Arthritogenic Alphaviruses: A Worldwide Emerging Threat?

1
Populations Virales et Pathogenèse, Institut Pasteur, CNRS UMR 3569, 75015 Paris, France
2
Ecole doctorale BioSPC, Université Paris Diderot, Sorbonne Paris Cité, 75013 Paris, France
*
Author to whom correspondence should be addressed.
Microorganisms 2019, 7(5), 133; https://doi.org/10.3390/microorganisms7050133
Submission received: 24 April 2019
/
Revised: 9 May 2019
/
Accepted: 10 May 2019
/
Published: 14 May 2019
(This article belongs to the Special Issue Emerging Vector Borne Infections: A Novel Threat for Global Health)
Abstract
:Arthritogenic alphaviruses are responsible for a dengue-like syndrome associated with severe debilitating polyarthralgia that can persist for months or years and impact life quality. Chikungunya virus is the most well-known member of this family since it was responsible for two worldwide epidemics with millions of cases in the last 15 years. However, other arthritogenic alphaviruses that are as of yet restrained to specific territories are the cause of neglected tropical diseases: O’nyong’nyong virus in Sub-Saharan Africa, Mayaro virus in Latin America, and Ross River virus in Australia and the Pacific island countries and territories. This review evaluates their emerging potential in light of the current knowledge for each of them and in comparison to chikungunya virus.
1. Introduction
Alphaviruses are a genus of enveloped positive-stranded RNA viruses belonging to the Togaviridae family. As arboviruses, they circulate between an invertebrate vector (mosquitoes) and a vertebrate host. They are distributed worldwide and are separated into two groups: the New World alphaviruses responsible for disease with neurological involvement and the Old World alphaviruses (or Semliki forest virus group) that have a rheumatic tropism. The latter, also called arthritogenic alphaviruses, notably include chikungunya virus (CHIKV), now widely distributed, O’nyong’nyong virus (ONNV) located in Sub-Saharan Africa, Mayaro virus (MAYV) in Latin America, and Ross River virus (RRV) in Australia and the Pacific island countries and territories [1] (Table 1).
CHIKV emergence in the Indian Ocean islands in 2005–2006 [2,3] and throughout the Caribbean states and the Americas in 2013–2014 [4] has raised awareness of the threat that other alphaviruses represent. While ONNV, MAYV, and RRV are currently responsible for smaller, local epidemics, the risk of dissemination worldwide is real, promoted by international trade and travel, globalization, and climate change.
In this work, we review the current knowledge on CHIKV and compare it to these three less-described alphaviruses (ONNV, MAYV, and RRV) circulating in three distinct continents, to try to understand their emergence potential in the near future.
2. Historical Description and Main Epidemics
2.1. Chikungunya Virus
Robinson first described chikungunya fever in 1955, after an epidemic of dengue-like fever with extremely severe joint pain in Southern Tanganyika (now Tanzania) in 1952–1953 [7]. Its name comes from the Kimakonde language meaning “that which bends up” describing this particular clinical manifestation.
Three main chikungunya virus genotypes, named after their original geographical distribution, are described: the West African, the East-Central-Southern African (ECSA, including Indian Ocean lineage), and the Asian genotypes (that include the Caribbean strains) [8,9]. Before 2000, chikungunya virus had been circulating mainly in Sub-Saharan Africa (Zimbabwe [10,11], Nigeria [12], Angola [13], South Africa [14], Democratic Republic of Congo [15,16], Senegal [17,18]) and South-East Asia (India [19,20,21,22], Sri-Lanka [21], Vietnam [23], Thailand [24], Malaysia [25], Indonesia [26,27]) where numerous local outbreaks have been reported. Since then, two worldwide epidemics occurred that pushed chikungunya virus into the spotlight.
The first epidemic, caused by the Indian Ocean lineage, started in coastal Kenya in august 2004 with an attack rate of over 50% [2] and rapidly disseminated to the Comoros islands in December 2004–March 2005 [28], and from there to Mayotte, Mauritius, La Reunion, and the Seychelles [29], infecting hundreds of thousands of people at the end of 2005 through the beginning of 2006. Because La Reunion Island is a French territory with a developed public health infrastructure and surveillance system, the epidemic gathered more global attention after making the headlines. It also disseminated through India and South-East Asia, and into southern Europe because of air travel, causing altogether approximately six million cases in more than 40 countries [2,3].
2.2. O’nyong’nyong Virus
Although genetically distinct from CHIKV, ONNV is its most closely related relative [8]. Similar to CHIKV, it can cause large-scale epidemics in Africa, but infection by ONNV has never been reported outside of this continent. The first described ONNV outbreak took place during the first half of 1959 in north-western Uganda (Gulu), before it crossed the border to Belgian Congo and Sudan, causing close to 750,000 cases [38]. This epidemic lasted until 1962, spreading from eastern to western Africa and permitting the first isolation of the virus in human serum [39]. In 1984–1985, it caused another outbreak in Ivory Coast [40], and although it was then called Igbo-Ora virus, it is now clear that it was in fact a lineage of ONNV [8,41]. A third epidemic took place in southern Uganda in 1996–1997 with 40–80% of the population infected [42,43]. More recently (2003), an outbreak in a Liberian refugee camp was reported in Ivory Coast [44].
2.3. Mayaro Virus
MAYV was first described in Trinidad where it caused mild to moderate short febrile illness in five humans in 1954 [45]. In 1959, it caused an epidemic among colonists in the Bolivian rain forest under the name of Uruma virus, which has since been proven to be MAYV [46]. Since then, it has been responsible for several small outbreaks or sporadic cases in rural areas around tropical forests in South and Central America (Brazil [47,48,49,50,51], Bolivia [52], Ecuador [53], Venezuela [54,55], Peru [56,57], French Guyana [58], Suriname [59], Mexico [60], Haiti [61]).
2.4. Ross River Virus
Epidemic polyarthritis has been described since 1886 in rural Australia [62,63]. The virus responsible for this was first isolated in 1959 from infected mosquitoes along the Ross River in Queensland, Australia [64]. Because patients suffering from epidemic polyarthritis had antibodies against RRV, it was thought to be the agent responsible for the disease [65,66]. In 1971, it was first isolated from an aboriginal boy in Australia [67], confirming this hypothesis. Since then, frequent RRV outbreaks have been reported in Australia [68,69,70] with close to 5000 cases/year [71]. RRV also circulates in the Pacific island countries and territories [72] since it was introduced in 1979–1980, causing an epidemic with over 500,000 cases and spectacular attack rates in Fiji (90%), the Cook Islands (69%), American Samoa (44%), and New Caledonia (33%) [73,74,75].
3. Sylvatic Versus Urban Cycle
3.1. Chikungunya Virus
Between outbreaks, CHIKV circulates in a sylvatic cycle where non-human primates are the main host [76,77,78,79,80], and sylvatic Aedes mosquitoes (such as Aedes africanus [78], Aedes furcifer-taylori, Ae. luteocephalus, Ae. Dalzieli [18], etc.) are the main vector. Even though these mosquitoes are not particularly anthropophilic, sporadic human cases can originate from that cycle if a human is bitten by an infected mosquito in a rural area. While the western African lineage has never switched to an urban cycle, both the Asian and the ECSA lineages are able to circulate in urban cycles between humans (that become the amplifying host) [81] and anthropophilic urban mosquitoes (Aedes aegypti and Aedes albopictus) [7,38,82]. Interestingly, while Aedes aegypti is usually the main vector of CHIKV in African urban cycles, Aedes albopictus (widely present on La Reunion Island in the Indian Ocean) was the vector responsible for the transmission during the epidemic that bore its name. Indeed, a single mutation, A226V in the E1 glycoprotein, favored the infection and dissemination of the virus in the new Aedes albopictus vector [83,84,85]. Interestingly, this same A226V mutation appeared independently in India, Sri Lanka, Cameroon, and Gabon in settings where Aedes albopictus was suspected to be the vector of the disease. This convergent evolution illustrates the ease with which the virus evolves to improve its transmissibility [4].
3.2. O’nyong’nyong Virus
Mainly circulating in an enzootic cycle, the vertebrate host of ONNV is not clearly defined. Nevertheless, forest buffalos, mandrills, and duikers were positive for ONNV in a serosurvey in the Congo basin [86]. Anopheles funestus and more rarely Anopheles gambiae are the main vectors [38,87,88,89]. Experimentally, ONNV can infect Aedes aegypti and disseminate to their salivary glands [90], but Aedes mosquitoes have not yet been demonstrated to be carriers in the wild. More likely, as for CHIKV, it switches to an urban cycle where humans are the amplifying host during bigger outbreaks.
3.3. Mayaro Virus
MAYV is circulating in an enzootic cycle between non-human primates [58,91,92,93,94] (or more rarely, small mammals [92] or birds [95]) and forest mosquitoes including Haemagogus sp. [49,91], Mansonia sp. [96], and Psophora sp. [5,6]. Nonetheless, two studies found pools of Aedes aegypti positive for MAYV [6,97], and experimental work confirms that they might be efficient vectors for the disease, as well as Aedes albopictus [98,99,100,101,102]. This raises the possibility of MAYV circulating in an urban setting. Furthermore, in an experimental setting, four Anopheles species (two North American species, one African, and one Southeast Asian) were able to get infected and to transmit MAYV, adding other potent MAYV vectors distributed worldwide to the list [101].
3.4. Ross River Virus
While twenty-one vertebrate hosts have been described for RRV [103], marsupials are considered to be the most important reservoir [104,105,106], even though proof is scarce [107], and some locations such as the islands of Samoa have circulation of RRV without the presence of marsupials [108]. Horses or cattle also play a role [105,109], and humans are the main host during outbreaks [106]. Different species of mosquitoes seem to play a role in the RRV cycle. Aedes vigilax are the most common ones in coastal and subcoastal areas and Culex annulirostris in both rural and urban settings, but Aedes notoscriptus, Aedes funereus, Aedes camptorhynchus, and Ochlerotatus camptorhynchus are also incriminated [69,70,110]. Experimentally, Aedes aegypti and albopictus are efficient vectors [111,112,113,114], but it has never been reported to happen in the wild.
4. Clinical Description
Contrary to what has been reported for most flaviviruses (for which asymptomatic cases can reach up to 94% [115,116]), most alphavirus infections are symptomatic with rates ranging from 72–97% for CHIKV [30,117,118,119,120] (only one study reporting an unusually low symptomatic infection rate of 18% [121]), 64–86% for ONN [42,122,123,124], 64–80% for MAYV [48,56], and 25–76% for RRV [73,125,126,127]. Rheumatic disease is the main clinical manifestation compared to other arboviral infections that are responsible for a flu-like syndrome. They all follow roughly the same timeline (Figure 1) and share the same major symptoms (Table 2). The severity of these infections, however, is difficult to compare between viruses because of considerable variability in absolute numbers and methods of clinical study (Figure 2).
4.1. Acute Phase
Following a 2.5-day incubation period (range of 2–12 days) [7,162], the acute phase of CHIKV infection is characterized by a brutal onset of symptoms typically associated with fever, very severe polyarthralgia (“frightening in its severity” as first described by Robinson [7]) with possible synovitis, and a delayed rash that is often pruriginous while rarely bullous [128,163,164]. Less well-known, but commonly associated manifestations include headaches, gastrointestinal symptoms, and more rarely conjunctival hyperemia or lymphadenopathy. While in the earliest descriptions of the disease the hemorrhagic, severe or lethal cases were questioned because of co-circulation with dengue fever [19,129,165,166], it is now clearly established that CHIKV infection can carry potentially lethal neurologic and cardiologic involvement [150,152,153] or be directly or indirectly linked to death, particularly in older patients with numerous comorbidities [128,150,156,167] or in neonates [156,157]. Overall, the global mortality rate is estimated at 0.01–0.1% [32,81,119,156].
The ONNV fever acute phase follows an eight-day or more incubation period [122]. It is characterized by the triad of fever, polyarthralgia, and lymphadenopathy. This last sign is more specific to ONNV infection and is mostly located in the cervical region. Skin rash is associated a few days later and is often itchy. Other reported complications include headaches, gastrointestinal symptoms, and eye involvement [44,122,141]. Bleeding gums and epistaxis have been reported for one patient each [141]. To our knowledge, no mortality linked to ONNV infection has been described.
After less than a week of incubation [47], MAYV infection causes brutal fever associated with arthromyalgia (sometimes with swollen joints). Headaches, retro-orbital pain, and gastrointestinal symptoms are frequent [47,49,50,51,56,142,143,144,145]. This acute phase usually lasts two to five days [49]. Three independent studies reported benign hemorrhagic signs in a total of seven patients (bleeding gums, epistaxis, petechiae) [56,60,142]. Only one patient with heavy comorbidities was reported to have died following MAYV infection, without certainty about the cause of death [60].
From traveler data, the incubation time of RRV infection is estimated to be 7–9 days [168] (ranging between three and 21 days [75,169]). Fever polyarthralgia and rash are, as is the case for the other rheumatic alphaviruses, typical, occurring during the acute phase [125,146,147,148,149]. If only nausea is reported in the main cohorts or retrospective studies, gastrointestinal symptoms are often mentioned in case reports [72,170]. Severe forms of infection include glomerulonephritis [158] and encephalitis [159,160,161], but to our knowledge, no lethality has been reported.
4.2. Chronic Phase
With over 40 clinical studies to date, the chronic joint pain (i.e., persisting after 12 weeks of onset of symptoms) is very well described and represents the major burden of CHIKV infection because it can be responsible for very heavy and long term incapacity [130]. A recent meta-analysis estimated that 43% of patients after three months and 21% after one year still experience symptoms linked to CHIKV. This rate seems to depend on which CHIKV strain is involved [171]. In a recent prospective cohort of La Reunion Island patients [172], chronic joint pain concerned up to 83% of patients at 32 months and was accompanied by asthenia and depression [173]. As the virus has never been isolated from chronic swollen joints, it is thought that CHIKV acute infection might trigger host autoimmunity [172,174,175]. However, it is important to differentiate chronic inflammatory rheumatism causing erosive arthritis [131] and for which the differential diagnosis is rheumatoid arthritis, from musculoskeletal disorder. Indeed, whereas the latter is only treated with pain killers possibly associated with steroids, the former requires a heavier treatment including methotrexate [176].
At the opposite end of the spectrum, accounts of ONNV chronic manifestations are scarce. While Shore et al. mentioned joint pain associated with residual weakness and depression in some patients in 1965 [122], other studies either report “no recurrent fever case” [141] or do not mention chronicity [44].
For MAYV, recurrent arthralgia has been reported in one patient [177], and some case reports have mentioned arthralgia lasting over 5–12 months after MAYV infection [178,179,180,181]. In 2013, one Peruvian prospective study of 13 patients confirmed these data and evaluated chronic arthralgia and headache to be present in 57% and 31% of patients 12 months after infection [143].
As for CHIKV, there is great heterogeneity between studies concerning chronic joint pain after RRV infection. Two studies reported them in 52.5% of patients at one year and 57% of patients at three years [146,147]. Two other studies reported progressive resolution of symptoms in 3–6 months [149] or a prevalence of chronic arthralgia in only 2% of patients with no other conditions than RRV infection [148]. This last study, apart from insisting on the difficulty of differentiating post-infectious chronic arthralgia from differential diagnosis, also implied a higher prevalence of chronic joint pain in the elderly, that also present with more comorbidities (even though this was not discussed in the paper). Although there is no human data available, in vitro and in vivo data suggest that post-RRV infection arthritis may be erosive [182,183].
5. Laboratory Features
5.1. Standard Blood Test
For CHIKV, standard biological tests usually show lymphopenia, more rarely associated with a moderate thrombocytopenia. Hypocalcemia is detected in more than half of the cases, and a mild rhabdomyolysis with moderately elevated creatinine kinase and transaminases (ASAT > ALAT) might be observed [128,132,133,134]. Very few data are available for the other three viruses, but leucopenia and thrombopenia have also been described for MAYV.
5.2. Positive Diagnosis
Viremia usually rises a few days before onset of symptoms. RT-PCR or virus isolation permit direct diagnosis; however, most of the time, RT-PCR can no longer detect virus seven days after onset of symptoms for CHIKV [32,184] (even though one patient had a positive RT-PCR 17 days after [185]) and for MAYV [186], and virus isolation is positive for an even shorter time [187]. This diagnostic tool is particularly useful because test specificity is very good between, and within, viral families, as specific assays exist for each virus [186,188,189,190].
Indirect diagnosis is achieved by serological tests to detect IgM and IgG. The antibodies arise later than viremia, but are long lasting in comparison. Indeed, as it has been shown for CHIKV, IgM can arise as soon as two days after onset of symptoms and is usually positive after a week [184,191]. IgM levels usually wane after three months [191], but in some cases can persist more than six months [128,192]. IgG usually appears after 7–14 days of the onset of illness and is long lasting [184,191]. Whatever the commercial or in-house serological test used (most often by enzymatic immune assay or hemagglutination inhibition), two samples per patient, taken at least 10 days apart, are needed to show the appearance of IgM and/or IgG or disappearance of IgM.
