizumab plus chemotherapy as first-line treatment for locally advanced or metastatic non-squamous NSCLC (RATIONALE 304): A randomized phase 3 trial. J. Thorac. Oncol. 2021, 16, 1512–1522. [Google Scholar] [CrossRef]
- Jotte, R.; Cappuzzo, F.; Vynnychenko, I.; Stroyakovskiy, D.; Rodríguez-Abreu, D.; Hussein, M.; Soo, R.; Conter, H.J.; Kozuki, T.; Huang, K.C.; et al. Atezolizumab in combination with Carboplatin and Nab-Paclitaxel in advanced squamous NSCLC (IMpower131): Results from a randomized phase III trial. J. Thorac. Oncol. 2020, 15, 1351–1360. [Google Scholar] [CrossRef]
- Govindan, R.; Szczesna, A.; Ahn, M.J.; Schneider, C.P.; Gonzalez, M.P.F.; Barlesi, F.; Han, B.; Ganea, D.E.; von Pawel, J.; Vladimirov, V.; et al. Phase III trial of Ipilimumab combined with Paclitaxel and Carboplatin in advanced squamous non-small-cell lung cancer. J. Clin. Oncol. 2017, 35, 3449–3457. [Google Scholar] [CrossRef]
- Paz-Ares, L.; Luft, A.; Vicente, D.; Tafreshi, A.; Gümüş, M.; Mazières, J.; Hermes, B.; Çay-Şenler, F.; Csőszi, T.; Fülöp, A.; et al. Pembrolizumab plus chemothe-rapy for squamous non-small-cell lung cancer. N. Engl. J. Med. 2018, 379, 2040–2051. [Google Scholar] [CrossRef]
- Wang, J.; Lu, S.; Yu, X.; Hu, Y.; Sun, Y.; Wang, Z.; Zhao, J.; Yu, Y.; Hu, C.; Yang, K.; et al. Tislelizumab plus chemotherapy vs chemotherapy alone as first-line treatment for advanced squamous non-small-cell lung cancer: A phase 3 randomized clinical trial. JAMA Oncol. 2021, 7, 709–717. [Google Scholar] [CrossRef]
- Ramalingam, S.S.; Novello, S.; Guclu, S.Z.; Bentsion, D.; Zvirbule, Z.; Szilasi, M.; Bernabe, R.; Syrigos, K.; Byers, L.A.; Clingan, P.; et al. Veliparib in combination with platinum-based chemotherapy for first-line treatment of advanced squamous cell lung cancer: A randomized, multicenter phase III study. J. Clin Oncol. 2021, 39, 3633–3644. [Google Scholar] [CrossRef]
- Spigel, D.R.; Townley, P.M.; Waterhouse, D.M.; Fang, L.; Adiguzel, I.; Huang, J.E.; Karlin, D.A.; Faoro, L.; Scappaticci, F.A.; Socinski, M.A. Randomized phase II study of Bevacizumab in combination with chemotherapy in previously untreated extensive-stage small-cell lung cancer: Results from the SALUTE trial. J. Clin. Oncol. 2011, 29, 2215–2222. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.V.; Reck, M.; Mansfield, A.S.; Mok, T.; Scherpereel, A.; Reinmuth, N.; Garassino, M.C.; De Castro, C.J.; Califano, R.; Nishio, M.; et al. Updated overall survival and PD-L1 subgroup analysis of patients with extensive-stage small-cell lung cancer treated with Atezolizumab, Carboplatin, and Etoposide (IMpower133). J. Clin. Oncol. 2021, 39, 619–630. [Google Scholar] [CrossRef] [PubMed]
- Reck, M.; Bondarenko, I.; Luft, A.; Serwatowski, P.; Barlesi, F.; Chacko, R.; Sebastian, M.; Lu, H.; Cuillerot, J.M.; Lynch, T.J. Ipilimumab in combination with paclitaxel and Carboplatin as first-line therapy in extensive-disease-small-cell lung cancer: Results from a randomized, double-blind, multicenter phase 2 trial. Ann. Oncol. 2013, 24, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Arnold, M.; Ferlay, J.; van Berge-Henegouwen, M.I.; Soerjomataram, I. Global burden of oesophageal and gastric cancer by histology and subsite in 2018. Gut 2020, 69, 1564–1571. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.M.; Shen, L.; Shah, M.A.; Enzinger, P.; Adenis, A.; Doi, T.; Kojima, T.; Metges, J.P.; Li, Z.; Kim, S.B.; et al. Pembrolizumab plus chemotherapy versus chemotherapy alone for first-line treatment of advanced oesophageal cancer (KEYNOTE-590): A randomised, placebo-controlled, phase 3 study. Lancet 2021, 398, 759–771. [Google Scholar] [CrossRef]
- Rao, S.; Starling, N.; Cunningham, D.; Sumpter, K.; Gilligan, D.; Ruhstaller, T.; Valladares-Ayerbes, M.; Wilke, H.; Archer, C.; Kurek, R.; et al. Matuzumab plus Epirubicin, Cisplatin and Capecitabine (ECX) compared with Epirubicin, Cisplatin and Capecitabine alone as first-line treatment in patients with advanced oesophago-gastric cancer: A randomised, multicentre open-label phase II study. Ann. Oncol. 2010, 21, 2213–2219. [Google Scholar] [CrossRef] [PubMed]
- Bang, Y.J.; VanCustem, E.; Fevereislova, A.; Chung, H.C.; Shen, L.; Sawaki, A.; Lordick, F.; Ohtsu, A.; Omuro, Y.; Satoh, T.; et al. Trastuzumabincombinationwithchemotherapyversuschemotherapyaloneforthetreatment of HER2 positive advanced gastric or gastro-oesophageal junction cancer (TOGA): A phase 3, open label, randomised, controlled clinical trial. Lancet 2010, 376, 687–697. [Google Scholar] [CrossRef]
- Yun, J.; Lee, J.; Park, S.H.; Park, J.O.; Park, Y.S.; Lim, H.Y.; Kang, W.K. A randomised phase II study of combination chemotherapy with epirubicin, cisplatin and capecitabine (ECX) or cisplatin and capecitabine (CX) in advanced gastric cancer. Eur. J. Cancer 2010, 46, 885–891. [Google Scholar] [CrossRef]
- Ahn, M.J.; Oh, H.S.; Choi, J.H.; Lee, Y.Y.; Kim, I.S.; Choi, I.Y.; Lee, O.Y.; Choi, H.S.; Kwon, S.J. Combination chemotherapy of Heptaplatin, Paclitaxel and 5-Fluorouracil in patients with advanced gastric cancer: A pilot study. Cancer Res. Treat. 2004, 36, 182. [Google Scholar] [CrossRef] [Green Version]
- Saito, S.; Yamaguchi, H.; Ohzawa, H.; Miyato, H.; Kanamaru, R.; Kurashina, K.; Hosoya, Y.; Lefor, A.K.; Sata, N.; Kitayama, J. Intraperitoneal administration of Paclitaxel combined with S-1 plus Oxaliplatin as induction therapy for patients with advanced gastric cancer with peritoneal metastases. Ann. Surg. Oncol. 2020, 28, 3863–3870. [Google Scholar] [CrossRef]
- Shi, M.; Yang, Z.; Lu, S.; Liu, W.; Ni, Z.; Yao, X.; Hua, Z.; Feng, R.; Zheng, Y.; Wang, Z.; et al. Oxaliplatin plus S-1 with intraperitoneal Paclitaxel for the treatment of Chinese advanced gastric cancer with peritoneal metastases. BMC Cancer 2021, 21, 1344. [Google Scholar] [CrossRef] [PubMed]
- Grothey, A.; Sobrero, A.F.; Shields, A.F.; Yoshino, T.; Paul, J.; Taieb, J.; Souglakos, J.; Shi, Q.; Kerr, R.; Labianca, R.; et al. Duration of adjuvant chemotherapy for stage III colon cancer. N. Engl. J. Med. 2018, 378, 1177–1188. [Google Scholar] [CrossRef] [PubMed]
- Sawicki, T.; Ruszkowska, M.; Danielewicz, A.; Niedźwiedzka, E.; Arłukowicz, T.; Katarzyna, E.; Przybyłowicz, A. Review of colorectal cancer in terms of epidemiology, risk factors, development, symptoms and diagnosis. Cancers 2021, 13, 2025. [Google Scholar] [CrossRef] [PubMed]
