
Alterations in Plasma Lipidomic Profiles in Adult Patients with Schizophrenia and Major Depressive Disorder

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects and Sampling
2.2. Lipidomics Analysis
2.3. Statistical Analyses
3. Results
3.1. Clinical Characteristics of the Recruited Participants
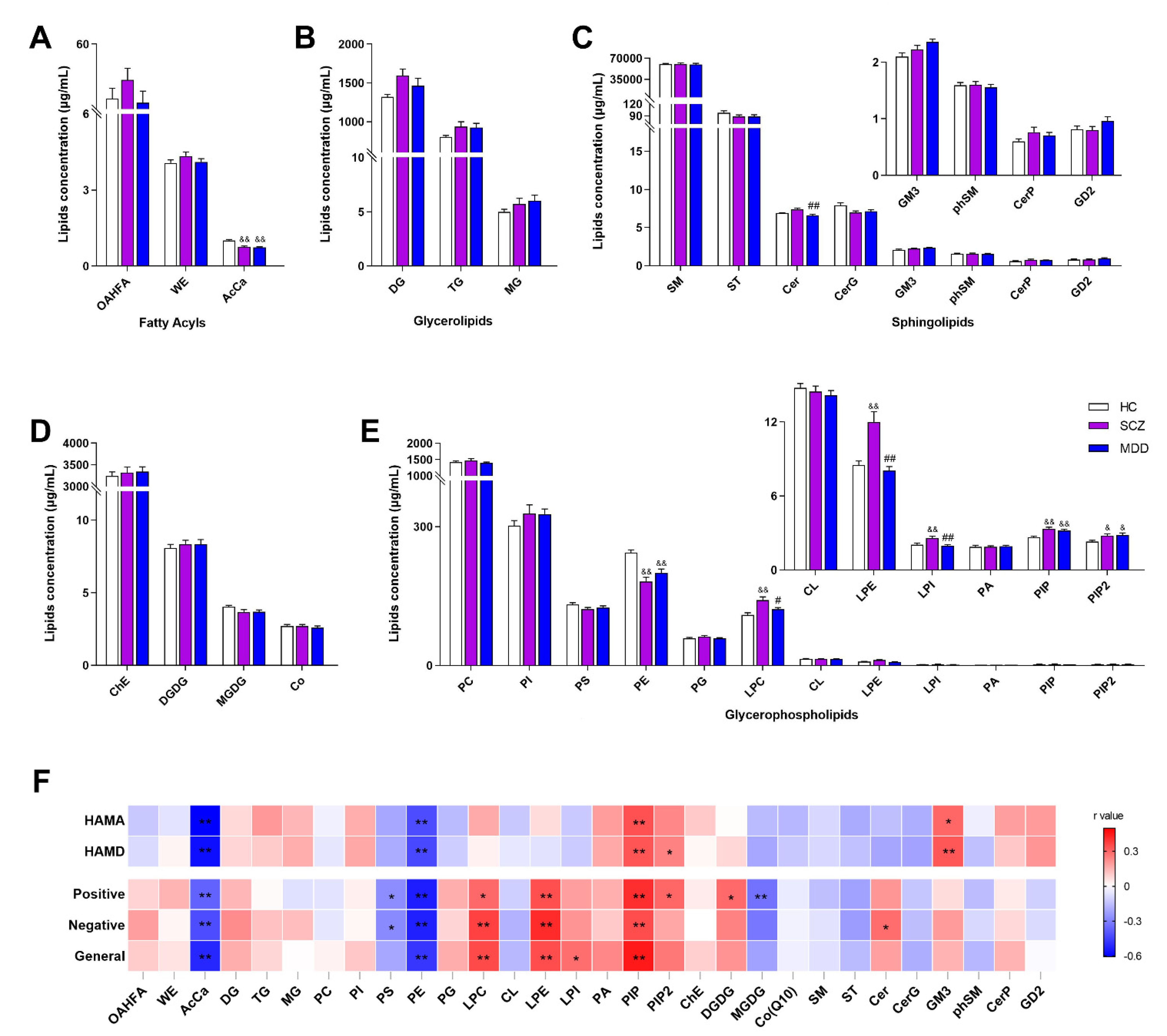
3.2. Alternation of Lipid at Class Level in SCZ and MDD
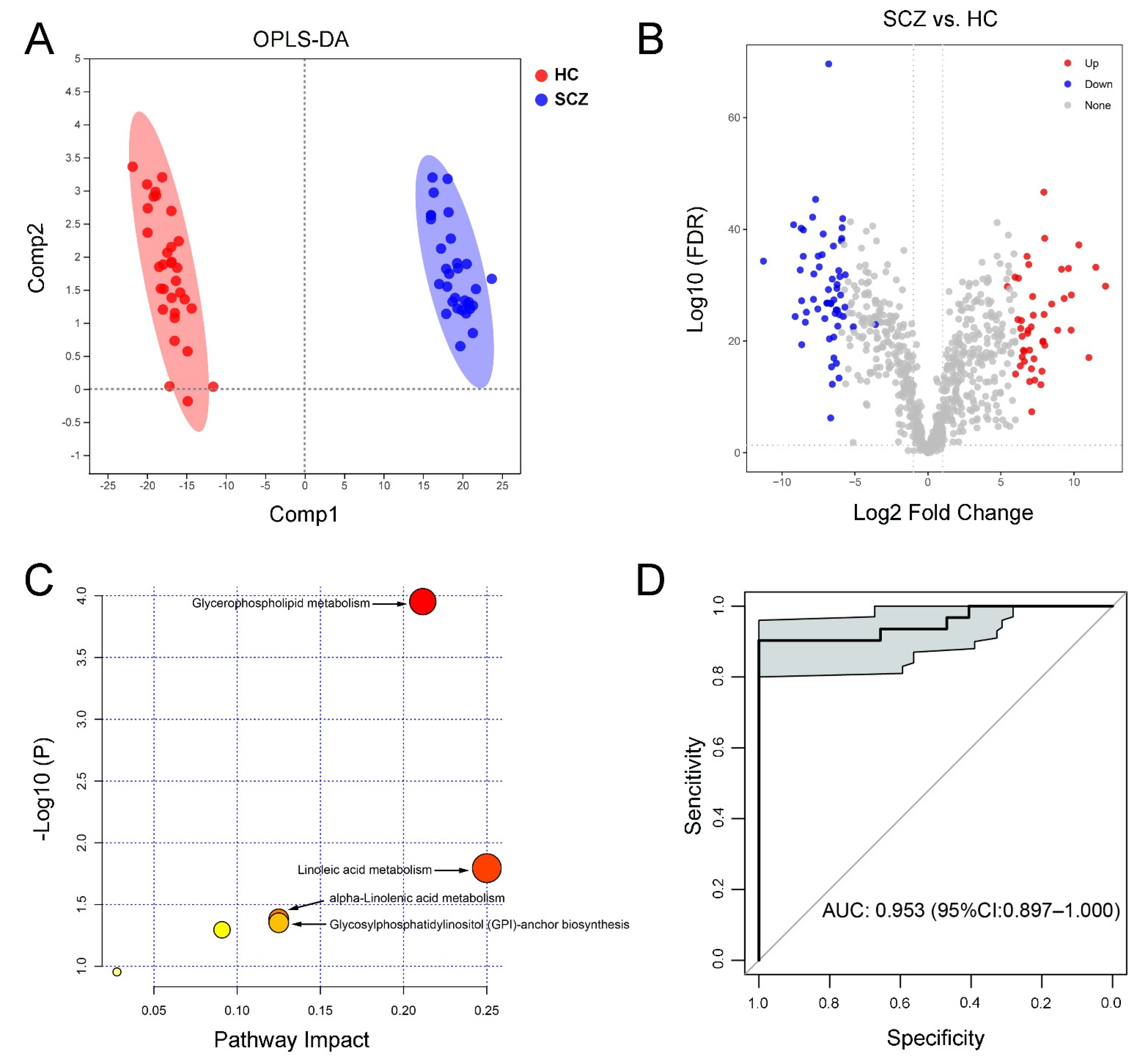
3.3. Characteristic Lipid Species between SCZ and HC
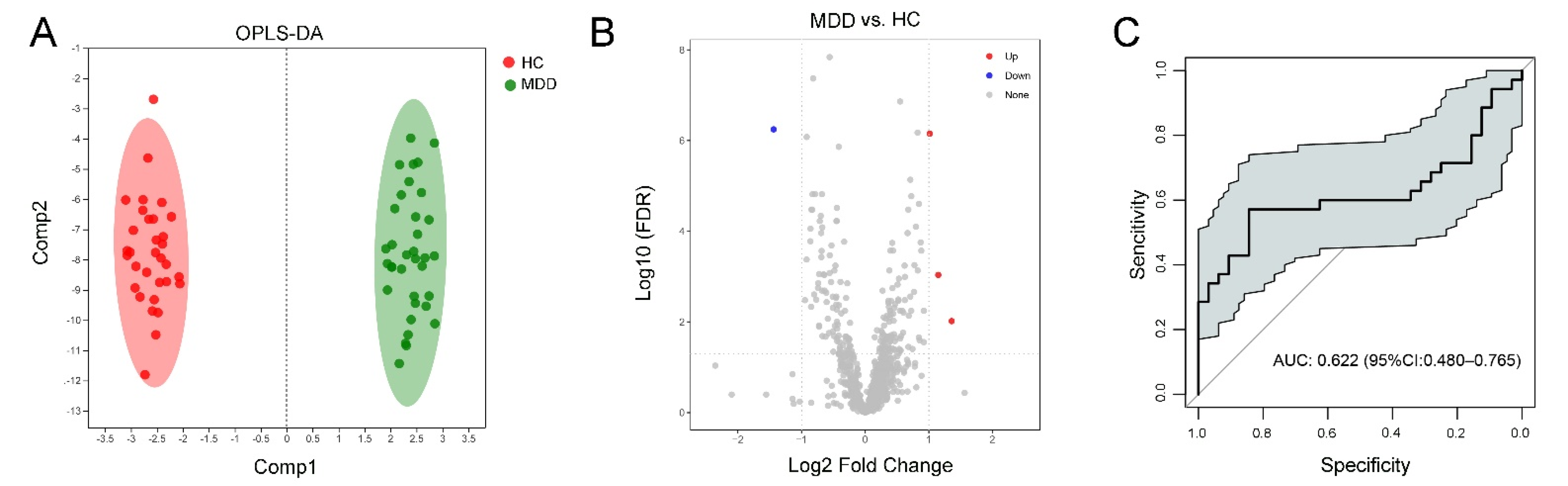
3.4. Characteristic Lipid Species in MDD and HC Groups
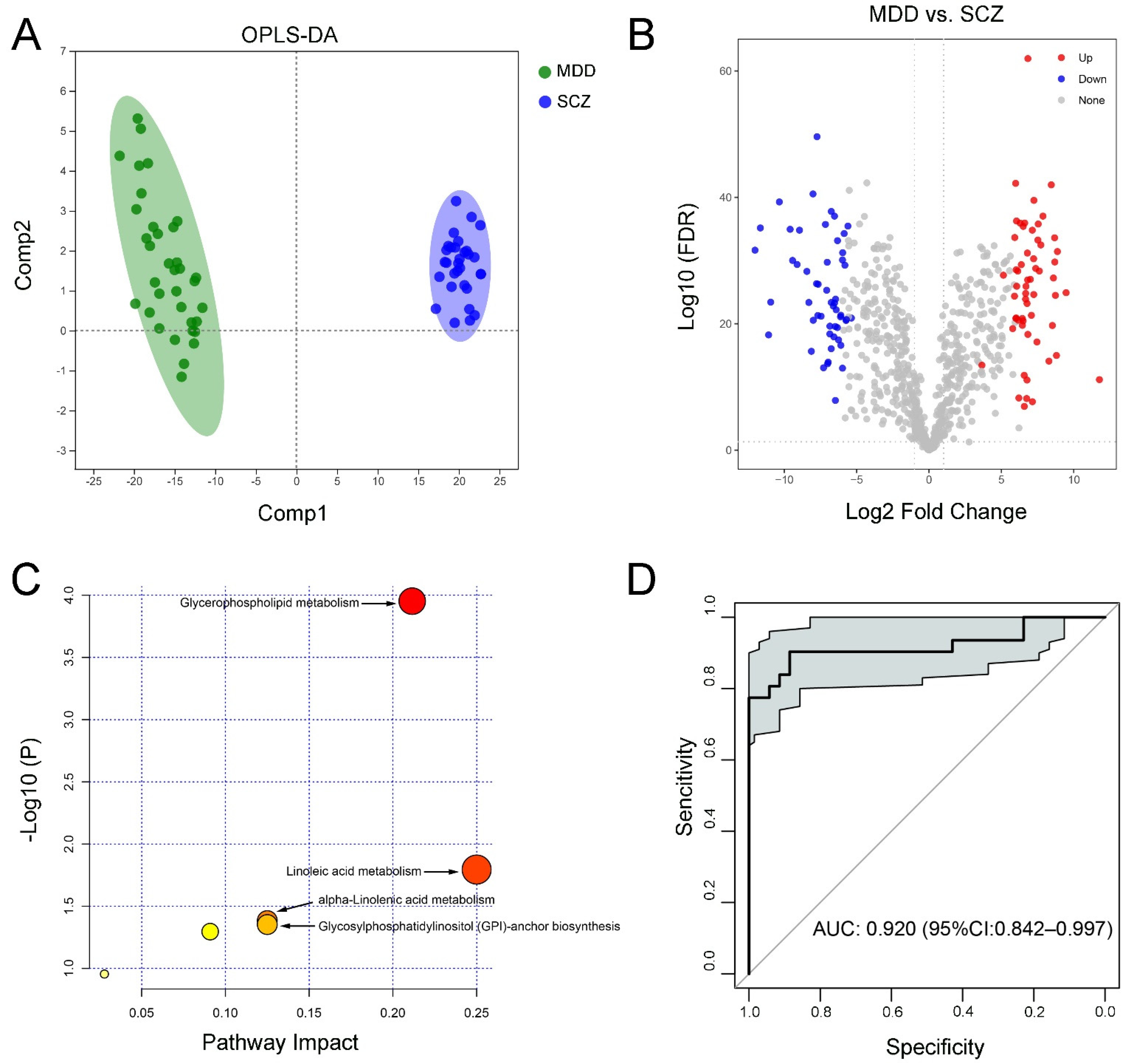
3.5. Characteristic Lipids between SCZ and MDD Groups
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gur, S.; Weizman, S.; Stubbs, B.; Matalon, A.; Meyerovitch, J.; Hermesh, H.; Krivoy, A. Mortality, morbidity and medical resources utilization of patients with schizophrenia: A case-control community-based study. Psychiatry Res. 2018, 260, 177–181. [Google Scholar] [CrossRef] [PubMed]
- Rotenstein, L.S.; Ramos, M.A.; Torre, M.; Segal, J.B.; Peluso, M.J.; Guille, C.; Sen, S.; Mata, D.A. Prevalence of Depression, Depressive Symptoms, and Suicidal Ideation Among Medical Students: A Systematic Review and Meta-Analysis. JAMA 2016, 316, 2214–2236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bromet, E.; Andrade, L.H.; Hwang, I.; Sampson, N.A.; Alonso, J.; de Girolamo, G.; de Graaf, R.; Demyttenaere, K.; Hu, C.; Iwata, N.; et al. Cross-national epidemiology of DSM-IV major depressive episode. BMC Med. 2011, 9, 90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Global Burden of Disease Study 2013 Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015, 386, 743–800. [Google Scholar] [CrossRef] [Green Version]
- Rosen, C.; Marvin, R.; Reilly, J.L.; Deleon, O.; Harris, M.S.; Keedy, S.K.; Solari, H.; Weiden, P.; Sweeney, J.A. Phenomenology of first-episode psychosis in schizophrenia, bipolar disorder, and unipolar depression: A comparative analysis. Clin. Schizophr. Relat. Psychoses 2012, 6, 145–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinez-Aran, A.; Vieta, E. Cognition as a target in schizophrenia, bipolar disorder and depression. Eur. Neuropsychopharmacol. 2015, 25, 151–157. [Google Scholar] [CrossRef]
- Grimm, O.; Heinz, A.; Walter, H.; Kirsch, P.; Erk, S.; Haddad, L.; Plichta, M.M.; Romanczuk-Seiferth, N.; Pohland, L.; Mohnke, S.; et al. Striatal response to reward anticipation: Evidence for a systems-level intermediate phenotype for schizophrenia. JAMA Psychiatry 2014, 71, 531–539. [Google Scholar] [CrossRef] [Green Version]
- Macoveanu, J.; Knorr, U.; Skimminge, A.; Sondergaard, M.G.; Jorgensen, A.; Fauerholdt-Jepsen, M.; Paulson, O.B.; Knudsen, G.M.; Siebner, H.R.; Kessing, L.V. Altered reward processing in the orbitofrontal cortex and hippocampus in healthy first-degree relatives of patients with depression. Psychol. Med. 2014, 44, 1183–1195. [Google Scholar] [CrossRef]
