
Correlation between the Perfusion Index and Intraoperative Hypothermia: A Prospective Observational Pilot Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
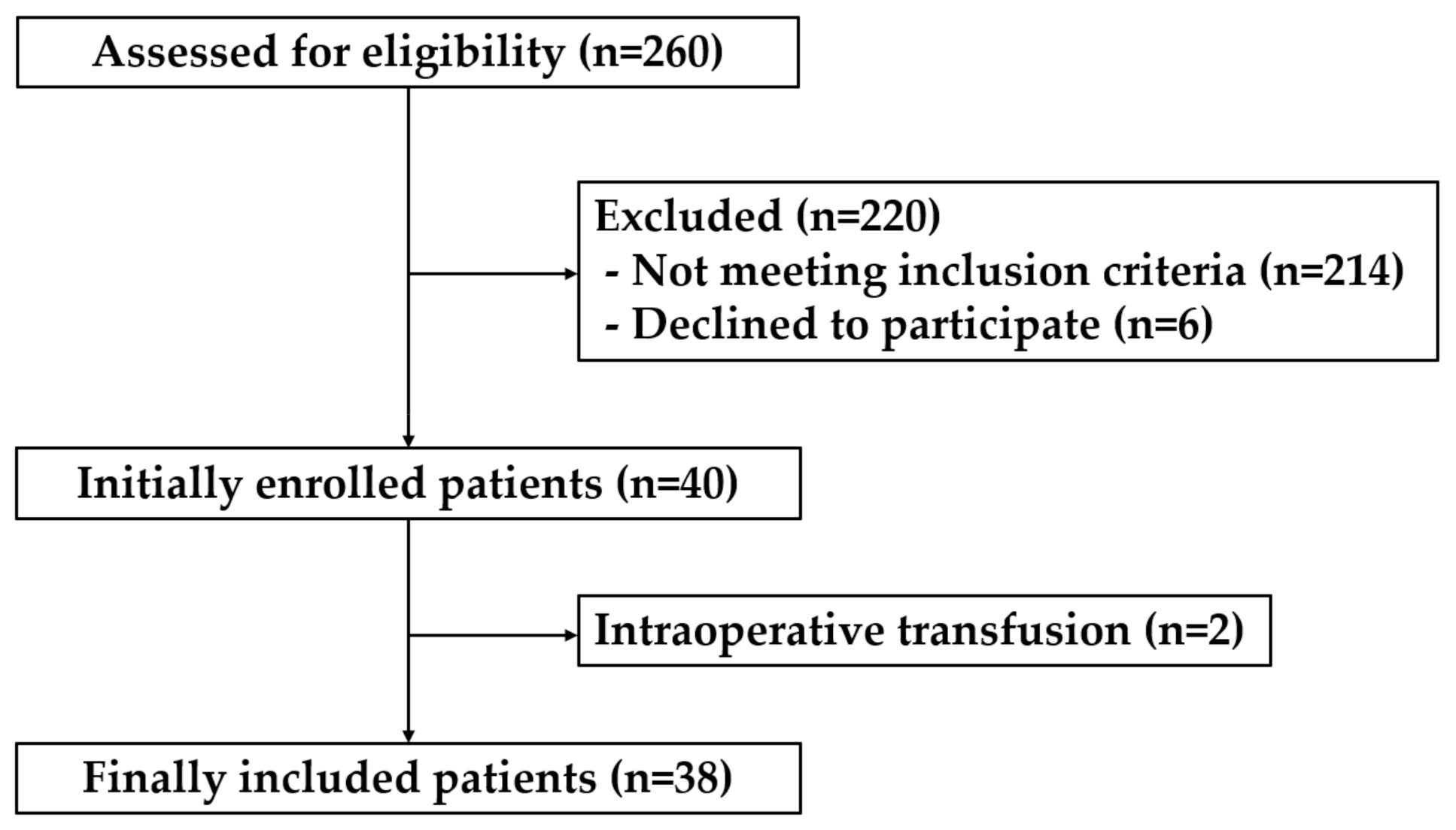
2.1. Patients
2.2. Intervention
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Frank, S.M.; Fleisher, L.A.; Breslow, M.J.; Higgins, M.S.; Olson, K.F.; Kelly, S.; Beattie, C. Perioperative maintenance of normothermia reduces the incidence of morbid cardiac events. A randomized clinical trial. JAMA 1997, 277, 1127–1134. [Google Scholar] [CrossRef] [PubMed]
- Kurz, A.; Sessler, D.I.; Lenhardt, R. Perioperative normothermia to reduce the incidence of surgical-wound infection and shorten hospitalization. Study of Wound Infection and Temperature Group. N. Engl. J. Med. 1996, 334, 1209–1215. [Google Scholar] [CrossRef] [PubMed]
- Sun, Z.; Honar, H.; Sessler, D.I.; Dalton, J.E.; Yang, D.; Panjasawatwong, K.; Deroee, A.F.; Salmasi, V.; Saager, L.; Kurz, A. Intraoperative core temperature patterns, transfusion requirement, and hospital duration in patients warmed with forced air. Anesthesiology 2015, 122, 276–285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weirich, T.L. Hypothermia/warming protocols: Why are they not widely used in the OR? AORN J. 2008, 87, 333–344. [Google Scholar] [CrossRef]
- Sessler, D.I. Perioperative heat balance. Anesthesiology 2000, 92, 578–596. [Google Scholar] [CrossRef]
- Huang, B.; Sun, K.; Zhu, Z.; Zhou, C.; Wu, Y.; Zhang, F.; Yan, M. Oximetry-derived perfusion index as an early indicator of CT-guided thoracic sympathetic blockade in palmar hyperhidrosis. Clin. Radiol. 2013, 68, 1227–1232. [Google Scholar] [CrossRef]
