
Sequential Use of CO2 Laser Prior to Nd:YAG and Dye Laser in the Management of Non-Facial Warts: A Retrospective Study

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Al Aboud, A.M.; Nigam, P.K. Wart; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Vlahovic, T.C.; Khan, M.T. The Human Papillomavirus and Its Role in Plantar Warts: A Comprehensive Review of Diagnosis and Management. Clin. Podiatr. Med. Surg. 2016, 33, 337–353. [Google Scholar] [CrossRef]
- Loo, S.K.; Tang, W.Y. Warts (non-genital). BMJ Clin. Evid. 2014, 2014, 1710. [Google Scholar] [PubMed]
- Iranmanesh, B.; Khalili, M.; Zartab, H.; Amiri, R.; Aflatoonian, M. Laser therapy in cutaneous and genital warts: A review article. Dermatol. Ther. 2021, 34, e14671. [Google Scholar] [CrossRef]
- García-Oreja, S.; Álvaro-Afonso, F.J.; García-Álvarez, Y.; García-Morales, E.; Sanz-Corbalán, I.; Lázaro Martínez, J.L. Topical treatment for plantar warts: A systematic review. Dermatol. Ther. 2021, 34, e14621. [Google Scholar] [CrossRef] [PubMed]
- Soenjoyo, K.R.; Chua, B.W.B.; Wee, L.W.Y.; Koh, M.J.A.; Ang, S.B. Treatment of cutaneous viral warts in children: A review. Dermatol. Ther. 2020, 33, e14034. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, J.; Korta, D.Z.; Chapman, L.W.; Kelly, K.M. Laser Treatment of Nongenital Verrucae: A Systematic Review. JAMA Dermatol. 2016, 152, 1025–1034. [Google Scholar] [CrossRef]
- Bennardo, L.; Del Duca, E.; Dattola, A.; Cannarozzo, G.; Nistico, S.P. Management of laser treatments during the coronavirus disease 2019 pandemic: The Italian experience. Clin. Dermatol. 2021, 39, 521–522. [Google Scholar] [CrossRef] [PubMed]
- Fazia, G.; Cannarozzo, G.; Bennardo, L.; Nisticò, S.P. CO2 laser in the management of eccrine hidrocystomas: A retrospective study. Lasers Med. Sci. 2021, 1–5. [Google Scholar] [CrossRef]
- Cannarozzo, G.; Bennardo, L.; Negosanti, F.; Nisticò, S.P. CO2 Laser Treatment in Idiopathic Scrotal Calcinosis: A Case Series. J. Lasers Med. Sci. 2020, 11, 500–501. [Google Scholar] [CrossRef] [PubMed]
- Dmovsek-Olup, B.; Vedlin, B. Use of Er:YAG laser for benign skin disorders. Lasers Surg. Med. 1997, 21, 13–19. [Google Scholar] [CrossRef]
- Kwok, C.S.; Gibbs, S.; Bennett, C.; Holland, R.; Abbott, R. Topical treatments for cutaneous warts. Cochrane Database Syst. Rev. 2012, 2012, CD001781. [Google Scholar] [CrossRef]
- Hruza, G.J. Laser treatment of warts and other epidermal and dermal lesions. Dermatol. Clin. 1997, 15, 487–506. [Google Scholar] [CrossRef]
- Mercuri, S.R.; Brianti, P.; Dattola, A.; Bennardo, L.; Silvestri, M.; Schipani, G.; Nisticò, S.P. CO2 laser and photodynamic therapy: Study of efficacy in periocular BCC. Dermatol. Ther. 2018, 31, e12616. [Google Scholar] [CrossRef]
- Takac, S. CO2 laser i Verruca vulgaris [The CO2 laser and Verruca vulgaris]. Med. Pregl. 2000, 53, 389–393. [Google Scholar]