- Blick, S.K.A.; Scott, L.J. Cetuximab: A review of it’s use in squamous cell carcinoma of the head and neck and metastatic colorectal cancer. Drugs 2007, 67, 2585–2607. [Google Scholar] [CrossRef]
- Baba, H.; Yamada, Y.; Takahari, D.; Matsumoto, H.; Yoshida, K.; Nakamura, M.; Yoshida, M.; Iwamoto, S.; Shimada, K.; Komatsu, Y.; et al. S-1 and Oxaliplatin (SOX) plus Bevacizumab versus mFOLFOX6 plus Bevacizumab as first-line treatment for patients with metastatic colorectal cancer: Updated overall survival analyses of the open-label, non-inferiority, randomised phase III: SOFT study. ESMO Open 2017, 2, e000135. [Google Scholar] [CrossRef] [Green Version]
- Aranda, E.; Viéitez, J.M.; Gómez-España, A.; Gil, C.S.; Salud-Salvia, A.; Graña, B.; Garcia-Alfonso, P.; Rivera, F.; Quintero-Aldana, G.A.; Reina-Zoilo, J.J.; et al. FOLFOXIRI plus Bevacizumab versus FOLFOX plus Bevacizumab for patients with metastatic colorectal cancer and ≥3 circulating tumour cells: The randomised phase III VISNÚ-1 trial. ESMO Open 2020, 5, e000944. [Google Scholar] [CrossRef]
- van Hazel, G.A.; Heinemann, V.; Sharma, N.K.; Findlay, M.P.N.; Ricke, J.; Peeters, M.; Perez, D.; Robinson, B.A.; Strickland, A.H.; Ferguson, T.; et al. SIRFLOX: Randomized phase III trial comparing first-line mFOLFOX6 (plus or minus Bevacizumab) versus mFOLFOX6 (plus or minus Bevacizumab) plus selective internal radiation therapy in patients with metastatic colorectal cancer. J. Clin. Oncol. 2016, 34, 1723–1731. [Google Scholar] [CrossRef]
- Klein, A.P. Pancreatic cancer epidemiology: Understanding the role of lifestyle and inherited risk factors. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 493–502. [Google Scholar] [CrossRef]
- Isacoff, W.H.; Reber, H.A.; Bedford, R.; Hoos, W.; Rahib, L.; Upfill-Brown, A.; Donahue, T.; Hines, O.J. Low-dose continuous 5-Fluorouracil combined with Leucovorin, Nab-Paclitaxel, Oxaliplatin, and Bevacizumab for patients with advanced pancreatic cancer: A retrospective analysis. Target Oncol. 2018, 13, 461–468. [Google Scholar] [CrossRef] [Green Version]
- Pillay, L.; Wadee, R. A retrospective study of the epidemiology and histological subtypes of ovarian epithelial neoplasms at Charlotte Maxeke Johannesburg Academic Hospital. S. Afr. J. Gynaecol. Oncol. 2021, 13, 26–35. [Google Scholar] [CrossRef]
- Anderson, H.; Wagstaff, J.; Crowther, D.; Swindell, R.; Lind, M.J.; Mc Gregor, J.; Timms, M.S.; Brown, D.; Palmer, P. Comparative toxicity of Cisplatin, Carboplatin (CBDCA) and Iproplatin (CHIP) in combination with Cyclophosphamide in patients with advanced epithelial ovarian cancer. Eur. J. Cancer Clin. Oncol. 1988, 24, 1471–1479. [Google Scholar] [CrossRef]
- Brown, J.; Jhingran, A.; Deavers, M. Stromal tumors of the ovary. In Textbook of Uncommon Cancer, 4th ed.; Raghavan, D., Blanke, C.D., Johnson, D., Moots, P.L., Reaman, G.H., Rose, P.G., Sekeres, M.E., Eds.; Wiley Blackwell: Hoboken, NJ, USA, 2012; pp. 508–518. [Google Scholar] [CrossRef]
- Matei, D.E.; Schilder, J.M.; Michael, H. Germ cell tumors of the ovary. In Textbook of Uncommon Cancer, 4th ed.; Raghavan, D., Blanke, C.D., Johnson, D., Moots, P.L., Reaman, G.H., Rose, P.G., Sekeres, M.E., Eds.; Wiley Blackwell: Hoboken, NJ, USA, 2012; pp. 519–530. [Google Scholar] [CrossRef]
- Monk, B.J.; Colombo, N.; Oza, A.M.; Fujiwara, K.; Birrer, M.J.; Randall, L.; Poddubskaya, E.V.; Scambia, G.; Shparyk, Y.V.; Lim, M.C.; et al. Chemotherapy with or without Avelumab followed by Avelumab maintenance versus chemotherapy alone in patients with previously untreated epithelial ovariancancer (JAVELIN Ovarian 100): An open-label, randomised, phase 3 trial. Lancet Oncol. 2021, 22, 1275–1289. [Google Scholar] [CrossRef]
- Ray-Coquard, I.; Cibula, D.; Mirza, M.R.; Reuss, A.; Ricci, C.; Colombo, N.; Koch, H.; Goffin, F.; González-Martin, A.; Ottevanger, P.B.; et al. Final results from GCIG/ENGOT/AGO-OVAR 12, a randomised placebo-controlled phase III trial of Nintedanib combined with chemotherapy for newly diagnosed advanced ovarian cancer. Int. J. Cancer 2020, 146, 439–448. [Google Scholar] [CrossRef] [PubMed]
- Vergote, I.; Scambia, G.; O’Malley, D.M.; vanCalster, B.; Park, S.Y.; DelCampo, J.M.; Meier, W.; Bamias, A.; Colombo, N.; Wenham, R.M.; et al. Trebananib or placebo plus Carboplatin and Paclitaxel as first-line treatment for advanced ovarian cancer (TRINOVA-3/ENGOT-ov2/GOG-3001): A randomised, double-blind, phase 3 trial. Lancet Oncol. 2019, 20, 862–876. [Google Scholar] [CrossRef]
- Spirtos, N.M.; Enserro, D.; Homesley, H.D.; Gibbons, S.K.; Cella, D.; Morris, R.T.; DeGeest, K.; Lee, R.B.; Miller, D.S. The addition of Paclitaxel to Doxorubicin and Cisplatin and volume-directed radiation does not improve overall survival (OS) or long-term recurrence-free survival (RFS) in advanced endometrial cancer (EC): A randomized phase III NRG/Gynecologic Oncology Group (GOG) study. Gynecol. Oncol. 2019, 154, 13–21. [Google Scholar] [CrossRef] [PubMed]
- Sikov, W.M.; Berry, D.A.; Perou, C.M.; Singh, B.; Cirrincione, C.T.; Tolaney, S.M.; Kuzma, C.S.; Pluard, T.J.; Somlo, G.; Port, E.R.; et al. Impact of the addition of Carboplatin and/or Bevacizumab to neoadjuvant once-per-week paclitaxel followed by dose-dense Doxorubicin and Cyclophosphamide on pathologic complete response rates in stage II to III triple-negative breast cancer: CALGB 40603 (Alliance). J. Clin. Oncol. 2015, 33, 13–21. [Google Scholar] [CrossRef] [Green Version]
- Colombo, N.; Dubot, C.; Lorusso, D.; Caceres, M.V.; Hasegawa, K.; Shapira-Frommer, R.; Tewari, K.S.; Salman, P.; Hoyos, U.E.; Yañez, E.; et al. Pembrolizumab for persistent, recurrent, or metastatic cervical cancer. N. Engl. J. Med. 2021, 385, 1856–1867. [Google Scholar] [CrossRef]
- Schmid, P.; Cortes, J.; Pusztai, L.; Mc Arthur, H.; Kümmel, S.; Bergh, J.; Denkert, C.; Park, Y.H.; Hui, R.; Harbeck, N.; et al. Pembrolizumab for early triple-negative breast cancer. N. Engl. J. Med. 2020, 382, 810–821. [Google Scholar] [CrossRef]
- Ryan, P.D.; Tung, N.M.; Isakoff, S.J.; Golshan, M.; Richardson, A.; Corben, A.D.; Smith, B.L.; Gelman, R.; Winer, E.P.; Garber, J.E. Neoadjuvant Cisplatin and Bevacizumab in triple negative breast cancer (TNBC): Safety and efficacy. J. Clin. Oncol. 2009, 27 (Suppl. S15), 551. [Google Scholar] [CrossRef]
