Environmental Risk Factors for Bipolar Disorders and High-Risk States in Adolescence: A Systematic Review

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Study Selection
2.3. Data Extraction
2.4. Risk of Bias Assessment
3. Results
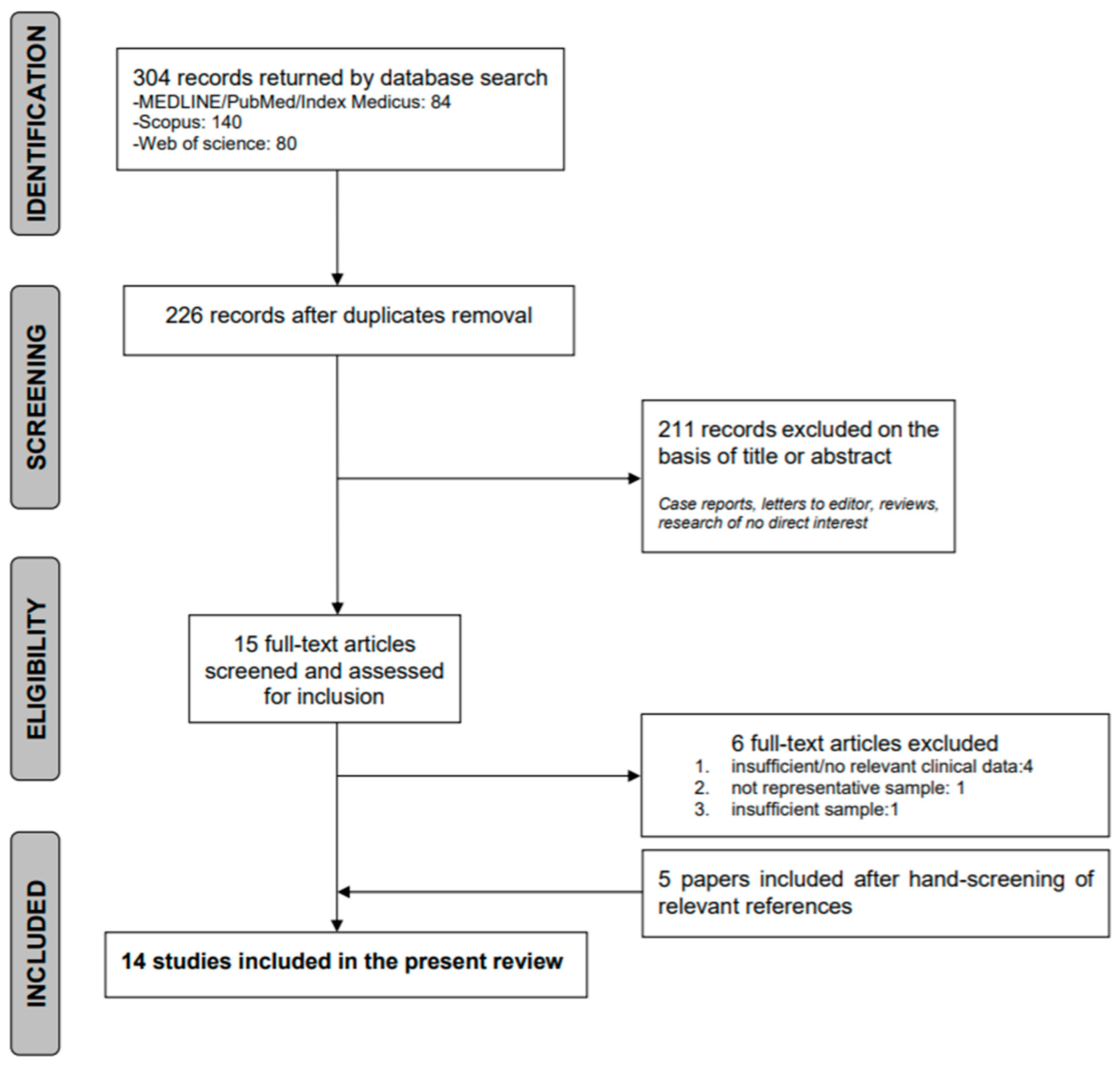
3.1. Systematich Search Results
3.2. Content Results
3.2.1. Environmental Risk Factors in Adolescents with BD
3.2.2. Environmental Risk Factors in BD High-Risk Adolescents
3.3. Risk of Bias Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Connor, D.F.; Ford, J.D.; Pearson, G.S.; Scranton, V.L.; Dusad, A. Early-Onset Bipolar Disorder: Characteristics and Outcomes in the Clinic. J. Child Adolesc. Psychopharmacol. 2017, 27, 875–883. [Google Scholar] [CrossRef]
- Geoffroy, P.A.; Etain, B.; Jamain, S.; Bellivier, F.; Leboyer, M. Early onset bipolar disorder: Validation from admixture analyses and biomarkers. Can. J. Psychiatry 2013, 58, 240–248. [Google Scholar] [CrossRef] [Green Version]
- Vieta, E.; Salagre, E.; Grande, I.; Carvalho, A.F.; Fernandes, B.S.; Berk, M.; Birmaher, B.; Tohen, M.; Suppes, T. Early intervention in Bipolar disorder. Am. J. Psychiatry 2018, 175, 411–426. [Google Scholar] [CrossRef]
- Baldessarini, R.J.; Bolzani, L.; Cruz, N.; Jones, P.B.; Lai, M.; Lepri, B.; Perez, J.; Salvatore, P.; Tohen, M.; Tondo, L. Onset-age of bipolar disorders at six international sites. J. Affect. Disord. 2010. [Google Scholar] [CrossRef]
- Altamura, A.C.; Buoli, M.; Albano, A.; Dell’Osso, B. Age at onset and latency to treatment (duration of untreated illness) in patients with mood and anxiety disorders: A naturalistic study. Int. Clin. Psychopharmacol. 2010, 25, 172–179. [Google Scholar] [CrossRef]
- Drancourt, N.; Etain, B.; Lajnef, M.; Henry, C.; Raust, A.; Cochet, B.; Mathieu, F.; Gard, S.; M’Bailara, K.; Zanouy, L.; et al. Duration of untreated bipolar disorder: Missed opportunities on the long road to optimal treatment. Acta Psychiatr. Scand. 2013, 127, 136–144. [Google Scholar] [CrossRef]
- Koenders, M.A.; Mesman, E.; Giltay, E.J.; Elzinga, B.M.; Hillegers, M.H.J. Traumatic experiences, family functioning, and mood disorder development in bipolar offspring. Br. J. Clin. Psychol. 2020, 59, 277–289. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.-I.; Lee, H.-J.; Cho, C.-H.; Kang, S.-G.; Yoon, H.-K.; Park, Y.-M.; Lee, S.-H.; Moon, J.-H.; Song, H.-M.; Lee, E.; et al. Association of CLOCK, ARNTL, and NPAS2 gene polymorphisms and seasonal variations in mood and behavior. Chronobiol. Int. 2015, 32, 785–791. [Google Scholar] [CrossRef]
- Craddock, N.; Sklar, P. Genetics of bipolar disorder. Lancet 2013, 381, 1654–1662. [Google Scholar] [CrossRef]
- Uher, R. Gene-environment interactions in severe mental illness. Front. Psychiatry 2014, 5. [Google Scholar] [CrossRef] [Green Version]