- Serour, F.; Somekh, E. Successful treatment of recalcitrant warts in pediatric patients with carbon dioxide laser. Eur. J. Pediatr. Surg. 2003, 13, 219–223. [Google Scholar] [CrossRef]
- Boroujeni, N.H.; Handjani, F.; Saki, N. CO2 laser treatment for plantar warts in children: A case series. Dermatol. Ther. 2020, 33, e13414. [Google Scholar] [CrossRef] [PubMed]
- Bennardo, L.; Bennardo, F.; Giudice, A.; Passante, M.; Dastoli, S.; Morrone, P.; Provenzano, E.; Patruno, C.; Nisticò, S.P. Local Chemotherapy as an Adjuvant Treatment in Unresectable Squamous Cell Carcinoma: What Do We Know So Far? Curr. Oncol. 2021, 28, 213. [Google Scholar] [CrossRef] [PubMed]
- Pentangelo, G.; Nisticò, S.P.; Provenzano, E.; Cisale, G.Y.; Bennardo, L. Topical 5% Imiquimod Sequential to Surgery for HPV-Related Squamous Cell Carcinoma of the Lip. Medicina (Kaunas) 2021, 57, 563. [Google Scholar] [CrossRef]
- Ramsay, H.M.; Fryer, A.A.; Reece, S.; Smith, A.G.; Harden, P.N. Clinical risk factors associated with nonmelanoma skin cancer in renal transplant recipients. Am. J. Kidney Dis. 2000, 36, 167–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Läuchli, S.; Kempf, W.; Dragieva, G.; Burg, G.; Hafner, J. CO2 laser treatment of warts in immunosuppressed patients. Dermatology 2003, 206, 148–152. [Google Scholar] [CrossRef]
- Nistico, S.P.; Silvestri, M.; Zingoni, T.; Tamburi, F.; Bennardo, L.; Cannarozzo, G. Combination of Fractional CO2 Laser and Rhodamine-Intense Pulsed Light in Facial Rejuvenation: A Randomized Controlled Trial. Photobiomodul. Photomed. Laser Surg. 2021, 39, 113–117. [Google Scholar] [CrossRef] [PubMed]
- Lodi, G.; Sannino, M.; Caterino, P.; Cannarozzo, G.; Bennardo, L.; Nisticò, S.P. Fractional CO2 laser-assisted topical rifamycin drug delivery in the treatment of pediatric cutaneous leishmaniasis. Pediatr. Dermatol. 2021, 38, 717–720. [Google Scholar] [CrossRef] [PubMed]
- Forbat, E.; Al-Niaimi, F. Nonvascular uses of pulsed dye laser in clinical dermatology. J. Cosmet. Dermatol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Kenton-Smith, J.; Tan, S.T. Pulsed dye laser therapy for viral warts. Br. J. Plast. Surg. 1999, 52, 554–558. [Google Scholar] [CrossRef]
- Robson, K.J.; Cunningham, N.M.; Kruzan, K.L.; Patel, D.S.; Kreiter, C.D.; O’Donnell, M.J.; Arpey, C.J. Pulsed-dye laser versus conventional therapy in the treatment of warts: A prospective randomized trial. J. Am. Acad. Dermatol. 2000, 43 Pt 1, 275–280. [Google Scholar] [CrossRef]
- Akhyani, M.; Ehsani, A.H.; Noormohammadpour, P.; Shamsodini, R.; Azizahari, S.; Sayanjali, S. Comparing Pulsed-dye Laser with Cryotherapy in the Treatment of Common Warts. J. Lasers Med. Sci. 2011, 1, 14–19. Available online: https://journals.sbmu.ac.ir/jlms/article/view/2132 (accessed on 15 November 2021).
