
Intraoperative Neuromonitoring and Optical Magnification in the Prevention of Recurrent Laryngeal Nerve Injuries during Total Thyroidectomy

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Riddell, V. Thyroidectomy: Prevention of bilateral recurrent nerve palsy. Results of identification of the nerve over 23 consec-utive years (1946-69) with a description of an additional safety measure. Br. J. Surg. 1970, 57, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Sturniolo, G.; D’Alia, C.; Tonante, A.; Gagliano, E.; Taranto, F.; Schiavo, M.G.L. The recurrent laryngeal nerve related to thyroid surgery. Am. J. Surg. 1999, 177, 485–488. [Google Scholar] [CrossRef]
- Bergenfelz, A.; Jansson, S.; Kristoffersson, A.-C.; Mårtensson, H.; Reihnér, E.; Wallin, G.; Lausen, I. Complications to thyroid surgery: Results as reported in a database from a multicenter audit comprising 3,660 patients. Langenbeck’s Arch. Surg. 2008, 393, 667–673. [Google Scholar] [CrossRef] [PubMed]
- Donatini, G.; Danion, J.; Zerrweck, C.; Etienne, P.; Lacoste, L.; Kraimps, J.-L. Single Dose Steroid Injection After Loss of Signal (LOS) During Thyroid Surgery is Effective to Recover Electric Signal Avoiding Vocal Cord Palsy and the Need of Staged Thyroidectomy: Prospective Evaluation on 702 Patients. World J. Surg. 2020, 44, 417–425. [Google Scholar] [CrossRef] [PubMed]
- D’Orazi, V.; Panunzi, A.; Di Lorenzo, E.; Ortensi, A.L.; Cialini, M.; Anichini, S.; Ortensi, A. Use of loupes magnification and microsur-gical technique in thyroid surgery: Ten years’ experience in a single center. G. Chir. 2016, 37, 101–107. [Google Scholar] [PubMed]
- Yang, S.; Zhou, L.; Lu, Z.; Ma, B.; Ji, Q.; Wang, Y. Systematic review with meta-analysis of intraoperative neuromonitoring during thyroidectomy. Int. J. Surg. 2017, 39, 104–113. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.-Y.; Chang, C.-P.; Hung, C.-L.; Hung, C.-J.; Huang, S.-M. Traction Injury of Recurrent Laryngeal Nerve During Thyroidectomy. World J. Surg. 2020, 44, 402–407. [Google Scholar] [CrossRef]
- Randolph, G.W.; Shin, J.J.; Grillo, H.C.; Mathisen, D.; Katlic, M.R.; Kamani, D.; Zurakowski, D. The surgical management of goiter: Part II. Surgical treatment and results. Laryngoscope 2011, 121, 68–76. [Google Scholar] [CrossRef]
- Lo, C.-Y.; Kwok, K.-F.; Yuen, P.-W. A Prospective Evaluation of Recurrent Laryngeal Nerve Paralysis during Thyroidectomy. Arch. Surg. 2000, 135, 204–207. [Google Scholar] [CrossRef] [Green Version]
