
Competitive Real-Time Near Infrared (NIR) Vein Finder Imaging Device to Improve Peripheral Subcutaneous Vein Selection in Venipuncture for Clinical Laboratory Testing

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Device Design with Its Components
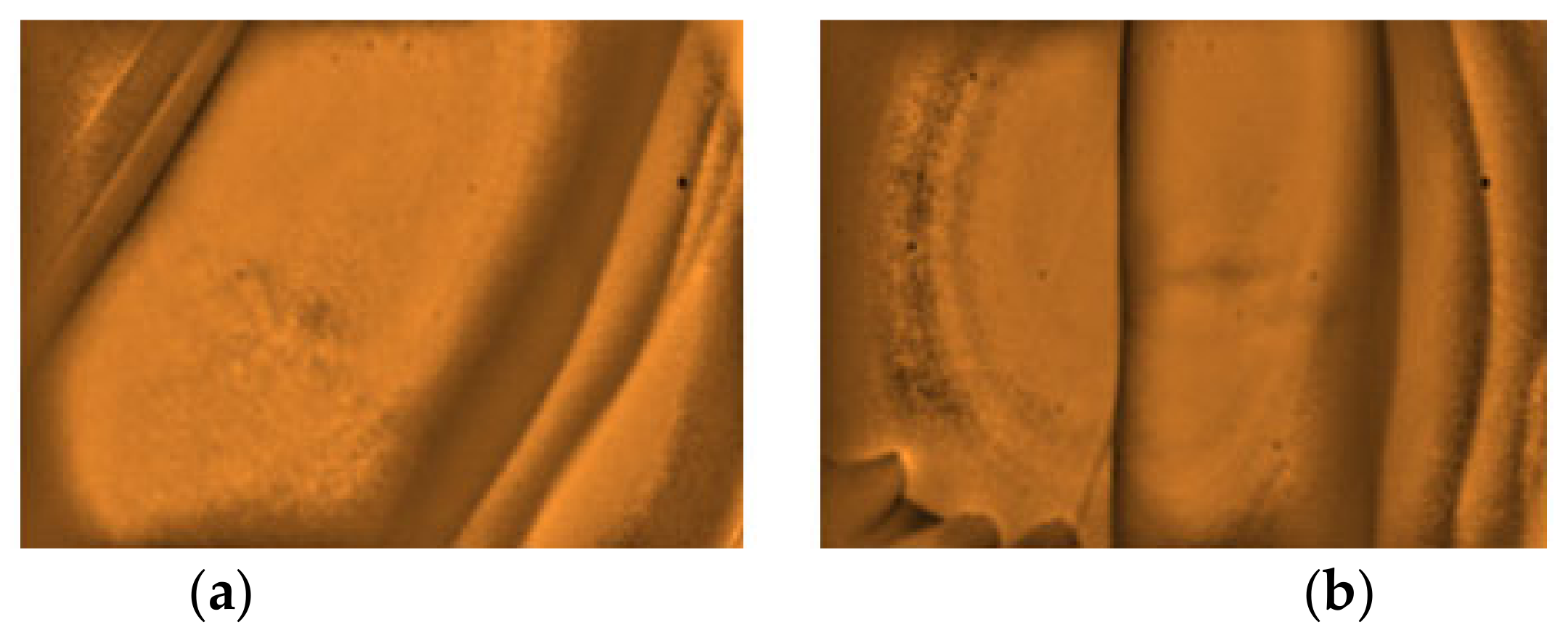
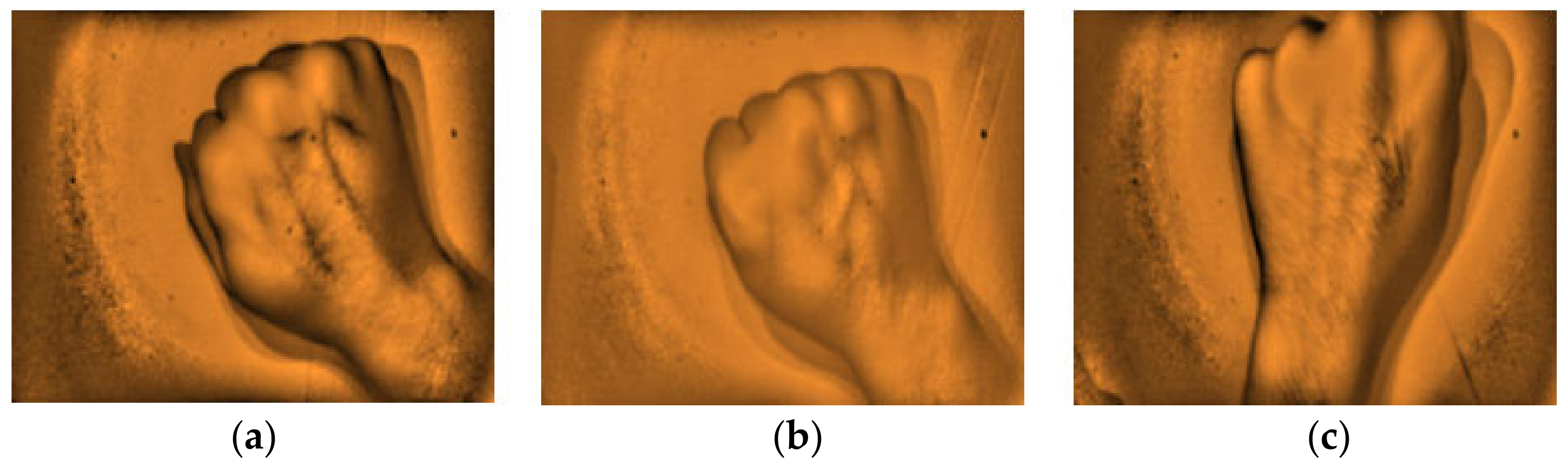
2.2. Assessment of the NIR Vein Finder Prototype (Image Analysis)
2.3. Statistical Analysis
3. Results
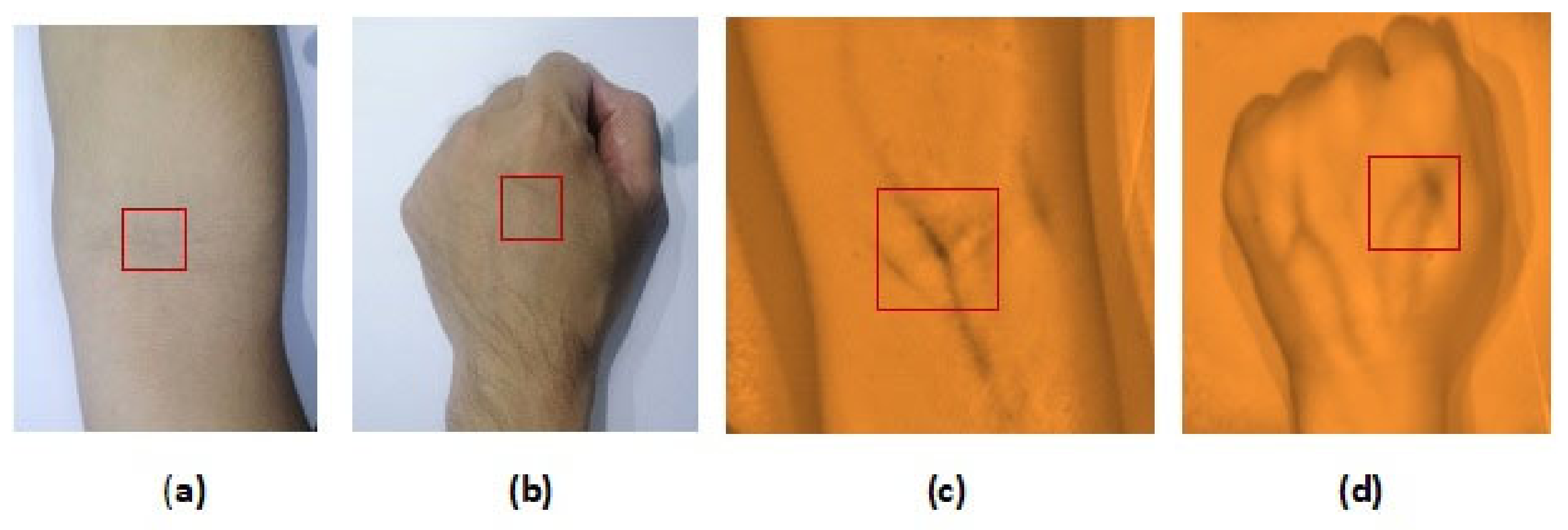
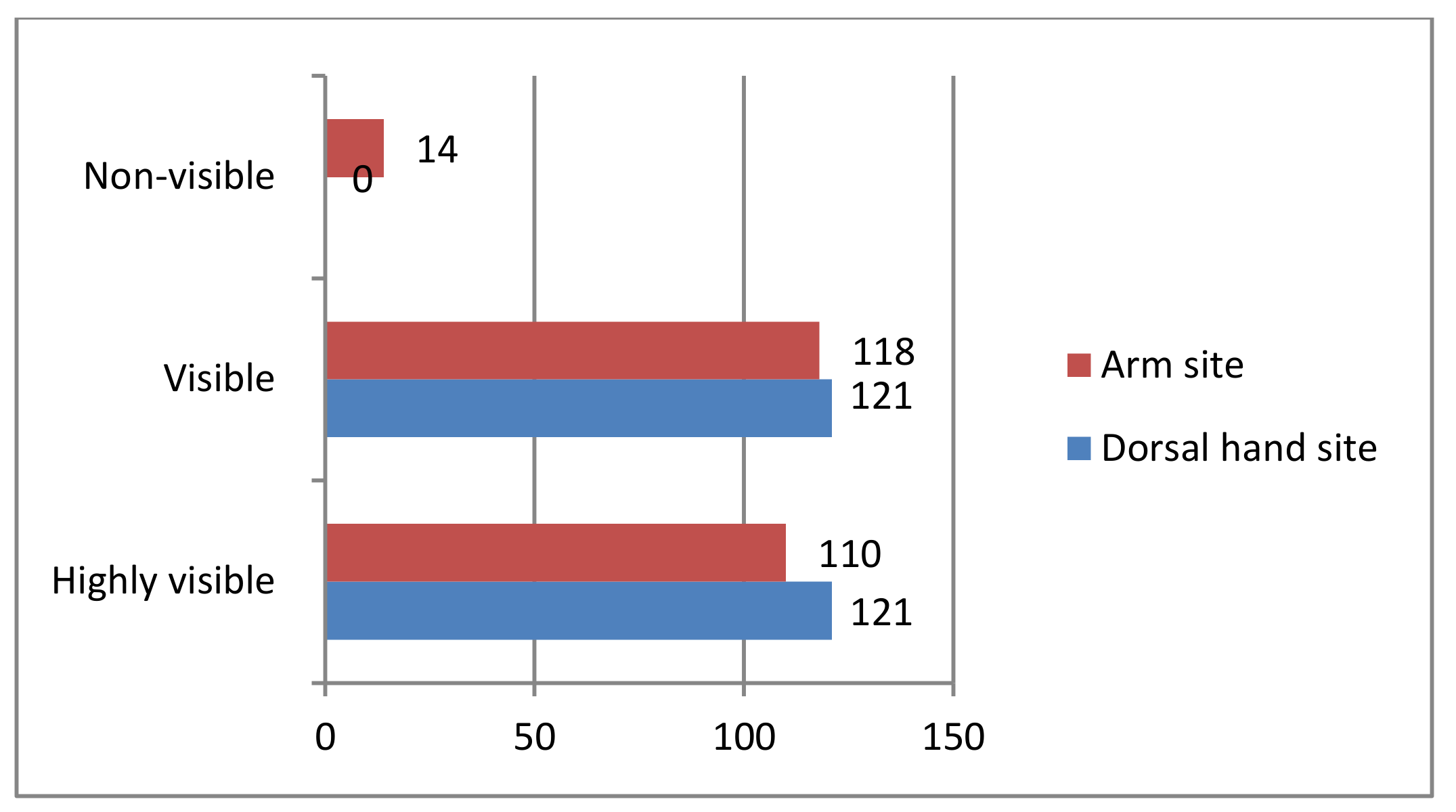
3.1. Vein Visualization Rate with the Developed Vein Finder in the Arm and Dorsal Hand Sites
3.2. Assessment of the Vein Finder with the Different Parameters such as: Gender, Age, Body Mass Index (BMI), Skin Color/Tone, and Arm Circumference
3.2.1. Arm Site: Results for Highly Visible and Visible Were Presented Based on the Given Parameters
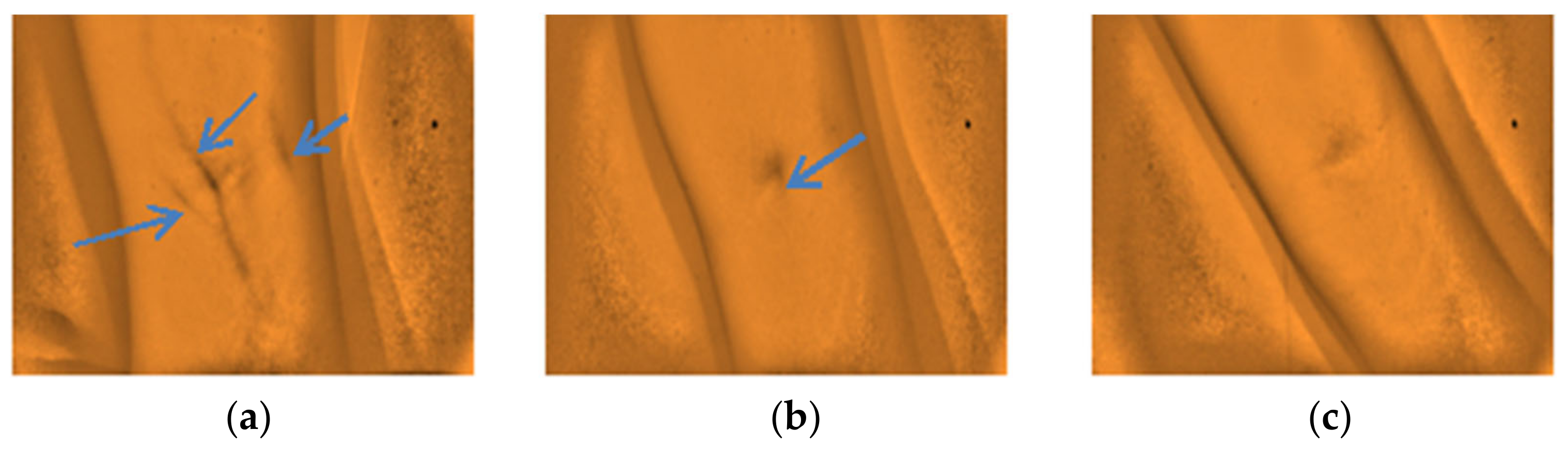
3.2.2. Arm Site: Results for Non-Visible Were Presented Based on the Given Parameters
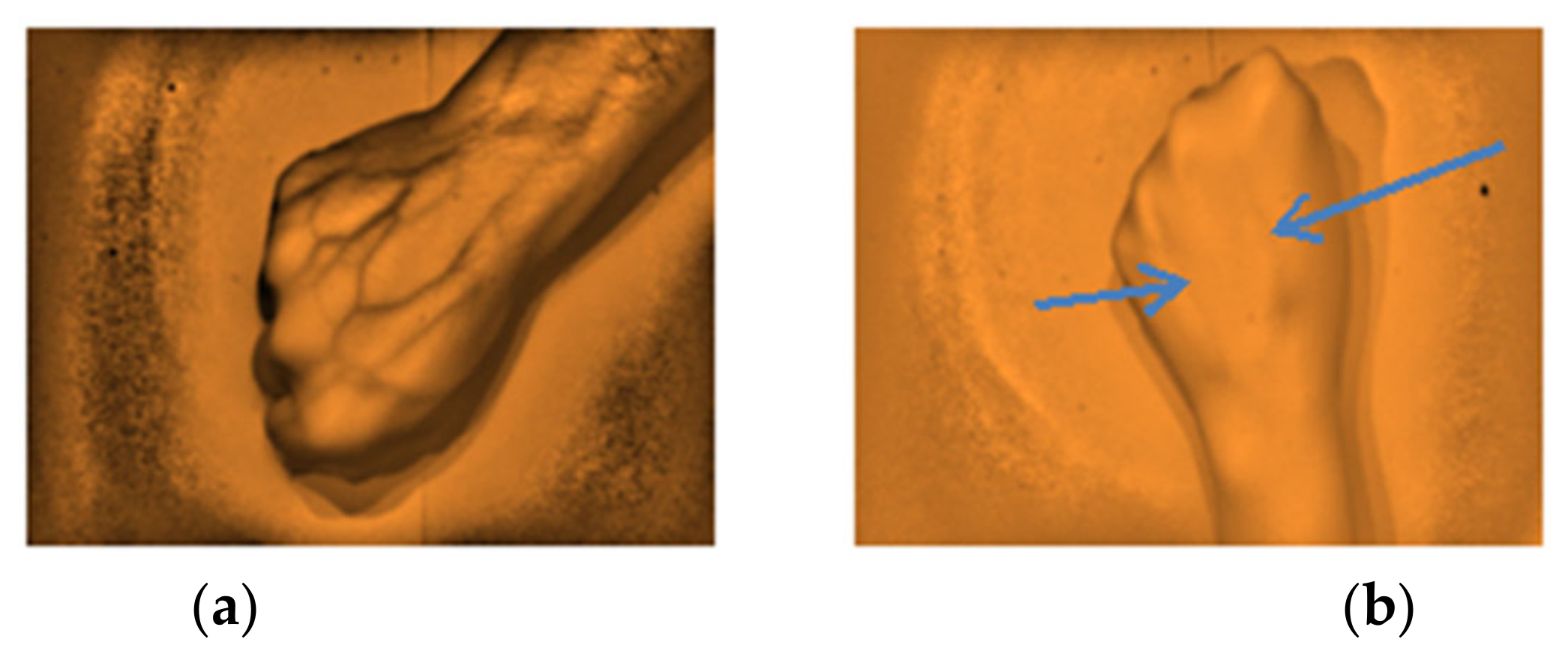
3.2.3. Dorsal Hand Site: Results for Highly Visible and Visible Subcutaneous Veins Were Presented Based on the Given Parameters
4. Discussion
4.1. Based on Parameters: Both Arm and Dorsal Hand Sites (for Highly Visible and Visible)
4.2. Results of Non-Visible in the Arm Site
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Ethical Statement
References