- Snast, I.; Kaftory, R.; Lapidoth, M.; Mazor, S.; Hodak, E.; Mimouni, D.; Davidovici, B.; Levi, A. Combined pulsed dye laser and systemic retinoids for the treatment of hypertrophic resistant warts among organ transplant patients. Lasers Med. Sci. 2020, 35, 1653–1657. [Google Scholar] [CrossRef] [PubMed]
- Elmaadawy, E.H.; Shams, S.S.; Hegab, D.S.; Zaki, R.A. Pulsed-dye laser versus intralesional Candida albicans antigen injection in treatment of genital warts. Acta Dermatovenerol. Alp. Pannonica Adriat. 2019, 28, 21–26. [Google Scholar] [PubMed]
- Focht, D.R., 3rd; Spicer, C.; Fairchok, M.P. The efficacy of duct tape vs. cryotherapy in the treatment of Verruca vulgaris (the common wart). Arch. Pediatrics Adolesc. Med. 2002, 156, 971–974. [Google Scholar] [CrossRef] [Green Version]
- Gibbs, S.; Harvey, I. Topical treatments for cutaneous warts. Cochrane Database Syst. Rev. 2006, CD001781. [Google Scholar] [CrossRef]
- Lipke, M.M. An armamentarium of wart treatments. Clin. Med. Res. 2006, 4, 273–293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baleg, S.M.; Bidin, N.; Suan, L.P.; Ahmad, M.F.; Krishnan, G.; Johari, A.R.; Hamid, A. The effect of CO2 laser treatment on skin tissue. J Cosmet Dermatol. 2015, 14, 246–253. [Google Scholar] [CrossRef] [PubMed]
- Sethuraman, G.; Richards, K.A.; Hiremagalore, R.N.; Wagner, A. Effectiveness of pulsed dye laser in the treatment of recalcitrant warts in children. Dermatol. Surg. 2010, 36, 58–65. [Google Scholar] [CrossRef]
- Huilgol, S.C.; Barlow, R.J.; Markey, A.C. Failure of pulsed dye laser therapy for resistant verrucae. Clin. Exp. Dermatol. 1996, 21, 93–95. [Google Scholar] [CrossRef] [PubMed]
- Del Duca, E.; Zingoni, T.; Bennardo, L.; di Raimondo, C.; Garofalo, V.; Sannino, M.; Petrini, N.; Cannarozzo, G.; Bianchi, L.; Nisticò, S.P. Long-Term Follow-Up for Q-Switched Nd:YAG Treatment of Nevus of Ota: Are High Number of Treatments Really Required? A Case Report. Photobiomodul. Photomed. Laser Surg. 2021, 39, 137–140. [Google Scholar] [CrossRef] [PubMed]
- Silvestri, M.; Bennardo, L.; Zappia, E.; Tamburi, F.; Cameli, N.; Cannarozzo, G.; Nisticò, S.P. Q-Switched 1064/532 nm Laser with Picosecond Pulse to Treat Benign Hyperpigmentations: A Single-Center Retrospective Study. Appl. Sci. 2021, 11, 7478. [Google Scholar] [CrossRef]
- Bennardo, L.; Cannarozzo, G.; Tamburi, F.; Patruno, C.; Provenzano, E.; Nisticò, S.P. Picosecond Q-Switched 1064/532 nm Laser in Tattoo Removal: Our Single Center Experience. Appl. Sci. 2021, 11, 9712. [Google Scholar] [CrossRef]
