
Clinical Characteristics Associated with the Development of Cystoid Macular Edema in Patients with Cytomegalovirus Retinitis



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Subjects
2.2. Ocular Exams and Treatments
2.3. Outcome Measures
2.4. Statistical Analysis
3. Results
3.1. Incidence and Clinical Characteristics of CME in CMV Retinitis
3.2. Clinical Characteristics of CME Eyes in CMV Retinitis according to the Presence of Active Retinitis
3.3. Risk Factors for the Development of CME in CMV Retinitis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jabs, D.A. Cytomegalovirus retinitis and the acquired immunodeficiency syndrome--bench to bedside: LXVII Edward Jackson Memorial Lecture. Am. J. Ophthalmol. 2011, 151, 198–216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jabs, D.A. Ocular manifestations of HIV infection. Trans. Am. Ophthalmol. Soc. 1995, 93, 623–683. [Google Scholar] [CrossRef]
- Jabs, D.A.; Ahuja, A.; Van Natta, M.L.; Lyon, A.T.; Yeh, S.; Danis, R. Long-term Outcomes of Cytomegalovirus Retinitis in the Era of Modern Antiretroviral Therapy: Results from a United States Cohort. Ophthalmology 2015, 122, 1452–1463. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Port, A.D.; Alabi, R.O.; Koenig, L.; Gupta, M.P. Cytomegalovirus retinitis in the post-cART era. Curr. Ophthalmol. Rep. 2018, 6, 133–144. [Google Scholar] [CrossRef] [PubMed]
- Son, G.; Lee, J.Y.; Kim, J.-G.; Kim, Y.J. Clinical features of cytomegalovirus retinitis after solid organ transplantation versus hematopoietic stem cell transplantation. Graefes Arch. Clin. Exp. Ophthalmol. 2021, 259, 585–591. [Google Scholar] [CrossRef] [PubMed]
- Silverstein, B.E.; Smith, J.H.; Sykes, S.O.; Jones, M.R.; Schwartz, D.; Cunningham, E.T., Jr. Cystoid macular edema associated with cytomegalovirus retinitis in patients with the acquired immunodeficiency syndrome. Am. J. Ophthalmol. 1998, 125, 411–415. [Google Scholar] [CrossRef]
- Maguire, A.M.; Nichols, C.W.; Crooks, G.W. Visual loss in cytomegalovirus retinitis caused by cystoid macular edema in patients without the acquired immune deficiency syndrome. Ophthalmology 1996, 103, 601–605. [Google Scholar] [CrossRef]
