1. Introduction
There is a high incidence of patients with human immunodeficiency virus (HIV) and
Mycobacterium tuberculosis co-infection. Out of the 10.4 million people that were diagnosed with tuberculosis (TB) in 2016, 1.4 million (13.4%) were HIV-positive [
1]. In 2016, about 0.4 million people died from tuberculosis associated with HIV. That same year, approximately 40% of the deaths recorded in the HIV-positive patients were due to tuberculosis [
1]. Pleural TB is the most common cause of extrapulmonary TB [
2]. Extrapulmonary TB is more common in HIV-positive patients when compared with HIV seronegative patients [
3].
The diagnosis of pleural TB depends on the demonstration of
Mycobacterium tuberculosis in sputum, pleural fluid, or pleural biopsy specimens. This is often difficult, thus other diagnostic tests have been proposed for the diagnosis of pleural tuberculosis, such as adenosine deaminase (ADA) assay. The ADA test has shown a high sensitivity and specificity in the diagnosis of pleural TB [
4], although its usefulness in diagnosis in immunocompromised patients is controversial due to the broad range in results that have been observed across studies [
5,
6,
7].
We aimed to evaluate the usefulness of the adenosine deaminase (ADA) assay in the diagnosis of pleural TB in HIV-infected patients and the usefulness of correlating this value with the cluster of differentiation 4 (CD4) lymphocyte serum count.
2. Materials and Methods
We retrospectively reviewed all patients with concomitant presentation of pleural effusion and HIV infection who underwent a diagnostic thoracentesis and ADA level determination in pleural fluid at Hospital Nacional Prof. Alejandro Posadas in Argentina between January 2013 and August 2016.
The pleural fluid samples were centrifuged, the sediment was sown in liquid medium “mycobacteria growth indicator tube” (MGIT), and the supernatant was stored at −20 °C to a dosage of ADA corresponding to the method of Galanti Giusty [
8]. The diagnosis of pleural TB was confirmed if culture for
Mycobacterium tuberculosis in pleural fluid, tissue, or another respiratory sample was positive. The presence of caseous granuloma in the pleural biopsy or an improvement after a tuberculosis treatment were also considered as diagnosis criteria.
