
Increase in Lower Limb Strength after Multimodal Pain Management in Patients with Low Back Pain

Abstract
:1. Introduction
2. Material and Methods
2.1. Study Population
2.2. Treatment Algorithm
2.3. Measurement
2.4. Statistical Analysis
3. Results
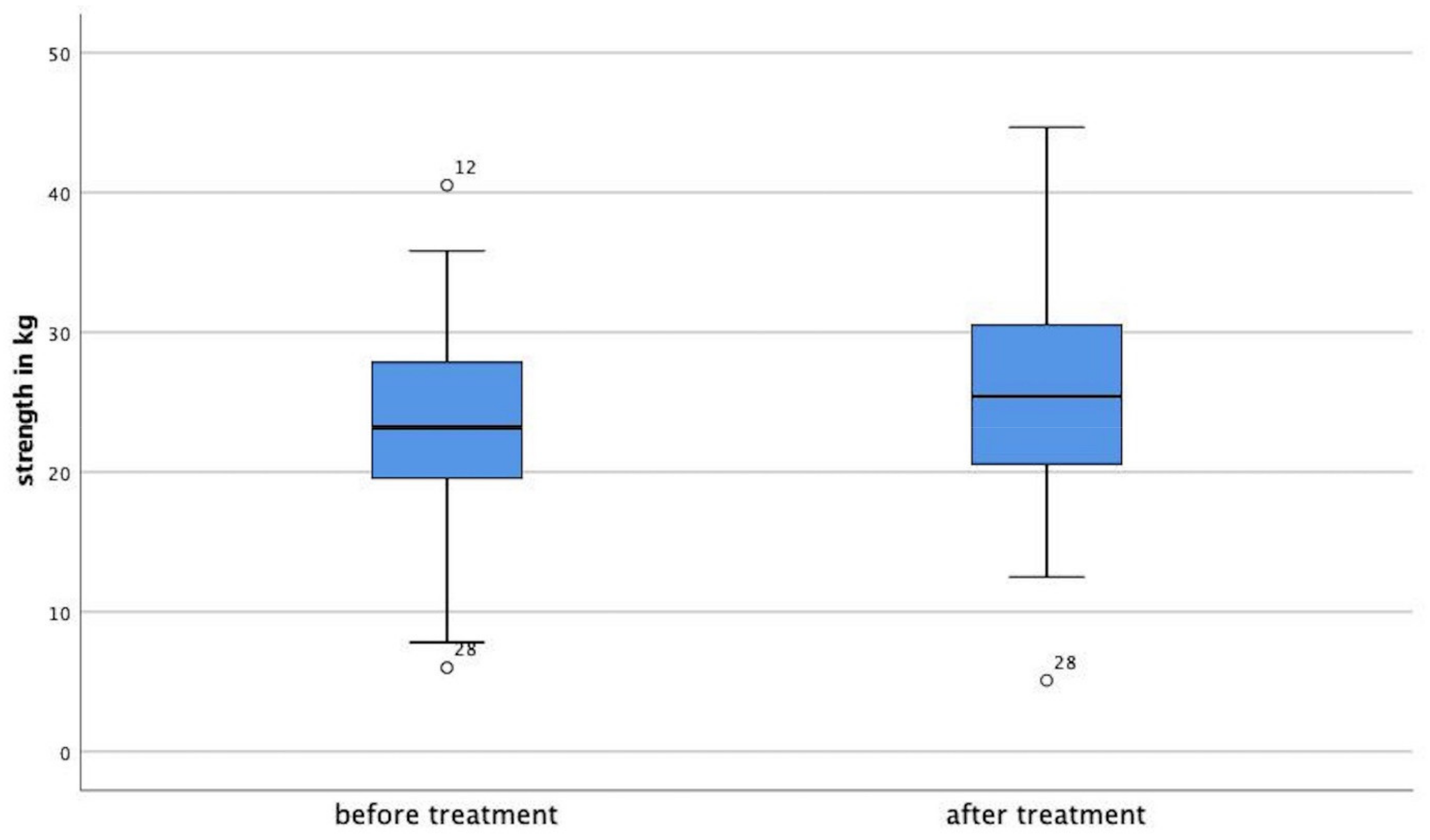
3.1. Strength Development
3.2. Side-to-Side Differences
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Katz, J.N. Lumbar disc disorders and low-back pain: Socioeconomic factors and consequences. JBJS 2006, 88, 21–24. [Google Scholar] [CrossRef]
- Benditz, A.; Loher, M.; Boluki, D.; Grifka, J.; Völlner, F.; Renkawitz, T.; Maderbacher, G.; Götz, J. Positive medium-term influence of multimodal pain management on socioeconomic factors and health care utilization in patients with lumbar radiculopathy: A prospective study. J. Pain Res. 2017, 10, 389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vos, T.; Abajobir, A.A.; Abate, K.H.; Abbafati, C.; Abbas, K.M.; Abd-Allah, F.; Abdulkader, R.S.; Abdulle, A.M.; Abebo, T.A.; Abera, S.F.; et al. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1211–1259. [Google Scholar] [CrossRef] [Green Version]
- Neuhauser, H.; Ellert, U.; Ziese, T. Chronic back pain in the general population in Germany 2002/2003: Prevalence and highly affected population groups. Gesundh. (Bundesverb. Arzte Offentlichen Gesundh.) 2005, 67, 685. [Google Scholar] [CrossRef]
- Freburger, J.K.; Holmes, G.M.; Agans, R.P.; Jackman, A.M.; Darter, J.D.; Wallace, A.S.; Castel, L.D.; Kalsbeek, W.D.; Carey, T.S. The rising prevalence of chronic low back pain. Arch. Intern. Med. 2009, 169, 251–258. [Google Scholar] [CrossRef] [Green Version]
- Heuch, I.; Heuch, I.; Hagen, K.; Zwart, J.A. Body mass index as a risk factor for developing chronic low back pain: A follow-up in the Nord-Trøndelag Health Study. Spine 2013, 38, 133–139. [Google Scholar] [CrossRef]
- Jacobs, J.M.; Hammerman-Rozenberg, R.; Cohen, A.; Stessman, J. Chronic back pain among the elderly: Prevalence, associations, and predictors. Spine 2006, 31, E203–E207. [Google Scholar] [CrossRef]
- Freynhagen, R.; Parada, H.A.; Calderon-Ospina, C.-A.; Chen, J.; Emril, D.R.; Fernandez-Villacorta, F.J.; Franco, H.; Ho, K.-Y.; Lara-Solares, A.; Li, C.C.-F.; et al. Current understanding of the mixed pain concept: A brief narrative review. Curr. Med. Res. Opin. 2019, 35, 1011–1018. [Google Scholar] [CrossRef] [Green Version]
- Knezevic, N.N.; Candido, K.D.; Vlaeyen, J.W.S.; Van Zundert, J.; Cohen, S.P. Low back pain. Lancet 2021, 398, 78–92. [Google Scholar] [CrossRef]
