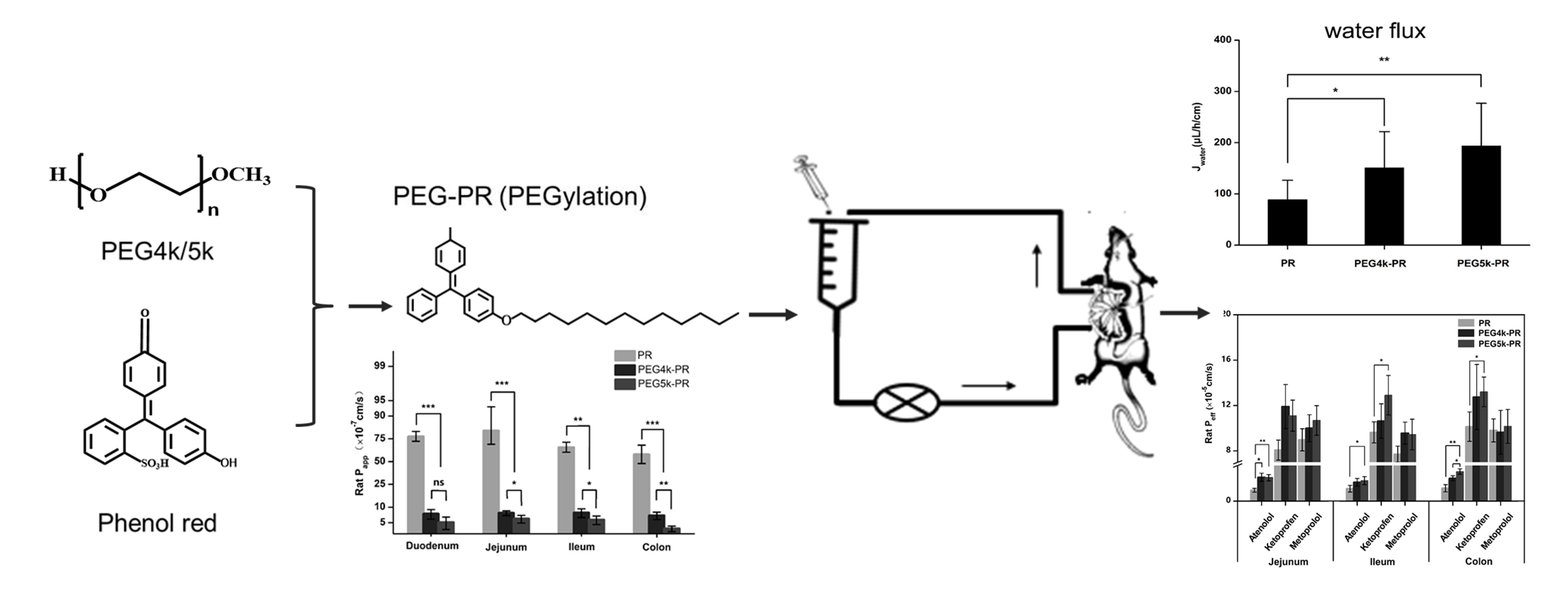
Synthesis and Evaluation of PEG-PR for Water Flux Correction in an In Situ Rat Perfusion Model

Abstract
:
1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Animals
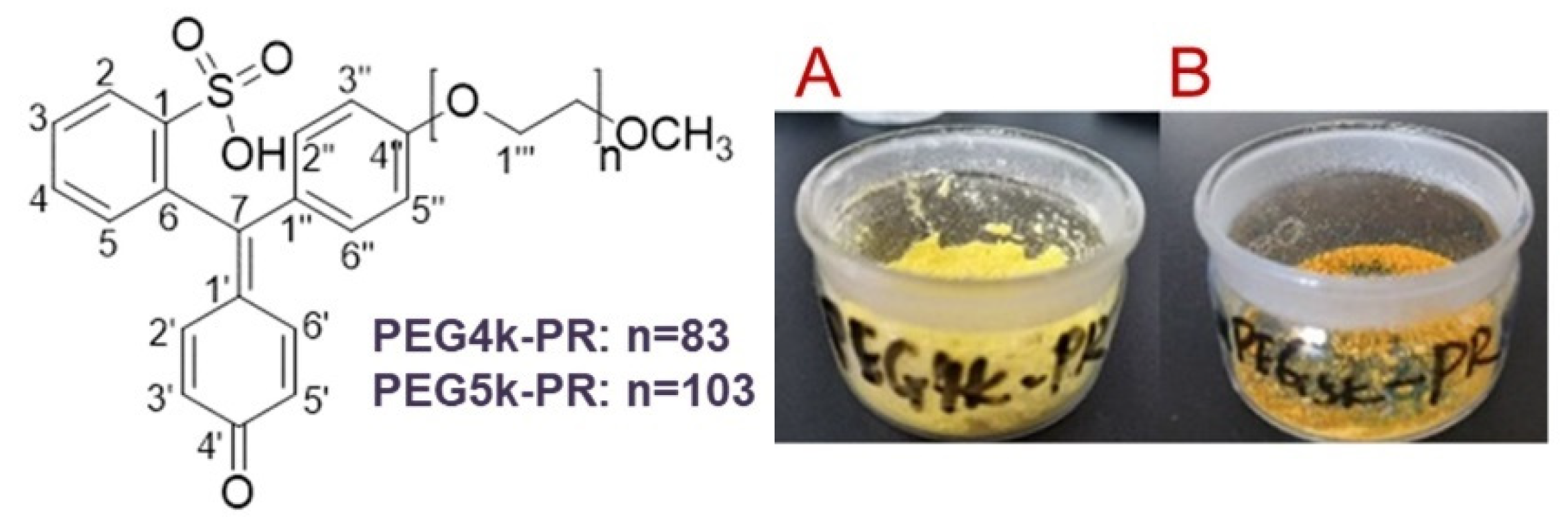
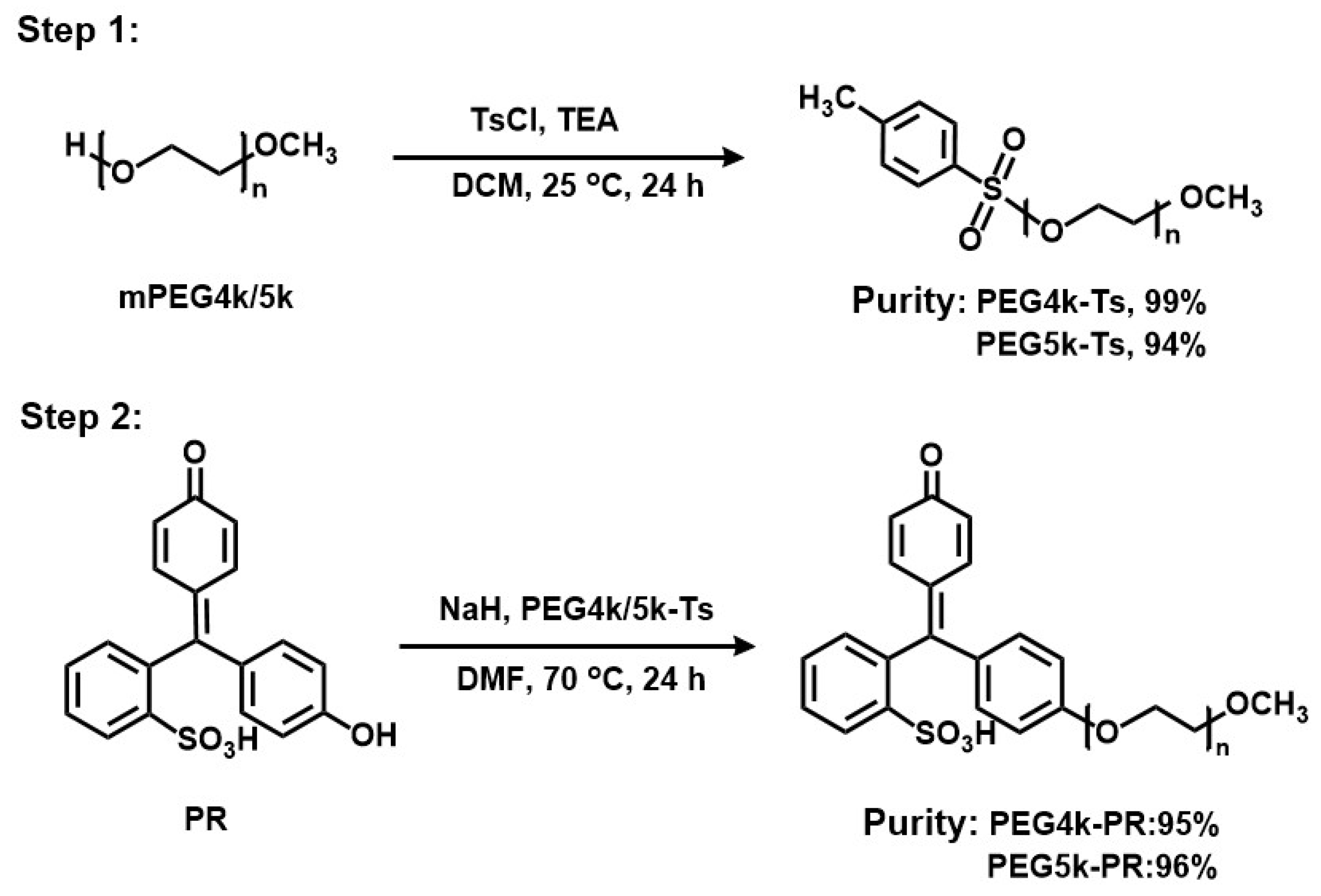
2.3. Synthesis of PEG-PR
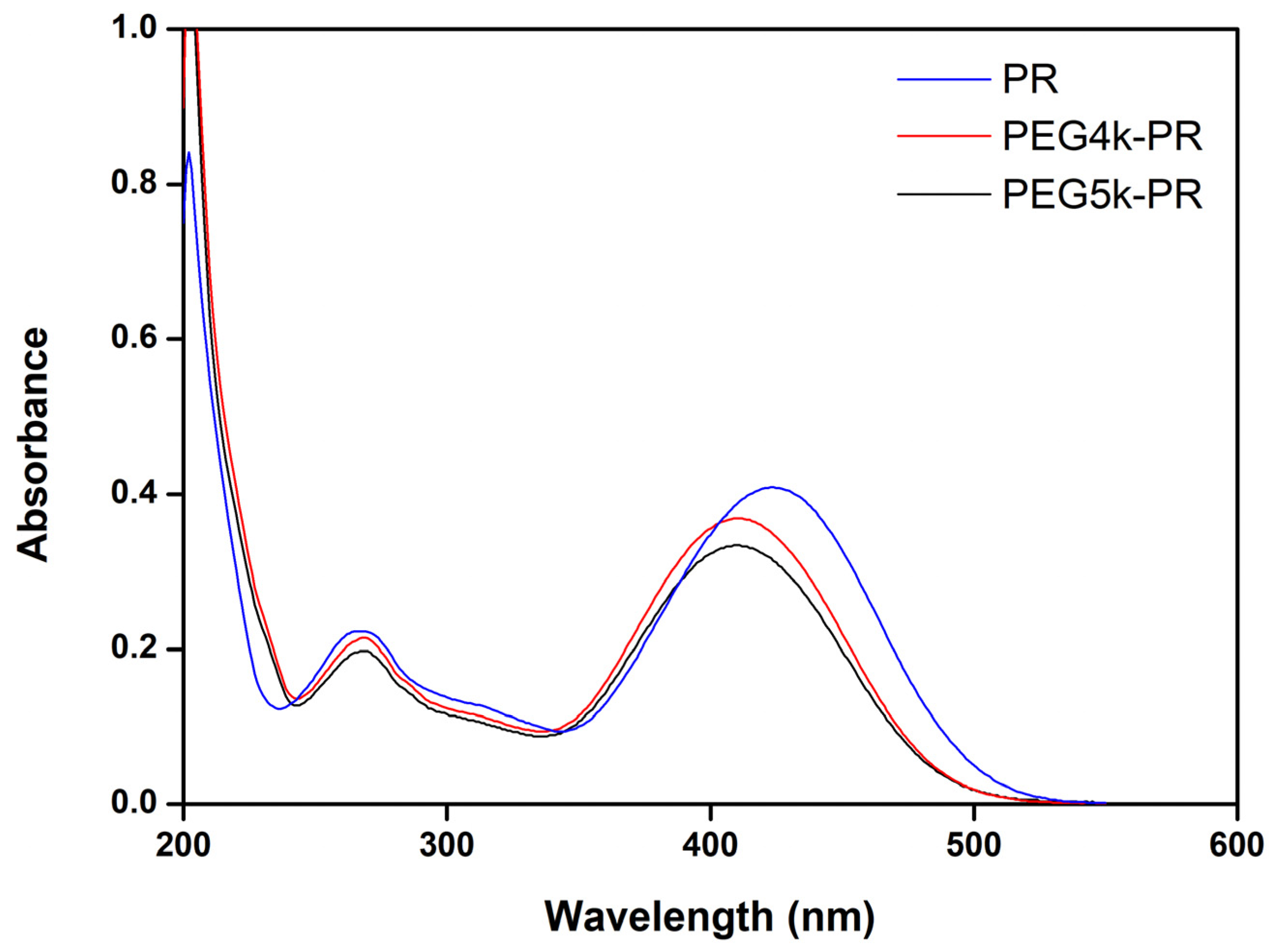
2.4. Characterization of PEG-PR
2.5. Stability of PR and PEG4K/5k-PR
2.6. Permeability of PEG4K/5k-PR in EGS
2.7. Evaluation of PEG4k/5k-PR with the In Situ Perfusion Model
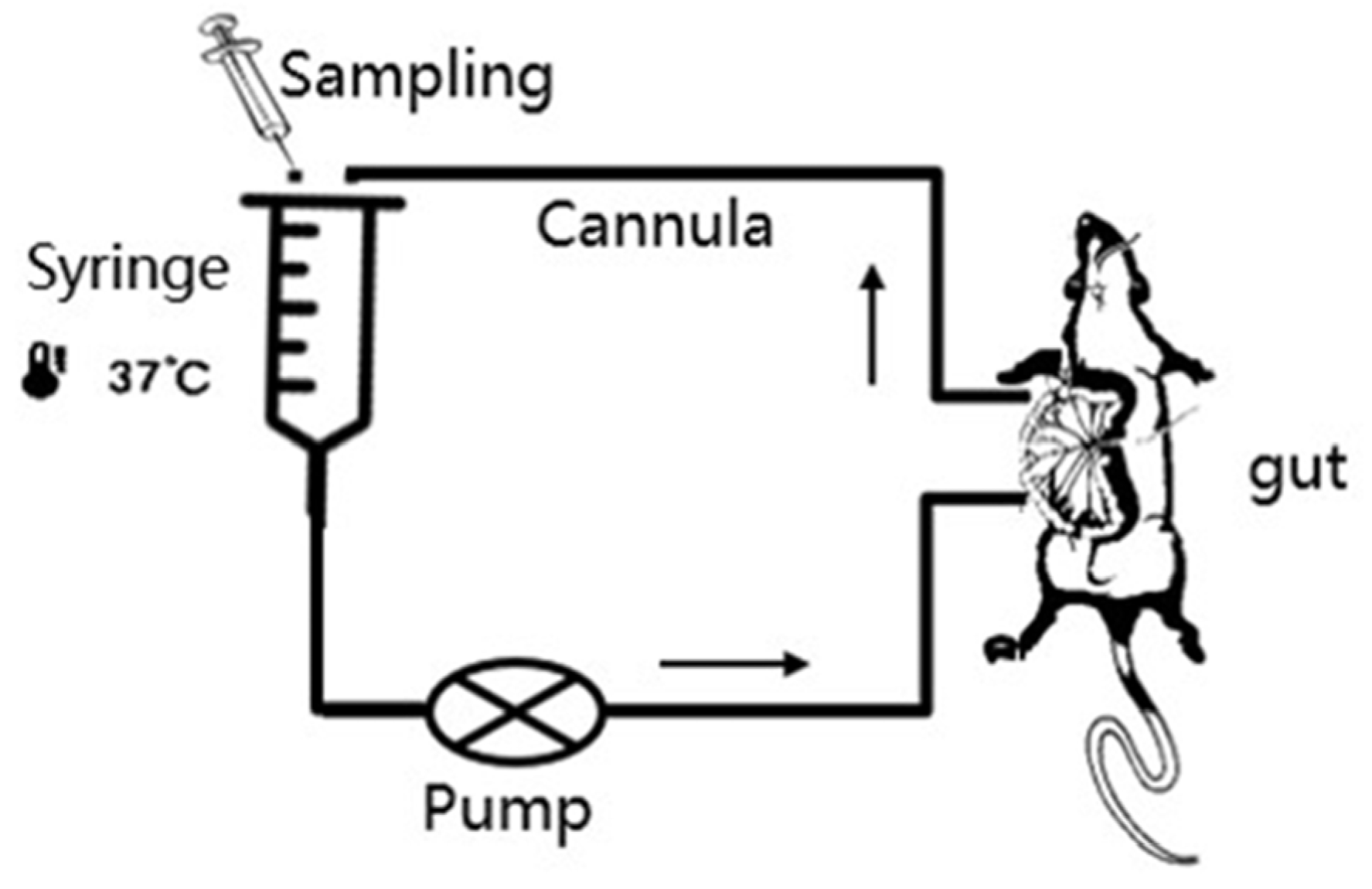
2.7.1. The Recirculation Perfusion Method
2.7.2. Validation of PR and PEG4k/5k-PR for Water Flux (Jwater) Correction
2.8. Analytical Methods
2.9. Statistical Analysis
3. Results and Discussion
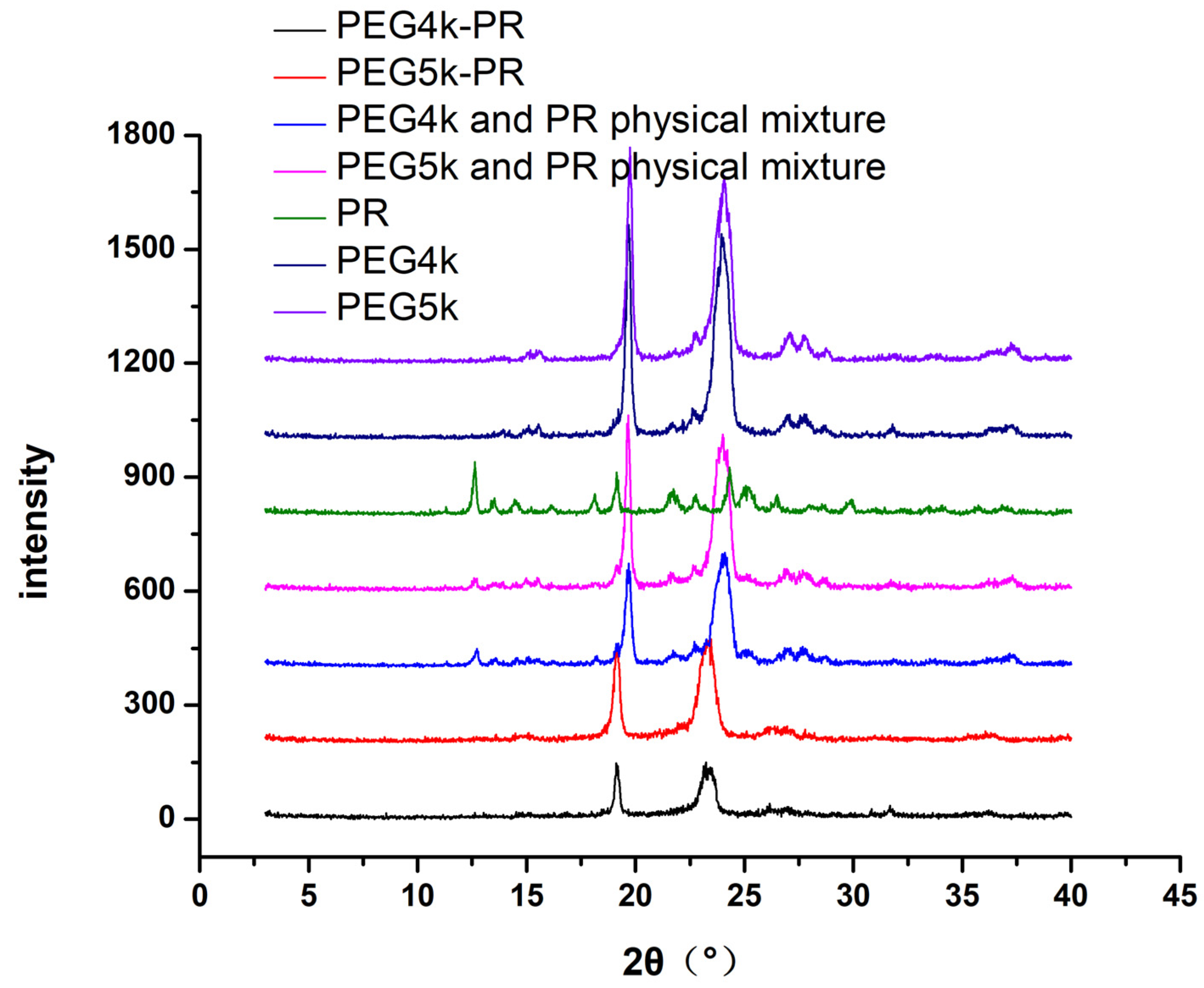
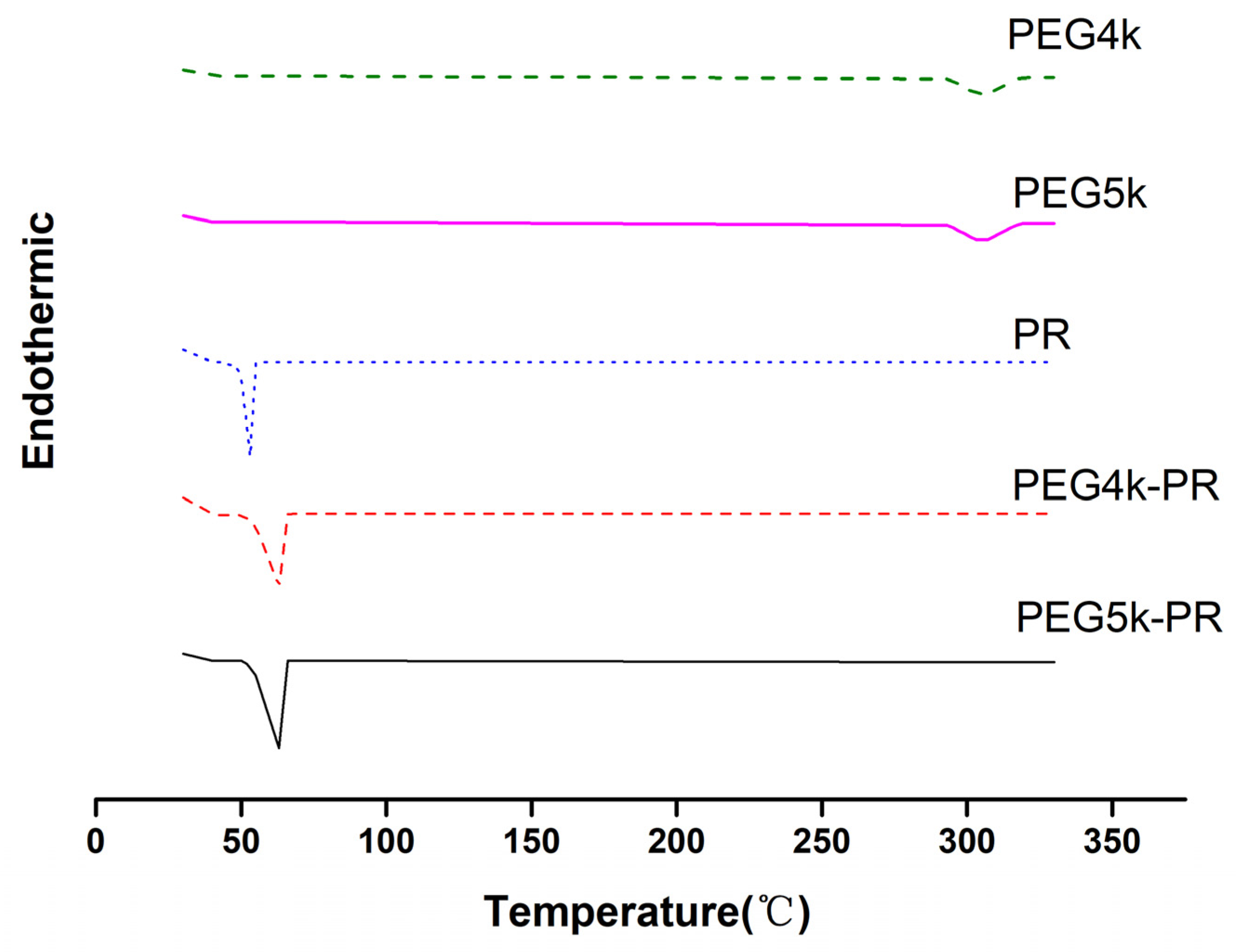
3.1. Synthesis and Characterization of PEG-PR
3.2. Stability of PR and PEG-PR
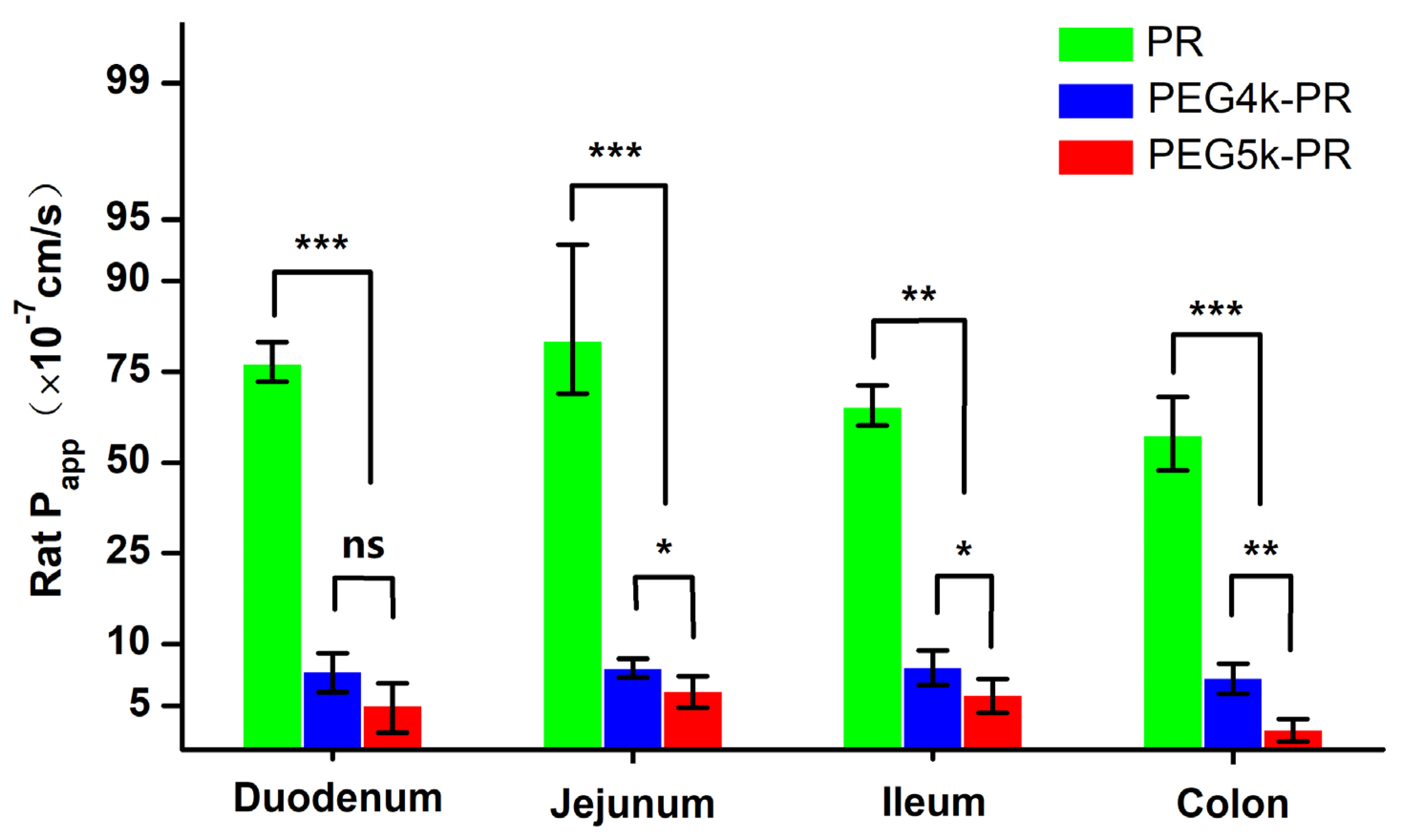
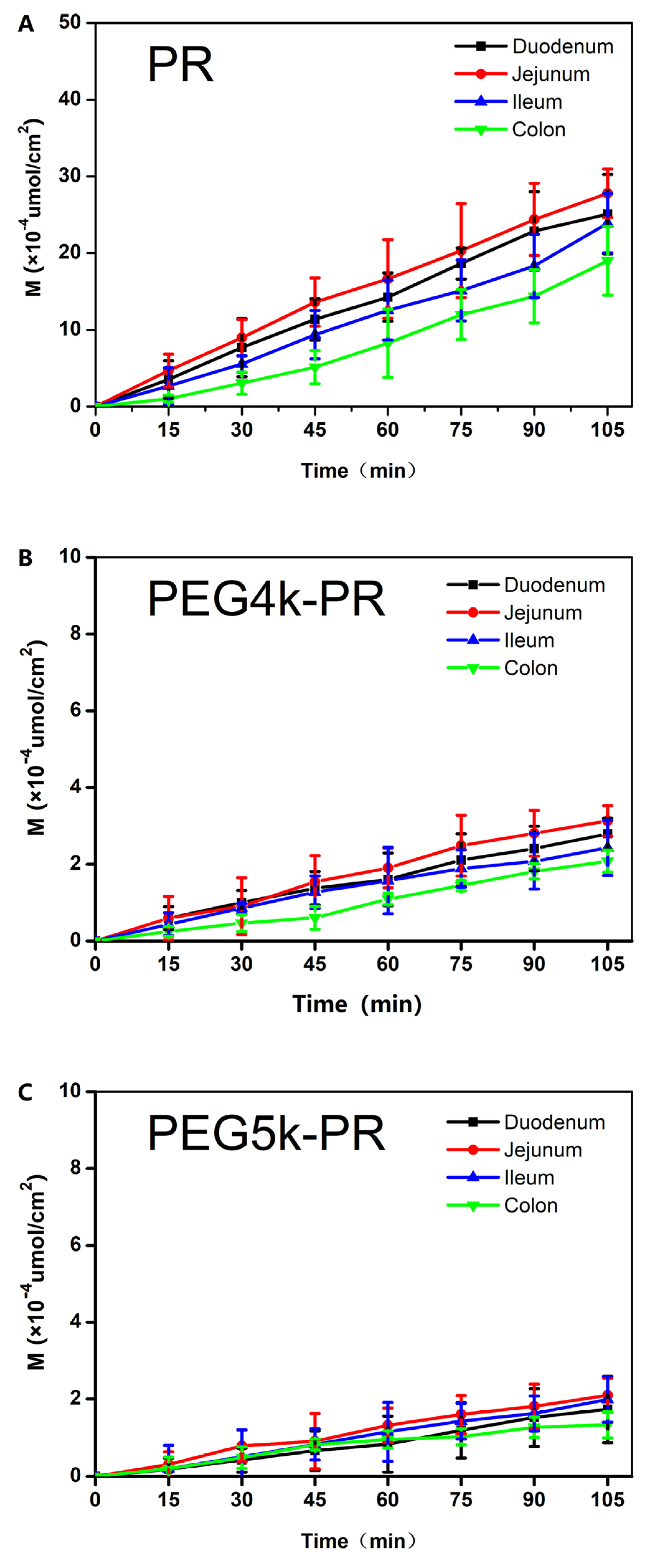
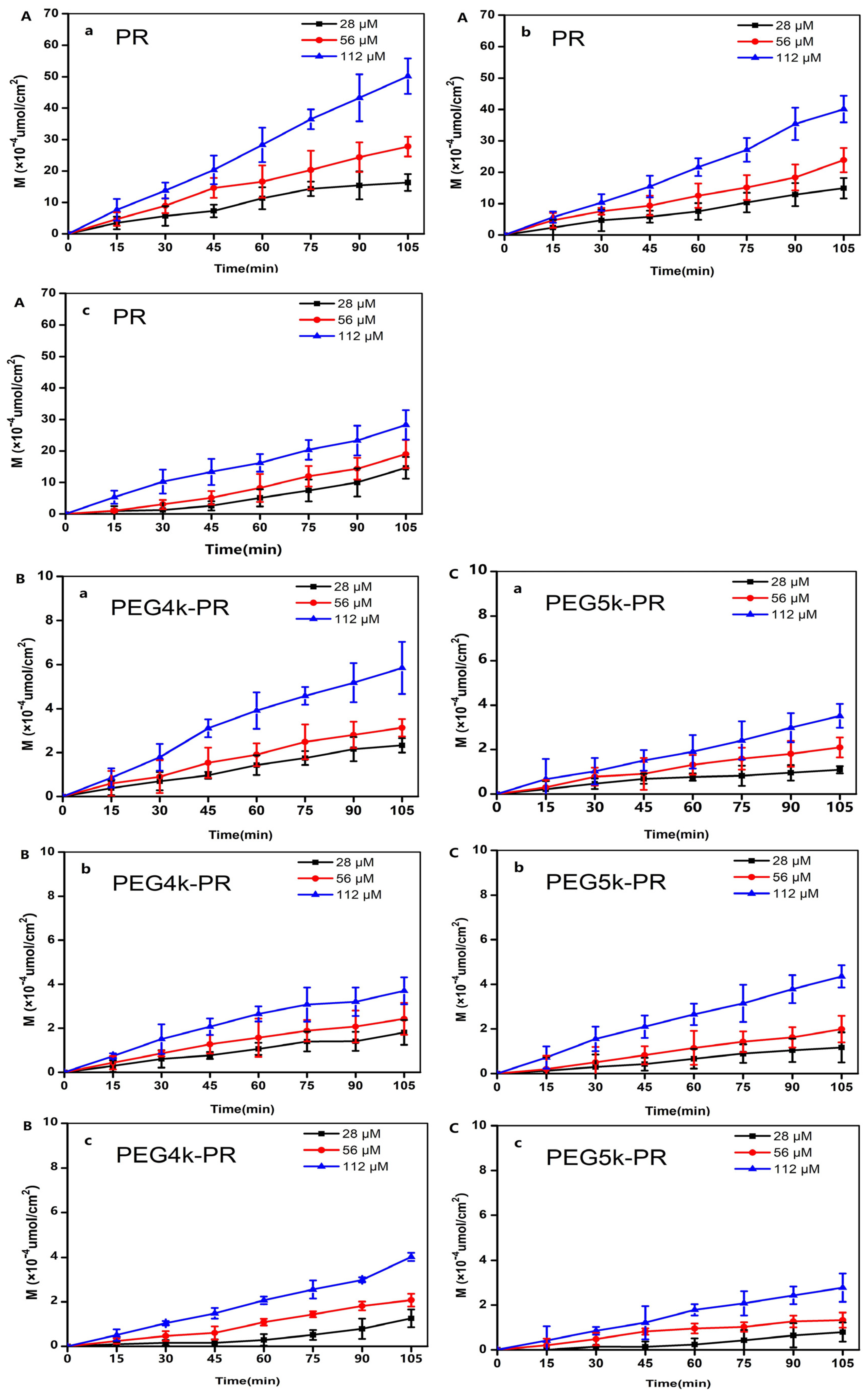
3.3. Permeability of PR and PEG-PR in EGS
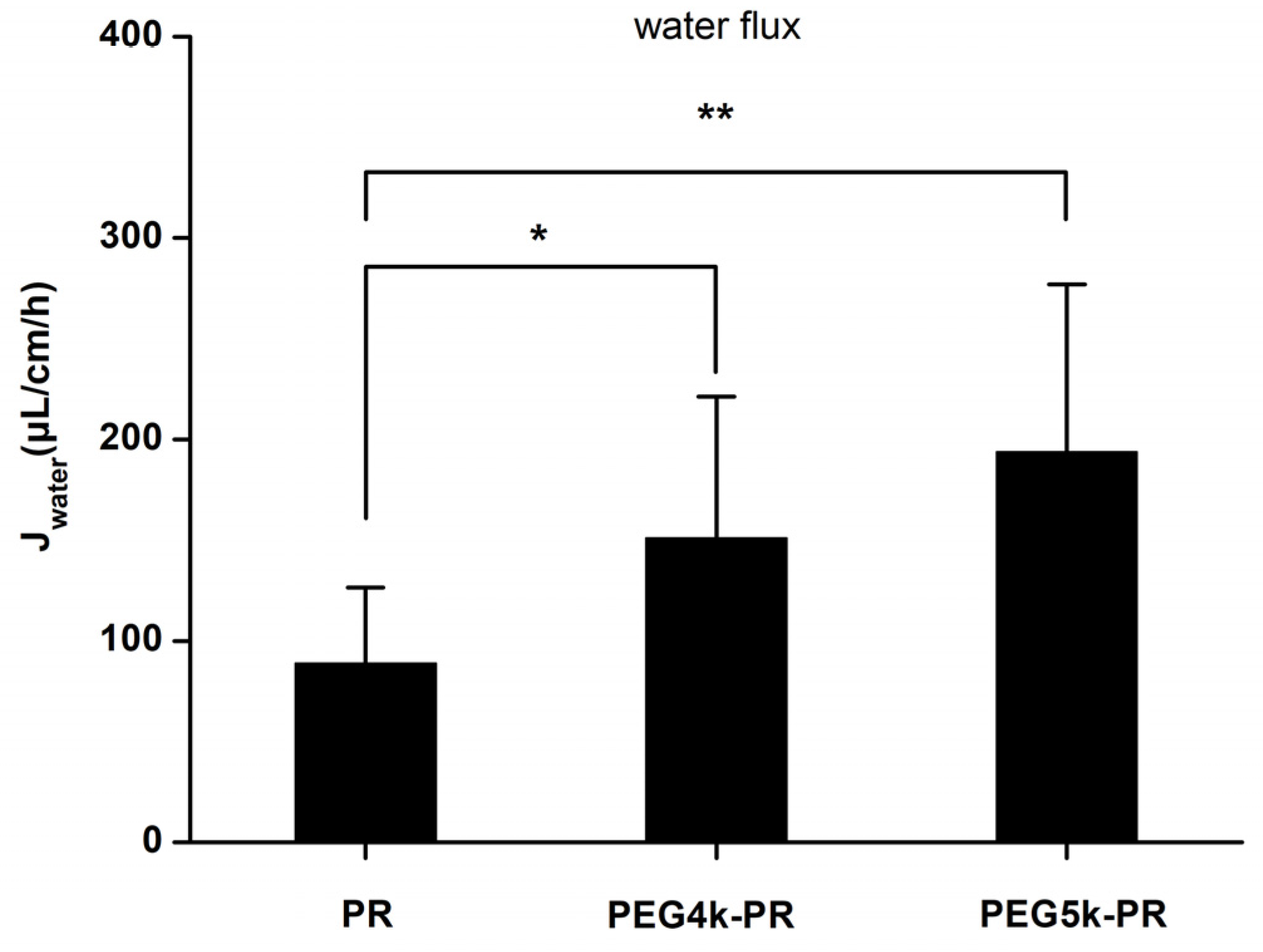
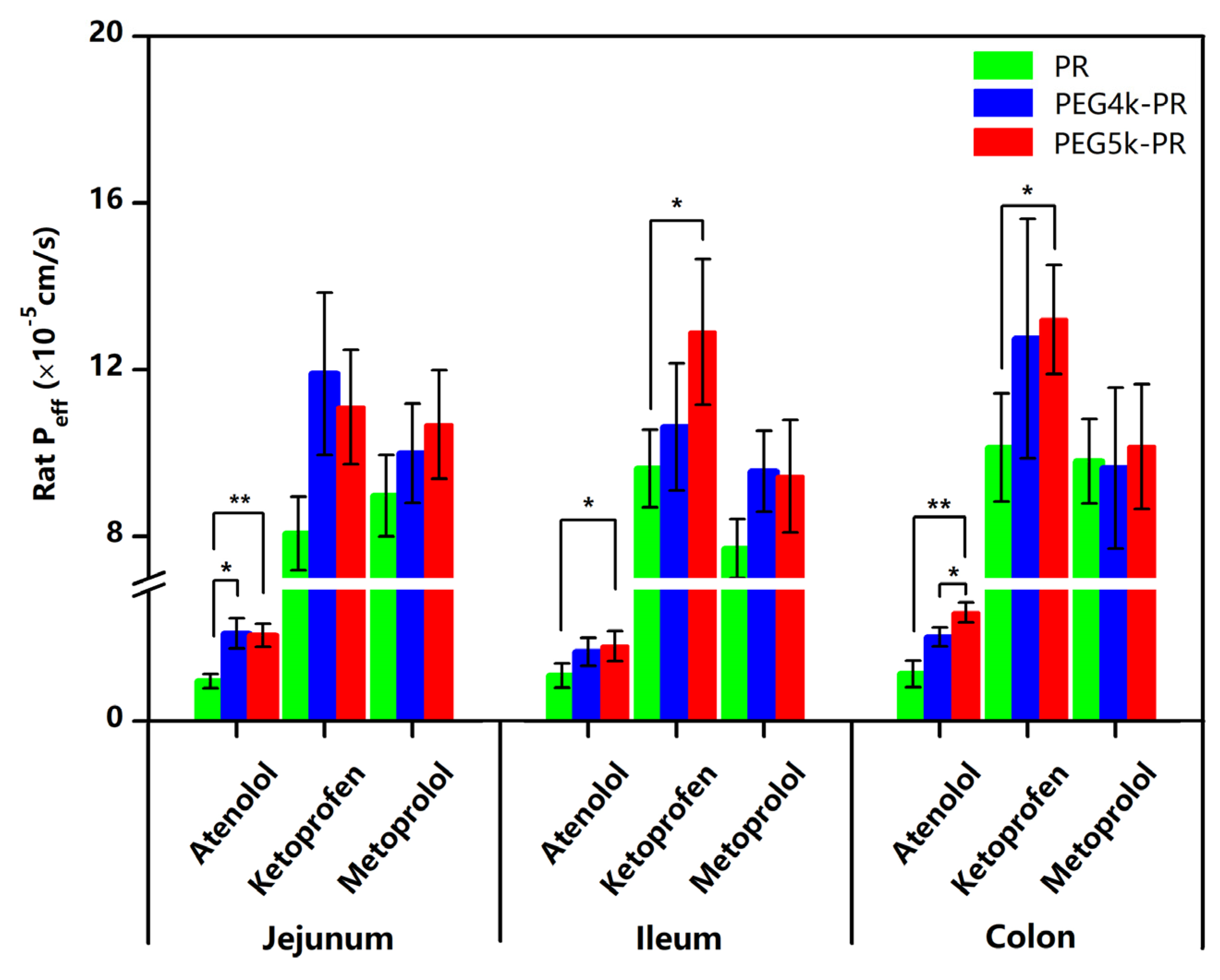
3.4. Evaluation of PR and PEG-PR with the In Situ Perfusion Model
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Amidon, G.L.; Lennernas, H.; Shah, V.P.; Crison, J.R. A theoretical basis for a biopharmaceutic drug classification: The correlation of in vitro drug product dissolution and in vivo bioavailability. Pharm. Res. 1995, 12, 413–420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amidon, K.S.; Langguth, P.; Lennernas, H.; Yu, L.; Amidon, G.L. Bioequivalence of oral products and the biopharmaceutics classification system: Science, regulation, and public policy. Clin. Pharm. 2011, 90, 467–470. [Google Scholar] [CrossRef]
