
Microbiota Transplantation in an Antibiotic-Induced Bacterial Depletion Mouse Model: Reproducible Establishment, Analysis, and Application

Abstract
:1. Introduction
2. The Development and Overview of the Procedure
3. Protocol
3.1. Materials
- (1)
- Phosphate-buffered saline (PBS), sterile.
- (2)
- Sample storage buffer: Glycerin in PBS = 1:1 (v/v), sterilization (see Note 1).
- (3)
- Placebo: Glycerin in PBS = 1:4 (v/v), sterilization (see Note 2).
- (4)
- Broad-spectrum antibiotic mix: 500 mg/L of vancomycin, 1 g/L of ampicillin, and 1 g/L of neomycin (see Note 3).
- (5)
- A 40 μm cell strainer.
- (6)
- Lavage needle, size 9 (Table 1) (see Note 4).
- (7)
- A total of 2 mL of cryotubes, round bottom (see Note 5).
- (8)
- A 1 mL syringe (see Note 6).
- (9)
- Cage, tweezers, cryotubes, and all other appliances and reagents need to be sterilized before use.
3.2. Procedure
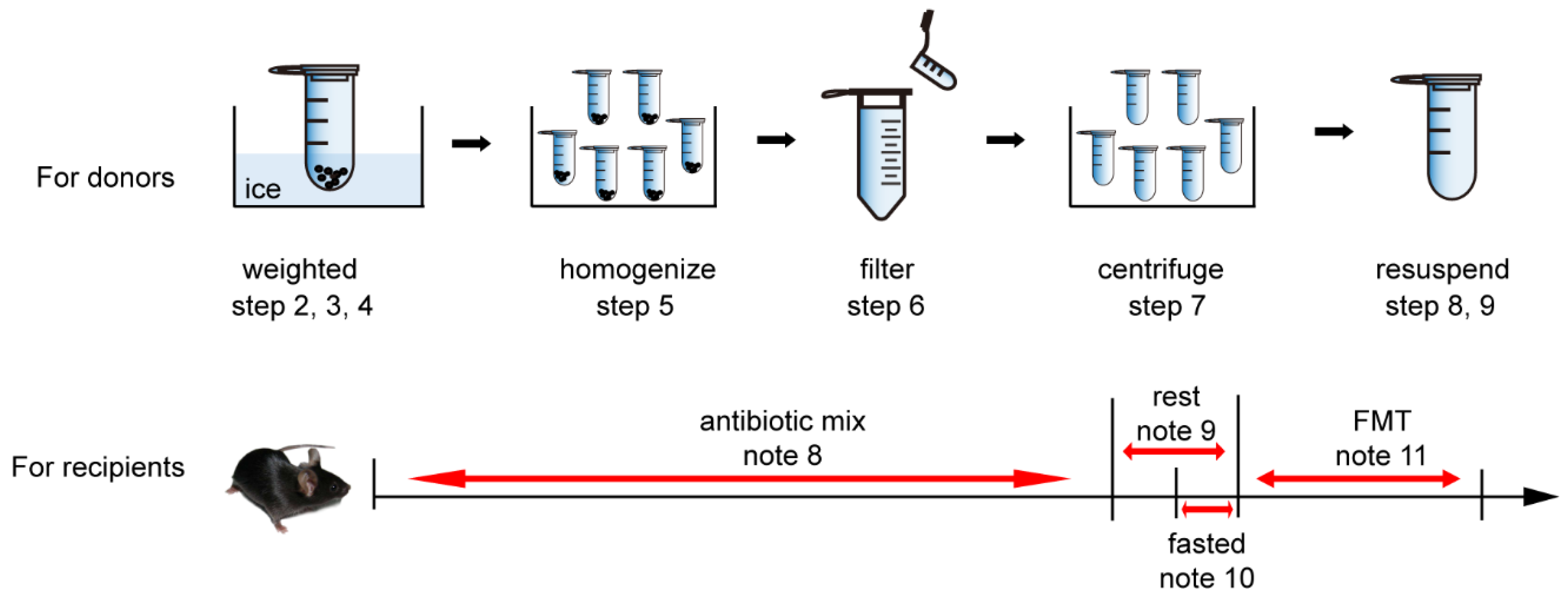
3.2.1. Donors
- (1)
- All the donors are raised in separate cages. Place all the regents and buffers on ice.