- Fernández, R.; Armada, M. Multisensory System for the Detection and Localization of Peripheral Subcutaneous Veins. Sensors 2017, 17, 897. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lamperti, M.; Pittiruti, M., II. Difficult peripheral veins: Turn on the lights. Br. J. Anaesth. 2013, 110, 888–891. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scales, K. Intravenous therapy: A guide to good practice. Br. J. Nurs. 2008, 17, S4–S12. [Google Scholar] [CrossRef] [PubMed]
- Lalongo, C.; Bernardini, S. Phlebotomy, a bridge between laboratory and patient. Biochemiamedica 2016, 26, 17–33. [Google Scholar]
- Kimori, K.; Sugama, J.; Nakatani, T.; Tnakayama, K.; Miyati, T.; Sanada, H. An observational study comparing the pro-totype device with the existing device for the effective visualization of invisible veins in elderly patients in Japan. SAGE Open Med. 2015, 3, 2050312115615365. [Google Scholar] [CrossRef] [Green Version]
- The Clinical & Laboratory Standards Institute (CLSI). NEW CLSI Venipuncture Guidelines-CLSI, Collection of Diagnostic Venous Blood Specimens, Standard GP41, 7th ed; The Clinical & Laboratory Standards Institute (CLSI): Annapolis Junction, MD, USA, 2017. [Google Scholar]
- Buowari, O. Complications of venipuncture. Adv. Biosci. Biotechnol. 2013, 4, 126–128. [Google Scholar] [CrossRef] [Green Version]
- Grable, H.; Gill, G. Phlebotomy Puncture Juncture Preventing Phlebotomy Errors—Potential For Harming Your Patients. Labmedicine 2005, 36, 430–433. [Google Scholar]
- Pan, C.-T.; Francisco, M.D.; Yen, C.-K.; Wang, S.-Y.; Shiue, Y.-L. Vein Pattern Locating Technology for Cannulation: A Review of the Low-Cost Vein Finder Prototypes Utilizing near Infrared (NIR) Light to Improve Peripheral Subcutaneous Vein Selection for Phlebotomy. Sensors 2019, 19, 3573. [Google Scholar] [CrossRef] [Green Version]