- Varma, M.V.; Gardner, I.; Steyn, S.J.; Nkansah, P.; Rotter, C.J.; Whitney-Pickett, C.; Zhang, H.; Di, L.; Cram, M.; Fenner, K.S.; et al. pH-Dependent solubility and permeability criteria for provisional biopharmaceutics classification (BCS and BDDCS) in early drug discovery. Mol. Pharm. 2012, 9, 1199–1212. [Google Scholar] [CrossRef] [PubMed]
- Lennernas, H. Intestinal permeability and its relevance for absorption and elimination. Xenobiotica 2007, 37, 1015–1051. [Google Scholar] [CrossRef] [PubMed]
- Lennernas, H. Regional intestinal drug permeation: Biopharmaceutics and drug development. Eur. J. Pharm. Sci. 2014, 57, 333–341. [Google Scholar] [CrossRef] [PubMed]
- Sjogren, E.; Dahlgren, D.; Roos, C.; Lennernas, H. Human in vivo regional intestinal permeability: Quantitation using site-specific drug absorption data. Mol. Pharm. 2015, 12, 2026–2039. [Google Scholar] [CrossRef] [PubMed]
- Dahlgren, D.; Roos, C.; Lundqvist, A.; Abrahamsson, B.; Tannergren, C.; Hellstrom, P.M.; Sjogren, E.; Lennernas, H. Regional Intestinal Permeability of Three Model Drugs in Human. Mol. Pharm. 2016, 13, 3013–3021. [Google Scholar] [CrossRef] [PubMed]
- Luo, Z.; Liu, Y.; Zhao, B.; Tang, M.; Dong, H.; Zhang, L.; Lv, B.; Wei, L. Ex vivo and in situ approaches used to study intestinal absorption. J. Pharm. Toxicol. Methods 2013, 68, 208–216. [Google Scholar] [CrossRef] [PubMed]
- Stappaerts, J.; Brouwers, J.; Annaert, P.; Augustijns, P. In situ perfusion in rodents to explore intestinal drug absorption: Challenges and opportunities. Int. J. Pharm. 2015, 478, 665–681. [Google Scholar] [CrossRef]
- Dahan, A.; Wolk, O.; Kim, Y.H.; Ramachandran, C.; Crippen, G.M.; Takagi, T.; Bermejo, M.; Amidon, G.L. Purely in silico BCS classification: Science based quality standards for the world’s drugs. Mol. Pharm. 2013, 10, 4378–4390. [Google Scholar] [CrossRef]
- Cao, X.; Gibbs, S.T.; Fang, L.; Miller, H.A.; Landowski, C.P.; Shin, H.C.; Lennernas, H.; Zhong, Y.; Amidon, G.L.; Yu, L.X.; et al. Why is it challenging to predict intestinal drug absorption and oral bioavailability in human using rat model. Pharm. Res. 2006, 23, 1675–1686. [Google Scholar] [CrossRef] [PubMed]