- Loibl, S.; O’Shaughnessy, J.; Untch, M.; Sikov, W.M.; Rugo, H.S.; Mc Kee, M.D.; Huober, J.; Golshan, M.; von Minckwitz, G.; Maag, D.; et al. Addition of the PARP inhibitor Veliparib plus Carboplatin or Carboplatin alone to standard neoadjuvant chemotherapy in triple-negative breast cancer (BrighTNess): A randomised, phase 3 trial. Lancet Oncol. 2018, 19, 497–509. [Google Scholar] [CrossRef]
- Buonerba, C.; Federico, P.; D’Aniello, C.; Rescigno, P.; Cavaliere, C.; Puglia, L.; Ferro, M.; Altieri, V.; Perdonà, S.; De Placido, S.; et al. Phase II trial of Cisplatin plus Prednisone in Docetaxel-refractory castration-resistant prostate cancer patients. Cancer Chemother. Pharmacol. 2011, 67, 1455–1461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fizazi, K.; Gravis, G.; Flechon, A.; Geoffrois, L.; Chevreau, C.; Laguerre, B.; Delva, R.; Eymard, J.C.; Rolland, F.; Houede, N.; et al. Combining Gemcitabine, Cisplatin, and Ifosfamide (GIP) is active in patients with relapsed metastatic germ-cell tumors (GCT): A prospective multicenter GETUG phase II trial. Ann. Oncol. 2014, 25, 987–991. [Google Scholar] [CrossRef] [PubMed]
- Feldman, D.R.; Hu, J.; Dorff, T.B.; Lim, K.; Patil, S.; Carousso, K.M.W.M.; Hughes, A.; Sheinfeld, J.; Bains, M.; Daneshmand, S.; et al. Paclitaxel, Ifosfamide, and Cisplatin efficacy for first-line treatment of patients with intermediate- or poor-risk germ cell tumors. J. Clin. Oncol. 2016, 34, 2478–2483. [Google Scholar] [CrossRef] [PubMed]
- Pectasides, D.; Pectasides, E.; Papaxoinis, G.; Xiros, N.; Kamposioras, K.; Tountas, N.; Economopoulos, T. Methotrexate, Paclitaxel, Ifosfamide, and Cisplatin in poor-risk nonseminomatous germ cell tumors. Urol. Oncol. 2010, 28, 617–623. [Google Scholar] [CrossRef]
- Huddart, R.A.; Gabe, R.; Cafferty, F.H.; Pollock, P.; White, J.D.; Shamash, J.; Cullen, M.H.; Stenning, S.P.; TE23 Trial Management Group and Collaborators; National Cancer Research Institute Testis Cancer Clinical Studies Group. A randomised phase 2 trial of intensive induction chemotherapy (CBOP/BEP) and standard BEP in poor-prognosis germ cell tumours (MRC TE23, CRUK 05/014, ISRCTN 53643604). Eur Urol. 2015, 67, 534–543. [Google Scholar] [CrossRef] [Green Version]
- Culine, S.; Kramar, A.; Theodore, C.; Geoffrois, L.; Chevreau, C.; Biron, P.; Nguyen, B.B.; Héron, J.F.; Kerbrat, P.; Caty, A.; et al. Randomized trial comparing Bleomycin/Etoposide/Cisplatin with alternating Cisplatin/Cyclophosphamide/Doxorubicin and Vinblastine/ Bleomycin regimens of chemotherapy for patients with intermediate- and poor-risk metastatic nonseminomatous germ cell tumors: Genito-Urinary Group of the French Federation of Cancer Centers Trial T93MP. J. Clin. Oncol. 2008, 26, 421–427. [Google Scholar] [CrossRef]
- Hiester, A.; Fingerhut, A.; Niegisch, G.; Siener, R.; Krege, S.; Schmelz, H.U.; Dieckmann, K.P.; Heidenreich, A.; Kwasny, P.; Pechoel, M.; et al. Late toxicities and recurrences in patients with clinical stage I non-seminomatous germ cell tumours after 1 cycle of adjuvant Bleomycin, Etoposide and Cisplatin versus primary retroperitoneal lymph node dissection-A 13-year follow-up analysis of a phase III trial cohort. Eur. J. Cancer 2021, 155, 64–72. [Google Scholar] [CrossRef]
- de Wit, R.; Skoneczna, I.; Daugaard, G.; De Santis, M.; Garin, A.; Aass, N.; Witjes, A.J.; Albers, P.; White, J.D.; Germa-Lluch, J.R.; et al. Randomized phase III study comparing Paclitaxel-Bleomycin, Etoposide, and Cisplatin (BEP) to standard BEP in intermediate-prognosis germ-cell cancer: Intergroup study EORTC 30983. J. Clin. Oncol. 2012, 30, 792. [Google Scholar] [CrossRef] [Green Version]
- Mego, M.; Svetlovska, D.; Reckova, M.; Angelis, D.; Kalavska, K.; Obertova, J.; Palacka, P.; Rejlekova, K.; Sycova-Mila, Z.; Chovanec, M.; et al. Gemcitabine, Carboplatin and Veliparib in multiple relapsed/refractory germ cell tumours: The GCT-SK-004 phase II trial. Investig. New Drugs 2021, 39, 1664–1670. [Google Scholar] [CrossRef]
- Bokemeyer, C.; Oechsle, K.; Honecker, F.; Mayer, F.; Hartmann, J.T.; Waller, C.F.; Böhlke, I.; Kollmannsberger, C.; German Testicular Cancer Study Group. Combination chemotherapy with Gemcitabine, Oxaliplatin, and Paclitaxel in patients with Cisplatin-refractory or multiply relapsed germ-cell tumors: A study of the German Testicular Cancer Study Group. Ann. Oncol. 2008, 19, 448–453. [Google Scholar] [CrossRef]
- Jain, A.; Brames, M.J.; Vaughn, D.J.; Einhorn, L.H. Phase II clinical trial of Oxaliplatin and Bevacizumab in refractory germ cell tumors. Am. J. Clin. Oncol. 2014, 37, 450–453. [Google Scholar] [CrossRef] [PubMed]
- Rose, T.L.; Harrison, M.R.; Deal, A.M.; Ramalingam, S.; Whang, Y.E.; Brower, B.; Dunn, M.; Osterman, C.K.; Heiling, H.M.; Bjurlin, M.A.; et al. Phase II study of Gemcitabine and split-dose Cisplatin plus Pembrolizumab as neoadjuvant therapy before radical cystectomy in patients with muscle-invasive bladder cancer. J. Clin. Oncol. 2021, 39, 3140–3148. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.; Wang, X.; Chen, F.; Ding, M.; Dong, M.; Yang, W.; Yin, M.; Wu, J.; Zhang, L.; Fu, X.; et al. Combination of Decitabine and a modified regimen of Cisplatin, Cytarabine and Dexamethasone: A potential salvage regimen for relapsed or refractory diffuse large B-cell lymphoma after second-line treatment gailure. Front. Oncol. 2021, 11, 687374. [Google Scholar] [CrossRef] [PubMed]
- Wiernik, P.H.; Balzarotti, M.; Santoro, A. Diagnosis and treatment of Hodgkin’s lymphoma. In Neoplastic Diseases of the Blood, 5th ed.; Wiernik, P.H., Goldman, J.M., Dutcher, J.P., Kyle, R.A., Eds.; Springer: Berlin/Heidelberg, Germany, 2013; Volume 45, pp. 985–1013. [Google Scholar]
- Mey, U.J.M.; Orlopp, K.S.; Flieger, D.; Strehl, J.W.; Ho, A.D.; Hensel, M.; Bopp, C.; Gorschlüter, M.; Wilhelm, M.; Birkmann, J.; et al. Dexamethasone, high-dose Cytarabine, and Cisplatin in combination with Rituximab as salvage treatment for patients with relapsed or refractory aggressive non-Hodgkin’s lymphoma. Cancer Investig. 2006, 24, 593–600. [Google Scholar] [CrossRef] [PubMed]
- Moskowitz, C.H.; Bertino, J.R.; Glassman, J.R.; Hedrick, E.E.; Hunte, S.; Coady-Lyons, N.; Agus, D.B.; Goy, A.; Jurcic, J.; Noy, A.; et al. Ifosfamide, Carboplatin, and Etoposide: A highly effective cytoreduction and peripheral-blood progenitor-cell mobilization regimen for transplant-eligible patients with non-Hodgkin’s lymphoma. J. Clin. Oncol. 1999, 17, 3776–3785. [Google Scholar] [CrossRef]