- Velthorst, E.; Nieman, D.H.; Becker, H.E.; van de Fliert, R.; Dingemans, P.M.; Klaassen, R.; de Haan, L.; van Amelsvoort, T.; Linszen, D.H. Baseline differences in clinical symptomatology between ultra high risk subjects with and without a transition to psychosis. Schizophr. Res. 2009, 109, 60–65. [Google Scholar] [CrossRef]
- Morgan, J.K.; Olino, T.M.; McMakin, D.L.; Ryan, N.D.; Forbes, E.E. Neural response to reward as a predictor of increases in depressive symptoms in adolescence. Neurobiol. Dis. 2013, 52, 66–74. [Google Scholar] [CrossRef]
- Fasmer, E.E.; Fasmer, O.B.; Berle, J.O.; Oedegaard, K.J.; Hauge, E.R. Graph theory applied to the analysis of motor activity in patients with schizophrenia and depression. PLoS ONE 2018, 13, e0194791. [Google Scholar] [CrossRef] [Green Version]
- Subodh, B.N.; Grover, S. Depression in schizophrenia: Prevalence and its impact on quality of life, disability, and functioning. Asian J. Psychiatry 2020, 54, 102425. [Google Scholar] [CrossRef]
- Peitl, V.; Vidrih, B.; Karlovic, Z.; Getaldic, B.; Peitl, M.; Karlovic, D. Platelet serotonin concentration and depressive symptoms in patients with schizophrenia. Psychiatry Res. 2016, 239, 105–110. [Google Scholar] [CrossRef] [PubMed]
- Rajkumar, R.P. Depressive Symptoms during an Acute Schizophrenic Episode: Frequency and Clinical Correlates. Depress. Res. Treat. 2015, 2015, 674641. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koyanagi, A.; Oh, H.; Stubbs, B.; Haro, J.M.; DeVylder, J.E. Epidemiology of depression with psychotic experiences and its association with chronic physical conditions in 47 low- and middle-income countries. Psychol. Med. 2017, 47, 531–542. [Google Scholar] [CrossRef] [Green Version]
- Shi, Y.; Song, R.; Wang, L.; Qi, Y.; Zhang, H.; Zhu, J.; Zhang, X.; Tang, X.; Zhan, Q.; Zhao, Y.; et al. Identifying Plasma Biomarkers with high specificity for major depressive disorder: A multi-level proteomics study. J. Affect. Disord. 2020, 277, 620–630. [Google Scholar] [CrossRef]
- Liu, J.Y.; Chen, H.Y.; Lin, J.J.; Lu, M.K.; Tan, H.P.; Jang, F.L.; Lin, S.H. Alterations of plasma cytokine biomarkers for identifying age at onset of schizophrenia with neurological soft signs. Int. J. Med. Sci. 2020, 17, 255–262. [Google Scholar] [CrossRef] [Green Version]
- Domenici, E.; Wille, D.R.; Tozzi, F.; Prokopenko, I.; Miller, S.; McKeown, A.; Brittain, C.; Rujescu, D.; Giegling, I.; Turck, C.W.; et al. Plasma protein biomarkers for depression and schizophrenia by multi analyte profiling of case-control collections. PLoS ONE 2010, 5, e9166. [Google Scholar] [CrossRef] [Green Version]
- Hashimoto, M.; Katakura, M.; Tanabe, Y.; Al Mamun, A.; Inoue, T.; Hossain, S.; Arita, M.; Shido, O. n-3 fatty acids effectively improve the reference memory-related learning ability associated with increased brain docosahexaenoic acid-derived docosanoids in aged rats. Biochim. Biophys. Acta 2015, 1851, 203–209. [Google Scholar] [CrossRef]
- McDougall, M.; Choi, J.; Magnusson, K.; Truong, L.; Tanguay, R.; Traber, M.G. Chronic vitamin E deficiency impairs cognitive function in adult zebrafish via dysregulation of brain lipids and energy metabolism. Free. Radic. Biol. Med. 2017, 112, 308–317. [Google Scholar] [CrossRef]