The main pitfall of serological methods is the cross-reactivity among alphaviruses that complicates identifying which of the arthritogenic alphaviruses is involved, especially in regions where they co-circulate. For this reason, the plaque-reduction neutralizing test (PRNT) remains a gold standard for diagnostics [193,194].
6. Treatment
6.1. Prevention
Because an efficient curative treatment does not exist, prevention measures are crucial to avoiding or limiting epidemics caused by these arboviruses. These include general measures to avoid mosquito bites and vaccination.
6.1.1. Public Health Measures: Surveillance and Vector Control
Public health response measures are essential to prevent and control any alphavirus outbreak. During disease-free periods, ongoing mosquito surveillance (e.g., population densities, distribution) has shown its effectiveness for predicting RRV epidemics in Australia [195]. Early detection of outbreaks is also favored by notification of cases, something that is mandatory for RRV in Australia and CHIKV in many other countries, leading to the early detection and increased surveillance of outbreaks [71,196,197,198,199]. As soon as detection occurs, intervention in mosquito habitats, using a combination of larvicides, adulticides, and removal of breeding sites, may be the best strategy [198,200,201,202]. Geovisualization tools might also help locate the source of infection to better target it [203]. Public outreach to educate individuals on how to avoid mosquito bites (e.g., protective clothing, mosquito repellents, and impregnated bed nets) is also common, but its effectiveness is still not clearly demonstrated [200].
6.1.2. Vaccination
Because CHIKV infection produces a life-lasting protection against a second infection and due to the limited antigenic variability of the virus, one might think that a CHIKV vaccine should be relatively easy to produce, or at least easier so than a dengue virus vaccine [204]. Nevertheless, there are still no licensed CHIKV vaccines available, although many candidates have been tested including live-attenuated vaccines [205,206], recombinant virus vaccines (measles virus [207,208,209], vesicular stomatitis virus [210,211]), inactivated vaccines [212,213], virus-like particles (VLPs) [214,215,216], DNA- [217,218] or mRNA-based vaccines [219], and subunit formulations of CHIKV [220].
Two candidates are currently in Phase II clinical trials. The first one is a recombinant measles virus encoding the CHIKV structural proteins. The first results of the Phase II trial are very encouraging with all vaccines fully immunized after two injections (regardless of the individual’s immunological status against measles virus) and excellent safety and tolerability [209]. The second candidate is a VLP vaccine containing CHIKV structural proteins that is immunogenic and protective against a challenge infection in mice and rhesus macaques [214]. A Phase I clinical trial confirmed immunogenicity in humans after two injections and the absence of serious adverse events [221,222]; a Phase II trial is currently underway.
While it still needs to be unequivocally demonstrated, a number of studies suggest that protection against one strain of CHIKV protects against all others [223,224,225,226]. Interestingly, Partidos et al. showed that passive monoclonal antibodies after immunization of mice with a CHIKV vaccine protect against ONNV infection (the closest related alphavirus) in AG129 mice [227]. Because there are no vaccine candidates for ONN, a broad-spectrum CHIKV vaccine is of particular interest; that should also be evaluated for MAYV and RRV.
Three vaccine candidates have been tested for MAYV. The first one was a formalin-inactivated vaccine with moderate efficiency in mice [228]. More recently, a live attenuated vaccine and a DNA vaccine showed good immunogenicity and protection after a lethal challenge in mice [229,230].
Since RRV has been a public health issue for some time now in Australia, vaccine research there has led to several candidates in preclinical studies [231,232,233,234], and formalin-inactivated vaccines have successfully passed Phase I, II, and III clinical trials [235,236]. However, this vaccine is not commercialized, and no RRV vaccine is currently available, highlighting the importance of public/private partnerships to invest in vaccine licensure [237].
6.2. Symptomatic and Curative Treatments
Symptomatic treatment with antalgics, such as paracetamol, and steroidal or non-steroidal anti-inflammatory drugs remains the main driver of action available [148,238,239]. As discussed above, in case of chronic inflammatory rheumatism, methotrexate treatment might be necessary [176].
Several studies have searched for efficient antiviral molecules that have a broad-spectrum activity inhibiting all arthritogenic alphaviruses [240,241,242,243,244,245,246]; however, despite a long list of antivirals efficient in vitro or in vivo, no treatment is currently available [247]. Indeed, all clinical trials conducted until now have either failed, such as for chloroquine [248,249], or have been inconclusive because of small test groups, such as for ribavirin [250]. Pentosan polysulfate has shown efficiency against cartilage damage in mice both with CHIKV and RRV, and a Phase II trial is now ongoing [251].
7. Discussion
With two worldwide epidemics causing close to 10 million cases all together during the 21st Century, chikungunya virus is undoubtedly a re-emerged disease threatening both tropical and temperate regions [2,3,4]. While it was a neglected tropical disease until the early 2000s, it has since gathered considerable interest as the number of publications through the years illustrates (Figure 2). In contrast, ONN, MAYV, and RRV are still understudied, even though specialists consider them as a Sword of Damocles. Indeed, some reviews raise the question of a possible emergence in the near future [186,254,255,256,257], especially for ONNV, which is known to have caused a large African outbreak with a hundred thousand cases in 1959–1962 [38].
One of the prerequisites to imagining a worldwide outbreak of any of these alphaviruses is a wide distribution of their mosquito vector. Indeed, no circulation of the disease would occur in a region free from competent mosquitoes. Interestingly, none of these four alphaviruses shares the same vector (Table 1), and they are currently more geographically restrained than the CHIKV vector: Anopheles sp. for ONNV in Africa and the Middle East, Haemagogus sp., Mansonia sp., and Psophora sp. for MAYV in America. and Aedes vigilax and Culex annulirostris for RRV in Oceania and South-East Asia [258]. However, globalization, travel, migration, trade, or climatic change might be leading forces of the redistribution of these mosquitoes. Indeed, climate and weather patterns are important factors in the occurrence of epidemics, which have become the focus of many modeling studies. For example, natural climatic and weather trends influenced RRV’s pattern of infection, especially hydrological features [125,259] and temperatures [260,261,262]; and a modeling study predicts that global warming might lead to the presence of MAYV across all of the Brazilian territory [263].
Furthermore, Aedes aegypti and/or albopictus have been proven to be competent vectors in experimental settings for ONNV, MAYV, and RRV [6,90,97,98,99,100,102,111,112,113,114]. While this does not mean it is currently happening in the wild, these observations are a warning of what could occur in the future, particular if vector populations expand and overlap and further adaptation to new vectors occurs. Public health services should keep this on their radar, especially because alphaviruses are single-stranded RNA viruses that are known to evolve rapidly [264]. One point mutation or one recombination event might favor infection of Aedes aegypti and/or albopictus compared to the original vector and trigger a worldwide epidemic, as has happened for CHIKV (during the La Reunion epidemic with the A226V mutation [83,84,85] and during the American outbreak with a duplication of the 3’UTR [265]). Because these vectors are widely distributed anthropophilic mosquitoes, the risk of initiating an urban cycle could be high, and further enabled by high viremia in humans.
On the other hand, the real risk and the severity of an outbreak are difficult to anticipate because little is known about ONNV, MAYV, and RRV. While a surveillance system has been well established in Australia for RRV (as it is a main health problem in a developed country), under-surveillance of ONNV and MAYV is an issue, as well as the low number of clinical studies. Thus, many open questions remain concerning possible under-the-radar outbreaks, the true incidence of the diseases, or their clinical manifestations: What is the real risk of chronicity? Can severe cases occur and which types? Can these infections be directly or indirectly lethal? Since CHIKV is more of a global concern, fundamental knowledge on alphaviruses in general is expanding, and many of these publications also tested their hypothesis on the related ONNV, MAYV, or RRV. As an example, recent findings on the still obscure entry pathway of alphaviruses identified Mxra8 as an entry mediator, not only for CHIKV, but also for ONNV, MAYV, and RRV [266].
Another potential pitfall, if an epidemic were to happen, is the speed of identifying which virus is responsible. Indeed, despite some virus-specific trends such as lymphadenopathy for ONNV, arthritogenic alphaviruses share very similar clinical manifestations that are also common to other arboviruses or other infectious diseases. Because they co-circulate in many geographical areas, an etiological diagnosis without biological testing seems impossible. Moreover, many cases of arbovirus co-infections have been reported, adding a layer of complexity to this problem [19,129,165,166,267,268,269]. As a further complication, these viruses currently circulate in remote rural areas with low access to health care facilities, including laboratories. Fortunately, many tests are now better adapted to the field [270,271,272], particularly for indirect diagnosis, but also with sequencing technology, such as MinION [273]. Regardless, cross-reactivity remains a main limitation in biological diagnostics, especially for immunological tests [274,275,276]. Hence, the closer alphaviruses are phylogenetically, the more cross-reactivity exists [194]. In response, considerable effort is made on developing technologies to avoid cross-reactivity both in direct [271,277] and indirect diagnosis [194,278].
Despite the problems stemming from cross-reactivity, it could be a major help in vaccine design, allowing broad-spectrum protection across all arthritogenic alphaviruses. Indeed, broad neutralizing antibodies against CHIKV can neutralize MAYV and ONNV by inhibiting entry and egress [227,279]. While no licensed vaccine exists for any of these viruses, several candidates have gone or are currently going through clinical trials for CHIKV and RRV, and it is reasonable to expect a CHIKV vaccine in the years to come. The immunity triggered by this vaccine would then need to be evaluated on other alphaviruses to validate its potent broad-spectrum activity. Strengthening the collective commitment of national and international actors and public/private partnerships will be necessary to develop and license vaccines [237] and to avoid what had happened for RRV: an efficient and safe vaccine that went through Phase I, II, and III clinical trials [235,236], yet is still not licensed.
In conclusion, enriched by lessons learned from recent CHIKV outbreaks, it is undeniable that ONN, MAYV, or RRV represent emerging threats favored by climatic changes, globalization, travel, migration, and trade. Surveillance is key for detecting any unusual activity of these diseases, so that preventive measures can be taken as soon as possible to tackle a starting epidemic. Hopefully, the availability of a CHIKV vaccine might enable a broad-spectrum activity on all arthritogenic viruses that would be key for future prevention.
Author Contributions
Conceptualization, L.I.L. and M.V.; writing, original draft preparation, L.I.L.; writing, review and editing L.I.L. and M.V; supervision, M.V.
Acknowledgments
The authors want to thank Djoshkun Shengjuler for helpful discussions. This work was funded by a PhD fellowship from the Defense Innovation Agency (AID) (L.I.L.) and by the DARPA PREEMPT program managed by Jim Gimlett and administered through DARPA Cooperative Agreement HR001118S0017-PREEMPT-BAA-PA-008 (the content of the information does not necessarily reflect the position or the policy of the U.S. government, and no official endorsement should be inferred).
Conflicts of Interest
The authors declare no conflict of interest.
References
- Suhrbier, A.; Jaffar-Bandjee, M.-C.; Gasque, P. Arthritogenic alphaviruses—An overview. Nat. Rev. Rheumatol. 2012, 8, 420–429. [Google Scholar] [CrossRef] [PubMed]
- Chretien, J.-P.; Anyamba, A.; Bedno, S.A.; Breiman, R.F.; Sang, R.; Sergon, K.; Powers, A.M.; Onyango, C.O.; Small, J.; Tucker, C.J.; et al. Drought-associated chikungunya emergence along coastal east africa. Am. J. Trop. Med. Hyg. 2007, 76, 405–407. [Google Scholar] [CrossRef]
- Weaver, S.C.; Osorio, J.E.; Livengood, J.A.; Chen, R.; Stinchcomb, D.T. Chikungunya virus and prospects for a vaccine. Expert Rev. Vaccines 2012, 11, 1087–1101. [Google Scholar] [CrossRef]
- Vignuzzi, M.; Higgs, S. The Bridges and Blockades to Evolutionary Convergence on the Road to Predicting Chikungunya Virus Evolution. Annu. Rev. Virol. 2017, 4, 181–200. [Google Scholar] [CrossRef]
- Groot, H.; Morales, A.; Vidales, H. VIRUS ISOLATIONS FROM FOREST MOSQUITOES IN SAN VICENTE. Am. J. Trop. Med. Hyg. 1961, 6, 397–402. [Google Scholar] [CrossRef]
- Serra, O.P.; Cardoso, B.F.; Ribeiro, A.L.M.; dos Santos, F.A.L.; Slhessarenko, R.D. Mayaro virus and dengue virus 1 and 4 natural infection in culicids from Cuiabá, state of Mato Grosso, Brazil. Mem. Inst. Oswaldo Cruz 2016, 111, 20–29. [Google Scholar] [CrossRef]
- Robinson, M.C. An epidemic of virus disease in southern province, tanganyika territory, in 1952-1953. Trans. R. Soc. Trop. Med. Hyg. 1955, 49, 28–32. [Google Scholar] [CrossRef]
- Powers, A.M.; Tesh, R.B.; Brault, A.C.; Weaver, S.C. Re-emergence of chikungunya and O’nyong’nyong viruses: Evidence for distinct geographical lineages and distant evolutionary relationships. J. Gen. Virol. 2000, 81, 471–479. [Google Scholar] [CrossRef]
- Volk, S.M.; Chen, R.; Tsetsarkin, K.A.; Adams, A.P.; Garcia, T.I.; Sall, A.A.; Nasar, F.; Schuh, A.J.; Holmes, E.C.; Higgs, S.; et al. Genome-Scale Phylogenetic Analyses of Chikungunya Virus Reveal Independent Emergences of Recent Epidemics and Various Evolutionary Rates. J. Virol. 2010, 84, 6497–6504. [Google Scholar] [CrossRef] [PubMed]
- Rodger, L.M. An outbreak of suspected Chikungunya fever in Northern Rhodesia. S. Afr. Med. J. 1961, 35, 126–128. [Google Scholar]
- McIntosh, B.M.; Harwin, R.M.; Paterson, H.E.; Westwater, M.L. An Epidemic of Chikungunya in South-Eastern Southern Rhodesia. Cent. Afr. J. Med. 1963, 9, 351–359. [Google Scholar]
- Tomori, O.; Fagbami, A.; Fabiyi, A. The 1974 epidemic of Chikungunya fever in children in Ibadan. Trop. Geogr. Med. 1975, 27, 413–417. [Google Scholar]
- Filipe, A.F.; Pinto, M.R. Arbovirus studies in Luanda, Angola. 2. Virological and serological studies during an outbreak of dengue-like disease caused by the Chikungunya virus. Bull. World Health Organ. 1973, 49, 37–40. [Google Scholar]
- Fourie, E.D.; Morrison, J.G. Rheumatoid arthritic syndrome after chikungunya fever. S. Afr. Med. J. 1979, 56, 130–132. [Google Scholar]
- Muyembe-Tamfum, J.J.; Peyrefitte, C.N.; Yogolelo, R.; Mathina Basisya, E.; Koyange, D.; Pukuta, E.; Mashako, M.; Tolou, H.; Durand, J.P. [Epidemic of Chikungunya virus in 1999 and 200 in the Democratic Republic of the Congo]. Med. Trop. Rev. Corps Sante Colon. 2003, 63, 637–638. [Google Scholar]
- Pastorino, B.; Muyembe-Tamfum, J.J.; Bessaud, M.; Tock, F.; Tolou, H.; Durand, J.P.; Peyrefitte, C.N. Epidemic resurgence of Chikungunya virus in democratic Republic of the Congo: Identification of a new central African strain. J. Med. Virol. 2004, 74, 277–282. [Google Scholar] [CrossRef]
- Saluzzo, J.F.; Cornet, M.; Digoutte, J.P. [Outbreak of a Chikungunya virus epidemic in western Senegal in 1982]. Dakar Med. 1983, 28, 497–500. [Google Scholar]
- Diallo, M.; Thonnon, J.; Traore-Lamizana, M.; Fontenille, D. Vectors of Chikungunya virus in Senegal: Current data and transmission cycles. Am. J. Trop. Med. Hyg. 1999, 60, 281–286. [Google Scholar] [CrossRef]
- Sarkar, J.K.; Chatterjee, S.N.; Chakravarti, S.K.; Mitra, A.C. Chikungunya Virus Infection with Haemorrhagic Manifestations. Indian J. Med. Res. 1965, 53, 921–925. [Google Scholar]
- Shah, K.V.; Gibbs, C.J.; Banerjee, G. Virological investigation of the epidemic of haemorrhagic fever in calcutta: Isolation of three strains of chikungunya virus. Indian J. Med. Res. 1964, 52, 676–683. [Google Scholar]
- Munasinghe, D.R.; Amarasekera, P.J.; Fernando, C.F.O. An epidemic of dengue-like fever in Ceylon (chikungunya)—A clinical and haematological study. Ceylon Med. J. 1966, 11, 129–142. [Google Scholar]
- Chaudhuri, R.N.; Chatterjea, J.B.; Saha, T.K.; Chaudhuri, A.D. clinical and haematological observations on a recent outbreak of dengue-like fever in calcutta with or without haemorrhagic manifestations. J. Indian Med. Assoc. 1964, 43, 579–584. [Google Scholar]
- Vu-Qui-Dai; Kim-Thoa, N.T. [Hemorrhagic fever in Vietnam in 1964-1965. Serologic study with a brief clinica and epidemiologic note]. Bull. Soc. Pathol. Exot. Fil. 1967, 60, 21–33. [Google Scholar]
- Thaikruea, L.; Charearnsook, O.; Reanphumkarnkit, S.; Dissomboon, P.; Phonjan, R.; Ratchbud, S.; Kounsang, Y.; Buranapiyawong, D. Chikungunya in Thailand: A re-emerging disease? Southeast Asian J. Trop. Med. Public Health 1997, 28, 359–364. [Google Scholar]
- Lam, S.; Chua, K.; Hooi, P.; Rahimah, M.; Kumari, S.; Tharmaratnam, M.; Chuah, S.; Smith, D.; Sampson, I. Chikungunya infection—An emerging disease in malaysia. Southeast Asian J. Trop. Med. Public Health 2001, 32, 5. [Google Scholar]
- Porter, K.R.; Tan, R.; Istary, Y.; Suharyono, W.; Sutaryo; Widjaja, S.; Ma’Roef, C.; Listiyaningsih, E.; Kosasih, H.; Hueston, L.; et al. A serological study of Chikungunya virus transmission in Yogyakarta, Indonesia: Evidence for the first outbreak since 1982. Southeast Asian J. Trop. Med. Public Health 2004, 35, 408–415. [Google Scholar]
- Laras, K.; Sukri, N.C.; Larasati, R.P.; Bangs, M.J.; Kosim, R.; Djauzi; Wandra, T.; Master, J.; Kosasih, H.; Hartati, S.; et al. Tracking the re-emergence of epidemic chikungunya virus in Indonesia. Trans. R. Soc. Trop. Med. Hyg. 2005, 99, 128–141. [Google Scholar] [CrossRef]
- Simon, F.; Tolou, H.; Jeandel, P. Chikungunya, l’épidémie que l’on n’attendait pas. Rev. Médecine Interne 2006, 27, 437–441. [Google Scholar] [CrossRef]
- Pialoux, G.; Gaüzère, B.-A.; Strobel, M. Infection à virus Chikungunya: Revue générale par temps d’épidémie. Médecine Mal. Infect. 2006, 36, 253–263. [Google Scholar] [CrossRef]
- Staples, J.E.; Fischer, M. Chikungunya Virus in the Americas—What a Vectorborne Pathogen Can Do. Available online: https://www.nejm.org/doi/10.1056/NEJMp1407698?url_ver=Z39.88-2003&rfr_id=ori%3Arid%3Acrossref.org&rfr_dat=cr_pub%3Dwww.ncbi.nlm.nih.gov (accessed on 14 March 2019).