- Skolnik, S.; Lin, X.; Wang, J.; Chen, X.H.; He, T.; Zhang, B. Towards prediction of in vivo intestinal absorption using a 96-well Caco-2 assay. J. Pharm. Sci. 2010, 99, 3246–3265. [Google Scholar] [CrossRef] [PubMed]
- Amidon, G.E.; Ho, N.F.H.; French, A.B.; Higuchi, W.I. Predicted absorption rates with simultaneous bulk fluid flow in the intestinal tract. J. Theor. Biol. 1981, 89, 195–210. [Google Scholar] [CrossRef]
- Doluisio, J.T.; Billups, N.F.; Dittert, L.W.; Sugita, E.T.; Swintosky, J.V. Drug absorption I: An in situ rat gut technique yielding realistic absorption rates. J. Pharm. Sci. 1969, 58, 1196–1200. [Google Scholar] [CrossRef] [PubMed]
- Rees, H.V.; Wolff, F.A.D.; Noach, E.L. The influence of diphenylhydantoin on intestinal glucose absorption in the rat. Eur. J. Pharmacol. 1974, 28, 310–315. [Google Scholar] [CrossRef]
- Lozoya-Agullo, I.; Gonzalez-Alvarez, I.; Gonzalez-Alvarez, M.; Merino-Sanjuan, M.; Bermejo, M. In Situ Perfusion Model in Rat Colon for Drug Absorption Studies: Comparison with Small Intestine and Caco-2 Cell Model. J. Pharm. Sci. 2015, 104, 3136–3145. [Google Scholar] [CrossRef] [PubMed]
- Lozoya-Agullo, I.; Zur, M.; Beig, A.; Fine, N.; Cohen, Y.; Gonzalez-Alvarez, M.; Merino-Sanjuan, M.; Gonzalez-Alvarez, I.; Bermejo, M.; Dahan, A. Segmental-dependent permeability throughout the small intestine following oral drug administration: Single-pass vs. Doluisio approach to in-situ rat perfusion. Int. J. Pharm. 2016, 515, 201–208. [Google Scholar] [CrossRef]
- Lozoya-Agullo, I.; Zur, M.; Fine-Shamir, N.; Markovic, M.; Cohen, Y.; Porat, D.; Gonzalez-Alvarez, I.; Gonzalez-Alvarez, M.; Merino-Sanjuan, M.; Bermejo, M.; et al. Investigating drug absorption from the colon: Single-pass vs. Doluisio approaches to in-situ rat large-intestinal perfusion. Int. J. Pharm. 2017, 527, 135–141. [Google Scholar] [CrossRef]
