Plasma Lipid Profiling of Three Types of Drug-Induced Liver Injury in Japanese Patients: A Preliminary Study

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Results
2.1. DILI Patients Recruited in the Present Study
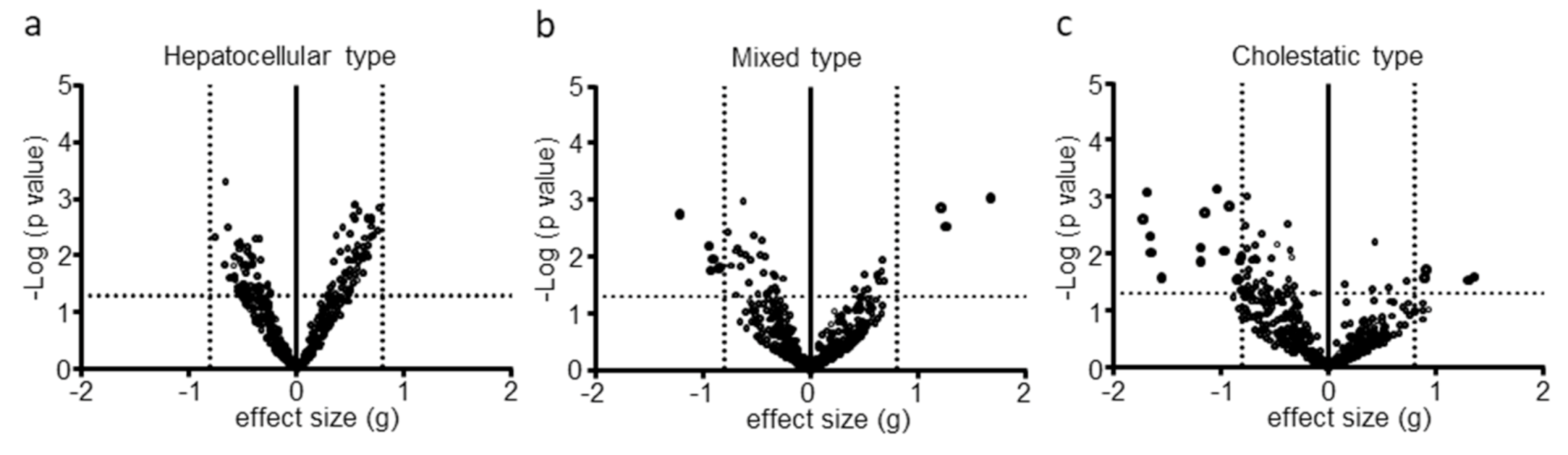
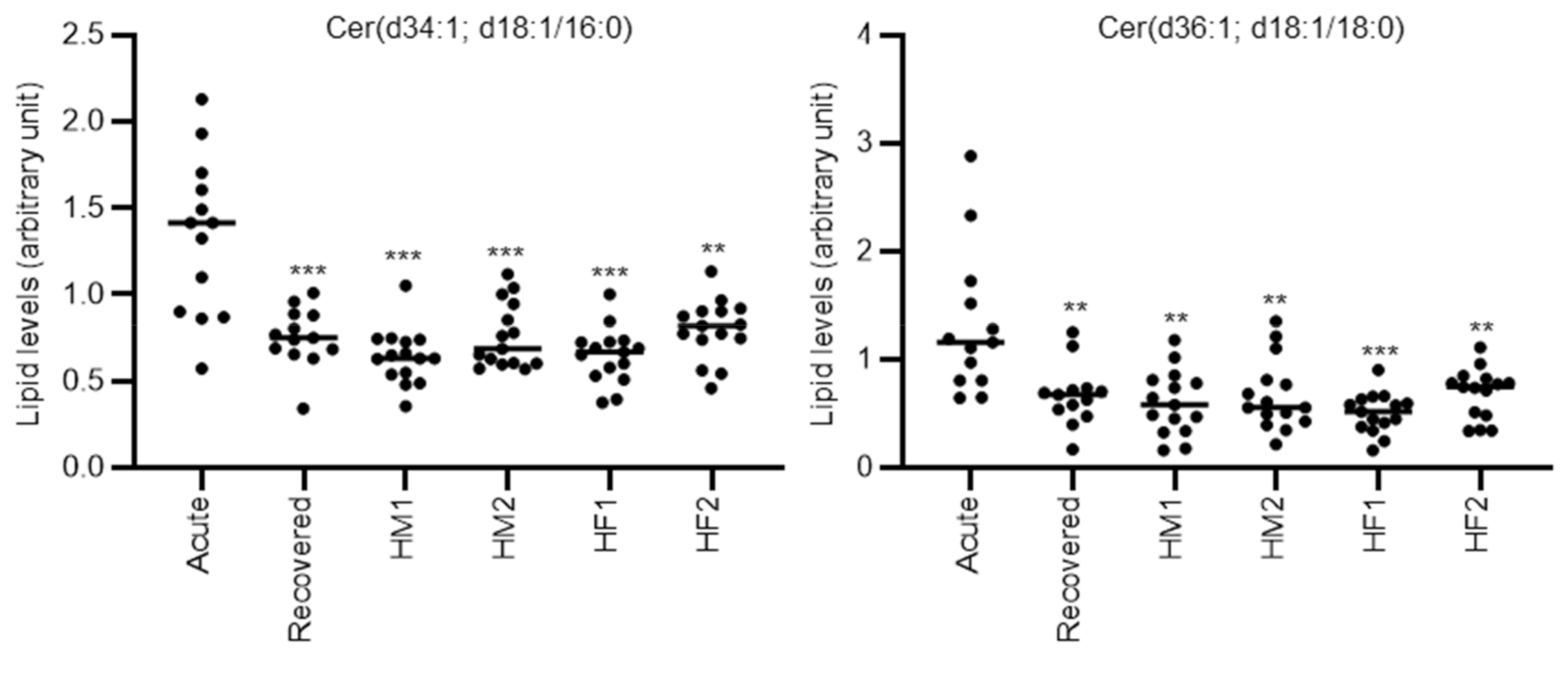
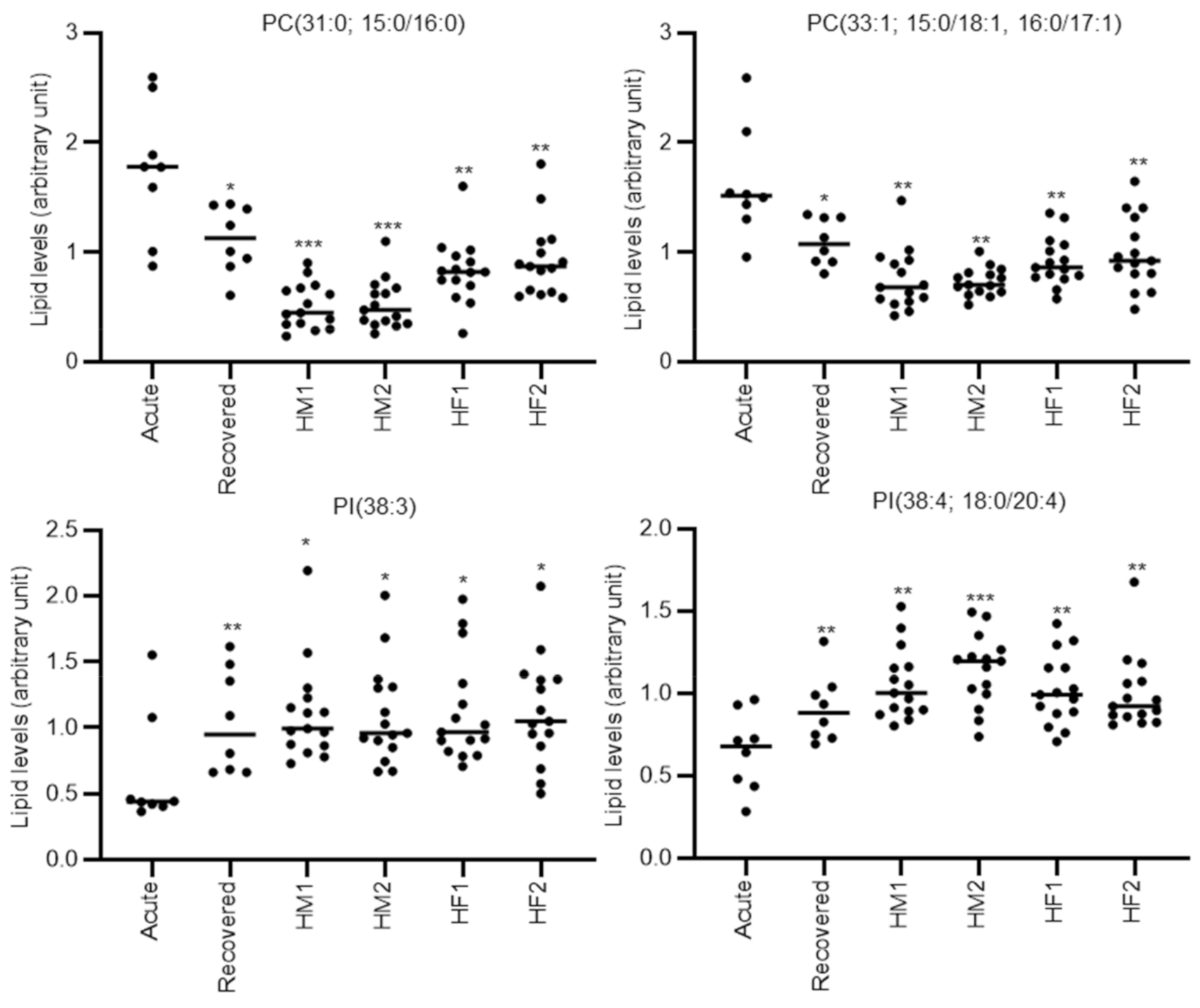
2.2. Global Plasma Lipid Profiling in the Three DILI Types
2.3. Discrimination Ability for Mixed-Type DILI between Acute Phase and Recovery Phase or Healthy Volunteers
2.4. Discrimination Ability for Cholestatic-Type DILI between Acute Phase and Recovery Phase or Healthy Volunteers
3. Discussion
4. Materials and Methods
4.1. Subjects and Sample Collection
4.2. Lipidomics
4.3. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Smith, D.A.; Schmid, E.F. Drug withdrawals and the lessons within. Curr. Opin. Drug Discov. Dev. 2006, 9, 38–46. [Google Scholar]
- Ostapowicz, G.; Fontana, R.J.; Schiødt, F.V.; Larson, A.; Davern, T.J.; Han, S.H.; McCashland, T.M.; Shakil, A.O.; Hay, J.E.; Hynan, L.; et al. Results of a prospective study of acute liver failure at 17 tertiary care centers in the United States. Ann. Intern. Med. 2002, 137, 947–954. [Google Scholar] [CrossRef] [PubMed]
- Danan, G.; Benichou, C. Causality assessment of adverse reactions to drugs-I. A novel method based on the conclusions of international consensus meetings: Application to drug-induced liver injuries. J. Clin. Epidemiol. 1993, 46, 1323–1330. [Google Scholar] [CrossRef]
- Takikawa, H.; Onji, M.; Takamori, Y.; Murata, Y.; Taniguchi, H.; Ito, T.; Watanabe, M.; Ayada, M.; Maeda, N.; Nomoto, M.; et al. Proposal of diagnostic criteria for drug-induced liver injury revised by the DDW-J 2004 Workshop. Kanzo 2005, 46, 85–90. (In Japanese) [Google Scholar] [CrossRef] [Green Version]
- Takikawa, H.; Onji, M. A proposal of the diagnostic scale of drug-induced liver injury. Hepatol. Res. 2005, 2, 250–251. [Google Scholar] [CrossRef] [PubMed]
- David, S.; Hamilton, J.P. Drug-induced Liver Injury. US Gastroenterol. Hepatol. Rev. 2010, 6, 73–80. [Google Scholar] [PubMed]
- Katarey, D.; Verma, S. Drug-induced liver injury. Clin. Med. 2016, 16 (Suppl. 6), s104–s109. [Google Scholar] [CrossRef]
- Park, B.K.; Kitteringham, N.R.; Maggs, J.L.; Pirmohamed, M.; Williams, D.P. The role of metabolic activation in drug-induced hepatotoxicity. Annu. Rev. Pharmacol. Toxicol. 2005, 45, 177–202. [Google Scholar] [CrossRef]
- Mené, P.; Simonson, M.S.; Dunn, M.J. Phospholipids in signal transduction of mesangial cells. Am. J. Physiol. 1989, 256, F375–F386. [Google Scholar] [CrossRef]