- Calderon-Ospina, C.A.; Nava-Mesa, M.O.; Arbeláez Ariza, C.E. Effect of Combined Diclofenac and B Vitamins (Thiamine, Pyridoxine, and Cyanocobalamin) for Low Back Pain Management: Systematic Review and Meta-analysis. Pain Med. 2020, 21, 766–781. [Google Scholar] [CrossRef] [Green Version]
- Buchner, M.; Zeifang, F.; Brocai, D.R.; Schiltenwolf, M. Epidural corticosteroid injection in the conservative management of sciatica. Clin. Orthop. Relat. Res. 2000, 375, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Karppinen, J.; Malmivaara, A.; Kurunlahti, M.; Kyllönen, E.; Pienimaki, T.; Nieminen, P.; Ohinmaa, A.; Tervonen, O.; Vanharanta, H. Periradicular infiltration for sciatica: A randomized controlled trial. Spine 2001, 26, 1059–1067. [Google Scholar] [CrossRef] [PubMed]
- Faber, F.; Benditz, A.; Boluki, D.; Grifka, J. Application of image-guided injection for cervical and lumbar syndromes. Z. Rheumatol. 2020, 79, 367–378. [Google Scholar] [CrossRef]
- Benditz, A.; Madl, M.; Loher, M.; Grifka, J.; Boluki, D.; Linhardt, O. Prospective medium-term results of multimodal pain management in patients with lumbar radiculopathy. Sci. Rep. 2016, 6, 28187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guzmán, J.; Esmail, R.; Karjalainen, K.; Malmivaara, A.; Irvin, E.; Bombardier, C. Multidisciplinary rehabilitation for chronic low back pain: Systematic review. BMJ 2001, 322, 1511–1516. [Google Scholar] [CrossRef] [Green Version]
- Neubauer, E.; Zahlten-Hinguranage, A.; Schiltenwolf, M.; Buchner, M. Multimodale Therapie bei chronischem HWS- und LWS-Schmerz. Der Schmerz 2006, 20, 210–218. [Google Scholar] [CrossRef]
- Kamper, S.J.; Apeldoorn, A.T.; Chiarotto, A.; Smeets, R.; Ostelo, R.; Guzman, J.; van Tulder, M. Multidisciplinary biopsychosocial rehabilitation for chronic low back pain. Cochrane Database Syst. Rev. 2014, CD000963. [Google Scholar] [CrossRef]
- Kraemer, J.; Ludwig, J.; Bickert, U.; Owczarek, V.; Traupe, M. Lumbar epidural perineural injection: A new technique. Eur. Spine J. 1997, 6, 357–361. [Google Scholar] [CrossRef]
- Mentiplay, B.F.; Perraton, L.G.; Bower, K.J.; Adair, B.; Pua, Y.-H.; Williams, G.P.; McGaw, R.; Clark, R.A. Assessment of Lower Limb Muscle Strength and Power Using Hand-Held and Fixed Dynamometry: A Reliability and Validity Study. PLoS ONE 2015, 10, e0140822. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burns, S.P.; Spanier, D.E. Break-technique handheld dynamometry: Relation between angular velocity and strength measurements. Arch. Phys. Med. Rehabil. 2005, 86, 1420–1426. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wadsworth, C.T.; Nielsen, D.H.; Corcoran, D.S.; Phillips, C.E.; Sannes, T.L. Interrater reliability of hand-held dynamometry: Effects of rater gender, body weight, and grip strength. J. Orthop. Sports Phys. Ther. 1992, 16, 74–81. [Google Scholar] [CrossRef] [PubMed]