- Khan, A.; Plana-Ripoll, O.; Antonsen, S.; Brandt, J.; Geels, C.; Landecker, H.; Sullivan, P.F.; Pedersen, C.B.; Rzhetsky, A. Environmental pollution is associated with increased risk of psychiatric disorders in the US and Denmark. PLoS Biol. 2019, 17. [Google Scholar] [CrossRef]
- Marrie, R.A.; Reingold, S.; Cohen, J.; Stuve, O.; Trojano, M.; Sorensen, P.S.; Cutter, G.; Reider, N. The incidence and prevalence of psychiatric disorders in multiple sclerosis: A systematic review. Mult. Scler. J. 2015, 21, 305–317. [Google Scholar] [CrossRef] [Green Version]
- Leo, R.J.; Singh, J. Migraine headache and bipolar disorder comorbidity: A systematic review of the literature and clinical implications. Scand. J. Pain 2016, 11, 136–145. [Google Scholar] [CrossRef]
- Šprah, L.; Dernovšek, M.Z.; Wahlbeck, K.; Haaramo, P. Psychiatric readmissions and their association with physical comorbidity: A systematic literature review. BMC Psychiatry 2017, 17, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Agnew-Blais, J.; Danese, A. Childhood maltreatment and unfavourable clinical outcomes in bipolar disorder: A systematic review and meta-analysis. Lancet Psychiatry 2016, 3, 342–349. [Google Scholar] [CrossRef]
- Sutterland, A.L.; Fond, G.; Kuin, A.; Koeter, M.W.J.; Lutter, R.; van Gool, T.; Yolken, R.; Szoke, A.; Leboyer, M.; De Haan, L. Beyond the association. Toxoplasma gondii in schizophrenia, bipolar disorder, and addiction: Systematic review and meta-analysis. Acta Psychiatr. Scand. 2015, 132, 161–179. [Google Scholar] [CrossRef]
- Janiri, D.; Sani, G.; Rossi, P.; Piras, F.; Iorio, M.; Banaj, N.; Giuseppin, G.; Spinazzola, E.; Maggiora, M.; Ambrosi, E.; et al. Amygdala and hippocampus volumes are differently affected by childhood trauma in patients with bipolar disorders and healthy controls. Bipolar Disord. 2017, 19, 353–362. [Google Scholar] [CrossRef]
- Janiri, D.; Sani, G.; De Rossi, P.; Piras, F.; Banaj, N.; Ciullo, V.; Simonetti, A.; Arciniegas, D.B.; Spalletta, G. Hippocampal subfield volumes and childhood trauma in bipolar disorders. J. Affect. Disord. 2019, 253, 35–43. [Google Scholar] [CrossRef]
- Raballo, A.; Mechelli, A.; Menculini, G.; Tortorella, A. Risk syndromes in psychiatry: A state-of-the-art overview. Arch. Psychiatry Psychother. 2019, 2, 7–14. [Google Scholar] [CrossRef]
- Bortolato, B.; Köhler, C.A.; Evangelou, E.; León-Caballero, J.; Solmi, M.; Stubbs, B.; Belbasis, L.; Pacchiarotti, I.; Kessing, L.V.; Berk, M.; et al. Systematic assessment of environmental risk factors for bipolar disorder: An umbrella review of systematic reviews and meta-analyses. Bipolar Disord. 2017, 19, 84–96. [Google Scholar] [CrossRef] [Green Version]
- Marangoni, C.; Hernandez, M.; Faedda, G.L. The role of environmental exposures as risk factors for bipolar disorder: A systematic review of longitudinal studies. J. Affect. Disord. 2016, 193, 165–174. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. 2014. Available online: www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 10 September 2020).