- Hannun, Y.A.; Linardic, C.M. Sphingolipid breakdown products: Anti-proliferative and tumor-suppressor lipids. Biochim. Biophys. Acta 1993, 1154, 223–236. [Google Scholar] [CrossRef]
- Kolesnick, R.N.; Haimovitz-Friedman, A.; Fuks, Z. The sphingomyelin signal transduction pathway mediates apoptosis for tumor necrosis factor, Fas, and ionizing radiation. Biochem. Cell Biol. 1994, 72, 471–474. [Google Scholar] [CrossRef] [PubMed]
- Ridgway, N.D. The role of phosphatidylcholine and choline metabolites to cell proliferation and survival. Crit. Rev. Biochem. Mol. Biol. 2013, 48, 20–38. [Google Scholar] [CrossRef] [PubMed]
- Kotronen, A.; Seppänen-Laakso, T.; Westerbacka, J.; Kiviluoto, T.; Arola, J.; Ruskeepää, A.L.; Yki-Järvinen, H.; Oresic, M. Comparison of lipid and fatty acid composition of the liver, subcutaneous and intra-abdominal adipose tissue, and serum. Obesity 2010, 18, 937–944. [Google Scholar] [CrossRef] [PubMed]
- Houjou, T.; Yamatani, K.; Imagawa, M.; Shimizu, T.; Taguchi, R. A shotgun tandem mass spectrometric analysis of phospholipids with normal-phase and/or reverse-phase liquid chromatography/electrospray ionization mass spectrometry. Rapid Commun. Mass Spectrom. 2005, 19, 654–666. [Google Scholar] [CrossRef]
- Han, X.; Gross, R.W. Shotgun lipidomics: Electrospray ionization mass spectrometric analysis and quantitation of cellular lipidomes directly from crude extracts of biological samples. Mass Spectrom. Rev. 2005, 24, 367–412. [Google Scholar] [CrossRef]
- Meikle, P.J.; Christopher, M.J. Lipidomics is providing new insight into the metabolic syndrome and its sequelae. Curr. Opin. Lipidol. 2011, 22, 210–215. [Google Scholar] [CrossRef]
- Quehenberger, O.; Armando, A.M.; Brown, A.H.; Milne, S.B.; Myers, D.S.; Merrill, A.H.; Bandyopadhyay, S.; Jones, K.N.; Kelly, S.; Shaner, R.L.; et al. Lipidomics reveals a remarkable diversity of lipids in human plasma. J. Lipid Res. 2010, 51, 3299–3305. [Google Scholar] [CrossRef] [Green Version]
- Patterson, A.D.; Maurhofer, O.; Beyoglu, D.; Lanz, C.; Krausz, K.W.; Pabst, T.; Gonzalez, F.J.; Dufour, J.F.; Idle, J.R. Aberrant lipid metabolism in hepatocellular carcinoma revealed by plasma metabolomics and lipid profiling. Cancer Res. 2011, 71, 6590–6600. [Google Scholar] [CrossRef] [Green Version]
- Chen, S.; Yin, P.; Zhao, X.; Xing, W.; Hu, C.; Zhou, L.; Xu, G. Serum lipid profiling of patients with chronic hepatitis B, cirrhosis, and hepatocellular carcinoma by ultra-fast LC/IT-TOF MS. Electrophoresis 2013, 34, 2848–2856. [Google Scholar] [CrossRef]