- Parker, S.; Benzies, K.; Hayden, K.; Lang, E. Effectiveness of interventions for adult peripheral intravenous catherization: A systematic review and meta-analysis of randomized controlled trials. Int. Emerg. Nurs. 2017, 31, 15–21. [Google Scholar] [CrossRef]
- Juric, S.; Flis, V.; Debevc, M.; Holzinger, A.; Zalik, B. Towards a Low-Cost Mobile Subcutaneous Vein Detection Solution Using Near-Infrared Spectroscopy. Sci. World J. 2014, 2014, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Goh, C.; Subaramaniam, R.; Saad, N.M.; Ali, S.A.; Meriaudeau, F. Subcutaneous veins depth measurement using diffuse re-flectance images. Opt. Express 2017, 25, 25741–25759. [Google Scholar] [CrossRef]
- Rothbart, A.; Yu, P.; Müller‑Lobeck, L.; Spies, C.; Wernecke, K.D.; Nachtigall, I. Peripheral intravenous cannulation with support of infrared laser vein viewing system in a pre-operation setting in pediatric patients. BMC Res. Notes 2015, 8, 463. [Google Scholar] [CrossRef] [Green Version]
- West, J.; Atherton, J.; Costelloe, S.J.; Pourmahram, G.; Stretton, A.; Cornes, M. Preanalytical errors in medical laboratories: A review of the available methodologies of data collection and analysis. Ann. Clin. Biochem. Int. J. Lab. Med. 2017, 54, 14–19. [Google Scholar] [CrossRef]
- Najat, D. Prevalence of Pre-Analytical Errors in Clinical Chemistry Diagnostic Labs in Sulaimani City of Iraqi Kurdistan. PLoS ONE 2017, 12, e0170211. [Google Scholar] [CrossRef]