- Herzog, R.; Álvarez-Pasquin, M.J.; Díaz, C.; Del Barrio, J.L.; Estrada, J.M.; Gil, Á. Are healthcare workers intentions to vaccinate related to their knowledge, beliefs and attitudes? A systematic review. BMC Public Health 2013, 13. [Google Scholar] [CrossRef] [Green Version]
- Romero, S.; Birmaher, B.; Axelson, D.A.; Iosif, A.M.; Williamson, D.E.; Gill, M.K.; Goldstein, B.I.; Strober, M.A.; Hunt, J.; Goldstein, T.R.; et al. Negative life events in children and adolescents with bipolar disorder. J. Clin. Psychiatry 2009, 70, 1452–1460. [Google Scholar] [CrossRef]
- Romero, S.; Birmaher, B.; Axelson, D.; Goldstein, T.; Goldstein, B.I.; Gill, M.K.; Iosif, A.-M.; Strober, M.A.; Hunt, J.; Esposito-Smythers, C. Prevalence and correlates of physical and sexual abuse in children and adolescents with bipolar disorder. J. Affect. Disord. 2009, 112, 144–150. [Google Scholar] [CrossRef] [Green Version]
- Bakare, M.O.; Agomoh, A.O.; Eaton, J.; Ebigbo, P.O.; Onwukwe, J.U. Functional status and its associated factors in Nigerian adolescents with bipolar disorder. Afr. J. Psychiatry 2011, 14, 388–391. [Google Scholar] [CrossRef] [Green Version]
- Shaffer, D.; Gould, M.S.; Brasic, J.; Fisher, P.; Aluwahlia, S.; Bird, H. A Children’s Global Assessment Scale (CGAS). Arch. Gen. Psychiatry 1983. [Google Scholar] [CrossRef]
- Goldstein, T.R.; Birmaher, B.; Axelson, D.; Goldstein, B.I.; Gill, M.K.; Esposito-Smythers, C.; Ryan, N.D.; Strober, M.A.; Hunt, J.; Keller, M. Family environment and suicidal ideation among bipolar youth. Arch. Suicide Res. 2009, 13, 378–388. [Google Scholar] [CrossRef] [Green Version]
- Olson, D.H.; Portner, J.; Bell, R. FACES II: Family Adaptability and Cohesion Evaluation Scales; University of Minnesota: St. Paul, MN, USA, 1982; pp. 4–24. [Google Scholar]
- Lau, P.; Hawes, D.J.; Hunt, C.; Frankland, A.; Roberts, G.; Wright, A.; Costa, D.S.; Mitchell, P.B. Family environment and psychopathology in offspring of parents with bipolar disorder. J. Affect. Disord. 2018, 226, 12–20. [Google Scholar] [CrossRef]
- Monck, E.; Dobbs, R. Measuring life events in an adolescent population: Methodological issues and related findings. Psychol. Med. 1985, 15, 841–850. [Google Scholar] [CrossRef]
- Kemner, S.M.; Mesman, E.; Nolen, W.A.; Eijckemans, M.J.C.; Hillegers, M.H.J. The role of life events and psychological factors in the onset of first and recurrent mood episodes in bipolar offspring: Results from the Dutch Bipolar Offspring Study. Psychol. Med. 2015, 45, 2571–2581. [Google Scholar] [CrossRef] [Green Version]
- Doucette, S.; Levy, A.; Flowerdew, G.; Horrocks, J.; Grof, P.; Ellenbogen, M.; Duffy, A. Early parent–child relationships and risk of mood disorder in a Canadian sample of offspring of a parent with bipolar disorder: Findings from a 16-year prospective cohort study. Early Interv. Psychiatry 2016, 10, 381–389. [Google Scholar] [CrossRef]
- Reichart, C.G.; Van Der Ende, J.; Hillegers, M.H.J.; Wals, M.; Bongers, I.L.; Nolen, W.A.; Ormel, J.; Verhulst, F.C. Perceived parental rearing of bipolar offspring. Acta Psychiatr. Scand. 2007, 115, 21–28. [Google Scholar] [CrossRef]
- Ferreira, G.S.; Moreira, C.R.L.; Kleinman, A.; Nader, E.C.G.P.; Gomes, B.C.; Teixeira, A.M.A.; Rocca, C.C.A.; Nicoletti, M.; Soares, J.C.; Busatto, G.F.; et al. Dysfunctional family environment in affected versus unaffected offspring of parents with bipolar disorder. Aust. N. Z. J. Psychiatry 2013, 47, 1051–1057. [Google Scholar] [CrossRef]
- Hillegers, M.H.J.; Burger, H.; Wals, M.; Reichart, C.G.; Verhulst, F.C.; Nolen, W.A.; Ormel, J. Impact of stressful life events, familial loading and their interaction on the onset of mood disorders: Study in a high-risk cohort of adolescent offspring of parents with bipolar disorder. Br. J. Psychiatry 2004, 185, 97–101. [Google Scholar] [CrossRef]
- Hanford, L.C.; Eckstrand, K.; Manelis, A.; Hafeman, D.M.; Merranko, J.; Ladouceur, C.D.; Graur, S.; McCaffrey, A.; Monk, K.; Bonar, L.K.; et al. The impact of familial risk and early life adversity on emotion and reward processing networks in youth at-risk for bipolar disorder. PLoS ONE 2019, 14. [Google Scholar] [CrossRef] [Green Version]