- Seymour, J.F.; Grigg, A.P.; Szer, J.; Fox, R.M. Cisplatin, Fludarabine, and Cytarabine: A novel, pharmacologically designed salvage therapy for patients with refractory, histologically aggressive or mantle cell non-Hodgkin’s lymphoma. Cancer 2002, 94, 585–593. [Google Scholar] [CrossRef]
- Heidegger, S.; Beer, A.; Geissinger, E.; Rosenwald, A.; Peschel, C.; Ringshausen, I.; Keller, U. Combination therapy with Brentuximab vedotin and Cisplatin/Cytarabine in a patient with primarily refractory anaplastic lymphoma kinase positive anaplastic large cell lymphoma. OncoTargets Ther. 2014, 7, 1123–1127. [Google Scholar] [CrossRef] [Green Version]
- Corrie, P.G.; Pippa, G. Cytotoxic chemotherapy: Clinical aspects. Medicine 2008, 36, 24–28. [Google Scholar] [CrossRef]
- Crump, M.; Kuruvilla, J.; Couban, S.; Mac Donald, D.A.; Kukreti, V.; Kouroukis, C.T.; Rubinger, M.; Buckstein, R.; Imrie, K.R.; Federico, M.; et al. Randomized comparison of Gemcitabine, Dexamethasone, and Cisplatin versus Dexamethasone, Cytarabine, and Cisplatin chemotherapy before autologous stem-cell transplantation for relapsed and refractory aggressive lymphomas: NCIC-CTG LY.12. J. Clin. Oncol. 2014, 32, 3490–3496. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; Cui, Y.; Sun, Z.; Zhang, L.; Li, L.; Wang, X.; Wu, J.; Fu, X.; Ma, W.; Zhang, X.; et al. DDGP versus SMILE in newly diagnosed advanced natural killer/T-cell lymphoma: A randomized controlled, multicenter, open-label study in China. Clin. Cancer Res. 2016, 22, 5223–5228. [Google Scholar] [CrossRef] [Green Version]
- Lorch, J.H.; Goloubeva, O.; Haddad, R.I.; Cullen, K.; Sarlis, N.; Tishler, R.; Tan, M.; Fasciano, J.; Sammartino, D.E.; Posner, M.R.; et al. Induction chemotherapy with Cisplatin and Fluorouracil alone or in combination with Docetaxel in locally advanced squamous-cell cancer of the head and neck: Long-term results of the TAX 324 randomised phase 3 trial. Lancet Oncol. 2011, 12, 153–159. [Google Scholar] [CrossRef] [Green Version]
- Lemma, G.L.; Lee, J.W.; Aisner, S.C.; Langer, C.J.; Tester, W.J.; Johnson, D.H.; Loehrer, P.J. Phase II study of Carboplatin and Paclitaxel in advanced thymoma and thymic carcinoma. J. Clin. Oncol. 2011, 29, 2060–2065. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.S.; Putnam, J.B.; Komaki, R.; Walsh, G.L.; Ro, J.Y.; Shin, H.J.; Truong, M.; Moon, H.; Swisher, S.G.; Fossella, F.V.; et al. Phase II study of a multidisciplinary approach with induction chemotherapy, followed by surgical resection, radiation therapy, and consolidation chemotherapy for unresectable malignant thymomas: Final report. Lung Cancer 2004, 44, 369–379. [Google Scholar] [CrossRef] [PubMed]
- Yoh, K.; Goto, K.; Ishii, G.I.; Niho, S.; Ohmatsu, H.; Kubota, K.; Kakinuma, R.; Nagai, K.; Suga, M.; Nishiwaki, Y. Weekly chemotherapy with Cisplatin, Vincristine, Doxorubicin, and Etoposide is an effective treatment for advanced thymic carcinoma. Cancer 2003, 98, 926–931. [Google Scholar] [CrossRef] [PubMed]
- Sakai, D.; Kanai, M.; Kobayashi, S.; Eguchi, H.; Baba, H.; Seo, S.; Taketomi, A.; Takayama, T.; Yamaue, H.; Ishioka, C.; et al. Randomized phase III study of Gemcitabine, Cisplatin plus S-1 (GCS) versus Gemcitabine, Cisplatin (GC) for advanced biliary tract cancer (KHBO1401-MITSUBA). Ann. Oncol. 2018, 29 (Suppl. S8), 205–270. [Google Scholar] [CrossRef]
- Shroff, R.T.; Javle, M.M.; Xiao, L.; Kaseb, A.O.; Varadhachary, G.R.; Wolff, R.A.; Raghav, K.P.S.; Iwasaki, M.; Masci, P.; Ramanathan, R.K.; et al. Gemcitabine, Cisplatin, andNab-Paclitaxelforthetreatmentofadvancedbiliarytractcancers: Aphase 2 clinicaltrial. JAMA Oncol. 2019, 5, 824–830. [Google Scholar] [CrossRef]
- Rao, S.; Cunningham, D.; Hawkins, R.E.; Hill, M.E.; Smith, D.; Daniel, F.; Ross, P.J.; Oates, J.; Norman, A.R. PhaseIIIstudyof 5FU, EtoposideandLeucovorin (FELV) comparedtoEpirubicin, Cisplatinand 5FU (ECF) inpreviouslyuntreatedpatientswithadvancedbiliarycancer. Br. J. Cancer 2005, 92, 1650–1654. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.T.; Kang, J.H.; Lee, J.; Lee, H.W.; Oh, S.Y.; Jang, J.S.; Lee, M.A.; Sohn, B.S.; Yoon, S.Y.; Choi, H.J.; et al. CapecitabineplusOxaliplatinversusGemcitabineplusOxaliplatinasfirst-linetherapyforadvancedbiliarytractcancers: A multicenter, open-label, randomized, phaseIII, noninferioritytrial. Ann. Oncol. 2019, 30, 788–795. [Google Scholar] [CrossRef]
- Edeline, J.; Benabdelghani, M.; Bertaut, A.; Watelet, J.; Hammel, P.; Joly, J.P.; Boudjema, K.; Fartoux, L.; Bouhier-Leporrier, K.; Jouve, J.L.; et al. Gemcitabine and Oxaliplatin chemotherapy or surveillance in resected biliary tract cancer (PRODIGE 12-ACCORD 18-UNICANCERGI): A randomizedphaseIIIstudy. J. Clin. Oncol. 2019, 37, 658–667. [Google Scholar] [CrossRef]
- Lee, J.; Park, S.H.; Chang, H.M.; Kim, J.S.; Choi, H.J.; Lee, M.A.; Jang, J.S.; Jeung, H.C.; Kang, J.H.; Lee, H.W.; et al. Gemcitabine and Oxaliplatin with or without Erlotinibin advanced biliary-tract cancer: A multicentre, open-label, randomised, phase 3 study. Lancet Oncol. 2012, 13, 181–188. [Google Scholar] [CrossRef]
- Zhu, A.X.; Meyerhardt, J.A.; Blaszkowsky, L.S.; Kambadakone, A.R.; Muzikansky, A.; Zheng, H.; Clark, J.W.; Abrams, T.; Chan, J.A.; Enzinger, P.C.; et al. Efficacy and safety of Gemcitabine, Oxaliplatin, and Bevacizumab in advanced biliary-tract cancers and correlation of changes in 18-fluorodeoxyglucose PET with clinical outcome: A phase 2 study. Lancet Oncol. 2010, 11, 48–54. [Google Scholar] [CrossRef]
- Lamarca, A.; Palmer, D.H.; Wasan, H.S.; Ross, P.J.; Ma, Y.T.; Arora, A.; Falk, S.; Gillmore, R.; Wadsley, J.; Patel, K.; et al. Second-line FOLFOX chemotherapy versus active symptom control for advanced biliary tract cancer (ABC-06): A phase 3, open-label, randomised, controlled trial. Lancet Oncol. 2021, 22, 690–701. [Google Scholar] [CrossRef]
- Sun, W.; Sohal, D.; Haller, D.G.; Mykulowycz, K.; Rosen, M.; Soulen, M.C.; Caparro, M.; Teitelbaum, U.R.; Giantonio, B.; O’Dwyer, P.J.; et al. Phase 2 trial of Bevacizumab, Capecitabine, and Oxaliplatin in treatment of advanced hepatocellular carcinoma. Cancer 2011, 117, 3187–3192. [Google Scholar] [CrossRef] [PubMed]
- Qin, S.; Bai, Y.; Lim, H.Y.; Thongprasert, S.; Chao, Y.; Fan, J.; Yang, T.S.; Bhudhisawasdi, V.; Kang, W.K.; Zhou, Y.; et al. Randomized, multicenter, open-label study of Oxaliplatin plus Fluorouracil/Leucovorin versus Doxorubicin as palliative chemotherapy in patients with advanced hepatocellular carcinoma from Asia. J. Clin. Oncol. 2013, 31, 3501–3508. [Google Scholar] [CrossRef] [PubMed]