- Salinas, M.; López-Garrigós, M.; Flores, E.; Santo-Quiles, A.; Gutierrez, M.; Lugo, J.; Lillo, R.; Leiva-Salinas, C. Ten years of preanalytical monitoring and control: Synthetic Balanced Score Card Indicator. Biochem. Med. 2015, 25, 49–56. [Google Scholar] [CrossRef]
- Patra, S.; Mukherjee, B.; Das, A. Pre-analytical errors in the clinical laboratory and how to minimize them. Int. J. Bioassays 2013. ISSN: 2278-778X. [Google Scholar]
- Hammerling, J.A. A Review of Medical Errors in Laboratory Diagnostics and Where We Are Today: Table 1. Lab. Med. 2012, 43, 41–44. [Google Scholar] [CrossRef] [Green Version]
- Lippi, G.; Chance, J.J.; Church, S.; Dazzi, P.; Fontana, R.; Giavarina, D.; Grankvist, K.; Huisman, W.; Kouri, T.; Palicka, V.; et al. Pre-analytical quality improvement: From dream to reality. Clin. Chem. Lab. Med. 2011, 49, 1113–1126. [Google Scholar] [CrossRef]
- Goswami, B.; Singh, B.; Chawla, R.; Mallika, V. Evaluation of errors in a clinical laboratory: A one-year experience. Clin. Chem. Lab. Med. 2010, 48, 63–66. [Google Scholar] [CrossRef] [Green Version]
- Chen, A.; Nikitczuk, K.; Nikitczuk, J.; Maguire, T.; Yarmush, M.L. Portable robot for autonomous venipuncture using 3D near infrared image guidance. Technology 2013, 1, 72–87. [Google Scholar] [CrossRef]
- Cuper, N.; Verdaasdonk, R.; de Roode, R.; de Vooght, K.; Viergever, M.; Kalkman, C.; de Graaff, J. Visualizing Veins with Near- Infrared Light to Facilitate Blood Withdrawal in Children. Clin. Pediatr. 2011, 50, 508–512. [Google Scholar] [CrossRef]