- (2)
- Weigh the dry, empty 2 mL cryotubes.
- (3)
- Collect fresh feces in cryotubes and weigh (see Note 7).
- (4)
- Add an appropriate amount of pre-cooled sterile PBS (V1) to produce a feces concentration of 50–100 mg/mL. Reach as close to the upper limit as possible.
- (5)
- Homogenize the solution at 4 °C.
- (6)
- Filter the solution through a 40 μm filter and collect the supernatant in a new tube.
- (7)
- Centrifuge at 8000× g for 5 min at 4 °C.
- (8)
- Discard the supernatant without disturbing the sediment.
- (9)
- Transplantation solution: Resuspend the pellet obtained from the steps above in cold PBS (the original volume, V1), and add an equal volume of sample storage buffer (see Note 1).
- (10)
- If not used immediately, freeze in liquid nitrogen and store at −80 °C.
3.2.2. Recipients
- (1)
- Administer to the recipients the broad-spectrum antibiotic mix instead of drinking water for at least 14 days (see Note 8), and allow to “rest” for 1–2 days (see Note 9).
- (2)
- Before intragastric administration, fast all recipients but allow them to drink freely for 1 day (see Note 10).
- (3)
- Intragastrically administer each recipient with 200–300 μL (see Note 6) of transplantation solution once a day for 5 consecutive days (Table 2) (see Note 11).
4. Notes
- (1)
- When the concentration of glycerol in the sample storage buffer is 50%, add the sample storage buffer to the resuspended solution at a ratio of 1:1 to prepare the transplantation solution and obtain a final glycerol concentration of 25%. The final concentration glycerol can be adjusted within the range of 10–30% according to different experimental purposes and conditions.
- (2)
- Use a placebo as a control for the transplantation solution. The final glycerol concentration in the placebo should be equal to that of the transplantation solution.
- (3)
- (4)
- (5)
- Compared to a tapered-bottom tube, using a round-bottom tube can achieve better homogenization effects.
- (6)
- A 1 mL syringe is suitable for commonly used 6-to-8-week-old mice (25–30 g). If using other target animals, refer to Table 2.The volume received by each recipient (200–300 μL) is calculated for approximately 10–20 mg feces/mouse. Generally, the ideal effect can be obtained from a feces concentration of 50–100 mg/mL in 200 μL of transplantation solution. To determine the optimum conditions for a particular model, a pilot experiment is required.
- (7)
- Generally, each mouse can provide 50–100 mg of fresh feces (6-to-8-week-old mice, 25–30 g). However, if the donors are enteritis-mouse models, there will be less feces. Therefore, the stool from mice of matched weight and sex can be mixed depending on the experimental design. The number of animals used can be customized to the experiment.
- (8)
- The duration of the broad-spectrum antibiotic mix treatment of mice can be customized, but, generally, it lasts for at least 14 days.
- (9)
- (10)
- Fasting should be started for at least 4–8 h before gavage to avoid the gastric contents hindering gavage injection and affecting the drug absorption rate.
- (11)
- The transplanting of recipients once a day for 5 consecutive days is suitable for commonly used 6-to-8-week-old mice (25–30 g). To determine the optimum conditions for a particular model, a pilot experiment is required.For the solutions to other common problems, see Table 3.
