Brain-Derived Neurotrophic Factor and Immune Cells in Osteoarthritis, Chronic Low Back Pain, and Chronic Widespread Pain Patients: Association with Anxiety and Depression

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.1.1. Patients
2.1.2. Healthy Subjects (HSs)
2.2. Outcome Parameters
2.2.1. Biological Mediators
2.2.2. Questionnaires
2.3. Statistical Analyses
2.4. Sample Size Calculation
3. Results
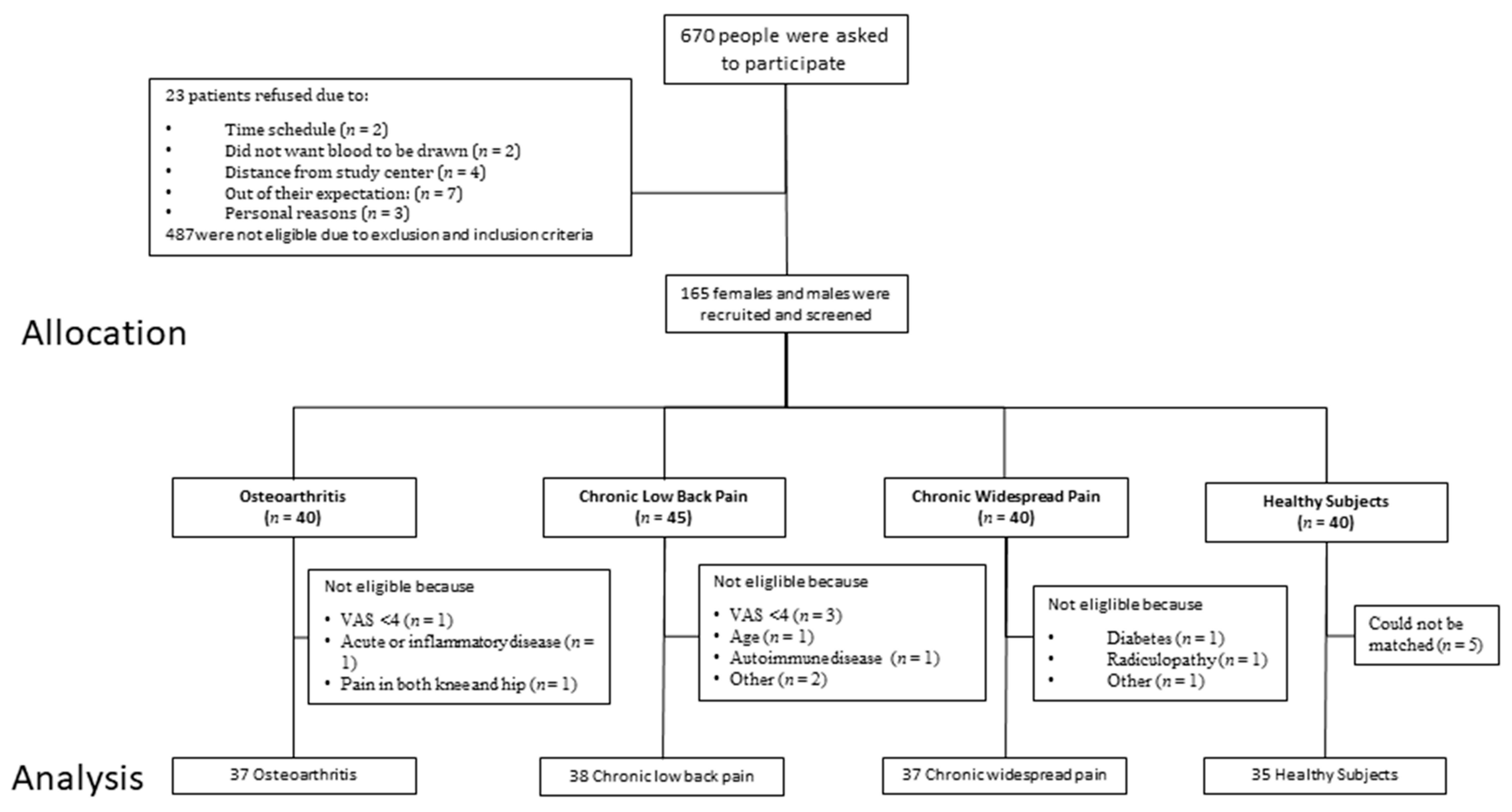
3.1. Patients Recruitment
3.2. Age, Sex, and Body-Related Composition Parameters
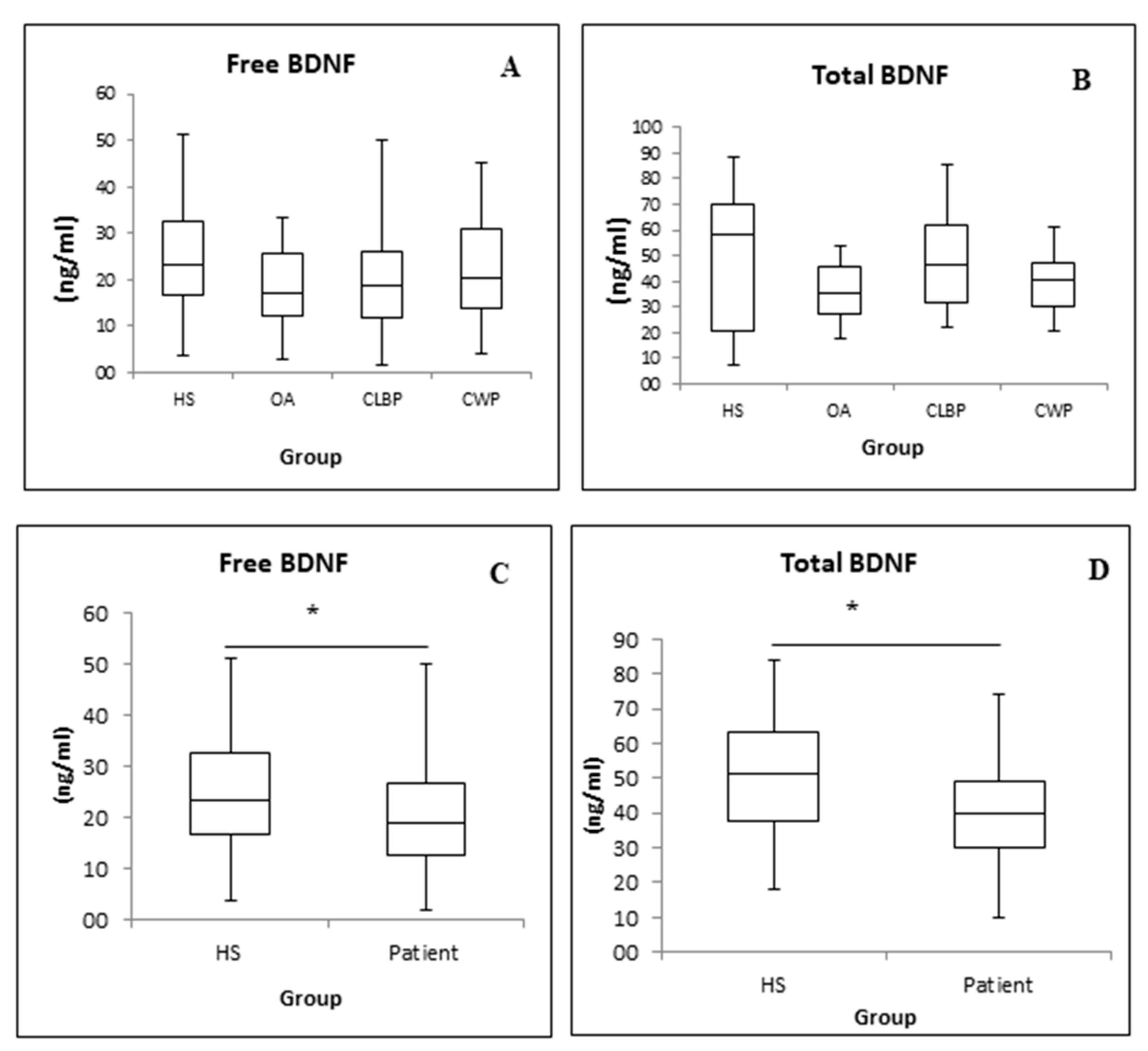
3.3. Free and Total BDNF
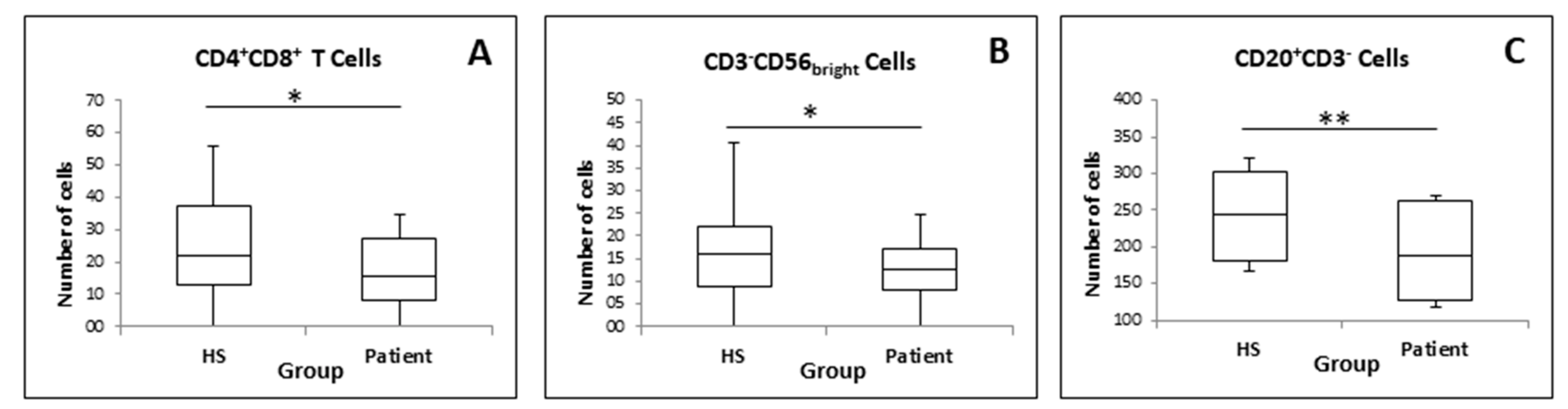
3.4. Phenotypic Profiles of Immune Cells in Chronic Pain Patients
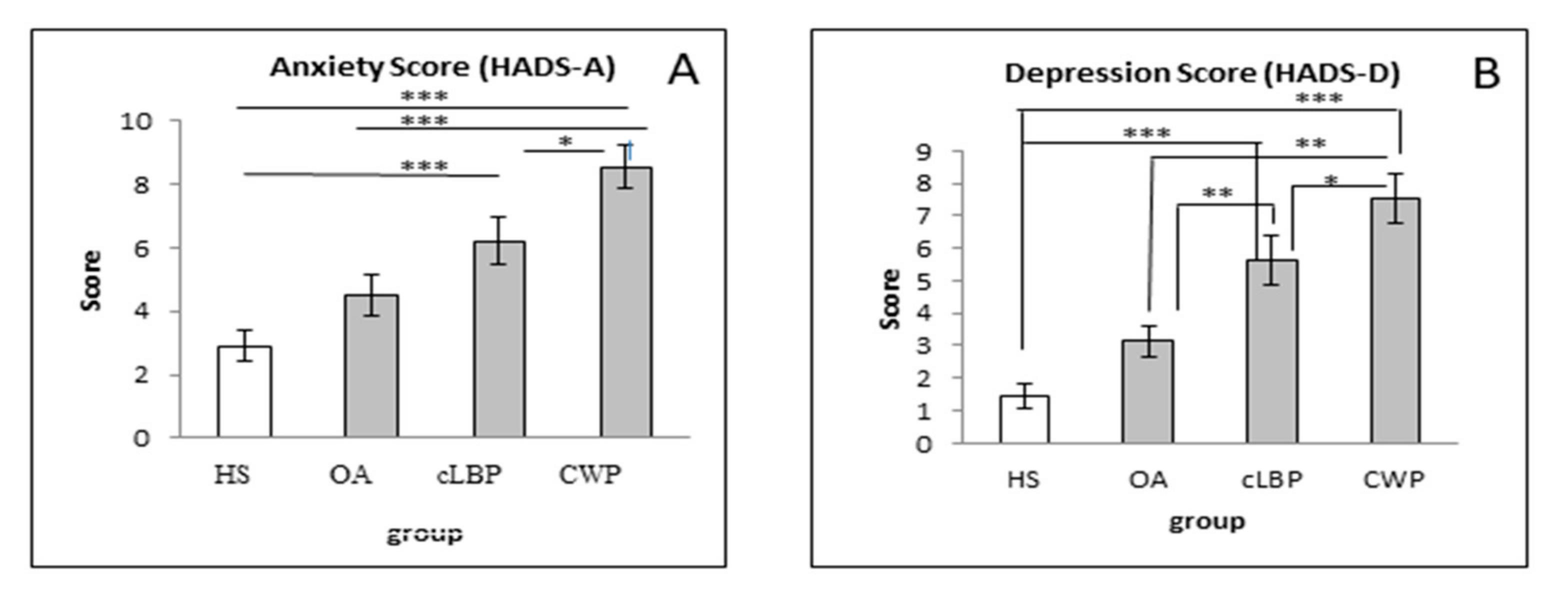
3.5. Anxiety and Depression
3.6. BDNF and Immune Cells Subgroup Analysis Based on Anxiety and Depression Score
3.7. Clinical Data and Biological Mediators
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Merskey, H.B.N. Classification of Chronic Pain; IASP Press: Seattle, WA, USA, 1994. [Google Scholar]
- Schaible, H.G.; Vanegas, H. How do we manage chronic pain? Baillieres Best Pract. Res. Clin. Rheumatol. 2000, 14, 797–811. [Google Scholar] [CrossRef] [PubMed]
- Treede, R.D.; Rief, W.; Barke, A.; Aziz, Q.; Bennett, M.I.; Benoliel, R.; Cohen, M.; Evers, S.; Finnerup, N.B.; First, M.B.; et al. Chronic pain as a symptom or a disease: The IASP Classification of Chronic Pain for the International Classification of Diseases (ICD-11). Pain 2019, 160, 19–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dieppe, P. Chronic musculoskeletal pain. BMJ 2013, 346, f3146. [Google Scholar] [CrossRef] [PubMed]
- Hadi, M.A.; McHugh, G.A.; Closs, S.J. Impact of Chronic Pain on Patients’ Quality of Life: A Comparative Mixed-Methods Study. J. Patient Exp. 2019, 6, 133–141. [Google Scholar] [CrossRef] [PubMed]
- Plotnikoff, R.; Karunamuni, N.; Lytvyak, E.; Penfold, C.; Schopflocher, D.; Imayama, I.; Johnson, S.T.; Raine, K. Osteoarthritis prevalence and modifiable factors: A population study. BMC Public Health 2015, 15, 1195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Man, G.S.; Mologhianu, G. Osteoarthritis pathogenesis—A complex process that involves the entire joint. J. Med. Life 2014, 7, 37–41. [Google Scholar]
- Nguyen, U.S.; Zhang, Y.; Zhu, Y.; Niu, J.; Zhang, B.; Felson, D.T. Increasing prevalence of knee pain and symptomatic knee osteoarthritis: Survey and cohort data. Ann. Intern. Med. 2011, 155, 725–732. [Google Scholar] [CrossRef] [PubMed]
- Miller, R.E.; Tran, P.B.; Obeidat, A.M.; Raghu, P.; Ishihara, S.; Miller, R.J.; Malfait, A.M. The Role of Peripheral Nociceptive Neurons in the Pathophysiology of Osteoarthritis Pain. Curr. Osteoporos. Rep. 2015, 13, 318–326. [Google Scholar] [CrossRef] [PubMed]