- Liukui, C.; Zuojin, L.; Ying, W.; Yi, X. A design of infrared finger vein image acquisition terminal. Int. Conf. Bus. Manag. Electron. Inf. 2011, 4, 626–629. [Google Scholar] [CrossRef]
- Marathe, M.; Bhatt, N.S.; Sundararajan, R. A Novel Wireless Vein Finder. In Proceedings of the International Conference on Circuits, Communication, Control and Computing, Bangalore, India, 21–22 November 2014; Institute of Electrical and Electronics Engineers: IEEE: Piscataway, NJ, USA; pp. 277–280. [Google Scholar]
- Chakravorty, T.; Sonawane, D.N.; Sharma, S.D.; Patil, T. Low-cost subcutaneous vein detection system using ARM9 based single board computer. Int. Conf. Electron. Comput. Technol. 2011, 2, 339–343. [Google Scholar] [CrossRef]
- Ayoub, Y.; Serhal, S.; Farhat, B.; Ali, A.; Amatoury, J.; Nasser, H.; Ali, M. Diagnostic Superficial Vein Scanner. In Proceedings of the 2018 International Conference on Computer and Applications (ICCA), Beirut, Lebanon, 25–26 August 2018; IEEE: Piscataway, New Jersey, USA, 2018. ISBN 978-1-5386-4371-6/18. [Google Scholar]
- Kauba, C.; Uhl, A. Shedding Light on the Veins—Reflected Light or Transillumination in Hand-Vein Recognition. In Proceedings of the 2018 International Conference on Biometrics (ICB), Gold Coast, QLD, Australia, 20–23 February 2018; Institute of Electrical and Electronics Engineers (IEEE): Piscataway, NJ, USA; pp. 283–290. [Google Scholar]