- Ginosar, Y.; Weiniger, C.F.; Meroz, Y.; Kurz, V.; Bdolah-Abram, T.; Babchenko, A.; Nitzan, M.; Davidson, E.M. Pulse oximeter perfusion index as an early indicator of sympathectomy after epidural anesthesia. Acta Anaesthesiol. Scand. 2009, 53, 1018–1026. [Google Scholar] [CrossRef]
- Mehandale, S.G.; Rajasekhar, P. Perfusion index as a predictor of hypotension following propofol induction—A prospective observational study. Indian J. Anaesth. 2017, 61, 990–995. [Google Scholar] [CrossRef]
- Lee, J.Y.; Kim, E.D.; Kim, Y.N.; Kim, J.S.; Sim, W.S.; Lee, H.J.; Park, H.J.; Park, H.J. Correlation of Perfusion Index Change and Analgesic Efficacy in Transforaminal Block for Lumbosacral Radicular Pain. J. Clin. Med. 2019, 8, 51. [Google Scholar] [CrossRef] [Green Version]
- Abdelnasser, A.; Abdelhamid, B.; Elsonbaty, A.; Hasanin, A.; Rady, A. Predicting successful supraclavicular brachial plexus block using pulse oximeter perfusion index. Br. J. Anaesth. 2017, 119, 276–280. [Google Scholar] [CrossRef] [Green Version]
- Hasanin, A.; Mohamed, S.A.R.; El-Adawy, A. Evaluation of perfusion index as a tool for pain assessment in critically ill patients. J. Clin. Monit. Comput. 2017, 31, 961–965. [Google Scholar] [CrossRef]
- Kupeli, I.; Kulhan, N.G. Can Perfusion Index be used as an Objective Tool for Pain Assessment in Labor Analgesia? Pak. J. Med. Sci. 2018, 34, 1262–1266. [Google Scholar] [CrossRef]
- Kwon, J.H.; Park, H.J.; Sim, W.S.; Park, J.H.; Jung, K.H.; Oh, M.S.; Seon, H.J.; Lee, J.Y. Evaluation of the Intraoperative Perfusion Index for Correlation with Acute Postoperative Pain in Patients Undergoing Laparoscopic Colorectal Cancer Surgery. J. Clin. Med. 2019, 8, 1299. [Google Scholar] [CrossRef] [Green Version]