- Jeannon, J.-P.; Orabi, A.A.; Bruch, G.A.; Abdalsalam, H.A.; Simo, R. Diagnosis of recurrent laryngeal nerve palsy after thyroidectomy: A systematic review. Int. J. Clin. Pract. 2009, 63, 624–629. [Google Scholar] [CrossRef]
- Jatzko, G.R.; Lisborg, P.H.; Müller, M.G.; Wette, V.M. Recurrent nerve palsy after thyroid operations--principal nerve identification and a literature review. Surgery 1994, 115, 139–144. [Google Scholar] [PubMed]
- Dionigi, G.; Wu, C.-W.; Kim, H.Y.; Rausei, S.; Boni, L.; Chiang, F.-Y. Severity of Recurrent Laryngeal Nerve Injuries in Thyroid Surgery. World J. Surg. 2016, 40, 1373–1381. [Google Scholar] [CrossRef] [PubMed]
- Schneider, R.; Randolph, G.; Dionigi, G.; Barczyński, M.; Chiang, F.-Y.; Triponez, F.; Vamvakidis, K.; Brauckhoff, K.; Musholt, T.J.; Almquist, M.; et al. Prospective study of vocal fold function after loss of the neuromonitoring signal in thyroid surgery: The International Neural Monitoring Study Group’s POLT study. Laryngoscope 2016, 126, 1260–1266. [Google Scholar] [CrossRef] [PubMed]
- Chiang, F.-Y.; Lu, I.-C.; Kuo, W.-R.; Lee, K.-W.; Chang, N.-C.; Wu, C.-W. The mechanism of recurrent laryngeal nerve injury during thyroid surgery—The application of intraoperative neuromonitoring. Surgery 2008, 143, 743–749. [Google Scholar] [CrossRef]
- Testini, M.; Nacchiero, M.; Piccinni, G.; Portincasa, P.; Di Venere, B.; Lissidini, G.; Bonomo, G.M. Total thyroidectomy is improved by loupe magnification. Microsurgery 2004, 24, 39–42. [Google Scholar] [CrossRef]
- Pata, G.; Casella, C.; Mittempergher, F.; Cirillo, L.; Salerni, B. Loupe magnification reduces postoperative hypocalcemia after total thyroidectomy. Am. Surg. 2010, 76, 1345–1350. [Google Scholar] [CrossRef]
- Sapalidis, K.; Papanastasiou, A.; Fyntanidou, V.; Aidoni, Z.; Michalopoulos, N.; Katsaounis, A.; Amaniti, A.; Zarogoulidis, P.; Koulouris, C.; Giannakidis, D.; et al. Comparison between Magnification Techniques and Direct Vision in Thyroid Surgery: A Systematic Review and Meta-Analysis. Medicina 2019, 55, 725. [Google Scholar] [CrossRef] [Green Version]
- Dionigi, G.; A Working Group for Neural Monitoring in Thyroid and Parathyroid Surgery in Italy; Lombardi, D.; Lombardi, C.P.; Carcoforo, P.; Boniardi, M.; Innaro, N.; Chiofalo, M.G.; Cavicchi, O.; Biondi, A.; et al. Intraoperative neuromonitoring in thyroid surgery: A point prevalence survey on utilization, management, and documentation in Italy. Updat. Surg. 2014, 66, 269–276. [Google Scholar] [CrossRef]