- Cassoux, N.; Lumbroso, L.; Bodaghi, B.; Zazoun, L.; Katlama, C.; LeHoang, P. Cystoid macular oedema and cytomegalovirus retinitis in patients with HIV disease treated with highly active antiretroviral therapy. Br. J. Ophthalmol. 1999, 83, 47–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Invernizzi, A.; Agarwal, A.; Ravera, V.; Oldani, M.; Staurenghi, G.; Viola, F. Optical Coherence Tomography Findings in Cytomegalovirus Retinitis: A Longitudinal Study. Retina 2018, 38, 108–117. [Google Scholar] [CrossRef] [PubMed]
- Gupta, M.P.; Patel, S.; Orlin, A.; Marlow, E.; Chee, R.I.; Nadelmann, J.; Chan, R.V.P.; D’Amico, D.J.; Kiss, S. Spectral Domain Optical Coherence Tomography Findings in Macula-Involving Cytomegalovirus Retinitis. Retina 2018, 38, 1000–1010. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weinberg, D.V.; Moorthy, R.S. Cystoid macular edema due to cytomegalovirus retinitis in a patient with acquired immune deficiency syndrome. Retina 1996, 16, 343–344. [Google Scholar] [CrossRef] [PubMed]
- Karavellas, M.P.; Lowder, C.Y.; Macdonald, C.; Avila, C.P., Jr.; Freeman, W.R. Immune recovery vitritis associated with inactive cytomegalovirus retinitis: A new syndrome. Arch. Ophthalmol. 1998, 116, 169–175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoshizumi, M.O.; Lee, D.; Vinci, V.; Fajardo, S. Ocular toxicity of multiple intravitreal DHPG injections. Graefes Arch. Clin. Exp. Ophthalmol. 1990, 228, 350–355. [Google Scholar] [CrossRef] [PubMed]
- Wong, M.H.; Cheung, G.C.; Chee, S.P. Posterior segment findings of ocular cytomegalovirus infection in immunocompetent patients. Graefes Arch. Clin. Exp. Ophthalmol. 2014, 252, 1811–1816. [Google Scholar] [CrossRef] [PubMed]
- Herbort, C.P.; Khairallah, M. Editorial: Fuchs’ uveitis: From Imperial Vienna to global appraisal. Int. Ophthalmol. 2010, 30, 449–452. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Patient Level | ||||
|---|---|---|---|---|
| Total (48 patients) | No CME (25 patients) | CME (23 patients) | p Value | |
| Demographics | ||||
| Age, years | 51.50 [35.00, 58.25] | 45.00 [31.00, 54.00] | 57.00 [46.50, 61.00] | 0.036 |
| Female, N (%) | 10 (20.8) | 7 (28.0) | 3 (13.0) | 0.292 |
| Underlying disease, N (%) | 0.304 | |||
| HIV | 6 (12.5) | 2 (8.0) | 4 (17.4) | |
| Solid organ transplantation | 14 (29.2) | 6 (24.0) | 8 (34.8) | |
| Hematologic malignancy | 27 (56.2) | 17 (68.0) | 10 (43.5) | |