5. Microbiological Analyses
5.1. The Detection of Donors
5.2. The Detection of the Transplantation Solution
5.3. The Detection of the Recipients
5.3.1. Baseline
5.3.2. After FMT
6. Application
6.1. Healthy Individuals as Donors
6.2. Disease Models as Donors
6.3. Customized Microbiota as Donors
6.4. A Combination of the above Donors
7. Conclusions and Perspectives
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Ley, R.E.; Hamady, M.; Lozupone, C.; Turnbaugh, P.J.; Ramey, R.R.; Bircher, J.S.; Schlegel, M.L.; Tucker, T.A.; Schrenzel, M.D.; Knight, R.; et al. Evolution of mammals and their gut microbes. Science 2008, 320, 1647–1651. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pedersen, H.K.; Gudmundsdottir, V.; Nielsen, H.B.; Hyotylainen, T.; Nielsen, T.; Jensen, B.A.; Forslund, K.; Hildebrand, F.; Prifti, E.; Falony, G.; et al. Human gut microbes impact host serum metabolome and insulin sensitivity. Nature 2016, 535, 376–381. [Google Scholar] [CrossRef] [PubMed]
- Le Chatelier, E.; Nielsen, T.; Qin, J.; Prifti, E.; Hildebrand, F.; Falony, G.; Almeida, M.; Arumugam, M.; Batto, J.M.; Kennedy, S.; et al. Richness of human gut microbiome correlates with metabolic markers. Nature 2013, 500, 541–546. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, F.; Tremaroli, V.; Nielsen, J.; Bäckhed, F. Assessing the human gut microbiota in metabolic diseases. Diabetes 2013, 62, 3341–3349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sender, R.; Fuchs, S.; Milo, R. Revised Estimates for the Number of Human and Bacteria Cells in the Body. PLoS Biol. 2016, 14, e1002533. [Google Scholar] [CrossRef] [Green Version]
- Turnbaugh, P.J.; Hamady, M.; Yatsunenko, T.; Cantarel, B.L.; Duncan, A.; Ley, R.E.; Sogin, M.L.; Jones, W.J.; Roe, B.A.; Affourtit, J.P.; et al. A core gut microbiome in obese and lean twins. Nature 2009, 457, 480–484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dominguez-Bello, M.G.; Godoy-Vitorino, F.; Knight, R.; Blaser, M.J. Role of the microbiome in human development. Gut 2019, 68, 1108–1114. [Google Scholar] [CrossRef]
- Leshem, A.; Liwinski, T.; Elinav, E. Immune-Microbiota Interplay and Colonization Resistance in Infection. Mol. Cell 2020, 78, 597–613. [Google Scholar] [CrossRef]
- Kabouridis, P.S.; Lasrado, R.; McCallum, S.; Chng, S.H.; Snippert, H.J.; Clevers, H.; Pettersson, S.; Pachnis, V. The gut microbiota keeps enteric glial cells on the move; prospective roles of the gut epithelium and immune system. Gut Microbes 2016, 6, 398–403. [Google Scholar] [CrossRef] [Green Version]
- Agirman, G.; Hsiao, E.Y. SnapShot: The microbiota-gut-brain axis. Cell 2021, 184, 2524. [Google Scholar] [CrossRef]
- Meroni, E.; Stakenborg, N.; Viola, M.F.; Boeckxstaens, G.E. Intestinal macrophages and their interaction with the enteric nervous system in health and inflammatory bowel disease. Acta Physiol. 2018, 225, e13163. [Google Scholar] [CrossRef]
- Wargo, J.A. Modulating gut microbes. Science 2020, 369, 1302–1303. [Google Scholar] [CrossRef]
- Gupta, A.; Khanna, S. Fecal Microbiota Transplantation. JAMA 2017, 318, 102. [Google Scholar] [CrossRef] [PubMed]
- Burrello, C.; Giuffrè, M.R.; Macandog, A.D.; Diaz-Basabe, A.; Cribiù, F.M.; Lopez, G.; Borgo, F.; Nezi, L.; Caprioli, F.; Vecchi, M.; et al. Fecal Microbiota Transplantation Controls Murine Chronic Intestinal Inflammation by Modulating Immune Cell Functions and Gut Microbiota Composition. Cells 2019, 8, 517. [Google Scholar] [CrossRef] [Green Version]