- Cannarozzo, G.; Nisticò, S.P.; Zappia, E.; del Duca, E.; Provenzano, E.; Patruno, C.; Negosanti, F.; Sannino, M.; Bennardo, L. Q-Switched 1064/532 nm Laser with Nanosecond Pulse in Tattoo Treatment: A Double-Center Retrospective Study. Life 2021, 11, 699. [Google Scholar] [CrossRef]
- Cannarozzo, G.; Negosanti, F.; Sannino, M.; Santoli, M.; Bennardo, L.; Banzola, N.; Negosanti, L.; Nisticò, S.P. Q-switched Nd:YAG laser for cosmetic tattoo removal. Dermatol. Ther. 2019, 32, e13042. [Google Scholar] [CrossRef]
- Bingol, U.A.; Cömert, A.; Cinar, C. The Overlapped Triple Circle Pulse Technique with Nd:YAG Laser for Refractory Hand Warts. Photomed. Laser Surg. 2015, 33, 338–342. [Google Scholar] [CrossRef]
- Kopera, D. Verrucae vulgares: Flashlamp-pumped pulsed dye laser treatment in 134 patients. Int. J. Dermatol. 2003, 42, 905–908. [Google Scholar] [CrossRef] [PubMed]
- Weiss, R.A.; Weiss, M.A. Early clinical results with a multiple synchronized pulse 1064 NM laser for leg telangiectasias and reticular veins. Dermatol. Surg. 1999, 25, 399–402. [Google Scholar] [CrossRef]
- Yeh, Y.T.; Peng, J.H.; Peng, P. Histology of ex vivo skin after treatment with fractionated picosecond Nd:YAG laser in high and low-energy settings. J. Cosmet. Laser Ther. 2020, 22, 43–47. [Google Scholar] [CrossRef]
- El-Tonsy, M.H.; Anbar, T.E.; El-Domyati, M.; Barakat, M. Density of viral particles in pre and post Nd: YAG laser hyperthermia therapy and cryotherapy in plantar warts. Int. J. Dermatol. 1999, 38, 393–398. [Google Scholar] [CrossRef] [PubMed]
- Han, T.Y.; Lee, J.H.; Lee, C.K.; Ahn, J.Y.; Seo, S.J.; Hong, C.K. Long-pulsed Nd:YAG laser treatment of warts: Report on a series of 369 cases. J. Korean Med. Sci. 2009, 24, 889–893. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El-Mohamady, A.e.l.-S.; Mearag, I.; El-Khalawany, M.; Elshahed, A.; Shokeir, H.; Mahmoud, A. Pulsed dye laser versus Nd:YAG laser in the treatment of plantar warts: A comparative study. Lasers Med. Sci. 2014, 29, 1111–1116. [Google Scholar] [CrossRef]
- Zorman, A.; Koron, N. Wart removal without anesthesia using long-pulse 1064-nm Nd:YAG laser. J. Cosmet. Dermatol. 2021, 20, 506–512. [Google Scholar] [CrossRef]
- Khattab, F.M.; Khashaba, S.A. Evaluation of combined treatment with long-pulsed neodymium-doped yttrium aluminum garnet laser and potassium hydroxide for the treatment of recalcitrant wart: A prospective comparative study. J. Dermatol. Treat. 2020, 31, 56–60. [Google Scholar] [CrossRef]