- Cassadou, S.; Boucau, S.; Petit-Sinturel, M.; Huc, P.; Leparc-Goffart, I.; Ledrans, M. Emergence of chikungunya fever on the French side of Saint Martin island, October to December 2013. Eurosurveillance 2014, 19, 20752. [Google Scholar] [CrossRef]
- Rezza, G.; Nicoletti, L.; Angelini, R.; Romi, R.; Finarelli, A.C.; Panning, M.; Cordioli, P.; Fortuna, C.; Boros, S.; Magurano, F.; et al. Infection with chikungunya virus in Italy: An outbreak in a temperate region. Lancet Lond. Engl. 2007, 370, 1840–1846. [Google Scholar] [CrossRef]
- Manica, M.; Guzzetta, G.; Poletti, P.; Filipponi, F.; Solimini, A.; Caputo, B.; Della Torre, A.; Rosà, R.; Merler, S. Transmission dynamics of the ongoing chikungunya outbreak in Central Italy: From coastal areas to the metropolitan city of Rome, summer 2017. Eurosurveillance 2017, 22, 17-00685. [Google Scholar] [CrossRef]
- Venturi, G.; Di Luca, M.; Fortuna, C.; Remoli, M.E.; Riccardo, F.; Severini, F.; Toma, L.; Del Manso, M.; Benedetti, E.; Caporali, M.G.; et al. Detection of a chikungunya outbreak in Central Italy, August to September 2017. Eurosurveillance 2017, 22. [Google Scholar] [CrossRef] [PubMed]
- Angelini, R.; Finarelli, A.C.; Angelini, P.; Po, C.; Petropulacos, K.; Silvi, G.; Macini, P.; Fortuna, C.; Venturi, G.; Magurano, F.; et al. Chikungunya in north-eastern Italy: A summing up of the outbreak. Eurosurveillance 2007, 12, E071122.2. [Google Scholar] [CrossRef]
- Delisle, E.; Rousseau, C.; Broche, B.; Leparc-Goffart, I.; L’Ambert, G.; Cochet, A.; Prat, C.; Foulongne, V.; Ferre, J.B.; Catelinois, O.; et al. Chikungunya outbreak in Montpellier, France, September to October 2014. Eurosurveillance 2015, 20. [Google Scholar] [CrossRef]
- Calba, C.; Guerbois-Galla, M.; Franke, F.; Jeannin, C.; Auzet-Caillaud, M.; Grard, G.; Pigaglio, L.; Decoppet, A.; Weicherding, J.; Savaill, M.-C.; et al. Preliminary report of an autochthonous chikungunya outbreak in France, July to September 2017. Eurosurveillance 2017, 22. [Google Scholar] [CrossRef]
- Haddow, A.J.; Davies, C.W.; Walker, A.J. O’nyong’nyong fever: An epidemic virus disease in East Africa 1. Introduction. Trans. R. Soc. Trop. Med. Hyg. 1960, 54, 517–522. [Google Scholar] [CrossRef]
- Williams, M.C.; Woodall, J.P. O’nyong’nyong fever: An epidemic virus disease in East Africa. II. Isolation and some properties of the virus. Trans. R. Soc. Trop. Med. Hyg. 1961, 55, 135–141. [Google Scholar] [CrossRef]
- Lhuillier, M.; Cunin, P.; Mazzariol, M.J.; Monteny, N.; Cordellier, R.; Bouchite, B. [A rural epidemic of Igbo Ora virus (with interhuman transmission) in the Ivory Coast 1984-1985]. Bull. Soc. Pathol. Exot. Fil. 1988, 81, 386–395. [Google Scholar]
- Lanciotti, R.S.; Ludwig, M.L.; Rwaguma, E.B.; Lutwama, J.J.; Kram, T.M.; Karabatsos, N.; Cropp, B.C.; Miller, B.R. Emergence of epidemic O’nyong’nyong fever in Uganda after a 35-year absence: Genetic characterization of the virus. Virology 1998, 252, 258–268. [Google Scholar] [CrossRef]
- Sanders, E.J.; Rwaguma, E.B.; Kawamata, J.; Kiwanuka, N.; Lutwama, J.J.; Ssengooba, F.P.; Lamunu, M.; Najjemba, R.; Were, W.A.; Bagambisa, G.; et al. O’nyong’nyong fever in south-central Uganda, 1996-1997: Description of the epidemic and results of a household-based seroprevalence survey. J. Infect. Dis. 1999, 180, 1436–1443. [Google Scholar] [CrossRef]
- Rwaguma, E.B.; Lutwama, J.J.; Sempala, S.D.; Kiwanuka, N.; Kamugisha, J.; Okware, S.; Bagambisa, G.; Lanciotti, R.; Roehrig, J.T.; Gubler, D.J. Emergence of epidemic O’nyong’nyong fever in southwestern Uganda, after an absence of 35 years. Emerg. Infect. Dis. 1997, 3, 77. [Google Scholar] [CrossRef]
- Posey, D.L.; O’rourke, T.; Roehrig, J.T.; Lanciotti, R.S.; Weinberg, M.; Maloney, S. O’nyong’nyong fever in West Africa. Am. J. Trop. Med. Hyg. 2005, 73, 32. [Google Scholar] [CrossRef]
- Anderson, C.R.; Downs, W.G.; Wattley, G.H.; Ahin, N.W.; Reese, A.A. Mayaro virus: A new human disease agent. II. Isolation from blood of patients in Trinidad, B.W.I. Am. J. Trop. Med. Hyg. 1957, 6, 1012–1016. [Google Scholar] [CrossRef]
- Schmidt, J.R.; Gajdusek, D.C.; Schaffer, M.; Gorrie, R.H. Epidemic jungle fever among Okinawan colonists in the Bolivian rain forest. II. Isolation and characterization of Uruma virus, a newly recognized human pathogen. Am. J. Trop. Med. Hyg. 1959, 8, 479–487. [Google Scholar] [CrossRef]
- Causey, O.R.; Maroja, O.M. Mayaro Virus: A New Human Disease Agent. Am. J. Trop. Med. Hyg. 1957, 6, 1017–1023. [Google Scholar] [CrossRef]
- LeDuc, J.W.; Pinheiro, F.P.; Travassos da Rosa, A.P. An outbreak of Mayaro virus disease in Belterra, Brazil. II. Epidemiology. Am. J. Trop. Med. Hyg. 1981, 30, 682–688. [Google Scholar] [CrossRef]
- Pinheiro, F.P.; Freitas, R.B.; Travassos da Rosa, J.F.; Gabbay, Y.B.; Mello, W.A.; LeDuc, J.W. An outbreak of Mayaro virus disease in Belterra, Brazil. I. Clinical and virological findings. Am. J. Trop. Med. Hyg. 1981, 30, 674–681. [Google Scholar] [CrossRef]
- Azevedo, R.S.S.; Silva, E.V.P.; Carvalho, V.L.; Rodrigues, S.G.; Nunes-Neto, J.P.; Monteiro, H.; Peixoto, V.S.; Chiang, J.O.; Nunes, M.R.T.; Vasconcelos, P.F.C. Mayaro fever virus, Brazilian Amazon. Emerg. Infect. Dis. 2009, 15, 1830–1832. [Google Scholar] [CrossRef]
- Brunini, S.; França, D.D.S.; Silva, J.B.; Silva, L.N.; Silva, F.P.A.; Spadoni, M.; Rezza, G. High Frequency of Mayaro Virus IgM among Febrile Patients, Central Brazil. Emerg. Infect. Dis. 2017, 23, 1025–1026. [Google Scholar] [CrossRef]
- Schaeffer, M.; Gajdusek, D.C.; Lema, A.B.; Eichenwald, H. Epidemic jungle fevers among Okinawan colonists in the Bolivian rain forest. I. Epidemiology. Am. J. Trop. Med. Hyg. 1959, 8, 372–396. [Google Scholar] [CrossRef]
- Izurieta, R.O.; Macaluso, M.; Watts, D.M.; Tesh, R.B.; Guerra, B.; Cruz, L.M.; Galwankar, S.; Vermund, S.H. Hunting in the Rainforest and Mayaro Virus Infection: An emerging Alphavirus in Ecuador. J. Glob. Infect. Dis. 2011, 3, 317–323. [Google Scholar] [CrossRef]
- Auguste, A.J.; Liria, J.; Forrester, N.L.; Giambalvo, D.; Moncada, M.; Long, K.C.; Morón, D.; de Manzione, N.; Tesh, R.B.; Halsey, E.S.; et al. Evolutionary and Ecological Characterization of Mayaro Virus Strains Isolated during an Outbreak, Venezuela, 2010. Emerg. Infect. Dis. 2015, 21, 1742–1750. [Google Scholar] [CrossRef]
- Torres, J.R.; Russell, K.L.; Vasquez, C.; Barrera, R.; Tesh, R.B.; Salas, R.; Watts, D.M. Family cluster of Mayaro fever, Venezuela. Emerg. Infect. Dis. 2004, 10, 1304–1306. [Google Scholar] [CrossRef]
- Tesh, R.B.; Watts, D.M.; Russell, K.L.; Damodaran, C.; Calampa, C.; Cabezas, C.; Ramirez, G.; Vasquez, B.; Hayes, C.G.; Rossi, C.A.; et al. Mayaro Virus Disease: An Emerging Mosquito-Borne Zoonosis in Tropical South America. Clin. Infect. Dis. 1999, 28, 67–73. [Google Scholar] [CrossRef]
- Neumayr, A.; Gabriel, M.; Fritz, J.; Günther, S.; Hatz, C.; Schmidt-Chanasit, J.; Blum, J. Mayaro virus infection in traveler returning from Amazon Basin, northern Peru. Emerg. Infect. Dis. 2012, 18, 695–696. [Google Scholar] [CrossRef]
- Talarmin, A.; Chandler, L.J.; Kazanji, M.; de Thoisy, B.; Debon, P.; Lelarge, J.; Labeau, B.; Bourreau, E.; Vié, J.C.; Shope, R.E.; et al. Mayaro virus fever in French Guiana: Isolation, identification, and seroprevalence. Am. J. Trop. Med. Hyg. 1998, 59, 452–456. [Google Scholar] [CrossRef]
- Metselaar, D. Isolation of arboviruses of group A and group C in Surinam. Trop. Geogr. Med. 1966, 18, 137–142. [Google Scholar]
- Navarrete-Espinosa, J.; Gómez-Dantés, H. [Arbovirus causing hemorrhagic fever at IMSS]. Rev. Medica Inst. Mex. Seguro Soc. 2006, 44, 347–353. [Google Scholar]
- Lednicky, J.; De Rochars, V.M.B.; Elbadry, M.; Loeb, J.; Telisma, T.; Chavannes, S.; Anilis, G.; Cella, E.; Ciccozzi, M.; Okech, B.; et al. Mayaro Virus in Child with Acute Febrile Illness, Haiti, 2015. Emerg. Infect. Dis. 2016, 22, 2000–2002. [Google Scholar] [CrossRef]
- Weber, J. On a outbreak of Dengue fever. Aust. Med. J. 1886, 8, 291–293. [Google Scholar]
- Wolstenholme, J. Ross River virus disease—The first recorded outbreak? Aust. N. Z. J. Med. 1993, 23, 417–418. [Google Scholar] [CrossRef]
- Doherty, R.; Carley, J.G.; Mackerras, M.J.; Marks, E.N. Studies of arthropod-borne virus infections in Queensland. III. Isolation and characterization of virus strains from wild-caught mosquitoes in North Queensland. Aust. J. Exp. Biol. Med. Sci. 1963, 41, 17–39. [Google Scholar] [CrossRef]
- Doherty, R.L.; Gorman, B.M.; Whitehead, R.H.; Carley, J.G. Studies of epidemic polyarthritis: The significance of three group a arboviruses isolated from mosquitoes in queensland. Australas. Ann. Med. 1964, 13, 322–327. [Google Scholar] [CrossRef]
- Doherty, R.L.; Barrett, E.J.; Gorman, B.M.; Whitehead, R.H. Epidemic polyarthritis in Eastern Australia, 1959-1970. Med. J. Aust. 1971, 1, 5–8. [Google Scholar]
- Doherty, R.L.; Carley, J.G.; Best, J.C. Isolation of Ross River virus from man. Med. J. Aust. 1972, 1, 1083–1084. [Google Scholar]
- Tai, K.; Whelan, P.; Patel, M.; Currie, B. An outbreak of epidemic polyarthritis (Ross River virus disease) in the Northern Territory during the 1990-1991 wet season. Med. J. Aust. 1993, 158, 522–525. [Google Scholar]
- Ritchie, S.A.; Fanning, I.D.; Phillips, D.A.; Standfast, H.A.; Mcginn, D.; Kay, B.H. Ross River Virus in Mosquitoes (Diptera: Culicidae) During the 1994 Epidemic Around Brisbane, Australia. J. Med. Entomol. 1997, 34, 156–159. [Google Scholar] [CrossRef]
- Robertson, G.; Doggett, S.; Seeman, O.; Russell, R.C.; Clancy, J.; Haniotis, J. Ross River virus and its vectors in Sorell Municipal Area, south-eastern Tasmania, January to March 2002. Commun. Dis. Intell. 2004, 28, 261–266. [Google Scholar]
- Knope, K.; Muller, M.; Kurucz, N.; Doggett, S.; Feldman, R.; Johansen, C.; Hobby, M.; Bennett, S.; Lynch, S.; Sly, A.; et al. Arboviral diseases and malaria in Australia, 2013-14: Annual report of the National Arbovirus and Malaria Advisory Committee. Commun. Dis. Intell. 2016, 40, E400–E436. [Google Scholar]
- Klapsing, P.; MacLean, J.D.; Glaze, S.; McClean, K.L.; Drebot, M.A.; Lanciotti, R.S.; Campbell, G.L. Ross River Virus Disease Reemergence, Fiji, 2003–2004. Emerg. Infect. Dis. 2005, 11, 613–615. [Google Scholar] [CrossRef]
- Aaskov, J.G.; Mataika, J.U.; Lawrence, G.W.; Rabukawaqa, V.; Tucker, M.M.; Miles, J.A.R. An Epidemic of Ross River Virus Infection in Fiji, 1979. Am. J. Trop. Med. Hyg. 1981, 30, 1053–1059. [Google Scholar] [CrossRef]
- Tesh, R.B.; McLean, R.G.; Shroyer, D.A.; Calisher, C.H.; Rosen, L. Ross River virus (Togaviridae: Alphavirus) infection (epidemic polyarthritis) in American Samoa. Trans. R. Soc. Trop. Med. Hyg. 1981, 75, 426–431. [Google Scholar] [CrossRef]
- Rosen, L.; Gubler, D.J.; Bennett, P.H. EPIDEMIC POLYARTHRTTIS (ROSS RIVER) VIRUS INFECTION IN THE COOK ISLANDS. Am. J. Trop. Med. Hyg. 1981, 30, 1294–1302. [Google Scholar] [CrossRef] [PubMed]
- Halstead, S.B.; Udomsakdi, S. Vertebrate hosts of chikungunya virus. Bull. World Health Organ. 1966, 35, 89. [Google Scholar] [PubMed]
- Eastwood, G.; Sang, R.C.; Guerbois, M.; Taracha, E.L.N.; Weaver, S.C. Enzootic Circulation of Chikungunya Virus in East Africa: Serological Evidence in Non-human Kenyan Primates. Am. J. Trop. Med. Hyg. 2017, 97, 1399–1404. [Google Scholar] [CrossRef] [PubMed]
- Weinbren, M.; Haddow, A.; Williams, M. The occurrence of chikungunya virus in Uganda I. Isolation from mosquitoes. Trans. R. Soc. Trop. Med. Hyg. 1958, 52, 253–262. [Google Scholar] [CrossRef]
- Harrison, V.R.; Marshall, J.D.; Guilloud, N.B. The Presence of Antibody to Chikungunya and Other Serologically Related Viruses in the Sera of Sub-Human Primate Imports to the United States. J. Immunol. 1966, 98, 5. [Google Scholar]
- McIntosh, B.M. Antibody against Chikungunya virus in wild primates in Southern Africa. S. Afr. J. Med. Sci. 1970, 35, 65–74. [Google Scholar] [PubMed]