- van Genderen, M.E.; Bartels, S.A.; Lima, A.; Bezemer, R.; Ince, C.; Bakker, J.; van Bommel, J. Peripheral perfusion index as an early predictor for central hypovolemia in awake healthy volunteers. Anesth. Analg. 2013, 116, 351–356. [Google Scholar] [CrossRef] [Green Version]
- Ryu, K.H.; Hwang, S.H.; Shim, J.G.; Ahn, J.H.; Cho, E.A.; Lee, S.H.; Byun, J.H. Comparison of vasodilatory properties between desflurane and sevoflurane using perfusion index: A randomised controlled trial. Br. J. Anaesth. 2020, 125, 935–942. [Google Scholar] [CrossRef]
- Jeng, E.I.; Gravenstein, N.; Klodell, C.T. Perfusion Index: An Indicator of Success During Endoscopic Thoracic Sympathectomy for Hyperhidrosis. Ann. Thorac. Surg. 2017, 104, 426–430. [Google Scholar] [CrossRef]
- Toyama, S.; Kakumoto, M.; Morioka, M.; Matsuoka, K.; Omatsu, H.; Tagaito, Y.; Numai, T.; Shimoyama, M. Perfusion index derived from a pulse oximeter can predict the incidence of hypotension during spinal anaesthesia for Caesarean delivery. Br. J. Anaesth. 2013, 111, 235–241. [Google Scholar] [CrossRef] [Green Version]
- John, M.; Crook, D.; Dasari, K.; Eljelani, F.; El-Haboby, A.; Harper, C.M. Comparison of resistive heating and forced-air warming to prevent inadvertent perioperative hypothermia. Br. J. Anaesth. 2016, 116, 249–254. [Google Scholar] [CrossRef] [Green Version]
- Horn, E.P.; Bein, B.; Broch, O.; Iden, T.; Böhm, R.; Latz, S.K.; Höcker, J. Warming before and after epidural block before general anaesthesia for major abdominal surgery prevents perioperative hypothermia: A randomised controlled trial. Eur. J. Anaesthesiol. 2016, 33, 334–340. [Google Scholar] [CrossRef]