- Freeman, E.E.; Semeere, A.; Osman, H.; Peterson, G.; Rajadhyaksha, M.; González, S.; Martin, J.N.; Anderson, R.R.; Tearney, G.J.; Kang, D. Smartphone confocal microscopy for imaging cellular structures in human skin in vivo. Biomed. Opt. Express 2018, 9, 1906–1915. [Google Scholar] [CrossRef] [Green Version]
- Meng, G.C.; Shahzad, A.; Saad, N.M.; Malik, A.S.; Mériaudeau, F.; Chuan, M.G. Prototype design for wearable veins localization system using near infrared imaging technique. Colloq. Signal Process. Appl. CSPA 2015, 112–115. [Google Scholar] [CrossRef]
- Ganesh, S. Depth and Size Limits for the Visibility of Veins Using the Vein Viewer Imaging System. Master’s Thesis, The University of Tennessee, Memphis, TN, USA, 2007. [Google Scholar]
- Chandra, F.; Wahyudianto, A.; Yasin, M. Design of vein finder with multi tuning wavelength using RGB LED. J. Phys. Conf. Ser. 2017, 853, 012019. [Google Scholar] [CrossRef]
- Anderson, R.R. Lasers in dermatology—A critical update. J. Dermatol. 2000, 27, 700–705. [Google Scholar] [CrossRef]
- Astner, S.; Anderson, R.R. Treating vascular lesions. Dermatol. Ther. 2005, 18, 267–281. [Google Scholar] [CrossRef] [PubMed]
- Mela, C.A.; Lemmer, D.P.; Bao, F.S.; Papay, F.; Hicks, T.; Liu, Y. Real-time dual-modal vein imaging system. Int. J. Comput. Assist. Radiol. Surg. 2019, 14, 203–213. [Google Scholar] [CrossRef]
- Peled, G.; Halak, M.; Blechman, Z. Peripheral vein locating techniques. Imaging Med. 2016, 8. [Google Scholar]
- China Medical Solution (CMS) Limited. Dr. Waffle. Available online: https://www.vein-finder.com (accessed on 20 September 2019).