- Pan, L.A.; Goldstein, T.R.; Rooks, B.T.; Hickey, M.; Fan, J.Y.; Merranko, J.; Monk, K.; Diler, R.S.; Sakolsky, D.J.; Hafeman, D.; et al. The relationship between stressful life events and Axis i diagnoses among adolescent offspring of probands with bipolar and non-bipolar psychiatric disorders and healthy controls: The Pittsburgh Bipolar Offspring Study (BIOS). J. Clin. Psychiatry 2017, 78, e234–e243. [Google Scholar] [CrossRef] [Green Version]
- Duffy, A.; Alda, M.; Trinneer, A.; Demidenko, N.; Grof, P.; Goodyer, I.M. Temperament, life events, and psychopathology among the offspring of bipolar parents. Eur. Child Adolesc. Psychiatry 2007, 16, 222–228. [Google Scholar] [CrossRef]
- Joyce, K.; Thompson, A.; Marwaha, S. Is treatment for bipolar disorder more effective earlier in illness course? A comprehensive literature review. Int. J. Bipolar Disord. 2016, 4. [Google Scholar] [CrossRef] [Green Version]
- Van Meter, A.R.; Burke, C.; Youngstrom, E.A.; Faedda, G.L.; Correll, C.U. The Bipolar Prodrome: Meta-Analysis of Symptom Prevalence Prior to Initial or Recurrent Mood Episodes. J. Am. Acad. Child Adolesc. Psychiatry 2016, 55, 543–555. [Google Scholar] [CrossRef]
- DelBello, M.P. A Risk Calculator for Bipolar Disorder in Youth: Improving the Odds for Personalized Prevention and Early Intervention? J. Am. Acad. Child Adolesc. Psychiatry 2018, 57, 725–727. [Google Scholar] [CrossRef]
- Tsuchiya, K.J.; Byrne, M.; Mortensen, P.B. Risk factors in relation to an emergence of bipolar disorder: A systematic review. Bipolar Disord. 2003, 5, 231–242. [Google Scholar] [CrossRef]
- Koenders, M.A.; Giltay, E.J.; Spijker, A.T.; Hoencamp, E.; Spinhoven, P.; Elzinga, B.M. Stressful life events in bipolar i and II disorder: Cause or consequence of mood symptoms? J. Affect. Disord. 2014, 161, 55–64. [Google Scholar] [CrossRef]
- Birmaher, B.; Merranko, J.A.; Goldstein, T.R.; Gill, M.K.; Goldstein, B.I.; Hower, H.; Yen, S.; Hafeman, D.; Strober, M.; Diler, R.S.; et al. A Risk Calculator to Predict the Individual Risk of Conversion From Subthreshold Bipolar Symptoms to Bipolar Disorder I or II in Youth. J. Am. Acad. Child Adolesc. Psychiatry 2018, 57, 755–763.e4. [Google Scholar] [CrossRef]
- Hafeman, D.M.; Merranko, J.; Goldstein, T.R.; Axelson, D.; Goldstein, B.I.; Monk, K.; Hickey, M.B.; Sakolsky, D.; Diler, R.; Iyengar, S.; et al. Assessment of a person-level risk calculator to predict new-onset bipolar spectrum disorder in youth at familial risk. JAMA Psychiatry 2017. [Google Scholar] [CrossRef]
- Mourão-Miranda, J.; Oliveira, L.; Ladouceur, C.D.; Marquand, A.; Brammer, M.; Birmaher, B.; Axelson, D.; Phillips, M.L. Pattern recognition and functional neuroimaging help to discriminate healthy adolescents at risk for mood disorders from low risk adolescents. PLoS ONE 2012, 7. [Google Scholar] [CrossRef] [Green Version]
- Sugranyes, G.; Solé-Padullés, C.; de la Serna, E.; Borras, R.; Romero, S.; Sanchez-Gistau, V.; Garcia-Rizo, C.; Goikolea, J.M.; Bargallo, N.; Moreno, D.; et al. Cortical Morphology Characteristics of Young Offspring of Patients With Schizophrenia or Bipolar Disorder. J. Am. Acad. Child Adolesc. Psychiatry 2017, 56, 79–88. [Google Scholar] [CrossRef]
- Goodday, S.M.; Horrocks, J.; Keown-Stoneman, C.; Grof, P.; Duffy, A. Repeated salivary daytime cortisol and onset of mood episodes in offspring of bipolar parents. Int. J. Bipolar Disord. 2016, 4. [Google Scholar] [CrossRef] [Green Version]
- Singh, M.K.; Jo, B.; Adleman, N.E.; Howe, M.; Bararpour, L.; Kelley, R.G.; Spielman, D.; Chang, K.D. Prospective neurochemical characterization of child offspring of parents with bipolar disorder. Psychiatry Res. Neuroimaging 2013, 214, 153–160. [Google Scholar] [CrossRef] [Green Version]
- Geoffroy, P.A.; Scott, J. Prodrome or risk syndrome: What’s in a name? Int. J. Bipolar Disord. 2017, 5, 7. [Google Scholar] [CrossRef] [Green Version]
- Jacka, F.N.; Mykletun, A.; Berk, M. Moving towards a population health approach to the primary prevention of common mental disorders. BMC Med. 2012, 10. [Google Scholar] [CrossRef] [Green Version]
