
Perioperative Red Cell Line Trend following Robot-Assisted Radical Prostatectomy for Prostate Cancer

 , , , , , , ,
, , , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mottet, N.; van den Bergh, R.C.N.; Briers, E.; Van den Broeck, T.; Cumberbatch, M.G.; De Santis, M.; Fanti, S.; Fossati, N.; Gandaglia, G.; Gillessen, S.; et al. EAU-EANM-ESTRO-ESUR-SIOG Guidelines on Prostate Cancer-2020 Update. Part 1: Screening, Diagnosis, and Local Treatment with Curative Intent. Eur. Urol. Febbraio 2021, 79, 243–262. [Google Scholar] [CrossRef] [PubMed]
- Celentano, G.; Creta, M.; Napolitano, L.; Abate, M.; La Rocca, R.; Capece, M.; Mirone, C.; Morra, S.; Di Bello, F.; Cirillo, L.; et al. Prostate Cancer Diagnosis, Treatment and Outcomes in Patients with Previous or Synchronous Colorectal Cancer: A Systematic Review of Published Evidence. Diagnostics 2022, 12, 1475. [Google Scholar] [CrossRef] [PubMed]
- Ilic, D.; Evans, S.M.; Allan, C.A.; Jung, J.H.; Murphy, D.; Frydenberg, M. Laparoscopic and robot-assisted vs open radical prostatectomy for the treatment of localized prostate cancer: A Cochrane systematic review. BJU Int. 2018, 121, 845–853. [Google Scholar] [CrossRef] [PubMed]
- Scandurra, C.; Muzii, B.; La Rocca, R.; Di Bello, F.; Bottone, M.; Califano, G.; Longo, N.; Maldonato, N.M.; Mangiapia, F. Social Support Mediates the Relationship between Body Image Distress and Depressive Symptoms in Prostate Cancer Patients. Int. J. Env. Res Public Health 2022, 19, 4825. [Google Scholar] [CrossRef] [PubMed]
- Knipper, S.; Graefen, M. Robot-assisted Radical Prostatectomy-So Successful Because It Is Better or Better Because It Is So Successful? Eur. Urol. Oncol. 2018, 1, 361–363. [Google Scholar] [CrossRef] [PubMed]
- Cao, L.; Yang, Z.; Qi, L.; Chen, M. Robot-assisted and laparoscopic vs open radical prostatectomy in clinically localized prostate cancer: Perioperative, functional, and oncological outcomes. Medicine 2019, 98, e15770. [Google Scholar] [CrossRef] [PubMed]
- Tewari, A.; Sooriakumaran, P.; Bloch, D.A.; Seshadri-Kreaden, U.; Hebert, A.E.; Wiklund, P. Positive Surgical Margin and Perioperative Complication Rates of Primary Surgical Treatments for Prostate Cancer: A Systematic Review and Meta-Analysis Comparing Retropubic, Laparoscopic, and Robotic Prostatectomy. Eur. Urol. 2012, 62, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Scandurra, C.; Mangiapia, F.; La Rocca, R.; Di Bello, F.; De Lucia, N.; Muzii, B.; Cantone, M.; Zampi, R.; Califano, G.; Maldonato, N.M.; et al. A cross-sectional study on demoralization in prostate cancer patients: The role of masculine self-esteem, depression, and resilience. Support. Care Cancer 2022, 30, 7021–7030. [Google Scholar] [CrossRef] [PubMed]
- Yaxley, J.W.; Coughlin, G.D.; Chambers, S.K.; Occhipinti, S.; Samaratunga, H.; Zajdlewicz, L.; Dunglison, N.; Carter, R.; Williams, S.; Payton, D.J.; et al. Robot-assisted laparoscopic prostatectomy versus open radical retropubic prostatectomy: Early outcomes from a randomised controlled phase 3 study. Lancet 2016, 388, 1057–1066. [Google Scholar] [CrossRef]
- Capece, M.; Creta, M.; Calogero, A.; La Rocca, R.; Napolitano, L.; Barone, B.; Sica, A.; Fusco, F.; Santangelo, M.; Dodaro, C.; et al. Does Physical Activity Regulate Prostate Carcinogenesis and Prostate Cancer Outcomes? A Narrative Review. Int. J. Environ. Res. Public Health 2020, 17, 1441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Porcaro, A.B.; Rizzetto, R.; Amigoni, N.; Tafuri, A.; Shakir, A.; Tiso, L.; Cerrato, C.; Antoniolli, S.Z.; Lacola, V.; Gozzo, A.; et al. Severe intraoperative bleeding predicts the risk of perioperative blood transfusion after robot-assisted radical prostatectomy. J. Robot. Surg. 2022, 16, 463–471. [Google Scholar] [CrossRef] [PubMed]
- EAU Guidelines on Prostate Cancer—Uroweb [Internet]. Uroweb—European Association of Urology. [Citato 24 April 2022]. Disponibile Su. Available online: https://uroweb.org/guidelines/prostate-cancer (accessed on 17 October 2022).