- Hussain, G.; Wang, J.; Rasul, A.; Anwar, H.; Imran, A.; Qasim, M.; Zafar, S.; Kamran, S.K.S.; Razzaq, A.; Aziz, N.; et al. Role of cholesterol and sphingolipids in brain development and neurological diseases. Lipids Health Dis. 2019, 18, 26. [Google Scholar] [CrossRef] [Green Version]
- Schneider, M.; Levant, B.; Reichel, M.; Gulbins, E.; Kornhuber, J.; Muller, C.P. Lipids in psychiatric disorders and preventive medicine. Neurosci. Biobehav. Rev. 2017, 76, 336–362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, E.Y.; Lee, J.W.; Lee, M.Y.; Kim, S.H.; Mok, H.J.; Ha, K.; Ahn, Y.M.; Kim, K.P. Serum lipidomic analysis for the discovery of biomarkers for major depressive disorder in drug-free patients. Psychiatry Res. 2018, 265, 174–182. [Google Scholar] [CrossRef] [PubMed]
- Aquino, A.; Alexandrino, G.L.; Guest, P.C.; Augusto, F.; Gomes, A.F.; Murgu, M.; Steiner, J.; Martins-de-Souza, D. Blood-Based Lipidomics Approach to Evaluate Biomarkers Associated With Response to Olanzapine, Risperidone, and Quetiapine Treatment in Schizophrenia Patients. Front. Psychiatry 2018, 9, 209. [Google Scholar] [CrossRef] [PubMed]
- Fu, Y.; Chen, N.; Wang, Z.; Luo, S.; Ding, Y.; Lu, B. Degradation of lipid droplets by chimeric autophagy-tethering compounds. Cell Res. 2021, 31, 965–979. [Google Scholar] [CrossRef]
- Sun, Y.; Song, K.; Liu, L.; Sun, L.; Qin, Q.; Jiang, T.; Zhou, B.; Zhu, C.; Xu, G.; Sun, S.; et al. Silencing of Sulfoquinovosyl Diacylglycerol Synthase 1 Impairs the Glycolipids Accumulation and Photosynthesis in Phosphate-deprived Rice. J. Exp. Bot. 2021, 72, 6510–6523. [Google Scholar] [CrossRef]
- Cajka, T.; Smilowitz, J.T.; Fiehn, O. Validating Quantitative Untargeted Lipidomics Across Nine Liquid Chromatography-High-Resolution Mass Spectrometry Platforms. Anal. Chem. 2017, 89, 12360–12368. [Google Scholar] [CrossRef]
- Gohar, S.M.; Dieset, I.; Steen, N.E.; Morch, R.H.; Iversen, T.S.; Steen, V.M.; Andreassen, O.A.; Melle, I. Association between serum lipid levels, osteoprotegerin and depressive symptomatology in psychotic disorders. Eur. Arch. Psychiatry Clin. Neurosci. 2019, 269, 795–802. [Google Scholar] [CrossRef] [Green Version]
- Walther, A.; Cannistraci, C.V.; Simons, K.; Duran, C.; Gerl, M.J.; Wehrli, S.; Kirschbaum, C. Lipidomics in Major Depressive Disorder. Front. Psychiatry 2018, 9, 459. [Google Scholar] [CrossRef] [Green Version]
- Guo, L.; Zhang, T.; Li, R.; Cui, Z.Q.; Du, J.; Yang, J.B.; Xue, F.; Chen, Y.H.; Tan, Q.R.; Peng, Z.W. Alterations in the Plasma Lipidome of Adult Women With Bipolar Disorder: A Mass Spectrometry-Based Lipidomics Research. Front. Psychiatry 2022, 13, 802710. [Google Scholar] [CrossRef]