- Goyal, L.; Zheng, H.; Abrams, T.A.; Miksad, R.; Bullock, A.J.; Allen, J.N.; Yurgelun, M.B.; Clark, J.W.; Kambadakone, A.; Muzikansky, A.; et al. A phase II and biomarker study of Sorafenib combined with modified FOLFOX in patients with advanced hepatocellular carcinoma. Clin. Cancer Res. 2019, 25, 80–89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zaanan, A.; Williet, N.; Hebbar, M.; Dabakuyo, T.S.; Fartoux, L.; Mansourbakht, T.; Dubreuil, O.; Rosmorduc, O.; Cattan, S.; Bonnetain, F.; et al. Gemcitabine plus Oxaliplatin in advanced hepatocellular carcinoma: A large multicenter AGEO study. J. Hepatol. 2013, 58, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Assenat, E.; Pageaux, G.P.; Thézenas, S.; Peron, J.M.; Bécouarn, Y.; Seitz, J.F.; Merle, P.; Blanc, J.F.; Bouché, O.; Ramdani, M.; et al. Sorafenib alone vs Sorafenib plus GEMOX as 1st-line treatment for advanced HCC: The phase II randomised PRODIGE 10 trial. Br. J. Cancer 2019, 120, 896–902. [Google Scholar] [CrossRef]
- von der Maase, H.; Sengelov, L.; Roberts, J.T.; Ricci, S.; Dogliotti, L.; Oliver, T.; Moore, M.J.; Zimmermann, A.; Arning, M. Long-term survival results of a randomized trial comparing Gemcitabine plus Cisplatin, with Methotrexate, Vinblastine, Doxorubicin, plus Cisplatin in patients with bladder cancer. J. Clin. Oncol. 2015, 23, 4602–4608. [Google Scholar] [CrossRef]
- Pattarawat, P.; Hong, T.; Wallace, S.; Hu, Y.; Donnell, R.; Wang, T.H.; Tsai, C.L.; Wang, J.; Wang, H.C.R. CompensatorycombinationofRomidepsinwithGemcitabineandCisplatintoeffectivelyandsafelycontrolurothelialcarcinoma. Br. J. Cancer 2020, 123, 226–239. [Google Scholar] [CrossRef]
- Pizzocaro, G.; Nicolai, N.; Milani, A. Taxanes in combination with Cisplatin and Fluorouracil for advanced penile cancer: Preliminary results. Eur. Urol. 2009, 55, 546–551. [Google Scholar] [CrossRef]
- Jefford, M.; Kiffer, J.D.; Somers, G.; Daniel, F.J.; Davis, I.D. Metastatic basal cell carcinoma: Rapid symptomatic response to Cisplatin and Paclitaxel. ANZ J. Surg. 2004, 74, 704–705. [Google Scholar] [CrossRef] [PubMed]
- Whelan, J.S.; Davis, L.E. Osteosarcoma, chondrosarcoma, and chordoma. J. Clin. Oncol. 2018, 36, 188–193. [Google Scholar] [CrossRef] [PubMed]
- Yu, D.; Zhang, S.; Feng, A.; Xu, D.; Zhu, Q.; Mao, Y.; Zhao, Y.; Lv, Y.; Han, C.; Liu, R.; et al. Methotrexate, Doxorubicin, and Cisplatinum regimen is still the preferred option for osteosarcoma chemotherapy. A meta-analysis and clinical observation. Medicine 2019, 98, e15582. [Google Scholar] [CrossRef] [PubMed]
- Marina, N.M.; Smeland, S.; Bielack, S.S.; Bernstein, M.; Jovic, G.; Krailo, M.D.; Hook, J.M.; Arndt, C.; van den Berg, H.; Brennan, B.; et al. Comparison of MAPIE versus MAP in patients with a poor response to preoperative chemotherapy for newly diagnosed high-grade osteosarcoma (EURAMOS-1): An open-label, international, randomised controlled trial. Lancet Oncol. 2016, 17, 1396–1408. [Google Scholar] [CrossRef] [Green Version]
- Bacci, G.; Briccoli, A.; Rocca, M.; Ferrari, S.; Donati, D.; Longhi, A.; Bertoni, F.; Bacchini, P.; Giacomini, S.; Forni, C.; et al. Neoadjuvant chemotherapy for osteosarcoma of the extremities with metastases at presentation: Recent experience at the Rizzoli Institute in 57 patients treated with Cisplatin, Doxorubicin, and a high dose of Methotrexate and Ifosfamide. Ann. Oncol. 2003, 14, 1126–1134. [Google Scholar] [CrossRef]
- Basaran, M.; Bavbek, E.S.; Saglam, S.; Eralp, L.; Sakar, B.; Atalar, A.C.; Bilgic, B.; Ozger, H.; Onat, H. A phase II study of Cisplatin, Ifosfamide and Epirubicin combination chemotherapy in adults with non-metastatic and extremity osteosarcomas. Oncology 2007, 72, 255–260. [Google Scholar] [CrossRef]
- Katzenstein, H.M.; Malogolowkin, M.H.; Krailo, M.D.; Piao, J.; Towbin, A.J.; Mc Carville, M.B.; Tiao, G.M.; Dunn, S.P.; Langham, M.R.; Mc Gahren, E.D.; et al. Doxorubicin in combination with Cisplatin, 5-Flourouracil, and Vincristine is feasible and effective in unresectable hepatoblastoma: A children’s Oncology Group study. Cancer 2022, 128, 1057–1065. [Google Scholar] [CrossRef]
- van Meerbeeck, J.P.; Gaafar, R.; Manegold, C.; van Klaveren, R.J.; van Marck, E.A.; Vincent, M.; Legrand, C.; Bottomley, A.; Debruyne, C.; Giaccone, G.; et al. Randomized phase III study of Cisplatin with or without Raltitrexed in patients with malignant pleural mesothelioma: An intergroup study of the European Organisation for Research and Treatment of Cancer, Lung Cancer Group and the National Cancer Institute of Canada. J. Clin. Oncol. 2005, 23, 6881–6889. [Google Scholar] [CrossRef]
- Ceresoli, G.L.; Aerts, J.G.; Dziadziuszko, R.; Ramlau, R.; Cedres, S.; van Meerbeeck, J.P.; Mencoboni, M.; Planchard, D.; Chella, A.; Crinò, L.; et al. Tumour treating fields in combination with Pemetrexed and Cisplatin or Carboplatin as first-line treatment for unresectable malignant pleural mesothelioma (STELLAR): A multicentre, single-arm phase 2 trial. Lancet Oncol. 2019, 20, 1702–1709. [Google Scholar] [CrossRef]
- Zalcman, G.; Mazieres, J.; Margery, J.; Greillier, L.; Audigier-Valette, C.; Moro-Sibilot, D.; Molinier, O.; Corre, R.; Monnet, I.; Gounant, V.; et al. Bevacizumab for newly diagnosed pleural mesothelioma in the Mesothelioma Avastin Cisplatin Pemetrexed Study (MAPS): A randomised, controlled, open-label, phase 3 trial. Lancet 2016, 387, 1405–1414. [Google Scholar] [CrossRef]
- Scagliotti, G.V.; Gaafar, R.; Nowak, A.K.; Nakano, T.; van Meerbeeck, J.; Popat, S.; Vogelzang, N.J.; Grosso, F.; Aboelhassan, R.; Jakopovic, M.; et al. Nintedanib in combination with Pemetrexed and Cisplatin for chemotherapy-naive patients with advanced malignant pleural mesothelioma (LUME-Meso): A double-blind, randomised, placebo-controlled phase 3 trial. Lancet Respir. Med. 2019, 7, 569–580. [Google Scholar] [CrossRef]
- Ridolfi, R.; Chiarion-Sileni, V.; Guida, M.; Romanini, A.; Labianca, R.; Freschi, A.; Lo-Re, G.; Nortilli, R.; Brugnara, S.; Vitali, P.; et al. Cisplatin, Dacarbazine with or without subcutaneous Interleukin-2, and Interferon alpha-2b in advanced melanoma outpatients: Results from an Italian multicenter phase III randomized clinical trial. J. Clin. Oncol. 2002, 20, 1600–1607. [Google Scholar] [CrossRef] [PubMed]
- Papadopoulos, N.E.; Bedikian, A.; Ring, S.; Kim, K.B.; Hwu, W.J.; Gerber, D.L.; Homsi, J.; Hwu, P. Phase I/II study of a Cisplatin-taxol-Dacarbazine regimen in metastatic melanoma. Am. J. Clin. Oncol. 2009, 32, 509–514. [Google Scholar] [CrossRef] [PubMed]