- Riley, C.; Andrzejowski, J. Inadvertent perioperative hypothermia. BJA Educ. 2018, 18, 227–233. [Google Scholar] [CrossRef] [Green Version]
- Åström, D.O.; Veber, T.; Martinsone, Ž.; Kaļužnaja, D.; Indermitte, E.; Oudin, A.; Orru, H. Mortality Related to Cold Temperatures in Two Capitals of the Baltics: Tallinn and Riga. Medicina 2019, 55, 429. [Google Scholar] [CrossRef] [Green Version]
- Reingardiene, D. [Hypothermia]. Medicina 2003, 39, 90–97. [Google Scholar]
- Kuroki, C.; Godai, K.; Hasegawa-Moriyama, M.; Kuniyoshi, T.; Matsunaga, A.; Kanmura, Y.; Kuwaki, T. Perfusion index as a possible predictor for postanesthetic shivering. J. Anesth. 2014, 28, 19–25. [Google Scholar] [CrossRef]
- Li, Y.; Liang, H.; Feng, Y. Prevalence and multivariable factors associated with inadvertent intraoperative hypothermia in video-assisted thoracoscopic surgery: A single-center retrospective study. BMC Anesthesiol. 2020, 20, 25. [Google Scholar] [CrossRef]
- Kasai, T.; Hirose, M.; Yaegashi, K.; Matsukawa, T.; Takamata, A.; Tanaka, Y. Preoperative risk factors of intraoperative hypothermia in major surgery under general anesthesia. Anesth. Analg. 2002, 95, 1381–1383. [Google Scholar] [CrossRef]
- Miyazaki, R.; Hoka, S. What is the predictor of the intraoperative body temperature in abdominal surgery? J. Anesth. 2019, 33, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Huang, C.Y.; Zhou, Z.B.; Wen, Z.S.; Zhang, G.R.; Liu, K.X.; Huang, W.Q. Risk factors for hypothermia in patients under general anesthesia: Is there a drawback of laminar airflow operating rooms? A prospective cohort study. Int. J. Surg. 2015, 21, 14–17. [Google Scholar] [CrossRef]