- Saito, K.; Maekawa, K.; Ishikawa, M.; Senoo, Y.; Urata, M.; Murayama, M.; Nakatsu, N.; Yamada, H.; Saito, Y. Glucosylceramide and lysophosphatidylcholines as potential blood biomarkers for drug-induced hepatic phospholipidosis. Toxicol. Sci. 2014, 141, 377–386. [Google Scholar] [CrossRef] [Green Version]
- Puri, P.; Wiest, M.M.; Cheung, O.; Mirshahi, F.; Sargeant, C.; Min, H.K.; Contos, M.J.; Sterling, R.K.; Fuchs, M.; Zhou, H.; et al. The plasma lipidomic signature of nonalcoholic steatohepatitis. Hepatology 2009, 50, 1827–1838. [Google Scholar] [CrossRef] [Green Version]
- Wu, J.M.; Xu, Y.; Skill, N.J.; Sheng, H.; Zhao, Z.; Yu, M.; Saxena, R.; Maluccio, M.A. Autotaxin expression and its connection with the TNF-alpha-NF-kappaB axis in human hepatocellular carcinoma. Mol. Cancer 2010, 9, 71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agellon, L.B.; Walkey, C.J.; Vance, D.E.; Kuipers, F.; Verkade, H.J. The unique acyl chain specificity of biliary phosphatidylcholines in mice is independent of their biosynthetic origin in the liver. Hepatology 1999, 30, 725–729. [Google Scholar] [CrossRef]
- Robins, S.J.; Fasulo, J.M.; Robins, V.F.; Patton, G.M. Utilization of different fatty acids for hepatic and biliary phosphatidylcholine formation and the effect of changes in phosphatidylcholine molecular species on biliary lipid secretion. J. Lipid Res. 1991, 32, 985–992. [Google Scholar] [PubMed]
- Shirouchi, B.; Nagao, K.; Inoue, N.; Furuya, K.; Koga, S.; Matsumoto, H.; Yanagita, T. Dietary phosphatidylinositol prevents the development of nonalcoholic fatty liver disease in Zucker (fa/fa) rats. J. Agric. Food Chem. 2008, 56, 2375–2379. [Google Scholar] [CrossRef] [PubMed]
- Ma, D.W.; Arendt, B.M.; Hillyer, L.M.; Fung, S.K.; McGilvray, I.; Guindi, M.; Allard, J.P. Plasma phospholipids and fatty acid composition differ between liver biopsy-proven nonalcoholic fatty liver disease and healthy subjects. Nutr. Diabetes 2016, 6, e220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saito, K.; Uebanso, T.; Maekawa, K.; Ishikawa, M.; Taguchi, R.; Nammo, T.; Nishimaki-Mogami, T.; Udagawa, H.; Fujii, M.; Shibazaki, Y.; et al. Characterization of hepatic lipid profiles in a mouse model with nonalcoholic steatohepatitis and subsequent fibrosis. Sci. Rep. 2015, 5, 12466. [Google Scholar] [CrossRef] [Green Version]
- Goda, K.; Saito, K.; Muta, K.; Kobayashi, A.; Saito, Y.; Sugai, S. Ether-phosphatidylcholine characterized by consolidated plasma and liver lipidomics is a predictive biomarker for valproic acid-induced hepatic steatosis. J. Toxicol. Sci. 2018, 43, 395–405. [Google Scholar] [CrossRef] [Green Version]
