
Management of a Major Carbapenem-Resistant Acinetobacter baumannii Outbreak in a French Intensive Care Unit While Maintaining Its Capacity Unaltered

 , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Setting
2.2. Population Concerned by the Outbreak
2.3. Definitions and Data Collection
2.4. Microbiological Methods
3. Results
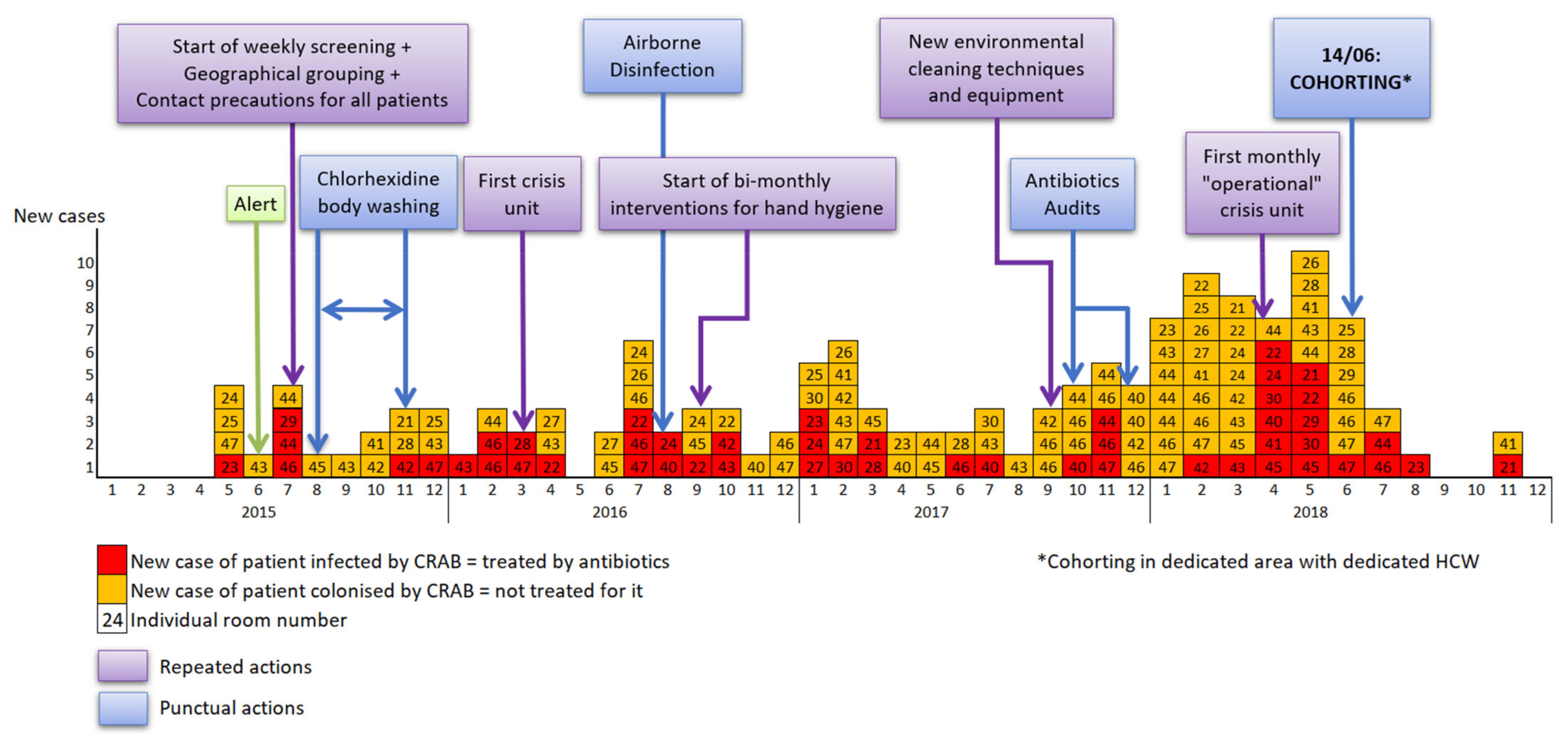
3.1. Patient Characteristics and Epidemic Curve
3.2. Microbiology and Samples
3.2.1. Microbiology
3.2.2. Patients Sampling
3.2.3. Environmental Sampling
3.2.4. Samples of HCWs’ Hands
3.3. Chronology of Actions, Results and Impact on the Outbreak
3.3.1. Detection of Outbreak and First Infection Prevention and Control (IPC) Measures
3.3.2. Extension of Conventional IPC Measures
3.3.3. Final Measure: Cohorting with Dedicated Area and Dedicated HCW
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Liu, W.-L.; Liang, H.-W.; Lee, M.-F.; Lin, H.-L.; Lin, Y.-H.; Chen, C.-C.; Chang, P.-C.; Lai, C.-C.; Chuang, Y.-C.; Tang, H.-J. The Impact of Inadequate Terminal Disinfection on an Outbreak of Imipenem-Resistant Acinetobacter baumannii in an Intensive Care Unit. PLoS ONE 2014, 9, e107975. [Google Scholar] [CrossRef] [PubMed]
- Wieland, K.; Chhatwal, P.; Vonberg, R.-P. Nosocomial outbreaks caused by Acinetobacter baumannii and Pseudomonas aeruginosa: Results of a systematic review. Am. J. Infect. Control 2018, 46, 643–648. [Google Scholar] [CrossRef] [PubMed]
- Teerawattanapong, N.; Panich, P.; Kulpokin, D.; Na Ranong, S.; Kongpakwattana, K.; Saksinanon, A.; Goh, B.H.; Lee, L.-H.; Apisarnthanarak, A.; Chaiyakunapruk, N. A Systematic Review of the Burden of Multidrug-Resistant Healthcare-Associated Infections Among Intensive Care Unit Patients in Southeast Asia: The Rise of Multidrug-Resistant Acinetobacter baumannii. Infect. Control Hosp. Epidemiol. 2018, 39, 525–533. [Google Scholar] [CrossRef]
- Howard, A.; O’Donoghue, M.; Feeney, A.; Sleator, R.D. Acinetobacter baumannii. Virulence 2012, 3, 243–250. [Google Scholar] [CrossRef] [PubMed]