- Sjoberg, A.; Lutz, M.; Tannergren, C.; Wingolf, C.; Borde, A.; Ungell, A.L. Comprehensive study on regional human intestinal permeability and prediction of fraction absorbed of drugs using the Ussing chamber technique. Eur. J. Pharm. Sci. 2013, 48, 166–180. [Google Scholar] [CrossRef]
- Grassi, M.; Cadelli, G.J. Theoretical considerations on the in vivo intestinal permeability determination by means of the single pass and recirculating techniques. Int. J. Pharm. 2001, 229, 95–105. [Google Scholar] [CrossRef]
- Tugcu-Demiroz, F.; Gonzalez-Alvarez, I.; Gonzalez-Alvarez, M.; Bermejo, M. Validation of phenol red versus gravimetric method for water reabsorption correction and study of gender differences in Doluisio’s absorption technique. Eur. J. Pharm. Sci. 2014, 62, 105–110. [Google Scholar] [CrossRef] [PubMed]
- Sutton, S.C.; Rinaldi, M.T.S.; Vukovinsky, K.E. Comparison of the gravimetric, phenol red, and 14C-PEG-3350 methods to determine water absorption in the rat single-pass intestinal perfusion model. AAPS Pharmsci. 2001, 3, 93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zakeri-Milani, P.; Barzegar-Jalali, M.; Tajerzadeh, H.; Azarmi, Y.; Valizadeh, H. Simultaneous determination of naproxen, ketoprofen and phenol red in samples from rat intestinal permeability studies: HPLC method development and validation. J. Pharm. Biomed. Anal. 2005, 39, 624–630. [Google Scholar] [CrossRef]
- Singh, S.P.; Raju, K.S.; Nafis, A.; Jain, G.K. Simultaneous determination of nine model compounds in permeability samples using RP-HPLC: Application to prove the cassette administration principle in single pass intestinal perfusion study in rats. J. Pharm. Biomed. Anal. 2012, 67–68, 71–76. [Google Scholar] [CrossRef]
- Winne, D.; Görig, H. Appearance of 14C-polyethylene glycol 4000 in intestinal venous blood: Influence of osmolarity and laxatives, effect on net water flux determination. Naunyn-Schmiedeberg’s Arch. Pharmacol. 1982, 321, 149–156. [Google Scholar] [CrossRef]