- Sanabria, A.; Ramirez, A.; Kowalski, L.P.; Silver, C.E.; Shaha, A.R.; Owen, R.P.; Suárez, C.; Khafif, A.; Rinaldo, A.; Ferlito, A. Neuromonitoring in thyroidectomy: A meta-analysis of effectiveness from ran-domized controlled trials. Eur. Arch. Oto-Rhino-Laryngol. 2013, 270, 2175–2189. [Google Scholar] [CrossRef]
- Barczyński, M.; Randolph, G.W.; Cernea, C.R. The International Neural Monitoring Study Group in Thyroid and Parathyroid Surgery International survey on the identification and neural monitoring of the EBSLN during thyroidectomy. Laryngoscope 2016, 126, 285–291. [Google Scholar] [CrossRef]
- Schneider, R.; Randolph, G.W.; Dionigi, G.; Wu, C.-W.; Barczynski, M.; Chiang, F.-Y.; Al-Quaryshi, Z.; Angelos, P.; Brauckhoff, K.; Cernea, C.R.; et al. International neural monitoring study group guideline 2018 part I: Staging bilateral thyroid surgery with monitoring loss of signal. Laryngoscope 2018, 128 (Suppl. 3), S1–S17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, S.-Y.; Shen, H.-Y.; Duh, Q.-Y.; Hsieh, C.-B.; Yu, J.-C.; Shih, M.-L. Routine Intraoperative Neuromonitoring of the Recurrent Laryngeal Nerve to Facilitate Complete Resection and Ensure Safety in Thyroid Cancer Surgery. Am. Surg. 2018, 84, 1882–1888. [Google Scholar] [CrossRef] [PubMed]
- Randolph, G.W.; Dralle, H.; Abdullah, H.; Barczynski, M.; Bellantone, R.; Brauckhoff, M.; Carnaille, B.; Cherenko, S.; Chiang, F.-Y.; Dionigi, G.; et al. Electrophysiologic recurrent laryngeal nerve monitoring during thyroid and parathyroid surgery: International standards guideline statement. Laryngoscope 2011, 121, S1–S16. [Google Scholar] [CrossRef] [PubMed]
- Cirocchi, R.; Arezzo, A.; D’Andrea, V.; Abraha, I.; Popivanov, G.I.; Avenia, N.; Gerardi, C.; Henry, B.M.; Randolph, J.; Barczyñski, M. Intraoperative neuromonitoring versus visual nerve identification for prevention of recurrent laryngeal nerve injury in adults undergoing thyroid surgery. Cochrane Database Syst. Rev. 2019, 1, CD012483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bai, B.; Chen, W. Protective Effects of Intraoperative Nerve Monitoring (IONM) for Recurrent Laryngeal Nerve Injury in Thy-roidectomy: Meta-analysis. Sci. Rep. 2018, 8, 7761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pardal-Refoyo, J.L.; Ochoa-Sangrador, C. Bilateral recurrent laryngeal nerve injury in total thyroidectomy with or without in-traoperative neuromonitoring. Systematic review and meta-analysis. Acta Otorrinolaringol. Esp. 2016, 67, 66–74. [Google Scholar] [CrossRef] [PubMed]