| Other disease | 1 (2.1) | 0 (0.0) | 1 (4.3) | |
| Mortality during follow-up, N (%) | 13 (27.1) | 8 (32.0) | 5 (21.7) | 0.523 |
| Total follow-up period, months | 20.37 [3.30, 40.16] | 14.37 [2.23, 45.10] | 22.40 [8.03, 34.63] | 0.445 |
| Clinical Laboratory Methods | ||||
| Peak CMV PCR level, log | 3.92 [3.15, 5.13] | 3.87 [3.19, 4.83] | 3.97 [2.91, 5.45] | 0.725 |
| ANC at diagnosis, count | 2048.50 [990.00, 3582.50] | 1624.00 [930.00, 2500.00] | 2140.00 [1050.00, 4060.00] | 0.317 |
| Viremia period, months | 2.18 [1.16, 5.15] | 2.10 [0.80, 3.27] | 2.57 [1.27, 12.78] | 0.024 |
| Ocular Characteristics | ||||
| Bilateral involvement, N (%) | 19 (39.6) | 11 (44.0) | 8 (34.8) | 0.566 |
| Eye Level | ||||
| Total (67 eyes) | No CME (42 eyes) | CME (25 eyes) | p value | |
| Ocular Characteristics | ||||
| Lens status: Pseudophakia, N (%) | 7 (10.4) | 3 (7.1) | 4 (16.0) | 0.411 |
| Involvement extent, N (%) | ||||
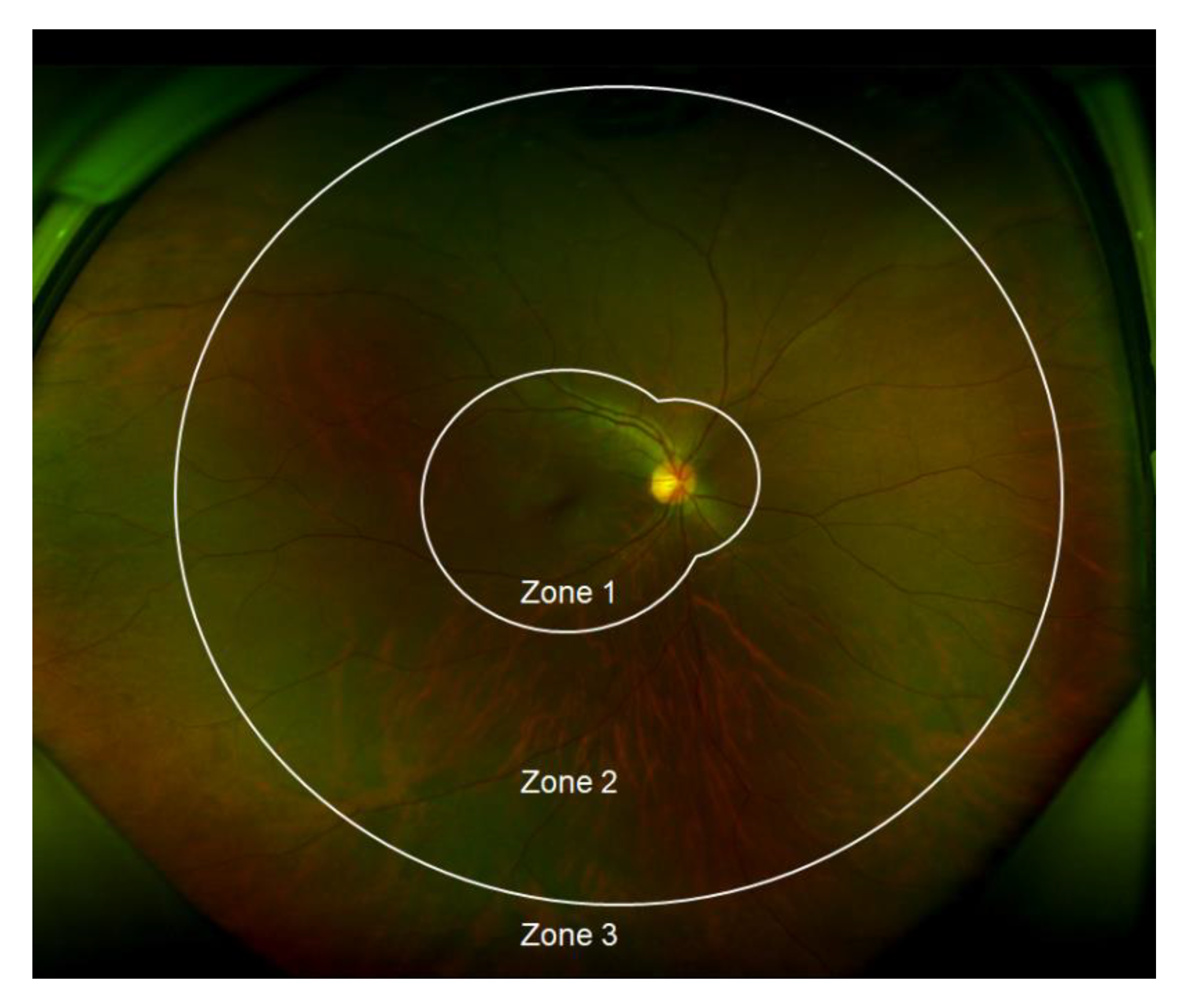
| Zone 1 involvement | 35 (52.2) | 15 (35.7) | 20 (80.0) | 0.001 |
| Foveal involvement | 19 (28.4) | 10 (23.8) | 9 (36.0) | 0.401 |
| ≥ 50% involvement of total retina | 24 (35.8) | 8 (19.0) | 16 (64.0) | < 0.001 |
| Intravitreal GCV injection | ||||
| Total number of injections, N | 5.00 [0.00, 10.00] | 3.00 [0.00, 6.75] | 10.00 [5.00, 17.00] | < 0.001 |
| Number of injections before CME, N | 2.00 [0.00, 8.50] | 3.00 [0.00, 6.75] | 0.00 [0.00, 11.00] | 0.798 |
| Eyes with injections, N (%) | 46 (68.7) | 24 (57.1) | 22 (88.0) | 0.013 |
| Recurrence of CMV retinitis, N (%) | 18 (26.9) | 9 (21.4) | 9 (36.0) | 0.256 |
| Vitrectomy, N (%) | 15 (22.4) | 7 (16.7) | 8 (32.0) | 0.225 |
| Visual outcome, LogMAR | ||||
| Baseline VA | 0.20 [0.10, 0.30] | 0.20 [0.10, 0.40] | 0.10 [0.00, 0.30] | 0.350 |
| Final VA | 0.50 [0.30, 1.35] | 0.35 [0.10, 0.70] | 1.30 [0.50, 1.50] | < 0.001 |
| Change in VA | 0.30 [0.00, 0.90] | 0.10 [−0.08, 0.38] | 0.80 [0.30, 1.30] | 0.001 |
| Patient Level | |||
|---|---|---|---|
| With Active Retinitis (17 Patients) | Without Active Retinitis (6 Patients) | p Value | |
| Demographics | |||
| Age, years | 57.00 [50.00, 62.00] | 50.50 [34.00, 58.00] | 0.248 |
| Female, N (%) | 2 (11.8) | 1 (16.7) | 1.000 |
| Underlying disease, N (%) | 0.867 | ||
| HIV | 3 (17.6) | 1 (16.7) | |
| Solid organ transplantation | 5 (29.4) | 3 (50.0) | |