- Chou, R. Low back pain (chronic). BMJ Clin. Evid. 2010, 2010, 1116. [Google Scholar]
- Andersson, G.B. Epidemiological features of chronic low-back pain. Lancet 1999, 354, 581–585. [Google Scholar] [CrossRef]
- Neuhauser, H.E.U.; Ziese, T. Chronische Rückenschmerzen in der Allgemeinbevölkerung in Deutschland 2002/2003: Prävalenz und besonders betroffene Bevölkerungsgruppen. Gesundheitswesen 2005, 67, 685–693. [Google Scholar] [CrossRef] [PubMed]
- Owen, P.J.; Miller, C.T.; Mundell, N.L.; Verswijveren, S.; Tagliaferri, S.D.; Brisby, H.; Bowe, S.J.; Belavy, D.L. Which specific modes of exercise training are most effective for treating low back pain? Network meta-analysis. Br. J. Sports Med. 2020, 54, 1279–1287. [Google Scholar] [CrossRef] [PubMed]
- Kjaer, P.; Kongsted, A.; Ris, I.; Abbott, A.; Rasmussen, C.D.N.; Roos, E.M.; Skou, S.T.; Andersen, T.E.; Hartvigsen, J. GLA:D((R)) Back group-based patient education integrated with exercises to support self-management of back pain—Development, theories and scientific evidence. BMC Musculoskelet Disord 2018, 19, 418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wieland, L.S.; Skoetz, N.; Pilkington, K.; Vempati, R.; D’Adamo, C.R.; Berman, B.M. Yoga treatment for chronic non-specific low back pain. Cochrane Database Syst. Rev. 2017, 1, CD010671. [Google Scholar] [CrossRef] [PubMed]
- Siegenthaler, A.; Schliessbach, J.; Vuilleumier, P.H.; Juni, P.; Zeilhofer, H.U.; Arendt-Nielsen, L.; Curatolo, M. Linking altered central pain processing and genetic polymorphism to drug efficacy in chronic low back pain. BMC Pharmacol. Toxicol. 2015, 16, 23. [Google Scholar] [CrossRef] [Green Version]
- Nugraha, B.; Korallus, C.; Gutenbrunner, C. Serum level of brain-derived neurotrophic factor in fibromyalgia syndrome correlates with depression but not anxiety. Neurochem. Int. 2013, 62, 281–286. [Google Scholar] [CrossRef] [PubMed]
- Andrews, P.; Steultjens, M.; Riskowski, J. Chronic widespread pain prevalence in the general population: A systematic review. Eur. J. Pain 2018, 22, 5–18. [Google Scholar] [CrossRef] [Green Version]
- Nugraha, B.; Karst, M.; Engeli, S.; Gutenbrunner, C. Brain-derived neurotrophic factor and exercise in fibromyalgia syndrome patients: A mini review. Rheumatol. Int. 2012, 32, 2593–2599. [Google Scholar] [CrossRef]
- Girbes, E.L.; Duenas, L.; Barbero, M.; Falla, D.; Baert, I.A.C.; Meeus, M.; Sanchez-Frutos, J.; Aguilella, L.; Nijs, J. Expanded Distribution of Pain as a Sign of Central Sensitization in Individuals With Symptomatic Knee Osteoarthritis. Phys. Ther. 2016, 96, 1196–1207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roussel, N.A.; Nijs, J.; Meeus, M.; Mylius, V.; Fayt, C.; Oostendorp, R. Central sensitization and altered central pain processing in chronic low back pain: Fact or myth? Clin. J. Pain 2013, 29, 625–638. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calabrese, F.; Rossetti, A.C.; Racagni, G.; Gass, P.; Riva, M.A.; Molteni, R. Brain-derived neurotrophic factor: A bridge between inflammation and neuroplasticity. Front. Cell Neurosci. 2014, 8, 430. [Google Scholar] [CrossRef] [PubMed]