- Berk, M.; Moylan, S.; Jacka, F.N. A Royal gift to prevention efforts. Aust. N. Z. J. Psychiatry 2014, 48, 110–111. [Google Scholar] [CrossRef]
- Etain, B.; Mathieu, F.; Henry, C.; Raust, A.; Roy, I.; Germain, A.; Leboyer, M.; Bellivier, F. Preferential association between childhood emotional abuse and bipolar disorder. J. Trauma. Stress 2010, 23, 376–383. [Google Scholar] [CrossRef]
- Rakofsky, J.J.; Ressler, K.J.; Dunlop, B.W. BDNF function as a potential mediator of bipolar disorder and post-traumatic stress disorder comorbidity. Mol. Psychiatry 2012, 17, 22–35. [Google Scholar] [CrossRef] [Green Version]
- Librenza-Garcia, D.; Suh, J.S.; Watts, D.P.; Ballester, P.L.; Minuzzi, L.; Kapczinski, F.; Frey, B.N. Structural and Functional Brain Correlates of Neuroprogression in Bipolar Disorder. Curr. Top. Behav. Neurosci. 2020. [Google Scholar] [CrossRef]
- Harnett, N.G.; Goodman, A.M.; Knight, D.C. PTSD-related neuroimaging abnormalities in brain function, structure, and biochemistry. Exp. Neurol. 2020, 330, 113331. [Google Scholar] [CrossRef]
- Barron, E.; Sharma, A.; Le Couteur, J.; Rushton, S.; Close, A.; Kelly, T.; Grunze, H.; Ferrier, I.N.; Le Couteur, A. Family environment of bipolar families: A UK study. J. Affect. Disord. 2014, 152–154, 522–525. [Google Scholar] [CrossRef]
- Tole, F.; Kopf, J.; Schröter, K.; Palladino, V.S.; Jacob, C.P.; Reif, A.; Kittel-Schneider, S. The role of pre-, peri-, and postnatal risk factors in bipolar disorder and adult ADHD. J. Neural. Transm. 2019, 126, 1117–1126. [Google Scholar] [CrossRef]
- Miklowitz, D.J.; Schneck, C.D.; George, E.L.; Taylor, D.O.; Sugar, C.A.; Birmaher, B.; Kowatch, R.A.; DelBello, M.P.; Axelson, D.A. Pharmacotherapy and family-focused treatment for adolescents with bipolar I and II disorders: A 2-year randomized trial. Am. J. Psychiatry 2014, 171, 658–667. [Google Scholar] [CrossRef] [Green Version]
- Miklowitz, D.J.; Chung, B. Family-Focused Therapy for Bipolar Disorder: Reflections on 30 Years of Research. Fam. Process 2016. [Google Scholar] [CrossRef] [Green Version]
- Kessing, L.V.; Vradi, E.; McIntyre, R.S.; Andersen, P.K. Causes of decreased life expectancy over the life span in bipolar disorder. J. Affect. Disord. 2015, 180, 142–147. [Google Scholar] [CrossRef]
- Correll, C.U.; Solmi, M.; Veronese, N.; Bortolato, B.; Rosson, S.; Santonastaso, P.; Thapa-Chhetri, N.; Fornaro, M.; Gallicchio, D.; Collantoni, E.; et al. Prevalence, incidence and mortality from cardiovascular disease in patients with pooled and specific severe mental illness: A large-scale meta-analysis of 3,211,768 patients and 113,383,368 controls. World Psychiatry 2017, 16, 163–180. [Google Scholar] [CrossRef] [Green Version]
- Bernardini, F.; Attademo, L.; Trezzi, R.; Gobbicchi, C.; Balducci, P.M.; Del Bello, V.; Menculini, G.; Pauselli, L.; Piselli, M.; Sciarma, T.; et al. Air pollutants and daily number of admissions to psychiatric emergency services: Evidence for detrimental mental health effects of ozone. Epidemiol. Psychiatr. Sci. 2019, 29, e66. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| References | Country | Study Design | Sample | Assessment Instruments | Considered Environmental Factors | Results |
|---|---|---|---|---|---|---|
| Goldstein et al., 2009 | USA | 4-year longitudinal study | 446 outpatients and inpatients (7–17) with BD-I, BD-II or BD-NOS according to DSM-IV (Course and Outcome of Bipolar Illness in Youth study) | DSM-IV K-SADS-P K-SADS-PL K-SADS-MRS CBQ FACES-II LEC FHS GIS C-GAS Clinical interview | SES Living with both parents History of physical and sexual abuse Family conflict Family closeness Family adaptability Family stress | BD youth with current suicidal ideation (n = 160, 36%) reported more conflict with their mother (mean CBQ score 4.9 ± 5.2 vs. 6.0 ± 5.4, p = 0.04) and less family adaptability (mean FACES-II score 44.3 ± 9.1 vs. 42.4 ± 9.2). A significantly higher rates of stressful family events was also reported, in particular: illness of a family member (40% vs. 28%, p = 0.04), death of a family member 35% vs. 24%, p = 0.03), increased absence of a parent from home (27% vs. 14%, p < 0.01), and trouble with a sibling (51% vs. 39%; p = 0.03). |