- Pialoux, G.; Gaüzère, B.-A.; Jauréguiberry, S.; Strobel, M. Chikungunya, an epidemic arbovirosis. Lancet Infect. Dis. 2007, 7, 319–327. [Google Scholar] [CrossRef]
- Lumsden, W.H. An epidemic of virus disease in Southern Province, Tanganyika territory, in 1952–1953 II. General description and epidemiology. Trans. R. Soc. Trop. Med. Hyg. 1955, 49, 33–57. [Google Scholar] [CrossRef]
- Schuffenecker, I.; Iteman, I.; Michault, A.; Murri, S.; Frangeul, L.; Vaney, M.-C.; Lavenir, R.; Pardigon, N.; Reynes, J.-M.; Pettinelli, F.; et al. Genome microevolution of chikungunya viruses causing the Indian Ocean outbreak. PLoS Med. 2006, 3, e263. [Google Scholar] [CrossRef]
- Vazeille, M.; Moutailler, S.; Coudrier, D.; Rousseaux, C.; Khun, H.; Huerre, M.; Thiria, J.; Dehecq, J.-S.; Fontenille, D.; Schuffenecker, I.; et al. Two Chikungunya isolates from the outbreak of La Reunion (Indian Ocean) exhibit different patterns of infection in the mosquito, Aedes albopictus. PLoS ONE 2007, 2, e1168. [Google Scholar] [CrossRef] [PubMed]
- Tsetsarkin, K.A.; Vanlandingham, D.L.; McGee, C.E.; Higgs, S. A single mutation in chikungunya virus affects vector specificity and epidemic potential. PLoS Pathog. 2007, 3, e201. [Google Scholar] [CrossRef] [PubMed]
- Kading, R.C.; Borland, E.M.; Cranfield, M.; Powers, A.M. Prevalence of antibodies to alphaviruses and flaviviruses in free-ranging game animals and nonhuman primates in the greater Congo basin. J. Wildl. Dis. 2013, 49, 587–599. [Google Scholar] [CrossRef]
- Corbet, P.S.; Williams, M.C.; Gillett, J.D. O’nyong’nyong fever: An epidemic virus disease in East Africa. IV. Vector studies at epidemic sites. Trans. R. Soc. Trop. Med. Hyg. 1961, 55, 463–480. [Google Scholar] [CrossRef]
- Johnson, B.K.; Gichogo, A.; Gitau, G.; Patel, N.; Ademba, G.; Kirui, R.; Highton, R.B.; Smith, D.H. Recovery of O’nyong’nyong virus from Anopheles funestus in Western Kenya. Trans. R. Soc. Trop. Med. Hyg. 1981, 75, 239–241. [Google Scholar] [CrossRef]
- Lutwama, J.J.; Kayondo, J.; Savage, H.M.; Burkot, T.R.; Miller, B.R. Epidemic O’nyong’nyong fever in southcentral Uganda, 1996-1997: Entomologic studies in Bbaale village, Rakai District. Am. J. Trop. Med. Hyg. 1999, 61, 158–162. [Google Scholar] [CrossRef]
- Vanlandingham, D.L.; Hong, C.; Klingler, K.; Tsetsarkin, K.; McElroy, K.L.; Powers, A.M.; Lehane, M.J.; Higgs, S. Differential infectivities of O’nyong’nyong and chikungunya virus isolates in Anopheles gambiae and Aedes aegypti mosquitoes. Am. J. Trop. Med. Hyg. 2005, 72, 616–621. [Google Scholar] [CrossRef]
- Hoch, A.L.; Peterson, N.E.; LeDuc, J.W.; Pinheiro, F.P. An outbreak of Mayaro virus disease in Belterra, Brazil. III. Entomological and ecological studies. Am. J. Trop. Med. Hyg. 1981, 30, 689–698. [Google Scholar] [CrossRef]
- Seymour, C.; Peralta, P.H.; Montgomery, G.G. Serologic evidence of natural togavirus infections in Panamanian sloths and other vertebrates. Am. J. Trop. Med. Hyg. 1983, 32, 854–861. [Google Scholar] [CrossRef] [PubMed]
- De Thoisy, B.; Vogel, I.; Reynes, J.M.; Pouliquen, J.F.; Carme, B.; Kazanji, M.; Vié, J.C. Health evaluation of translocated free-ranging primates in French Guiana. Am. J. Primatol. 2001, 54, 1–16. [Google Scholar] [CrossRef]
- De Thoisy, B.; Gardon, J.; Salas, R.A.; Morvan, J.; Kazanji, M. Mayaro virus in wild mammals, French Guiana. Emerg. Infect. Dis. 2003, 9, 1326–1329. [Google Scholar] [CrossRef] [PubMed]
- Calisher, C.H.; Gutiérrez, E.; Maness, K.S.; Lord, R.D. Isolation of Mayaro virus from a migrating bird captured in Louisiana in 1967. Bull. Pan Am. Health Organ. 1974, 8, 243–248. [Google Scholar] [PubMed]
- Aitken, T.H.; Downs, W.G.; Anderson, C.R.; Spence, L.; Casals, J. Mayaro virus isolated from a Trinidadian mosquito, Mansonia venezuelensis. Science 1960, 131, 986. [Google Scholar] [CrossRef]
- Maia, L.M.S.; Bezerra, M.C.F.; Costa, M.C.S.; Souza, E.M.; Oliveira, M.E.B.; Ribeiro, A.L.M.; Miyazaki, R.D.; Slhessarenko, R.D. Natural vertical infection by dengue virus serotype 4, Zika virus and Mayaro virus in Aedes (Stegomyia) aegypti and Aedes (Stegomyia) albopictus. Med. Vet. Entomol. 2019. [Google Scholar] [CrossRef]
- Smith, G.C.; Francy, D.B. Laboratory studies of a Brazilian strain of Aedes albopictus as a potential vector of Mayaro and Oropouche viruses. J. Am. Mosq. Control Assoc. 1991, 7, 89–93. [Google Scholar]
- Long, K.C.; Ziegler, S.A.; Thangamani, S.; Hausser, N.L.; Kochel, T.J.; Higgs, S.; Tesh, R.B. Experimental transmission of Mayaro virus by Aedes aegypti. Am. J. Trop. Med. Hyg. 2011, 85, 750–757. [Google Scholar] [CrossRef] [PubMed]
- Wiggins, K.; Eastmond, B.; Alto, B.W. Transmission potential of Mayaro virus in Florida Aedes aegypti and Aedes albopictus mosquitoes. Med. Vet. Entomol. 2018, 32, 436–442. [Google Scholar] [CrossRef] [PubMed]
- Brustolin, M.; Pujhari, S.; Henderson, C.A.; Rasgon, J.L. Anopheles mosquitoes may drive invasion and transmission of Mayaro virus across geographically diverse regions. PLoS Negl. Trop. Dis. 2018, 12, e0006895. [Google Scholar] [CrossRef] [PubMed]
- Kantor, A.M.; Lin, J.; Wang, A.; Thompson, D.C.; Franz, A.W.E. Infection Pattern of Mayaro Virus in Aedes aegypti (Diptera: Culicidae) and Transmission Potential of the Virus in Mixed Infections With Chikungunya Virus. J. Med. Entomol. 2019, 56, 832–843. [Google Scholar] [CrossRef]
- Walsh, M.G. Ecological and life history traits are associated with Ross River virus infection among sylvatic mammals in Australia. BMC Ecol. 2019, 19, 2. [Google Scholar] [CrossRef]
- Potter, A.; Johansen, C.A.; Fenwick, S.; Reid, S.A.; Lindsay, M.D.A. The seroprevalence and factors associated with Ross river virus infection in western grey kangaroos (Macropus fuliginosus) in Western Australia. Vector Borne Zoonotic Dis. 2014, 14, 740–745. [Google Scholar] [CrossRef]
- Flies, E.J.; Flies, A.S.; Fricker, S.R.; Weinstein, P.; Williams, C.R. Regional Comparison of Mosquito Bloodmeals in South Australia: Implications for Ross River Virus Ecology. J. Med. Entomol. 2016, 53, 902–910. [Google Scholar] [CrossRef]
- Koolhof, I.S.; Carver, S. Epidemic host community contribution to mosquito-borne disease transmission: Ross River virus. Epidemiol. Infect. 2017, 145, 656–666. [Google Scholar] [CrossRef]
- Stephenson, E.B.; Peel, A.J.; Reid, S.A.; Jansen, C.C.; McCallum, H. The non-human reservoirs of Ross River virus: A systematic review of the evidence. Parasit. Vectors 2018, 11, 188. [Google Scholar] [CrossRef]
- Lau, C.; Aubry, M.; Musso, D.; Teissier, A.; Paulous, S.; Desprès, P.; de-Lamballerie, X.; Pastorino, B.; Cao-Lormeau, V.-M.; Weinstein, P. New evidence for endemic circulation of Ross River virus in the Pacific Islands and the potential for emergence. Int. J. Infect. Dis. 2017, 57, 73–76. [Google Scholar] [CrossRef]
- Gummow, B.; Tan, R.; Joice, R.K.; Burgess, G.; Picard, J. Seroprevalence and associated risk factors of mosquito-borne alphaviruses in horses in northern Queensland. Aust. Vet. J. 2018, 96, 243–251. [Google Scholar] [CrossRef]
- Jacups, S.P.; Whelan, P.I.; Currie, B.J. Ross River Virus and Barmah Forest Virus Infections: A Review of History, Ecology, and Predictive Models, with Implications for Tropical Northern Australia. Vector Borne Zoonotic Dis. 2008, 8, 283–298. [Google Scholar] [CrossRef]
- Gratz, N.G. Critical review of the vector status of Aedes albopictus. Med. Vet. Entomol. 2004, 18, 215–227. [Google Scholar] [CrossRef]
- Nasci, R.S.; Mitchell, C.J. Larval diet, adult size, and susceptibility of Aedes aegypti (Diptera: Culicidae) to infection with Ross River virus. J. Med. Entomol. 1994, 31, 123–126. [Google Scholar] [CrossRef]
- Mitchell, C.J.; Miller, B.R.; Gubler, D.J. Vector competence of Aedes albopictus from Houston, Texas, for dengue serotypes 1 to 4, yellow fever and Ross River viruses. J. Am. Mosq. Control Assoc. 1987, 3, 460–465. [Google Scholar]
- Mitchell, C.J.; Gubler, D.J. Vector competence of geographic strains of Aedes albopictus and Aedes polynesiensis and certain other Aedes (Stegomyia) mosquitoes for Ross River virus. J. Am. Mosq. Control Assoc. 1987, 3, 142–147. [Google Scholar]
- Subissi, L.; Daudens-Vaysse, E.; Cassadou, S.; Ledrans, M.; Bompard, P.; Gustave, J.; Aubry, M.; Cao-Lormeau, V.-M.; Mallet, H.-P. Revising rates of asymptomatic Zika virus infection based on sentinel surveillance data from French Overseas Territories. Int. J. Infect. Dis. 2017, 65, 116–118. [Google Scholar] [CrossRef]
- Grange, L.; Simon-Loriere, E.; Sakuntabhai, A.; Gresh, L.; Paul, R.; Harris, E. Epidemiological Risk Factors Associated with High Global Frequency of Inapparent Dengue Virus Infections. Front. Immunol. 2014, 5, 280. [Google Scholar] [CrossRef]
- Moro, M.L.; Gagliotti, C.; Silvi, G.; Angelini, R.; Sambri, V.; Rezza, G.; Massimiliani, E.; Mattivi, A.; Grilli, E.; Finarelli, A.C.; et al. Chikungunya virus in North-Eastern Italy: A seroprevalence survey. Am. J. Trop. Med. Hyg. 2010, 82, 508–511. [Google Scholar] [CrossRef]
- Brouard, C.; Bernillon, P.; Quatresous, I.; Pillonel, J.; Assal, A.; De Valk, H.; Desenclos, J.-C. Estimated risk of Chikungunya viremic blood donation during an epidemic on Reunion Island in the Indian Ocean, 2005 to 2007. Transfusion 2008, 48, 1333–1341. [Google Scholar] [CrossRef]
- Simon, F.; Javelle, E.; Cabie, A.; Bouquillard, E.; Troisgros, O.; Gentile, G.; Leparc-Goffart, I.; Hoen, B.; Gandjbakhch, F.; Rene-Corail, P.; et al. French guidelines for the management of chikungunya (acute and persistent presentations). November 2014. Médecine Mal. Infect. 2015, 45, 243–263. [Google Scholar] [CrossRef]
- Aubry, M.; Teissier, A.; Huart, M.; Merceron, S.; Vanhomwegen, J.; Mapotoeke, M.; Mariteragi-Helle, T.; Roche, C.; Vial, A.-L.; Teururai, S.; et al. Seroprevalence of Dengue and Chikungunya Virus Antibodies, French Polynesia, 2014–2015. Emerg. Infect. Dis. 2018, 24, 558–561. [Google Scholar] [CrossRef]
- Yoon, I.-K.; Alera, M.T.; Lago, C.B.; Tac-An, I.A.; Villa, D.; Fernandez, S.; Thaisomboonsuk, B.; Klungthong, C.; Levy, J.W.; Velasco, J.M.; et al. High rate of subclinical chikungunya virus infection and association of neutralizing antibody with protection in a prospective cohort in the Philippines. PLoS Negl. Trop. Dis. 2015, 9, e0003764. [Google Scholar] [CrossRef]
- Shore, H. O’nyong’nyong fever: An epidemic virus disease in east africa. III. Some clinical and epidemiological observations in the northern province of uganda. Trans. R. Soc. Trop. Med. Hyg. 1961, 5, 361–373. [Google Scholar] [CrossRef]
- Williams, M.C.; Woodall, J.P.; Porterfield, J.S. O’nyong’nyong fever: An epidemic virus disease in East Africa. V Human antibody studies by plaque inhibition and other serological tests. Trans. R. Soc. Trop. Med. Hyg. 1962, 56, 166–172. [Google Scholar] [CrossRef]
- Williams, M.C.; Woodall, J.P.; Gillett, J.D. O’nyong’nyong fever: An epidemic virus disease in east africa. VII. Virus isolations from man and serological studies up to july 1961. Trans. R. Soc. Trop. Med. Hyg. 1965, 59, 186–197. [Google Scholar] [CrossRef]
- Hawkes, R.A.; Boughton, C.R.; Naim, H.M.; Stallman, N.D. A major outbreak of epidemic polyarthritis in New South Wales during the summer of 1983/1984. Med. J. Aust. 1985, 143, 330–333. [Google Scholar]
- Harley, D.; Sleigh, A.; Ritchie, S. Ross River Virus Transmission, Infection, and Disease: A Cross-Disciplinary Review. Clin. Microbiol. Rev. 2001, 14, 909–932. [Google Scholar] [CrossRef]
- Shanks, G.D. Could Ross River Virus Be the Next Zika? J. Travel Med. 2019. [Google Scholar] [CrossRef]
- Borgherini, G.; Poubeau, P.; Staikowsky, F.; Lory, M.; Moullec, N.L.; Becquart, J.P.; Wengling, C.; Michault, A.; Paganin, F. Outbreak of Chikungunya on Reunion Island: Early Clinical and Laboratory Features in 157 Adult Patients. Clin. Infect. Dis. 2007, 44, 1401–1407. [Google Scholar] [CrossRef]