- Wikholm, J.B.; Bohannon, R.W. Hand-held dynamometer measurements: Tester strength makes a difference. J. Orthop. Sports Phys. Ther. 1991, 13, 191–198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krause, D.A.; Neuger, M.D.; Lambert, K.A.; Johnson, A.E.; DeVinny, H.A.; Hollman, J.H. Effects of examiner strength on reliability of hip-strength testing using a handheld dynamometer. J. Sport Rehabil. 2014, 23, 56–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thorborg, K.; Bandholm, T.; Schick, M.; Jensen, J.; Hölmich, P. Hip strength assessment using handheld dynamometry is subject to intertester bias when testers are of different sex and strength. Scand. J. Med. Sci. Sports 2013, 23, 487–493. [Google Scholar] [CrossRef]
- Baschung Pfister, P.; de Bruin, E.D.; Sterkele, I.; Maurer, B.; de Bie, R.A.; Knols, R.H. Manual muscle testing and hand-held dynamometry in people with inflammatory myopathy: An intra- and interrater reliability and validity study. PLoS ONE 2018, 13, e0194531. [Google Scholar] [CrossRef]
- Bandinelli, S.; Benvenuti, E.; Del Lungo, I.; Baccini, M.; Benvenuti, F.; Di Iorio, A.; Ferrucci, L. Measuring muscular strength of the lower limbs by hand-held dynamometer: A standard protocol. Aging Clin. Exp. Res. 1999, 11, 287–293. [Google Scholar] [CrossRef]
- Poulsen, E.; Christensen, H.W.; Penny, J.Ø.; Overgaard, S.; Vach, W.; Hartvigsen, J. Reproducibility of range of motion and muscle strength measurements in patients with hip osteoarthritis–an inter-rater study. BMC Musculoskelet. Disord. 2012, 13, 242. [Google Scholar] [CrossRef] [Green Version]
- Malliaras, P.; Hogan, A.; Nawrocki, A.; Crossley, K.; Schache, A. Hip flexibility and strength measures: Reliability and association with athletic groin pain. Br. J. Sports Med. 2009, 43, 739–744. [Google Scholar] [CrossRef]
- Andrews, A.W.; Thomas, M.W.; Bohannon, R.W. Normative values for isometric muscle force measurements obtained with hand-held dynamometers. Phys Ther. 1996, 76, 248–259. [Google Scholar] [CrossRef] [Green Version]
- Ishøi, L.; Hölmich, P.; Thorborg, K. Measures of hip muscle strength and rate of force development using a fixated handheld dynamometer: Intra-tester intra-day reliability of a clinical set up. Int. J. Sports Phys. Ther. 2019, 14, 715–723. [Google Scholar] [CrossRef]