| Hematologic malignancy | 8 (47.1) | 2 (33.3) | |
| Other disease | 1 (5.9) | 0 (0.0) | |
| Mortality during follow-up, N (%) | 4 (23.5) | 1 (16.7) | 1.000 |
| Total follow-up period, months | 12.03 [4.90, 34.40] | 26.31 [24.11, 34.35] | 0.093 |
| Clinical Laboratory Methods | |||
| Peak CMV PCR level, log | 3.54 [2.80, 5.43] | 4.27 [3.78, 5.34] | 0.420 |
| ANC at diagnosis, count | 2140.00 [1010.00, 4100.00] | 2030.00 [1210.00, 3637.50] | 0.889 |
| Viremia period, months | 1.80 [1.20, 4.03] | 16.75 [9.07, 20.61] | 0.050 |
| Ocular Characteristics | |||
| Bilateral involvement, N (%) | 5 (29.4) | 3 (50.0) | 0.621 |
| Eye Level | |||
| With active retinitis (17 eyes) | Without active retinitis (8 eyes) | p value | |
| Ocular Characteristics | |||
| Timing of CME development, months | 0.17 [0.00,2.34] | 15.80 [10.98, 20.88] | < 0.001 |
| Lens status: Pseudophakia, N (%) | 2 (11.8) | 2 (25.0) | 0.570 |
| Involvement extent, N (%) | |||
| Zone 1 involvement | 13 (76.5) | 7 (87.5) | 1.000 |
| Foveal involvement | 9 (52.9) | 0 (0.0) | 0.022 |
| ≥ 50% involvement of total retina | 8 (47.1) | 8 (100.0) | 0.022 |
| Intravitreal GCV injection | |||
| Total number of injections, N | 9.00 [5.00, 13.00] | 13.50 [9.25, 23.75] | 0.280 |
| Number of injections before CME, N | 0.00 [0.00, 2.00] | 13.00 [8.25, 21.00] | 0.006 |
| Posterior vitreous cell, N (%) | 12 (70.6) | 8 (100.0) | 0.140 |
| Vitreous opacity, N (%) | 6 (35.3) | 4 (50.0) | 0.667 |
| Recurrence of CMV retinitis, N (%) | 2 (11.8) | 7 (87.5) | 0.001 |
| Vitrectomy, N (%) | 4 (23.5) | 4 (50.0) | 0.359 |
| Visual outcome, LogMAR | |||
| Baseline VA | 0.30 [0.10, 0.30] | 0.00 [0.00, 0.10] | 0.016 |
| Final VA | 1.40 [0.90, 1.50] | 0.45 [0.38, 2.22] | 0.279 |
| Change in VA | 1.00 [0.50, 1.20] | 0.40 [0.27, 2.15] | 0.793 |
| Total (25 Eyes) | With Active Retinitis (17 Eyes) | Without Active Retinitis (8 Eyes) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Treatment Modality | Treatment Response | Treatment Modality | Treatment Response | ||||||
| Complete Resolution | Partial Resolution | No Response | Complete Resolution | Partial Resolution | No Response | ||||
| Systemic antiviral treatment | |||||||||
| Ganciclovir/Foscarnet | 19 | 17 | 11 | 5 | 1 | 2 | 0 | 1 | 1 |
| Local treatment | |||||||||