- Juric, D.M.; Loncar, D.; Carman-Krzan, M. Noradrenergic stimulation of BDNF synthesis in astrocytes: Mediation via alpha1- and beta1/beta2-adrenergic receptors. Neurochem. Int. 2008, 52, 297–306. [Google Scholar] [CrossRef] [PubMed]
- Sikandar, S.; Minett, M.S.; Millet, Q.; Santana-Varela, S.; Lau, J.; Wood, J.N.; Zhao, J. Brain-derived neurotrophic factor derived from sensory neurons plays a critical role in chronic pain. Brain 2018, 141, 1028–1039. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Qian, Y.L.; Li, C.; Liu, D.; Wang, L.; Wang, X.Y.; Liu, M.J.; Liu, H.; Zhang, S.; Guo, X.Y.; et al. Brain-Derived Neurotrophic Factor in the Mesolimbic Reward Circuitry Mediates Nociception in Chronic Neuropathic Pain. Biol. Psychiatry 2017, 82, 608–618. [Google Scholar] [CrossRef]
- O’Mahony, L.F.; Srivastava, A.; Mehta, P.; Ciurtin, C. Is fibromyalgia associated with a unique cytokine profile? Rheumatology 2021. [Google Scholar] [CrossRef]
- Chun, M.Y.; Cho, B.J.; Yoo, S.H.; Oh, B.; Kang, J.S.; Yeon, C. Association between sleep duration and musculoskeletal pain: The Korea National Health and Nutrition Examination Survey 2010–2015. Medicine 2018, 97, e13656. [Google Scholar] [CrossRef]
- Nugraha, B.G.C. Depressive Symptoms, Exercise, and Brain-Derived Neurotrophic Factor in Fibromyalgia Syndrome: A Mini Review. J. Autoimmune Dis. Rheumatol. 2013, 1, 19–23. [Google Scholar] [CrossRef] [Green Version]
- Haas, L.; Portela, L.V.; Bohmer, A.E.; Oses, J.P.; Lara, D.R. Increased plasma levels of brain derived neurotrophic factor (BDNF) in patients with fibromyalgia. Neurochem. Res. 2010, 35, 830–834. [Google Scholar] [CrossRef]
- Laske, C.; Stransky, E.; Eschweiler, G.W.; Klein, R.; Wittorf, A.; Leyhe, T.; Richartz, E.; Kohler, N.; Bartels, M.; Buchkremer, G.; et al. Increased BDNF serum concentration in fibromyalgia with or without depression or antidepressants. J. Psychiatr. Res. 2007, 41, 600–605. [Google Scholar] [CrossRef]
- Gowler, P.R.W.; Li, L.; Woodhams, S.G.; Bennett, A.J.; Suzuki, R.; Walsh, D.A.; Chapman, V. Peripheral brain-derived neurotrophic factor contributes to chronic osteoarthritis joint pain. Pain 2020, 161, 61–73. [Google Scholar] [CrossRef]
- Vardeh, D.; Mannion, R.J.; Woolf, C.J. Toward a Mechanism-Based Approach to Pain Diagnosis. J. Pain Off. J. Am. Pain Soc. 2016, 17, T50–T69. [Google Scholar] [CrossRef] [Green Version]