- Ghosh, S.; Dyer, R.A.; Beasley, C.L. Evidence for altered cell membrane lipid composition in postmortem prefrontal white matter in bipolar disorder and schizophrenia. J. Psychiatry Res. 2017, 95, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Cheng, S.L.; Fei, Q.; Gu, H.; Raftery, D.; Cao, B.; Sun, X.; Yan, J.; Zhang, C.; Wang, J. Metabolic profiling identifies phospholipids as potential serum biomarkers for schizophrenia. Psychiatry Res. 2019, 272, 18–29. [Google Scholar] [CrossRef] [PubMed]
- Demirkan, A.; Isaacs, A.; Ugocsai, P.; Liebisch, G.; Struchalin, M.; Rudan, I.; Wilson, J.F.; Pramstaller, P.P.; Gyllensten, U.; Campbell, H.; et al. Plasma phosphatidylcholine and sphingomyelin concentrations are associated with depression and anxiety symptoms in a Dutch family-based lipidomics study. J. Psychiatry Res. 2013, 47, 357–362. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A.T.; MahmoudianDehkordi, S.; Bhattacharyya, S.; Arnold, M.; Liu, D.; Neavin, D.; Moseley, M.A.; Thompson, J.W.; Williams, L.S.J.; Louie, G.; et al. Acylcarnitine metabolomic profiles inform clinically-defined major depressive phenotypes. J. Affect. Disord. 2020, 264, 90–97. [Google Scholar] [CrossRef] [PubMed]
- Maldonado, C.; Vazquez, M.; Fagiolino, P. Potential Therapeutic Role of Carnitine and Acetylcarnitine in Neurological Disorders. Curr. Pharm. Des. 2020, 26, 1277–1285. [Google Scholar] [CrossRef] [PubMed]
- MahmoudianDehkordi, S.; Ahmed, A.T.; Bhattacharyya, S.; Han, X.; Baillie, R.A.; Arnold, M.; Skime, M.K.; John-Williams, L.S.; Moseley, M.A.; Thompson, J.W.; et al. Alterations in acylcarnitines, amines, and lipids inform about the mechanism of action of citalopram/escitalopram in major depression. Transl. Psychiatry 2021, 11, 153. [Google Scholar] [CrossRef]
- Cao, B.; Wang, D.; Pan, Z.; Brietzke, E.; McIntyre, R.S.; Musial, N.; Mansur, R.B.; Subramanieapillai, M.; Zeng, J.; Huang, N.; et al. Characterizing acyl-carnitine biosignatures for schizophrenia: A longitudinal pre- and post-treatment study. Transl. Psychiatry 2019, 9, 19. [Google Scholar] [CrossRef] [Green Version]
- Bruno, A.; Pandolfo, G.; Crucitti, M.; Lorusso, S.; Zoccali, R.A.; Muscatello, M.R. Acetyl-L-Carnitine Augmentation of Clozapine in Partial-Responder Schizophrenia: A 12-Week, Open-Label Uncontrolled Preliminary Study. Clin. Neuropharmacol. 2016, 39, 277–280. [Google Scholar] [CrossRef]
- van Meer, G.; Voelker, D.R.; Feigenson, G.W. Membrane lipids: Where they are and how they behave. Nat. Rev. Mol. Cell Biol. 2008, 9, 112–124. [Google Scholar] [CrossRef]
- Jones, L.L.; McDonald, D.A.; Borum, P.R. Acylcarnitines: Role in brain. Prog. Lipid Res. 2010, 49, 61–75. [Google Scholar] [CrossRef]
- Steenbergen, R.; Nanowski, T.S.; Beigneux, A.; Kulinski, A.; Young, S.G.; Vance, J.E. Disruption of the phosphatidylserine decarboxylase gene in mice causes embryonic lethality and mitochondrial defects. J. Biol. Chem. 2005, 280, 40032–40040. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, Y.; Vadodaria, K.C.; Lenkei, Z.; Kato, T.; Gage, F.H.; Marchetto, M.C.; Santos, R. Mitochondria, Metabolism, and Redox Mechanisms in Psychiatric Disorders. Antioxid. Redox Signal. 2019, 31, 275–317. [Google Scholar] [CrossRef] [PubMed]