- Alesina, P.F.; Hinrichs, J.; Meier, B.; Cho, E.Y.; Bolli, M.; Walz, M.K. Intraoperative neuromonitoring for surgical training in thyroid surgery: It’s routine use allows a safe operation instead of lack of experienced mentoring. World J. Surg. 2014, 38, 592–598. [Google Scholar] [CrossRef]
- Sarı, S.; Erbil, Y.; Sümer, A.; Agcaoglu, O.; Bayraktar, A.; Issever, H.; Ozarmagan, S. Evaluation of recurrent laryngeal nerve monitoring in thyroid surgery. Int. J. Surg. 2010, 8, 474–478. [Google Scholar] [CrossRef] [Green Version]
- Phelan, E.; Schneider, R.; Lorenz, K.; Dralle, H.; Kamani, D.; Potenza, A.; Sritharan, N.; Shin, J.; Randolph, G.W. Continuous vagal IONM prevents recurrent laryngeal nerve paralysis by revealing initial EMG changes of impending neuropraxic injury: A prospective, multicenter study. Laryngoscope 2014, 124, 1498–1505. [Google Scholar] [CrossRef]
- Pisanu, A.; Porceddu, G.; Podda, M.; Cois, A.; Uccheddu, A. Systematic review with meta-analysis of studies comparing intraoperative neuromon-itoring of recurrent laryngeal nerves versus visualization alone during thyroidectomy. J. Surg. Res. 2014, 188, 152–161. [Google Scholar] [CrossRef]
- Kamani, D.; Potenza, A.S.; Cernea, C.R.; Kamani, Y.V.; Randolph, G.W. The non-recurrent laryngeal nerve: Anatomic and electro-physiologic algorithm for reliable identification. Laryngoscope 2015, 125, 503–508. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.Y.; Son, Y.-I. Intraoperative Neuromonitoring for Thyroid Surgery: The Proven Benefits and Limitations. Clin. Exp. Otorhinolaryngol. 2019, 12, 335–336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mirallié, É.; Caillard, C.; Pattou, F.; Brunaud, L.; Hamy, A.; Dahan, M.; Prades, M.; Mathonnet, M.; Landecy, G.; Dernis, H.-P.; et al. Does intraoperative neuromonitoring of recurrent nerves have an impact on the postoperative palsy rate? Results of a prospective multicenter study. Surgery 2018, 163, 124–129. [Google Scholar] [CrossRef] [PubMed]
- Higgins, T.S.; Gupta, R.; Ketcham, A.S.; Sataloff, R.T.; Wadsworth, J.T.; Sinacori, J.T. Recurrent laryngeal nerve monitoring versus identification alone on post-thyroidectomy true vocal fold palsy: A meta-analysis. Laryngoscope 2011, 121, 1009–1017. [Google Scholar] [CrossRef] [PubMed]