- da Silva, T.F.; Sousa, V.F.; Malheiro, A.R.; Brites, P. The importance of ether-phospholipids: A view from the perspective of mouse models. Biochim. Biophys. Acta 2012, 1822, 1501–1508. [Google Scholar] [CrossRef] [Green Version]
- Brites, P.; Ferreira, A.S.; Ferreira da Silva, T.; Sousa, V.F.; Malheiro, A.R.; Duran, M.; Waterham, H.R.; Baes, M.; Wanders, R.J.A. 2 Alkyl-Glycerol Rescues Plasmalogen Levels and Pathology of Ether-Phospholipid Deficient Mice. PLoS ONE, 2011; 6, e28539. [Google Scholar]
- Jang, J.E.; Park, H.S.; Yoo, H.J.; Baek, I.J.; Yoon, J.E.; Ko, M.S.; Kim, A.R.; Kim, H.S.; Park, H.S.; Lee, S.E.; et al. Protective role of endogenous plasmalogens against hepatic steatosis and steatohepatitis in mice. Hepatology 2017, 66, 416–431. [Google Scholar] [CrossRef] [Green Version]
- Teichgräber, V.; Ulrich, M.; Endlich, N.; Riethmüller, J.; Wilker, B.; Conceição De Oliveira-Munding, C.; van Heeckeren, A.M.; Barr, M.L.; von Kürthy, G.; Schmid, K.W.; et al. Ceramide accumulation mediates inflammation, cell death and infection susceptibility in cystic fibrosis. Nat. Med. 2008, 14, 382–391. [Google Scholar] [CrossRef] [PubMed]
- Colombini, M. Ceramide channels and their role in mitochondria-mediated apoptosis. Biochim. Biophys. Acta 2010, 1797, 1239–1244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shea, B.S.; Tager, A.M. Sphingolipid regulation of tissue fibrosis. Open Rheumatol. J. 2012, 6, 123–129. [Google Scholar] [CrossRef]
- Ziobro, R.; Henry, B.; Edwards, M.J.; Lentsch, A.B.; Gulbins, E. Ceramide mediates lung fibrosis in cystic fibrosis. Biochem. Biophys. Res. Commun. 2013, 434, 705–709. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moriya, T.; Satomi, Y.; Kobayashi, H. Metabolomics of postprandial plasma alterations: A comprehensive Japanese study. J. Biochem. 2018, 163, 113–121. [Google Scholar] [CrossRef]
- Saito, K.; Hattori, K.; Andou, T.; Satomi, Y.; Gotou, M.; Kobayashi, H.; Hidese, S.; Kunugi, H. Characterization of postprandial effects on CSF metabolomics: A pilot study with parallel comparison to plasma. Metabolites 2020, 10, 185. [Google Scholar] [CrossRef]
- Takikawa, H.; Murata, Y.; Horiike, N.; Fukui, H.; Onji, M. Drug-induced liver injury in Japan: An analysis of 1676 cases between 1997 and 2006. Hepatol. Res. 2009, 39, 427–431. [Google Scholar] [CrossRef]
- Aiso, M.; Takikawa, H.; Tsuji, K.; Kagawa, T.; Watanabe, M.; Tanaka, A.; Sato, K.; Sakisaka, S.; Hiasa, Y.; Takei, Y.; et al. Analysis of 307 cases with drug-induced liver injury between 2010 and 2018 in Japan. Hepatol. Res. 2019, 49, 105–110. [Google Scholar] [CrossRef] [Green Version]