- Barnes, S.L.; Morgan, D.J.; Harris, A.D.; Carling, P.C.; Thom, K.A. Preventing the Transmission of Multidrug-Resistant Organisms: Modeling the Relative Importance of Hand Hygiene and Environmental Cleaning Interventions. Infect. Control Hosp. Epidemiol. 2014, 35, 1156–1162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tacconelli, E.; Cataldo, M.A.; Dancer, S.J.; De Angelis, G.; Falcone, M.; Frank, U.; Kahlmeter, G.; Pan, A.; Petrosillo, N.; Rodríguez-Baño, J.; et al. ESCMID guidelines for the management of the infection control measures to reduce transmission of multidrug-resistant Gram-negative bacteria in hospitalized patients. Clin. Microbiol. Infect. 2014, 20, 1–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaynes, R.; Edwards, J.R.; System, N.N.I.S. Overview of Nosocomial Infections Caused by Gram-Negative Bacilli. Clin. Infect. Dis. 2005, 41, 848–854. [Google Scholar] [CrossRef] [PubMed]
- Henig, O.; Weber, G.; Hoshen, M.B.; Paul, M.; German, L.; Neuberger, A.; Gluzman, I.; Berlin, A.; Shapira, C.; Balicer, R.D. Risk factors for and impact of carbapenem-resistant Acinetobacter baumannii colonization and infection: Matched case–control study. Eur. J. Clin. Microbiol. 2015, 34, 2063–2068. [Google Scholar] [CrossRef]
- Abbo, A.; Carmeli, Y.; Navon-Venezia, S.; Siegman-Igra, Y.; Schwaber, M.J. Impact of multi-drug-resistant Acinetobacter baumannii on clinical outcomes. Eur. J. Clin. Microbiol. 2007, 26, 793–800. [Google Scholar] [CrossRef]
- Garnacho-Montero, J.; Dimopoulos, G.; Poulakou, G.; Akova, M.; Cisneros, J.M.; De Waele, J.; Petrosillo, N.; Seifert, H.; Timsit, J.F.; Vila, J.; et al. Task force on management and prevention of Acinetobacter baumannii infections in the ICU. Intensive Care Med. 2015, 41, 2057–2075. [Google Scholar] [CrossRef]
- World Health Organization. Guidelines for the Prevention and Control of Carbapenem-Resistant Enterobacteriaceae, Acinetobacter baumannii, and Pseudomonas aeruginosa in Health Care Facilities. Available online: https://www.who.int/publications-detail-redirect/9789241550178 (accessed on 28 February 2022).