| Intravitreal ganciclovir injection | 13 | 12 | 9 | 3 | 0 | 1 | 0 | 1 | 0 |
| Intravitreal bevacizumab injection | 3 | 1 | 0 | 1 | 0 | 2 | 0 | 1 | 1 |
| Intravitreal ganciclovir and bevacizumab injection | 3 | 2 | 2 | 0 | 0 | 1 | 0 | 1 | 0 |
| Topical steroid | 1 | 0 | 0 | 1 | 0 | 2 | 0 | 2 | 0 |
| Topical NSAIDs | 5 | 2 | 0 | 1 | 1 | 3 | 2 | 1 | 0 |
| Univariate Analysis | Multivariable Analysis | |||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p Value | OR | 95% CI | p Value | |
| Demographics | ||||||
| Age | 1.03 | 1.00–1.07 | 0.132 | |||
| Female (vs. male) | 0.29 | 0.08–1.16 | 0.079 | |||
| HIV (vs. non-HIV) | 1.92 | 0.42–8.77 | 0.399 | |||
| Mortality during follow-up | 0.81 | 0.24–2.79 | 0.736 | |||
| Serology | ||||||
| Peak CMV PCR level | 1.05 | 0.70–1.60 | 0.800 | |||
| ANC at diagnosis | 1.00 | 1.00–1.01 | 0.296 | |||
| Viremia period | 1.11 | 1.04–1.18 | 0.002 | 1.10 | 1.00–1.20 | 0.045 |
| Ocular characteristics | ||||||
| Involvement extent | ||||||
| Zone 1 involvement(vs. no involvement) | 7.16 | 2.32–22.16 | <0.001 | 4.25 | 1.25–14.48 | 0.021 |
| Foveal involvement | 1.94 | 0.58–6.62 | 0.288 | |||
| ≥ 50% involvement of total retina | 7.94 | 2.38–26.57 | <0.001 | 3.82 | 0.94–15.57 | 0.062 |
| Intravitreal GCV injection | 1.00 | 0.97–1.07 | 0.532 | |||
| Recurrence of CMV retinitis | 1.88 | 0.58–6.18 | 0.300 | |||
| Visual outcome | ||||||
| Baseline visual acuity | 1.04 | 0.38–2.94 | 0.934 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kwon, H.-J.; Son, G.; Lee, J.-Y.; Kim, J.-G.; Kim, Y.-J. Clinical Characteristics Associated with the Development of Cystoid Macular Edema in Patients with Cytomegalovirus Retinitis. Microorganisms 2021, 9, 1114. https://doi.org/10.3390/microorganisms9061114
Kwon H-J, Son G, Lee J-Y, Kim J-G, Kim Y-J. Clinical Characteristics Associated with the Development of Cystoid Macular Edema in Patients with Cytomegalovirus Retinitis. Microorganisms. 2021; 9(6):1114. https://doi.org/10.3390/microorganisms9061114
Chicago/Turabian StyleKwon, Hye-Ji, Gisung Son, Joo-Yong Lee, June-Gone Kim, and Yoon-Jeon Kim. 2021. "Clinical Characteristics Associated with the Development of Cystoid Macular Edema in Patients with Cytomegalovirus Retinitis" Microorganisms 9, no. 6: 1114. https://doi.org/10.3390/microorganisms9061114