- Abaza, R.; Martinez, O.; Ferroni, M.C.; Bsatee, A.; Gerhard, R.S. Same Day Discharge after Robotic Radical Prostatectomy. J. Urol. 2019, 202, 959–963. [Google Scholar] [CrossRef] [PubMed]
- Ploussard, G.; Almeras, C.; Beauval, J.-B.; Gautier, J.-R.; Loison, G.; Salin, A.; Tollon, C. Same-day discharge surgery for robot-assisted radical prostatectomy in the era of ERAS and prehabilitation pathways: A contemporary, comparative, feasibility study. World J. Urol. 2020, 40, 1359–1365. [Google Scholar] [CrossRef]


{kind=link}
| Preoperative Day | POD 1 | POD 2 | POD 3 | ∆ Preoperative– POD 1 | p Value | ∆ Preoperative– POD 2 | p Value | ∆ POD 2– POD 3 | p Value | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
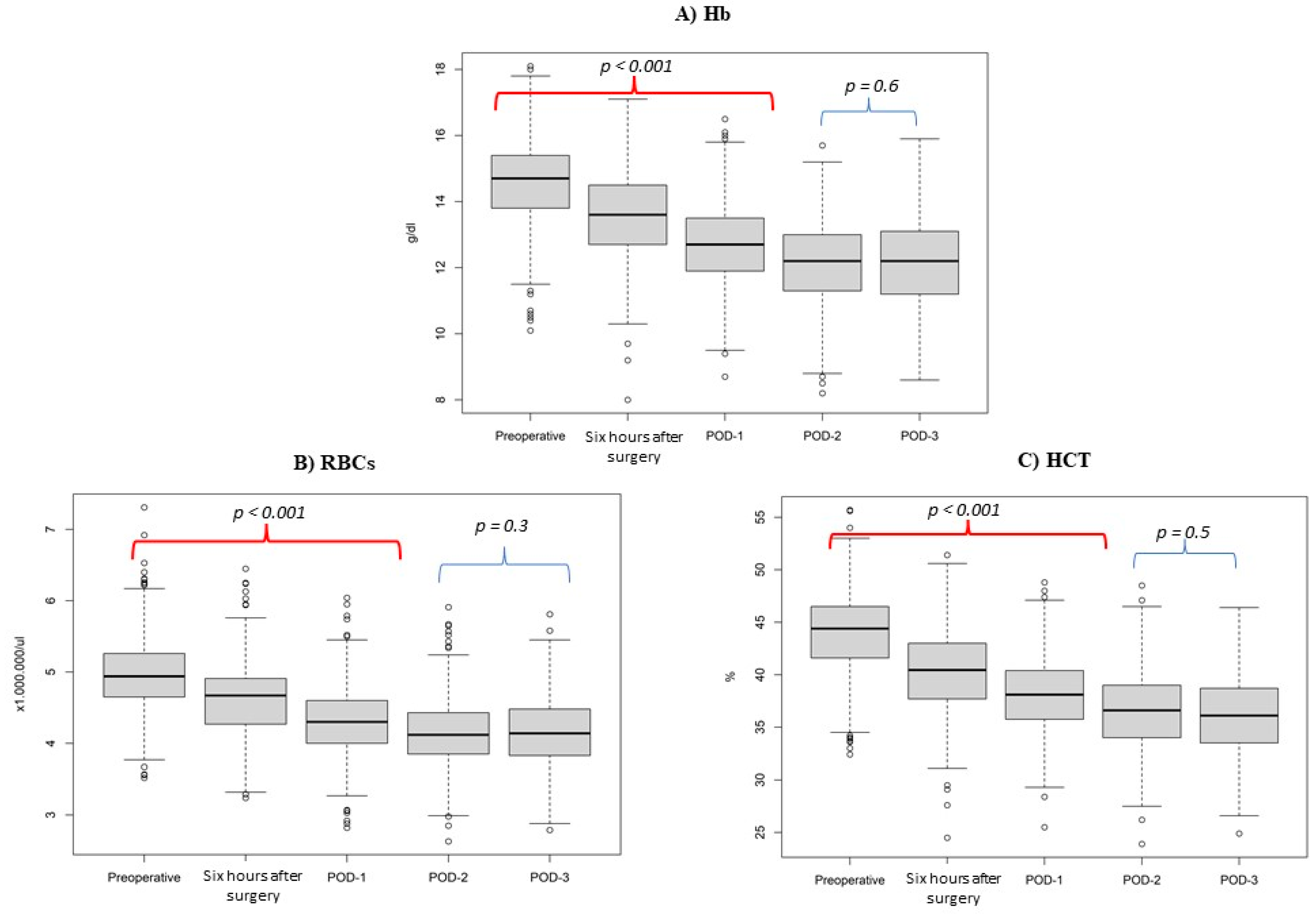
| Hb (g/dL) | Mean (SD) | 14.6 (0.071) | 12.6 (0.064) | 12.1 (0.068) | 12.1 (0.071) | 2.0 | <0.001 | 2.5 | <0.001 | 0.6 | 0.6 |
| Median (IQR) | 14.7 (13.9–15.4) | 12.6 (11.8–13.4) | 12.1 (11.2–12.9) | 12.2 (11.2–13.1) | 2.1 | 2.5 | 0.5 | ||||
| RBCs (×106/μL) | Mean (SD) | 5 (0.028) | 4.3 (0.025) | 4.1 (0.026) | 4.1 (0.027) | 0.7 | <0.001 | 0.9 | <0.001 | 0.2 | 0.3 |
| Median (IQR) | 4.9 (4.7–5.3) | 4.3 (4.0–4.6) | 4.1 (3.8–4.4) | 4.1 (3.8–4.5) | 0.6 | 0.9 | 0.2 | ||||