The Ethics Committee of the Hospital Nacional Alejandro Posadas approved the study. The study was conducted in accordance with the Declaration of Helsinki 2013, Law 25.326 of the Ministry of Health and the protocol was approved by the ethics committee of Dr. Vicente Federico Del Giùdice (ref: 216 LUPOSO) on 8 October 2018.The need for written informed consent was waived due to the non-interventional nature of this study. Patients’ identity remained anonymous.
Statistical analysis was performed using SPSS (Version 18.0. Chicago: SPSS Inc.) statistical software. Continuous variables were compared using the Student’s t-test or Mann-Whitney. Receiver operating characteristic curve was performed to ADA assay and diagnosis of pleural tuberculosis. Linear regression model was performed to evaluate the correlation between ADA level and CD4 lymphocytes serum counts in patients with diagnosis of pleural tuberculosis.
3. Results
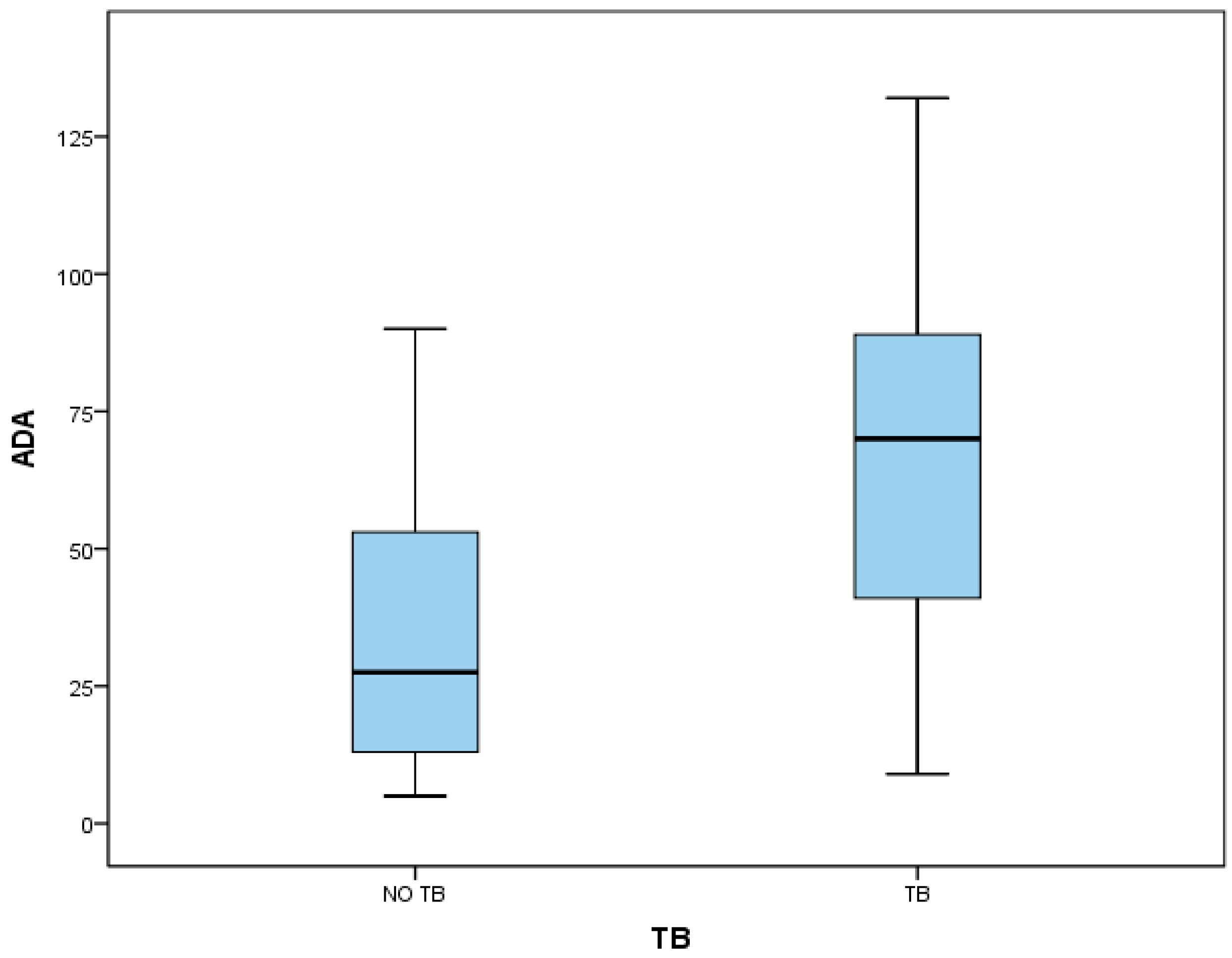
Forty-three HIV infected patients with pleural effusion were evaluated. Out of the 43 patients, 25 presented diagnosis of TB, 22 of them with positive culture (11 from pleural fluid and 11 from others respiratory samples), and three improved after tuberculosis treatment. In the non-TB group, four patients presented diagnosis of empyema, two of parapneumonic effusions, four of transudate effusions, and three malignant effusions. In five patients, the diagnosis was not achieved, although tuberculosis was ruled out. Patients with TB diagnosis showed a median value of ADA of 70 IU/L (interquartile range (IQR) 41–89) and the non-TB group, 27.5 IU/L (IQR 13.5–52). Patients with diagnosis of TB had a median CD4 count of 174 (IQR 86–274) and the non-TB group, 134 (IQR 71–371) (
Figure 1). The mean age in the TB group was 40 (±10) years and 41 (±10) years in the non-TB group; 19 (76%) patients were male in the TB group and 13 (72%) in the non-TB group. Non-differences were observed in fluid characteristics in pH (7.39 ± 0.07 vs. 7.41 ± 0.13), glucose (66 mg/dL ± 27 vs. 83 mg/dL ± 26), proteins (3.95 g/dL ± 1.15 vs. 3.27 g/dL ± 1.47), lactate dehydrogenase (LDH, 882 mmol/L ± 497 vs. 1046 ± 635), and leukocytes (1173/mm
3 ± 1733 vs. 1375/mm
3 ± 1024) (
Table 1).