- Tur, K.M.; Ch’ng, H.S.; Baie, S. Effect of bioadhesive polymer on phenol red absorption in normal and ulcer rats. Int. J. Pharm. 1997, 156, 59–65. [Google Scholar] [CrossRef]
- Waiver of In Vivo Bioavailability and Bioequivalence Studies for Immediate-Release Solid Oral Dosage Forms Base on a Biopharmaceutics Classification System; Food and Drug Administration: Rockville, MD, USA, 2000.
- An, T.; Liu, Z.; Zhang, Z.; Zhou, J.; Wang, M.; Zou, M.; Cheng, G. Design, synthesis and performance evaluation of mPEG-PR: A novel non-absorbable marker. Eur. J. Pharm. Sci. 2019, 131, 50–57. [Google Scholar] [CrossRef]
- Sha, X.; Fang, X. Transport characteristics of 9-nitrocamptothecin in the human intestinal cell line Caco-2 and everted gut sacs. Int. J. Pharm. 2004, 272, 161–171. [Google Scholar] [CrossRef]
- Barthe, L.; Bessouet, M.; Woodley, J.F.; Houin, G. The improved everted gut sac: A simple method to study intestinal P-glycoprotein. Int. J. Pharm. 1998, 173, 255–258. [Google Scholar] [CrossRef]
- Schedl, H.P.J. Use of polyethylene glycol and phenol red as unabsorbed indicators for intestinal absorption studies in man. Gut 1966, 7, 159–163. [Google Scholar] [CrossRef] [Green Version]
- Higaki, K.; Kato, M.; Hashida, M.; Sezaki, H.J. Enhanced Membrane Permeability to Phenol Red by Medium-Chain Glycerides: Studies on the Membrane Permeability and Microviscosity. Pharm. Res. 1988, 5, 309–312. [Google Scholar] [CrossRef] [PubMed]
- Gotoh, S.; Nakamura, R.; Nishiyama, M.; Quan, Y.S.; Fujita, T.; Yamamoto, A.; Muranishi, S. Effects of protease inhibitors on the absorption of phenol red and fluorescein isothiocyanate dextrans from the rat intestine. J. Pharm. Sci. 1996, 85, 858–862. [Google Scholar] [CrossRef] [PubMed]