- Ling, M.L.; Ang, A.; Wee, M.; Wang, G.C.Y. A Nosocomial Outbreak of Multiresistant Acinetobacter baumannii Originating From an Intensive Care Unit. Infect. Control Hosp. Epidemiol. 2001, 22, 48–49. [Google Scholar] [CrossRef] [PubMed]
- Fierobe, L.; Lucet, J.-C.; Decré, D.; Muller-Serieys, C.; Deleuze, A.; Joly-Guillou, M.-L.; Mantz, J.; Desmonts, J.-M. An Outbreak of Imipenem-Resistant Acinetobacter baumannii in Critically Ill Surgical Patients. Infect. Control Hosp. Epidemiol. 2001, 22, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Siegel, J.D.; Rhinehart, E.; Jackson, M.; Chiarello, L. Management of multidrug-resistant organisms in health care settings, 2006. Am. J. Infect. Control 2007, 35, S165–S193. [Google Scholar] [CrossRef] [PubMed]
- Société Française D’hygiène Hospitalière Recommandations Nationales. Prévention de La Transmission Croisée: Précautions Complémentaires Contact. Available online: https://www.sf2h.net/publications/prevention-de-transmission-croisee-precautions-complementaires-contact (accessed on 28 February 2022).
- Coyle, J.R.; Kaye, K.S.; Taylor, T.; Tansek, R.; Campbell, M.; Hayakawa, K.; Marchaim, D. Effectiveness and cost of implementing an active surveillance screening policy for Acinetobacter baumannii: A Monte Carlo simulation model. Am. J. Infect. Control. 2014, 42, 283–287. [Google Scholar] [CrossRef] [PubMed]
- Marchaim, D.; Navon-Venezia, S.; Schwartz, D.; Tarabeia, J.; Fefer, I.; Schwaber, M.J.; Carmeli, Y. Surveillance Cultures and Duration of Carriage of Multidrug-Resistant Acinetobacter baumannii. J. Clin. Microbiol. 2007, 45, 1551–1555. [Google Scholar] [CrossRef] [Green Version]
- Apisarnthanarak, A.; Warren, D. Screening for Carbapenem-Resistant Acinetobacter baumannii Colonization Sites: An Implication for Combination of Horizontal and Vertical Approaches. Clin. Infect. Dis. 2012, 56, 1057–1059. [Google Scholar] [CrossRef] [Green Version]
- Corbella, X.; Pujol, M.; Argerich, M.J.; Ayats, J.; Sendra, M.; Peña, C.; Ariza, J. Environmental Sampling of Acinetobacter baumannii: Moistened Swabs Versus Moistened Sterile Gauze Pads. Infect. Control. Hosp. Epidemiol. 1999, 20, 458–460. [Google Scholar] [CrossRef]
- Mendoza-Olazarán, S.; Camacho-Ortiz, A.; Martínez-Reséndez, M.F.; Llaca-Díaz, J.M.; Pérez-Rodríguez, E.; Garza-González, E. Influence of whole-body washing of critically ill patients with chlorhexidine on Acinetobacter baumannii isolates. Am. J. Infect. Control. 2014, 42, 874–878. [Google Scholar] [CrossRef]
- Gray, A.; Allard, R.; Paré, R.; Tannenbaum, T.; Lefebvre, B.; Lévesque, S.; Mulvey, M.; Maalouf, L.; Perna, S.; Longtin, Y. Management of a hospital outbreak of extensively drug-resistant Acinetobacter baumannii using a multimodal intervention including daily chlorhexidine baths. J. Hosp. Infect. 2016, 93, 29–34. [Google Scholar] [CrossRef]
- Société Française D’hygiène Hospitalière. Prévention de la Transmission Croisée: Précautions Complémentaires Contact—Consensus Formalisé D’experts. Available online: https://bdsp-ehesp.inist.fr/vibad/index.php?action=getRecordDetail&idt=401433 (accessed on 28 February 2022).