- Yi, J.; Zhan, L.; Lei, Y.; Xu, S.; Si, Y.; Li, S.; Xia, Z.; Shi, Y.; Gu, X.; Yu, J.; et al. Establishment and Validation of a Prediction Equation to Estimate Risk of Intraoperative Hypothermia in Patients Receiving General Anesthesia. Sci. Rep. 2017, 7, 13927. [Google Scholar] [CrossRef] [Green Version]
- Macario, A.; Dexter, F. What are the most important risk factors for a patient’s developing intraoperative hypothermia? Anesth. Analg. 2002, 94, 215–220. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| All Patients (n = 38) | Normothermia (n = 20) | Hypothermia (n = 18) | p-Value | |
|---|---|---|---|---|
| Age (years) | 57.8 ± 7.2 | 58.5 ± 5.6 | 57.1 ± 8.7 | 0.556 |
| Sex (n (%)) | 0.914 | |||
| Female | 25 (65.8%) | 13 (65.0%) | 12 (66.7%) | |
| Male | 13 (34.2%) | 7 (35.0%) | 6 (33.3%) | |
| Height (cm) | 160.2 ± 7.9 | 158.7 ± 7.9 | 161.8 ± 7.9 | 0.221 |
| Weight (kg) | 62.7 ± 10.7 | 61.3 ± 11.4 | 64.3 ± 9.9 | 0.399 |
| BMI (kg/m2) | 24.3 ± 2.6 | 24.2 ± 2.8 | 24.5 ± 2.4 | 0.759 |
| ASA (n (%)) | 0.606 | |||
| I | 4 (10.5%) | 3 (15.0%) | 1 (5.6%) | |
| II | 34 (89.5%) | 17 (85.0%) | 17 (94.4%) | |
| Diabetes Mellitus (n (%)) | 8 (21.1%) | 4 (20.0%) | 4 (22.2%) | 1.000 |
| Hypertension (n (%)) | 17 (44.7%) | 7 (35.0%) | 10 (55.6%) | 0.203 |
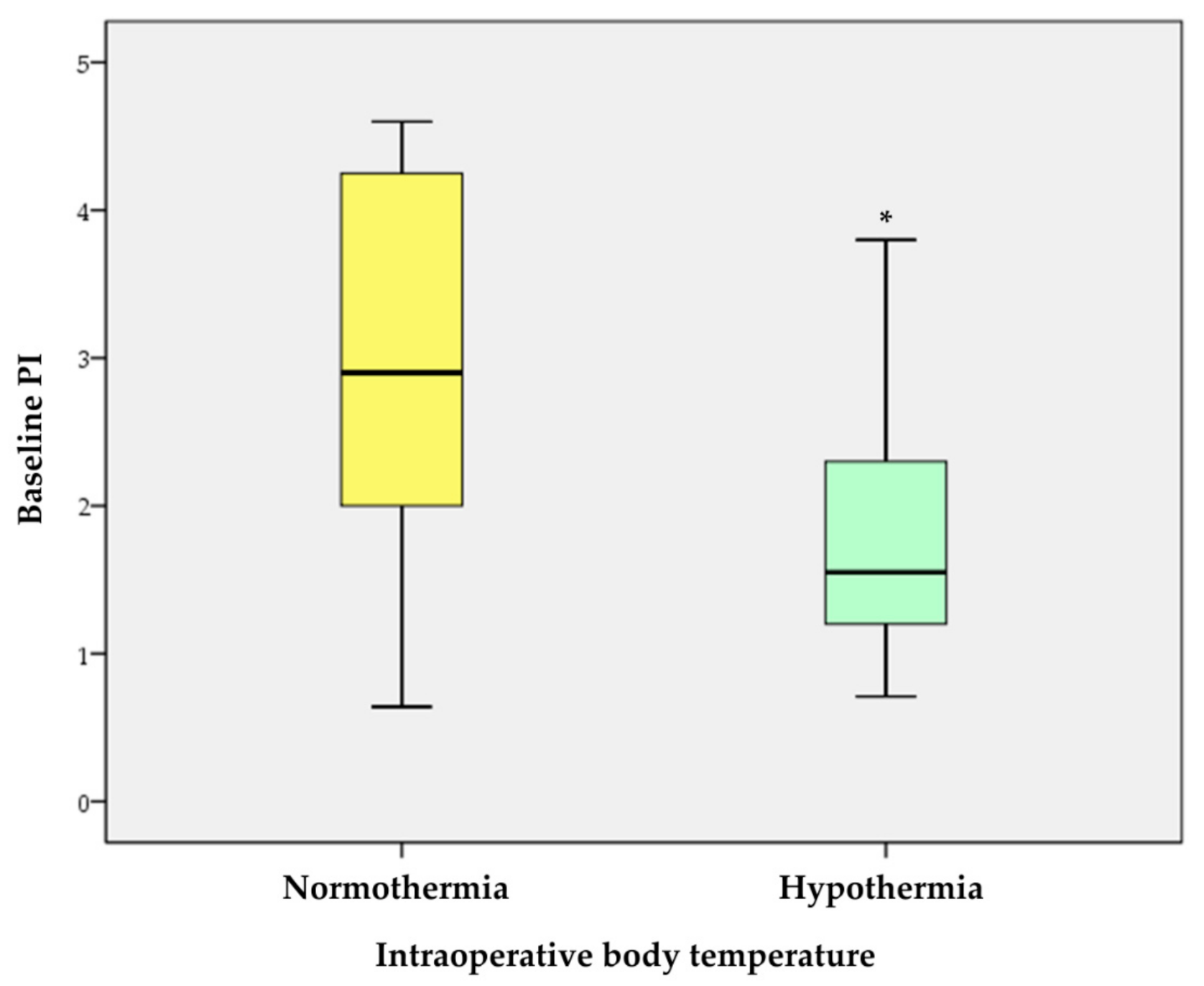
| Baseline PI | 2.4 ± 1.2 | 3.0 ± 1.2 | 1.8 ± 0.7 | <0.001 * |
| Duration of surgery (min) | 192.1 ± 62.0 | 194.0 ± 54.7 | 190 ± 70.8 | 0.846 |