- Thiruvengadam, K.V.; Kalyanasundaram, V.; Rajgopal, J. Clinical and pathological studies on chikungunya fever in Madras city. Indian J. Med. Res. 1965, 53, 729–744. [Google Scholar]
- Couturier, E.; Guillemin, F.; Mura, M.; Léon, L.; Virion, J.-M.; Letort, M.-J.; De Valk, H.; Simon, F.; Vaillant, V. Impaired quality of life after chikungunya virus infection: A 2-year follow-up study. Rheumatology 2012, 51, 1315–1322. [Google Scholar] [CrossRef]
- Manimunda, S.P.; Vijayachari, P.; Uppoor, R.; Sugunan, A.P.; Singh, S.S.; Rai, S.K.; Sudeep, A.B.; Muruganandam, N.; Chaitanya, I.K.; Guruprasad, D.R. Clinical progression of chikungunya fever during acute and chronic arthritic stages and the changes in joint morphology as revealed by imaging. Trans. R. Soc. Trop. Med. Hyg. 2010, 104, 392–399. [Google Scholar] [CrossRef]
- Staikowsky, F.; Talarmin, F.; Grivard, P.; Souab, A.; Schuffenecker, I.; Roux, K.L.; Lecuit, M.; Michault, A. Prospective Study of Chikungunya Virus Acute Infection in the Island of La Réunion during the 2005–2006 Outbreak. PLoS ONE 2009, 4, e7603. [Google Scholar] [CrossRef]
- Thiberville, S.-D.; Boisson, V.; Gaudart, J.; Simon, F.; Flahault, A.; de Lamballerie, X. Chikungunya fever: A clinical and virological investigation of outpatients on Reunion Island, South-West Indian Ocean. PLoS Negl. Trop. Dis. 2013, 7, e2004. [Google Scholar] [CrossRef] [PubMed]
- Perti, T.; Lucero-Obusan, C.A.; Schirmer, P.L.; Winters, M.A.; Holodniy, M. Chikungunya Fever Cases Identified in the Veterans Health Administration System, 2014. PLoS Negl. Trop. Dis. 2016, 10, e0004630. [Google Scholar] [CrossRef]
- Sarkar, J.K.; Chatterjee, S.N.; Chakravarty, S.K. Three-year study of mosquito-borne haemorrhagic fever in Calcutta. Trans. R. Soc. Trop. Med. Hyg. 1967, 61, 725–735. [Google Scholar] [CrossRef]
- Deller, J.J.; Russell, P.K. An analysis of fevers of unknown origin in American soldiers in Vietnam. Ann. Intern. Med. 1967, 66, 1129–1143. [Google Scholar] [CrossRef]
- Vijayakumar, K.P.; Anish, T.S.N.; George, B.; Lawrence, T.; Muthukkutty, S.C.; Ramachandran, R. Clinical profile of chikungunya patients during the epidemic of 2007 in Kerala, India. J. Glob. Infect. Dis. 2011, 3, 221. [Google Scholar] [PubMed]
- Zingman, M.A.; Paulino, A.T.; Payano, M.P. Clinical manifestations of chikungunya among university professors and staff in Santo Domingo, the Dominican Republic. Rev. Panam. Salud Pública 2017, 41, e64. [Google Scholar] [PubMed]
- Huits, R.; de Kort, J.; van Den Berg, R.; Chong, L.; Tsoumanis, A.; Eggermont, K.; Bartholomeeusen, K.; Ariën, K.K.; Jacobs, J.; van Esbroeck, M.; et al. Chikungunya virus infection in Aruba: Diagnosis, clinical features and predictors of post-chikungunya chronic polyarthralgia. PLoS ONE 2018, 13, e0196630. [Google Scholar] [CrossRef]
- Kennedy, A.C.; Fleming, J.; Solomon, L. Chikungunya viral arthropathy: A clinical description. J. Rheumatol. 1980, 7, 231–236. [Google Scholar] [PubMed]
- Kiwanuka, N.; Sanders, E.J.; Rwaguma, E.B.; Kawamata, J.; Ssengooba, F.P.; Najjemba, R.; Were, W.A.; Lamunu, M.; Bagambisa, G.; Burkot, T.R.; et al. O’nyong’nyong Fever in South-Central Uganda, 1996–1997: Clinical Features and Validation of a Clinical Case Definition for Surveillance Purposes. Clin. Infect. Dis. 1999, 29, 1243–1250. [Google Scholar] [CrossRef] [PubMed]
- Mourão, M.P.G.; Bastos, M.D.S.; de Figueiredo, R.P.; Gimaque, J.B.L.; dos Santos Galusso, E.; Kramer, V.M.; de Oliveira, C.M.C.; Naveca, F.G.; Figueiredo, L.T.M. Mayaro fever in the city of Manaus, Brazil, 2007–2008. Vector Borne Zoonotic Dis. 2012, 12, 42–46. [Google Scholar]
- Halsey, E.S.; Siles, C.; Guevara, C.; Vilcarromero, S.; Jhonston, E.J.; Ramal, C.; Aguilar, P.V.; Ampuero, J.S. Mayaro virus infection, Amazon Basin region, Peru, 2010-2013. Emerg. Infect. Dis. 2013, 19, 1839–1842. [Google Scholar] [CrossRef]
- Vieira, C.J.D.S.P.; Silva, D.J.F.D.; Barreto, E.S.; Siqueira, C.E.H.; Colombo, T.E.; Ozanic, K.; Schmidt, D.J.; Drumond, B.P.; Mondini, A.; Nogueira, M.L.; et al. Detection of Mayaro virus infections during a dengue outbreak in Mato Grosso, Brazil. Acta Trop. 2015, 147, 12–16. [Google Scholar] [CrossRef] [PubMed]
- Da Costa, V.G.; de Rezende Féres, V.C.; Saivish, M.V.; de Lima Gimaque, J.B.; Moreli, M.L. Silent emergence of Mayaro and Oropouche viruses in humans in Central Brazil. Int. J. Infect. Dis. 2017, 62, 84–85. [Google Scholar] [CrossRef] [PubMed]
- Condon, R.J.; Rouse, I.L. Acute symptoms and sequelae of Ross River virus infection in South-Western Australia: A follow-up study. Clin. Diagn. Virol. 1995, 3, 273–284. [Google Scholar] [CrossRef]
- Westley-Wise, V.J.; Beard, J.R.; Sladden, T.J.; Dunn, T.M.; Simpson, J. Ross River virus infection on the North Coast of New South Wales. Aust. N. Z. J. Public Health 1996, 20, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Mylonas, A.D.; Brown, A.M.; Carthew, T.L.; McGrath, B.; Purdie, D.M.; Pandeya, N.; Vecchio, P.C.; Collins, L.G.; Gardner, I.D.; de Looze, F.J.; et al. Natural history of Ross River virus-induced epidemic polyarthritis. Med. J. Aust. 2002, 177, 356–360. [Google Scholar]
- Harley, D.; Bossingham, D.; Purdie, D.M.; Pandeya, N.; Sleigh, A.C. Ross River virus disease in tropical Queensland: Evolution of rheumatic manifestations in an inception cohort followed for six months. Med. J. Aust. 2002, 177, 352–355. [Google Scholar]
- Economopoulou, A.; Dominguez, M.; Helynck, B.; Sissoko, D.; Wichmann, O.; Quenel, P.; Germonneau, P.; Quatresous, I. Atypical Chikungunya virus infections: Clinical manifestations, mortality and risk factors for severe disease during the 2005–2006 outbreak on Réunion. Epidemiol. Infect. 2009, 137, 534. [Google Scholar] [CrossRef]
- Mazaud, R.; Salaün, J.J.; Montabone, H.; Goube, P.; Bazillio, R. [Acute neurologic and sensorial disorders in dengue and Chikungunya fever]. Bull. Soc. Pathol. Exot. Fil. 1971, 64, 22–30. [Google Scholar]
- Oehler, E.; Fournier, E.; Leparc-Goffart, I.; Larre, P.; Cubizolle, S.; Sookhareea, C.; Lastère, S.; Ghawche, F. Increase in cases of Guillain-Barré syndrome during a Chikungunya outbreak, French Polynesia, 2014 to 2015. Eurosurveillance 2015, 20, 30079. [Google Scholar] [CrossRef]
- Mohite, A.A.; Agius-Fernandez, A. Chikungunya fever presenting with acute optic neuropathy. BMJ Case Rep. 2015, 2015, bcr2015210081. [Google Scholar] [CrossRef]
- Maiti, C.R.; Mukherjee, A.K.; Bose, B.; Saha, G.L. Myopericarditis following chikungunya virus infection. J. Indian Med. Assoc. 1978, 70, 256–258. [Google Scholar]
- Obeyesekere, I.; Hermon, Y. Arbovirus heart disease: Myocarditis and cardiomyopathy following dengue and chikungunya fever—A follow-up study. Am. Heart J. 1973, 85, 186–194. [Google Scholar] [CrossRef]
- Dorléans, F.; Hoen, B.; Najioullah, F.; Herrmann-Storck, C.; Schepers, K.M.; Abel, S.; Lamaury, I.; Fagour, L.; Césaire, R.; Guyomard, S.; et al. Outbreak of Chikungunya in the French Caribbean Islands of Martinique and Guadeloupe: Findings from a Hospital-Based Surveillance System (2013-2015). Am. J. Trop. Med. Hyg. 2018, 98, 1819–1825. [Google Scholar] [CrossRef]
- Evans-Gilbert, T. Chikungunya and Neonatal Immunity: Fatal Vertically Transmitted Chikungunya Infection. Am. J. Trop. Med. Hyg. 2017, 96, 913–915. [Google Scholar] [CrossRef]
- Fraser, J.R.; Cunningham, A.L.; Muller, H.K.; Sinclair, R.A.; Standish, H.G. Glomerulonephritis in the acute phase of Ross River virus disease (epidemic polyarthritis). Clin. Nephrol. 1988, 29, 149–152. [Google Scholar]
- Scrimgeour, E.M.; Aaskov, J.G.; Matz, L.R. Ross River virus arthritis in Papua New Guinea. Trans. R. Soc. Trop. Med. Hyg. 1987, 81, 833–834. [Google Scholar] [CrossRef]
- Scrimgeour, E.M. Suspected Ross River virus encephalitis in Papua New Guinea. Aust. N. Z. J. Med. 1999, 29, 559. [Google Scholar] [CrossRef]
- Lucas, R.E.; Qiao, M. A case of encephalitis in central Australia due to Ross River virus? Aust. N. Z. J. Med. 1999, 29, 268–270. [Google Scholar] [CrossRef]
- Gallian, P.; Leparc-Goffart, I.; Richard, P.; Maire, F.; Flusin, O.; Djoudi, R.; Chiaroni, J.; Charrel, R.; Tiberghien, P.; de Lamballerie, X. Epidemiology of Chikungunya Virus Outbreaks in Guadeloupe and Martinique, 2014: An Observational Study in Volunteer Blood Donors. PLoS Negl. Trop. Dis. 2017, 11, e0005254. [Google Scholar] [CrossRef]
- Robin, S.; Ramful, D.; Zettor, J.; Benhamou, L.; Jaffar-Bandjee, M.-C.; Rivière, J.-P.; Marichy, J.; Ezzedine, K.; Alessandri, J.-L. Severe bullous skin lesions associated with Chikungunya virus infection in small infants. Eur. J. Pediatr. 2010, 169, 67–72. [Google Scholar] [CrossRef]
- Garg, T.; Sanke, S.; Ahmed, R.; Chander, R.; Basu, S. Stevens-Johnson syndrome and toxic epidermal necrolysis-like cutaneous presentation of chikungunya fever: A case series. Pediatr. Dermatol. 2018, 35, 392–396. [Google Scholar] [CrossRef]
- Jadhav, M.; Namboodripad, M.; Carman, R.H.; Carey, D.E.; Myers, R.M. Chikungunya disease in infants and children in Vellore: A report of clinical and haematological features of virologically proved cases. Indian J. Med. Res. 1965, 53, 764–776. [Google Scholar]
- De Ranitz, C.M.; Myers, R.M.; Varkey, M.J.; Isaac, Z.H.; Carey, D.E. Clinical impressions of chikungunya in Vellore gained from study of adult patients. Indian J. Med. Res. 1965, 53, 756–763. [Google Scholar]
- Godaert, L.; Bartholet, S.; Dorléans, F.; Najioullah, F.; Colas, S.; Fanon, J.-L.; Cabié, A.; Césaire, R.; Dramé, M. Prognostic factors of inhospital death in elderly patients: A time-to-event analysis of a cohort study in Martinique (French West Indies). BMJ Open 2018, 8, e018838. [Google Scholar] [CrossRef]
- Fraser, J.R.; Cunningham, A.L. Incubation time of epidemic polyarthritis. Med. J. Aust. 1980, 1, 550–551. [Google Scholar]
- Mudge, P.R. A survey of epidemic polyarthritis in the Riverland area, 1976. Med. J. Aust. 1977, 1, 649–651. [Google Scholar]
- Tappe, D.; Schmidt-Chanasit, J.; Ries, A.; Ziegler, U.; Müller, A.; Stich, A. Ross River virus infection in a traveller returning from northern Australia. Med. Microbiol. Immunol. 2009, 198, 271–273. [Google Scholar] [CrossRef]
- Paixão, E.S.; Rodrigues, L.C.; Costa, M.D.C.N.; Itaparica, M.; Barreto, F.; Gérardin, P.; Teixeira, M.G. Chikungunya chronic disease: A systematic review and meta-analysis. Trans. R. Soc. Trop. Med. Hyg. 2018, 112, 301–316. [Google Scholar]
- Bouquillard, E.; Fianu, A.; Bangil, M.; Charlette, N.; Ribéra, A.; Michault, A.; Favier, F.; Simon, F.; Flipo, R.-M. Rheumatic manifestations associated with Chikungunya virus infection: A study of 307 patients with 32-month follow-up (RHUMATOCHIK study). Jt. Bone Spine Rev. Rhum. 2018, 85, 207–210. [Google Scholar] [CrossRef]
- Schilte, C.; Staikowsky, F.; Staikovsky, F.; Couderc, T.; Madec, Y.; Carpentier, F.; Kassab, S.; Albert, M.L.; Lecuit, M.; Michault, A. Chikungunya virus-associated long-term arthralgia: A 36-month prospective longitudinal study. PLoS Negl. Trop. Dis. 2013, 7, e2137. [Google Scholar] [CrossRef]
- Bouquillard, É.; Combe, B. A report of 21 cases of rheumatoid arthritis following Chikungunya fever. A mean follow-up of two years. Joint Bone Spine 2009, 76, 654–657. [Google Scholar] [CrossRef]
- Chang, A.Y.; Martins, K.A.O.; Encinales, L.; Reid, S.P.; Acuña, M.; Encinales, C.; Matranga, C.B.; Pacheco, N.; Cure, C.; Shukla, B.; et al. Chikungunya Arthritis Mechanisms in the Americas: A Cross-Sectional Analysis of Chikungunya Arthritis Patients Twenty-Two Months After Infection Demonstrating No Detectable Viral Persistence in Synovial Fluid. Arthritis Rheumatol. 2018, 70, 585–593. [Google Scholar] [CrossRef]