- Dahlgren, D.; Roos, C.; Peters, K.; Lundqvist, A.; Tannergren, C.; Sjögren, E.; Sjöblom, M.; Lennernäs, H. Biopharmaceutics. Evaluation of drug permeability calculation based on luminal disappearance and plasma appearance in the rat single-pass intestinal perfusion model. Eur. J. Pharm. Biopharm. 2019, 142, 31–37. [Google Scholar] [CrossRef]
- Whittamore, J.M.; Genz, J.; Grosell, M.; Wilson, R.W. Measuring intestinal fluid transport in vitro: Gravimetric method versus non-absorbable marker. Comp. Biochem. Physiol. Part A Mol. Integr. Physiol. 2016, 194, 27–36. [Google Scholar] [CrossRef] [Green Version]
- Zur, M.; Hanson, A.S.; Dahan, A. The complexity of intestinal permeability: Assigning the correct BCS classification through careful data interpretation. Eur. J. Pharm. Sci. 2014, 61, 11–17. [Google Scholar] [CrossRef]
- Zakeri-Milani, P.; Valizadeh, H.; Tajerzadeh, H.; Islambulchilar, Z.J.D.D.; Pharmacy, I. The utility of rat jejunal permeability for biopharmaceutics classification system. Drug Dev. Ind. Pharm. 2009, 35, 1496–1502. [Google Scholar] [CrossRef]
- Neuhoff, S.; Yeo, K.R.; Barter, Z.; Jamei, M.; Turner, D.B.; Rostami-Hodjegan, A. Application of permeability-limited physiologically-based pharmacokinetic models: Part II-prediction of p-glycoprotein mediated drug–drug interactions with digoxin. J. Pharm. Sci. 2013, 102, 3161–3173. [Google Scholar] [CrossRef]
- Ruiz-Picazo, A.; Lozoya-Agullo, I.; Ortiz-Azcarate, M.; Merino-Sanjuan, M.; Gonzalez-Alvarez, M.; Gonzalez-Alvarez, I.; Bermejo, M. Comparison of segmental-dependent permeability in human and in situ perfusion model in rat. Eur. J. Pharm. Sci. 2017, 107, 191–196. [Google Scholar] [CrossRef] [PubMed]
- Balimane, P.V.; Chong, S.; Morrison, R.A.; Methods, T. Current methodologies used for evaluation of intestinal permeability and absorption. J. Pharmacol. Toxicol. Methods 2000, 44, 301–312. [Google Scholar] [CrossRef]