- Mixter, R.C.; Carson, L.V.; Walton, B.J.; Gerson, R.W. Optic nerve decompression in fibrous dysplasia: Indications, efficacy, and safety. Plast. Reconstr. Surg. 1997, 100, 1612–1613. [Google Scholar] [CrossRef]
- Geronemus, R.G.; Kauvar, A.N.; McDaniel, D.H. Treatment of recalcitrant verrucae with both the ultrapulse CO2 and PLDL pulsed dye lasers. Plast. Reconstr. Surg. 1998, 101, 2010. [Google Scholar] [CrossRef]
- Kong, S.H.; Suh, H.S.; Choi, Y.S. Treatment of Melasma with Pulsed-Dye Laser and 1,064-nm Q-Switched Nd:YAG Laser: A Split-Face Study. Ann. Dermatol. 2018, 30, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonan, P.; Bassi, A.; Bruscino, N.; Schincaglia, E.; Gavrilova, M.; Troiano, M.; Verdelli, A. Combined pulsed dye laser and Q-switched Nd:YAG laser intraumatic facial tattoo removal: A case series. Dermatol. Ther. 2019, 32, e13069. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.; Guo, P.; Wang, X.; Huo, R.; Li, Q.; Yin, S.; Cao, Y. Effective treatment for hypertrophic scar with dual-wave-length PDL and Nd:YAG in Chinese patients. J. Cosmet. Laser Ther. 2019, 21, 228–233. [Google Scholar] [CrossRef]
- Alcántara-González, J.; Boixeda, P.; Truchuelo-Díez, M.T.; Jiménez-Gómez, N.; Pérez-García, B.; Pérez-Carmona, L.; Olasolo, P.J. Capillary Malformations Treated With Sequential Pulsed Dye and Nd:YAG Laser Therapy: A Retrospective Study. Malformaciones capilares tratadas con aplicación secuencial de láser de colorante pulsado y Nd:YAG: Estudio retrospectivo. Actas Dermo-Sifiliográficas (Engl. Ed.) 2018, 109, 155–161. [Google Scholar] [CrossRef]
- Hartmann, F.; Lockmann, A.; Himpel, O.; Kühnle, I.; Hensen, J.; Schön, M.P.; Thoms, K. Combination therapy of oral propranolol and combined Nd:YAG/pulsed dye laser therapy in infantile hemangiomas: A retrospective analysis of 48 treated hemangiomas in 30 children. J. Dtsch. Dermatol. Ges. 2020, 18, 984–993. [Google Scholar] [CrossRef]
- Wang, T.; Chen, D.; Yang, J.; Ma, G.; Yu, W.; Lin, X. Safety and efficacy of dual-wavelength laser (1064 + 595 nm) for treatment of non-treated port-wine stains. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 260–264. [Google Scholar] [CrossRef]
- Negosanti, F.; Silvestri, M.; Bennardo, L.; Durastante, C.; del Duca, E.; Cannarozzo, G.; Nisticò, S.P. Nd:YAG laser in association with pulsed dye laser for the treatment of PHACES syndrome. Derm. Rep. 2021, 13, 8751. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Y.; Li, X.Q.; Lin, Q.Z.; Zhan, K. Treatment of angiokeratoma of Mibelli alone or in combination with pulsed dye laser and long-pulsed Nd: YAG laser. Dermatol. Ther. 2014, 27, 348–351. [Google Scholar] [CrossRef]