- Saito, K.; Ikeda, M.; Kojima, Y.; Hosoi, H.; Saito, Y.; Kondo, S. Lipid profiling of pre-treatment plasma reveals biomarker candidates associated with response rates and hand-foot skin reactions in sorafenib-treated patients. Cancer Chemother. Pharmacol. 2018, 82, 677–684. [Google Scholar] [CrossRef]
- Saito, K.; Ohno, Y.; Saito, Y. Enrichment of resolving power improves ion-peak quantification on a lipidomics platform. J. Chromatogr. B Analyt. Technol. Biomed. Life Sci. 2017, 1055, 20–28. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| DILI Type | Hepatocellular | Mixed | Cholestatic |
|---|---|---|---|
| no. of subjects | 33 | 13 | 8 |
| CIOMS/RUCAM scale; median (quartile) | 8 (7–9) | 9 (7–9) | 8 (7.5–9) |
| DDW-J 2004 score; median (quartile) | 8 (7–9) | 8 (7–8) | 8 (7–8.5) |
| Sex; male/female | 11/22 | 9/4 | 4/4 |
| Age; median (quartile) | 56 (46–68) | 60 (57–76) | 69 (64.5–72.5) |
| BMI; median (quartile) | 22.7 (19.8–24.1) | 22.1 (21.3–23.3) | 25.3 (22.8–26.1) |
| acute phase AST(U/L); median (quartile) | 239 (102–526) | 130 (96–191) | 81 (55.75–200.5) |
| acute phase ALT(U/L); median (quartile) | 336 (204–963) | 196 (161–423) | 97 (84.75–131) |
| acute phase ALP(U/L); median (quartile) | 360 (277–410) | 555 (448–914) | 1465 (1129.5–1721.5) |
| acute phase T. Bil(mg/dl); median (quartile) | 1 (0.7–2.2) | 0.6 (0.5–1.3) | 1.5 (0.8–3.65) |
| recovered phase AST(U/L); median (quartile) | 23 (19–29) | 31 (20–34) | 28.5 (19.5–30.25) |
| recovered phase ALT(U/L); median (quartile) | 25 (17–35) | 32 (23–48) | 22 (15–30.25) |
| recovered phase ALP(U/L); median (quartile) | 249 (185.75–324.75) | 316 (244–373) | 266.5 (190.25–332) |
| recovered phase T. Bil(mg/dl); median (quartile) | 0.7 (0.525–0.975) | 0.65 (0.5–0.925) | 0.7 (0.6–0.9) |
| Cause | |||
| -Prescribed drugs | 26 | 10 | 6 |
| -Other | 1 | 1 | 0 |
| -Undefined | 6 | 2 | 2 |
| Suspected drugs; ad. in over 2 DILI patients | |||
| -Acetaminophen | 2 | 1 | 0 |
| -Cefditoren | 2 | 0 | 0 |
| -Cyclophosphamide | 2 | 0 | 0 |
| -Febuxostat | 0 | 1 | 1 |
| -Gemcitabine | 2 | 0 | 0 |
| -Loxoprofen | 2 | 1 | 1 |
| -Nifedipine | 1 | 0 | 1 |
| ATC level 2 of suspected drugs; ad. in over 3 DILI patients (ATC code in parenthesis) | |||
| -calcium channel blockers (C08) | 2 | 0 | 1 |
| -antibacterials for systemic use (J01) | 6 | 2 | 0 |
| -antineoplastic agents (L01) | 5 | 1 | 0 |
| -anti-inflammatory and antirheumatic products (M01) | 3 | 2 | 1 |
| -psycholeptics (N05) | 4 | 1 | 1 |
| Category | Class (Abbreviation) | Class | Number of Lipids |
|---|---|---|---|
| Phosphoglycerolipid | LPC | Lysophosphatidylcholine | 12 |
| Phosphoglycerolipid | LPCe | Ether-type lysophosphatidylcholine | 2 |
| Phosphoglycerolipid | LPE | Lysophosphatidylethanolamine | 5 |