- Sun, J.; Xu, J.; Ling, Y.; Wang, F.; Liu, J. Fecal microbiota transplantation alleviated Alzheimer’s disease-like pathogenesis in APP/PS1 transgenic mice. Transl. Psychiatry 2019, 9, 189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhan, G.; Yang, N.; Li, S.; Huang, N.; Luo, A. Abnormal gut microbiota composition contributes to cognitive dysfunction in SAMP8 mice. Aging 2018, 10, 1257–1267. [Google Scholar] [CrossRef]
- Fujii, Y.; Nguyen, T.; Fujimura, Y.; Kameya, N.; Morita, H. Fecal metabolite of a gnotobiotic mouse transplanted with gut microbiota from a patient with Alzheimer’s disease. Biosci. Biotechnol. Biochem. 2019, 83, 1–9. [Google Scholar] [CrossRef]
- Sampson, T.; De Belius, J.; Thron, T.; Janssen, S.; Shastri, G.; Ilhan, Z.; Challis, C.; Schretter, C.; Rocha, S.; Gradinaru, V. Gut Microbiota Regulate Motor Deficits and Neuroinflammation in a Model of Parkinson’s Disease. Cell 2016, 167, 1469–1480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shang, L.; Liu, H.; Yu, H.; Chen, M.; Yang, T.; Zeng, X.; Qiao, S. Core Altered Microorganisms in Colitis Mouse Model: A Comprehensive Time-Point and Fecal Microbiota Transplantation Analysis. Antibiotics 2021, 10, 643. [Google Scholar] [CrossRef]
- Olson, C.A.; Vuong, H.E.; Yano, J.M.; Liang, Q.Y.; Nusbaum, D.J.; Hsiao, E.Y. The Gut Microbiota Mediates the Anti-Seizure Effects of the Ketogenic Diet. Cell 2018, 173, 1728–1741. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boehme, M.; Guzzetta, K.E.; Bastiaanssen, T.F.S.; van de Wouw, M.; Moloney, G.M.; Gual-Grau, A.; Spichak, S.; Olavarría-Ramírez, L.; Fitzgerald, P.; Morillas, E.; et al. Microbiota from young mice counteracts selective age-associated behavioral deficits. Nat. Aging 2021, 1, 666–676. [Google Scholar] [CrossRef]
- Cammarota, G.; Ianiro, G.; Tilg, H.; Rajilić-Stojanović, M.; Kump, P.; Satokari, R.; Sokol, H.; Arkkila, P.; Pintus, C.; Hart, A.; et al. European consensus conference on faecal microbiota transplantation in clinical practice. Gut 2017, 66, 569–580. [Google Scholar] [CrossRef] [PubMed]
- Sokol, H.; Galperine, T.; Kapel, N.; Bourlioux, P.; Seksik, P.; Barbut, F.; Scanzi, J.; Chast, F.; Batista, R.; Joly, F.; et al. Faecal microbiota transplantation in recurrent Clostridium difficile infection: Recommendations from the French Group of Faecal microbiota Transplantation. Dig. Liver Dis. 2016, 48, 242–247. [Google Scholar] [CrossRef]
- Mullish, B.H.; Quraishi, M.N.; Segal, J.P.; McCune, V.L.; Baxter, M.; Marsden, G.L.; Moore, D.J.; Colville, A.; Bhala, N.; Iqbal, T.H.; et al. The use of faecal microbiota transplant as treatment for recurrent or refractory Clostridium difficile infection and other potential indications: Joint British Society of Gastroenterology (BSG) and Healthcare Infection Society (HIS) guidelines. J. Hosp. Infect. 2018, 67, 1920–1941. [Google Scholar]
- Zhang, F.; Cui, B.; He, X.; Nie, Y.; Wu, K.; Fan, D. Microbiota transplantation: Concept, methodology and strategy for its modernization. Protein Cell 2018, 9, 462–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, F.; Luo, W.; Shi, Y.; Fan, Z.; Ji, G. Should we standardize the 1700-year-old fecal microbiota transplantation? Am. J. Gastroenterol. 2012, 107, 1755. [Google Scholar] [CrossRef] [PubMed]
- Hong, G. Zhou Hou Bei Ji Fang; Tianjin Science & Technology Press: Tianjin, China, 2000. [Google Scholar]
- Mei, Q.X.; Hui-Fei, W.U. The Book Zhou Hou Bei Ji Fang Make a Great Contribution to the Progress of Medicine. Study J. Tradit. Chin. Med. 2005. Available online: https://xueshu.baidu.com/usercenter/paper/show?paperid=1343fc06ebec0f7b5b467a92fbfbad4b&site=xueshu_se&hitarticle=1 (accessed on 27 February 2022).