- Park, J.S.; Kim, H.S.; Choi, C.P. Utilizing Combined Pulsed Dye and Nd: YAG Lasers in the Treatment of Connective Tissue Disease Cutaneous Symptoms. J. Clin. Rheumatol. 2019, 27, S451–S452. [Google Scholar] [CrossRef] [PubMed]
- Nisticò, S.P.; Bennardo, L.; Sannino, M.; Negosanti, F.; Tamburi, F.; del Duca, E.; Giudice, A.; Cannarozzo, G. Combined CO2 and dye laser technique in the treatment of outcomes due to flap necrosis after surgery for basal cell carcinoma on the nose. Lasers Surg. Med. 2021. [Google Scholar] [CrossRef] [PubMed]
- Piccolo, D.; Crisman, G.; Bovani, B.; Gennai, A.; Melfa, F.; Clementoni, M.T.; Conforti, C. Combined laser treatment for ear keloids: Case series: Comparison between two mini-invasive protocols. J. Cosmet. Dermatol. 2021, 21, 296–306. [Google Scholar] [CrossRef] [PubMed]
- Sannino, M.; Ambrosio, A.G.; Lodi, G.; Cannarozzo, G.; Bennardo, L.; Nisticò, S.P. A giant epidermal nevus of the face treated with a CO2 and dye laser combination: A case report and literature review. J. Cosmet. Laser Ther. 2021, 23, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Shin, Y.S.; Cho, E.B.; Park, E.J.; Kim, K.H.; Kim, K.J. A comparative study of pulsed dye laser versus long pulsed Nd:YAG laser treatment in recalcitrant viral warts. J. Dermatol. Treat. 2017, 28, 411–416. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Number | Sex | Age | Number of Warts | Location | Resolution | Relapse | Side Effects | VAS Score | Anesthesia |
|---|---|---|---|---|---|---|---|---|---|
| 1 | M | 71 | 1 | PP | T | 10 | Yes | ||
| 2 | M | 9 | 4 | O | T | 10 | No | ||
| 3 | F | 29 | 3 | O | T | 10 | Yes | ||
| 4 | F | 38 | 5 | PP | T | H | 8 | Yes | |
| 5 | M | 68 | 4 | O | T | 10 | Yes | ||
| 6 | F | 12 | 1 | PP | T | 10 | Yes | ||
| 7 | M | 28 | 4 | O | T | 9 | No | ||
| 8 | F | 67 | 3 | O | T | H | 7 | Yes | |
| 9 | M | 23 | 2 | O | T | 9 | Yes | ||
| 10 | F | 65 | 1 | PP | P | 7 | Yes | ||
| 11 | F | 14 | 4 | O | T | R | 8 | No | |
| 12 | M | 45 | 3 | PP | T | 10 | Yes | ||
| 13 | F | 34 | 7 | O | T | 10 | Yes | ||
| 14 | F | 22 | 3 | PP | T | 10 | Yes | ||
| 15 | F | 74 | 3 | O | T | 10 | Yes | ||
| 16 | M | 67 | 1 | PP | T | H | 9 | Yes | |
| 17 | F | 68 | 1 | PP | P | 10 | Yes | ||
| 18 | M | 25 | 5 | O | T | 10 | No | ||
| 19 | M | 54 | 1 | PP | T | 10 | Yes | ||
| 20 | F | 52 | 2 | O | T | 10 | No | ||
| 21 | M | 78 | 1 | PP | T | R | 7 | Yes | |
| 22 | F | 15 | 6 | O | T | 9 | Yes | ||
| 23 | M | 19 | 3 | PP | T | R | 9 | Yes | |
| 24 | F | 64 | 5 | O | T | 10 | No | ||