- Javelle, E.; Ribera, A.; Degasne, I.; Gaüzère, B.-A.; Marimoutou, C.; Simon, F. Specific Management of Post-Chikungunya Rheumatic Disorders: A Retrospective Study of 159 Cases in Reunion Island from 2006–2012. PLoS Negl. Trop. Dis. 2015, 9, e0003603. [Google Scholar] [CrossRef]
- Taylor, S.F.; Patel, P.R.; Herold, T.J.S. Recurrent arthralgias in a patient with previous Mayaro fever infection. South. Med. J. 2005, 98, 484–485. [Google Scholar] [CrossRef]
- Theilacker, C.; Held, J.; Allering, L.; Emmerich, P.; Schmidt-Chanasit, J.; Kern, W.V.; Panning, M. Prolonged polyarthralgia in a German traveller with Mayaro virus infection without inflammatory correlates. BMC Infect. Dis. 2013, 13, 369. [Google Scholar] [CrossRef]
- Receveur, M.C.; Grandadam, M.; Pistone, T.; Malvy, D. Infection with Mayaro virus in a French traveller returning from the Amazon region, Brazil, January, 2010. Eurosurveillance 2010, 15. [Google Scholar] [CrossRef]
- Hassing, R.-J.; Leparc-Goffart, I.; Blank, S.N.; Thevarayan, S.; Tolou, H.; van Doornum, G.; van Genderen, P.J. Imported Mayaro virus infection in the Netherlands. J. Infect. 2010, 61, 343–345. [Google Scholar] [CrossRef]
- Tappe, D.; Pérez-Girón, J.V.; Just-Nübling, G.; Schuster, G.; Gómez-Medina, S.; Günther, S.; Muñoz-Fontela, C.; Schmidt-Chanasit, J. Sustained Elevated Cytokine Levels during Recovery Phase of Mayaro Virus Infection. Emerg. Infect. Dis. 2016, 22, 750–752. [Google Scholar] [CrossRef]
- Chen, W.; Foo, S.-S.; Rulli, N.E.; Taylor, A.; Sheng, K.-C.; Herrero, L.J.; Herring, B.L.; Lidbury, B.A.; Li, R.W.; Walsh, N.C.; et al. Arthritogenic alphaviral infection perturbs osteoblast function and triggers pathologic bone loss. Proc. Natl. Acad. Sci. USA 2014, 111, 6040–6045. [Google Scholar] [CrossRef] [PubMed]
- Lim, E.X.Y.; Supramaniam, A.; Lui, H.; Coles, P.; Lee, W.S.; Liu, X.; Rudd, P.A.; Herrero, L.J. Chondrocytes Contribute to Alphaviral Disease Pathogenesis as a Source of Virus Replication and Soluble Factor Production. Viruses 2018, 10, 86. [Google Scholar] [CrossRef] [PubMed]
- Panning, M.; Grywna, K.; van Esbroeck, M.; Emmerich, P.; Drosten, C. Chikungunya Fever in Travelers Returning to Europe from the Indian Ocean Region, 2006. Emerg. Infect. Dis. 2008, 14, 416–422. [Google Scholar] [CrossRef] [PubMed]
- Appassakij, H.; Khuntikij, P.; Kemapunmanus, M.; Wutthanarungsan, R.; Silpapojakul, K. Viremic profiles in asymptomatic and symptomatic chikungunya fever: A blood transfusion threat? Transfusion 2013, 53, 2567–2574. [Google Scholar] [CrossRef] [PubMed]
- Acosta-Ampudia, Y.; Monsalve, D.M.; Rodríguez, Y.; Pacheco, Y.; Anaya, J.-M.; Ramírez-Santana, C. Mayaro: An emerging viral threat? Emerg. Microbes Infect. 2018, 7, 163. [Google Scholar] [CrossRef]
- Gibney, K.B.; Fischer, M.; Prince, H.E.; Kramer, L.D.; St. George, K.; Kosoy, O.L.; Laven, J.J.; Staples, J.E. Chikungunya Fever in the United States: A Fifteen Year Review of Cases. Clin. Infect. Dis. 2011, 52, e121–e126. [Google Scholar] [CrossRef] [PubMed]
- Telles, J.-N.; Le Roux, K.; Grivard, P.; Vernet, G.; Michault, A. Evaluation of real-time nucleic acid sequence-based amplification for detection of Chikungunya virus in clinical samples. J. Med. Microbiol. 2009, 58, 1168–1172. [Google Scholar] [CrossRef]
- Waggoner, J.; Heath, C.J.; Ndenga, B.; Mutuku, F.; Sahoo, M.K.; Mohamed-Hadley, A.; Vulule, J.; Mukoko, D.; Desiree LaBeaud, A.; Pinsky, B.A. Development of a Real-Time Reverse Transcription Polymerase Chain Reaction for O’nyong’nyong Virus and Evaluation with Clinical and Mosquito Specimens from Kenya. Am. J. Trop. Med. Hyg. 2017, 97, 121–124. [Google Scholar] [CrossRef]
- Waggoner, J.J.; Rojas, A.; Mohamed-Hadley, A.; de Guillén, Y.A.; Pinsky, B.A. Real-time RT-PCR for Mayaro virus detection in plasma and urine. J. Clin. Virol. 2018, 98, 1–4. [Google Scholar] [CrossRef]
- Bozza, F.A.; Moreira-Soto, A.; Rockstroh, A.; Fischer, C.; Nascimento, A.D.; Calheiros, A.S.; Drosten, C.; Bozza, P.T.; Souza, T.M.L.; Ulbert, S.; et al. Differential Shedding and Antibody Kinetics of Zika and Chikungunya Viruses, Brazil. Emerg. Infect. Dis. 2019, 25, 311–315. [Google Scholar] [CrossRef]
- Malvy, D.; Ezzedine, K.; Mamani-Matsuda, M.; Autran, B.; Tolou, H.; Receveur, M.-C.; Pistone, T.; Rambert, J.; Moynet, D.; Mossalayi, D. Destructive arthritis in a patient with chikungunya virus infection with persistent specific IgM antibodies. BMC Infect. Dis. 2009, 9, 200. [Google Scholar] [CrossRef]
- Azami, N.A.M.; Moi, M.L.; Takasaki, T. Neutralization Assay for Chikungunya Virus Infection: Plaque Reduction Neutralization Test; Humana Press: New York, NY, USA, 2016; pp. 273–282. [Google Scholar]
- Henss, L.; Yue, C.; Kandler, J.; Faddy, H.M.; Simmons, G.; Panning, M.; Lewis-Ximenez, L.L.; Baylis, S.A.; Schnierle, B.S. Establishment of an Alphavirus-Specific Neutralization Assay to Distinguish Infections with Different Members of the Semliki Forest complex. Viruses 2019, 11, 82. [Google Scholar] [CrossRef]
- Walker, L.J.; Selvey, L.A.; Jardine, A.; Johansen, C.A.; Lindsay, M.D.A. Mosquito and Virus Surveillance as a Predictor of Human Ross River Virus Infection in South-West Western Australia: How Useful Is It? Am. J. Trop. Med. Hyg. 2018, 99, 1066–1073. [Google Scholar] [CrossRef]
- Curren, E.J.; Lehman, J.; Kolsin, J.; Walker, W.L.; Martin, S.W.; Staples, J.E.; Hills, S.L.; Gould, C.V.; Rabe, I.B.; Fischer, M.; et al. West Nile Virus and Other Nationally Notifiable Arboviral Diseases—United States, 2017. MMWR Morb. Mortal. Wkly. Rep. 2018, 67, 1137–1142. [Google Scholar] [CrossRef]
- Silva, N.M.D.; Teixeira, R.A.G.; Cardoso, C.G.; Siqueira Junior, J.B.; Coelho, G.E.; Oliveira, E.S.F. Chikungunya surveillance in Brazil: Challenges in the context of Public Health. Epidemiol. Serviços Saúde 2018, 27, e2017127. [Google Scholar]
- Trentini, F.; Poletti, P.; Baldacchino, F.; Drago, A.; Montarsi, F.; Capelli, G.; Rizzoli, A.; Rosà, R.; Rizzo, C.; Merler, S.; et al. The containment of potential outbreaks triggered by imported Chikungunya cases in Italy: A cost utility epidemiological assessment of vector control measures. Sci. Rep. 2018, 8, 9034. [Google Scholar] [CrossRef]
- Bitar, D.; Che, D.; Capek, I.; de Valk, H.; Saura, C. [Public health surveillance and assessment of emerging infectious threats: Method and criteria for risk analysis]. Med. Mal. Infect. 2011, 41, 53–62. [Google Scholar] [CrossRef]
- Hierlihy, C.; Waddell, L.; Young, I.; Greig, J.; Corrin, T.; Mascarenhas, M. A systematic review of individual and community mitigation measures for prevention and control of chikungunya virus. PLoS ONE 2019, 14, e0212054. [Google Scholar] [CrossRef]
- Kurucz, N.; Jacups, S.; Carter, J.M. Determining Culex annulirostris larval densities and control efforts across a coastal wetland, Northern Territory, Australia. J. Vector Ecol. 2016, 41, 271–278. [Google Scholar] [CrossRef]
- Staples, K.; Oosthuizen, J.; Lund, M. Effectiveness of S-Methoprene Briquets and Application Method for Mosquito Control in Urban Road Gullies/Catch Basins/Gully Pots in a Mediterranean Climate: Implications for Ross River Virus Transmission. J. Am. Mosq. Control Assoc. 2016, 32, 203–209. [Google Scholar] [CrossRef]
- Flies, E.J.; Williams, C.R.; Weinstein, P.; Anderson, S.J. Improving public health intervention for mosquito-borne disease: The value of geovisualization using source of infection and LandScan data. Epidemiol. Infect. 2016, 144, 3108–3119. [Google Scholar] [CrossRef]
- Erasmus, J.H.; Rossi, S.L.; Weaver, S.C. Development of Vaccines for Chikungunya Fever. J. Infect. Dis. 2016, 214, S488–S496. [Google Scholar] [CrossRef]
- Edelman, R.; Tacket, C.O.; Wasserman, S.S.; Bodison, S.A.; Perry, J.A.; Perry, J.G. Phase II safety and immunogenicity study of live chikungunya virus vaccine TSI-GSD-218. Am. J. Trop. Med. Hyg. 2000, 62, 681–685. [Google Scholar] [CrossRef]
- Wang, E.; Volkova, E.; Adams, A.P.; Forrester, N.; Xiao, S.-Y.; Frolov, I.; Weaver, S.C. Chimeric alphavirus vaccine candidates for chikungunya. Vaccine 2008, 26, 5030–5039. [Google Scholar] [CrossRef]
- Brandler, S.; Ruffié, C.; Combredet, C.; Brault, J.-B.; Najburg, V.; Prevost, M.-C.; Habel, A.; Tauber, E.; Desprès, P.; Tangy, F. A recombinant measles vaccine expressing chikungunya virus-like particles is strongly immunogenic and protects mice from lethal challenge with chikungunya virus. Vaccine 2013, 31, 3718–3725. [Google Scholar] [CrossRef]
- Ramsauer, K.; Schwameis, M.; Firbas, C.; Müllner, M.; Putnak, R.J.; Thomas, S.J.; Desprès, P.; Tauber, E.; Jilma, B.; Tangy, F. Immunogenicity, safety, and tolerability of a recombinant measles-virus-based chikungunya vaccine: A randomised, double-blind, placebo-controlled, active-comparator, first-in-man trial. Lancet Infect. Dis. 2015, 15, 519–527. [Google Scholar] [CrossRef]
- Reisinger, E.C.; Tschismarov, R.; Beubler, E.; Wiedermann, U.; Firbas, C.; Loebermann, M.; Pfeiffer, A.; Muellner, M.; Tauber, E.; Ramsauer, K. Immunogenicity, safety, and tolerability of the measles-vectored chikungunya virus vaccine MV-CHIK: A double-blind, randomised, placebo-controlled and active-controlled phase 2 trial. Lancet 2018, 392, 2718–2727. [Google Scholar] [CrossRef]
- Chattopadhyay, A.; Wang, E.; Seymour, R.; Weaver, S.C.; Rose, J.K. A chimeric vesiculo/alphavirus is an effective alphavirus vaccine. J. Virol. 2013, 87, 395–402. [Google Scholar] [CrossRef]
- Chattopadhyay, A.; Aguilar, P.V.; Bopp, N.E.; Yarovinsky, T.O.; Weaver, S.C.; Rose, J.K. A recombinant virus vaccine that protects against both Chikungunya and Zika virus infections. Vaccine 2018, 36, 3894–3900. [Google Scholar] [CrossRef]
- Harrison, V.R.; Eckels, K.H.; Hampton, C. Production and Evaluation of a Formalin-Killed Chikungunya Vaccine. J. Immunol. 1971, 107, 6. [Google Scholar]
- Tiwari, M.; Parida, M.; Santhosh, S.R.; Khan, M.; Dash, P.K.; Rao, P.V.L. Assessment of immunogenic potential of Vero adapted formalin inactivated vaccine derived from novel ECSA genotype of Chikungunya virus. Vaccine 2009, 27, 2513–2522. [Google Scholar] [CrossRef]
- Akahata, W.; Yang, Z.-Y.; Andersen, H.; Sun, S.; Holdaway, H.A.; Kong, W.-P.; Lewis, M.G.; Higgs, S.; Rossmann, M.G.; Rao, S.; et al. A virus-like particle vaccine for epidemic Chikungunya virus protects nonhuman primates against infection. Nat. Med. 2010, 16, 334–338. [Google Scholar] [CrossRef]
- Metz, S.W.; Martina, B.E.; van den Doel, P.; Geertsema, C.; Osterhaus, A.D.; Vlak, J.M.; Pijlman, G.P. Chikungunya virus-like particles are more immunogenic in a lethal AG129 mouse model compared to glycoprotein E1 or E2 subunits. Vaccine 2013, 31, 6092–6096. [Google Scholar] [CrossRef]
- Metz, S.W.; Gardner, J.; Geertsema, C.; Le, T.T.; Goh, L.; Vlak, J.M.; Suhrbier, A.; Pijlman, G.P. Effective Chikungunya Virus-like Particle Vaccine Produced in Insect Cells. PLoS Negl. Trop. Dis. 2013, 7, e2124. [Google Scholar] [CrossRef]
- Mallilankaraman, K.; Shedlock, D.J.; Bao, H.; Kawalekar, O.U.; Fagone, P.; Ramanathan, A.A.; Ferraro, B.; Stabenow, J.; Vijayachari, P.; Sundaram, S.G.; et al. A DNA Vaccine against Chikungunya Virus Is Protective in Mice and Induces Neutralizing Antibodies in Mice and Nonhuman Primates. PLoS Negl. Trop. Dis. 2011, 5, e928. [Google Scholar] [CrossRef]
- Tretyakova, I.; Hearn, J.; Wang, E.; Weaver, S.; Pushko, P. DNA Vaccine Initiates Replication of Live Attenuated Chikungunya Virus In Vitro and Elicits Protective Immune Response in Mice. J. Infect. Dis. 2014, 209, 1882–1890. [Google Scholar] [CrossRef]
- A Phase 1, Randomized, Placebo-Controlled, Dose-Ranging Study to Evaluate the Safety and Immunogenicity of VAL-181388 in Healthy Adults in a Non Endemic Chikungunya Region—ICH GCP—Clinical Trials Registry. Available online: https://ichgcp.net/clinical-trials-registry/NCT03325075 (accessed on 2 April 2019).