- Li, S. Ben Cao Gang Mu; Huaxia Press: Beijing, China, 2011. [Google Scholar]
- Eiseman, B.; Silen, W.; Bascom, G.S.; Kauvar, A.J. Fecal enema as an adjunct in the treatment of pseudomembranous enterocolitis. Surgery 1958, 44, 854–859. [Google Scholar]
- Borody, T.J.; Campbell, J. Fecal microbiota transplantation: Current status and future directions. Expert Rev. Gastroenterol. Hepatol. 2011, 5, 653–655. [Google Scholar] [CrossRef]
- Surawicz, C.M.; Brandt, L.J.; Binion, D.G.; Ananthakrishnan, A.N.; Curry, S.R.; Gilligan, P.H.; McFarland, L.V.; Mellow, M.; Zuckerbraun, B.S. Guidelines for diagnosis, treatment, and prevention of Clostridium difficile infections. Am. J. Gastroenterol. 2013, 108, 478–498, 499. [Google Scholar] [CrossRef]
- Allegretti, J.R.; Mullish, B.H.; Kelly, C.; Fischer, M. The evolution of the use of faecal microbiota transplantation and emerging therapeutic indications. Lancet 2019, 394, 420–431. [Google Scholar] [CrossRef]
- Moayyedi, P.; Surette, M.G.; Kim, P.T.; Libertucci, J.; Wolfe, M.; Onischi, C.; Armstrong, D.; Marshall, J.K.; Kassam, Z.; Reinisch, W.; et al. Fecal Microbiota Transplantation Induces Remission in Patients with Active Ulcerative Colitis in a Randomized Controlled Trial. Gastroenterology 2015, 149, 102–109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suskind, D.L.; Brittnacher, M.J.; Wahbeh, G.; Shaffer, M.L.; Hayden, H.S.; Qin, X.; Singh, N.; Damman, C.J.; Hager, K.R.; Nielson, H.; et al. Fecal microbial transplant effect on clinical outcomes and fecal microbiome in active Crohn’s disease. Inflamm. Bowel Dis. 2015, 21, 556–563. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ishikawa, D.; Sasaki, T.; Takahashi, M.; Kuwahara-Arai, K.; Haga, K.; Ito, S.; Okahara, K.; Nakajima, A.; Shibuya, T.; Osada, T.; et al. The Microbial Composition of Bacteroidetes Species in Ulcerative Colitis Is Effectively Improved by Combination Therapy with Fecal Microbiota Transplantation and Antibiotics. Inflamm. Bowel Dis. 2018, 24, 2590–2598. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheon, D.J.; Orsulic, S. Mouse models of cancer. Annu. Rev. Pathol. Mech. Dis. 2011, 6, 95–119. [Google Scholar] [CrossRef]
- Vanhooren, V.; Libert, C. The mouse as a model organism in aging research: Usefulness, pitfalls and possibilities. Ageing Res. Rev. 2013, 12, 8–21. [Google Scholar] [CrossRef]
- Seishima, J.; Iida, N.; Kitamura, K.; Yutani, M.; Wang, Z.; Seki, A.; Yamashita, T.; Sakai, Y.; Honda, M.; Yamashita, T.; et al. Gut-derived Enterococcus faecium from ulcerative colitis patients promotes colitis in a genetically susceptible mouse host. Genome Biol. 2019, 20, 252. [Google Scholar] [CrossRef]
- Administrator. Guidelines for Routine Administration of Drugs in Animals. Available online: https://lac.nankai.edu.cn/2020/0529/c19628a275201/page.htm (accessed on 29 May 2020).