- Di Paolo, G.; De Camilli, P. Phosphoinositides in cell regulation and membrane dynamics. Nature 2006, 443, 651–657. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.J.; Jeong, M.J.; Jo, H.J.; Jung, J.H.; Kaang, B.K.; Choi, Y.B.; Kim, J.H. Identification of postsynaptic phosphatidylinositol-4,5-bisphosphate (PIP2) roles for synaptic plasticity using chemically induced dimerization. Sci. Rep. 2017, 7, 3351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, L.; Chao, Y.; Cheng, P.; Li, N.; Zheng, H.; Yang, Y. UPLC-QTOF/MS-Based Metabolomics Reveals the Protective Mechanism of Hydrogen on Mice with Ischemic Stroke. Neurochem. Res. 2019, 44, 1950–1963. [Google Scholar] [CrossRef]
- Yang, L.V.; Radu, C.G.; Wang, L.; Riedinger, M.; Witte, O.N. Gi-independent macrophage chemotaxis to lysophosphatidylcholine via the immunoregulatory GPCR G2A. Blood 2005, 105, 1127–1134. [Google Scholar] [CrossRef] [Green Version]
- Qin, X.; Qiu, C.; Zhao, L. Lysophosphatidylcholine perpetuates macrophage polarization toward classically activated phenotype in inflammation. Cell. Immunol. 2014, 289, 185–190. [Google Scholar] [CrossRef]
- Law, S.H.; Chan, M.L.; Marathe, G.K.; Parveen, F.; Chen, C.H.; Ke, L.Y. An Updated Review of Lysophosphatidylcholine Metabolism in Human Diseases. Int. J. Mol. Sci. 2019, 20, 1149. [Google Scholar] [CrossRef] [Green Version]
- Qiao, J.; Huang, F.; Naikawadi, R.P.; Kim, K.S.; Said, T.; Lum, H. Lysophosphatidylcholine impairs endothelial barrier function through the G protein-coupled receptor GPR4. Am. J. Physiol. Lung Cell. Mol. Physiol. 2006, 291, L91–L101. [Google Scholar] [CrossRef]
- Plemel, J.R.; Michaels, N.J.; Weishaupt, N.; Caprariello, A.V.; Keough, M.B.; Rogers, J.A.; Yukseloglu, A.; Lim, J.; Patel, V.V.; Rawji, K.S.; et al. Mechanisms of lysophosphatidylcholine-induced demyelination: A primary lipid disrupting myelinopathy. Glia 2018, 66, 327–347. [Google Scholar] [CrossRef]
- Llano, D.A.; Devanarayan, V.; Alzheimer’s Disease Neuroimaging Initiative. Serum Phosphatidylethanolamine and Lysophosphatidylethanolamine Levels Differentiate Alzheimer’s Disease from Controls and Predict Progression from Mild Cognitive Impairment. J. Alzheimers Dis. 2021, 80, 311–319. [Google Scholar] [CrossRef] [PubMed]
- Kurano, M.; Kobayashi, T.; Sakai, E.; Tsukamoto, K.; Yatomi, Y. Lysophosphatidylinositol, especially albumin-bound form, induces inflammatory cytokines in macrophages. FASEB J. 2021, 35, e21673. [Google Scholar] [CrossRef]
- Minamihata, T.; Takano, K.; Moriyama, M.; Nakamura, Y. Lysophosphatidylinositol, an Endogenous Ligand for G Protein-Coupled Receptor 55, Has Anti-inflammatory Effects in Cultured Microglia. Inflammation 2020, 43, 1971–1987. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Xiu, M.; Liu, H.; Wang, J.; Li, X. Plasma Lysophosphatidylcholine and Lysophosphatidylethanolamine Levels Were Associated With the Therapeutic Response to Olanzapine in Female Antipsychotics-naive First-episode Patients With Schizophrenia. Front. Pharmacol. 2021, 12, 735196. [Google Scholar] [CrossRef]