- Lima-Oliveira, G.; Volanski, W.; Lippi, G.; Picheth, G.; Guidi, G.C. Pre-analytical phase management: A review of the procedures from patient preparation to laboratory analysis. Scand. J. Clin. Lab. Investig. 2017, 77, 153–163. [Google Scholar] [CrossRef]
- Dhakshayani, M.; Yacin, S. Economically Affordable and Clinically Reliable Vein Finder. In Proceedings of the 30th Indian Engineering Congress, the 21st Century Engineering: The Make in India Pathway, Guwahati, India, 17–20 December 2015; pp. 63–69. [Google Scholar]
- Shahzad, A.; Saad, M.N.; Walter, N.; Malik, A.S.; Mériaudeau, F. Hyperspectral venous image quality assessment for optimum illumination range selection based on skin tone characteristics. Biomed. Eng. Online 2014, 13, 109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amipongongctrch, P.; Khaosomboon, K.; Keawgun, T. Design and Construction of Median Cubital Vein Transillumination Device by Using LED. In Proceedings of the 2015 8th Biomedical Engineering International Conference (BMEiCON), Pattaya, Thailand, 25–27 November 2015; Institute of Electrical and Electronics Engineers (IEEE): Piscataway, NJ, USA; pp. 1–4. [Google Scholar]
- Wang, F.; Behrooz, A.; Morris, M.; Adibi, A. High-contrast subcutaneous vein detection and localization using multispectral imaging. J. Biomed. Opt. 2013, 18, 050504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yarlagadda, A.; Murthy, J.; Prasad, M. A novel method for human age group classification based on correlation fractal di-mension of facial edges. J. King Saud Univ. Comput. Inf. Sci. 2015, 27, 468–476. [Google Scholar]
- Lim, J.U.; Lee, J.; Kim, J.; Hwang, Y.; Kim, T.; Lim, S.; Yoo, K.; Jung, K.; Kim, Y.; Kook rhee, C. Comparison of World health Organization and Asia-Pacific body mass index classifications in COPD patients. Int. J. COPD 2017, 12, 2465–2475. [Google Scholar] [CrossRef] [Green Version]
- Ash, C.; Town, G.; Bjerring, P.; Webster, S. Evaluation of a novel skin tone meter and the correlation between Fitzpatrick skin type and skin color. Photon Lasers Med. 2015, 4, 177–186. [Google Scholar] [CrossRef]
- Krogera, K.; Oseb, C.; Rudofskya, G.; Roesenerb, J.; Weilandb., D.; Hircheb, H. Peripheral veins: Influence of gender, body mass index, age and varicose veins on cross-sectional area. Vasc. Med. 2003, 8, 249–255. [Google Scholar] [CrossRef] [Green Version]
- Kam, J.; Taylor, D.M. Obesity significantly increases the difficulty of patient management in the emergency department. Emerg. Med. Australas. 2010, 22, 316–323. [Google Scholar] [CrossRef]
- Accu Vein. Vein Visualization Technology. Available online: https://www.accuvein.com/why-accuvein/vein-visualization-technology/ (accessed on 15 June 2020).
- Asrar, M.; Al-Habaibeh, A.; Houda, M. Innovative algorithm to evaluate the capabilities of visual, near infrared, and infrared technologies for the detection of veins for intravenous cannulation. Appl. Opt. 2016, 55, D67. [Google Scholar] [CrossRef] [Green Version]
- Vein Viewer® Flex with HD Imaging and Df2 Technology. Available online: https://christiemed.com/products/vienviewer-models/veinviewer-flex/ (accessed on 15 June 2020).
- VascuLuminator Vein Imaging System Mk2 an Overview. Available online: https://www.do-pa.com/downloads/Vasculuminator/VasculuminatorMk2.pdf (accessed on 15 June 2020).



















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. of Subjects | Highly Visible | Visible | |
|---|---|---|---|
| Male | 88 | 56 | 32 |
| Female | 140 | 54 | 86 |
| TOTAL | 228 | 110 | 118 |
| No. of Subjects | Highly Visible | Visible | ||
|---|---|---|---|---|
| Child | 0–15 | 10 | 4 | 6 |
| Young adult | 16–30 | 173 | 87 | 86 |
| Middle-aged adult | 31–50 | 36 | 14 | 22 |
| Senior adult | >50 | 9 | 5 | 4 |
| TOTAL | 228 | 110 | 118 | |
| No. of Subjects | Highly Visible | Visible | ||
|---|---|---|---|---|
| Underweight | <18.5 | 23 | 12 | 11 |
| Normal | 18.5–22.9 | 74 | 47 | 27 |
| Overweight | 23.0–24.9 | 39 | 20 | 19 |
| Obese | ≥25.0 | 82 | 27 | 55 |
| TOTAL | 218 | 106 | 112 | |
| No. of Subjects | Highly Visible | Visible | ||
|---|---|---|---|---|
| Light complexion | II | 6 | 2 | 4 |
| Medium complexion | III | 84 | 43 | 41 |
| Darker complexion | IV | 133 | 65 | 68 |
| Dark complexion | V | 5 | 0 | 5 |
| TOTAL | 228 | 110 | 118 | |
| In Centimeter (cm) | No. of Subjects | Highly Visible | Visible |
|---|---|---|---|
| 30–34 | 10 | 2 | 8 |
| 25–29 | 89 | 43 | 46 |
| 20–24 | 123 | 62 | 61 |
| 15–19 | 6 | 3 | 3 |