- Huo, Y. Experimental Zoology of Cardiovascular Diseases; People’s Medical Publishing House: Beijing, China, 2011. [Google Scholar]
- Vicentini, F.A.; Keenan, C.M.; Wallace, L.E.; Woods, C.; Cavin, J.; Flockton, A.R.; Macklin, W.B.; Belkind-Gerson, J.; Hirota, S.A.; Sharkey, K.A. Intestinal microbiota shapes gut physiology and regulates enteric neurons and glia. Microbiome 2021, 9, 210. [Google Scholar] [CrossRef] [PubMed]
- Reikvam, D.H.; Erofeev, A.; Sandvik, A.; Grcic, V.; Jahnsen, F.L.; Gaustad, P.; McCoy, K.D.; Macpherson, A.J.; Meza-Zepeda, L.A.; Johansen, F.E. Depletion of murine intestinal microbiota: Effects on gut mucosa and epithelial gene expression. PLoS ONE 2011, 6, e17996. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ishikawa, D.; Sasaki, T.; Osada, T.; Kuwahara-Arai, K.; Haga, K.; Shibuya, T.; Hiramatsu, K.; Watanabe, S. Changes in Intestinal Microbiota Following Combination Therapy with Fecal Microbial Transplantation and Antibiotics for Ulcerative Colitis. Inflamm. Bowel Dis. 2016, 23, 116–125. [Google Scholar] [CrossRef] [PubMed]
- Chu, N.D.; Smith, M.B.; Perrotta, A.R.; Kassam, Z.; Alm, E.J. Profiling Living Bacteria Informs Preparation of Fecal Microbiota Transplantations. PLoS ONE 2017, 12, e170922. [Google Scholar] [CrossRef]
- Gorzelak, M.A.; Gill, S.K.; Tasnim, N.; Ahmadi-Vand, Z.; Jay, M.; Gibson, D.L. Methods for Improving Human Gut Microbiome Data by Reducing Variability through Sample Processing and Storage of Stool. PLoS ONE 2015, 10, e134802. [Google Scholar] [CrossRef] [PubMed]
- Cui, B.; Li, P.; Xu, L.; Zhao, Y.; Wang, H.; Peng, Z.; Xu, H.; Xiang, J.; He, Z.; Zhang, T.; et al. Step-up fecal microbiota transplantation strategy: A pilot study for steroid-dependent ulcerative colitis. J. Transl. Med. 2015, 13, 298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fang, H.; Fu, L.; Wang, J. Protocol for Fecal Microbiota Transplantation in Inflammatory Bowel Disease: A Systematic Review and Meta-Analysis. BioMed Res. Int. 2018, 2018, 8941340. [Google Scholar] [CrossRef] [Green Version]
- Lima, S.F.; Gogokhia, L.; Viladomiu, M.; Chou, L.; Putzel, G.; Jin, W.; Pires, S.; Guo, C.; Gerardin, Y.; Crawford, C.V.; et al. Transferable Immunoglobulin A–Coated Odoribacter splanchnicus in Responders to Fecal Microbiota Transplantation for Ulcerative Colitis Limits Colonic Inflammation. Gastroenterology 2022, 162, 166–178. [Google Scholar] [CrossRef] [PubMed]
- Paramsothy, S.; Kamm, M.A.; Kaakoush, N.O.; Walsh, A.J.; van den Bogaerde, J.; Samuel, D.; Leong, R.; Connor, S.; Ng, W.; Paramsothy, R.; et al. Multidonor intensive faecal microbiota transplantation for active ulcerative colitis: A randomised placebo-controlled trial. Lancet 2017, 389, 1218–1228. [Google Scholar] [CrossRef]
- Carabotti, M.; Scirocco, A.; Maselli, M.A.; Severi, C. The gut-brain axis: Interactions between enteric microbiota, central and enteric nervous systems. Ann. Gastroenterol. 2015, 28, 203–209. [Google Scholar]
- Kim, N.; Jeon, S.H.; Ju, I.G.; Gee, M.S.; Do, J.; Oh, M.S.; Lee, J.K. Transplantation of gut microbiota derived from Alzheimer’s disease mouse model impairs memory function and neurogenesis in C57BL/6 mice. Brain Behav. Immun. 2021, 98, 357–365. [Google Scholar] [CrossRef]