| Duration of anesthesia (min) | 261.8 ± 70.6 | 260.3 ± 63.5 | 263.6 ± 79.6 | 0.886 |
| Type of surgery (n (%)) | 0.370 | |||
| Aneurysm neck clip | 18 (47.4%) | 9 (45.0%) | 9 (50.0%) | |
| Microvascular decompression | 16 (42.1%) | 10 (50.0%) | 6 (33.3%) | |
| Mass removal | 4 (10.5%) | 1 (5.0%) | 3 (16.7%) | |
| Propofol (mg) | 1343.5 ± 366.1 | 1319.0 ± 308.7 | 1370.8 ± 428.5 | 0.669 |
| Remifentanil (mcg) | 2888.4 ± 1075.5 | 3005.9 ± 1052.9 | 2757.8 ± 1115.5 | 0.485 |
| Total fluid (mL) | 1256.6 ± 444.2 | 1257.5 ± 411.4 | 1255.6 ± 490.2 | 0.989 |
| Estimated blood loss (mL) | 305.3 ± 165.9 | 285.0 ± 175.5 | 327.8 ± 156.5 | 0.435 |
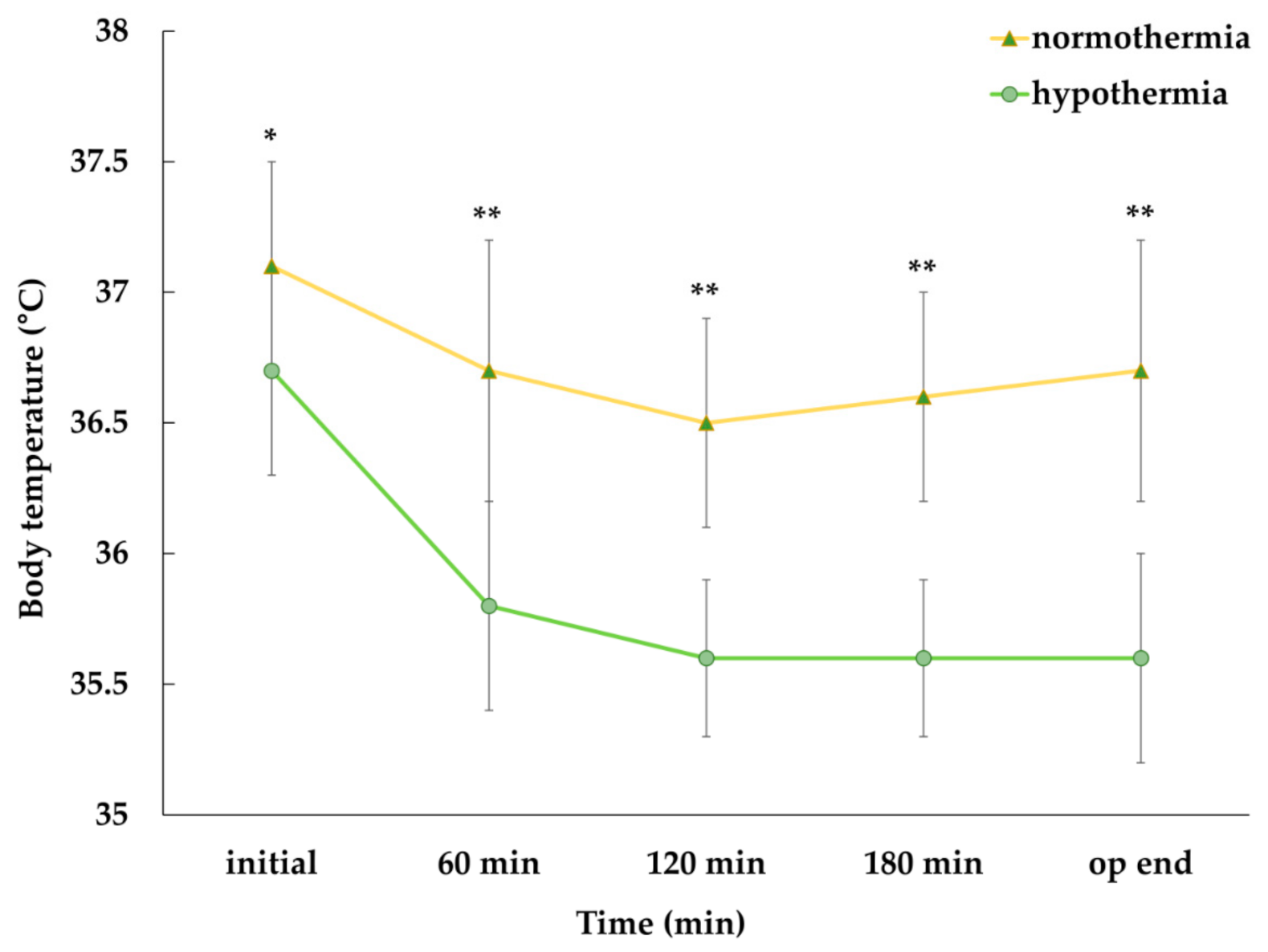
| Baseline temperature (°C) † | 36.9 ± 0.5 | 37.1 ± 0.4 | 36.7 ± 0.4 | 0.010 * |
| OR temperature (°C) | 20.8 ± 0.8 | 21.0 ± 0.8 | 20.6 ± 0.8 | 0.186 |
| β | Wals | Odds Ratio | 95% Confidence Interval | p-Value | ||
|---|---|---|---|---|---|---|
| Age (years) | −0.028 | 0.366 | 0.972 | 0.888 | 1.065 | 0.545 |
| Male | 0.074 | 0.012 | 1.077 | 0.281 | 4.127 | 0.914 |
| BMI (kg/m2) | 0.040 | 0.100 | 1.041 | 0.813 | 1.332 | 0.752 |
| ASA | ||||||
| II † | 1.099 | 0.832 | 3.000 | 0.283 | 31.802 | 0.362 |
| Diabetes Mellitus | −0.134 | 0.028 | 0.875 | 0.184 | 4.166 | 0.867 |
| Hypertension | −0.842 | 1.595 | 0.431 | 0.117 | 1.592 | 0.207 |
| Baseline PI | −1.270 | 7.945 | 0.281 | 0.116 | 0.679 | 0.005 * |
| Duration of anesthesia (min) | 0.001 | 0.022 | 1.001 | 0.992 | 1.010 | 0.882 |
| Type of surgery | ||||||
| Aneurysm neck clip | / | 1.751 | / | / | / | 0.417 |
| Microvascular decompression | −1.099 | 0.776 | 0.333 | 0.029 | 3.842 | 0.378 |