| Romero et al., 2009a | USA | Cross-sectional study with data from a 6-year period | 446 outpatients and inpatients (7–17) with BD-I, BD-II or BD-NOS according to DSM-IV (Course and Outcome of Bipolar Illness in Youth study) 65 youths with depression/anxiety disorders (DEP/ANX group) 65 HCs youths | K-SADS-PL LEC | Negative dependent, independent, and uncertain life events | Subjects with BD reported a similar rate of NLEs as DEP/ANX group (mean number 5.5 ± 0.3 vs. 6.1 ± 0.5, NS). Both groups had more NLEs than HCs (mean number 5.5 ± 0.3 vs. 2.3 ± 0.2, p < 0.001). NLEs were associated with lower socioeconomic status (p = 0.005), non-intact family (p = 0.003), and psychiatric comorbidity, namely conduct disorders (p = 0.003), anxiety disorders (p = 0.02), ADHD (p = 0.03), and ODD (p = 0.03). |
| Romero et al., 2009b | USA | Cross-sectional study | 446 outpatients and inpatients (7–17) with BD-I, BD-II or BD-NOS according to DSM-IV (Course and Outcome of Bipolar Illness in Youth study) | K-SADS-PL, PTSD section FHS Hollingshead four-factor scale | SES Intact family History of physical and sexual abuse | Sexual and/or physical abuse were found to be common (n = 92, 20.6%; physical abuse: n = 40, 9%, sexual abuse: n = 30, 7%, both: n = 22, 5%). Physical abuse was associated with PTSD (OR 10.4, CI 3.2–34.4), non-intact family (OR 4.2, CI 1.5–11.7), first-degree family history of mood disorder (OR 3.4, CI 1.1–10.6), and psychosis (OR 2.3, CI 1.1–5). Sexual abuse was associated with PTSD (OR 7.8, CI 2–30.4). Subjects with both types of abuse were older (p = 0.015), with longer illness duration (p = 0.01), non-intact family (p = 0.003), and greater prevalence of PTSD (<0.001) and CD (p = 0.03) as compared with the non-abused group. |
| Bakare et al., 2011 | Nigeria | One-year cross-sectional study | 46 outpatient adolescents (15–18) with BD-I or BD-II diagnosed according to DSM-IV | Socio-demographic questionnaire C-GAS Clinical interview | Marital status of the parents Premorbid peer relationship Religion activities History of sexual risky behavior Relationship with siblings Substance use | Poor premorbid peer relationship (p < 0.001), poor relationship with siblings (p < 0.001), low level of religion activities (p < 0.001), and history of sexual risky behavior (p < 0.001), comorbidities (p < 0.001), and number of hospital admissions (p < 0.001) were significantly associated with lower functioning. |
| References | Country | Study Design | Sample | Assessment Instruments | Considered Environmental Factors | Results |
|---|---|---|---|---|---|---|
| Hillegers et al., 2004 | The Netherlands | Cohort study (preliminary findings from a first 16-month assessment) | 140 adolescents (12–21), offspring of 86 BD parents (Dutch Bipolar Offspring Study) | DSM-IV K-LEDS FH-RDC Life event load (time-dependent variable calculated according to four different models) | Stressful life events | 27% of youth included in the sample developed a mood disorder during follow-up (median age 14). The life event load, not depending on the model, was associated with a 10% increased risk for mood disorders (HR = 1.1), with no modification of the significant relationship after controlling for the familial component. |
| Duffy et al., 2006 | Canada | Cross-sectional study | 126 (8–25) youths, offspring of BD subjects. Parents were stratified according to lithium response (responders = 36, non-responders = 27) | K-SADS-PL Semi-structured interview by Goodyear et al. for life events, difficulties, and permanent losses EAS | Stressful life events Early permanent losses | The number of NLEs was higher in affected BD offspring when compared to unaffected ones (mean number of NLEs 1.50 ± 1.42 vs. 0.76 ± 0.97, p = 0.03). This result was not replicated for early losses. This relationship was detected to be mediated by emotionality, which contributed to lifetime mood disorders at the stepwise regression analysis (OR 2.47, 95% CI 4.56–1.34, p < 0.01). |