- Wong, K.P.; Mak, K.L.; Wong, C.K.H.; Lang, B. Systematic review and meta-analysis on intra-operative neuro-monitoring in high-risk thyroidectomy. Int. J. Surg. 2017, 38, 21–30. [Google Scholar] [CrossRef] [PubMed]
- Barczyński, M.; Konturek, A.; Pragacz, K.; Papier, A.; Stopa, M.; Nowak, W. Intraoperative Nerve Monitoring Can Reduce Prevalence of Recurrent Laryngeal Nerve Injury in Thyroid Reoperations: Results of a Retrospective Cohort Study. World J. Surg. 2014, 38, 599–606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dralle, H.; Sekulla, C.; Haerting, J.; Timmermann, W.; Neumann, H.J.; Kruse, E.; Grond, S.; Mühlig, H.P.; Richter, C.; Gimm, O.; et al. Risk factors of paralysis and functional outcome after recurrent laryngeal nerve monitoring in thyroid surgery. Surgery 2004, 136, 1310–1322. [Google Scholar] [CrossRef]
- Melin, M.; Schwarz, K.; Lammers, B.J.; Goretzki, P.E. IONM-guided goiter surgery leading to two-stage thyroidectomy—Indication and results. Langenbeck’s Arch. Surg. 2013, 398, 411–418. [Google Scholar] [CrossRef]
- Dionigi, G.; Bacuzzi, A.; Boni, L.; Rausei, S.; Rovera, F.; Dionigi, R. Visualization versus neuromonitoring of recurrent laryngeal nerves during thyroidectomy: What about the costs? World J. Surg. 2012, 36, 748–754. [Google Scholar] [CrossRef]
- Goretzki, P.E.; Schwarz, K.; Brinkmann, J.; Wirowski, D.; Lammers, B.J. The impact of intraoperative neuromonitoring (IONM) on surgical strategy in bilateral thyroid diseases: Is it worth the effort? World J. Surg. 2010, 34, 1274–1284. [Google Scholar] [CrossRef]
- Wu, C.W.; Lee, K.D.; Tae, K.; Ji, Y.B.; Kim, S.U.; Lee, H.S.; Lee, K.W.; Chiang, F.Y. Recurrent laryngeal nerve (RLN) injury in thyroid surgery: Lessons learned from the intraoperative neural monitoring (IONM). Int. J. Head Neck Sci. 2017, 1, 19–26. [Google Scholar]
- Sitges-Serra, A.; Fontané, J.; Dueñas, J.P.; Duque, C.S.; Lorente, L.; Trillo, L.; Sancho, J.J. Prospective study on loss of signal on the first side during neuromonitoring of the recurrent laryngeal nerve in total thyroidectomy. Br. J. Surg. 2013, 100, 662–666. [Google Scholar] [CrossRef] [PubMed]
- Dionigi, G.; Bacuzzi, A.; Boni, L.; Rovera, F.; Dionigi, R. What is the learning curve for intraoperative neuromonitoring in thyroid surgery? Int. J. Surg. 2008, 6 (Suppl. 1), 7–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Orazi, V.; Sacconi, A.; Trombetta, S.; Karpathiotakis, M.; Pichelli, D.; Di Lorenzo, E.; Ortensi, A.; Urciuoli, P.; Biffoni, M.; Ortensi, A. May predictors of difficulty in thyroid surgery increase the incidence of complications? Prospective study with the proposal of a preoperative score. BMC Surg. 2019, 18, 116. [Google Scholar] [CrossRef] [PubMed]