| 25 | F | 43 | 1 | PP | T | H | 10 | Yes | |
| 26 | M | 37 | 4 | O | T | 8 | Yes | ||
| 27 | F | 34 | 1 | PP | T | 9 | Yes | ||
| 28 | M | 25 | 3 | O | T | H | 10 | Yes | |
| 29 | F | 27 | 4 | O | T | 9 | No | ||
| 30 | F | 58 | 1 | PP | T | 9 | Yes | ||
| 31 | M | 67 | 4 | O | T | 10 | Yes | ||
| 32 | M | 65 | 3 | O | T | 9 | No | ||
| 33 | M | 64 | 4 | PP | T | 10 | Yes | ||
| 34 | F | 43 | 5 | PP | T | 10 | Yes |
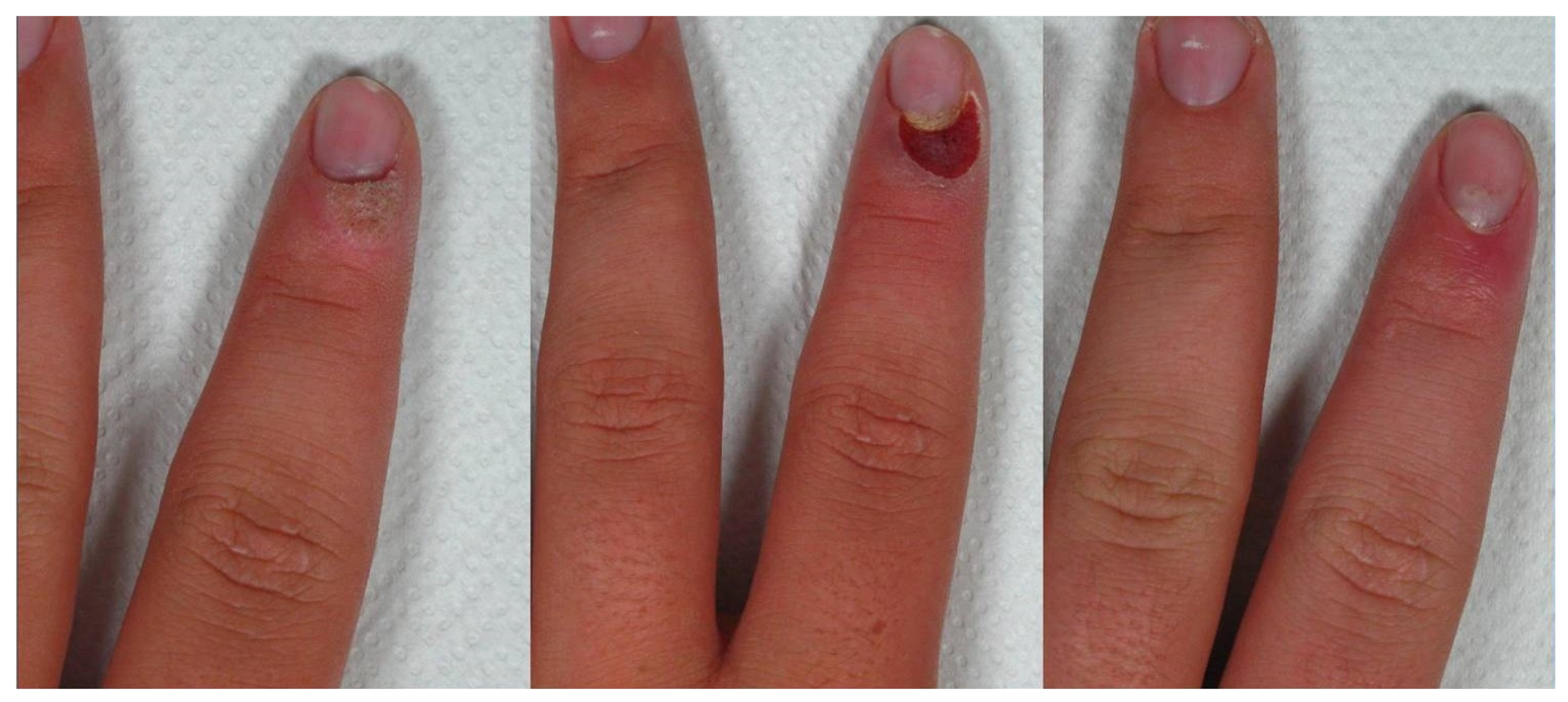
| First session of CO2 laser in super-pulsed mode, with a focused beam of 0.1–0.2 mm diameter, power 0.3–0.8 W, fre-quency 10 Hz, with the intent to remove the superficial layer of the epidermis, exposing the superficial dermis but without causing bleeding. |
| Right after CO2 laser, a second session with long-pulsed Nd:YAG laser for lesions interesting the palmoplantar region (90–120 J/cm2, 5 mm spot size, slightly defocused, double pulse 5–15 ms with a 10 ms interval performing multiple passes), and with a 595 nm Dye laser for all other regions (10 mm size spot, fluence 9–10 J/cm2, and frequency 0.5/s, per-forming multiple passes) was performed on the treated spot, in order to reduce the vascularization to the treated area. |
| After the combined treatment, topical fusidic acid was applied to the lesion twice a day for one week. |
| From the second week, a 20% salicylic acid cream in the evening and 40% urea in the morning were applied for the other three weeks up to clinical follow-up. |
| A first clinical follow-up at one month evaluated lesion disappearance. |
| A second clinical follow up at four months evaluated relapses. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bennardo, L.; Fasano, G.; Tamburi, F.; Zappia, E.; Rizzuto, F.; Nisticò, S.P.; Cannarozzo, G. Sequential Use of CO2 Laser Prior to Nd:YAG and Dye Laser in the Management of Non-Facial Warts: A Retrospective Study. Medicina 2022, 58, 115. https://doi.org/10.3390/medicina58010115
Bennardo L, Fasano G, Tamburi F, Zappia E, Rizzuto F, Nisticò SP, Cannarozzo G. Sequential Use of CO2 Laser Prior to Nd:YAG and Dye Laser in the Management of Non-Facial Warts: A Retrospective Study. Medicina. 2022; 58(1):115. https://doi.org/10.3390/medicina58010115
Chicago/Turabian StyleBennardo, Luigi, Gaia Fasano, Federica Tamburi, Elena Zappia, Francesco Rizzuto, Steven Paul Nisticò, and Giovanni Cannarozzo. 2022. "Sequential Use of CO2 Laser Prior to Nd:YAG and Dye Laser in the Management of Non-Facial Warts: A Retrospective Study" Medicina 58, no. 1: 115. https://doi.org/10.3390/medicina58010115