| Reichart et al., 2007 | The Netherlands | Cross-sectional study (third, 5-year measurement of a longitudinal prospective study) | 129 offspring of 80 BD parents (Dutch Bipolar Offspring Study) 1122 young adults from the general population | DSM-IV K-SADS-PL EMBU Clinical history features for BD course characteristics | Parental rearing behavior Parental psychopathology | Offspring with a father affected by BD perceived more rejection than those with a mother with BD (mean scores at the EMBU Rejection subscale: 9.33 vs. 8.19, p < 0.05). The development of psychopathology in BD offspring was associated with higher rates of parent rejecting (unstandardized coefficient B = 2.82 for father, B = 1.29 for mother, p = 0.05). |
| Ferreira et al., 2013 | Brazil | Cross-sectional study | 46 subjects (18–65) diagnosed with BD-I according to DSM-IV and their offspring (6–17) 30 healthy subjects (18–65) and their offspring (6–17) | K-SADS-PL FES | Family environment | BD families were characterized by lower cohesion (p = 0.001), intellectual-cultural orientation (p = 0.005), active-recreational orientation (p = 0.002), moral-religious emphasis (p = 0.004) and organization (p < 0.001), and higher conflict (p < 0.001). Offspring of BD parents presented more frequent development of Axis I disorders (BD = 12.8%). In the affected group, lower cohesion (p = 0.003), intellectual-cultural orientation (p = 0.01) and active-recreational orientation (p = 0.007) and higher conflict (p = 0.001) and control (p = 0.01) were detected. |
| Kemner et al., 2015 | The Netherlands | Cohort study with a 12-year follow-up | 140 adolescents (12–21), offspring of 86 BD parents (Dutch Bipolar Offspring Study) | DSM-IV K-SADS-PL LEDS TCI UCL Short-EMBU | Stressful life events | 24% BD offspring developed BD, with a 54% incidence of mood disorders during follow-up. First mood episode was associated to the total load of stressful life events (HR = 1.14). Subsequent episodes, although to a lesser extent, were as well associated with life events (HR = 1.12). Passive coping style increased the risk of mood episode onset and recurrent episodes HR = 1.23, HR = 1.18), but also altered the effect of life events on mood disorders. |
| Doucette et al., 2016 | Canada | Cohort study with a 25-year follow-up | 233 offspring (mean age 16.6) of BD parents | DSM-IV K-SADS-PL AMI CECA.Q EAS LEQ Hollingsead SES Scale Self-report measures of temperament and early adversities | Early childhood adversity Emotionality Exposure to parental BD Stressful life events | Perceived maternal neglect predicted mood and anxiety disorders onset in high-risk adolescents (HR = 1.1, 95% CI 1.0–1.2), even after adjusting for further factors, e.g., exposure to parental BD. High offspring emotionality appeared to be as well associated to the development of mood disorders (HR = 1.7, 95% CI 1.9–3.1), also being the possible mediator of the relationship between maternal neglect and the development of psychopathology. |
| Pan et al., 2017 | USA | Cross-sectional study of a sample from a 7-year cohort study | Offspring (13–18) of parents affected by BD (n = 269), non-BD Axis I disorders (n = 88), and offspring of HCs (n = 81) (Pittsburgh Bipolar Offspring Study) | DSM-IV K-SADS-PL SLES | Stressful live events during the year before evaluation | Offspring of BD probands had greater number of severe stressful life events than HCs offspring (mean (SE) 13.89 (0.05) vs. 10.22 (0.08), p = 0.001), but not non-BD offspring. Total number and severity of negative stressful life events was associated with higher rates of Axis I disorders in both BD and non-BD affected probands. |