- Campana, F.P.; Marchesi, M.; Tartaglia, F.; Biffoni, M.; Pugliese, F.R.; Nobili-Benedetti, R.; Orlando, M.; Santangeli, E.; Santangeli, S.; Campana, C. Total thyroidectomy for goiter. Chirurgia 1992, 5, 102–105. [Google Scholar]
- Baldini, E.; Tuccilli, C.; Prinzi, N.; Sorrenti, S.; Falvo, L.; DE Vito, C.; Catania, A.; Tartaglia, F.; Mocini, R.; Coccaro, C.; et al. Deregulated Expression of Aurora Kinases Is Not a Prognostic Biomarker in Papillary Thyroid Cancer Patients. PLoS ONE 2015, 10, e0121514. [Google Scholar] [CrossRef] [PubMed]
- Peparini, N.; Maturo, A.; DI Matteo, F.M.; Tartaglia, F.; Marchesi, M.; Campana, F. Blue-dye Sentinel Node Mapping in Thyroid Carcinoma: Debatable Results of Feasibility. Acta Chir. Belg. 2006, 106, 523–527. [Google Scholar] [CrossRef]
- Tartaglia, F.; Blasi, S.; Tromba, L.; Sgueglia, M.; Russo, G.; DI Matteo, F.M.; Carbotta, G.; Campana, F.P.; Berni, A. Duplex ultrasound and magnetic resonance imaging of the supra-aortic arches in patients with non recurrent inferior laryngeal nerve: A comparative study. G. Chir.-J. Surg. 2011, 32, 245–250. [Google Scholar]
- Tartaglia, F.; Maturo, A.; DI Matteo, F.M.; De Anna, L.; Karpathiotakis, M.; Pelle, F.; Tromba, L.; Carbotta, S.; Carbotta, G.; Biancucci, A.; et al. Transoral video assisted thyroidectomy: A systematic review. G. Chir.-J. Surg. 2018, 39, 276–283. [Google Scholar]
- Baldini, E.; Odorisio, T.; Sorrenti, S.; Catania, A.; Tartaglia, F.; Carbotta, G.; Pironi, D.; Rendina, R.; D’Armiento, E.; Persechino, S.; et al. Vitiligo and Autoimmune Thyroid Disorders. Front. Endocrinol. 2017, 8, 290. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographics and Pathophysiological Characteristics | OM Group (n = 50) | IONM Group (n = 50) | Total (n = 100) | p |
|---|---|---|---|---|
| Gender (F, %F) | 41 (82%) | 42 (84%) | 83 (100%) | ns |
| Age (median, IQR) | 53.5 (42–62) | 55 (43–65) | 55 (43–65) | ns |
Admission diagnosis (n, %)
| 27 (54%) 21 (42%) 2 (4%) | 22 (44%) 25 (50%) 3 (6%) | 49 (49%) 46 (46%) 5 (5%) | ns |
| Hyperthyroidism (n, %) | 7 (14%) | 6 (12%) | 13 (13%) | ns |
FNA with cytological examination
| 19 (38%) | 28 (56%) | 47 (47%) | ns |