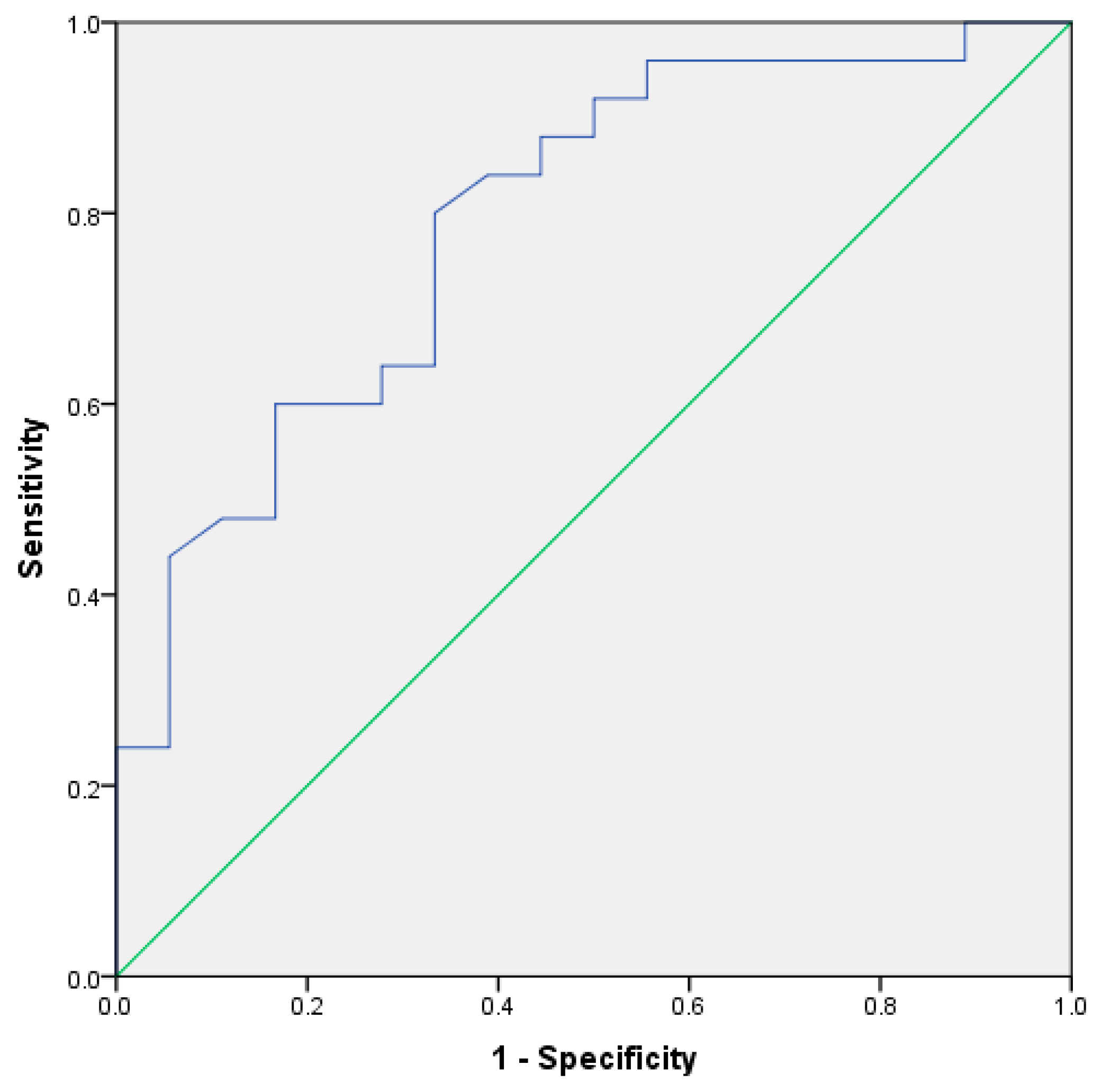
Receiver operating characteristic (ROC) curve was performed (
Figure 2) with an area under the curve of 0.79 (95% confidence interval (CI) 0.65–0.92).
The best cut-off obtained was 35 IU/L with a sensitivity of 80% (95% CI 59–93) and a specificity of 66% (95% CI 41–86).
In the TB patients group, the correlation between CD4 lymphocytes count and the value of ADA was low (r − 0.12) and without statistical significance.
4. Discussion
In this study, the sensitivity and specificity of the ADA assay to diagnose pleural tuberculosis in HIV infected patients were lower than that reported in non-HIV infected patients [
9]. There was no relationship between the level of immunodeficiency, measured by CD4 lymphocyte serum count, and the value of ADA in the pleural fluid. Our research found significance differences between groups in ADA level. The AUC of the ROC curve achieved the threshold level of 0.75 that was reported as clinically useful. An high number of patients (88%) had confirmed bacteriologic disease.