| TOTAL | 228 | 110 | 118 |
| Ref No. | Gender | Age | BMI | Skin Tone | Arm Circumference | Remarks |
|---|---|---|---|---|---|---|
| 011 | F | 20 | O | III | 29 | Stretch marks |
| 046 | M | 21 | O | IV | 26 | Obese, Darker complexion |
| 058 | M | 19 | O | IV | 29 | Skin marks |
| 060 | F | 19 | O | IV | 27 | Skin marks |
| 069 | M | 19 | O | IV | 31 | Obese, Darker complexion |
| 095 | M | 50 | O | IV | 33 | Obese, Medium complexion |
| 112 | F | 18 | N | III | 24 | Tiny/deep vein * |
| 125 | F | 34 | O | IV | 26 | Obese, Darker complexion |
| 131 | F | 21 | UW | III | 21 | Tiny/deep vein * |
| 228 | F | 20 | N | III | 21 | Tiny/deep vein * |
| 232 | M | 39 | O | IV | 29 | Stretch marks |
| 233 | M | 67 | OW | V | 26 | Stretch marks |
| 241 | F | 13 | NA | III | 23 | Child, Tiny/deep vein * |
| 245 | F | 2 | NA | III | 15 | Child, Tiny/deep vein * |
| No. of Subjects | Highly Visible | Visible | |
|---|---|---|---|
| Male | 93 | 57 | 36 |
| Female | 149 | 64 | 85 |
| TOTAL | 242 | 121 | 121 |
| No. of Subjects | Highly Visible | Visible | ||
|---|---|---|---|---|
| Child | 0–15 | 12 | 2 | 10 |
| Young adult | 16–30 | 181 | 97 | 84 |
| Middle-aged adult | 31–50 | 39 | 18 | 21 |
| Senior adult | >50 | 10 | 4 | 6 |
| TOTAL | 242 | 121 | 121 | |
| No. of Subjects | Highly Visible | Visible | ||
|---|---|---|---|---|
| Underweight | <18.5 | 24 | 8 | 16 |
| Normal | 18.5–22.9 | 76 | 47 | 29 |
| Overweight | 23–24.9 | 40 | 24 | 16 |
| Obese | ≥25 | 90 | 40 | 50 |
| TOTAL | 230 | 119 | 111 | |
| No. of Subjects | Highly Visible | Visible | ||
|---|---|---|---|---|
| Light complexion | II | 6 | 2 | 4 |
| Medium complexion | III | 91 | 47 | 44 |
| Darker complexion | IV | 139 | 70 | 69 |
| Dark complexion | V | 6 | 2 | 4 |
| TOTAL | 242 | 121 | 121 | |
| Parameters | Developed Vein Finder Device | Commercial Vein Finder Devices |
|---|---|---|
| 1. Minimal used components (for the vein finder prototype) | a. 3 NIR LED (Fongsam) 960 nm b. IR (IMX238 Sony) CMOS camera with IR filter c. Free software and laptop as the image processing unit d. Power consumption: 4.5 V e. Size: 7 × 9 × 10 cm f. Working distance: 15–20 cm g. Weight: 0.4 kg | 1. AccuVein (AccuVein Inc.) a. two safe barcode-scanner class lasers: an invisible infrared and a visible red b. Dual lens [47] c. Projector system [48] d. Power consumption: 3.6 V, 180 min lasting, 3100 mAh e. Size: 5 × 6 × 20 cm f. Working distance: 10 to 45 cm g. Weight: 0.275 kg [47] 2. VeinViewer Flex (Christie Medical Holdings Inc.) a. NIR light (Minimum of 5 lumens) b. HD imaging and exclusive Df2 (digital full field) technology [49] c. Projector system [48] d. Power consumption: Fast-swap lithium ion batteries or AC (outlet) Up to 2 h continuous run time per battery e. Size: 29.464 × 10.16 × 4.318 cm f. Working distance: 30 cm g. Weight: 0.7 kg [49] 3. VascuLuminator (DKMP) a. LED, SFH 4235, (Osram, Munich, Germany) 850 nm [22] b. IR CCD camera with VGA resolution (640 × 480) and adjustable focus lens with IR filter. [22] c. Monitor LCD system [48] d. Power consumption: DKMS bv charger type 330–00 at least 8 h e. Size: 54 × 48 × 170 cm (when assembled) [50] f. Working distance: ∼20 cm [22] g. Weight: 23 kg [50] |
| 2. Estimated cost in USD (Highly reproducible based on its production cost) | 80–100 | 4000 to 7000 [36] |
| 3. Reliability Rate (%) a. Human in-vitro testing | Arm site: 94.21% Dorsal hand site: 100.00% of the 242 human subjects | 93.00% [35] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Francisco, M.D.; Chen, W.-F.; Pan, C.-T.; Lin, M.-C.; Wen, Z.-H.; Liao, C.-F.; Shiue, Y.-L. Competitive Real-Time Near Infrared (NIR) Vein Finder Imaging Device to Improve Peripheral Subcutaneous Vein Selection in Venipuncture for Clinical Laboratory Testing. Micromachines 2021, 12, 373. https://doi.org/10.3390/mi12040373
Francisco MD, Chen W-F, Pan C-T, Lin M-C, Wen Z-H, Liao C-F, Shiue Y-L. Competitive Real-Time Near Infrared (NIR) Vein Finder Imaging Device to Improve Peripheral Subcutaneous Vein Selection in Venipuncture for Clinical Laboratory Testing. Micromachines. 2021; 12(4):373. https://doi.org/10.3390/mi12040373
Chicago/Turabian StyleFrancisco, Mark D., Wen-Fan Chen, Cheng-Tang Pan, Ming-Cheng Lin, Zhi-Hong Wen, Chien-Feng Liao, and Yow-Ling Shiue. 2021. "Competitive Real-Time Near Infrared (NIR) Vein Finder Imaging Device to Improve Peripheral Subcutaneous Vein Selection in Venipuncture for Clinical Laboratory Testing" Micromachines 12, no. 4: 373. https://doi.org/10.3390/mi12040373