- Vierck, C.J., Jr. Mechanisms underlying development of spatially distributed chronic pain (fibromyalgia). Pain 2006, 124, 242–263. [Google Scholar] [CrossRef] [PubMed]
- Latremoliere, A.; Woolf, C.J. Central sensitization: A generator of pain hypersensitivity by central neural plasticity. J. Pain Off. J. Am. Pain Soc. 2009, 10, 895–926. [Google Scholar] [CrossRef] [Green Version]
- Altman, R.; Alarcon, G.; Appelrouth, D.; Bloch, D.; Borenstein, D.; Brandt, K.; Brown, C.; Cooke, T.D.; Daniel, W.; Feldman, D.; et al. The American College of Rheumatology criteria for the classification and reporting of osteoarthritis of the hip. Arthritis Rheum. 1991, 34, 505–514. [Google Scholar] [CrossRef]
- Zhang, W.; Doherty, M.; Peat, G.; Bierma-Zeinstra, M.A.; Arden, N.K.; Bresnihan, B.; Herrero-Beaumont, G.; Kirschner, S.; Leeb, B.F.; Lohmander, L.S.; et al. EULAR evidence-based recommendations for the diagnosis of knee osteoarthritis. Ann. Rheum. Dis. 2010, 69, 483–489. [Google Scholar] [CrossRef] [Green Version]
- AWMF. VersorgungsLeitlinie, Nationale. “Nicht-spezifischer Kreuzschmerz.” 2. Auflage; AWMF: Frankfurt, German, 2017. [Google Scholar]
- MacFarlane, G.J.; Croft, P.R.; Schollum, J.; Silman, A.J. Widespread pain: Is an improved classification possible? J. Rheumatol. 1996, 23, 1628–1632. [Google Scholar]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seifert, T.; Brassard, P.; Wissenberg, M.; Rasmussen, P.; Nordby, P.; Stallknecht, B.; Adser, H.; Jakobsen, A.H.; Pilegaard, H.; Nielsen, H.B.; et al. Endurance training enhances BDNF release from the human brain. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2010, 298, R372–R377. [Google Scholar] [CrossRef] [Green Version]
- Caumo, W.; Deitos, A.; Carvalho, S.; Leite, J.; Carvalho, F.; Dussan-Sarria, J.A.; Lopes-Tarrago-Mda, G.; Souza, A.; Torres, I.L.; Fregni, F. Motor Cortex Excitability and BDNF Levels in Chronic Musculoskeletal Pain According to Structural Pathology. Front. Hum. Neurosci. 2016, 10, 357. [Google Scholar] [CrossRef] [PubMed]
- Baumeister, D.; Eich, W.; Saft, S.; Geisel, O.; Hellweg, R.; Finn, A.; Svensson, C.I.; Tesarz, J. No evidence for altered plasma NGF and BDNF levels in fibromyalgia patients. Sci. Rep. 2019, 9, 13667. [Google Scholar] [CrossRef] [PubMed]
- Williams, M.S.; Ngongang, C.K.; Ouyang, P.; Betoudji, F.; Harrer, C.; Wang, N.Y.; Ziegelstein, R.C. Gender differences in platelet brain derived neurotrophic factor in patients with cardiovascular disease and depression. J. Psychiatr. Res. 2016, 78, 72–77. [Google Scholar] [CrossRef]