| HCT (%) | Mean (SD) | 44.2 (0.213) | 37.9 (0.186) | 36.3 (0.209) | 36.1 (0.211) | 6.3 | <0.001 | 7.9 | <0.001 | 2.0 | 0.5 |
| Median (IQR) | 44.4 (41.7–46.6) | 38 (35.5–40.1) | 36.4 (33.8–38.9) | 36.1 (33.5–38.7) | 6.3 | 7.8 | 1.5 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Bello, F.; Di Mauro, E.; Collà Ruvolo, C.; Creta, M.; La Rocca, R.; Celentano, G.; Capece, M.; Napolitano, L.; Morra, S.; Pezone, G.; et al. Perioperative Red Cell Line Trend following Robot-Assisted Radical Prostatectomy for Prostate Cancer. Medicina 2022, 58, 1520. https://doi.org/10.3390/medicina58111520
Di Bello F, Di Mauro E, Collà Ruvolo C, Creta M, La Rocca R, Celentano G, Capece M, Napolitano L, Morra S, Pezone G, et al. Perioperative Red Cell Line Trend following Robot-Assisted Radical Prostatectomy for Prostate Cancer. Medicina. 2022; 58(11):1520. https://doi.org/10.3390/medicina58111520
Chicago/Turabian StyleDi Bello, Francesco, Ernesto Di Mauro, Claudia Collà Ruvolo, Massimiliano Creta, Roberto La Rocca, Giuseppe Celentano, Marco Capece, Luigi Napolitano, Simone Morra, Gabriele Pezone, and et al. 2022. "Perioperative Red Cell Line Trend following Robot-Assisted Radical Prostatectomy for Prostate Cancer" Medicina 58, no. 11: 1520. https://doi.org/10.3390/medicina58111520