| Phosphoglycerolipid | LPEe | Ether-type lysophosphatidylethanolamine | 1 |
| Phosphoglycerolipid | LPI | Lysophosphaidylinositol | 2 |
| Phosphoglycerolipid | PC | Phosphatidylcholine | 56 |
| Phosphoglycerolipid | PC+O | Oxidized phosphatidylcholine | 2 |
| Phosphoglycerolipid | ether-linked PC | Ether-type phosphatidylcholine | 40 |
| Phosphoglycerolipid | PE | Phosphatidylethanolamine | 15 |
| Phosphoglycerolipid | ether-linked PE | Ether-type phosphatidylethanolamine | 29 |
| Phosphoglycerolipid | PI | Phosphatidylinositol | 18 |
| Phosphoglycerolipid | PS | Phosphatidylserine | 2 |
| Sphingolipid | Cer | Ceramide | 14 |
| Sphingolipid | CerG1 | Monoglycosylceramide | 6 |
| Sphingolipid | CerG1+O | Oxidized monoglycosylceramide | 3 |
| Sphingolipid | CerG2 | Diglycosylceramide | 4 |
| Sphingolipid | CerG3 | Triglycosylceramide | 4 |
| Sphingolipid | Gb4 | Ganglioside Gb4 | 1 |
| Sphingolipid | GM3 | Ganglioside GM3 | 7 |
| Sphingolipid | GM3+O | Oxidized ganglioside GM3 | 1 |
| Sphingolipid | SM | Sphingomyelin | 37 |
| Sphingolipid | SM+O | Oxidized sphingomyelin | 2 |
| Sphingolipid | Su1G1 | Sulfatide | 1 |
| Neutral lipid | ChE | Cholesterolester | 19 |
| Neutral lipid | DG | Diacylglycerol | 22 |
| Neutral lipid | TG | Triacylglycerol | 138 |
| Other lipid | Car | Acylcarnitine | 6 |
| Other lipid | CoQ | CoenzymeQ | 1 |
| Other lipid | FA | Fatty acid | 5 |
| Other lipid | FAA | Fatty amide | 5 |
| Other lipid | Other | Other | 3 |
| vs. Recovered Phase | vs. Healthy M1 | vs. Healthy M2 | vs. Healthy F1 | vs. Healthy F2 | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Metabolite ID | Name | p Value | Effect Size | ROC–AUC | p Value | Effect Size | ROC–AUC | p Value | Effect Size | ROC–AUC | p Value | Effect Size | ROC–AUC | p Value | Effect Size | ROC–AUC |
| M008 | LPC(18:2) | 1.07 × 10−2 | −0.91 | 0.75 | 4.09 × 10−3 | −1.17 | 0.81 | 3.85 × 10−5 | −1.85 | 0.91 | 2.94 × 10−2 | −0.89 | 0.72 | 3.06 × 10−2 | −0.85 | 0.72 |
| M014 | LPC(16:1e) | 6.48 × 10−3 | −0.94 | 0.78 | 3.40 × 10−4 | −1.6 | 0.89 | 3.16 × 10−5 | −2 | 0.9 | 1.24 × 10−2 | −1 | 0.79 | 8.68 × 10−4 | −1.4 | 0.85 |
| M104 | PC(38:6e) | 1.74 × 10−2 | −0.93 | 0.78 | 8.23 × 10−2 | −0.67 | 0.71 | 3.46 × 10−2 | −0.82 | 0.72 | 2.84 × 10−2 | −0.86 | 0.75 | 3.72 × 10−3 | −1.2 | 0.78 |
| M140 | PE(36:4e) | 1.52 × 10−2 | −0.85 | 0.76 | 2.70 × 10−1 | −0.43 | 0.69 | 3.60 × 10−1 | −0.36 | 0.66 | 5.05 × 10−3 | −1.14 | 0.84 | 2.13 × 10−1 | −0.49 | 0.74 |
| M146 | PE(38:4e) | 1.74 × 10−3 | −1.22 | 0.82 | 2.74 × 10−1 | −0.4 | 0.56 | 1.00 × 10−1 | −0.62 | 0.67 | 2.60 × 10−3 | −1.24 | 0.82 | 3.24 × 10−2 | −0.84 | 0.73 |