- Khan, M.; Dhanwani, R.; Rao, P.V.L.; Parida, M. Subunit vaccine formulations based on recombinant envelope proteins of Chikungunya virus elicit balanced Th1/Th2 response and virus-neutralizing antibodies in mice. Virus Res. 2012, 167, 236–246. [Google Scholar] [CrossRef]
- Chang, L.-J.; Dowd, K.A.; Mendoza, F.H.; Saunders, J.G.; Sitar, S.; Plummer, S.H.; Yamshchikov, G.; Sarwar, U.N.; Hu, Z.; Enama, M.E.; et al. Safety and tolerability of chikungunya virus-like particle vaccine in healthy adults: A phase 1 dose-escalation trial. Lancet 2014, 384, 2046–2052. [Google Scholar] [CrossRef]
- DeZure, A.D.; Berkowitz, N.M.; Graham, B.S.; Ledgerwood, J.E. Whole-Inactivated and Virus-Like Particle Vaccine Strategies for Chikungunya Virus. J. Infect. Dis. 2016, 214, S497–S499. [Google Scholar] [CrossRef]
- Goo, L.; Dowd, K.A.; Lin, T.-Y.; Mascola, J.R.; Graham, B.S.; Ledgerwood, J.E.; Pierson, T.C. A Virus-Like Particle Vaccine Elicits Broad Neutralizing Antibody Responses in Humans to All Chikungunya Virus Genotypes. J. Infect. Dis. 2016, 214, 1487–1491. [Google Scholar] [CrossRef]
- Auerswald, H.; Boussioux, C.; In, S.; Mao, S.; Ong, S.; Huy, R.; Leang, R.; Chan, M.; Duong, V.; Ly, S.; et al. Broad and long-lasting immune protection against various Chikungunya genotypes demonstrated by participants in a cross-sectional study in a Cambodian rural community. Emerg. Microbes Infect. 2018, 7, 13. [Google Scholar] [CrossRef]
- Powers, A.M. Licensed chikungunya virus vaccine: A possibility? Lancet 2018, 392, 2660–2661. [Google Scholar] [CrossRef]
- Langsjoen, R.M.; Haller, S.L.; Roy, C.J.; Vinet-Oliphant, H.; Bergren, N.A.; Erasmus, J.H.; Livengood, J.A.; Powell, T.D.; Weaver, S.C.; Rossi, S.L. Chikungunya Virus Strains Show Lineage-Specific Variations in Virulence and Cross-Protective Ability in Murine and Nonhuman Primate Models. mBio 2018, 9, e02449-17. [Google Scholar] [CrossRef]
- Partidos, C.D.; Paykel, J.; Weger, J.; Borland, E.M.; Powers, A.M.; Seymour, R.; Weaver, S.C.; Stinchcomb, D.T.; Osorio, J.E. Cross-protective immunity against O’nyong’nyong virus afforded by a novel recombinant chikungunya vaccine. Vaccine 2012, 30, 4638–4643. [Google Scholar] [CrossRef]
- Robinson, D.M.; Cole, F.E.; McManus, A.T.; Pedersen, C.E. Inactivated Mayaro vaccine produced in human diploid cell cultures. Mil. Med. 1976, 141, 163–166. [Google Scholar] [CrossRef]
- Weise, W.J.; Hermance, M.E.; Forrester, N.; Adams, A.P.; Langsjoen, R.; Gorchakov, R.; Wang, E.; Alcorn, M.D.H.; Tsetsarkin, K.; Weaver, S.C. A novel live-attenuated vaccine candidate for mayaro Fever. PLoS Negl. Trop. Dis. 2014, 8, e2969. [Google Scholar] [CrossRef]
- Choi, H.; Kudchodkar, S.B.; Reuschel, E.L.; Asija, K.; Borole, P.; Ho, M.; Wojtak, K.; Reed, C.; Ramos, S.; Bopp, N.E.; et al. Protective immunity by an engineered DNA vaccine for Mayaro virus. PLoS Negl. Trop. Dis. 2019, 13, e0007042. [Google Scholar] [CrossRef]
- Yu, S.; Aaskov, J.G. Development of a candidate vaccine against Ross River virus infection. Vaccine 1994, 12, 1118–1124. [Google Scholar] [CrossRef]
- Aaskov, J.; Williams, L.; Yu, S. A candidate Ross River virus vaccine: Preclinical evaluation. Vaccine 1997, 15, 1396–1404. [Google Scholar] [CrossRef]
- Kistner, O.; Barrett, N.; Brühmann, A.; Reiter, M.; Mundt, W.; Savidis-Dacho, H.; Schober-Bendixen, S.; Dorner, F.; Aaskov, J. The preclinical testing of a formaldehyde inactivated Ross River virus vaccine designed for use in humans. Vaccine 2007, 25, 4845–4852. [Google Scholar] [CrossRef]
- Holzer, G.W.; Coulibaly, S.; Aichinger, G.; Savidis-Dacho, H.; Mayrhofer, J.; Brunner, S.; Schmid, K.; Kistner, O.; Aaskov, J.G.; Falkner, F.G.; et al. Evaluation of an inactivated Ross River virus vaccine in active and passive mouse immunization models and establishment of a correlate of protection. Vaccine 2011, 29, 4132–4141. [Google Scholar] [CrossRef]
- Aichinger, G.; Ehrlich, H.J.; Aaskov, J.G.; Fritsch, S.; Thomasser, C.; Draxler, W.; Wolzt, M.; Müller, M.; Pinl, F.; Van Damme, P.; et al. Safety and immunogenicity of an inactivated whole virus Vero cell-derived Ross River virus vaccine: A randomized trial. Vaccine 2011, 29, 9376–9384. [Google Scholar] [CrossRef]
- Wressnigg, N.; van der Velden, M.V.W.; Portsmouth, D.; Draxler, W.; O’Rourke, M.; Richmond, P.; Hall, S.; McBride, W.J.H.; Redfern, A.; Aaskov, J.; et al. An Inactivated Ross River Virus Vaccine Is Well Tolerated and Immunogenic in an Adult Population in a Randomized Phase 3 Trial. Clin. Vaccine Immunol. 2015, 22, 267–273. [Google Scholar] [CrossRef]
- Rezza, G.; Weaver, S.C. Chikungunya as a paradigm for emerging viral diseases: Evaluating disease impact and hurdles to vaccine development. PLoS Negl. Trop. Dis. 2019, 13, e0006919. [Google Scholar] [CrossRef]
- Suhrbier, A.; La Linn, M. Clinical and pathologic aspects of arthritis due to Ross River virus and other alphaviruses. Curr. Opin. Rheumatol. 2004, 16, 374–379. [Google Scholar] [CrossRef]
- Padmakumar, B.; Jayan, J.B.; Menon, R.M.; Krishnankutty, B.; Payippallil, R.; Nisha, R. Comparative evaluation of four therapeutic regimes in chikungunya arthritis: A prospective randomized parallel-group study. Indian J. Rheumatol. 2009, 4, 94–101. [Google Scholar] [CrossRef]
- Wolf, S.; Taylor, A.; Zaid, A.; Freitas, J.; Herrero, L.J.; Rao, S.; Suhrbier, A.; Forwood, M.R.; Bucala, R.; Mahalingam, S. Inhibition of IL-1β signaling by anakinra shows a critical role for bone loss in experimental arthritogenic alphavirus infections. Arthritis Rheumatol. 2019. [Google Scholar] [CrossRef]
- Chen, W.; Foo, S.-S.; Taylor, A.; Lulla, A.; Merits, A.; Hueston, L.; Forwood, M.R.; Walsh, N.C.; Sims, N.A.; Herrero, L.J.; et al. Bindarit, an Inhibitor of Monocyte Chemotactic Protein Synthesis, Protects against Bone Loss Induced by Chikungunya Virus Infection. J. Virol. 2015, 89, 581–593. [Google Scholar] [CrossRef]
- Rulli, N.E.; Guglielmotti, A.; Mangano, G.; Rolph, M.S.; Apicella, C.; Zaid, A.; Suhrbier, A.; Mahalingam, S. Amelioration of alphavirus-induced arthritis and myositis in a mouse model by treatment with bindarit, an inhibitor of monocyte chemotactic proteins. Arthritis Rheum. 2009, 60, 2513–2523. [Google Scholar] [CrossRef]
- Ching, K.-C.; Kam, Y.-W.; Merits, A.; Ng, L.F.P.; Chai, C.L.L. Trisubstituted Thieno[3,2-b]pyrrole 5-Carboxamides as Potent Inhibitors of Alphaviruses. J. Med. Chem. 2015, 58, 9196–9213. [Google Scholar] [CrossRef]
- Byler, K.G.; Collins, J.T.; Ogungbe, I.V.; Setzer, W.N. Alphavirus protease inhibitors from natural sources: A homology modeling and molecular docking investigation. Comput. Biol. Chem. 2016, 64, 163–184. [Google Scholar] [CrossRef]
- Gall, B.; Pryke, K.; Abraham, J.; Mizuno, N.; Botto, S.; Sali, T.M.; Broeckel, R.; Haese, N.; Nilsen, A.; Placzek, A.; et al. Emerging Alphaviruses Are Sensitive to Cellular States Induced by a Novel Small-Molecule Agonist of the STING Pathway. J. Virol. 2018, 92, e01913-17. [Google Scholar] [CrossRef]
- Neris, R.L.S.; Figueiredo, C.M.; Higa, L.M.; Araujo, D.F.; Carvalho, C.A.M.; Verçoza, B.R.F.; Silva, M.O.L.; Carneiro, F.A.; Tanuri, A.; Gomes, A.M.O.; et al. Co-protoporphyrin IX and Sn-protoporphyrin IX inactivate Zika, Chikungunya and other arboviruses by targeting the viral envelope. Sci. Rep. 2018, 8, 9805. [Google Scholar] [CrossRef]
- Bhat, S.M.; Mudgal, P.P.; N, S.; Arunkumar, G. Spectrum of candidate molecules against Chikungunya virus—An insight into the antiviral screening platforms. Expert Rev. Anti-Infect. Ther. 2019, 17, 1–22. [Google Scholar] [CrossRef]
- De Lamballerie, X.; Boisson, V.; Reynier, J.-C.; Enault, S.; Charrel, R.N.; Flahault, A.; Roques, P.; Le Grand, R. On chikungunya acute infection and chloroquine treatment. Vector Borne Zoonotic Dis. 2008, 8, 837–839. [Google Scholar] [CrossRef]
- Roques, P.; Thiberville, S.-D.; Dupuis-Maguiraga, L.; Lum, F.-M.; Labadie, K.; Martinon, F.; Gras, G.; Lebon, P.; Ng, L.F.P.; de Lamballerie, X.; et al. Paradoxical Effect of Chloroquine Treatment in Enhancing Chikungunya Virus Infection. Viruses 2018, 10, 268. [Google Scholar] [CrossRef]
- Ravichandran, R.; Manian, M. Ribavirin therapy for Chikungunya arthritis. J. Infect. Dev. Ctries. 2008, 2, 140–142. [Google Scholar] [CrossRef]
- Herrero, L.J.; Foo, S.-S.; Sheng, K.-C.; Chen, W.; Forwood, M.R.; Bucala, R.; Mahalingam, S. Pentosan Polysulfate: A Novel Glycosaminoglycan-Like Molecule for Effective Treatment of Alphavirus-Induced Cartilage Destruction and Inflammatory Disease. J. Virol. 2015, 89, 8063–8076. [Google Scholar] [CrossRef]
- Couderc, T.; Khandoudi, N.; Grandadam, M.; Visse, C.; Gangneux, N.; Bagot, S.; Prost, J.-F.; Lecuit, M. Prophylaxis and therapy for Chikungunya virus infection. J. Infect. Dis. 2009, 200, 516–523. [Google Scholar] [CrossRef]
- Prevention of Chikungunya Infection in Neonates: Clinical Evaluation of Anti-CHIKV Hyperimmune Intravenous Immunoglobulins—ICH GCP—Clinical Trials Registry. Available online: https://clinicaltrials.gov/ct2/show/NCT02230163 (accessed on 4 April 2019).
- Rezza, G.; Chen, R.; Weaver, S.C. O’nyong’nyong fever: A neglected mosquito-borne viral disease. Pathog. Glob. Health 2017, 111, 271–275. [Google Scholar] [CrossRef]
- Mackay, I.M.; Arden, K.E. Mayaro virus: A forest virus primed for a trip to the city? Microbes Infect. 2016, 18, 724–734. [Google Scholar] [CrossRef]
- Esposito, D.L.A.; Fonseca, B.A.L. da Will Mayaro virus be responsible for the next outbreak of an arthropod-borne virus in Brazil? Braz. J. Infect. Dis. 2017, 21, 540–544. [Google Scholar] [CrossRef]
- Liu, X.; Tharmarajah, K.; Taylor, A. Ross River virus disease clinical presentation, pathogenesis and current therapeutic strategies. Microbes Infect. 2017, 19, 496–504. [Google Scholar] [CrossRef]
- Walter Reed Biosystematics Unit. Available online: http://www.wrbu.org/index.html (accessed on 5 April 2019).
- Walsh, M.G.; Webb, C. Hydrological features and the ecological niches of mammalian hosts delineate elevated risk for Ross River virus epidemics in anthropogenic landscapes in Australia. Parasit. Vectors 2018, 11, 192. [Google Scholar] [CrossRef]
- Mackenzie, J.S.; Lindsay, M.D.A.; Smith, D.W.; Imrie, A. The ecology and epidemiology of Ross River and Murray Valley encephalitis viruses in Western Australia: Examples of One Health in Action. Trans. R. Soc. Trop. Med. Hyg. 2017, 111, 248–254. [Google Scholar] [CrossRef]
- Koolhof, I.S.; Bettiol, S.; Carver, S. Fine-temporal forecasting of outbreak probability and severity: Ross River virus in Western Australia. Epidemiol. Infect. 2017, 145, 2949–2960. [Google Scholar] [CrossRef]
- Shocket, M.S.; Ryan, S.J.; Mordecai, E.A. Temperature explains broad patterns of Ross River virus transmission. eLife 2018, 7, e37762. [Google Scholar] [CrossRef]
- Lorenz, C.; Azevedo, T.S.; Virginio, F.; Aguiar, B.S.; Chiaravalloti-Neto, F.; Suesdek, L. Impact of environmental factors on neglected emerging arboviral diseases. PLoS Negl. Trop. Dis. 2017, 11, e0005959. [Google Scholar] [CrossRef]
- Manrubia, S.C.; Escarmís, C.; Domingo, E.; Lázaro, E. High mutation rates, bottlenecks, and robustness of RNA viral quasispecies. Gene 2005, 347, 273–282. [Google Scholar] [CrossRef]
- Stapleford, K.A.; Moratorio, G.; Henningsson, R.; Chen, R.; Matheus, S.; Enfissi, A.; Weissglas-Volkov, D.; Isakov, O.; Blanc, H.; Mounce, B.C.; et al. Whole-Genome Sequencing Analysis from the Chikungunya Virus Caribbean Outbreak Reveals Novel Evolutionary Genomic Elements. PLoS Negl. Trop. Dis. 2016, 10, e0004402. [Google Scholar] [CrossRef]
- Zhang, R.; Kim, A.S.; Fox, J.M.; Nair, S.; Basore, K.; Klimstra, W.B.; Rimkunas, R.; Fong, R.H.; Lin, H.; Poddar, S.; et al. Mxra8 is a receptor for multiple arthritogenic alphaviruses. Nature 2018, 557, 570–574. [Google Scholar] [CrossRef]
- Bessaud, M.; Peyrefitte, C.N.; Pastorino, B.A.M.; Gravier, P.; Tock, F.; Boete, F.; Tolou, H.J.; Grandadam, M. O’nyong’nyong Virus, Chad. Emerg. Infect. Dis. 2006, 12, 1248–1250. [Google Scholar] [CrossRef]
- Zuchi, N.; Heinen, L.B.D.S.; Santos, M.A.M.D.; Pereira, F.C.; Slhessarenko, R.D. Molecular detection of Mayaro virus during a dengue outbreak in the state of Mato Grosso, Central-West Brazil. Mem. Inst. Oswaldo Cruz 2014, 109, 820–823. [Google Scholar] [CrossRef]
- De Souza Costa, M.C.; Siqueira Maia, L.M.; Costa de Souza, V.; Gonzaga, A.M.; Correa de Azevedo, V.; Ramos Martins, L.; Chavez Pavoni, J.H.; Gomes Naveca, F.; Dezengrini Slhessarenko, R. Arbovirus investigation in patients from Mato Grosso during Zika and Chikungunya virus introdution in Brazil, 2015-2016. Acta Trop. 2019, 190, 395–402. [Google Scholar] [CrossRef]
- Liu, J.; Ochieng, C.; Wiersma, S.; Ströher, U.; Towner, J.S.; Whitmer, S.; Nichol, S.T.; Moore, C.C.; Kersh, G.J.; Kato, C.; et al. Development of a TaqMan Array Card for Acute-Febrile-Illness Outbreak Investigation and Surveillance of Emerging Pathogens, Including Ebola Virus. J. Clin. Microbiol. 2016, 54, 49–58. [Google Scholar] [CrossRef]
- Smith, D.R.; Lee, J.S.; Jahrling, J.; Kulesh, D.A.; Turell, M.J.; Groebner, J.L.; O’Guinn, M.L. Development of field-based real-time reverse transcription-polymerase chain reaction assays for detection of Chikungunya and O’nyong’nyong viruses in mosquitoes. Am. J. Trop. Med. Hyg. 2009, 81, 679–684. [Google Scholar] [CrossRef]
- Inglis, T.J.J.; Bradbury, R.S.; McInnes, R.L.; Frances, S.P.; Merritt, A.J.; Levy, A.; Nicholson, J.; Neville, P.J.; Lindsay, M.; Smith, D.W. Deployable Molecular Detection of Arboviruses in the Australian Outback. Am. J. Trop. Med. Hyg. 2016, 95, 633–638. [Google Scholar] [CrossRef]
- Batovska, J.; Lynch, S.E.; Rodoni, B.C.; Sawbridge, T.I.; Cogan, N.O. Metagenomic arbovirus detection using MinION nanopore sequencing. J. Virol. Methods 2017, 249, 79–84. [Google Scholar] [CrossRef]
- Calisher, C.H.; el-Kafrawi, A.O.; Al-Deen Mahmud, M.I.; Travassos da Rosa, A.P.; Bartz, C.R.; Brummer-Korvenkontio, M.; Haksohusodo, S.; Suharyono, W. Complex-specific immunoglobulin M antibody patterns in humans infected with alphaviruses. J. Clin. Microbiol. 1986, 23, 155–159. [Google Scholar]
- Xiao, Z.S.; Jia, L.L.; Qu, X.S.; Zhang, Y.H. Application of enzyme immunoassay on infected cells (EIA-IC) for arboviruses. Acta Virol. 1986, 30, 487–493. [Google Scholar]
- Greiser-Wilke, I.M.; Moennig, V.; Kaaden, O.R.; Shope, R.E. Detection of alphaviruses in a genus-specific antigen capture enzyme immunoassay using monoclonal antibodies. J. Clin. Microbiol. 1991, 29, 131–137. [Google Scholar]
- Kumar, J.S.; Parida, M.; Lakshmana Rao, P.V. Development & evaluation of biotinylated DNA probe for clinical diagnosis of chikungunya infection in patients’ acute phase serum & CSF samples. Indian J. Med. Res. 2013, 138, 117–124. [Google Scholar]
- Tuekprakhon, A.; Puiprom, O.; Sasaki, T.; Michiels, J.; Bartholomeeusen, K.; Nakayama, E.E.; Meno, M.K.; Phadungsombat, J.; Huits, R.; Ariën, K.K.; et al. Broad-spectrum monoclonal antibodies against chikungunya virus structural proteins: Promising candidates for antibody-based rapid diagnostic test development. PLoS ONE 2018, 13, e0208851. [Google Scholar] [CrossRef]
- Fox, J.M.; Long, F.; Edeling, M.A.; Lin, H.; van Duijl-Richter, M.K.S.; Fong, R.H.; Kahle, K.M.; Smit, J.M.; Jin, J.; Simmons, G.; et al. Broadly Neutralizing Alphavirus Antibodies Bind an Epitope on E2 and Inhibit Entry and Egress. Cell 2015, 163, 1095–1107. [Google Scholar] [CrossRef]
Figure 1.