- Jungnelius, U.; Ringborg, U.; Aamdal, S.; Mattsson, J.; Stierner, U.; Ingvar, C.; Malmström, P.; Andersson, R.; Karlsson, M.; Willman, K.; et al. Dacarbazine-Vindesine versus Dacarbazine-Vindesine-Cisplatin in disseminated malignant melanoma: A randomised phase III trial. Eur. J. Cancer 1998, 34, 1368–1374. [Google Scholar] [CrossRef]
- Lian, B.; Si, L.; Cui, C.; Chi, Z.; Sheng, X.; Mao, L.; Li, S.; Kong, Y.; Tang, B.; Guo, J. Phase II randomized trial comparing high-dose IFN-α2b with Temozolomide plus Cisplatin as systemic adjuvant therapy for resected mucosal melanoma. Clin. Cancer Res. 2013, 19, 4488–4498. [Google Scholar] [CrossRef] [Green Version]
- Flaherty, K.T.; Lee, S.J.; Zhao, F.; Schuchter, L.M.; Flaherty, L.; Kefford, R.; Atkins, M.B.; Leming, P.; Kirkwood, J.M. Phase III trial of Carboplatin and Paclitaxel with or without Sorafenib in metastatic melanoma. J. Clin. Oncol. 2013, 31, 373–379. [Google Scholar] [CrossRef] [Green Version]
- Yan, X.; Sheng, X.; Chi, Z.; Si, L.; Cui, C.; Kong, Y.; Tang, B.; Mao, L.; Wang, X.; Lian, B.; et al. Randomized phase II study of Bevacizumab in Combination with Carboplatin plus Paclitaxel in patients with previously untreated advanced mucosal melanoma. J. Clin. Oncol. 2021, 39, 881–889. [Google Scholar] [CrossRef]
- Kottschade, L.A.; Suman, V.J.; Perez, D.G.; Mc Williams, R.R.; Kaur, J.S.; Amatruda, T.T.; Geoffroy, F.J.; Gross, H.M.; Cohen, P.A.; Jaslowski, A.J.; et al. A randomized phase 2 study of Temozolomide and Bevacizumab or Nab-Paclitaxel, Carboplatin, and Bevacizumab in patients with unresectable stage IV melanoma: A North Central Cancer Treatment Group study, N0775. Cancer 2013, 119, 586–592. [Google Scholar] [CrossRef] [Green Version]
- Campagna, R.; Bacchetti, T.; Salvolini, E.; Pozzi, V.; Molinelli, E.; Brisigotti, V.; Sartini, D.; Campanati, A.; Ferretti, G.; Offidani, A.; et al. Paraoxonase-2 silencing enhances sensitivity of A375 melanoma cells to treatment with Cisplatin. Antioxidants 2020, 9, 1238. [Google Scholar] [CrossRef]
- Bacchetti, T.; Salvolini, E.; Pompei, V.; Campagna, R.; Molinelli, E.; Brisigotti, V.; Togni, L.; Lucarini, G.; Sartini, D.; Campanati, A.; et al. Paraoxonase-2: A potential biomarker for skin cancer aggressiveness. Eur. J. Clin. Investig. 2021, 51, e13452. [Google Scholar] [CrossRef]
- Fumarola, S.; Cecati, M.; Sartini, D.; Ferretti, G.; Milanese, G.; Galosi, A.B.; Pozzi, V.; Campagna, R.; Morresi, C.; Emanuelli, M.; et al. Bladder cancer chemosensitivity is affected by paraoxonase-2 expression. Antioxidants 2020, 9, 175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bryde, S.; de Kroon, M.A.I.P. Nanocapsules of platinum anticancer drugs: Development towards therapeutic use. Future Med. Chem. 2009, 1, 1467–1480. [Google Scholar] [CrossRef] [PubMed]
- Mylonakis, N.; Athanasiou, A.; Ziras, N.; Angel, J.; Rapti, A.; Lampaki, S.; Politis, N.; Karanikas, C.; Kosmas, C. Phase II study of liposomal Cisplatin (Lipoplatin) plus Gemcitabine versus Cisplatin plus Gemcitabine as first line treatment in Inoperable (stage IIIB/IV) non-small cell lung cancer. Lung Cancer 2010, 68, 240–247. [Google Scholar] [CrossRef]
- Stathopoulos, G.P.; Boulikas, T.; Kourvetaris, A.; Stathopoulos, I. Liposomal Oxaliplatin in the treatment of advanced cancer: A phase I study. Anticancer Res. 2006, 26, 1489–1494. [Google Scholar] [PubMed]
- Koukourakis, M.I.; Giatromanolaki, A.; Pitiakoudis, M.; Kouklakis, G.; Tsoutsou, P.; Abatzoglou, I.; Panteliadou, M.; Sismanidou, K.; Sivridis, E.; Boulikas, T. Concurrent liposomal Cisplatin (Lipoplatin), 5-Fluorouracil and radiotherapy for the treatment of locally advanced gastric cancer: A phase I/II study. Int. J. Radiat. Oncol. Biol. Phys. 2010, 78, 150–155. [Google Scholar] [CrossRef] [PubMed]
- White, S.C.; Lorigan, P.; Margison, G.P.; Margison, J.M.; Martin, F.; Thatcher, N.; Anderson, H.; Ranson, M. Phase II study of SPI-77 (sterically stabilised liposomal Cisplatin) in advanced non-small-cell lung cancer. Br. J. Cancer 2006, 95, 822–828. [Google Scholar] [CrossRef] [Green Version]
Figure 1.
Chemical structure of Cisplatin.

Figure 2.
Regulations for Cisplatin and its derivatives in countries or regions.

Figure 3.
Chemical structure of Carboplatin.

Figure 4.
Chemical structure of Oxaliplatin.

Figure 5.
Chemical structure of Nedaplatin.

Figure 6.
Chemical structure of Heptaplatin.

Figure 7.
Chemical structure of Lobaplatin.

Figure 8.
Chemical structure of Satraplatin.

Table 1.
Cisplatin synergistic combinations.
| Cisplatin Synergistic Combinations | Disease |
|---|---|
| (1) Cisplatin/Fluorouracil/Docetaxel/Cetuximab [21] | head and neck squamous cell carcinoma |
| (2) Cisplatin/Gemcitabine [22] (3) Cisplatin/Gemcitabine/Necitumumab [23] | squamous non-small-cell lung cancer |
| (4) Cisplatin/Vinorelbine [24] | non-squamous non-small-cell lung cancer |
| (5) Cisplatin/Etoposide/Irinotecan [25] (6) Cisplatin/Etoposide/Durvalumab [26] (7) Cisplatin/Vinorelbine [27] | small-cell lung cancer |
| (8) Cisplatin/Capecitabine [28] (9) Cisplatin/Cetuximab [29] | breast cancer |
| (10) Cisplatin/Docetaxel [30] (11) Cisplatin/Paclitaxel [31] (12) Cisplatin/Tegafur-Gimeracil-Oteracil potassium (S-1) [32] | esophageal squamous cell carcinoma |
| (13) Cisplatin/Capecitabine/Docetaxel [33] (14) Cisplatin/Capecitabine/Epirubicin [34] (15) Cisplatin/Capecitabine/Epirubicin/Rilotumumab [35] (16) Cisplatin/Fluorouracil/Epirubicin [34] | gastroesophageal adenocarcinoma |
| (17) Cisplatin/Capecitabine [36] (18) Cisplatin/Capecitabine/Paclitaxel [37] (19) Cisplatin/Tegafur-Gimeracil-Oteracil potassium (S-1) [36] (20) Cisplatin/Tegafur-Gimeracil-Oteracil potassium (S-1)/Trastuzumab [38] | gastric cancer |
| (21) Cisplatin/Capecitabine/Gemcitabine/Docetaxel [39] (22) Cisplatin/Capecitabine/Gemcitabine/Epirubicin [39] (23) Cisplatin/Capecitabine/Gemcitabine/Nab-Paclitaxel [39] | pancreatic adenocarcinoma |
| (24) Cisplatin/Capecitabine [40] (25) Cisplatin/Gemcitabine [40] | biliary cancer |
| (26) Cisplatin/Gemcitabine/Everolimus [41] | urothelial carcinoma |
| (27) Cisplatin/Capecitabine/radiation therapy [42] (28) Cisplatin/Fluorouracil/Docetaxel [43] (29) Cisplatin/Fluorouracil/Docetaxel/Atezolizumab [43] | anal squamous cell carcinoma |
| (30) Cisplatin/Cemiplimab [44] | metastatic penile cancer |
Table 2.