- Lommatzsch, M.; Zingler, D.; Schuhbaeck, K.; Schloetcke, K.; Zingler, C.; Schuff-Werner, P.; Virchow, J.C. The impact of age, weight and gender on BDNF levels in human platelets and plasma. Neurobiol. Aging 2005, 26, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Yoo, J.J.; Cho, N.H.; Lim, S.H.; Kim, H.A. Relationships between body mass index, fat mass, muscle mass, and musculoskeletal pain in community residents. Arthritis Rheumatol. 2014, 66, 3511–3520. [Google Scholar] [CrossRef]
- Griffin, E.W.; Mullally, S.; Foley, C.; Warmington, S.A.; O’Mara, S.M.; Kelly, A.M. Aerobic exercise improves hippocampal function and increases BDNF in the serum of young adult males. Physiol. Behav. 2011, 104, 934–941. [Google Scholar] [CrossRef]
- Bathina, S.; Das, U.N. Brain-derived neurotrophic factor and its clinical implications. Arch. Med. Sci. 2015, 11, 1164–1178. [Google Scholar] [CrossRef] [PubMed]
- Xu, B.; Xie, X. Neurotrophic factor control of satiety and body weight. Nat. Rev. Neurosci. 2016, 17, 282–292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tao, Y.S.; Piao, S.G.; Jin, Y.S.; Jin, J.Z.; Zheng, H.L.; Zhao, H.Y.; Lim, S.W.; Yang, C.W.; Li, C. Expression of brain-derived neurotrophic factor in kidneys from normal and cyclosporine-treated rats. BMC Nephrol. 2018, 19, 63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gureje, O.; von Korff, M.; Simon, G.E.; Gater, R. Persistent pain and well-being: A World Health Organization Study in Primary Care. JAMA 1998, 280, 147–151. [Google Scholar] [CrossRef]
- Mundal, I.; Grawe, R.W.; Bjorngaard, J.H.; Linaker, O.M.; Fors, E.A. Psychosocial factors and risk of chronic widespread pain: An 11-year follow-up study—The HUNT study. Pain 2014, 155, 1555–1561. [Google Scholar] [CrossRef]
- Price, D.D.; Staud, R.; Robinson, M.E.; Mauderli, A.P.; Cannon, R.; Vierck, C.J. Enhanced temporal summation of second pain and its central modulation in fibromyalgia patients. Pain 2002, 99, 49–59. [Google Scholar] [CrossRef]
- Hunfeld, J.A.; Perquin, C.W.; Duivenvoorden, H.J.; Hazebroek-Kampschreur, A.A.; Passchier, J.; van Suijlekom-Smit, L.W.; van der Wouden, J.C. Chronic pain and its impact on quality of life in adolescents and their families. J. Pediatr. Psychol. 2001, 26, 145–153. [Google Scholar] [CrossRef] [Green Version]
- Nugraha, B.; Korallus, C.; Kielstein, H.; Gutenbrunner, C. CD3+CD56+natural killer T cells in fibromyalgia syndrome patients: Association with the intensity of depression. Clin. Exp. Rheumatol. 2013, 31, S9–S15. [Google Scholar]
- Huss, R.S.; Huddleston, J.I.; Goodman, S.B.; Butcher, E.C.; Zabel, B.A. Synovial tissue-infiltrating natural killer cells in osteoarthritis and periprosthetic inflammation. Arthritis Rheum. 2010, 62, 3799–3805. [Google Scholar] [CrossRef]
- Majidi-Zolbanin, S.F.A.; Nourazar, S.G.; Movasaghpour, A.; Ghojazadeh, M.; Jafar, R.; Majidi, J. Correlation between major depressive disorder and circulating natural killer cells. Arch. Med. Lab. Sci. 2015, 1, 51–55. [Google Scholar]