- Alfandari, S. Origine et attente des référents antibiotiques dans les établissements de santé en France. Résultats d’une enquête de la SPILF. Méd. Mal. Infect. 2006, 36, 513–516. [Google Scholar] [CrossRef]
- Shimose, L.A.; Masuda, E.; Sfeir, M.; Caban, A.B.; Bueno, M.X.; Depascale, D.; Spychala, C.N.; Cleary, T.; Namias, N.; Kett, D.H.; et al. Carbapenem-Resistant Acinetobacter baumannii: Concomitant Contamination of Air and Environmental Surfaces. Infect. Control. Hosp. Epidemiol. 2016, 37, 777–781. [Google Scholar] [CrossRef] [PubMed]
- Otter, J.; Mutters, N.; Tacconelli, E.; Gikas, A.; Holmes, A. Controversies in guidelines for the control of multidrug-resistant Gram-negative bacteria in EU countries. Clin. Microbiol. Infect. 2015, 21, 1057–1066. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Microbiological Technique | Agar | Contact Agar | Swab | Cloth |
|---|---|---|---|---|
| Type of sample | HCWs’ handprints | Environmental sampling | Patient skin or rectum and environmental sampling | Environmental sampling |
| Sampling | Palm and fingertip application on Columbia agar + sheep blood plus (Thermoscientific, OXOID Wesel, Germany) | Agar (TSA with disinhibitor plus, Thermoscientific, OXOID) in contact with the surface | Scrubbing of the target area (skin, rectum, or surface) | Application of a non-woven sterile compresses (Laboratoires Euromédis, ref: 175572, Picardy, France) soaked in sterile water |
| 1st step | Agar media incubated at 35 °C during 24–48 h | − | Suspension of the cloth in 10 mL of fluid D (Merck-Millipore, Alsace, France) and mix with a bag mixer | |
| 2nd step | Identification of each colony type with MALDI-TOF MS (Bruker daltonic, Bremen, Germany) | Inoculation onto a selective medium for the detection of carbapenemase producing bacteria (chromID CARBA SMART agar, and incubation at 35 °C during 24–48 h | ||
| 3rd step | If positive to Acinetobacter baumannii, colonies are repicked onto a selective medium for the detection of carbapenemase producing bacteria (chromID CARBA SMART agar, bioMérieux, Craponne, France) and incubation at 35 °C during 24–48 h | − | − | − |
| Patient Characteristics | n (%) |
|---|---|
| Age (years) | |
| Mean | 58.1 |
| Median | 60 |
| SD | 16.7 |
| IQR | 47−72 |
| Gender | |
| Females | 41 (29.1) |
| Males | 100 (70.9) |
| Length of Stay in ICU (days) | |
| Mean | 30.3 |
| Median | 25 |
| SD | 29.2 |
| Length of Stay Before Contamination (days) | |
| Mean | 13.8 |
| Median | 11 |
| SD | 10.4 |
| Number of CRAB Contaminations | |
| Colonization without infection | 91 (64.5) |
| Infection (treated by antibiotics) | 50 (35.5) |
| Mortality at 6 months after contamination | 37 (26.2) |
| Among colonization cases (n = 91) | 17 (18.7) |
| Among infection cases (n = 50) | 20 (40.0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Risser, C.; Pottecher, J.; Launoy, A.; Ursenbach, A.; Belotti, L.; Boyer, P.; Willemain, R.; Lavigne, T.; Deboscker, S. Management of a Major Carbapenem-Resistant Acinetobacter baumannii Outbreak in a French Intensive Care Unit While Maintaining Its Capacity Unaltered. Microorganisms 2022, 10, 720. https://doi.org/10.3390/microorganisms10040720
Risser C, Pottecher J, Launoy A, Ursenbach A, Belotti L, Boyer P, Willemain R, Lavigne T, Deboscker S. Management of a Major Carbapenem-Resistant Acinetobacter baumannii Outbreak in a French Intensive Care Unit While Maintaining Its Capacity Unaltered. Microorganisms. 2022; 10(4):720. https://doi.org/10.3390/microorganisms10040720
Chicago/Turabian StyleRisser, Clémence, Julien Pottecher, Anne Launoy, Axel Ursenbach, Laure Belotti, Pierre Boyer, Rosalie Willemain, Thierry Lavigne, and Stéphanie Deboscker. 2022. "Management of a Major Carbapenem-Resistant Acinetobacter baumannii Outbreak in a French Intensive Care Unit While Maintaining Its Capacity Unaltered" Microorganisms 10, no. 4: 720. https://doi.org/10.3390/microorganisms10040720