Carboplatin synergistic combinations.
| Carboplatin Synergistic Combinations | Disease |
|---|---|
| (1) Carboplatin/Gemcitabine [54] | salivary gland cancer |
| (2) Carboplatin/Fluorouracil [56] (3) Carboplatin/Paclitaxel/Cetuximab [21] | head and neck squamous cell carcinoma |
| (4) Carboplatin/Gemcitabine [57] (5) Carboplatin/Gemcitabine/Avelumab [58] (6) Carboplatin/Paclitaxel [59] (7) Carboplatin/Nab-Paclitaxel/Atezolizumab [60] (8) Carboplatin/Paclitaxel/Bevacizumab [61] (9) Carboplatin/Paclitaxel/Nivolumab [62] (10) Carboplatin/Pemetrexed [61] (11) Carboplatin/Pemetrexed/Avelumab [58] (12) Carboplatin/Tegafur-Gimeracil-Oteracil potassium (S-1) [63] (13) Carboplatin/Vinorelbine [64] | non-small-cell lung cancer |
| (14) Carboplatin/Amrubicin [65] (15) Carboplatin/Etoposide [66] (16) Carboplatin/Etoposide/Atezolizumab [26,67] (17) Carboplatin/Etoposide/Durvalumab [26,66] (18) Carboplatin/Etoposide/Durvalumab/Tremelimumab [66] (19) Carboplatin/Etoposide/Obatoclax mesylate [68] (20) Carboplatin/Irinotecan [65] | small-cell lung cancer |
| (21) Carboplatin/Gemcitabine [69] (22) Carboplatin/Gemcitabine/Iniparib [69] (23) Carboplatin/Gemcitabine/Pembrolizumab [70] (24) Carboplatin/Docetaxel/Trastuzumab [71] | breast cancer |
| (25) Carboplatin/Paclitaxel [72] | esophageal squamous cell carcinoma |
| (26) Carboplatin/Docetaxel/Capecitabine [73] | gastroesophageal adenocarcinoma |
| (27) Carboplatin/Paclitaxel [74] | gastric cancer |
| (28) Carboplatin/Bortezomib [75] | ovarian cancer |
| (29) Carboplatin/Paclitaxel [70] (30) Carboplatin/Paclitaxel/Trastuzumab [76] | urotelial carcinoma |
Table 3.
Oxaliplatin synergistic combinations.
| Oxaliplatin Synergistic Combinations | Disease |
|---|---|
| (1) Oxaliplatin/Cytarabine/Fludarabine [82] | leukemia |
| (2) Oxaliplatin/Cytarabin/Docetaxel [83] | non-small-cell lung cancer |
| (3) Oxaliplatin/Capecitabine [72] (4) Oxaliplatin/Fluorouracil/Leucovorin [84] | esophageal adenocarcinoma |
| (5) Oxaliplatin/Capecitabine/Epirubicin [73] (6) Oxaliplatin/Capecitabine/Sintilimab [85] (7) Oxaliplatin/Fluorouracil/Leucovorin [86] (8) Oxaliplatin/Fluorouracil/Leucovorin/Docetaxel [34] (9) Oxaliplatin/Fluorouracil/Leucovorin/Onartuzumab [86] (10) Oxaliplatin/Fluorouracil/Leucovorin/Panitumumab [87] (11) Oxaliplatin/Fluorouracil/Leucovorin/Rilotumumab [87] (12) Oxaliplatin/Tegafur-Gimeracil-Oteracil potassium (S-1)/Pembrolizumab [88] | gastroesophageal adenocarcinoma |
| (13) Oxaliplatin/Capecitabine [89] (14) Oxaliplatin/Capecitabine/Docetaxel [90,91] (15) Oxaliplatin/Capecitabine/Sintilimab [85] (16) Oxaliplatin/Capecitabine/Trastuzumab [92] (17) Oxaliplatin/Capecitabine/Tegafur-Gimeracil-Oteracil potassium (S-1)/Nivolumab [93] (18) Oxaliplatin/Fluorouracil/Epirubicin [91] (19) Oxaliplatin/Fluorouracil/Leucovorin [94] (20) Oxaliplatin/Fluorouracil/Leucovorin/Docetaxel [95] (21) Oxaliplatin/Fluorouracil/Avelumab [96] (22) Oxaliplatin/Tegafur-Gimeracil-Oteracil potassium (S-1) [97] (23) Oxaliplatin/Tegafur-Gimeracil-Oteracil potassium (S-1)/Pembrolizumab [88] | gastric cancer |
| (24) Oxaliplatin/Fluorouracil/Irinotecan/Leucovorin [98] (25) Oxaliplatin/Fluorouracil/Irinotecan/Bevacizumab [99] (26) Oxaliplatin/Fluorouracil/Leucovorin/Atezolizumab [99] (27) Oxaliplatin/Fluorouracil/Leucovorin/Bevacizumab [99] (28) Oxaliplatin/Fluorouracil/Leucovorin/Durvalumab [100] (29) Oxaliplatin/Fluorouracil/Leucovorin/Tremelimumab [100] (30) Oxaliplatin/Trifluridine/Tipiracil Limagne [101] | colorectal cancer |
| (31) Oxaliplatin/Tegafur-Gimeracil-Oteracil potassium (S-1) [102] | hepatocellular carcinoma |
| (32) Oxaliplatin/Bortezomib [75] | ovarian cancer |
Table 4.
Nedaplatin synergistic combinations.
| Nedaplatin Synergistic Combinations | Disease |
|---|---|
| (1) Nedaplatin/Tegafur-Gimeracil-Oteracil potassium (S-1) [108] | head and neck squamous cell carcinoma |
| (2) Nedaplatin/Docetaxel [109] (3) Nedaplatin/Docetaxel/Paclitaxel [83] (4) Nedaplatin/Gemcitabine [110] (5) Nedaplatin/Irinotecan [111] (6) Nedaplatin/Nab-Paclitaxel [112] (7) Nedaplatin/Paclitaxel/Sintilimab [113] | non-small-cell lung cancer |
| (8) Nedaplatin/Irinotecan [114] | neuroendocrine lung carcinoma |
| (9) Nedaplatin/Paclitaxel/Nivolumab [115] | lymphoepithelioma |
| (10) Nedaplatin/Docetaxel [116] (11) Nedaplatin/Docetaxel/Fluorouracil [117] (12) Nedaplatin/Docetaxel/Tegafur-Gimeracil-Oteracil potassium (S-1) [118] (13) Nedaplatin/Fluorouracil [119] (14) Nedaplatin/Paclitaxel [120] (15) Nedaplatin/Paclitaxel/Nimotuzumab [121] (16) Nedaplatin/Gemcitabine/Nimotuzumab [121] (17) Nedaplatin/Fluorouracil/Nimotuzumab [121] | esophageal squamous cell carcinoma |
| (18) Nedaplatin/Gemcitabine [122] (19) Nedaplatin/Fluorouracil [123] (20) Nedaplatin/Paclitaxel/Tegafur-Gimeracil-Oteracil potassium (S-1) [124] (21) Nedaplatin/radiotherapy [125] | nasopharyngeal carcinoma |
| (22) Nedaplatin/Docetaxel [126] (23) Nedaplatin/Gemcitabine [127] (24) Nedaplatin/Irinotecan [128] | squamous lung cell carcinoma |
| (25) Nedaplatin/Gemcitabine [129] (26) Nedaplatin/Paclitaxel/Ifosfamide [130] | urothelial cancer |
| (27) Nedaplatin/Paclitaxel [131] (28) Nedaplatin/Bevacizumab [132] | ovarian cancer |
| (29) Nedaplatin/Irinotecan [133] | endometrial carcinoma |
| (30) Nedaplatin/Paclitaxel [134,135] | cervical cancer |
Table 5.
Lobaplatin synergistic combinations.
| Lobaplatin Synergistic Combinations | Disease |
|---|---|
| (1) Lobaplatin/Fluorouracil [156,157] | nasopharyngeal carcinoma |
| (2) Lobaplatin/Etoposide [158] (3) Lobaplatin/Irinotecan [159] | small-cell lung cancer |
| (4) Lobaplatin/Pemetrexed/Bevacizumab/Temozolomide [160] | lung adenocarcinoma |
| (5) Lobaplatin/Capecitabine [161] (6) Lobaplatin/Docetaxel [162] | breast cancer |
| (7) Lobaplatin/Fluorouracil [163] (8) Lobaplatin/Fluorouracil/Leucovorin [164] (9) Lobaplatin/Paclitaxel [165] | esophageal carcinoma |
| (10) Lobaplatin/Paclitaxel [166] | gastric cancer |
Table 6.