- Wang, H.Q.; Zeng, Y.; Zhang, M.H.; Ma, H.B.; Xu, B.; Jiang, H.; Wang, J.R.; Li, G. CD56(bright)CD16(-) natural killer cells are shifted toward an IFN-gamma-promoting phenotype with reduced regulatory capacity in osteoarthritis. Hum. Immunol. 2019, 80, 871–877. [Google Scholar] [CrossRef] [PubMed]
- Brennan, P.C.; Graham, M.A.; Triano, J.J.; Hondras, M.A.; Anderson, R.J. Lymphocyte profiles in patients with chronic low back pain enrolled in a clinical trial. J. Manip. Physiol. Ther. 1994, 17, 219–227. [Google Scholar]
- Landis, C.A.; Lentz, M.J.; Tsuji, J.; Buchwald, D.; Shaver, J.L. Pain, psychological variables, sleep quality, and natural killer cell activity in midlife women with and without fibromyalgia. Brain Behav. Immun. 2004, 18, 304–313. [Google Scholar] [CrossRef] [PubMed]
- Laumet, G.; Ma, J.; Robison, A.J.; Kumari, S.; Heijnen, C.J.; Kavelaars, A. T Cells as an Emerging Target for Chronic Pain Therapy. Front. Mol. Neurosci. 2019, 12, 216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ziv, Y.; Ron, N.; Butovsky, O.; Landa, G.; Sudai, E.; Greenberg, N.; Cohen, H.; Kipnis, J.; Schwartz, M. Immune cells contribute to the maintenance of neurogenesis and spatial learning abilities in adulthood. Nat. Neurosci. 2006, 9, 268–275. [Google Scholar] [CrossRef] [PubMed]
- Castren, E.; Kojima, M. Brain-derived neurotrophic factor in mood disorders and antidepressant treatments. Neurobiol. Dis. 2017, 97, 119–126. [Google Scholar] [CrossRef] [Green Version]
- Axford, J.; Butt, A.; Heron, C.; Hammond, J.; Morgan, J.; Alavi, A.; Bolton, J.; Bland, M. Prevalence of anxiety and depression in osteoarthritis: Use of the Hospital Anxiety and Depression Scale as a screening tool. Clin. Rheumatol. 2010, 29, 1277–1283. [Google Scholar] [CrossRef]
- Martinowich, K.; Manji, H.; Lu, B. New insights into BDNF function in depression and anxiety. Nat. Neurosci. 2007, 10, 1089–1093. [Google Scholar] [CrossRef]
- Rovner, G.S.; Sunnerhagen, K.S.; Bjorkdahl, A.; Gerdle, B.; Borsbo, B.; Johansson, F.; Gillanders, D. Chronic pain and sex-differences; women accept and move, while men feel blue. PLoS ONE 2017, 12, e0175737. [Google Scholar] [CrossRef] [Green Version]
- Phillips, C. Brain-Derived Neurotrophic Factor, Depression, and Physical Activity: Making the Neuroplastic Connection. Neural. Plast. 2017, 2017, 7260130. [Google Scholar] [CrossRef]
- Hu, J.; Cai, M.; Shang, Q.; Li, Z.; Feng, Y.; Liu, B.; Xue, X.; Lou, S. Elevated Lactate by High-Intensity Interval Training Regulates the Hippocampal BDNF Expression and the Mitochondrial Quality Control System. Front. Physiol. 2021, 12, 629914. [Google Scholar] [CrossRef] [PubMed]