- Brunkhorst-Kanaan, N.; Klatt-Schreiner, K.; Hackel, J.; Schroter, K.; Trautmann, S.; Hahnefeld, L.; Wicker, S.; Reif, A.; Thomas, D.; Geisslinger, G.; et al. Targeted lipidomics reveal derangement of ceramides in major depression and bipolar disorder. Metabolism 2019, 95, 65–76. [Google Scholar] [CrossRef] [PubMed]
- Kornhuber, J.; Muller, C.P.; Becker, K.A.; Reichel, M.; Gulbins, E. The ceramide system as a novel antidepressant target. Trends Pharmacol. Sci. 2014, 35, 293–304. [Google Scholar] [CrossRef] [PubMed]
- Kurz, J.; Parnham, M.J.; Geisslinger, G.; Schiffmann, S. Ceramides as Novel Disease Biomarkers. Trends Mol. Med. 2019, 25, 20–32. [Google Scholar] [CrossRef]
- Yang, J.; Chen, T.; Sun, L.; Zhao, Z.; Qi, X.; Zhou, K.; Cao, Y.; Wang, X.; Qiu, Y.; Su, M.; et al. Potential metabolite markers of schizophrenia. Mol. Psychiatry 2013, 18, 67–78. [Google Scholar] [CrossRef] [Green Version]
- Yin, X.; Mongan, D.; Cannon, M.; Zammit, S.; Hyotylainen, T.; Oresic, M.; Brennan, L.; Cotter, D.R. Plasma lipid alterations in young adults with psychotic experiences: A study from the Avon Longitudinal Study of Parents and Children cohort. Schizophr. Res. 2022, 243, 78–85. [Google Scholar] [CrossRef]
- Oresic, M.; Seppanen-Laakso, T.; Sun, D.; Tang, J.; Therman, S.; Viehman, R.; Mustonen, U.; van Erp, T.G.; Hyotylainen, T.; Thompson, P.; et al. Phospholipids and insulin resistance in psychosis: A lipidomics study of twin pairs discordant for schizophrenia. Genome Med. 2012, 4, 1. [Google Scholar] [CrossRef]
- McEvoy, J.; Baillie, R.A.; Zhu, H.; Buckley, P.; Keshavan, M.S.; Nasrallah, H.A.; Dougherty, G.G.; Yao, J.K.; Kaddurah-Daouk, R. Lipidomics reveals early metabolic changes in subjects with schizophrenia: Effects of atypical antipsychotics. PLoS ONE 2013, 8, e68717. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y.; Song, X.; Liu, X.; Pu, J.; Gui, S.; Xu, S.; Tian, L.; Zhong, X.; Zhao, L.; Wang, H.; et al. Alteration of lipids and amino acids in plasma distinguish schizophrenia patients from controls: A targeted metabolomics study. Psychiatry Clin. Neurosci. 2021, 75, 138–144. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Li, J.; Zheng, P.; Zhao, X.; Zhou, C.; Hu, C.; Hou, X.; Wang, H.; Xie, P.; Xu, G. Plasma lipidomics reveals potential lipid markers of major depressive disorder. Anal. Bioanal. Chem. 2016, 408, 6497–6507. [Google Scholar] [CrossRef] [PubMed]
- Robinson, D.G.; Gallego, J.A.; John, M.; Hanna, L.A.; Zhang, J.P.; Birnbaum, M.L.; Greenberg, J.; Naraine, M.; Peters, B.D.; McNamara, R.K.; et al. A potential role for adjunctive omega-3 polyunsaturated fatty acids for depression and anxiety symptoms in recent onset psychosis: Results from a 16week randomized placebo-controlled trial for participants concurrently treated with risperidone. Schizophr. Res. 2019, 204, 295–303. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.J.; Lim, S.Y.; Lee, H.J.; Lee, J.Y.; Choi, S.; Kim, S.Y.; Kim, J.M.; Shin, I.S.; Yoon, J.S.; Yang, S.J.; et al. Low dietary intake of n-3 fatty acids, niacin, folate, and vitamin C in Korean patients with schizophrenia and the development of dietary guidelines for schizophrenia. Nutr. Res. 2017, 45, 10–18. [Google Scholar] [CrossRef]