- Stoll, T.; Huber, E.; Seifert, B.; Michel, B.A.; Stucki, G. Maximal isometric muscle strength: Normative values and gender-specific relation to age. Clin. Rheumatol. 2000, 19, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Jönsson, B.; Strömqvist, B. Motor Affliction of the L5 Nerve Root in Lumbar Nerve Root Compression Syndromes. Spine 1995, 20, 2012–2015. [Google Scholar] [CrossRef] [PubMed]
- Hara, Y.; Matsudaira, K.; Hara, N.; Oka, H. A comparison of muscle strength testing for great toe extension. J. Orthop. Sci. 2011, 16, 765–767. [Google Scholar] [CrossRef] [PubMed]
- Riandini, T.; Wee, H.L.; Khoo, E.Y.H.; Tai, B.C.; Wang, W.; Koh, G.C.H.; Tai, E.S.; Tavintharan, S.; Chandran, K.; Hwang, S.W.; et al. Functional status mediates the association between peripheral neuropathy and health-related quality of life in individuals with diabetes. Acta Diabetol. 2018, 55, 155–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lanshammar, K.; Ribom, E.L. Differences in muscle strength in dominant and non-dominant leg in females aged 20–39 years—A population-based study. Phys. Ther. Sport 2011, 12, 76–79. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| n | 52 |
| Gender (male/female) | 25/27 |
| Age (years ± SD) | 63.2 ± 12.1 |
| BMI (kg/m2 ± SD) | 30.6 ± 6.3 |
| Painful side (right/left/both) | 12/15/25 |
| Treatment days (±SD) | 9.19 ± 0.56 |
| Muscle Group | M1 in kg | M2 in kg | p-Values |
|---|---|---|---|
| HF | 23.17 ± 8.61 | 24.84 ± 9.70 | p = 0.013 |
| KE | 26.92 +/− 10.26 | 30.30 ± 12.09 | p ≤ 0.001 |
| KF | 20.26 ± 7.03 | 21.75 ± 7.31 | p ≤ 0.001 |
| ADE | 29.75 ± 9.76 | 30.90 ± 10.29 | p = 0.041 |
| APF | 34.02 ± 7.13 | 37.24 ± 7.3 | p ≤ 0.001 |
| GTE | 7.71 ± 2.64 | 7.40 ± 2.31 | p = 0.103 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaiser, M.; Brambrink, S.; Benditz, A.; Achenbach, L.; Gehentges, M.; König, M.A. Increase in Lower Limb Strength after Multimodal Pain Management in Patients with Low Back Pain. Medicina 2022, 58, 837. https://doi.org/10.3390/medicina58070837
Kaiser M, Brambrink S, Benditz A, Achenbach L, Gehentges M, König MA. Increase in Lower Limb Strength after Multimodal Pain Management in Patients with Low Back Pain. Medicina. 2022; 58(7):837. https://doi.org/10.3390/medicina58070837
Chicago/Turabian StyleKaiser, Moritz, Sara Brambrink, Achim Benditz, Leonard Achenbach, Matthias Gehentges, and Matthias Alexander König. 2022. "Increase in Lower Limb Strength after Multimodal Pain Management in Patients with Low Back Pain" Medicina 58, no. 7: 837. https://doi.org/10.3390/medicina58070837