Histology
| 20 (40%) 0 (0%) 9 (18%) 1 (2%) 20 (40%) | 10 (20%) 5 (10%) 0 (0%) 0 (0%) 35 (70%) | 30 (30%) 5 (5%) 9 (9%) 1 (1%) 55 (55%) | <0.05 |
Thyroiditis (n, %)
| 36 (72%) 6 (12%) 6 (12%) 2 (4%) | 36 (72%) 8 (16%) 3 (6%) 3 (6%) | 72 (72%) 13 (13%) 8 (8%) 7 (7%) | ns |
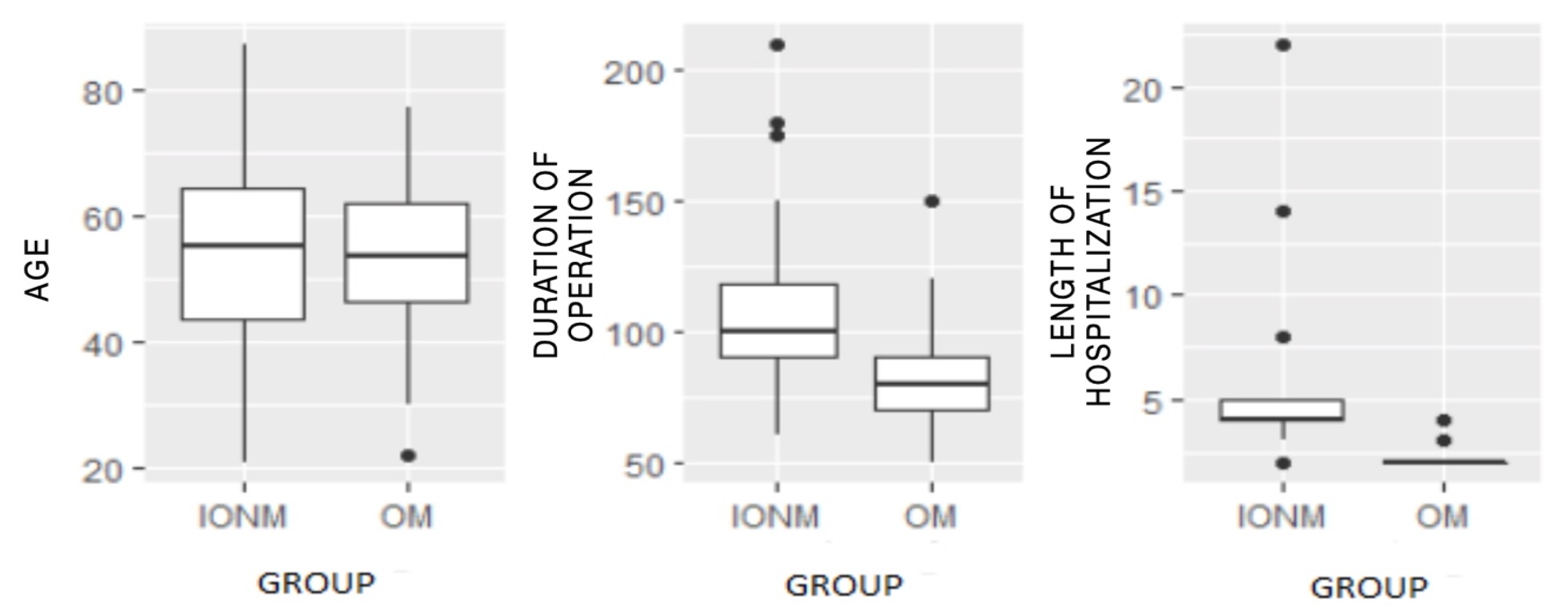
| Duration of the operation in minutes (median, IQR) | 80 (70–90) | 100 (90–119) | 90 (75–102) | <0.05 |
| Length of hospitalization in days (median, IQR) | 2 (2–2) | 4 (4–5) | 3 (2–4) | <0.05 |
Cortisone therapy (n, %)
| 50 (100%) 1 (2%) | 50 (100%) 8 (16%) | 100 (100%) 9 (9%) | <0.05 |
Hypoparathyroidism (n, %)
| 33 (66%) 17 (34%) 0 (0%) | 44 (88%) 6 (12%) 0 (0%) | 77 (77%) 23 (23%) 0 (0%) | <0.05 |
Dysphonia (transient) (n, %)
| 45 (90%) 5 (10%) | 44 (88%) 6 (12%) | 89 (89%) 11 (11%) | ns |
RLN paralysis (temporary) (n, %)
| 50 (100%) 0 (0%) 0 (0%) | 48 (96%) 0 (0%) 2 (4%) | 98 (98%) 0 (0%) 2 (2%) | ns |
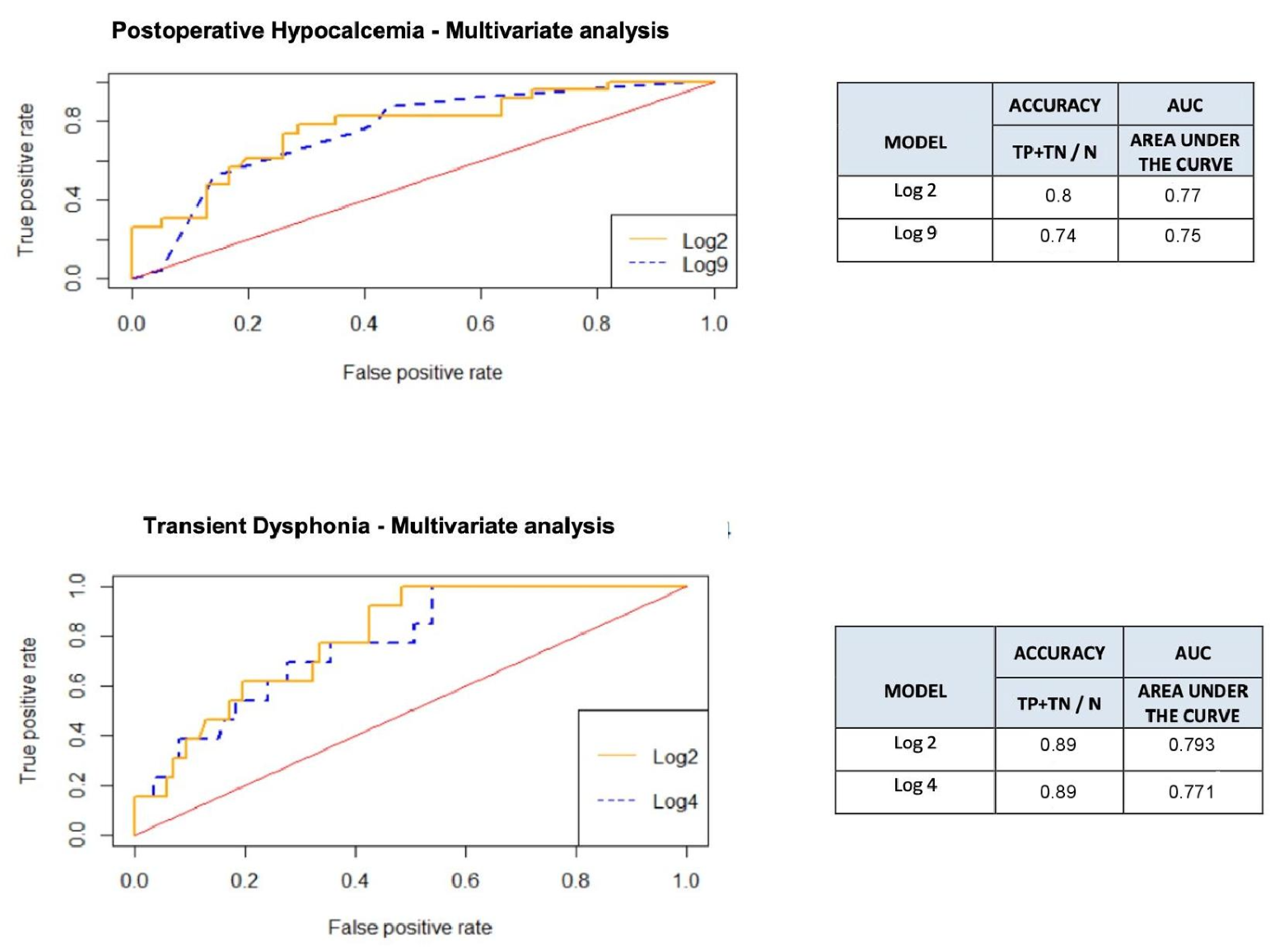
| Transient Dysphonia Gender | Univariate Analysis | Multivariate Analysis | ||||
| OR | IC (95%) | p | Adj OR | IC (95%) | p | |
| F M | 1 2.53 | 0.68–9.44 | 0.28 | 1 5.19 | 0.99–27.18 | 0.05 |
| Transient Hypocalcemia Group | Univariate Analysis | Multivariate Analysis | ||||
| OR | IC (95%) | p | Adj OR | IC (95%) | p | |
| IONM OM | 1 3.78 | 1.34–10.62 | 0.02 | 1 4.11 | 1.42–11.93 | 0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karpathiotakis, M.; D’Orazi, V.; Ortensi, A.; Biancucci, A.; Melcarne, R.; Borcea, M.C.; Scorziello, C.; Tartaglia, F. Intraoperative Neuromonitoring and Optical Magnification in the Prevention of Recurrent Laryngeal Nerve Injuries during Total Thyroidectomy. Medicina 2022, 58, 1560. https://doi.org/10.3390/medicina58111560
Karpathiotakis M, D’Orazi V, Ortensi A, Biancucci A, Melcarne R, Borcea MC, Scorziello C, Tartaglia F. Intraoperative Neuromonitoring and Optical Magnification in the Prevention of Recurrent Laryngeal Nerve Injuries during Total Thyroidectomy. Medicina. 2022; 58(11):1560. https://doi.org/10.3390/medicina58111560
Chicago/Turabian StyleKarpathiotakis, Menelaos, Valerio D’Orazi, Andrea Ortensi, Andrea Biancucci, Rossella Melcarne, Maria Carola Borcea, Chiara Scorziello, and Francesco Tartaglia. 2022. "Intraoperative Neuromonitoring and Optical Magnification in the Prevention of Recurrent Laryngeal Nerve Injuries during Total Thyroidectomy" Medicina 58, no. 11: 1560. https://doi.org/10.3390/medicina58111560