- Slade, E.; Irvin, M.R.; Xie, K.; Arnett, D.K.; Claas, S.A.; Kind, T.; Fardo, D.W.; Graf, G.A. Age and sex are associated with the plasma lipidome: Findings from the GOLDN study. Lipids Health Dis. 2021, 20, 30. [Google Scholar] [CrossRef]
- Wong, M.W.K.; Braidy, N.; Pickford, R.; Vafaee, F.; Crawford, J.; Muenchhoff, J.; Schofield, P.; Attia, J.; Brodaty, H.; Sachdev, P.; et al. Plasma lipidome variation during the second half of the human lifespan is associated with age and sex but minimally with BMI. PLoS ONE 2019, 14, e0214141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Winter, G.; Hart, R.A.; Charlesworth, R.P.G.; Sharpley, C.F. Gut microbiome and depression: What we know and what we need to know. Rev. Neurosci. 2018, 29, 629–643. [Google Scholar] [CrossRef]
- Zhu, F.; Guo, R.; Wang, W.; Ju, Y.; Wang, Q.; Ma, Q.; Sun, Q.; Fan, Y.; Xie, Y.; Yang, Z.; et al. Transplantation of microbiota from drug-free patients with schizophrenia causes schizophrenia-like abnormal behaviors and dysregulated kynurenine metabolism in mice. Mol. Psychiatry 2020, 25, 2905–2918. [Google Scholar] [CrossRef]
- Chen, L.M.; Bao, C.H.; Wu, Y.; Liang, S.H.; Wang, D.; Wu, L.Y.; Huang, Y.; Liu, H.R.; Wu, H.G. Tryptophan-kynurenine metabolism: A link between the gut and brain for depression in inflammatory bowel disease. J. Neuroinflamm. 2021, 18, 135. [Google Scholar] [CrossRef]
- Yuan, B.; Sun, X.; Xu, Z.; Pu, M.; Yuan, Y.; Zhang, Z. Influence of genetic polymorphisms in homocysteine and lipid metabolism systems on antidepressant drug response. BMC Psychiatry 2020, 20, 408. [Google Scholar] [CrossRef] [PubMed]
- Bekhbat, M.; Chu, K.; Le, N.A.; Woolwine, B.J.; Haroon, E.; Miller, A.H.; Felger, J.C. Glucose and lipid-related biomarkers and the antidepressant response to infliximab in patients with treatment-resistant depression. Psychoneuroendocrinology 2018, 98, 222–229. [Google Scholar] [CrossRef] [PubMed]
- Dietrich-Muszalska, A.; Kolinska-Lukaszuk, J. Comparative effects of aripiprazole and selected antipsychotic drugs on lipid peroxidation in plasma. Psychiatry Clin. Neurosci. 2018, 72, 329–336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Himmerich, H.; Minkwitz, J.; Kirkby, K.C. Weight Gain and Metabolic Changes During Treatment with Antipsychotics and Antidepressants. Endocr. Metab. Immune Disord. Drug Targets 2015, 15, 252–260. [Google Scholar] [CrossRef] [PubMed]
- Murashita, M.; Inoue, T.; Kusumi, I.; Nakagawa, S.; Itoh, K.; Tanaka, T.; Izumi, T.; Hosoda, H.; Kangawa, K.; Koyama, T. Glucose and lipid metabolism of long-term risperidone monotherapy in patients with schizophrenia. Psychiatry Clin. Neurosci. 2007, 61, 54–58. [Google Scholar] [CrossRef]
- Wang, Z.H.; Zheng, K.I.; Wang, X.D.; Qiao, J.; Li, Y.Y.; Zhang, L.; Zheng, M.H.; Wu, J. LC-MS-based lipidomic analysis in distinguishing patients with nonalcoholic steatohepatitis from nonalcoholic fatty liver. Hepatobiliary Pancreat Dis. Int. 2021, 20, 452–459. [Google Scholar] [CrossRef]