Timeline after arthritogenic alphavirus infection. After infection by a bite from an infected mosquito, an incubation period of 3–8 days takes place. Viremia starts before the onset of symptoms and lasts only a few days, leaving a very short window for direct diagnosis by RT-PCR or virus isolation. If the infection is symptomatic (>60% of cases), the patient presents with brutal onset of fever associated with polyarthralgia and other general symptoms, and after a few days, a delayed rash often appears. Lymphadenopathy is particularly frequent in ONNV infection. General blood tests during the acute phase can show lymphopenia, thrombopenia, hypocalcemia and mild rhabdomyolysis (with cytolysis and increased creatinine kinase). Polyarthralgia with or without arthritis and asthenia might be prolonged during the sub-acute phase (2 weeks to 3 months) or as chronic symptoms, sometimes as post-infectious chronic inflammatory rheumatism mimicking rheumatoid arthritis. Indirect diagnosis by serology requires two blood samples separated by at least 12 days to show appearance and/or disappearance of IgM (that may stay positive for over 6 months) and appearance of IgG.
Figure 1.
Timeline after arthritogenic alphavirus infection. After infection by a bite from an infected mosquito, an incubation period of 3–8 days takes place. Viremia starts before the onset of symptoms and lasts only a few days, leaving a very short window for direct diagnosis by RT-PCR or virus isolation. If the infection is symptomatic (>60% of cases), the patient presents with brutal onset of fever associated with polyarthralgia and other general symptoms, and after a few days, a delayed rash often appears. Lymphadenopathy is particularly frequent in ONNV infection. General blood tests during the acute phase can show lymphopenia, thrombopenia, hypocalcemia and mild rhabdomyolysis (with cytolysis and increased creatinine kinase). Polyarthralgia with or without arthritis and asthenia might be prolonged during the sub-acute phase (2 weeks to 3 months) or as chronic symptoms, sometimes as post-infectious chronic inflammatory rheumatism mimicking rheumatoid arthritis. Indirect diagnosis by serology requires two blood samples separated by at least 12 days to show appearance and/or disappearance of IgM (that may stay positive for over 6 months) and appearance of IgG.

Figure 2.
Number of publications for each virus reported in PubMed through the years. CHIKV publications were rare before 2006 (under 10 per year), except during the South-East Asia epidemic in the late 1960s, when it reached around 20 publications per year. Since the La Reunion outbreak, and followed by the Caribbean epidemic, attention has increased tremendously, and publications now number around 500 per year. While Ross River virus has 10–20 publications a year since 1979, MAYV and ONNV had less than 10 publications a year until 2015, and only MAYV has slightly exceeded this number since then.
Figure 2.
Number of publications for each virus reported in PubMed through the years. CHIKV publications were rare before 2006 (under 10 per year), except during the South-East Asia epidemic in the late 1960s, when it reached around 20 publications per year. Since the La Reunion outbreak, and followed by the Caribbean epidemic, attention has increased tremendously, and publications now number around 500 per year. While Ross River virus has 10–20 publications a year since 1979, MAYV and ONNV had less than 10 publications a year until 2015, and only MAYV has slightly exceeded this number since then.


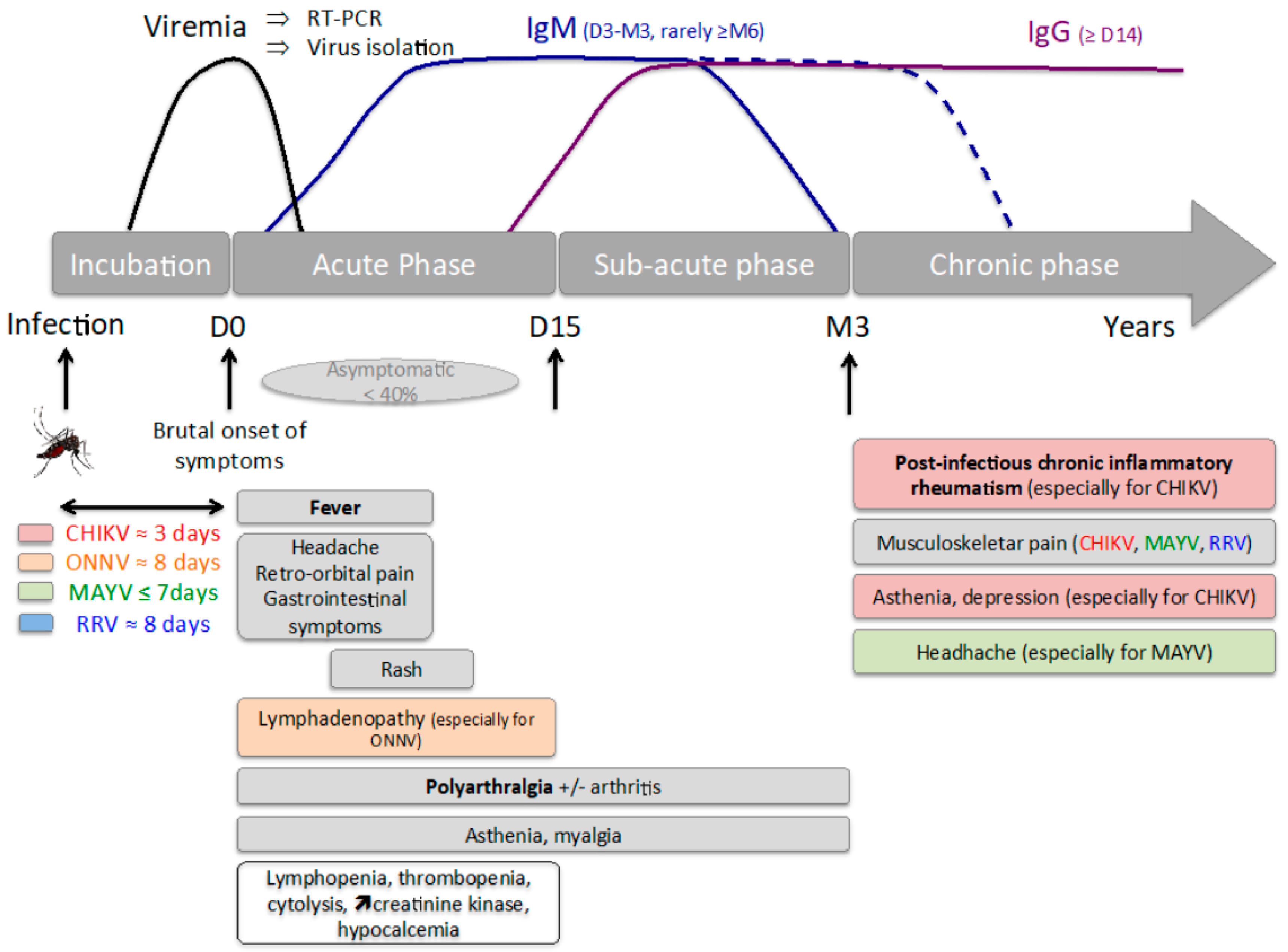{kind=link}
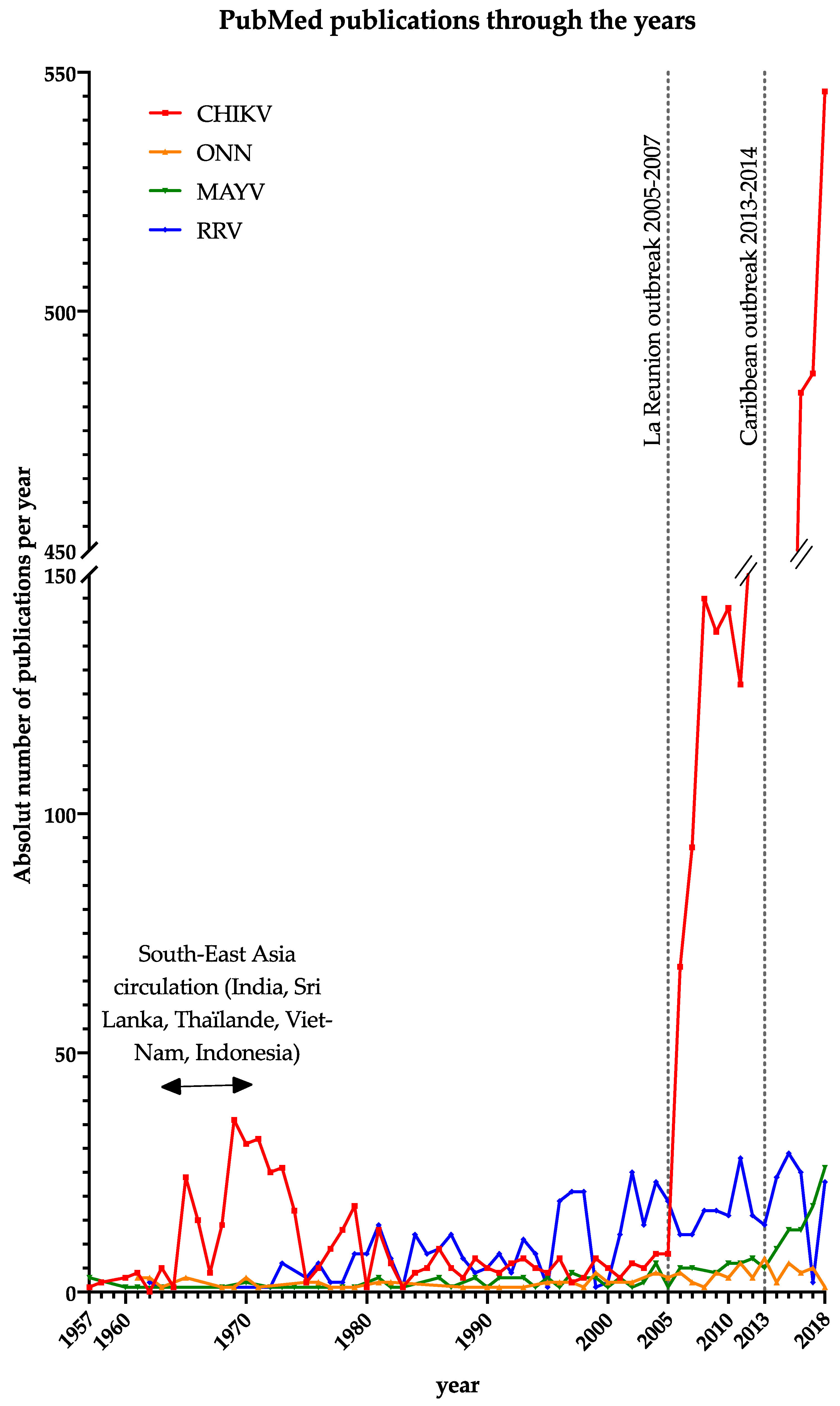{kind=link}
Table 1.
Arthritogenic alphavirus general characteristics. CHIKV, chikungunya virus; ONNV, O’nyong’nyong virus; MAYV, Mayaro virus; RRV, Ross River virus.
Table 1.
Arthritogenic alphavirus general characteristics. CHIKV, chikungunya virus; ONNV, O’nyong’nyong virus; MAYV, Mayaro virus; RRV, Ross River virus.
| CHIKV | ONNV | MAYV | RRV | |
|---|---|---|---|---|
| Other Name | Uruma virus | Igbo-Ora virus | Epidemic polyarthritis | |
| Location of circulation | Endemic: Africa, Asia (South-East and India), Pacific Islands, Central and South America. Sporadically: Mediterranean Europe, USA | Sub-Saharan Africa | Central and South America | Australia, South Pacific Island, Papua New Guinea |
| Cycle | Enzootic cycle and urban cycle during epidemic | Enzootic cycle and urban cycle during epidemic | Enzootic cycle | Enzootic cycle and urban cycle during epidemic |
| Vertebrate host | Non-human primate | Mostly unknown (possibly forest buffalo, monkeys, duikers) | Non-human primate | Marsupials mainly, horses, cattle |
| Invertebrate vector | Aedes sp. (enzootic cycle: africanus, furcifer-taylori, luteocephalus, dalzieli; urban cycle: aegypti and albopictus) | Anopheles funestus and more rarely Anopheles gambiae | Haemagogus sp., Mansonia sp., and Psophora sp. [5,6] | Aedes vigilax and Culex annulirostris mainly, Aedes notoscriptus, Aedes funereus, Aedes camptorhynchus, Ochlerotatus camptorhynchus |
Table 2.
Arthritogenic alphavirus acute infection symptoms, range of frequency reported in the listed studies.
Table 2.
Arthritogenic alphavirus acute infection symptoms, range of frequency reported in the listed studies.
| CHIKV Median | Min | Max | ONNV Median | Min | Max | MAYV Median | Min | Max | RRV Median | Min | Max | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| % of symptomatic cases | 18–97 [30,117,118,119,121] | 64–86 [42,122,123,124] | 64–80 [48,56] | 25–76 [73,125,126,127] | ||||||||
| Incubation time | 2,5 days (2–12) | Approximately 8 days | <7 days | 8 days (3–21) | ||||||||
| Symptoms | ||||||||||||
| Arthralgia | 95 | 69 | 100 | 79 | 58 | 100 | 86 | 50 | 100 | 94.35 | 83 | 98 |
| Joint Stiffness | 93 | 93 | 93 | 84.9 | 78.8 | 89 | ||||||
| Fever | 94 | 83 | 100 | 90 | 72 | 100 | 100 | 100 | 100 | 54.4 | 49 | 60 |
| Asthenia | 77.5 | 49 | 91 | 87 | 42 | 100 | 92.3 | 91.3 | 93.3 | |||
| Anorexia | 70 | 30 | 86 | 48.5 | 22 | 75 | ||||||
| Myalgia | 59 | 24 | 85 | 71 | 71 | 71 | 78.5 | 49 | 100 | 61.25 | 45 | 66.7 |
| Headache | 57.5 | 8 | 80 | 84.5 | 74 | 95 | 87 | 57 | 100 | 51 | 50.9 | 60 |
| Gastrointestinal Symptom | 55 | 10 | 63 | |||||||||
| Post Orbital Pain | 49.5 | 14 | 85 | 60 | 60 | 60 | 60 | 39 | 100 | |||
| Skin Rash | 49 | 14 | 68 | 77 | 65 | 84 | 50 | 24 | 93 | 58.25 | 57 | 59.5 |
| Nausea | 44 | 26 | 69 | 42.5 | 18 | 69 | 25.3 | 24.6 | 26 | |||
| Pruritus | 30.5 | 14 | 50 | 87 | 87 | 87 | 33 | 20 | 40 | |||
| Swollen Joints | 40 | 26 | 100 | 58 | 23 | 93 | 52.15 | 38 | 64.7 | |||
| Vomiting | 35 | 19 | 43 | 17.5 | 4 | 100 | ||||||
| Diarrhea | 22.5 | 4 | 38 | 9 | 5 | 60 | ||||||
| Conjunctival Hyperemia | 18.5 | 3 | 33 | 51 | 51 | 51 | ||||||
| Abdominal Pain | 17 | 13 | 32 | 50 | 14 | 80 | ||||||
| Lymphadenopathy | 9 | 3 | 100 | 46 | 46 | 46 | 17 | 13 | 53 | 10 | 10 | 10 |
| Number of study/total number of patients [references] | 18/4502 [21,25,32,117,128,129,130,131,132,133,134,135,136,137,138,139,140] | 3/891 [44,122,141] | 9/179 [47,49,50,51,56,142,143,144,145] | 5/626 [125,146,147,148,149] | ||||||||
| Severe forms | Meningo-encephalopathy [150,151], Guillain-Barré syndrome [152], acute optic neuropathy [153], Myo-pericarditis [150,154,155], shock [150], neonatal infection [156,157] | unknown | unknown | Glomerulonephritis [158], encephalitis [159,160,161] | ||||||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Levi, L.I.; Vignuzzi, M. Arthritogenic Alphaviruses: A Worldwide Emerging Threat? Microorganisms 2019, 7, 133. https://doi.org/10.3390/microorganisms7050133
AMA Style
Levi LI, Vignuzzi M. Arthritogenic Alphaviruses: A Worldwide Emerging Threat? Microorganisms. 2019; 7(5):133. https://doi.org/10.3390/microorganisms7050133
Chicago/Turabian StyleLevi, Laura I., and Marco Vignuzzi. 2019. "Arthritogenic Alphaviruses: A Worldwide Emerging Threat?" Microorganisms 7, no. 5: 133. https://doi.org/10.3390/microorganisms7050133
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.