| Mass removal | −1.609 | 1.619 | 0.200 | 0.017 | 2.386 | 0.203 |
| Baseline temperature (°C) †† | −2.140 | 5.507 | 0.118 | 0.020 | 0.703 | 0.019 * |
| OR temperature (°C) | −0.567 | 1.748 | 0.567 | 0.245 | 1.315 | 0.186 |
| β | Wals | Odds Ratio | 95% Confidence Interval | p-Value | ||
|---|---|---|---|---|---|---|
| Baseline PI | −1.398 | 6.881 | 0.247 | 0.087 | 0.702 | 0.009 * |
| Male | 1.839 | 1.749 | 6.288 | 0.412 | 95.949 | 0.186 |
| BMI (kg/m2) | −0.024 | 0.013 | 0.976 | 0.643 | 1.482 | 0.909 |
| Duration of anesthesia (min) | −0.002 | 0.069 | 0.998 | 0.985 | 1.012 | 0.794 |
| OR temperature (°C) | −0.559 | 0.650 | 0.572 | 0.147 | 2.225 | 0.420 |
| Baseline temperature (°C) † | −4.278 | 5.198 | 0.014 | 0.000 | 0.549 | 0.023 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.; Kim, K.-S.; Park, S.-W.; You, A.-H.; Lee, S.-W.; Kim, Y.-J.; Kim, M.; Lee, J.-Y.; Choi, J.-H. Correlation between the Perfusion Index and Intraoperative Hypothermia: A Prospective Observational Pilot Study. Medicina 2021, 57, 364. https://doi.org/10.3390/medicina57040364
Lee S, Kim K-S, Park S-W, You A-H, Lee S-W, Kim Y-J, Kim M, Lee J-Y, Choi J-H. Correlation between the Perfusion Index and Intraoperative Hypothermia: A Prospective Observational Pilot Study. Medicina. 2021; 57(4):364. https://doi.org/10.3390/medicina57040364
Chicago/Turabian StyleLee, Sangho, Keon-Sik Kim, Sung-Wook Park, Ann-Hee You, Sang-Wook Lee, Yun-Jong Kim, Mihyeon Kim, Ji-Yoo Lee, and Jeong-Hyun Choi. 2021. "Correlation between the Perfusion Index and Intraoperative Hypothermia: A Prospective Observational Pilot Study" Medicina 57, no. 4: 364. https://doi.org/10.3390/medicina57040364