- de Poli, R.A.B.; Lopes, V.H.F.; Lira, F.S.; Zagatto, A.M.; Jimenez-Maldonado, A.; Antunes, B.M. Peripheral BDNF and psycho-behavioral aspects are positively modulated by high-intensity intermittent exercise and fitness in healthy women. Sci. Rep. 2021, 11, 4113. [Google Scholar] [CrossRef] [PubMed]
- Nugraha, B.; Anwar, S.L.; Gutenbrunner, C.; Korallus, C. Polymorphisms of brain-derived neurotrophic factor genes are associated with anxiety and body mass index in fibromyalgia syndrome patients. BMC Res. Notes 2020, 13, 402. [Google Scholar] [CrossRef] [PubMed]
- Kotlega, D.; Zembron-Lacny, A.; Morawin, B.; Golab-Janowska, M.; Nowacki, P.; Szczuko, M. Free Fatty Acids and Their Inflammatory Derivatives Affect BDNF in Stroke Patients. Mediat. Inflamm. 2020, 2020, 6676247. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | HS | OA | cLBP | CWP | p-Value |
|---|---|---|---|---|---|
| Mean ± SEM | Mean ± SEM | Mean ± SEM | Mean ± SEM | ||
| Age (years) | 49.97 ± 1.97 | 55.86 ± 1.91 | 52.24 ± 2.34 | 55.92 ± 1.28 | 0.076 |
| Sex (N; male/female) | 10/25 | 15/22 | 12/26 | 3/34 | 0.014 § |
| Pain (VAS) | 0.03 ± 0.03 | 5.43 ± 0.19 | 5.88 ± 0.20 | 6.39 ± 0.28 | 0.00 |
| Height (cm) | 169.33 ± 1.42 | 173.05 ± 1.57 | 170.39 ± 1.20 | 166.59 ± 1.09 | 0.008 |
| Body weight (kg) | 71.69 ± 2.96 | 88.06 ± 3.91 | 77.75 ± 2.81 | 77.40 ± 3.17 | 0.006 |
| BMI (kg/cm2) | 24.77 ± 0.76 | 29.14 ± 1.03 | 26.70 ± 0.86 | 27.68 ± 0.92 | 0.008 |
| SMM (kg) | 28.76 ± 1.20 | 32.37 ± 1.40 | 28.49 ± 0.92 | 26.90 ± 0.89 | 0.006 |
| BFM (kg) | 19.91 ± 1.71 | 29.97 ± 2.29 | 26.17 ± 2.10 | 28.54 ± 1.89 | 0.004 |
| BWM (kg) | 37.97 ± 1.45 | 42.65 ± 1.72 | 37.88 ± 1.12 | 35.87 ± 1.07 | 0.005 |
| FFM (kg) | 51.78 ± 1.97 | 58.09 ± 2.34 | 51.58 ± 1.52 | 48.60 ± 1.45 | 0.004 |
| BFP (%) | 27.10 ± 1.33 | 33.18 ± 1.40 | 32.21 ± 1.72 | 35.74 ± 1.06 | 0.000 |
| WHR | 0.92 ± 0.01 | 0.99 ± 0.01 | 0.97 ± 0.02 | 0.98 ± 0.01 | 0.001 |
| HS (N = 35) | OA (N = 37) | cLBP (N = 38) | CWP (N = 37) | p-Value | |
|---|---|---|---|---|---|
| Median (IQR) | Median (IQR) | Median (IQR) | Median (IQR) | ||
| CD3+ (number of cells) | 1390.00 (1023.00–1671.00) | 1206.00 (931.00–1436.50) | 1219.50 (1066.25–1716.75) | 1305.00 (1112.50–1573.50) | N.S |
| CD3+ CD4+ (number of cells) | 865.00 (675.00–1171.00) | 787.00 (545.00–1043.00) | 859.50 (703.50–1080.25) | 889.00 (732.00–1064.00) | N.S |
| CD3+ CD8+ (number of cells) | 452.00 (309.00–579.00) | 386.00 (254.50–494.00) | 385.50 (272.25–564.25) | 426.00 (284.00–510.00) | N.S |
| CD8+ (number of cells) | 628.00 (466.00–737.00) | 507.00 (364.00–686.00) | 557.50 (372.00–763.25) | 527.00 (423.00–658.50) | N.S |
| CD4− CD8− T cells (number of cells) | 32.00 (21.00–59.00) | 29.00 (18.50–61.00) | 37.00 (28.25–61.00) | 33.00 (24.00–67.50) | N.S |