Dose-limiting effects of Cisplatin its derivatives.
| Toxicity | Drugs |
|---|---|
| Neurotoxicity | Cisplatin [51], Carboplatin [51], Oxaliplatin [51] |
| Nephrotoxicity | Cisplatin [178], Heptaplatin [179] |
| Ototoxicity | Cisplatin [180] |
| Myelosuppression (thrombocytopenia) | Carboplatin [51], Oxaliplatin [104], Nedaplatin [105], Lobaplatin [152], Satraplatin [174] |
| Myelosuppression (neutropenia) | Carboplatin [51], Satraplatin [174] |
| Gastrointestinal toxicity | Oxaliplatin [104] |
Table 7.
Mechanisms of action of anticancer drugs, applied in combination therapy with platinum derivatives.
Table 7.
Mechanisms of action of anticancer drugs, applied in combination therapy with platinum derivatives.
| Drugs | Mechanism | Target |
|---|---|---|
| Cyclophosphamide, Ifosfamide, Mitomycin C | DNA alkylators | DNA breaks |
| Bleomycin, Dactinomycin, Peplomycin | DNA cross-link breaks | |
| Capecitabine, Fluorouracil, S-1 | thymidilate synthase inhibition | DNA-related proteins |
| Gemcitabine | ribonucleotide reductase inhibition | |
| Pemetrexed | dihydrofolic reductase, thymidilate synthase, formyltransferase ribonucleotide inhibition | |
| Cytarabine, Fludarabine | DNA polymerase and ribonucleotide reductase inhibition | |
| Decitabine | DNA demethylation | |
| Methotrexate | dihydrofolic reductase inhibition | |
| Camptotecins: Belotecan, Irinotecan, Topotecan | topoisomerase I inhibition | |
| Etoposide, Amrubicin, Doxorubicin, Epirubicin | topoisomerase II inhibition | |
| Dexamethasone, Prednisolone, Prednisone | transcriptional interaction with specific genes | Modification of genes |
| Trastuzumab | HER 2 inhibition | Tumor cells membrane receptors |
| Cetuximab | epidermalgrowth factor receptors (EGFR) (Her-1) inhibition | |
| Bevacizumab | vascular endothelial growth factor receptors (VEGFR) inhibition | |
| Imatinib | tyrosine kinase inhibition | Tumor cells intracellular pathways |
| Cabazitaxel, Docetaxel, Paclitaxel, Nab-Paclitaxel | microtubule stabilization | |
| Viblastine, Vincristine, Vinorelbine | inhibition of microtubule polymerization |
Table 8.
Combinations of Cisplatin derivatives with antimetabolites and with S-1.
| Drugs | Cisplatin and Derivatives |
|---|---|
| Cisplatin | |
| Capecitabine | breast [28], gastric [36], and biliary cancer [40], esophageal carcinoma [216] |
| Fluorouracil | head and neck cancer [56,217], esophageal [216], conjunctival [218], and nasopharyngeal [219] squamous cell carcinoma [218], nasopharyngeal [220], bladder [221], and cervical cancer [222] |
| S-1 | pancreatic [223], and cervical cancer [224] |
| Gemcitabine | breast [225], pancreatic [226], bladder [221], biliary [40], ovarian [227], cervical [228], and non-small-cell lung cancer [22], urothelial carcinoma [229] |
| Pemetrexed | non-squamous non-small-cell lung cancer [221,230] |
| Methotrexate | bladder cancer [221] |
| Carboplatin | |
| Fluorouracil | non-small-cell lung cancer [209], esophageal [216], and head and neck squamous cell carcinoma [56] |
| Gemcitabine | breast [69], ovarian [231], salivary gland [54], and non-small-cell lung cancer [57], urothelial carcinoma [229] |
| Pemetrexed | non-small-cell lung cancer [61] |
| Oxaliplatin | |
| Capecitabine | esophageal adenocarcinoma [72,216], gastric [89], colon [232], and colorectal cancer [233] |
| Fluorouracil | esophageal [216], colorectal [234], pancreatic [235], and prostate cancer [236] |
| S-1 | colon cancer [237], hepatocellular carcinoma [102] |
| Gemcitabine | pancreatic [226], prostate [238], and germ cell cancer [239] |
| Pemetrexed | head and neck [240], gastric [220], colorectal [241], and prostate cancer [242] |
| Nedaplatin | |
| Capecitabine | nasopharyngeal carcinoma [243] |
| Fluorouracil | head and neck cancer [209], nasopharyngeal [123], and esophageal squamous cell carcinoma [119] |
| S-1 | head and neck squamous cell carcinoma [108] |
| Gemcitabine | non-small-cell lung cancer [110], nasopharyngeal [122], urothelial [129], and lung squamous cell carcinoma [127] |
| Lobaplatin | |
| Capecitabine | breast cancer [161] |
| Fluorouracil | nasopharyngeal [156,157], and esophageal carcinoma [163] |
| Satraplatin | |
| Gemcitabine | prostate, gastric, pancreatic, bladder cancer, hepatocellular and papillary renal carcinoma [174] |
Table 11.
Combinations of Cisplatin derivatiives for therapy of breast and cervical cancer.
| Breast Cancer | Cervical Carncer [222] |
|---|---|
| (1) Cisplatin/Capecitabine [28] | (1) Cisplatin/Ifosfamide |
| (2) Cisplatin/Gemcitabine [225] | (2) Cisplatin/Mitomycin |
| (3) Cisplatin/Docetaxel [259] | |
| (4) Cisplatin/Vinorebine [260] | (3) Cisplatin/Fluorouracil |
| (5) Cisplatin/Cetuximab [29] | (4) Cisplatin/S-1 [224] |
| (6) Cisplatin/Bevacizumab [332] | |
| (7) Cisplatin/Fluorouracil/Vinorelbine (VIFUP) | (5) Cisplatin/Gemcitabine [228] |
| (8) Carboplatin/Gemcitabine [69] | (6) Cisplatin/Topotecan [209] |
| (9) Carboplatin/Docetaxel [261] | |
| (10) Carboplatin/Paclitaxel [262] | (7) Cisplatin/Paclitaxel |
| (11) Carboplatin/Nab-Paclitaxel [264] | (8) Cisplatin/Vinorelbine |
| (12) Carboplatin/Vinorebine [260] | |
| (13) Carboplatin/Veliparib [333] | (9) Cisplatin/Paclitaxel/ |
| (14) Carboplatin/Gemcitabine/Iniparib [69] | Bevacizumab/Pembrolizumab [330] |
| (15) Carboplatin/Gemcitabine/Pembrolizumab [70] | |
| (16) Carboplatin/Docetaxel/Trastuzumab [71] | (10) Carboplatin/Paclitaxel/ |
| (17) Carboplatin/Docetaxel/Trastuzumab/Pertuzumab [71] | Bevacizumab/Pembrolizumab [330] |
| (18) Carboplatin/Paclitaxel/Bevacizumab [329] | |
| (19) Carboplatin/Paclitaxel/Pembrolizumab [331] | (11) Carboplatin/Paclitaxel/ |
| (20) Oxaliplatin/Vinorebine [269] | Bevacizumab [330] |
| (21) Nedaplatin/Docetaxel [260] | |
| (22) Nedaplatin/Vinorebin [260] | (12) Carboplatin/Paclitaxel/ |
| (23) Lobaplatin/Capecitabine [161] | Pembrolizumab [330] |
| (24) Lobaplatin/Docetaxel [162] | |
| (25) Lobaplatin/Vinorebine [260] | (13) Nedaplatin/Paclitaxel [134,135] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Tsvetkova, D.; Ivanova, S. Application of Approved Cisplatin Derivatives in Combination Therapy against Different Cancer Diseases. Molecules 2022, 27, 2466. https://doi.org/10.3390/molecules27082466
AMA Style
Tsvetkova D, Ivanova S. Application of Approved Cisplatin Derivatives in Combination Therapy against Different Cancer Diseases. Molecules. 2022; 27(8):2466. https://doi.org/10.3390/molecules27082466
Chicago/Turabian StyleTsvetkova, Dobrina, and Stefka Ivanova. 2022. "Application of Approved Cisplatin Derivatives in Combination Therapy against Different Cancer Diseases" Molecules 27, no. 8: 2466. https://doi.org/10.3390/molecules27082466