The diagnostic utility of the ADA assay for pleural TB in HIV infected patients is still controversial. Hsu et al. found no statistical differences in the ADA assay between patients with immunodeficiency and TB diagnosis versus patients with pleural effusion of malignant etiology. They concluded that the diagnostic value of ADA in immunocompromised hosts with pleural tuberculosis effusions is not as significant as in immunocompetent hosts [
5]. However, recent studies have showed a greater sensitivity and specificity for ADA assay, even in patients with low CD4 count [
6,
7]. In contrast, ADA assay showed a low sensitivity to diagnosis of TB in patients co-infected with HIV in other corporal fluids such as pericardial effusions and cerebrospinal fluid [
10,
11].
In conclusion, ADA level determination could be useful to diagnose pleural tuberculosis in HIV infected patients, although larger multicentric studies are necessary to confirm this. Conventional bacteriologic determinations are necessary to evaluate these patients in the meantime.
Author Contributions
Study concept and design: G.Y., A.G., and A.C.; data collection: G.Y., A.C., A.Z., and A.G.; statistical analysis: A.C. and M.F.; analysis and interpretation of data: G.Y., A.G., M.F., A.Z., G.T., and A.C.; drafting of the manuscript: G.Y. and A.C.; critical revision of the manuscript for important intellectual content: A.G., M.F., A.Z., and G.T.; and study supervision: A.G. A.G. had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Funding
This research received no external funding.
Acknowledgments
We are indebted to all medical and nursing colleagues for their assistance and cooperation in this study.
Conflicts of Interest
The authors declare have no conflicts of interest.
References
- WHO World Health Organization. Global Tuberculosis Report 2017. 2017. Available online: http://www.who.int/tb/publications/global_report/gtbr2017_main_text.pdf (accessed on 2 October 2018).
- Zhai, K.; Lu, Y.; Shi, H.-Z. Tuberculous pleural effusion. J. Thorac. Dis. 2016, 8, E486–E494. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aljohaney, A.; Amjadi, K.; Alvarez, G.G. A systematic review of the epidemiology, immunopathogenesis, diagnosis, and treatment of pleural TB in HIV-infected patients. Clin. Dev. Immunol. 2012, 2012, 842045. [Google Scholar] [CrossRef] [PubMed]
- Gopi, A.; Madhavan, S.M.; Sharma, S.K.; Sahn, S.A. Diagnosis and treatment of tuberculous pleural effusion in 2006. Chest 2007, 131, 880–889. [Google Scholar] [CrossRef] [PubMed]
- Hsu, W.H.; Chiang, C.D.; Huang, P.L. Diagnostic value of pleural adenosine deaminase in tuberculous effusions of immunocompromised hosts. J. Formos. Med. Assoc. Taiwan Yi Zhi 1993, 92, 668–670. [Google Scholar] [PubMed]
- Baba, K.; Hoosen, A.A.; Langeland, N.; Dyrhol-Riise, A.M. Adenosine Deaminase Activity Is a Sensitive Marker for the Diagnosis of Tuberculous Pleuritis in Patients with Very Low CD4 Counts. PLoS ONE 2008, 3, e2788. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riantawan, P.; Chaowalit, P.; Wongsangiem, M.; Rojanaraweewong, P. Diagnostic value of pleural fluid adenosine deaminase in tuberculous pleuritis with reference to HIV coinfection and a Bayesian analysis. Chest 1999, 116, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Giusti, G. Adenosine Deaminase. In Methods of Enzymatic Analysis; Academic Press: New York, NY, USA, 1972; pp. 1092–1099. [Google Scholar]
- Liang, Q.-L.; Shi, H.-Z.; Wang, K.; Qin, S.-M.; Qin, X.-J. Diagnostic accuracy of adenosine deaminase in tuberculous pleurisy: A meta-analysis. Respir. Med. 2008, 102, 744–754. [Google Scholar] [CrossRef] [PubMed]
- Reuter, H.; Burgess, L.J.; Carstens, M.E.; Doubell, A.F. Adenosine deaminase activity--more than a diagnostic tool in tuberculous pericarditis. Cardiovasc. J. S. Afr. 2005, 16, 143–147. [Google Scholar] [PubMed]
- Corral, I.; Quereda, C.; Navas, E.; Martín-Dávila, P.; Pérez-Elías, M.-J.; Casado, J.-L.; Pintado, V.; Cobo, J.; Pallarés, E.; Rubí, J.; et al. Adenosine deaminase activity in cerebrospinal fluid of HIV-infected patients: Limited value for diagnosis of tuberculous meningitis. Eur. J. Clin. Microbiol. Infect. Dis. 2004, 23, 471–476. [Google Scholar] [CrossRef] [PubMed]
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).

 ,
, 


{kind=link}
{kind=link}