- Dahlgren, D.; Roos, C.; Sjogren, E.; Lennernas, H. Direct In Vivo Human Intestinal Permeability (Peff) Determined with Different Clinical Perfusion and Intubation Methods. J. Pharm. Sci. 2015, 104, 2702–2726. [Google Scholar] [CrossRef] [Green Version]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Compound (Internal Standard) | Mobile Phase (Aqueous: Organic) | λ (nm) | Retention Time (min) |
|---|---|---|---|
| Phenol red (cresol red) | A: Acetonitrile (40:60, v/v) | 430 | 8.1 (13.2) |
| PEG4k/5k-PR (cresol red) | A: Acetonitrile (46:54, v/v) | 410 | 5.2 (7.9) |
| Atenolol (ranitidine) | B: Acetonitrile (90:10, v/v) | 226 | 7.8 (9.3) |
| Ketoprofen (ibuprofen) | B: Acetonitrile (45:55, v/v) | 220 | 7.5 (17.3) |
| Metoprolol (phenytoin sodium) | C: Methanol (56:44, v/v) | 226 | 7.6 (9.4) |
| NO. | PEG4k-PR | PEG5k-PR |
|---|---|---|
| δH | δH | |
| 2 | 7.90 (1H, dd J = 7.6, 1.1 Hz) | 7.90 (1H, dd J = 7.8, 1.1 Hz) |
| 3 | 7.42 (1H, t, J = 7.3 Hz) | 7.42 (1H, t, J = 6.9 Hz) |
| 4 | 7.37 (1H, t, J = 7.3 Hz) | 7.37 (1H, t, J = 7.4 Hz) |
| 5 | 6.97 (1H, overlapped) | 6.98 (1H, overlapped) |
| 2′ | 7.48 (1H, dd, J = 9.9, 2.5 Hz) | 7.48 (1H, dd, J = 10.0, 2.6 Hz) |
| 3′ | 6.32 (1H, dd, J = 9.9, 1.8 Hz) | 6.32 (1H, dd, J = 10, 2.1 Hz) |
| 5′ | 6.10 (1H, dd, J = 9.9, 1.8 Hz) | 6.10 (1H, dd, J = 10.0, 2.1 Hz) |
| 6′ | 6.85 (1H, dd, J = 9.9, 2.5 Hz) | 6.85 (1H, dd, J = 10.0, 2.6 Hz) |
| 2′’ | 7.35 (1H, d, J = 8.7 Hz) | 7.33 (1H, d, J = 8.8 Hz) |
| 3′’ | 6.97 (1H, d, J = 8.7 Hz) | 6.97 (1H, d, J = 8.8 Hz) |
| 5′’ | 6.97 (1H, d, J = 8.7 Hz) | 6.97 (1H, d, J = 8.8 Hz) |
| 6′’ | 7.35 (1H, d, J = 8.7 Hz) | 7.32 (1H, d, J = 8.7 Hz) |
| 1′’’ | 4.14 (2H, t, J = 4.5 Hz) | 4.14 (2H, t, J = 4.8 Hz) |
| -(OCH2CH2O)n | 3.38–3.74 (457H, overlapped) | 3.38–3.74 (504H, overlapped) |
| -OCH3 | 3.25 (3H, s) | 3.25 (3H, s) |
| Conc. | Jejunum | Ileum | Colon | ||||
|---|---|---|---|---|---|---|---|
| (μM) | Papp (×10−6 cm/s) | W (%) | Papp (×10−6 cm/s) | W (%) | Papp (×10−6 cm/s) | W (%) | |
| P | 28 | 7.68 ± 2.04 | 4.44 ± 1.98 | 6.17 ± 2.17 | 3.55 ± 1.50 | 4.07 ± 1.33 | 2.50 ± 0.82 |