- Chevalier, G.; Siopi, E.; Guenin-Macé, L.; Pascal, M.; Laval, T.; Rifflet, A.; Boneca, I.G.; Demangel, C.; Colsch, B.; Pruvost, A.; et al. Effect of gut microbiota on depressive-like behaviors in mice is mediated by the endocannabinoid system. Nat. Commun. 2020, 11, 6363. [Google Scholar] [CrossRef]
- Li, J.; Zhao, F.; Wang, Y.; Chen, J.; Tao, J.; Tian, G.; Wu, S.; Liu, W.; Cui, Q.; Geng, B.; et al. Gut microbiota dysbiosis contributes to the development of hypertension. Microbiome 2017, 5, 14. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.Y.; Chen, J.; Yi, K.; Peng, L.; Xie, J.; Gou, X.; Peng, T.; Tang, L. Phlorizin ameliorates obesity-associated endotoxemia and insulin resistance in high-fat diet-fed mice by targeting the gut microbiota and intestinal barrier integrity. Gut Microbes 2020, 12, 1–18. [Google Scholar] [CrossRef]
- Zhang, P.P.; Li, L.L.; Han, X.; Li, Q.W.; Zhang, X.H.; Liu, J.J.; Wang, Y. Fecal microbiota transplantation improves metabolism and gut microbiome composition in db/db mice. Acta Pharmacol. Sin. 2020, 41, 678–685. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Huang, R.; Cheng, M.; Wang, L.; Chao, J.; Li, J.; Zheng, P.; Xie, P.; Zhang, Z.; Yao, H. Gut microbiota from NLRP3-deficient mice ameliorates depressive-like behaviors by regulating astrocyte dysfunction via circHIPK2. Microbiome 2019, 7, 116. [Google Scholar] [CrossRef] [PubMed]
- Bárcena, C.; Valdés-Mas, R.; Mayoral, P.; Garabaya, C.; Durand, S.; Rodríguez, F.; Fernández-García, M.T.; Salazar, N.; Nogacka, A.M.; Garatachea, N.; et al. Healthspan and lifespan extension by fecal microbiota transplantation into progeroid mice. Nat. Med. 2019, 25, 1234–1242. [Google Scholar] [CrossRef] [PubMed]
- Yu, F.; Han, W.; Zhan, G.; Li, S.; Jiang, X.; Wang, L.; Xiang, S.; Zhu, B.; Yang, L.; Luo, A.; et al. Abnormal gut microbiota composition contributes to the development of type 2 diabetes mellitus in db/db mice. Aging 2019, 11, 10454–10467. [Google Scholar] [CrossRef]
- Trikha, S.; Lee, D.M.; Ecton, K.E.; Wrigley, S.D.; Vazquez, A.R.; Litwin, N.S.; Thomas, K.N.; Wei, Y.; Battson, M.L.; Johnson, S.A.; et al. Transplantation of an obesity-associated human gut microbiota to mice induces vascular dysfunction and glucose intolerance. Gut Microbes 2021, 13, 1940791. [Google Scholar] [CrossRef]
- Sharon, G.; Cruz, N.J.; Kang, D.W.; Gandal, M.J.; Wang, B.; Kim, Y.M.; Zink, E.M.; Casey, C.P.; Taylor, B.C.; Lane, C.J.; et al. Human Gut Microbiota from Autism Spectrum Disorder Promote Behavioral Symptoms in Mice. Cell 2019, 177, 1600–1618. [Google Scholar] [CrossRef] [Green Version]
- Kundu, P.; Lee, H.U.; Garcia-Perez, I.; Tay, E.; Kim, H.; Faylon, L.E.; Martin, K.A.; Purbojati, R.; Drautz-Moses, D.I.; Ghosh, S.; et al. Neurogenesis and prolongevity signaling in young germ-free mice transplanted with the gut microbiota of old mice. Sci. Transl. Med. 2019, 11, eaau4760. [Google Scholar] [CrossRef]
- Britton, G.J.; Contijoch, E.J.; Mogno, I.; Vennaro, O.H.; Llewellyn, S.R.; Ng, R.; Li, Z.; Mortha, A.; Merad, M.; Das, A.; et al. Microbiotas from Humans with Inflammatory Bowel Disease Alter the Balance of Gut Th17 and RORγt+ Regulatory T Cells and Exacerbate Colitis in Mice. Immunity 2019, 50, 212–224. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Type | Length | Needle Diameter | Apply |
|---|---|---|---|