| M151 | PE(38:6e) | 1.61 × 10−2 | −0.85 | 0.75 | 2.21 × 10−2 | −0.9 | 0.73 | 6.88 × 10−3 | −1.09 | 0.76 | 5.98 × 10−3 | −1.14 | 0.79 | 1.60 × 10−2 | −0.96 | 0.75 |
| M185 | Cer(d34:1) | 9.02 × 10−4 | 1.68 | 0.87 | 1.21 × 10−4 | 2.08 | 0.93 | 7.00 × 10−4 | 1.69 | 0.87 | 1.33 × 10−4 | 2.06 | 0.93 | 1.18 × 10−3 | 1.6 | 0.85 |
| M186 | Cer(d36:1) | 2.90 × 10−3 | 1.26 | 0.86 | 2.62 × 10−3 | 1.42 | 0.88 | 5.66 × 10−3 | 1.26 | 0.85 | 8.77 × 10−4 | 1.71 | 0.96 | 5.91 × 10−3 | 1.29 | 0.85 |
| M224 | GM3(d34:1)+O | 1.37 × 10−3 | 1.22 | 0.83 | 9.78 × 10−5 | 2.23 | 0.94 | 2.30 × 10−4 | 1.97 | 0.91 | 6.28 × 10−4 | 1.75 | 0.89 | 2.33 × 10−3 | 1.49 | 0.81 |
| vs. Recovered Phase | vs. Healthy M1 | vs. Healthy M2 | vs. Healthy F1 | vs. Healthy F2 | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Metabolite ID | Name | p Value | Effect Size | ROC–AUC | p value | Effect SIZE | ROC–AUC | p Value | Effect Size | ROC–AUC | p Value | Effect Size | ROC-AUC | p Value | Effect Size | ROC–AUC |
| M023 | PC(30:0) | 2.68 × 10−2 | 0.89 | 0.72 | 3.05 × 10−3 | 2.59 | 0.99 | 5.61 × 10−3 | 2.23 | 0.96 | 1.54 × 10−2 | 1.66 | 0.89 | 3.39 × 10−2 | 1.31 | 0.82 |
| M024 | PC(31:0) | 2.92 × 10−2 | 1.31 | 0.84 | 5.89 × 10−4 | 3.16 | 0.99 | 6.21 × 10−4 | 3.06 | 0.98 | 3.25 × 10−3 | 2.16 | 0.93 | 6.31 × 10−3 | 1.82 | 0.88 |
| M026 | PC(32:1) | 1.90 × 10−2 | 0.91 | 0.72 | 7.82 × 10−3 | 2.23 | 0.98 | 1.10 × 10−2 | 2.05 | 0.94 | 1.86 × 10−2 | 1.74 | 0.87 | 2.73 × 10−2 | 1.57 | 0.83 |
| M028 | PC(33:1) | 2.60 × 10−2 | 1.36 | 0.88 | 1.29 × 10−3 | 2.37 | 0.96 | 1.44 × 10−3 | 2.88 | 0.99 | 4.99 × 10−3 | 2.05 | 0.94 | 9.55 × 10−3 | 1.58 | 0.88 |
| M096 | PC(36:5e) | 4.36 × 10−2 | −0.8 | 0.69 | 1.27 × 10−2 | −1.45 | 0.83 | 8.67 × 10−3 | −1.14 | 0.8 | 6.55 × 10−3 | −1.45 | 0.86 | 2.30 × 10−2 | −1.24 | 0.77 |
| M104 | PC(38:6e) | 1.45 × 10−3 | −0.92 | 0.73 | 5.38 × 10−2 | −1.06 | 0.78 | 2.23 × 10−2 | −1.09 | 0.81 | 2.41 × 10−2 | −1.16 | 0.78 | 1.46 × 10−2 | -1.49 | 0.83 |
| M140 | PE(36:4e) | 9.57 × 10−3 | −1.65 | 0.86 | 7.10 × 10−2 | −0.78 | 0.73 | 1.03 × 10−1 | −0.7 | 0.74 | 1.18 × 10−3 | −1.39 | 0.88 | 5.27 × 10−2 | −0.85 | 0.76 |
| M146 | PE(38:4e) | 2.68 × 10−2 | −1.55 | 0.89 | 9.48 × 10−2 | −0.62 | 0.68 | 2.93 × 10−2 | −0.85 | 0.78 | 8.03 × 10−4 | −1.38 | 0.91 | 9.08 × 10−3 | −1.2 | 0.84 |
| M157 | PE(40:6e) | 4.92 × 10−3 | −1.66 | 0.89 | 6.09 × 10−2 | −0.69 | 0.72 | 8.24 × 10−3 | −0.99 | 0.88 | 6.23 × 10−5 | −1.83 | 0.95 | 2.43 × 10−4 | −1.61 | 0.98 |
| M160 | PE(40:7e) | 2.45 × 10−3 | −1.73 | 0.91 | 4.44 × 10−2 | −0.76 | 0.74 | 2.30 × 10−4 | −1.63 | 0.96 | 8.09 × 10−5 | −1.73 | 0.93 | 2.99 × 10−4 | −1.65 | 0.94 |