| 56 | 8.36 ± 3.11 | 4.92 ± 1.12 | 6.77 ± 2.32 | 4.23 ± 1.38 | 5.83 ± 1.9 | 3.36 ± 0.79 | |
| 112 | 10.42 ± 2.58 | 5.77 ± 1.70 | 8.90 ± 1.65 | 5.27 ± 2.31 | 8.57 ± 3.54 | 5.18 ± 1.22 | |
| PEG4k-PR | 28 | 0.87 ± 0.15 | 0.81 ± 0.11 | 0.61 ± 0.13 | 0.32 ± 0.05 | ND * | ND * |
| 56 | 0.83 ± 0.21 | 0.55 ± 0.07 | 0.66 ± 0.37 | 0.42 ± 0.13 | 0.51 ± 0.08 | 0.36 ± 0.05 | |
| 112 | 1.36 ± 0.32 | 0.54 ± 0.1 | 0.97 ± 0.28 | 0.63 ± 0.19 | 0.65 ± 0.14 | 0.44 ± 0.13 | |
| PEG5k-PR | 28 | 0.55 ± 0.16 | 0.39 ± 0.15 | 0.69 ± 0.13 | 0.42 ± 0.16 | ND * | ND * |
| 56 | 0.60 ± 0.08 | 0.37 ± 0.07 | 0.57 ± 0.28 | 0.36 ± 0.10 | 0.39 ± 0.07 | 0.24 ± 0.04 | |
| 112 | 0.54 ± 0.23 | 0.35 ± 0.08 | 0.61 ± 0.16 | 0.39 ± 0.04 | 0.41 ± 0.18 | 0.25 ± 0.07 | |
| Drug | Peff (×10−5 cm/s) | ||
|---|---|---|---|
| PR | PEG4k-PR | PEG5k-PR | |
| Atenolol | 0.49 ± 0.10 | 1.06 ± 0.24 | 1.38 ± 0.34 |
| Ketoprofen | 6.76 ± 2.43 | 7.47 ± 1.04 | 8.63 ± 1.26 |
| Metoprolol | 5.11 ± 0.85 | 5.06 ± 0.57 | 5.29 ± 1.49 |
Sample Availability: Samples of the compounds PEG4k-PR and PEG5k-PR are available from the authors. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, G.; Min, X.; Zhang, Q.; Zhang, Z.; Wen, M.; Yang, J.; Zou, M.; Sun, W.; Cheng, G. Synthesis and Evaluation of PEG-PR for Water Flux Correction in an In Situ Rat Perfusion Model. Molecules 2020, 25, 5123. https://doi.org/10.3390/molecules25215123
Chen G, Min X, Zhang Q, Zhang Z, Wen M, Yang J, Zou M, Sun W, Cheng G. Synthesis and Evaluation of PEG-PR for Water Flux Correction in an In Situ Rat Perfusion Model. Molecules. 2020; 25(21):5123. https://doi.org/10.3390/molecules25215123
Chicago/Turabian StyleChen, Guo, Xingqi Min, Qunqun Zhang, Zhiqiang Zhang, Meiqiang Wen, Jun Yang, Meijuan Zou, Wei Sun, and Gang Cheng. 2020. "Synthesis and Evaluation of PEG-PR for Water Flux Correction in an In Situ Rat Perfusion Model" Molecules 25, no. 21: 5123. https://doi.org/10.3390/molecules25215123