| CD4+ CD8+ T cells (number of cells) | 22.00 (13.00–37.00) | 16.00 (9.00–27.50) | 15.00 (7.00–27.75) | 14.00 (9.00–28.00) | N.S |
| CD3+ CD20+ (number of cells) | 58.00 (37.00–94.00) | 52.00 (32.00–79.50) | 45.50 (28.00–91.00) | 38.00 (25.50–66.50) | N.S |
| CD3+ CD56+ (number of cells) | 97.00 (36.00–141.00) | 63.00 (38.50–140.50) | 78.00 (44.00–183.25) | 112.00 (36.00–191.50) | N.S |
| CD3− CD56dim (number of cells) | 262.00 (236.00–347.00) | 226.00 (152.50–320.50) | 241.50 (152.50–391.00) | 215.00 (153.50–359.50) | N.S |
| CD3− CD56bright (number of cells) | 16.00 (9.00–22.00) | 11.00 (7.50–17.50) | 13.00 (8.00–17.00) | 13.00 (8.00-16.00) | 0.03 |
| CD3− CD56+ CD8+ (number of cells) | 287.00 (247.00–356.00) | 288.00 (165.00–328.00) | 256.00 (166.00–398.25) | 224.00 (167.00–370.50) | N.S |
| CD20+ CD3− (number of cells) | 243.00 (180.00–302.00) | 180.00 (121.00–228.00) | 192.50 (122.75–281.50) | 184.00 (140.00–260.00) | N.S |
| HADS-A Score | |||
|---|---|---|---|
| ≤7 | 8–10 | ≥11 | |
| OA | 81.1% | 8.1% | 10.8% |
| cLBP | 71.1% | 10.5% | 18.4% |
| CWP | 43.2% | 21.7% | 35.1% |
| HADS-D Score | |||
| ≤7 | 8–10 | ≥11 | |
| OA | 94.6% | 0.0% | 5.4% |
| cLBP | 71.1% | 10.5% | 18.4% |
| CWP | 56.8% | 16.2% | 27.0% |
| Clinical Parameters | Clinical Biomediator Parameters | Correlation and p-Value | ||
|---|---|---|---|---|
| OA | BW | BNDF Free | R: −0.357; p = 0.030 | |
| BW | BDNF Total | R: −0.479; p = 0.003 | ||
| HADS-D | CD3− CD56bright | R: −0.395; p = 0.015 | ||
| cLBP | Pain (VAS) | NADS-A | R: 0.532; p = 0.001 | |
| NADS-D | R: 0.595; p = 0.000 | |||
| CWP | Pain (VAS) | HADS-A | R: 0.328; p = 0.047 | |
| HADS-D | R: 0.328; p = 0.047 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dimmek, D.J.; Korallus, C.; Buyny, S.; Christoph, G.; Lichtinghagen, R.; Jacobs, R.; Nugraha, B. Brain-Derived Neurotrophic Factor and Immune Cells in Osteoarthritis, Chronic Low Back Pain, and Chronic Widespread Pain Patients: Association with Anxiety and Depression. Medicina 2021, 57, 327. https://doi.org/10.3390/medicina57040327
Dimmek DJ, Korallus C, Buyny S, Christoph G, Lichtinghagen R, Jacobs R, Nugraha B. Brain-Derived Neurotrophic Factor and Immune Cells in Osteoarthritis, Chronic Low Back Pain, and Chronic Widespread Pain Patients: Association with Anxiety and Depression. Medicina. 2021; 57(4):327. https://doi.org/10.3390/medicina57040327
Chicago/Turabian StyleDimmek, Dominique Josephine, Christoph Korallus, Sabine Buyny, Gutenbrunner Christoph, Ralf Lichtinghagen, Roland Jacobs, and Boya Nugraha. 2021. "Brain-Derived Neurotrophic Factor and Immune Cells in Osteoarthritis, Chronic Low Back Pain, and Chronic Widespread Pain Patients: Association with Anxiety and Depression" Medicina 57, no. 4: 327. https://doi.org/10.3390/medicina57040327