| Lau et al., 2018 | Australia | Cross-sectional study of a sample from a cohort study | 146 offspring (12–21): High-risk (n = 90) BD offspring and control (n = 56) offspring (Bipolar Kids and Sibs Study) | DSM-IV-TR K-SADS-BP FIGS DIGS v.4 FACES-II PBI CBCL/ 6—18 YSR ABCL/18–59 ASR | Family cohesion Parental bonding | BD offspring presented significantly higher internalizing and externalizing problems, both on self- (Int: M (SE) 55.95 (1.31) vs. 48.27 (1.74), p = 0.001, Ext: M (SE) 53.74 (1.19) vs. 49.00 (1.52), p = 0.03) self- and parent- (Ext: 56.37 (4.71) vs. 47.17 (6.36), p = 0.029) reports. Internalizing problems displayed a significant association with low maternal (p = 0.025) and paternal (p = 0.025) care, whilst externalizing problems were associated with low maternal care (p = 0.011). Family environment-related factors did not mediate the relationship between high-risk BD state and dimensional psychopathology. |
| Hanford et al., 2019 | USA | Cross-sectional study of samples from larger cohort studies | 22 offspring (mean age 14.1 ± 2.4 years) of BD parents, 22 offspring of healthy controls (mean age 13.7 ± 1.8 years) (Pittsburgh Bipolar Offspring Study, Longitudinal Assessment of Manic Symptoms) | DSM-IV K-SADS-PL K-SADS-MRS CALS SCARED C-GAS SLES Predictive 5-year risk calculator MRI for investigation of emotional and reward networks | Stressful live events | Higher risk calculator score showed greater positive associations between number of recent exposure to negative stressful life events and activity within bilateral fusiform gyri (right: Z = 5, p < 0.001, left: Z = 3.6, p < 0.001) and the right amygdala (Z = 4.1, p < 0.001). Risk calculator score alone showed positive relationships with activity in bilateral lateral occipital cortices (right: Z = 3.7; p < 0.001; left: Z = 4.0 p = 0.001). |
| Koenders et al., 2020 | The Netherlands | 12-year cohort study | 102 offspring (12–21) of parents with BD (Dutch Bipolar Offspring Study) | DSM-IV K-SADS-PL QFP CTQ | Childhood trauma Family functioning | 52.9% (n = 54) offspring developed a mood disorder, of which 12.7% (n = 24) developed BD. Emotional maltreatment was significantly associated with mood disorder onset (HR = 1.07, 95% CI 1.18–2.82, p = 0.007). Family functioning, nor its subscales, shows significant associations with mood disorder onset (HR = 1.01, 95% CI: 0.89–1.14, p = 0.889. |
| Author(s) (Year) | Selection | Comparability | Outcome | Total Stars | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| S1 | S2 | S3 | S4 | C1a | C1b | O1 | O2 | O3 | ||
| Hillegers et al., (2004) | * | * | * | * | * | * | * | 7 | ||
| Duffy et al., (2007) | * | * | * | * | * | * | * | * | 8 | |
| Goldstein et al., (2009) | * | * | * | * | * | 5 | ||||
| Kemner et al., (2015) | * | * | * | * | * | * | * | * | 8 | |
| Doucette et al., (2016) | * | * | * | * | * | * | 6 | |||
| Koenders et al., (2020) | * | * | * | * | * | * | * | 7 | ||
| Author(s) (Year) | Selection | Comparability | Outcome | Total Stars | |||||
|---|---|---|---|---|---|---|---|---|---|
| S1 | S2 | S3 | S4 | C1a | C1b | O1 | O2 | ||
| Reichart et al., (2007) | * | * | ** | * | ** | * | 8 | ||
| Romero et al., (2009a) | * | ** | * | * | 5 | ||||
| Romero et al., (2009b) | * | ** | * | * | ** | * | 8 | ||
| Bakare et al., (2011) | * | ** | ** | * | 6 | ||||
| Ferreira et al., (2013) | * | ** | * | * | 5 | ||||
| Pan et al., (2017) | * | ** | * | * | ** | * | 8 | ||
| Lau et al., (2018) | * | ** | * | * | * | * | 7 | ||
| Hanford et al., (2019) | * | ** | * | ** | * | 7 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Menculini, G.; Balducci, P.M.; Attademo, L.; Bernardini, F.; Moretti, P.; Tortorella, A. Environmental Risk Factors for Bipolar Disorders and High-Risk States in Adolescence: A Systematic Review. Medicina 2020, 56, 689. https://doi.org/10.3390/medicina56120689
Menculini G, Balducci PM, Attademo L, Bernardini F, Moretti P, Tortorella A. Environmental Risk Factors for Bipolar Disorders and High-Risk States in Adolescence: A Systematic Review. Medicina. 2020; 56(12):689. https://doi.org/10.3390/medicina56120689
Chicago/Turabian StyleMenculini, Giulia, Pierfrancesco Maria Balducci, Luigi Attademo, Francesco Bernardini, Patrizia Moretti, and Alfonso Tortorella. 2020. "Environmental Risk Factors for Bipolar Disorders and High-Risk States in Adolescence: A Systematic Review" Medicina 56, no. 12: 689. https://doi.org/10.3390/medicina56120689