| M161 | PE(40:7e) | 1.11 × 10−2 | −0.8 | 0.75 | 3.58 × 10−1 | −0.42 | 0.61 | 1.12 × 10−2 | −1.24 | 0.81 | 4.52 × 10−2 | −0.98 | 0.73 | 6.81 × 10−3 | −1.44 | 0.84 |
| M174 | PI(38:3) | 8.80 × 10−3 | −0.96 | 0.83 | 2.36 × 10−2 | −1.18 | 0.83 | 2.72 × 10−2 | −1.14 | 0.82 | 2.15 × 10−2 | −1.17 | 0.82 | 2.28 × 10−2 | −1.14 | 0.83 |
| M175 | PI(38:4) | 7.65 × 10−3 | −1.18 | 0.83 | 1.24 × 10−3 | −1.85 | 0.9 | 2.65 × 10−4 | −2.2 | 0.95 | 2.56 × 10−3 | −1.68 | 0.88 | 3.88 × 10−3 | −1.54 | 0.86 |
| M179 | PI(40:4) | 1.90 × 10−3 | −1.15 | 0.82 | 1.19 × 10−1 | -0.86 | 0.73 | 5.49 × 10−2 | −1.07 | 0.74 | 9.32 × 10−3 | −1.41 | 0.78 | 7.07 × 10−2 | −1.09 | 0.71 |
| M213 | CerG3(d40:1) | 1.38 × 10−2 | −1.19 | 0.81 | 7.12 × 10−2 | −0.69 | 0.7 | 2.04 × 10−3 | −1.26 | 0.86 | 4.20 × 10−3 | −1.19 | 0.84 | 3.09 × 10−5 | −1.9 | 0.96 |
| M214 | CerG3(d42:1) | 8.26 × 10−4 | −1.68 | 0.86 | 5.45 × 10−2 | −0.78 | 0.72 | 2.75 × 10−3 | −1.17 | 0.88 | 8.50 × 10−3 | −1.06 | 0.81 | 2.85 × 10−6 | −2.39 | 0.98 |
| M215 | CerG3(d42:2) | 1.34 × 10−2 | −0.82 | 0.69 | 6.34 × 10−2 | 0.88 | 0.78 | 9.13 × 10−1 | 0.04 | 0.58 | 4.44 × 10−1 | 0.34 | 0.62 | 2.92 × 10−1 | −0.53 | 0.61 |
| M243 | SM(d40:1) | 2.86 × 10−2 | −0.84 | 0.77 | 6.17 × 10−3 | −1.82 | 0.89 | 8.18 × 10−4 | −2.33 | 0.97 | 8.43 × 10−3 | −1.77 | 0.89 | 7.56 × 10−4 | −1.95 | 0.97 |
| M316 | TG(44:0) | 2.79 × 10−2 | −0.84 | 0.78 | 4.52E-01 | 0.38 | 0.67 | 3.30E-01 | 0.56 | 0.62 | 2.11 × 10−1 | 0.79 | 0.68 | 8.15 × 10−1 | 0.11 | 0.5 |
| M450 | CoQ10 | 7.22 × 10−4 | −1.04 | 0.8 | 5.17 × 10−3 | −1.55 | 0.85 | 1.79 × 10−3 | −1.96 | 0.92 | 5.59 × 10−2 | −1.23 | 0.82 | 1.05 × 10−1 | −0.81 | 0.78 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saito, K.; Kagawa, T.; Tsuji, K.; Kumagai, Y.; Sato, K.; Sakisaka, S.; Sakamoto, N.; Aiso, M.; Hirose, S.; Mori, N.; et al. Plasma Lipid Profiling of Three Types of Drug-Induced Liver Injury in Japanese Patients: A Preliminary Study. Metabolites 2020, 10, 355. https://doi.org/10.3390/metabo10090355
Saito K, Kagawa T, Tsuji K, Kumagai Y, Sato K, Sakisaka S, Sakamoto N, Aiso M, Hirose S, Mori N, et al. Plasma Lipid Profiling of Three Types of Drug-Induced Liver Injury in Japanese Patients: A Preliminary Study. Metabolites. 2020; 10(9):355. https://doi.org/10.3390/metabo10090355
Chicago/Turabian StyleSaito, Kosuke, Tatehiro Kagawa, Keiji Tsuji, Yuji Kumagai, Ken Sato, Shotaro Sakisaka, Naoya Sakamoto, Mitsuhiko Aiso, Shunji Hirose, Nami Mori, and et al. 2020. "Plasma Lipid Profiling of Three Types of Drug-Induced Liver Injury in Japanese Patients: A Preliminary Study" Metabolites 10, no. 9: 355. https://doi.org/10.3390/metabo10090355