- You, Q.; Peng, Q.; Yu, Z.; Jin, H.; Zhang, J.; Sun, W.; Huang, Y. Plasma lipidomic analysis of sphingolipids in patients with large artery atherosclerosis cerebrovascular disease and cerebral small vessel disease. Biosci. Rep. 2020, 40, BSR20201519. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | HC (n = 32) | MDD (n = 35) | SCZ (n = 31) | H/χ2/F/Z Value | p-Value |
|---|---|---|---|---|---|
| Sociodemographic | |||||
| Age [years, M (P25, P75)] a | 29 (25, 36.75) | 34.5 (28.5, 38) | 28 (24, 37) | H = 5.435 | 0.066 |
| Gender (male/female) b | 10/22 | 12 / 23 | 12 / 19 | χ2 = 0.391 | 0.803 |
| BMI [kg/m2, [M (P25, P75)]] a | 20.7 (18.89, 23.55) | 21.45 (18.75, 23.23) | 20.76 (19.28, 24.46) | H = 1.113 | 0.573 |
| Marital status (single/married) b | 13/19 | 2/33 | 22/9 | χ2 = 29.953 | <0.001 |
| Duration of illness [mouths, M (P25, P75)] c | - | 36 (12, 60) | 48 (24, 48) | Z = −0.466 | 0.641 |
| Smoking or exposure to secondhand smoke situation in the past six months b | 24/8 | 19/16 | 23/8 | χ2 = 4.228 | 0.13 |
| TG [mmol/L, M (P25, P75)] a | 0.91 (0.7, 1.27) | 0.82 (0.7, 1.29) | 1.21 (0.69, 2.01) | H = 4.35 | 0.114 |
| LDL c | 2.21 ± 0.91 | 2.89 ± 0.90 * | 2.50 ± 0.66 | F = 5.802 | 0.004 |
| HDL a | 1.25 ± 0.38 | 1.41 ± 0.28 | 1.28 ± 0.21 | H = 5.071 | 0.079 |
| CHOL c | 4.18 ± 0.84 | 4.32 ± 0.84 | 4.12 ± 0.86 | F = 0.461 | 0.632 |
| Scale evaluation | |||||
| HAM-D [M (P25, P75)] d | 3 (2, 5) | 25 (21, 26) | - | Z = −6.926 | <0.001 |
| HAM-A [M (P25, P75)] d | 4.5 (2.25, 6.75) | 25 (20, 29) | - | Z = −7.045 | <0.001 |
| PANSS total score [mean ± SD (range)] a | 35.78 ± 3.63 (30–42) | 59.11 ± 10.84 (37–80) * | 72.74 ± 17.99 (38–121) * | H = 64.436 | <0.001 |
| PANSS positive scale [M (P25, P75)] a | 7 (7, 9) | 7 (7, 7) | 20 (16, 25) *# | H = 68.09 | <0.001 |
| PANSS negative scale [M (P25, P75)] a | 8 (7, 9) | 11 (7, 14) * | 15 (12, 20) *# | H = 42.988 | <0.001 |
| PANSS general scale [M (P25, P75)] a | 19.5 (17.25, 22) | 42 (35, 46) * | 37 (34, 43) * | H = 61.577 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, F.; Guo, L.; Zhang, T.; Cui, Z.; Wang, J.; Zhang, C.; Xue, F.; Zhou, C.; Li, B.; Tan, Q.; et al. Alterations in Plasma Lipidomic Profiles in Adult Patients with Schizophrenia and Major Depressive Disorder. Medicina 2022, 58, 1509. https://doi.org/10.3390/medicina58111509
Wang F, Guo L, Zhang T, Cui Z, Wang J, Zhang C, Xue F, Zhou C, Li B, Tan Q, et al. Alterations in Plasma Lipidomic Profiles in Adult Patients with Schizophrenia and Major Depressive Disorder. Medicina. 2022; 58(11):1509. https://doi.org/10.3390/medicina58111509
Chicago/Turabian StyleWang, Fei, Lin Guo, Ting Zhang, Zhiquan Cui, Jinke Wang, Chi Zhang, Fen Xue, Cuihong Zhou, Baojuan Li, Qingrong Tan, and et al. 2022. "Alterations in Plasma Lipidomic Profiles in Adult Patients with Schizophrenia and Major Depressive Disorder" Medicina 58, no. 11: 1509. https://doi.org/10.3390/medicina58111509