| 6 | 5 cm | 0.6 mm | Nude mice, about 5 weeks old |
| 7 | 5 cm | 0.7 mm | ≤25 g mice |
| 8 | 4.5 cm | 0.8 mm | ≤30 g mice |
| 9 | 6 cm | 0.9 mm | ≤30 g mice |
| 12 | 4 cm | 1.2 mm | ~50 g mice |
| 12 | 5 cm | 1.2 mm | ~100 g mice |
| 12 | 6 cm | 1.2 mm | ~150 g mice |
| 16 | 8 cm | 1.6 mm | 150~250 g rat |
| 16 | 9 cm | 1.6 mm | ~250 g rats |
| 16 | 11 cm | 1.6 mm | ~350 g rats |
| 18 | 10 cm | 1.8 mm | ≥350 g rats |
| 20 | 10 cm | 2.0 mm | Rats (≥350 g), dogs, rabbits, and birds |
| Animal Species | Weight (g) | Gastric Volume (mL) |
|---|---|---|
| Mice | 20–24 | 0.8 |
| 25–30 | 0.9 | |
| ≥30 | 1.0 | |
| Rats | 100–199 | 3.0 |
| 200–249 | 4–5 | |
| 250–300 | 6.0 | |
| ≥300 | 8.0 | |
| Guinea pigs | 250–300 | 4–5 |
| ≥300 | 6.0 | |
| Rabbits | 2000–2400 | 100 |
| 2500–3500 | 150 | |
| ≥3500 | 200 | |
| Cats | 2500–3000 | 50–80 |
| ≥3000 | 100–150 | |
| Dogs | 10,000–15,000 | 200–500 |
| Pigs | - | 500 |
| Problem | Possible Reason | Solution |
|---|---|---|
| High incidence of animal death | Unskilled intragastric operation, resulting in excessive stress | Gavage should be painless. If the animal persistently struggles, has difficulty breathing, or resists needle insertion, immediately stop needle insertion and pull the needle out. Try again after the animal has become calm. After the mice have been injected and released, and observations have been conducted for any respiratory abnormalities, the success of the gavage insertion should be confirmed |
| Low colonization efficiency | (1) Low volume of feces collected; (2) short duration of intragastric administration of bacterial liquid; (3) operation from solution preparation to intragastric administration more than 6 h; (4) and inappropriate glycerin concentration | (1) To increase the amount of feces collected, feces from several mice can be mixed on the basis of experimental needs; (2) intragastric administration should last at least 2 weeks; (3) operation should be fast to reduce the exposure time under oxygen; and (4) the glycerin concentration should be appropriate |
| High degree of variability within experimental groups | (1) Excessive differences in donor flora; (2) Failed intragastric administration of some recipients | (1) Donors should be rigorously selected, and detection of donor flora is necessary; (2) gavage operations should be skillfully conducted to ensure that mice do not spit out the bacterial fluid |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shang, L.; Tu, J.; Dai, Z.; Zeng, X.; Qiao, S. Microbiota Transplantation in an Antibiotic-Induced Bacterial Depletion Mouse Model: Reproducible Establishment, Analysis, and Application. Microorganisms 2022, 10, 902. https://doi.org/10.3390/microorganisms10050902
Shang L, Tu J, Dai Z, Zeng X, Qiao S. Microbiota Transplantation in an Antibiotic-Induced Bacterial Depletion Mouse Model: Reproducible Establishment, Analysis, and Application. Microorganisms. 2022; 10(5):902. https://doi.org/10.3390/microorganisms10050902
Chicago/Turabian StyleShang, Lijun, Jiayu Tu, Ziqi Dai, Xiangfang Zeng, and Shiyan Qiao. 2022. "Microbiota Transplantation in an Antibiotic-Induced Bacterial Depletion Mouse Model: Reproducible Establishment, Analysis, and Application" Microorganisms 10, no. 5: 902. https://doi.org/10.3390/microorganisms10050902